
Abstract
Background
Asphyxial event can compromise the function of many vital organs like brain, heart, and kidneys. Cardiac dysfunction results from hypoxic injury to subendocardial tissue, papillary muscle, and myocardium. The aim of this work was to assess correlation between cardiac troponin T levels, myocardial dysfunction, inotrope requirements, hypoxic ischemic encephalopathy (HIE) stages, and outcome in asphyxiated neonates.
Methods
This cohort study was conducted on 48 neonates aged (1–28) days old, both sexes, exposed to perinatal asphyxia, and admitted in NICU unit in Benha University Hospital during the period from September 2022 to August 2023. Neonates had blood drawn for CBC, liver, kidney functions, and serum troponin T levels. Also, assessment by echocardiography and MRI were done to these patients in the first 3 days.
Results
Troponin T levels were significantly higher in neonates with myocardial dysfunction (systolic or diastolic), who required inotropic support, mechanical ventilation, or who were non-survivors. Troponin T levels significantly correlated with HIE severity, as assessed by Apgar scores and Sarnat staging. ROC curve revealed that cardiac troponin T levels have high accuracy at a cutoff value of >0.18 ng/mL, >0.18 ng/mL, and >0.18 ng/mL, respectively, in detecting myocardial dysfunction, morbidity, and mortality in patients with HIE with reliable sensitivity (84.2%–92.3%) and specificity (88.2%–93.1%).
Conclusions
Elevated cardiac troponin T is highly suggestive of myocardial dysfunction in cases of HIE. It is significantly correlated to severity of HIE, morbidity, and mortality in asphyxiated neonate.
Introduction
Perinatal asphyxia is a leading cause of neonatal morbidity and mortality especially in low and middle income countries, in high-income countries, perinatal asphyxia affects 16/1000 live births. 1 The reported incidence varies from 2% to 16.2% in community based studies with mortality rates ranging between 38.5% and 74%. In hospital-based studies, approximately 2.8% and 5.6% of all live births have moderate and severe asphyxia, respectively. 2
When an asphyxiated event occurs in fetus and newborn, it leads to multiorgan involvement, 3 commonly affected abnormalities of birth asphyxia involve kidneys in about 50% of neonates, central nervous system 28%, and pulmonary system in 23%. 4 Cardiac dysfunction is detected in 24%–31% of patients and is usually secondary to transient myocardial ischemia. 5
Serum creatinine kinase muscle-brain isoenzyme (CK-MB) lacks cardiac specificity in the neonate and the levels are affected by gestational age, mode of delivery, and birth weight. Unlike CK-MB, cardiac troponin T (cTnT) is not affected by gestational age, mode of delivery, and other related factors, 6 and cardiac troponin T (cTnT) has been explored as a more specific biomarker for the diagnosis of myocardial injury in asphyxiated neonates.7,8 Troponin T can be detected at earlier stages than CK-MB and it also remains high for a longer period. 7 Further, cTnT levels are found to be elevated in 30%–50% of cases having normal CK-MB levels. 9
Myocardium of neonates is thought to be resistant to hypoxia but cardiac failure is one of the most important manifestations of myocardial dysfunction among cases having perinatal asphyxia. 10
Hemodynamic assessment with echocardiography enables enhanced diagnostic precision with a targeted approach to intervention that may complement a clinical examination and more accurately optimize post insult cerebral blood flow and oxygen delivery. Although echocardiography may offer a blueprint for formulating a diagnostic impression, further investigation is needed to determine the risk/benefit ratio of treatment and the thresholds for initiating treatment. 11
The aim of this work was to assess correlation between cardiac troponin T levels and echocardiography, inotrope requirements, HIE stages, and outcome in asphyxiated neonates.
Patients and methods
This cohort study was conducted on 48 neonates diagnosed with hypoxic ischemic encephalopathy (HIE) aged (1–28) days old, both sexes during the period from September 2022 to August 2023. An informed written consent was obtained from the relatives of the patients. The study was done after approval from the Ethical Committee Benha University Hospitals, matching the Helsinki declaration of interest. 12
Neonate was considered to have perinatal asphyxia if he/she in need of bag and mask or bag and tube ventilation at birth with Apgar score of ≤6 at 5 min; hypoxic encephalopathy features (lethargy, seizures, hypotonia, coma, or irritability); cord blood pH ≤ 7.0; or arterial pH in neonates ≤7.2. 13
Exclusion criteria were patients expired during the first 72 hours of birth (before fulfillment of investigations), neonates with other comorbidities such as major congenital malformations, renal failure and liver failure, or other conditions that could elevate troponin levels aside from HIE, such as sepsis, severe infections (e.g., pneumonia and meningitis), significant metabolic disturbances (e.g., metabolic acidosis), myocarditis, or severe respiratory distress syndrome.
All neonates were subjected to detailed history taking.
General examination
Vital signs, general characteristics, and anthropometric measurements were taken. Sarnat staging for degree of HIE was applied to all neonates. 14
Laboratory investigations
Blood gas analysis was performed using a heparinized needle. Additionally, 1 mL of peripheral blood was collected for kidney and liver function tests, with renal dysfunction indicated by high creatinine levels or low urine output, and hepatic dysfunction defined by elevated transaminase levels. 9
Blood sample was processed for estimation of cTnT levels by human cardiac troponin T (cTnT) ELISA kit (Catalogue No. 201-12-5490). Samples were prepared for analysis by adding standards and test samples to designated wells, with blank wells containing only chromogen solutions and stop solution. The assay involved adding cTnT-antibody and streptavidin-HRP to the test wells, sealing, shaking, and incubating at 37°C for 60 minutes. Following a 30-fold dilution of washing concentrate, the wells were washed, and chromogen solutions A and B were added, with further incubation and reaction stopped by adding stop solution. Optical density (OD) was measured at 450 nm within 15 minutes of stopping the reaction. A standard curve was generated to calculate sample concentrations using OD values, with assay sensitivity determined by subtracting two standard deviations from the mean OD of zero standards. The assay range was 1 ng/L to 300 ng/L, with intra-assay precision tested across 20 replicates and inter-assay precision across 8 replicates on different plates, yielding a coefficient of variation (CV) of less than 12%.
Radiological investigations
Brain MRI was done to detect different patterns of brain injury in these patients. Echocardiography was done by pediatric cardiologist using Philips machine and 6 Hz probe. Myocardial dysfunction was assessed by American Society of Echocardiography (ASE) standards with systolic dysfunction defined by ejection fraction <54% and fractional shortening <28% and diastolic dysfunction via the E/A ratio. Other parameters involved tricuspid and mitral regurgitation, systolic pulmonary artery pressure, and persistence of patent ductus arteriosus (PDA). 8
Neonates were followed up during their period of NICU stay and outcomes recorded: 1ry outcome in terms of myocardial dysfunction, need for inotropes, and mechanical ventilation. 2ry outcome in terms of mortality.
Statistical analysis
Statistical analysis was done by SPSS version 16 software (Inc, Chicago, ILL Company). Categorical data were presented as number and percentages. Quantitative data were tested for normality using Shapiro–Wilks test assuming normality at p > 0.05. Normally distributed variables were expressed as mean ± standard deviation and analyzed by Student “t” for 2 independent groups, while non parametric data were presented as median and range, and analyzed by Mann–Whitney U-test for 2 independent group and Kruskal–Wallis (KW) test for 3 independent groups. p ≤ 0.05 was considered significant.
Results
Characteristics of the studied group.
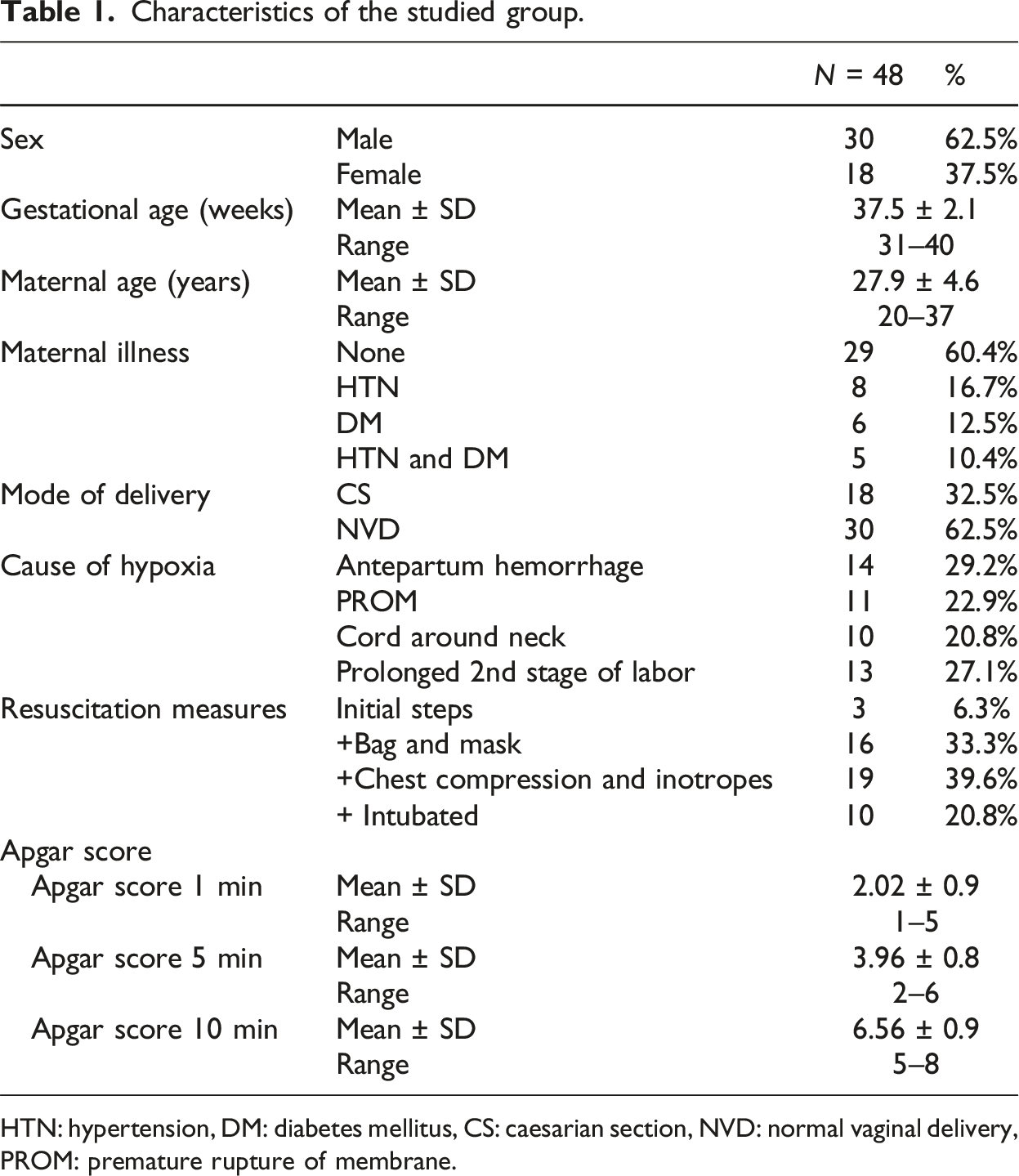
HTN: hypertension, DM: diabetes mellitus, CS: caesarian section, NVD: normal vaginal delivery, PROM: premature rupture of membrane.
Cardiac troponin T level according to gestational age in the studied group.
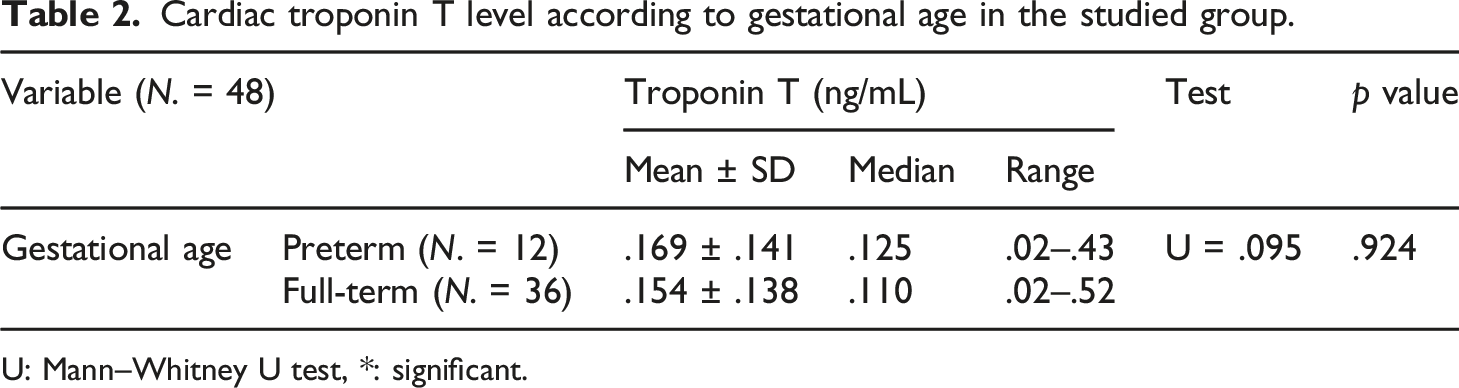
U: Mann–Whitney U test, *: significant.
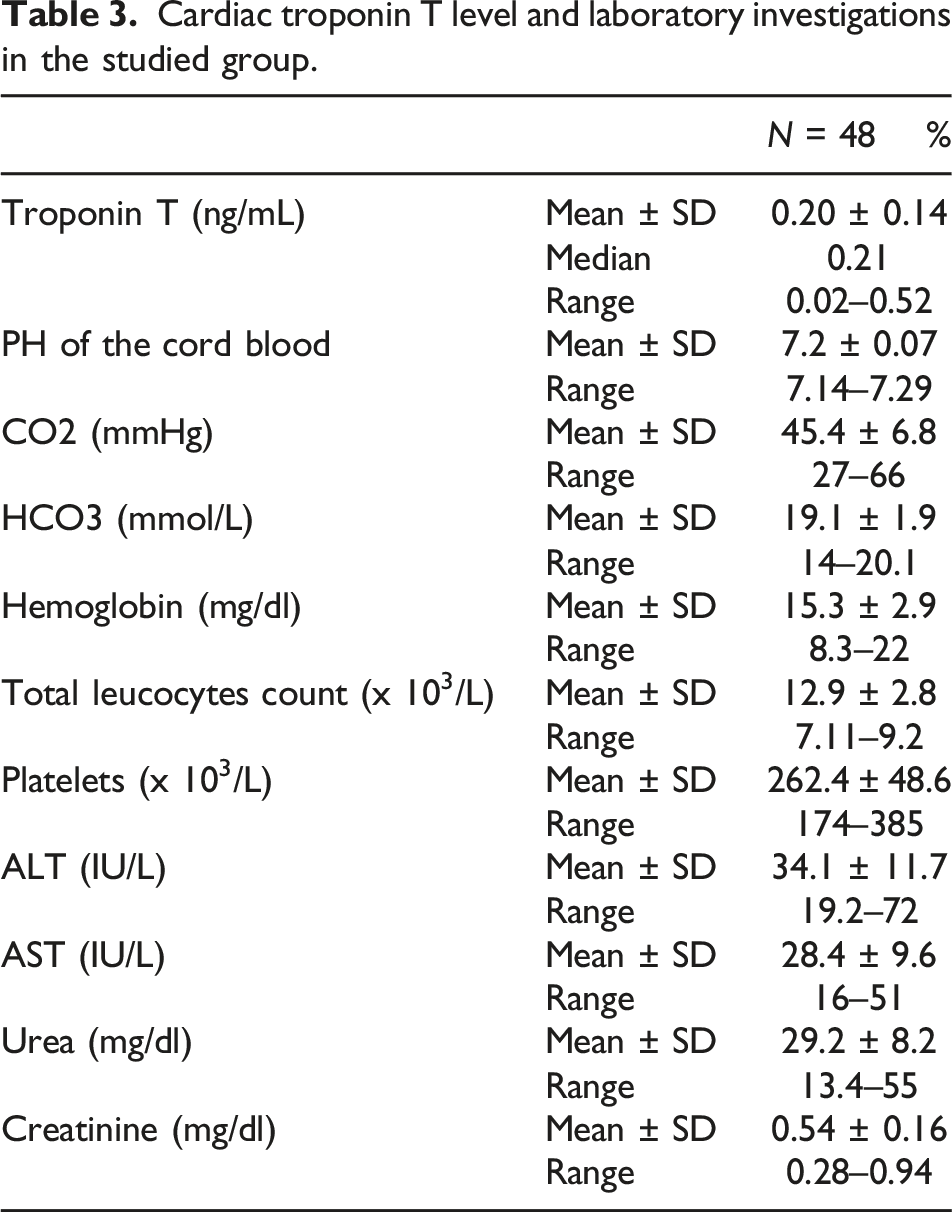
Cardiac troponin T level and laboratory investigations in the studied group.
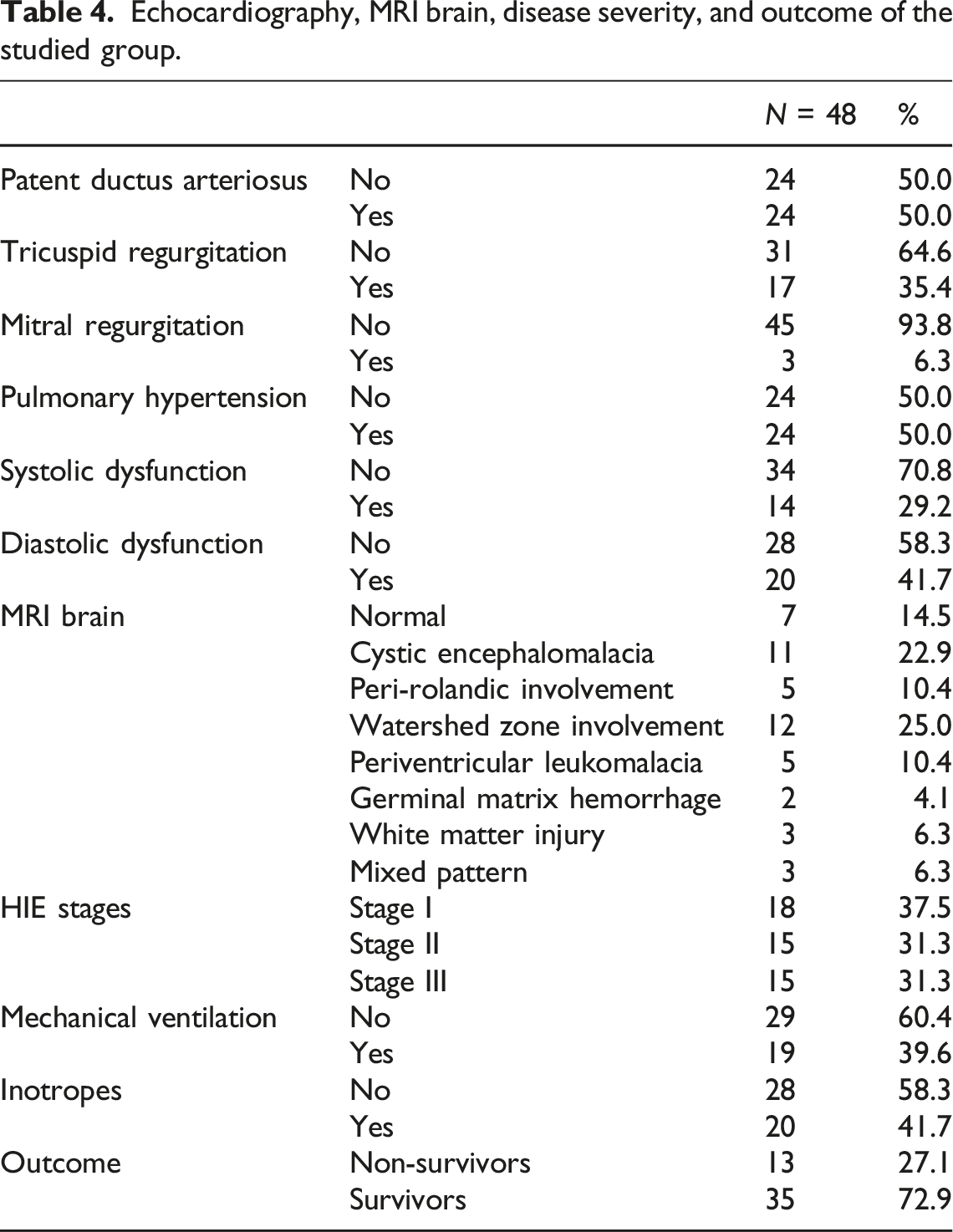
Echocardiographic evaluation showed that 50% of neonates had patent ductus arteriosus, 50% had pulmonary hypertension, 29.2% had systolic dysfunction, and 41.7% had diastolic dysfunction.
Echocardiography, MRI brain, disease severity, and outcome of the studied group.
Cardiac troponin T level according to echocardiography in the studied group.
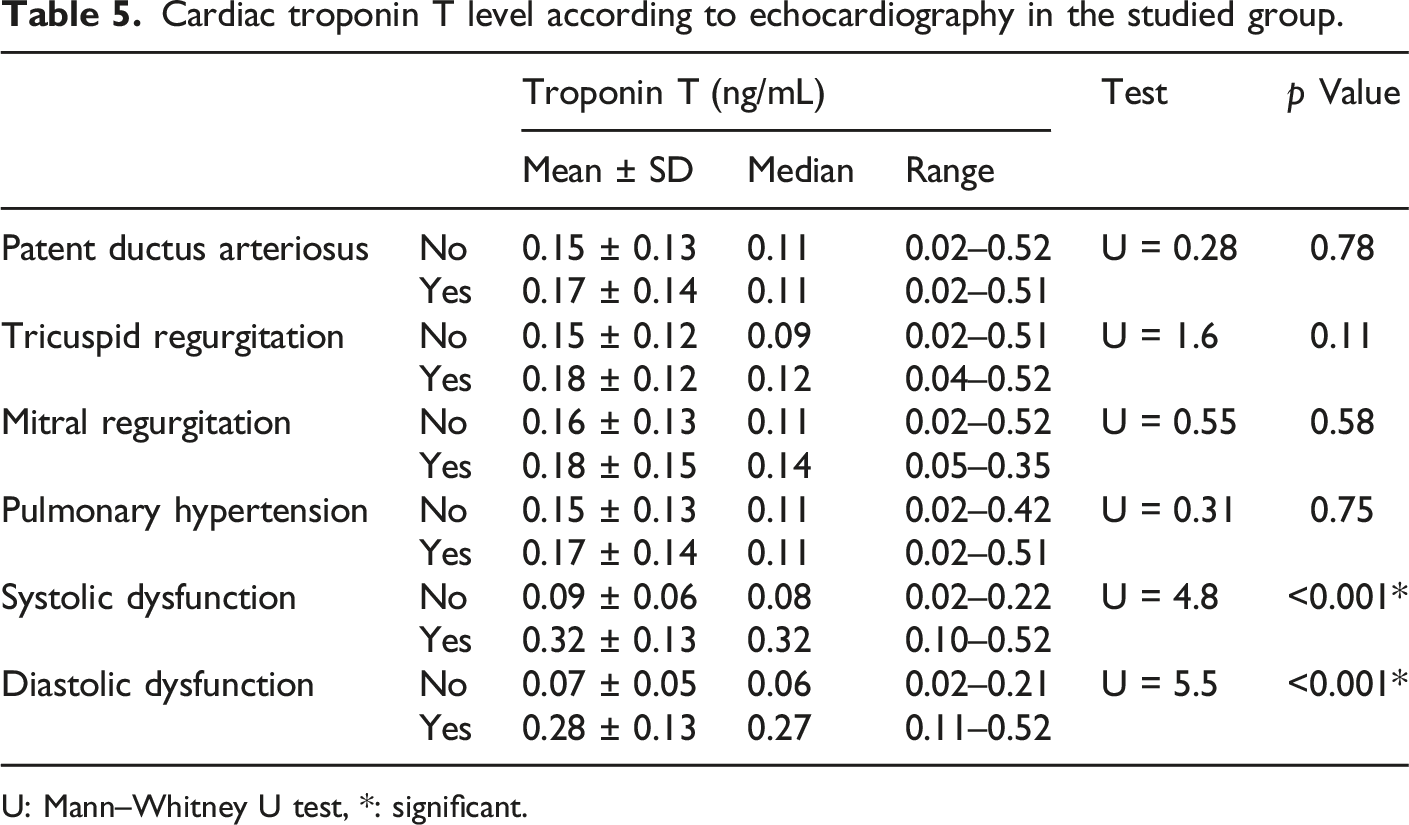
U: Mann–Whitney U test, *: significant.
Cardiac troponin T level according to HIE staging, disease severity, and outcome in the studied group.
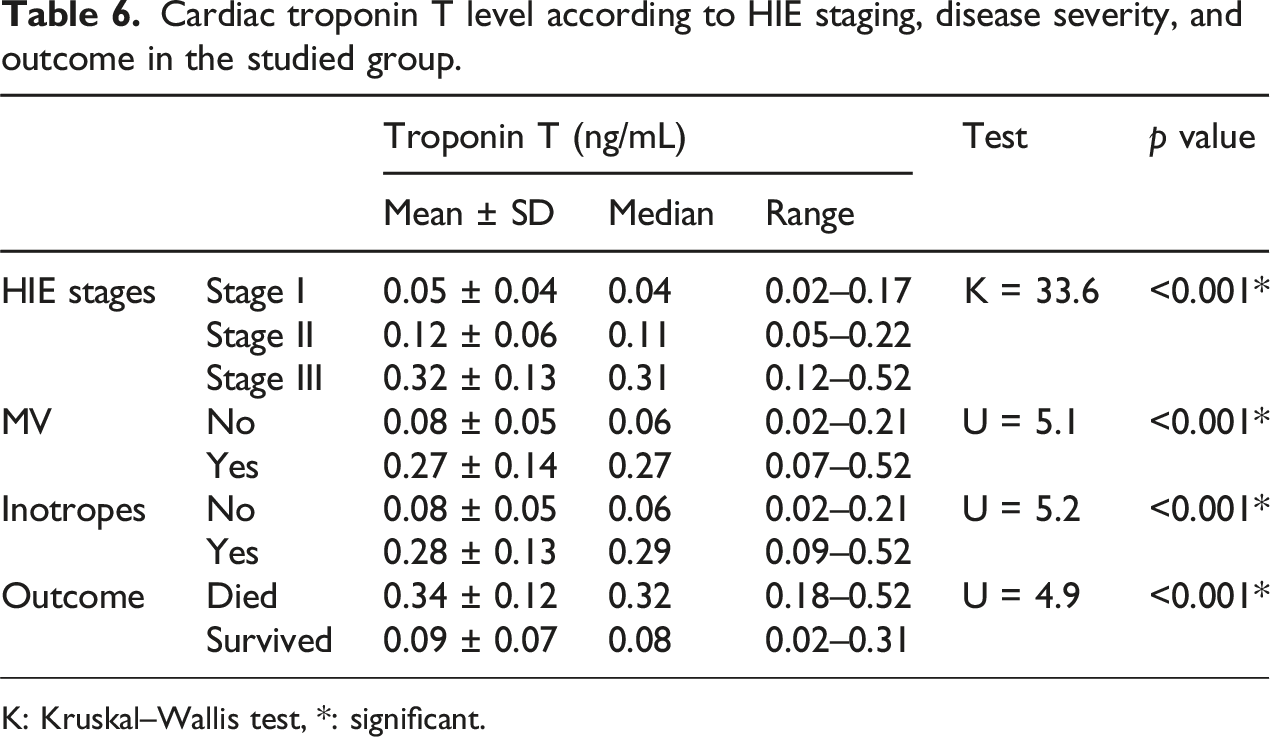
K: Kruskal–Wallis test, *: significant.
There was statistically significant negative correlation between cardiac troponin T and (Apgar score at 5th and 10th minutes and PH of the cord blood). However, there was no statistically significant correlation between cardiac troponin T and (gestational age, maternal age, Apgar score at 1st min, CO2, or HCO3) (Figure 1). Correlation between cardiac troponin T and (a) Apgar score at 10 min (b).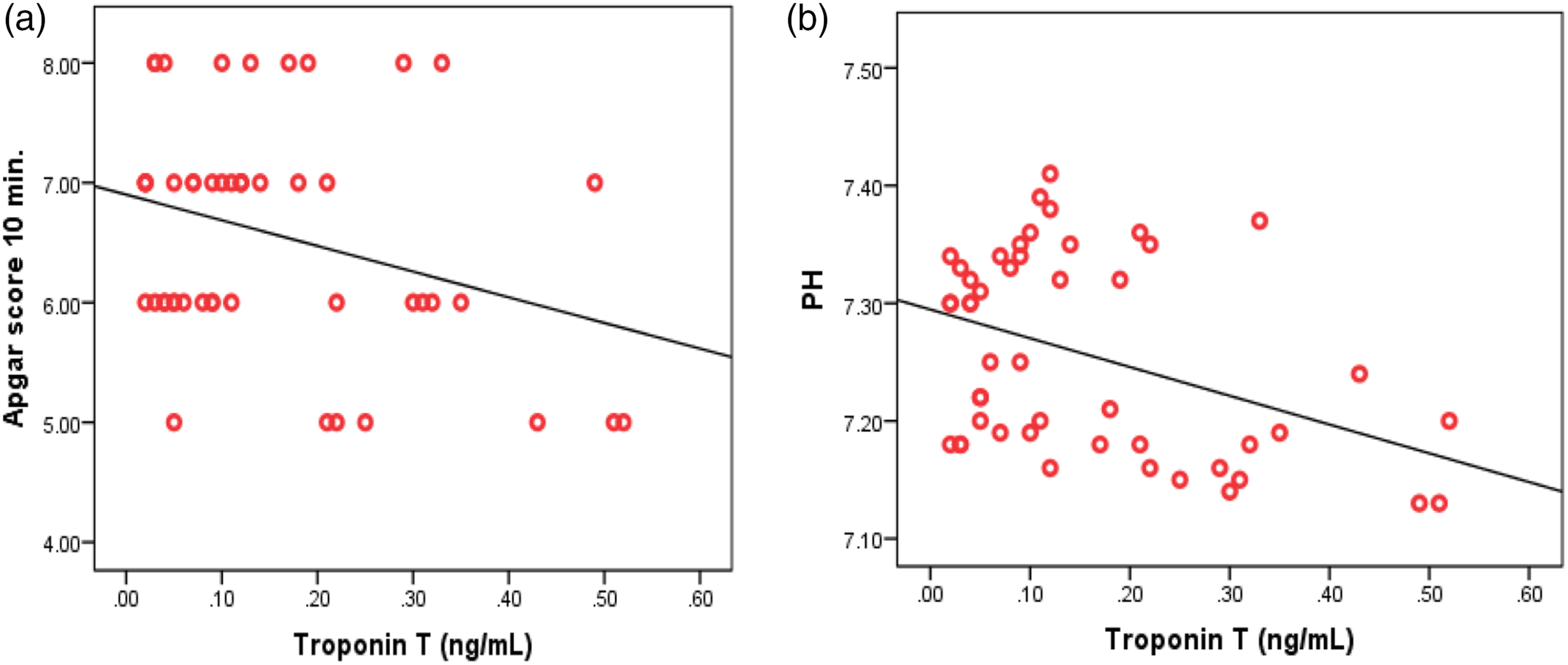
Performance of cTnT to detect myocardial dysfunction by echocardiography, cases of HIE who needed inotropic support, and mortality in cases of HIE.
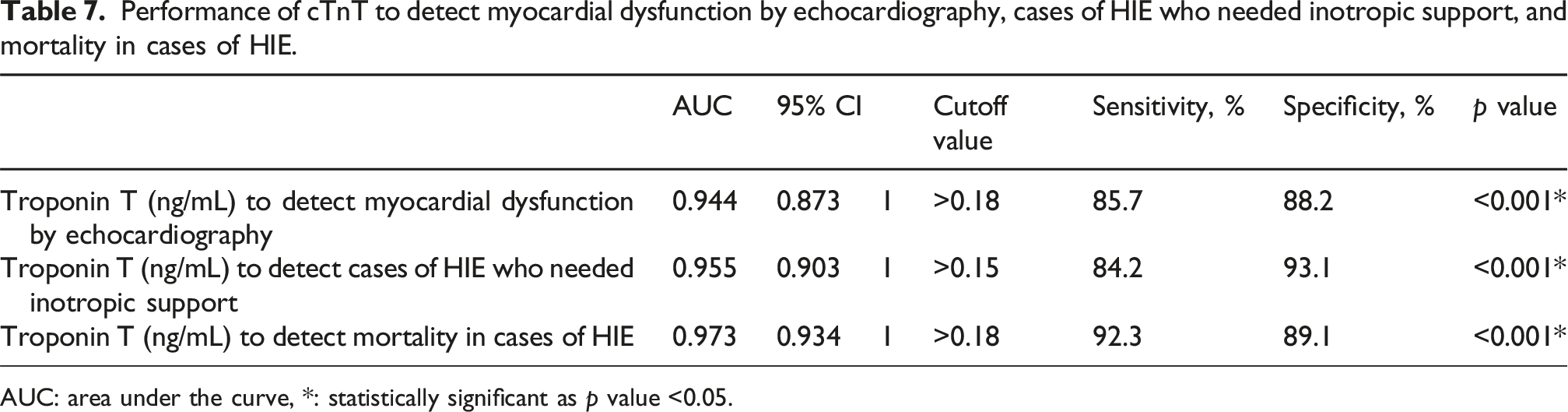
AUC: area under the curve, *: statistically significant as p value <0.05.
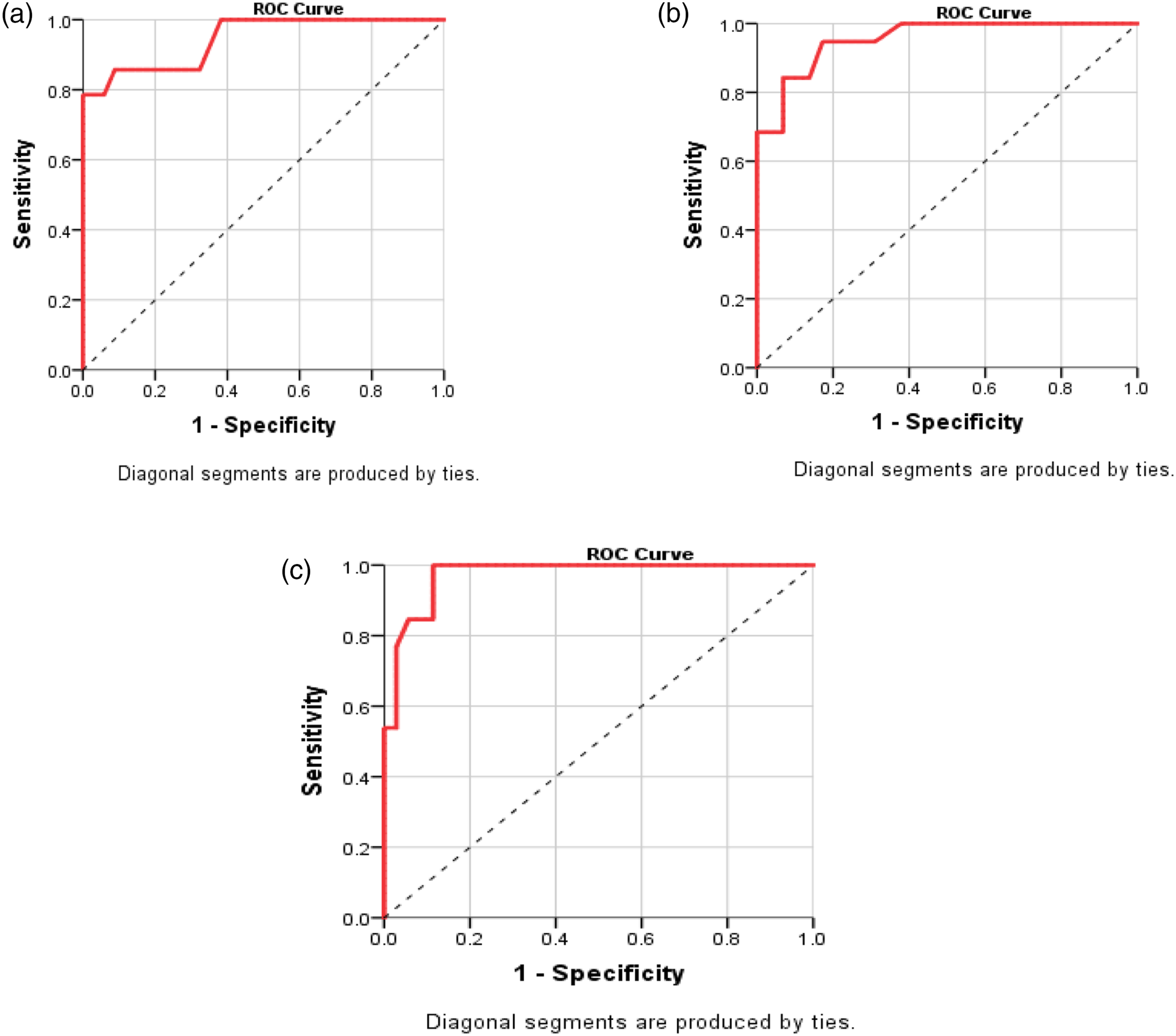
ROC curve of performance of cardiac troponin to detect (a) myocardial dysfunction by echocardiography [cutoff >0.18 ng/mL (sensitivity: 85.7% and specificity: 88.2%), AUC = 0.944 (95% CI: 0.873–1.0, p < 0.001], (b) cases of HIE who needed inotropic support [cutoff >0.15 ng/mL (sensitivity: 84.2% and specificity: 93.1%), AUC = 0.955 (95% CI: 0.903–1.0, p < 0.001], and (c) mortality in cases of HIE [cutoff >0.18 ng/mL (sensitivity: 92.3% and specificity: 89.1%), AUC = 0.973 (95% CI: 0.934–1.0, p < 0.001].
Discussion
This cohort study was done on 48 neonates with perinatal asphyxia including 30 males and 18 females; their mean gestational age was 37.5 ± 2.1 weeks. That was in agreement with Yellanthoor and Rajamanickam 13 who studied correlation of cardiac troponin T levels with inotrope requirements in 57 neonates with perinatal asphyxia. His results revealed that incidence of HIE is more common in males and full-term babies with mean gestational age 38.4 ± 1.6 weeks.
In the present study, the mean maternal age was 27.9 ± 4.6 years. Most cases (60.4%) had no history of maternal diseases, while 16.7%, 12.5%, and 10.4% had diabetes, hypertension, or both, respectively. Most cases (62.5%) were born by NVD. Regarding cause of hypoxia, the most common cause was antepartum hemorrhage (29.2%), followed by prolonged 2nd stage of labor (27.1%), PROM (22.9%), and cord around neck (20.8%).
In the same way, Namusoke et al., 15 who enrolled 751 newborns with 399 (53%) male and 352 (47%) female, reported that the factors that were significantly associated with HIE at bivariate analysis included prolonged labor, prolonged rupture of membranes, antepartum hemorrhage, and prolonged pregnancy. The incidence of HIE was 30.6 per 1000 live births and the mortality in HIE was 26% (6/23), predominantly in severe HIE.
Most of the asphyxiated neonates in this study required aggressive resuscitative maneuvers in the form of mask and bag, chest compression, and inotropes or intubation at birth room with only 6.3% of cases responding to initial resuscitation steps.
In agreement with Yellanthoor and Rajamanickam 13 who reported that mode of resuscitation at birth included intubation in 26 (45.6%) and bag and mask ventilation is 15 (26.3%). However, the study by Joseph et al. 16 who included 120 term neonates found that incidence of myocardial dysfunction was 55% (66/120) in asphyxiated neonates with mean cTnT levels 0.277 ± 0.231 ng/mL where all neonates required positive pressure ventilation and 85% of them required endotracheal intubation in the delivery room .
The mean Apgar score at 1st min was 2.02 ± 0.9, at 5 min was 3.96 ± 0.8 and at 10 min was 6.56 ± 0.9. Similarly, Lally et al., 17 who included 223 infants, reported that the mean (SD) Apgar score at 10 min was 5.6 (2.2). This correlates with accepted criteria for diagnosing neonates with perinatal asphyxia.
In the present study, the mean weight was 3.3 ± 0.5 kg, the mean height was 47.8 ± 0.8 cm, and the mean head circumference was 34.8 ± 0.9 cm. Similarly, Mahmoud et al., 18 who included 50 full-term neonates [32 males (64%) and 18 females (36 %)], reported that the mean weight of neonates with HIE was 3.7 kg, with a range of 3–4 kg suggesting that macrosomia of babies with traumatic deliveries may be one of risk factors for perinatal asphyxia. While in the study by Joseph et al., 16 mean (SD) birth weight was 2.816 kg.
Neonates in the study commonly displayed cyanosis, bradycardia, hypotension, hypothermia, and hypoglycemia. Most of these respiratory complications may be attributed to persistent pulmonary hypertension in these asphyxiated neonates. Many also exhibited hypotonia and flaccidity, with a range of neurological symptoms including hyperactivity, lethargy, stupor, and convulsions. Neonatal reflexes were absent in a majority of cases. In agreement with Mahmoud et al. 19 whose study was carried out on 40 neonates with perinatal asphyxia, he reported that cardiac injury was common with cardiac troponin I serving as an early biomarker for myocardial damage. The asphyxiated group had statistically higher frequencies of tachycardia, bradycardia, tender liver, tachypnea, lung crepitations, poor reflexes, decreased consciousness, convulsions, and hypotension.
The study revealed that the mean cord blood pH was lower than normal, with elevated CO2 and reduced bicarbonate levels. This reflects the effect of perinatal hypoxia in the development of CO2 retention and acidosis, therefore increasing the risk of myocardial injury. Routine laboratory investigations showed that hemoglobin, total leucocytes count, platelets, and liver enzymes (ALT and AST) were within normal ranges. Urea and creatinine levels were also found to be normal.
Mahmoud et al. 19 reported that WBCs × 103/mm3 of asphyxiated neonates were significantly higher than that of the healthy control neonates, while mean value of RBCs of asphyxiated neonates were significantly lower. There was no significant difference between the two studied groups in the platelets count. The mean values of pH and PaO2 of asphyxiated neonates were significantly lower, while mean PaCO2 was significantly higher than that of the healthy control neonates. There was no significant difference between the two studied groups in HCO3.
In the current study, the mean cardiac troponin T level was 0.20 ± 0.14 ng/mL and the median was 0.21 ng/mL. Yellanthoor and Rajamanickam 13 reported that elevated cTnT levels were observed in 41 (71.9%) neonates studied, with median (IQR) of 0.285 (0.211–0.422) ng/mL. The maximum value observed was 1.99 ng/mL. Also Mahmoud et al. 18 reported that asphyxiated neonates had significantly higher cTnT levels (4.6 ± 4.4 ng/mL) compared to controls (0.55 ± 0.6 ng/mL). Higher cTnT correlated with lower Apgar scores, acidosis (lower pH and higher PaCO2), and worse outcomes (neurological abnormalities or death).
Echocardiography was used as the gold standard for detection of myocardial dysfunction. 50% of neonates had patent ductus arteriosus, 6.3% had mitral regurgitation, 50% had pulmonary hypertension, 29.2% had systolic dysfunction, and 41.7% had diastolic dysfunction.
In agreement with Shahidi et al., 20 who examined cardiovascular complications following birth asphyxia in 29 asphyxiated term neonates , found that patent arterial duct was a common finding in asphyxiated neonates (62%) while mitral valve regurgitation was relatively rare. About one-third of asphyxiated neonates had different levels of systolic dysfunction. Diastolic dysfunction and pulmonary hypertension were detected in about half and near two-thirds of asphyxiated neonates, respectively. Left ventricular dysfunction is attributed to ischemic insult and reactive oxygen species from reperfusion injury, while hypoxic induced vasoconstriction of pulmonary vascular bed leads to pulmonary hypertension.
The most common MRI findings in our study with decreasing order of frequency included 25% with watershed zone involvement, 22.9% with cystic encephalomalacia, 10.4% peri-rolandic involvement, 10.4% periventricular leucomalacia, 6.3% white matter injury, and 6.3% had a mixed pattern.
In the same way, Li et al. 21 who studied pattern of MRI brain injury in 149 infants with HIE, reported that prevalence of brain injury was 61% of infants with mild injury predominant in 44% of neonates and fewer cases of moderate (11%) or severe (4%) injury. The most common brain injury patterns were watershed (22%), deep gray nuclei (20%), punctate white matter (18%), and atypical lesions (18%).
While in the study by Jose et al., 22 who identified 31 babies with perinatal asphyxia and hypoxic ischemic encephalopathy, the MRI was normal in 16 (61.5%). There were abnormal signals in basal ganglia in two (7.7%) in the cerebral cortex and scattered signal abnormalities in both cortex and basal ganglia in six (23.1%).
In the present study, according to Sarnat staging, most neonates (37.5%) were stage I, 31.3% were stage II, and 31.3% were stage III. 14
In the same way, Mahmoud et al. 18 reported that 46% of the cases had Sarnat stage I, 40% had Sarnat stage II while only 14% had stage III. While in the study by Michniewicz et al., 23 patients were divided into groups according to Sarnat staging: 27 out of 57 (47.4%) met the criteria of a group HIE - A moderate; the rest of them 30 out of 57 (52.6%) were classified as cases of severe HIE.
In the current study, 39.6% of neonates required ventilation, 41.7% needed inotropes, and 27.1% of cases expired out.
In agreement with Yellanthoor and Rajamanickam, 13 mechanical ventilation was needed in 20 (35.1%) neonates, inotropic support in 19 (33.3%) neonates, and 6 cases (10.5%) were non-survivors. In contrast to Bruckmann et al. 24 who reported the incidence of asphyxia was between 8.7 and 15.2 per 1000 live births, and moderate to severe HIE was seen in 60% of cases. The overall mortality rate was 7.8%, with mortality rates of 7.1% in moderate and 62.5% in severe HIE cases.
Cardiac troponin TnT level in our study was significantly higher in neonates with myocardial dysfunction, and other echo findings showed no statistical difference in troponin level.
In the same way, Joseph et al. 16 reported that the mean cTnT value in birth asphyxia was 0.207 ± 0.289 ng/mL with significant difference in the mean cTnT values between asphyxiated neonates with and without myocardial dysfunction. However, Yellanthoor and Rajamanickam 13 reported that the median cTnT level showed an increasing trend with the increase in changes in echocardiography (p = 0.002).
In the current study, increasing severity of HIE showed increasing troponin T level significantly from stage I to stage II to stage III, which is in the same line with Yellanthoor and Rajamanickam, 13 who reported that neonates who had HIE stage III had significantly higher levels of cTnT levels when compared to neonates with HIE stage I and II (p = 0.013).
Similarly, Yellanthoor and Rajamanickam 13 reported that cTnT levels were significantly higher in neonates requiring inotropic support. Moreover, median cTnT levels were comparatively higher in the six neonates who succumbed.
Our results showed a significant negative correlation between cardiac troponin T and (Apgar score at 5th &10th minutes and PH of the cord blood). However, there was no statistically significant correlation between cardiac troponin T and (gestational age, maternal age, Apgar score at 1st min, CO2, or HCO3).
This goes in agreement with Mahmoud et al, 19 who reported that there was a highly significant negative correlation between cTnT and the Apgar score in the asphyxiated group (p < 0.001). There was a highly significant negative correlation between cTnT and pH (r = −0.6, p < 0.001), HCO3 (r = −0.6, p < 0.001), and a highly significant positive correlation between cTnT and PaCO2 (r = 0.7, p < 0.001).
Using ROC analysis to evaluate the effectiveness of cardiac troponin T in identifying myocardial dysfunction, yielding AUC values of 0.966 and 0.944 (p<0.001). At a cutoff of >0.18 ng/mL, sensitivity was 86.7% and 85.7%, with specificity at 91.1% and 88.2%, respectively. The analysis also assessed cardiac troponin T’s ability to identify HIE cases requiring inotropic support and mortality, showing AUC values of 0.955 and 0.973 (p<0.001). For cutoffs of >0.15 ng/mL and >0.18 ng/mL, sensitivity was 84.2% and 92.3%, respectively, and specificity was 93.1% and 89.1%.
This was in agreement with Joseph et al. 16 reported that the sensitivity of cTnT in diagnosing myocardial dysfunction (gold standard as echocardiography and cutoff cTnT as 0.1 ng/mL) was 92.4%; specificity 74.5%. Using ROC curve analysis, cutoff cTnT of 0.11 ng/mL, increased the specificity to 94.1% with sensitivity remaining at 92.4%. Using ROC curve analysis, a cutoff cTnT of 0.13 ng/mL had 83.6% sensitivity and 94.3% specificity for diagnosing clinical shock. For mortality, a cutoff cTnT of 0.25 ng/mL had a sensitivity of 83.9% and specificity of 96.6 %. For severe HIE (HIE 3), a sensitivity of 81.6% and specificity of 91.5% with a cutoff cTnT of 0.188 ng/mL was found.
While in the study by Sweetman et al., 9 they reported that troponin T levels on days 1, 2, and 3 were highly significant predictors of mortality (AUC = 0.99, 0.99, and 0.99; p = 0.005, 0.005, and 0.02, respectively). The cutoff values of troponin T for best prediction of mortality were 0.84 ng/mL, 0.63 ng/mL, and 0.58 ng/mL on days 1, 2, and 3, respectively.
Limitation
Limited number of cases, lack of healthy controls and serial monitoring of cardiac troponin T values was not done.
Conclusions
Cardiac troponin T increased significantly with severity of HIE and correlated negatively with Apgar score. In addition, cardiac troponin T demonstrates good sensitivity to predict myocardial dysfunction and mortality in asphyxiated neonates. So, it may be a candidate for a biomarker panel to aid outcome prediction, but requires validation in larger multicenter studies.
Footnotes
Author contributions
EGA, ERA, and DSA conceived and supervised the study; MAA was responsible for data collection and analyzed and interpreted the data. All authors provided comments on the manuscript at various stages of development. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.