
Abstract
Background
Morphine is commonly used in ventilated neonates as an analgesic with many side effects like respiratory depression and hypotension. Only a few studies have investigated morphine’s influence on biliary tract dynamics. Therefore, we planned this study to find out the relationship between morphine and liver function in preterm neonates.
Methods
This retrospective study was conducted at the Women’s Wellness and Research Centre by reviewing the case records of neonates admitted between 01st January 2015 and 31st December 2020. Preterm infants on mechanical ventilation, between gestational ages (GA) ≥24 and ≤37 weeks, were included in the study. Participants were divided into two groups according to morphine use, and liver function test values were compared, including direct (DB), total bilirubin (TB), alanine transaminase (ALT), and aspartate transaminase (AST).
Results
The study comprised 133 preterm newborns; out of them, 73 received morphine (Group A) and 60 did not receive it (Group B). The mean GA was 29.90 ± 5.18 weeks, and birth weight was 1250 ± 418 grams. At admission, DB levels were higher in group B than in group A (54.71 ± 50.0 vs. 36.77 ± 48.53, p = .038). However, the peak and discharge values were higher in group A than in group B (p = .001 and p = .196, respectively). The peak AST, DB, and TB values were higher in group A.
Conclusion
The present study showed the impact of morphine on liver function in preterm neonates and the possibility of morphine hepatotoxicity. Clinicians should use morphine cautiously in preterm neonates to avoid the risk of developing cholestasis and hepatotoxicity.
Introduction
Cholestasis is caused by decreased bile flow and is diagnosed clinically as a direct bilirubin concentration of more than 20% of total bilirubin when total bilirubin exceeds 5 mg/dL or when the conjugated bilirubin level is above the typical ranges for newborns within the first 5 days of life. 1 Neonatal cholestasis is estimated to occur in one out of every 2500 live births. The causes include both intrahepatic and extrahepatic illnesses such as anatomic blockages (e.g., cholelithiasis, choledochal cysts, and biliary atresia), infections, genetic abnormalities, drugs (e.g., morphine), hypoxia/ischemia, and parenteral nutrition-related cholestasis. 1
Pain management in neonatal intensive care units (NICUs) uses pharmacological interventions, such as acetaminophen and opioids, for more severe pain and non-pharmacological techniques, such as sucrose, nursing, swaddling, and skin-to-skin contact, for mild discomfort. Particularly during invasive surgeries, morphine is frequently used to manage extreme discomfort. It provides efficient analgesia by binding to opioid receptors in the central nervous system. 2 In neonates, morphine has a complicated pharmacology. Its pharmacokinetics are considerably distinct from those of older children and adults due to underdeveloped liver and kidney function, which results in a longer half-life and drug accumulation. 2
Morphine is predominantly metabolized in the liver, generating two primary metabolites: morphine-3-glucuronide (M3G) and morphine-6-glucuronide (M6G). At high levels, M3G may lead to neurotoxicity even though it has no analgesic effect. On the other hand, M6G has analgesic effects that can intensify the pain-relieving properties of morphine. 3 Several adverse effects are linked to morphine use in newborns, including respiratory depression, excessive sedation, decreased gastrointestinal motility that causes constipation and feeding intolerance, possible cardiovascular abnormalities like hypotension and bradycardia, and neurobehavioral problems. 4
Morphine has been associated with significant gallbladder dilation, suggesting its adverse effects on the biliary system, including biliary stasis, particularly in infants. Morphine and fentanyl can decrease the width of the common bile duct while simultaneously increasing pressure inside the biliary duct and the sphincter of Oddi. 5 Gallbladder dilatation may also be exacerbated by total parenteral nutrition (TPN). TPN is the most used therapy in the NICU for providing nutritional support to ill neonates; however, it has adverse effects, including increased gallbladder dilatation. TPN and morphine together may affect drug processing and increase the risk of gallbladder-related complications. 6
Research indicates that preterm infants receiving morphine may require extended time to achieve full enteral feeds due to morphine’s inhibitory effects on mature gut neuromuscular activity. 7 Since preterm gut maturation depends on neuromuscular activity, delays in structural integrity could increase the risk of necrotizing enterocolitis (NEC). 8 Menon et al. reported that morphine delayed the initiation and attainment of full enteral feeding in preterm infants. However, their study also concluded that morphine did not increase the risk of acquired gastrointestinal pathologies. 9
TPN-associated liver disease is a treatable cause of neonatal cholestasis. Hepatic manifestations include cholestasis, steatosis, bile duct proliferation, portal fibrosis, and cirrhosis. Management strategies encompass early initiation of enteral feeding, avoidance of excessive intravenous calories and proteins, utilization of neonatal amino acid formulations, and administration of ursodeoxycholic acid.10–13 Nevertheless, studies elucidating the precise mechanisms or effects of morphine on neonatal liver function remain scarce.
We encountered cholestasis in many extremely premature neonates admitted to NICU and received morphine; however, only a few studies are available investigating morphine’s influence on biliary tract dynamics. Therefore, we planned this retrospective study to find out the relationship between morphine and liver function in preterm neonates.
Methods
This retrospective study was conducted in the neonatal unit at the Women’s Wellness and Research Centre (WWRC), one of the region’s largest units, equipped with cutting-edge medical facilities and a multidisciplinary care team. The case records of neonates admitted to the NICU between 01st January 2015 and 31st December 2020 were reviewed. Preterm infants {gestational age (GA) ≥24 weeks to ≤37 weeks)} admitted to the NICU for mechanical ventilation or intubated after admission were included in the study. Neonates with gastrointestinal obstructions, congenital biliary malformations, significant congenital cardiovascular defects, hypoxia, neonatal hepatitis, or direct hyperbilirubinemia were excluded from the study.
The following information was collected from CERNER electronic patient charts using a data collection sheet: demographic details, TPN, and morphine use, and liver function tests (LFTs) including prothrombin time (PT), total protein (TP), alkaline phosphatase (ALP), albumin, gamma-glutamyl transferase (GGT), alanine transaminase (ALT), aspartate transaminase (AST), direct bilirubin (DB), and total bilirubin (TB).
For the morphine administration, the standard dosage ranged from 100 to 150 mcg/kg administered over 1 hour, followed by a continuous infusion of 10–20 mcg/kg/hr. The dosages vary based on clinical needs, such as higher doses during surgeries for acute pain management and lower, continuous doses for long-term sedation, especially in ventilated babies. These dosages are calculated based on the baby’s weight to ensure safe and effective administration. Participants were divided into two groups: Group A included neonates who received morphine, and Group B consisted of those who did not. Additional analysis was done after dividing the participants into two groups according to GA (group C: <30 weeks and group D: ≥30 weeks). Morphine dosages were not adjusted based on liver function as the correlation between morphine metabolism and liver function was not evident from the available evidence at that time.
Statistical analysis
Separate sample t-tests were performed to compare biochemical indicators among groups based on gestational age, morphine use, and TPN administration. Means and standard deviations were calculated for every parameter, and t-values and p-values were provided. Statistical significance was defined as a p-value of <.05.
Results
The study comprised 133 preterm newborns; out of them, 73 received morphine (Group A) and 60 did not receive it (Group B). The mean GA of the study population was 29.90 ± 5.18 weeks, and the mean birth weight was 1250 ± 418 grams. The mean GA of the newborns who received morphine was higher (31.1 ± 4.16 vs 28.8 ± 5.73 weeks) than those who did not (unpaired t-test = 2.450, p = .016). For the neonates who received morphine, the mean duration was 27.39 ± 5.35 days, and the median duration was only 1 day (range: 0–320 days).
Liver function tests among neonates who received morphine (n = 73) versus those who did not receive morphine (n = 60).
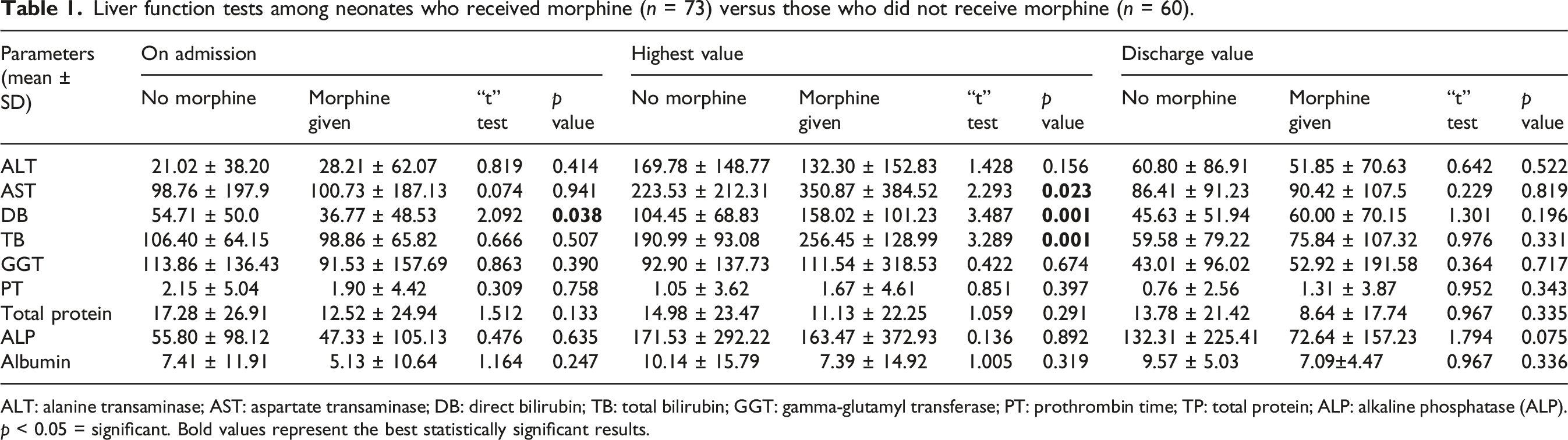
ALT: alanine transaminase; AST: aspartate transaminase; DB: direct bilirubin; TB: total bilirubin; GGT: gamma-glutamyl transferase; PT: prothrombin time; TP: total protein; ALP: alkaline phosphatase (ALP).
p < 0.05 = significant. Bold values represent the best statistically significant results.
Liver function parameters in neonates with gestational age <30 weeks (n = 79) and >30 weeks (n = 54).
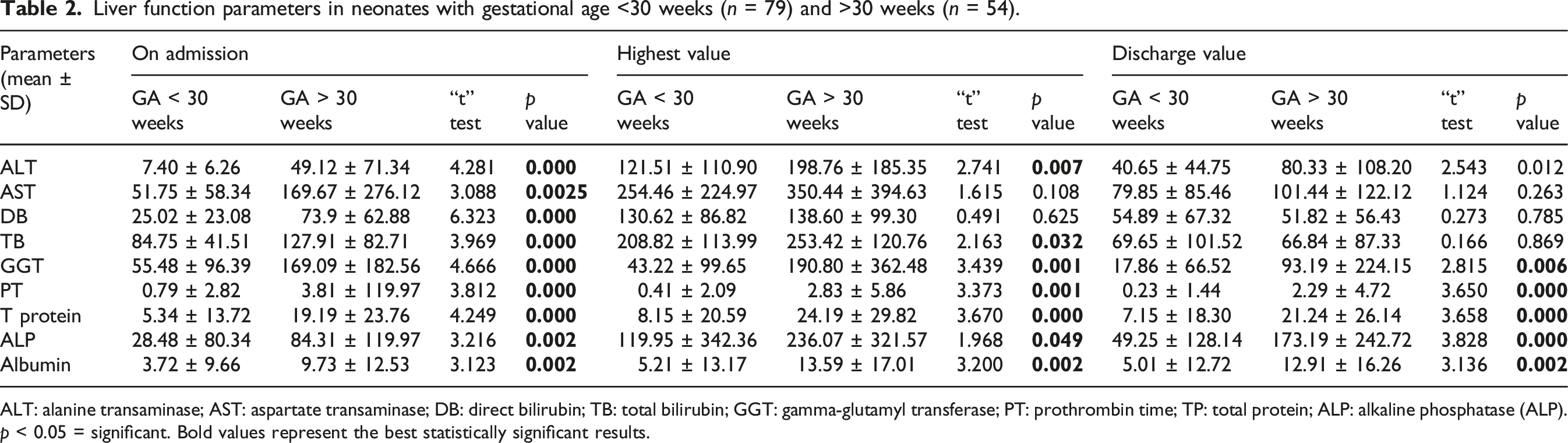
ALT: alanine transaminase; AST: aspartate transaminase; DB: direct bilirubin; TB: total bilirubin; GGT: gamma-glutamyl transferase; PT: prothrombin time; TP: total protein; ALP: alkaline phosphatase (ALP).
p < 0.05 = significant. Bold values represent the best statistically significant results.
Liver function tests in neonates with gestational age <30 weeks versus >30 weeks amongst those who received morphine.
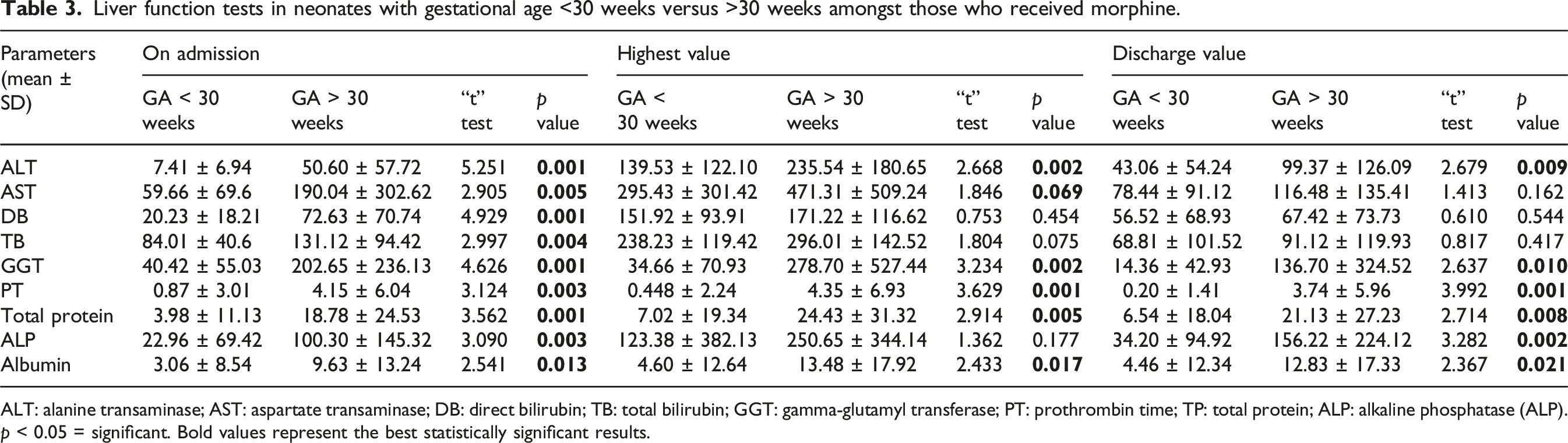
ALT: alanine transaminase; AST: aspartate transaminase; DB: direct bilirubin; TB: total bilirubin; GGT: gamma-glutamyl transferase; PT: prothrombin time; TP: total protein; ALP: alkaline phosphatase (ALP).
p < 0.05 = significant. Bold values represent the best statistically significant results.
Liver function parameters in neonates who received morphine (n = 23) and those who did not (n = 31) amongst neonates with gestational age >30 weeks.
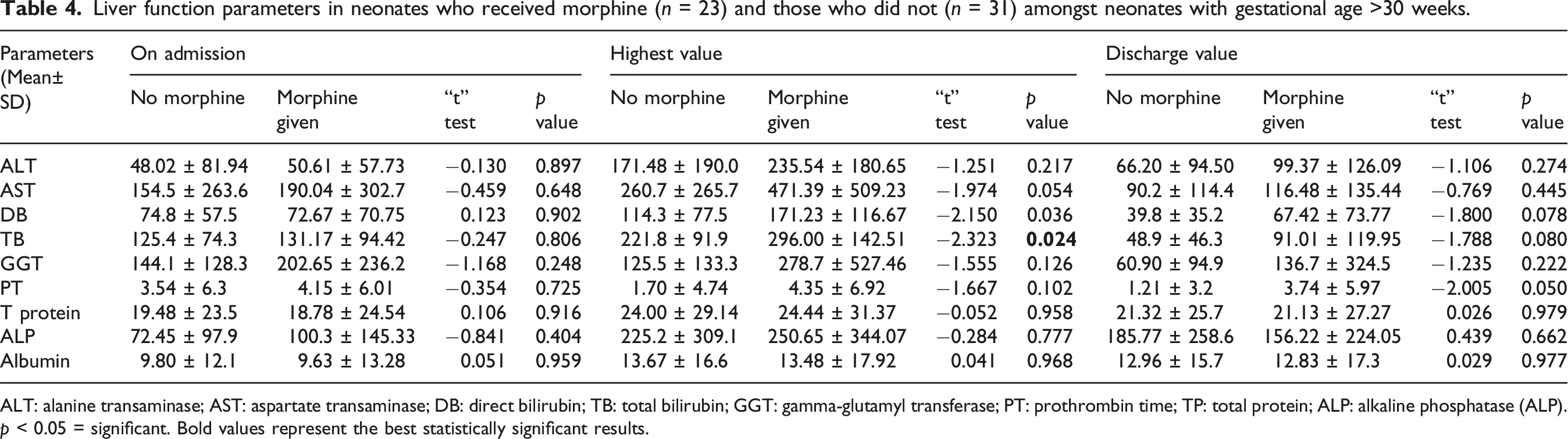
ALT: alanine transaminase; AST: aspartate transaminase; DB: direct bilirubin; TB: total bilirubin; GGT: gamma-glutamyl transferase; PT: prothrombin time; TP: total protein; ALP: alkaline phosphatase (ALP).
p < 0.05 = significant. Bold values represent the best statistically significant results.
Liver function parameters in neonates who received morphine (n = 50) and those who did not (n = 29) amongst neonates with gestational age <30 weeks.
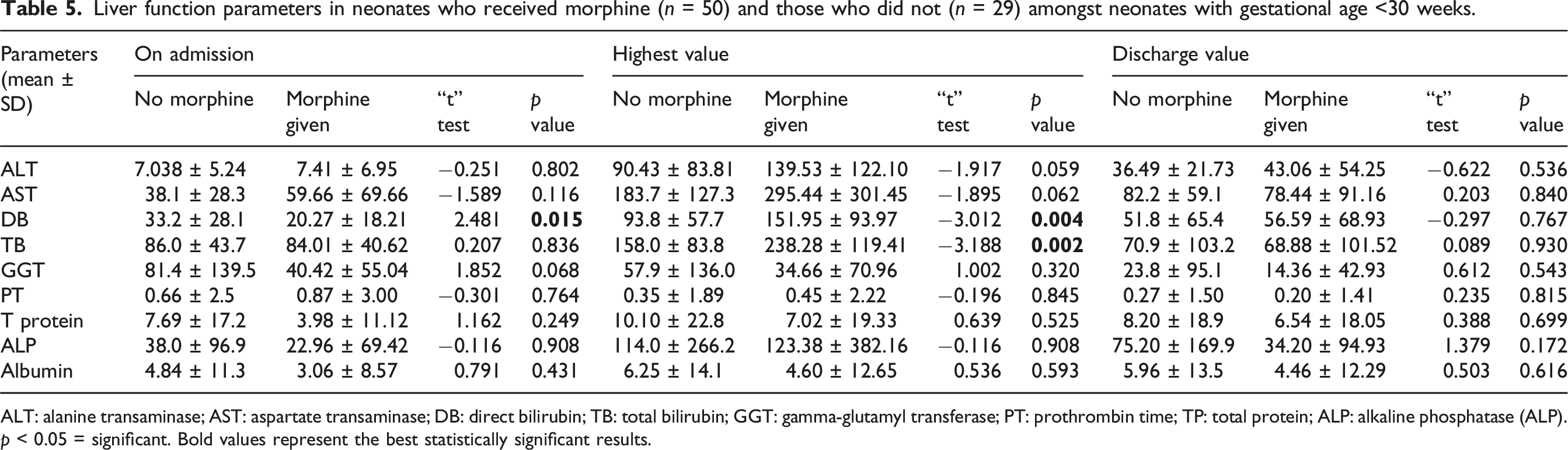
ALT: alanine transaminase; AST: aspartate transaminase; DB: direct bilirubin; TB: total bilirubin; GGT: gamma-glutamyl transferase; PT: prothrombin time; TP: total protein; ALP: alkaline phosphatase (ALP).
p < 0.05 = significant. Bold values represent the best statistically significant results.
Liver function parameters among neonates who received TPN (n = 117) versus those who did not receive TPN (n = 16).
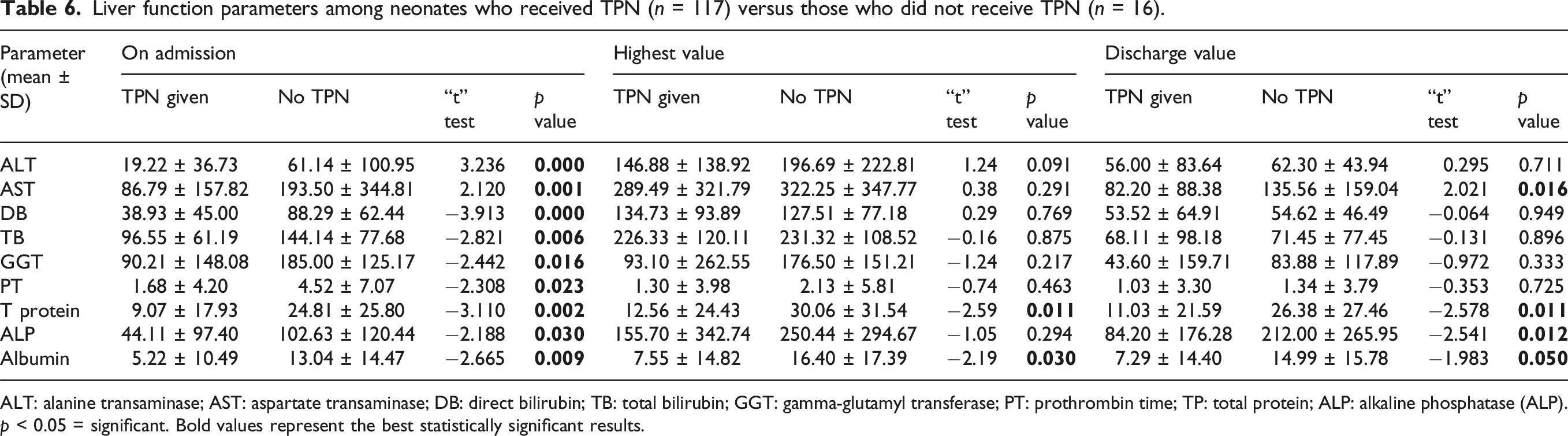
ALT: alanine transaminase; AST: aspartate transaminase; DB: direct bilirubin; TB: total bilirubin; GGT: gamma-glutamyl transferase; PT: prothrombin time; TP: total protein; ALP: alkaline phosphatase (ALP).
p < 0.05 = significant. Bold values represent the best statistically significant results.
Discussion
Our study’s findings demonstrated that morphine might have a substantial effect on neonates’ liver function, as suggested by significantly higher levels of AST and direct and total bilirubin in neonates receiving morphine than in those who did not receive morphine. Of those neonates who received morphine, LFT parameters were significantly higher in neonates with GA >30 weeks than in neonates with GA <30 weeks at all points of time. group showed a significant rise in ALT and AST, indicating elevated liver enzyme levels. However, a similar trend was also observed in the overall study cohort, irrespective of the morphine exposure. Higher levels of LFT parameters in older neonates suggest a relationship between increasing liver maturity and increasing GA.
Morphine is a commonly prescribed medication in NICU to provide analgesia and sedation in neonates on mechanical ventilators or undergoing acute painful procedures (e.g., chest drain insertion and central line placement). However, different studies have shown variable results on its efficacy and even harmful effects such as bradycardia, hypotension, and respiratory depression.14,15 A recent Cochrane review reported insufficient evidence regarding the effects of opioids (morphine or fentanyl) on pain and neurodevelopmental outcomes at 18–24 months, and their use had little or no effect in reducing the duration of mechanical ventilation and neonatal mortality. 16 Another Cochrane review showed an increase in apnea episodes when opioids were used for the procedure pain in neonates. 17
However, we could not find any neonatal study assessing the effect of morphine therapy on hepatic functions or cholestasis in preterm neonates, and this is the first study trying to evaluate this aspect of morphine therapy. Elevated enzyme and bilirubin levels may suggest hepatic injury or cholestasis, although a long-term follow-up is necessary to see if these deranged liver functions transform into clinically significant liver disease. Our findings raise the question of whether morphine usage is hepatotoxic due to rising enzyme and bilirubin levels; thus, precautions should be taken while considering morphine use in the most susceptible group.
Morphine is a µ and κ receptor agonist that produces analgesia, sedation, and euphoria. In the preterm infant, the half-life of morphine ranges from 6 to 12 hours and is inversely related to gestational age. Accumulation is associated with prolonged administration; hence, the overall management of doses should be cautious, particularly in neonates being treated with therapeutic hypothermia. Metabolism majorly occurs via glucuronidation, which results in morphine-3-glucuronide and morphine-6-glucuronide, the latter being an active analgesic. The pharmacokinetics significantly differ with age and weight, making individualized dosing imperative due to increased clearance with age and disease severity. Clinical monitoring shall achieve maximum effect in terms of pain relief with minimal adverse effects.3,18
The study by Bouwmeester et al. examined 197 pediatric patients from a heterogeneous population, giving insight into morphine pharmacokinetics and the need for dosing during major surgery. It shows that the youngest neonates, under 4 weeks of age, require significantly less morphine; indeed, 38% needed supplementary doses compared to older infants and children. Plasma concentrations of morphine and its metabolites, M3G and M6G, varied by age, which suggests that the younger patients have higher levels, therefore indicating developmental differences in metabolism. Age, the total bilirubin level, and the surgical stress score were significant factors in the dosage of morphine. The younger patients required a lesser dose but had higher plasma concentrations of morphine, which suggested a reduced capability for its clearance. 19
There is a direct contribution of opioids like morphine to liver disease. Morphine is metabolized in the liver, mainly through glucuronidation by the enzyme UGT2B7, a process that can worsen the disease since it involves lipid oxidation and mitochondrial oxidative injury. Chronic exposure to morphine has been shown to cause liver injury, including sinusoidal dilatation, necrosis, hemorrhage, and microvesicular steatosis in rat hepatocytes. Chronic users in humans show elevated levels of biochemical markers such as ALT and LDH, which point toward the hepatotoxic effects exerted by morphine and its metabolites. Opioids can also cause severe constipation, which increases the permeability of the intestines, thereby increasing bacterial translocation; thus, it adds to liver injury. Morphine has been associated with changes in cholesterol and bile acid metabolism; however, the mechanisms of action remain unknown. Further studies should be performed to clarify the direct and indirect effects of morphine on liver disease and distinguish them from those possibly caused by other opioid-related liver conditions, such as viral hepatitis. 20
Samarghandian et al., conducted research in which the impact of chronic morphine treatment on liver function and oxidative stress was studied in male Sprague-Dawley rats. Serum ALT, AST, and LDH levels were elevated in the morphine-treated rats compared to control rats, indicating its hepatotoxic effects. Malondialdehyde (MDA), a marker of lipid peroxidation, levels were increased in morphine-treated rats compared to the controls, suggesting the possible risk to hepatic function with long-term use of morphine. 21
In their study, Naderi et al. included 32 newborns, aged between 26 and 38 weeks, requiring mechanical ventilation in the NICU. Those receiving morphine at 100 mcg/kg as a loading dose followed by an infusion of 12 mcg/kg/hour showed significant dilation of the gallbladder; however, length was unaffected, but width, depth, and volume were much larger, and this may suggest its possible effects on biliary flow. The biliary system was shown to experience alteration, including gallstone formation and reduced diameter of the common bile duct. There were no significant changes in the common bile duct diameter. This study highlights the problems in the use of morphine in preterm neonates, especially those on TPN, and it requires cautious application within the NICU setting. 4
This study investigated the effects of morphine on liver function in two gestational age groups (<30 weeks and ≥30 weeks) using liver function tests. A previous study examined morphine clearance and its effects in newborn infants across varying gestational ages. In that study, morphine administration was assessed in infants with gestational ages ranging from 24 to 41 weeks over 60 hours. The results indicated that increased morphine concentrations did not correlate with morphine administration but were associated with reduced gastrointestinal motility. 22
Smits et al. reviewed the pharmacological aspects, especially analgesic and sedative effects in neonates, to assess their safe and effective clinical application. Their analysis of neonates with untreated stress or pain, as well as those treated with opioids (including morphine) and paracetamol, revealed that opioid use can lead to both short- and long-term adverse effects. These effects include prolonged ventilation, delayed enteral feeding, hypotension, and negative impacts on neurocognitive development, pain perception, and behavioral changes. 23
Parenteral nutrition-associated cholestasis (PNAC) is an adverse effect of prolonged parenteral nutrition administration and a recognized risk factor for cholestasis, a poorly understood complication of TPN. 24 PNAC is defined as a serum-conjugated bilirubin level greater than 2 mg/dL (34.2 μmol/L) in infants receiving PN for ≥14 days. 25 In a study assessing the incidence and risk factors of PNAC, morphine was identified as the second most common hepatotoxic medication, following caffeine. 26 The results of the present study are consistent with those reported in the previous study. 26 However, despite advancements in understanding the molecular basis of neonatal cholestasis, the precise mechanism by which PN induces liver injury remains unclear.27,28
The absence of prior research on the effects of morphine on neonatal liver function underscores the groundbreaking nature of this study. This pioneering effort fills a critical gap in medical knowledge, offering new insights into neonatal pharmacology and the potential to influence future research and clinical practices. However, the current study has a few limitations, such as the retrospective design having inherent problems like incomplete data and selection bias. Secondly, the sample size was small. Many other factors can affect the liver function, having confounding effects, and this study design cannot establish the casual association of morphine use with deranged liver function. We could not perform the regression analysis to show the confounding effects of TPN or hepatotoxic drugs or antibiotics.
These findings highlight the necessity for larger, prospective studies to evaluate the generalizability of these results. Future research should implement a standardized morphine administration protocol and utilize rigorous inclusion criteria to assess the potential effects of morphine in neonates comprehensively. Also, a long-term follow-up of the morphine-exposed neonates is necessary to see if these deranged liver functions transform into clinically significant liver disease.
Conclusion
This study underscores the impact of morphine on liver function in preterm neonates. These findings suggest the possibility of morphine hepatotoxicity and highlight the need for careful monitoring of at-risk neonates exposed to opioids. Considering these results, clinicians should be careful with the use of morphine in preterm neonates to avoid the risk of developing cholestasis and hepatotoxicity.
Footnotes
Statements and declarations
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hamad Medical Corporation (MRC-01-21-341).
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.