
Abstract
We present a case of a 24-week gestation neonate who developed severe, reversible hypertrophic cardiomyopathy (HCM) with mid-cavity obstruction within the first 14 days of life. This occurred while the infant was receiving early low-dose hydrocortisone therapy according to the PREMILOC protocol. The patent ductus arteriosus (PDA) was small and functionally restricted following concurrent medical management with paracetamol at the time of diagnosis of HCM. Genetic, endocrine, and metabolic causes were ruled out, and the infant was not receiving any other pharmacological therapy associated with HCM. Our case highlights the need for clinical awareness of the potential association between HCM and low-dose hydrocortisone. This is a rare occurrence and may represent a multifactorial response involving heightened myocardial stress induced by hydrocortisone and increased left ventricular afterload following PDA restriction. The resulting rise in hemodynamic burden could contribute to cardiac remodeling, highlighting the need for clinical caution, close cardiac monitoring, and further research in this vulnerable population.
Keywords
Introduction
Early (<8 days) low-dose hydrocortisone (0.5 mg/kg/dose twice daily for 7 days, followed by 0.5 mg/kg/dose once daily for 3 days) as per the PREMILOC protocol has been associated with a significant reduction in the composite outcome of mortality or bronchopulmonary dysplasia (BPD) at 36 weeks postmenstrual age (PMA), without a statistically significant increase in impaired neurodevelopmental outcomes at 2 years of age.1,2
Hypertrophic cardiomyopathy (HCM) is an uncommon and heterogeneous condition characterized by abnormal thickening of a non-dilated ventricular wall, leading to structural and functional cardiac alterations. It may be classified as primary, resulting from sarcomeric gene mutations, or secondary, associated with metabolic, endocrine, or syndromic disorders. Accurate diagnosis necessitates the exclusion of physiological or pathological abnormal loading conditions that could account for the degree of hypertrophy, such as coarctation of the aorta, valvular heart disease, or long-standing patent ductus arteriosus (PDA).3,4
High-dose dexamethasone has been linked to reversible HCM, which usually responds to discontinuation of dexamethasone and supportive management. However, some cases may need medical treatment.5–7 Persistent PDA in preterm infants can also lead to adaptive myocardial remodeling, resulting in structural changes such as hypertrophy.8–10
Identifying the underlying etiology is important for accurate diagnosis, management, and prognostic assessment. This report highlights the rare occurrence of HCM associated with low-dose hydrocortisone administered according to the PREMILOC protocol in an extremely preterm infant, emphasizing the importance of early recognition and careful monitoring in these infants.
Case presentation
A 680 g female infant was born at 24 weeks and 2 days gestation via spontaneous vaginal delivery (SVD). The mother was a primigravida with normal antenatal scans, a low-risk pregnancy, and normal glucose and HbA1c profiles. There was no family history of cardiac conditions, sudden deaths, or syncope. The pregnancy was complicated by preterm pre-labor rupture of membranes (PPROM), followed by spontaneous labor. Antenatal corticosteroids and magnesium sulfate were administered before delivery.
The infant’s Apgar scores were 5 at 1 minute, 9 at 5 minutes, and 9 at 10 minutes. Arterial cord gases showed pH 7.45, pCO2 4.64 kPa, BE 0.50, and lactate 2.0 mmol/L. She was intubated at 5 minutes of life and received surfactant at 13 minutes. The initial oxygen requirement was 80%, which was weaned to 40% before transfer to the NICU. She was transferred to the NICU at 25 minutes on SIMV (RR 60, FiO2 40%, PIP 24, PEEP 5). The first postnatal arterial blood gas revealed pH 7.352, pCO2 5.03 kPa, pO2 9.44 kPa, BE -4.7, and lactate 2.5 mmol/L.
Respiratory management
The infant was managed on pressure-controlled assist/control volume guarantee ventilation (PCAC VG), targeting a tidal volume of 5 mL/kg. Caffeine citrate was administered at a loading dose of 20 mg/kg, followed by a maintenance dose of 5–10 mg/kg. A second dose of surfactant was given at 16 hours of life.
She was successfully extubated to BiPAP on day 4 but required reintubation on day 14 due to severe apneas and suspected sepsis. Subsequently, she was extubated to BiPAP on day 21 in a FiO2 of 45%, transitioned to CPAP on day 55, and gradually weaned to Vapotherm (8 L/min, FiO2 25%) on day 71, which was progressively tapered.
Fluid management
Initial fluids started at 80 mL/kg/day, increased to 100 mL/kg/day in response to elevated lactate levels, and increased to 120 mL/kg/day by day 2. On day 3, fluids were increased to 165 mL/kg/day due to negative fluid balance and rising sodium, followed by a further increase to 180 mL/kg/day for hypernatremia (Na 147 mmol/L). Urine output was well-maintained at 8.4 mL/kg/hr. Fluids were reduced to 160 mL/kg/day on day 4 and 150 mL/kg/day by day 7 while maintaining trophic feeds.
Full enteral feeds were established by day 37, enabling discontinuation of parenteral nutrition.
Infection management
The infant was treated for suspected sepsis with amikacin and benzylpenicillin (days 1–5), followed by piperacillin-tazobactam and teicoplanin (days 6–8) and meropenem (days 14–19). Despite low CRP levels, the white cell count (WCC) was significantly elevated, peaking at 50.7 ×109/L with neutrophilia (41.1 ×109/L) and remaining elevated at 35.0 ×109/L during days 6–8.
Microbiological cultures identified Pseudomonas aeruginosa from skin (day 4) and throat swabs (day 5), which persisted throughout admission, although blood cultures remained negative. Later antibiotic courses included flucloxacillin, amikacin, meropenem, and piperacillin-tazobactam based on evolving clinical needs and the medical management of NEC.
Hemodynamic and cardiac management
The infant developed hypotension (BP 25/11 mmHg, mean BP 17) on day 1, managed with a fluid bolus and dopamine infusion (maximum dose 15 mcg/kg/min) for 35 hours.
Low-dose hydrocortisone was initiated on day 1 as per the PREMILOC protocol (0.5 mg/kg twice daily for 7 days, followed by 0.5 mg/kg once daily for 3 days) and discontinued on day 11. • An echocardiogram (ECHO) on day 2 showed normal cardiac structure, good biventricular function, and a large PDA with a left-to-right shunt. • By day 6, ECHO showed a large hemodynamically significant PDA with pulsatile left-to-right shunt, which was treated with paracetamol for 3 days
Clinical deterioration and HCM diagnosis
The infant required reintubation on day 14 for frequent bradycardias and apneas. Sepsis was suspected and treated with meropenem for 5 days. Blood culture and CRP remained negative. There was no anemia; hypoglycemia and intraventricular hemorrhage were ruled out. An ECHO on day 14 showed a small restrictive PDA and severe left ventricular (LV) hypertrophy with mid-cavity outflow obstruction in systole. Cardiology, metabolic, and genetic specialists were consulted. Investigations were normal for dysrhythmia (12-lead ECG), metabolic, autoimmune, genetic, and viral infectious causes.
The infant remained hemodynamically stable and did not require specific medical therapy for HCM. Serial echocardiograms showed reduced LV hypertrophy with no mid-cavity obstruction by day 36 and complete resolution by day 69 (Figure 1). Normal heart (day 2), development of hypertrophic cardiomyopathy and its resolution (days 14 and 36). Serial echocardiography images in parasternal long axis view. PW = posterior wall of the left ventricle; LVOT = left ventricular outflow tract; Ao = aorta, LA = left atrium, IVS = interventricular septum, right ventricle.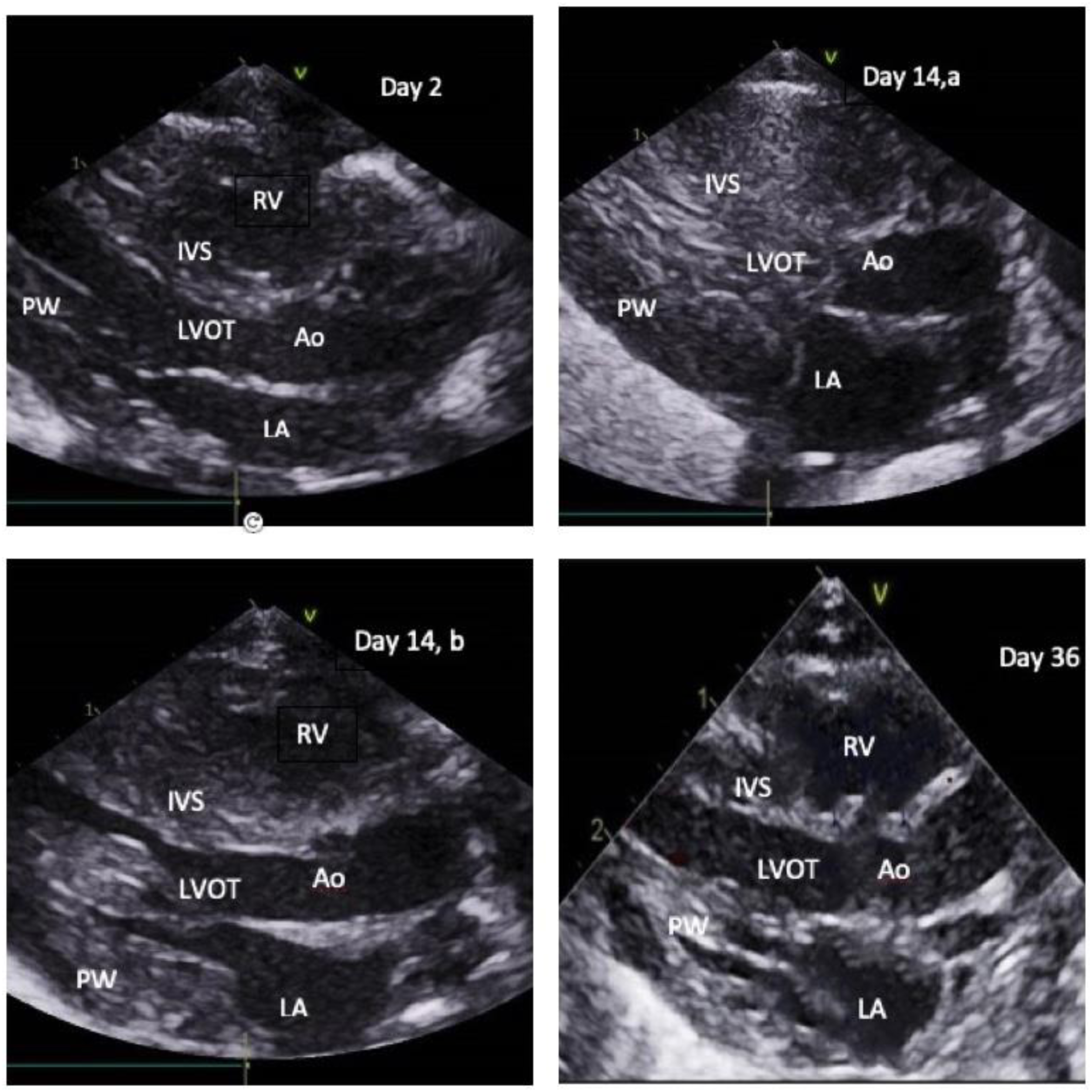
The infant was successfully extubated to NIPPV on day 21, transitioned to CPAP on day 55, and later to a high-flow nasal cannula on day 71.
Discussion
Cardiomyopathies are structural and functional abnormalities of the heart muscle that cannot be explained by abnormal loading conditions—such as coarctation of the aorta, arrhythmias, aortic stenosis, physiological stressors like sepsis, patent ductus arteriosus (PDA), or valvular diseases. A thickened, non-dilated ventricular wall characterizes HCM without any hemodynamic condition that could explain the degree of hypertrophy. This definition excludes physiological hypertrophy (resulting from physical training) and pathological hypertrophy (caused by conditions like hypertension, aortic valve stenosis, or other related disorders).3,4
Extremely preterm, low birth weight infants (<1000 g) are at a high risk of developing a persistent PDA, with 57%–69% remaining patent by 7–10 days of life. Without medical intervention, the median time for spontaneous closure is approximately 56 days. 11 PDA can lead to acute decompensation of the left ventricular myocardium or to adaptive remodeling, depending on the rate of pulmonary vascular resistance (PVR) decline after birth. A rapid decline can result in sudden volume overload, increasing the risk of heart failure, pulmonary edema, and the need for enhanced respiratory support before the myocardium can adequately adapt. In contrast, a gradual decline in PVR allows for adaptive hypertrophy, enabling the left ventricle to accommodate the increased load better and reducing the risk of early cardiac decompensation. When PDA exposure is prolonged, it leads to persistent volume overload, resulting in increased ventricular wall thickness and dilation of the left atrium and ventricle. These changes typically peak within the first 4 weeks and gradually resolve over 10 weeks.8–10,12
PDA closure, mainly through surgical ligation, can significantly increase myocardial stress. PDA contributes to biventricular loading and functional abnormalities in preterm infants, with notable changes occurring post-surgery. 13 This often leads to post-ligation cardiac syndrome (PLCS), characterized by acute cardiorespiratory instability within 6–12 hours post-surgery, affecting up to 50% of infants. In contrast, such complications have not been reported following successful medical management of PDA. Additionally, transcatheter closure offers an effective, less invasive alternative to surgical ligation associated with fewer complications and reduced myocardial stress. To date, no documented reports link PLCS with the development of cardiac hypertrophy.11,14,15
Myocardial stress can be assessed using biomarkers like B-type natriuretic peptide (BNP), a hormone released by ventricular cells in response to increased wall tension from elevated volume or pressure. BNP levels typically rise with heightened myocardial stress and decrease following successful PDA closure. However, this is not a routine investigation, as no consensus exists on reference BNP levels in newborns, particularly preterm infants. We did not assess BNP levels due to the lack of standardized reference values and limited clinical utility.15,16
In our case, medical treatment was initiated within the first week of life, and by 14 days, when hypertrophy was identified, the PDA was small and functionally restricted. This does not align with the typical pattern of sustained overload as the cause of remodeling and hypertrophy.
Insulin therapy and hyperinsulinism in infants of diabetic mothers have also been linked to the development of HCM in extremely preterm infants, with some cases showing resolution after discontinuation of insulin.4,17,24 However, in our case, the infant was not on insulin therapy, and there was no history of diabetes in the mother; she has normal HbA1c profiles, making it unlikely that insulin-induced hypertrophy contributed to the observed cardiac changes.
Reversible HCM has been reported in preterm infants following dexamethasone therapy for the prevention of BPD, sometimes requiring treatment with beta-blockers and angiotensin-converting enzyme (ACE) inhibitors. While typically associated with high-dose and long courses of dexamethasone, there are published reports of acute HCM and cardiogenic shock linked to even small doses and short courses of dexamethasone.7,18 Additionally, multiple high doses of hydrocortisone, administered for managing blood pressure instability, septic shock, and persistent pulmonary hypertension (PPHN), have been implicated in secondary HCM.19,20
Cardiomyocytes possess a high density of glucocorticoid receptors (GRs), through which steroids exert both genomic and non-genomic effects. These effects stimulate protein synthesis, leading to cardiac hypertrophy, apoptosis, and fibrosis. Key signaling molecules, including transforming growth factor-β (TGF-β), angiotensin II (Ang-II), endothelin-1 (ET-1), and interleukin-6 (IL-6), contribute to this process by increasing intracellular calcium levels, thereby activating hypertrophic and fibrotic gene pathways that drive myocardial remodeling.5,6
While high doses of hydrocortisone have been associated with the development of hypertrophic cardiomyopathy (HCM), its occurrence with low-dose hydrocortisone is extremely rare.6,19–21 The authors of the PREMILOC study acknowledged the occurrence of one case of HCM in each of the two study groups. 22
Glucocorticoids enhance myocardial contractility and systemic vascular resistance, potentially increasing the hemodynamic burden on already strained preterm cardiomyocytes. Given their immaturity and limited regenerative capacity, these cells are more susceptible to stress-induced cardiac complications.5,6,23
Although direct evidence is lacking, the potential interplay between hydrocortisone therapy and the restriction of the PDA following medical management, as observed in our case, in exacerbating myocardial stress in vulnerable preterm cardiomyocytes remains a plausible hypothesis. In our case, the infant developed hypertrophic cardiomyopathy (HCM) while receiving early low-dose hydrocortisone between days 6 and 14 of life with concurrent medical management of PDA. This may represent a multifactorial response involving an increased left ventricular afterload following PDA closure/restriction and potential augmentation of myocardial stress or remodeling associated with hydrocortisone therapy. This warrants careful consideration in clinical practice and underscores the need for further research to explore this possible association.
While this therapy is generally considered a safe intervention for the prevention of BPD, this case highlights its potential association with a severe cardiac complication—a rarely reported phenomenon. Awareness of this risk is crucial for ensuring safe clinical practice. We strongly recommend maintaining a high index of suspicion for this potentially life-threatening adverse effect. Close clinical observation and rigorous cardiac monitoring, including a low threshold for performing echocardiography, are essential in extremely preterm infants receiving early low-dose hydrocortisone with or without concurrent therapies for PDA closure. Such vigilance is vital to promptly identify and manage potential complications, thereby improving outcomes in this vulnerable population.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.