
Abstract
Background
Separating mothers and newborns after caesarean delivery prevents early skin-to-skin contact (SSC), despite WHO recommendations to initiate SSC immediately at birth. Early SSC promotes breastfeeding success, enhances thermoregulation, reduces maternal postpartum complications, and fosters bonding. In our hospital, SSC was not practiced after caesarean deliveries, prompting this quality improvement (QI) initiative.
Methods
Conducted in the operating theatre of a tertiary care hospital over 4 months (January–April 2024), with a 3-month sustenance phase. Inborn infants ≥34 weeks gestation and ≥1.8 kg delivered via caesarean section, with good tone and breathing at birth, were eligible. Sequential Plan-Do-Study-Act (PDSA) cycles were implemented to introduce SSC within 5 minutes of birth, aiming for ≥90% compliance. Interventions included staff training, SSC protocol development, operating room reorganization, and maternal support during recovery.
Results
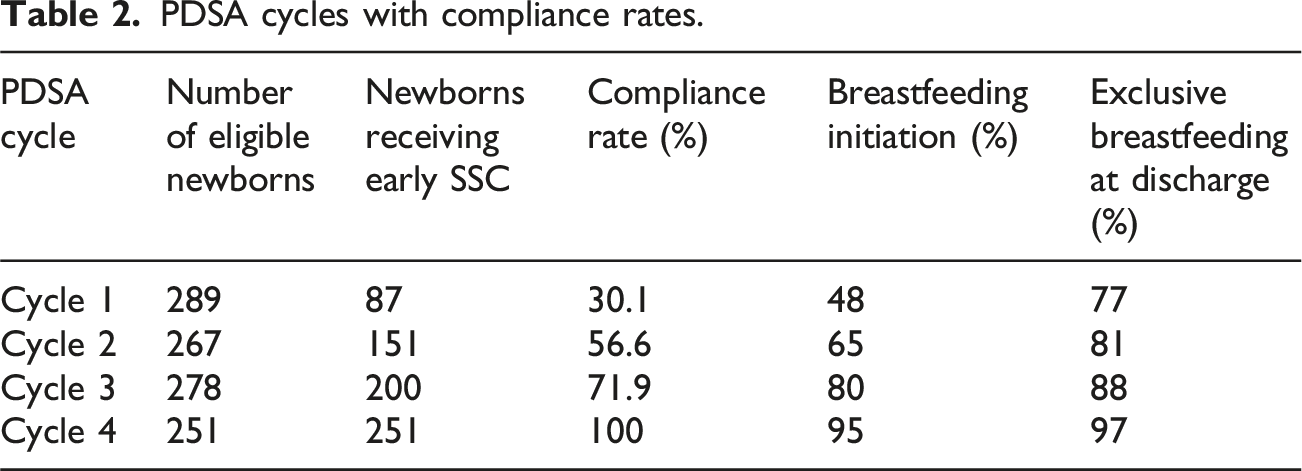
SSC compliance increased from 0% at baseline to 100% by cycle 4. Breastfeeding initiation improved from 48% to 95%, and exclusive breastfeeding at discharge increased from 77% to 97%. Deferred weighing and vitamin K administration rates increased from 10% to 100%.
Conclusion
Through systematic interventions, we achieved and sustained 100% SSC compliance for caesarean births. This study demonstrates that with a structured, multidisciplinary approach, SSC can be successfully integrated into caesarean delivery routines, potentially enhancing maternal-infant bonding and early breastfeeding initiation.
Introduction
Separating mothers and newborns post-caesarean often prevents immediate Skin-to-skin contact (SSC), despite WHO’s recommendation to begin SSC at birth for all deliveries, including caesareans, and continue for at least 1 hour to promote early breastfeeding. 1 SSC improves newborn outcomes, reducing morbidity when initiated early. 2 It also enhances breastfeeding rates in caesarean-born infants, matching those of vaginal births. 3
Skin-to-skin contact is linked to successful first lactation, longer breastfeeding duration up to 4 months, and a higher chance of exclusive breastfeeding for 6 months.4,5 Exclusive breastfeeding significantly reduces the risk of morbidity and mortality in the first 6 months of life, including neonatal mortality.6–8 Additionally, SSC improves thermoregulation, and reduces weight loss at discharge.9,10 For mothers, SSC enhances birth experience, induces uterine contractions, reduces postpartum haemorrhage risk, shortens placenta expulsion time, lowers postpartum depression incidence, and strengthens maternal-infant bonding. 11 Evidence suggests that while one-third of newborns do not initiate breastfeeding within the first hour, most do by 90 minutes, making prolonged SSC until a full breastfeed (at least 90 minutes) a more effective clinical indicator. 3 Additionally, many preterm infants are born by caesarean section, making SSC even more crucial for this vulnerable group. Studies show that even infants born <34 weeks gestation can achieve high exclusive breastfeeding rates with SSC. 12
In India, no national data on SSC is available. Reports suggest that only 15% of vaginally delivered babies receive early SSC. 13 SSC is not routinely practiced during caesarean deliveries in most hospitals, despite the rising rate of caesarean sections. At our institution, 80–90% of stable infants born via vaginal delivery receive SSC, but this is not the case for caesarean deliveries. To address this, we launched a quality initiative to increase SSC rates at birth for infants delivered by caesarean section.
Methods
The study was conducted at IPGMER & SSKM Hospital, Kolkata, a tertiary care teaching hospital with
Eligible participants were inborn infants ≥34 weeks gestation, ≥1.8 kg, with good tone and breathing at birth. Mothers had to be alert or recover post-anaesthesia. Exclusions included infants with congenital malformations, those needing ventilation, and maternal complications during or post-surgery (Figure 1). Algorithm for implementing skin-to-skin contact during caesarean section.
Baseline data were collected December 15–31, 2023, showing a 0-minute SSC baseline. The intervention aimed to initiate SSC within 5 minutes of birth for at least 1 hour, with a target of increasing SSC rates from 0% to 90% in 3 months using Plan-Do-Study-Act (PDSA) cycles (Video).
A QI team was formed, led by the neonatology consultant, including OT nursing in-charge, nursing staff, paediatric and obstetric trainees, and the head of the obstetrics department. The team was briefed on the evidence supporting early SSC and its absence in our unit. Regular meetings addressed concerns and identified obstacles, documented using fishbone analysis (Figure 2). Frontline OT nursing staff, led by the motivated sister-in-charge, played a key role in driving the initiative. Fish bone analysis.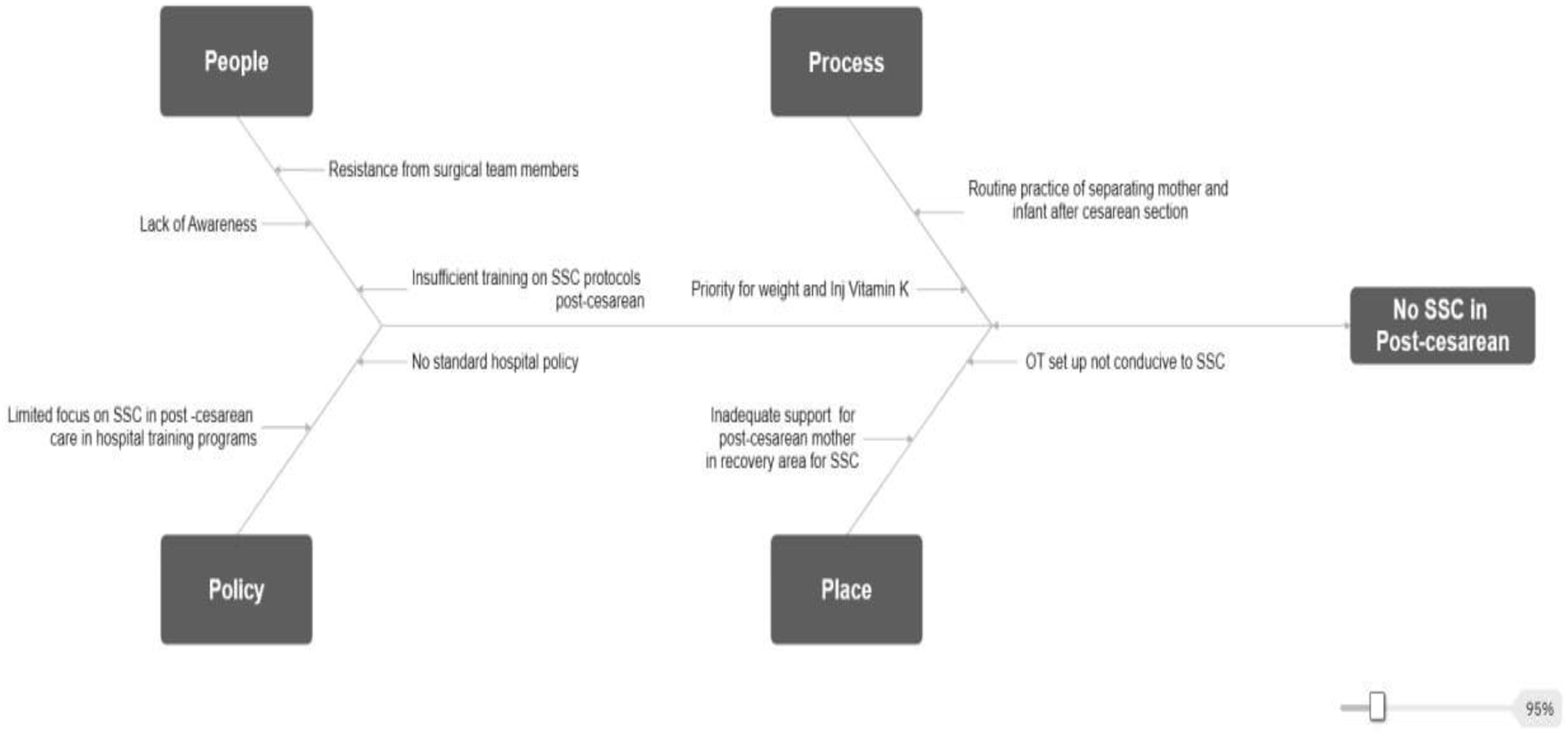
PDSA cycles.
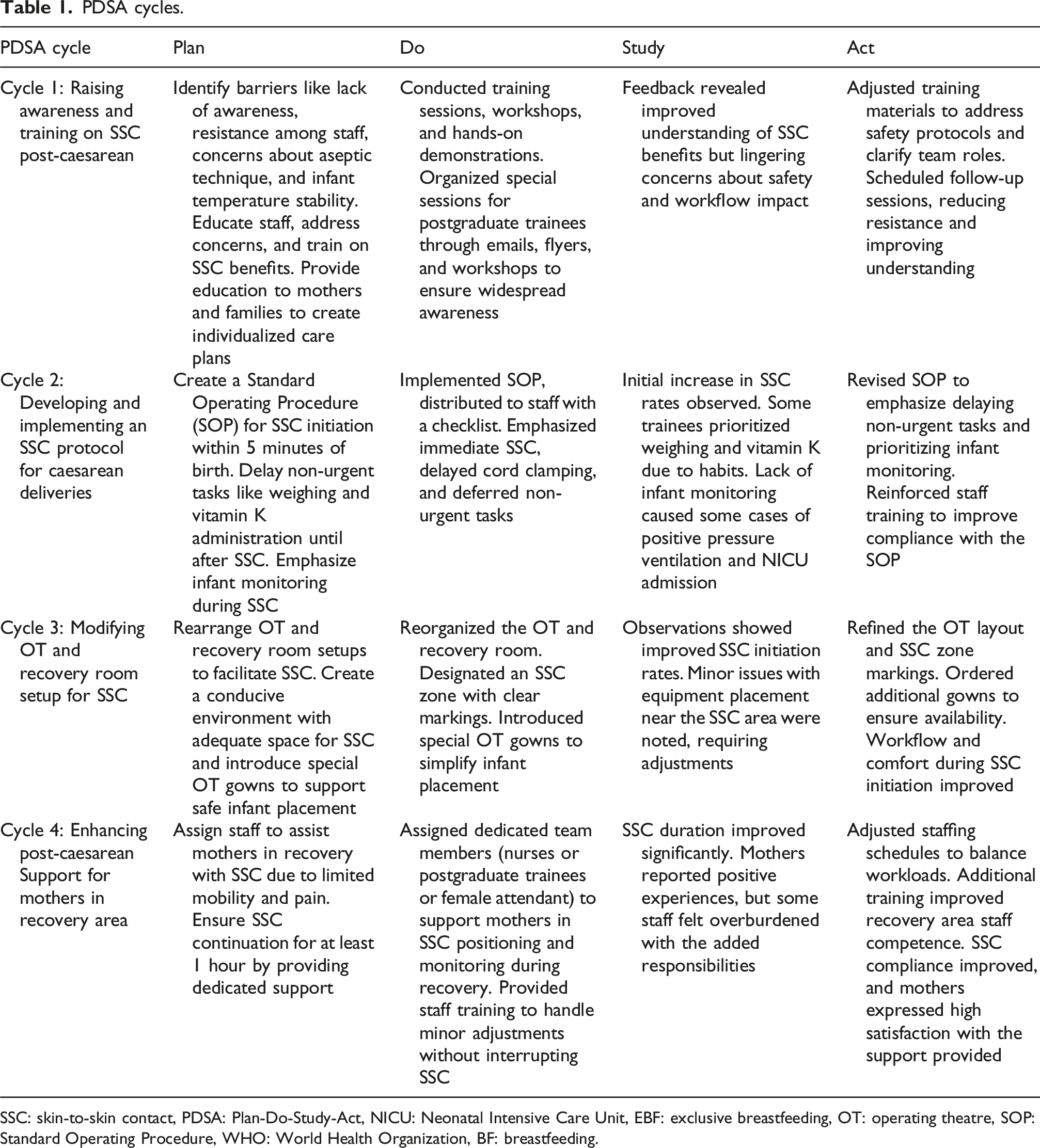
SSC: skin-to-skin contact, PDSA: Plan-Do-Study-Act, NICU: Neonatal Intensive Care Unit, EBF: exclusive breastfeeding, OT: operating theatre, SOP: Standard Operating Procedure, WHO: World Health Organization, BF: breastfeeding.
Results
PDSA cycles with compliance rates.
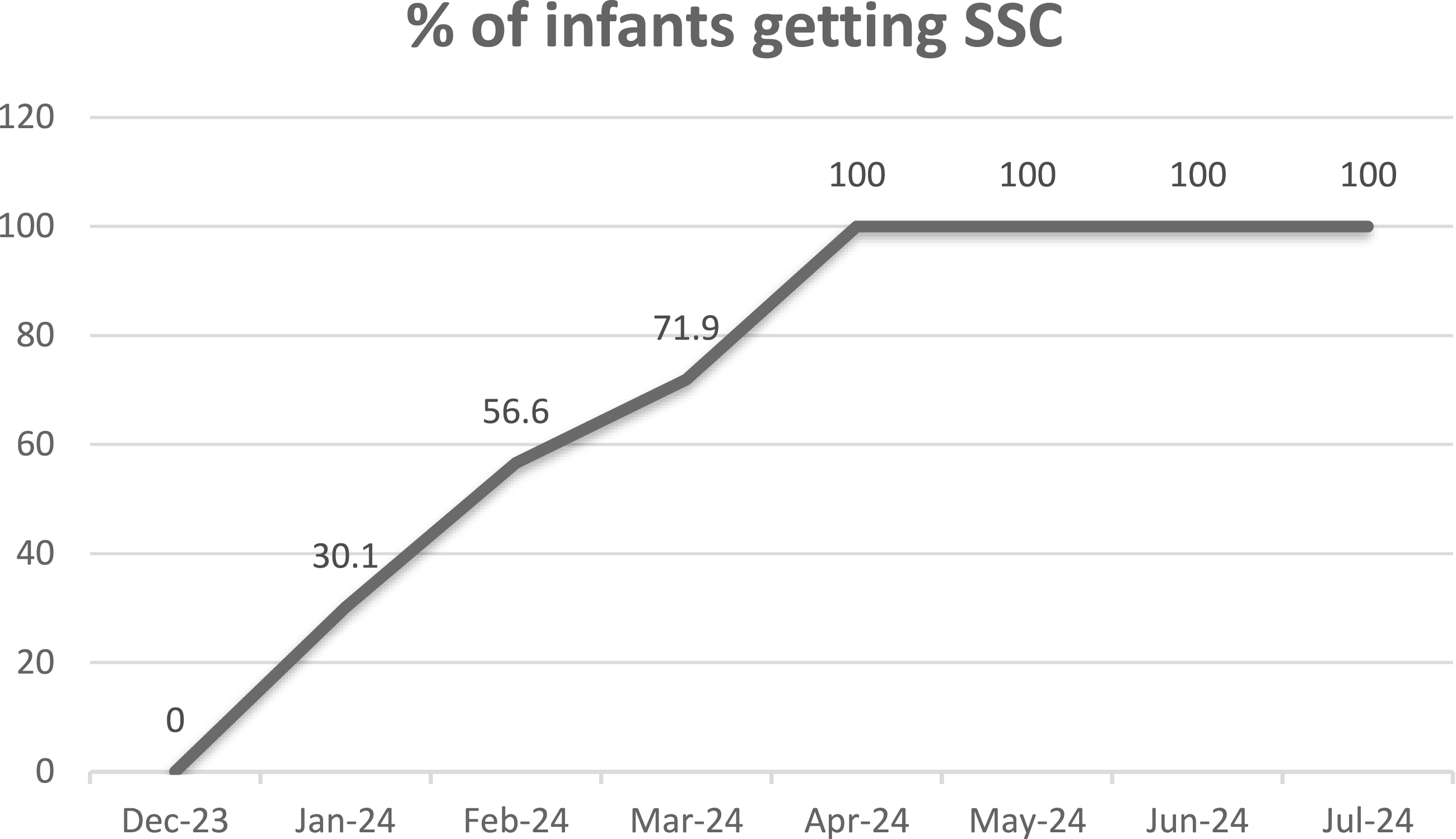
Line diagram for SSC compliance rate.
Discussion
This study shows that implementing early SSC for caesarean-born infants in a tertiary care hospital is achievable with systematic interventions and teamwork. Baseline data revealed no early SSC, highlighting a gap from WHO recommendations. Through PDSA cycles, compliance reached 100% by the fourth cycle and was sustained for 3 months, demonstrating the potential of a well-executed quality improvement initiative to make enduring changes in clinical practice. Additionally, breastfeeding initiation rates improved from 48% in cycle 1 to 95% in cycle 4, while exclusive breastfeeding at discharge increased from 77% to 97%, reinforcing the impact of SSC on early feeding practices.
The challenges addressed in each PDSA cycle highlight the complexity of changing practices in high-stakes settings like operating theatres. Barriers such as lack of awareness, absence of protocols, and logistical issues were systematically targeted in each cycle.
The first PDSA cycle focused on raising awareness and training healthcare providers, resulting in a modest increase in SSC compliance. However, anaesthetists, surgeons, and OT nurses initially resisted due to concerns about safety, sterility, and workflow disruption. Targeted training, strengthened safety protocols, and interdisciplinary discussions effectively addressed these concerns, securing their support for SSC implementation. The second cycle introduced a structured protocol, clarifying roles and prioritizing SSC over routine tasks like weighing and vitamin K administration, with added emphasis on infant monitoring. Aligning with AAP NRP guidelines, ongoing assessment of newborn breathing, tone, activity, colour, and temperature was emphasized. 14 Compliance improved significantly, demonstrating the critical role of standardized protocols in addressing barriers and changing practice patterns effectively.
The third PDSA cycle tackled logistical barriers by reorganizing the OT and recovery room and introducing specialized gowns, facilitating SSC implementation and boosting compliance. The fourth cycle improved maternal support in recovery by assigning designated nursing staff. In some cases, a female attendant was allowed to assist the mother, ensuring comfort and sustaining SSC for at least 1 hour post-operatively. This intervention extended SSC duration and enhanced maternal satisfaction and bonding, as reflected in positive feedback from mothers. A mother shared her experience, saying: “The doctors placed my baby on my chest immediately—I never expected it! It felt so good, like I could protect and hold my baby close.”
The 3-month sustenance phase showed 100% SSC compliance post-intervention, supported by continuous monitoring and staff reinforcement. Empowering OT and recovery nurses with ownership of the SSC protocol ensured success. This project offers a replicable framework for improving SSC rates in resource-limited, high-demand settings.
Our QI project aligns with the study by Maria et al. at Dr. RML Hospital, New Delhi, which demonstrated an increase in early SSC rates from 0% to 80% within 8 weeks for caesarean deliveries. 15 Maria et al. achieved 100% SSC compliance through staff sensitization, formal policies, and procedural adjustments. While their initiative also targeted early breastfeeding, our focus was on sustaining SSC, with plans to track breastfeeding rates in future cycles.
Several similar studies from developed countries have been conducted on this topic, often in similar settings, with comparable interventions and varying durations.3,12,16–19 Li et al. found that in a study across 150 hospitals, SSC lasting less than 30 minutes had no significant impact on exclusive breastfeeding at discharge compared to no SSC, while SSC lasting 60–90 minutes resulted in the highest EBF rates at discharge. This aligns with our findings, where sustained SSC contributed to improved breastfeeding initiation and EBF rates. 3 Similarly, Hoang et al. demonstrated that early essential newborn care, including SSC, significantly improved neonatal outcomes, reducing morbidity and increasing breastfeeding success. 2 These findings highlight the importance of not just initiating SSC but ensuring an adequate duration of at least 60–90 minutes for optimal breastfeeding outcomes. Thompson and Maeder’s (2021) initiative at a U.S. Midwest tertiary hospital demonstrated a significant increase in SSC after caesarean sections, rising from 30.4% to 61.3% for SSC lasting at least 15 minutes within the first hour after birth. This was achieved through nurse education, the incorporation of SSC into the interdisciplinary time-out (TTO) protocol, and the implementation of a new SSC guideline. 16 Brady k. et al. emphasizes the importance of interprofessional collaboration in implementing skin-to-skin contact during caesarean deliveries. 17 Key factors for success included data analysis and educational support among disciplines, reinforcing the need for teamwork in promoting SSC practices effectively in the operating room setting.
Few studies have examined the benefits of extending early SSC beyond the standard 60 minutes, with positive findings.3,12,20,21 Extended SSC (60–90 minutes) is associated with higher exclusive breastfeeding rates at discharge and improved neonatal morbidity outcomes.3,12 Additionally, research indicates that while the global indicator defines breastfeeding initiation within 60 minutes, the median time for natural initiation is 55 minutes, with over a third of newborns initiating after 60 minutes. Based on this, extending SSC to at least 90 minutes may further optimize breastfeeding outcomes. We maintained SSC for up to 60 minutes. Sustaining quality improvement initiatives is challenging due to staff workload, distractions, and the difficulty of keeping motivation high over time.
Another important aspect is that 70% of deliveries in our unit are by caesarean section (CS). As a tertiary care teaching hospital and statewide referral centre, we handle high-risk pregnancies, leading to a higher CS rate. However, we recognize this issue and are actively working to reduce unnecessary CS deliveries.
Limitations
The study focused on SSC compliance without evaluating outcomes such as temperature stability, maternal bonding, or mental health. Maternal pain perception and comfort during SSC were also not assessed, which could impact feasibility and satisfaction. Staff awareness of being monitored may have temporarily increased compliance, potentially differing under routine conditions. Additionally, the study was conducted in a single tertiary care hospital, limiting generalizability. As a pre-post intervention study, it is susceptible to temporal changes that could have influenced outcomes. However, no major changes in hospital policies or staffing occurred during the study period that would have significantly impacted SSC practices. Potential measurement challenges include observation bias, interrater variability, and day-night staffing differences, which may have influenced SSC compliance rates. Future studies should incorporate blinded assessments and standardized training to minimize these biases.
Conclusion
Early SSC for infants born via caesarean is feasible and sustainable in a tertiary hospital setting. Using a structured QI approach, we overcame logistical and cultural barriers, achieving 100% compliance. Multidisciplinary teamwork, standardized protocols, and ongoing monitoring were key to success. Future studies should assess SSC’s long-term effects on breastfeeding and bonding and explore its implementation in other settings.
Supplemental Material
Footnotes
Authors’ contributions
Dr. Md Habibullah Sk – Conceptualized and designed the study, led the implementation of the PDSA cycles, analyzed data, and drafted the manuscript. Dr. Sougata Chowdhury – Contributed to the study design, facilitated training sessions, supported protocol development, and reviewed the manuscript for intellectual content. Dr. Bijan Saha – Led the implementation of the PDSA cycles, assisted in data collection, contributed to protocol adjustments in the operating theatre, and participated in manuscript revisions.
Ethical consideration
Each author approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.