
Abstract
Background
Accurate blood pressure (BP) measurement is crucial for assessing hemodynamic features in infants with very low birth weight (VLBW). Various methods are available to monitor BP, including both invasive arterial blood pressure (IBP) and non-invasive blood pressure (NIBP). IBP monitoring, although accurate, poses risks due to its invasive approach, while NIBP monitoring, despite being safer, may lack precision.
Objective
To evaluate the agreement between IBP and NIBP measurements and assess the reliability of NIBP in diagnosing hypotension among VLBW infants.
Methods
This study was conducted in the neonatal intensive care unit (NICU) of King Fahd Armed Forces Hospital, Jeddah, Saudi Arabia. VLBW infants (n = 40) with IBP measured via an umbilical arterial catheter (UAC) or peripheral arterial line (PAL) were included. Simultaneous NIBP measurements were taken using appropriately sized cuffs.
Results
Across 3260 paired measurements, NIBP showed a mean bias of −6 ± 10 mmHg compared to IBP, with 95% limits of agreement from −25.6 to 13.6 mmHg. NIBP overestimated systolic, diastolic, and mean arterial pressures (MAP) by 8.9 mmHg, 7.47 mmHg, and 6.76 mmHg, respectively (all p < 0.001). Overall, 58% of pairs exceeded ±15% of invasive MAP. Invasive hypotension prevalence was 4.3% (MAP < gestational age) and 21.7% (MAP <30 mmHg). Receiver operating characteristics analysis showed modest diagnostic accuracy of NIBP (area under the curve = 0.627 and 0.707), with specificity >90% but sensitivity only 26.6%.
Conclusions
NIBP overestimates blood pressure, and IBP is the gold standard method for accurate BP assessment in VLBW infants.
Keywords
Introduction
Physicians often use blood pressure (BP) to indicate any hemodynamic illness in infants. Blood pressure is usually known as arterial pressure as well. The blood pressure, along with other indicators, helps the physicians determine the tissue perfusion and oxygenation status. 1 Managing hypotension among infants is still a debatable topic, as there is no well-developed consensus among physicians on what kind of pharmacotherapy should be utilized to manage it. However, despite the lack of consensus, the decision about pharmacotherapy critically relies on the measured blood pressure. 2
Measuring the blood pressure of neonates in the intensive care unit consists of both invasive and noninvasive methods. Invasive blood pressure (IBP) is estimated by transducing either an umbilical or a peripheral arterial line and is considered the “gold standard” for accuracy. However, this accuracy comes with the cost of many complications, such as infection or events which are associated with this invasive method. 3 On the other hand, the noninvasive blood pressure (NIBP) measuring method relies on automated oscilloscopes, which use inflation and deflation methods using a cuff placed on an arm or a leg. Physicians often rely upon this method despite inaccuracies due to the ease of obtaining results and avoiding complications. 3
Epidemiological data indicate that hypotension occurs in up to 30–50% of extremely low birth weight infants (<1000 g), and BP variability has been linked to higher rates of intraventricular hemorrhage (IVH) and mortality hypotension in very low birth weight (VLBW) infants can be explained by their immature cardiovascular system, limited myocardial contractility, and reduced vascular tone. These infants often experience rapid fluctuations in BP during the transitional circulation period, making close monitoring essential to prevent end-organ hypoperfusion and complications such as intraventricular hemorrhage (IVH), making accurate measurement of BP in VLBW infants important to prevent these complications.4,5
IBP monitoring using either an umbilical arterial catheter (UAC) or peripheral arterial line (PAL) by inserting a catheter either in radial or posterior tibial arteries are the gold standard for BP monitoring in the NICU, although studies show that UAC use is associated with thromboembolic complications in approximately 10–20% of cases, while PAL placement can lead to limb ischemia in 5–10% of infants also IBP carrying other risks including technical difficulty in tiny arteries, infection, limb, hemorrhage, catheter malposition, and need for meticulous damping/zeroing. Despite these risks, invasive monitoring remains widely used in NICUs because of its superior accuracy compared to NIBP. 6
NIBP monitoring using an oscillometer with an appropriately sized cuff is commonly used in NICU without consistent published data about its accuracy, agreement with IBP, and reliability to diagnose hypotension in sick newborn infants, especially during the early transition period and with a trend for losing that correlation with lower blood pressure and with decreasing both weight and gestational age (GA). 7
Despite that, non-invasive monitoring of blood pressure using a proper cuff size and oscillometer is commonly used in the NICU, published data on agreement with invasive BP or accuracy are not consistent. Moreover, its reliability in diagnosing hypotension in the early transitional period, especially with lower gestation, postnatal age, and/or birth weight, is highly questionable, requiring better clarification on a larger scale of data in sick infants. 1
This study aims to assess the accuracy of NIBP in VLBW infants by measuring the agreement and clinically acceptable differences (pre-specified as ±15% from invasive MAP, based on neonatal hemodynamic practice and prior literature), the ability of NIBP to diagnose hypotension using the most acceptable definitions (mean arterial blood pressure (MAP) less than 30 mmHg, and MAP less than gestational age), as well as to identify clinical factors affecting NIBP reliability. 8
Methods
Patients
This prospective study was conducted in the Neonatal Intensive Care Unit (NICU) at King Fahd Armed Forces Hospital (KFAFH) in Jeddah, Saudi Arabia. The hospital used to have an average annual delivery of 6500 deliveries per year. The study was conducted for 14 months, from December 2018 to January 2020.
VLBW infants (less than 1500 gm) whose primary treating team according to our NICU policy (intubated newborn infants less than 28 weeks GA or sicker older infants needed high respiratory setting or inotropic support) inserted either an umbilical arterial Catheter (UAC) or peripheral arterial line (PAL) without having any complex congenital heart disease or severe dysmorphic features including limb anomalies and after getting consent from one of the parents.
This study was conducted in accordance with the ethical standards of the institutional research committee and with the Helsinki Declaration. The study was approved by the KFAFH research and ethics committee with reference number REC 248.
Study protocol
NIBP measurements were taken regularly from the right arm unless a PAL was inserted in the right radial artery; we used the left arm with intervals between 30 min and 1 h according to the acuity of the patient as per unit nursing protocol.
NICU-trained nurses used either cuff sizes 1 or 2 according to mid-arm circumference 3–6 and 4–8 cm, using Spacelab SL 2700 monitor (Spacelabs Health Care, LCC USA). These measurements were recorded by bedside nurses as systolic, mean, and diastolic NIBP.
At the same moment recorded IBP was recorded using the same monitor attached to either a peripheral arterial line or appropriate high position UAC lying between T6-T9 with VYGON 3.5 French polyurethane Umbilical catheters connected to transducer kit (Meritrans DTXPlus®, Merit Medical Singapore Ltd) Meritrans DTXPlus® (Merit Medical Singapore, LTD) after zeroing and removing air bubbles, and to be sure of an acceptable waveform with the presence of the dicrotic notch and not dumping with running heparinized half normal saline 0.25 unit heparin/ml at a rate 0.5 ml/hour, systolic, mean and diastolic IBP were recorded simultaneously with NIBP.
We analyzed simultaneous, time-matched reading pairs, yielding 3260 paired IBP–NIBP comparisons across the cohort. Bedside nurses continue to record both NIBP and IBP as well as any boluses or inotropes given to the baby till removal of the arterial line, according to the stability of the patient, according to our NICU practices. Bedside staff could view both IBP and NIBP as part of standard care; acquisition followed a standardized protocol (site, cuff size, positioning, and timing). Datasets were analyzed by investigators not involved in bedside care.
Other variables and outcomes that could be affected by blood pressure, like initial hemoglobin, gestational age, birth weight, Days of life, early mortality within the first week of life, intraventricular hemorrhage, and survival, were recorded in the data collection sheet and then transferred to the data Excel sheet.1,8
Statistical analysis
Statistical analysis was done by using SPSS version 26 (IBM: Armonk, NY, USA). Continuous variables were presented as the mean ± standard deviation (SD). The mean values of blood pressure readings for each infant across the hospitalization days were used to describe the characteristics of the patients.
Bland-Altman test and univariate correlation analysis were used to compare the obtained mean arterial pressure values between the invasive and non-invasive measures. For each comparison between the two devices’ values, the statistical analyses were performed twice:
(1) using all the obtained values regardless of the differences between the two readings (real-world performance). (2) using the values where the absolute difference between the two readings is ≤15% (best-case scenario) (pre-specified as a clinically acceptable difference following neonatal literature, including Zhou et al., 2016). 8
Receiver operating characteristics (ROC) were used to determine the sensitivity and specificity of non-invasive mean arterial blood pressure to diagnose hypotension using MAP <30 mmHg and MAP < gestational age by week, reported separately for each definition. Due to the natural blood pressure fluctuation after delivery, within-day MAP variability was calculated using (highest MAP – lowest MAP) of each patient for the first 3 days. Analysis of variance with repeated measures was conducted to compare mean blood pressure variability between and within the subjects for each day. 2-Way ANOVA (Device x time) with repeated measures were utilized for the first 3 days. Post-hoc Tukey’s test was used to determine the differences between means. Statistical significance was defined as p < 0.05. Given repeated measures per infant, we acknowledge within-infant clustering; diagnostic metrics are reported at the reading level, and this clustering is noted as a limitation.
Results
Patient characteristics
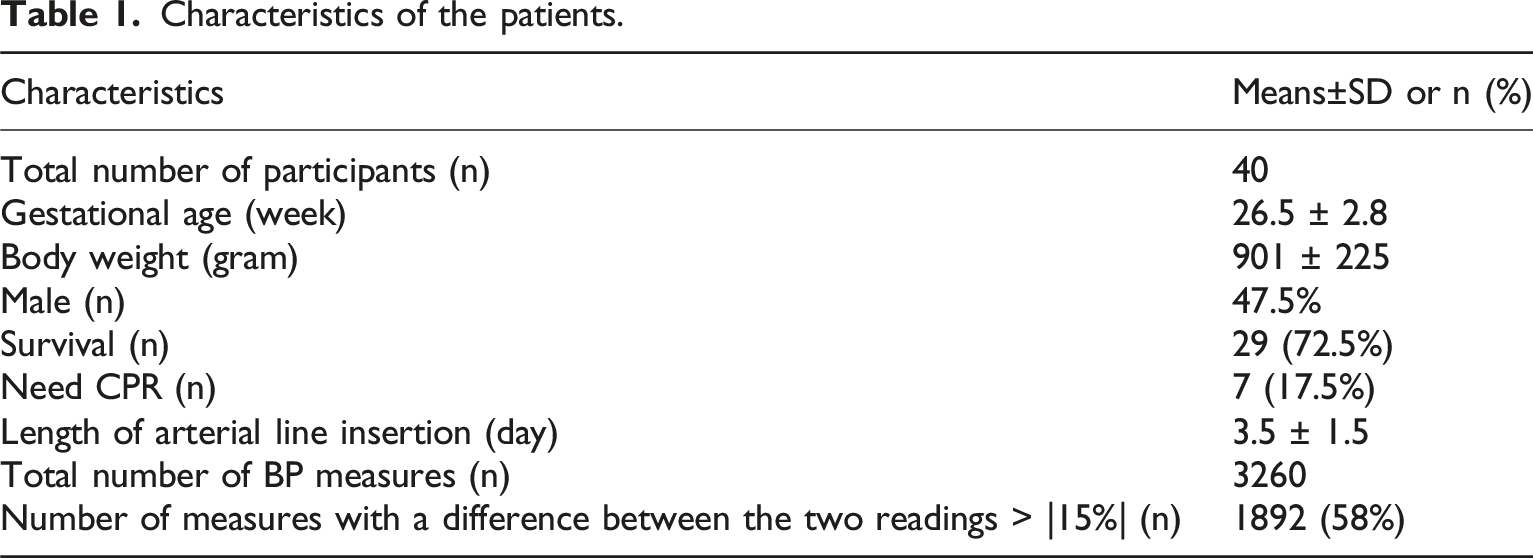
Characteristics of the patients.
Blood pressure values
Agreement between non-invasive (NIBP) and invasive (IBP) blood pressure—full cohort. Direction of difference is NIBP−IBP (mmHg).
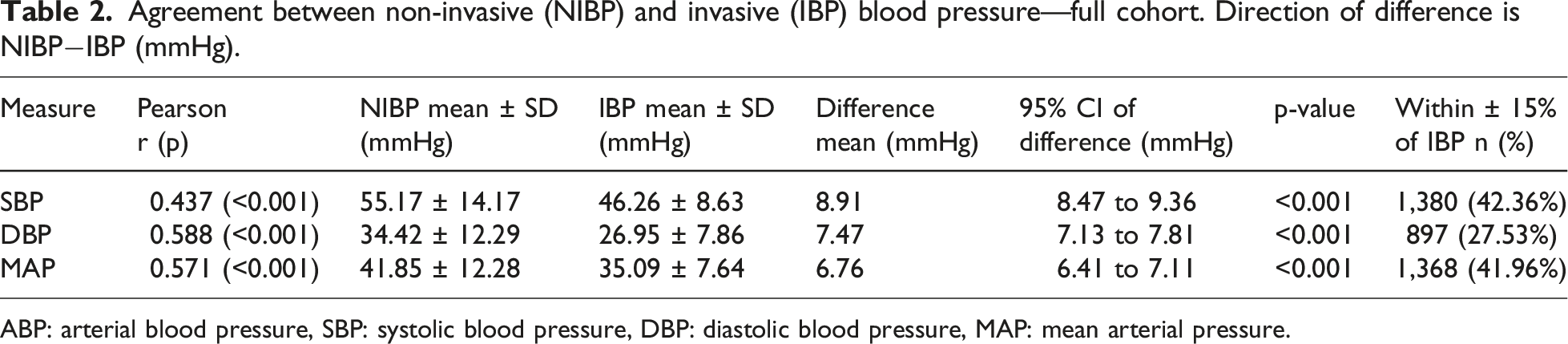
ABP: arterial blood pressure, SBP: systolic blood pressure, DBP: diastolic blood pressure, MAP: mean arterial pressure.
The comparison of blood pressure (BP) values obtained from IBP and NIBP measurements across different subgroups of gestational age and birth weight is summarized in Table S1. Given the small size of several subgroups (e.g., BW <700 g n = 6; GA >29 weeks n = 4) and to avoid over-interpretation, subgroup comparisons are presented as exploratory in Supplemental Table S1. The original GA cut-off (≤29 vs > 29 weeks) was selected to balance group sizes in this cohort; we acknowledge that ≤28 weeks is a standard definition for extreme prematurity. Across subgroups, directionality is consistent with the primary analysis: NIBP overestimates IBP (MAP typically by ∼ 7–11 mmHg), with larger absolute differences at lower GA and birth weight.
MAP variability increased over the first 3 days by both methods, and NIBP values remained consistently higher than IBP, directionally consistent with the overall systematic NIBP overestimation. These modality differences in early postnatal days are directionally consistent with the overall systematic NIBP overestimation detailed in Supplemental Table S2.
Figure 1(a) shows a Bland–Altman plot of the difference between invasive MAP and non-invasive MAP against the average MAP (mmHg) for all paired readings. It demonstrated a negative mean difference (invasive MAP – non-invasive MAP <0), indicating that the non-invasive method consistently measures higher values than the invasive method. Mean bias = −6 mmHg (non-invasive MAP higher), 95% limits of agreement −25.6 to 13.6 mmHg; evidence of proportional bias with greater dispersion at higher MAPs and systematic overestimation in the low MAP range. Despite this trend, the variability between the two modalities was significant, as evidenced by the wide limits of agreement (±1.96 SD) and the presence of data points outside these limits. This suggests limited agreement between invasive and non-invasive blood pressure measurements. The correlation plot (Figure 1(b)) revealed a statistically significant, weak-to-moderate positive correlation between invasive MAP and non-invasive MAP ( (a) Bland–Altman plot demonstrating the difference between invasive mean arterial blood pressure (MAP) and non-invasive MAP against the average MAP (all paired readings). (b) Correlation plot demonstrating a weak-to-moderate positive association between invasive mean arterial blood pressure (MAP) and non-invasive MAP.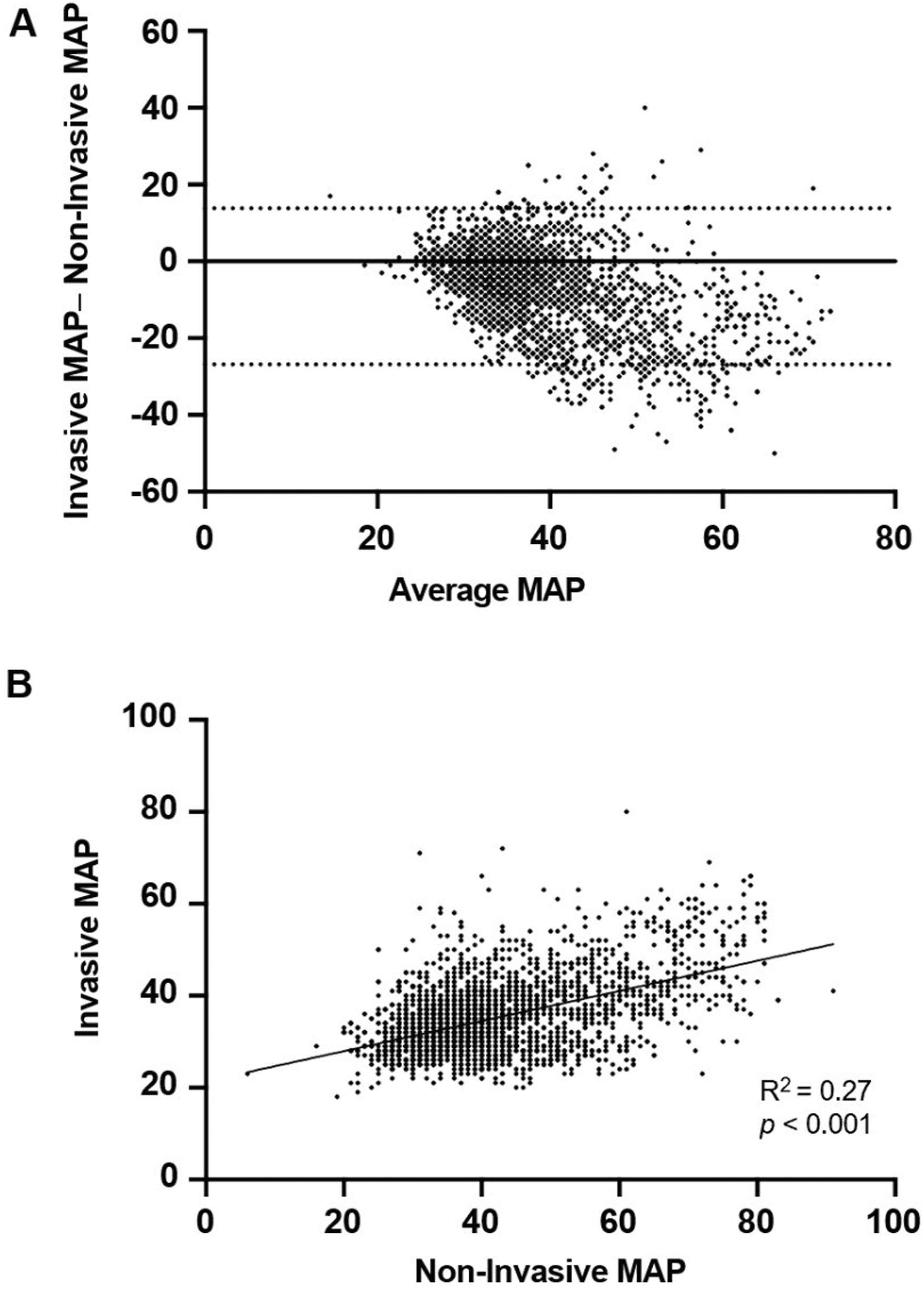
Figure 2 highlights the discrepancy between the two methods (Figure 2(a)), demonstrating reduced apparent bias after restricting to pairs within the pre-specified acceptable difference of ±15% of invasive MAP (Bias ≈ −0.7 ± 3 mmHg with narrow dispersion); this restriction is expected to narrow the limits of agreement and should not be interpreted as overall agreement. The correlation plot (Figure 2(b)) revealed a stronger correlation between invasive MAP and non-invasive MAP (R2 = 0.81, p < 0.001), illustrating a best-case scenario within the acceptable-difference subset. Figure 2 is presented for illustration and was not used for diagnostic accuracy estimates. (a) Bland–Altman plot demonstrating the difference between invasive mean arterial blood pressure (MAP) and non-invasive MAP against the average MAP (MAP) mmHg (pairs with absolute disagreement ≤15% of invasive MAP). (b) Correlation plot showing a strong positive relationship between invasive mean arterial blood pressure (MAP) and non-invasive MAP.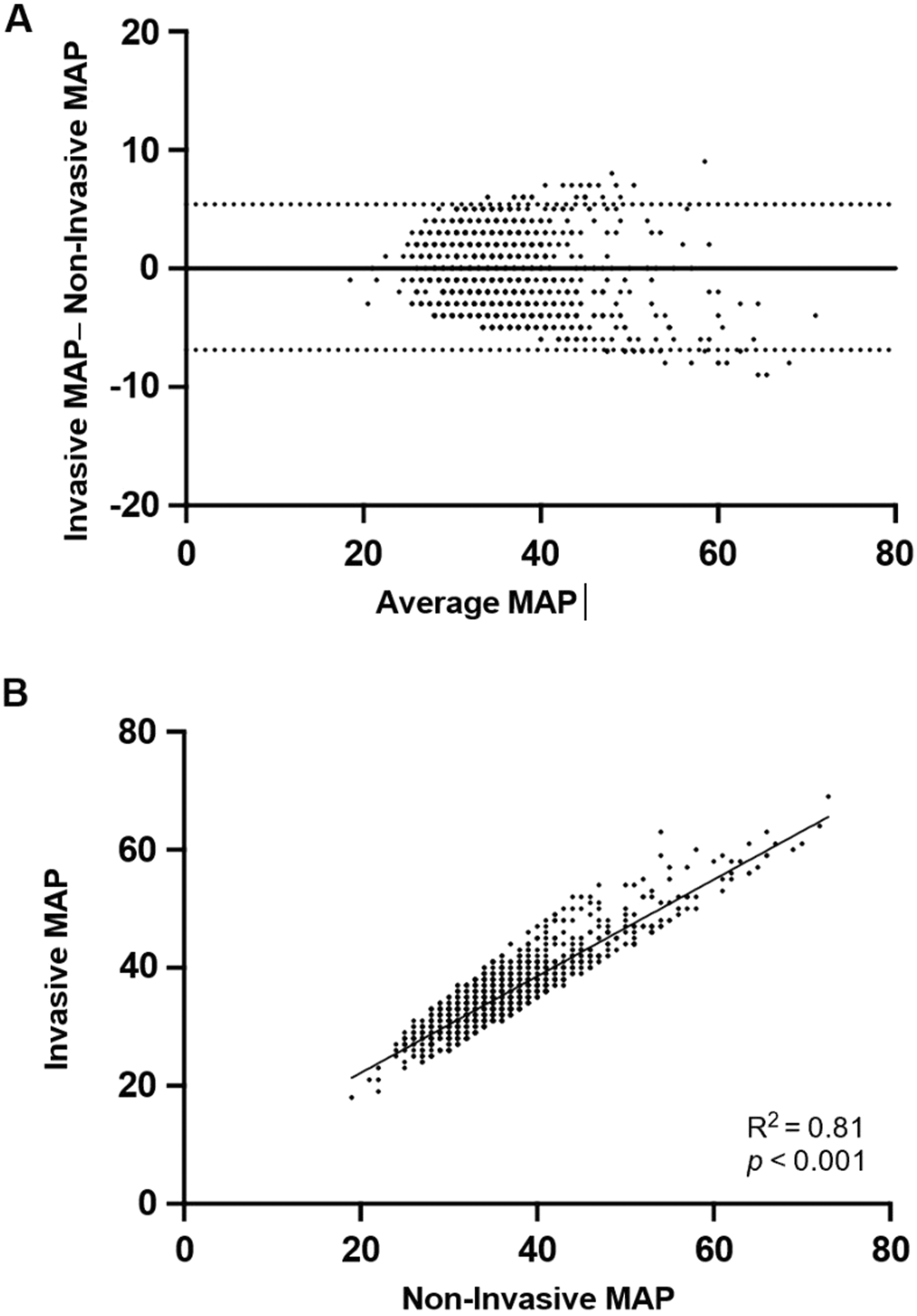
Regression analyses were conducted to explore factors associated with the clinical outcomes S-S, D-D, and M-M. For S-S, the overall model did not reach statistical significance, but age by days at assessment was positively associated with higher S-S values and explained about 18% of the variation when tested alone. For D-D, none of the variables were significant in the full model, although the need for inotropes showed a tendency toward lower D-D values. For M-M, the overall model was also not significant, but prolonged rupture of membranes and inotrope use showed trends toward association. Some variables, such as delayed cord clamping and arterial line use, were excluded from the models because they did not vary in the dataset. Sensitivity analyses that accounted for within-infant clustering yielded inferences consistent with the primary analyses.
We found that the ROC curve assessing the diagnostic accuracy of NIBP in detecting hypotension, defined as an invasive MAP lower than gestational age, yielded an area under the curve (AUC) of 0.627, reflecting only modest discriminative power. At the optimal threshold of ≤30.5 mmHg, NIBP demonstrated very low sensitivity (26.6%) but high specificity (90%). The overall accuracy was 87.3%, with a positive predictive value (PPV) of merely 10.6% and a negative predictive value (NPV) of 96.5%. At this cut-point, NIBP missed 102/139 (73.4%) true hypotensive episodes (MAP < GA). The high NPV (96.5%) reflects low prevalence (4.3%) rather than strong test performance; therefore, normal or borderline NIBP values cannot reliably exclude hypotension.
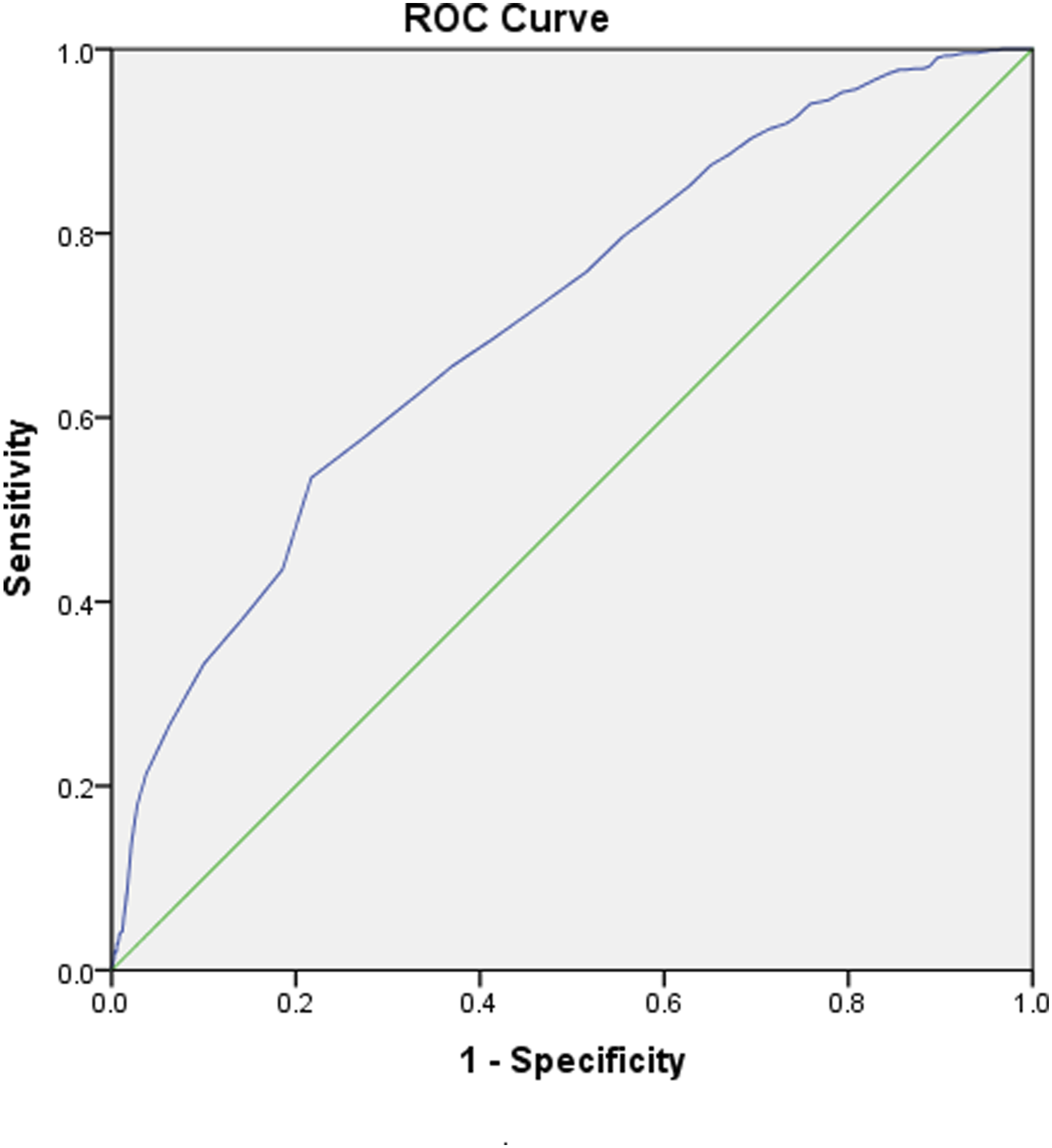
Using the alternative definition of hypotension (MAP <30 mmHg), the ROC curve showed an AUC of 0.707. At the NIBP threshold of ≤30.5 mmHg, sensitivity was 26.6%, specificity 93.7%, PPV 54.0%, and NPV 82.2%, with an overall accuracy of 85.6%. NIBP missed 519 of 707 (73.4%) true hypotensive episodes. At this cutoff, classification counts were 37 true positives, 312 false positives, 102 false negatives, and 2807 true negatives for MAP < GA (prevalence 4.3%), and 188 true positives, 161 false positives, 519 false negatives, and 2390 true negatives for MAP <30 mmHg (prevalence 21.7%). Figures 3 and 4 present the separate ROC curves for both definitions. The predictive accuracy of the Non-Invasive Mean Blood Pressure (NIBP) for hypotension diagnosis (considering a patient hypotensive when the mean blood pressure is below gestational age), ROC, Receiver operating characteristic. The predictive accuracy of the Non-Invasive Mean Blood Pressure (NIBP) for hypotension diagnosis (considering a patient hypotensive when the mean blood pressure is less than 30 mmHg), ROC, Receiver operating characteristic.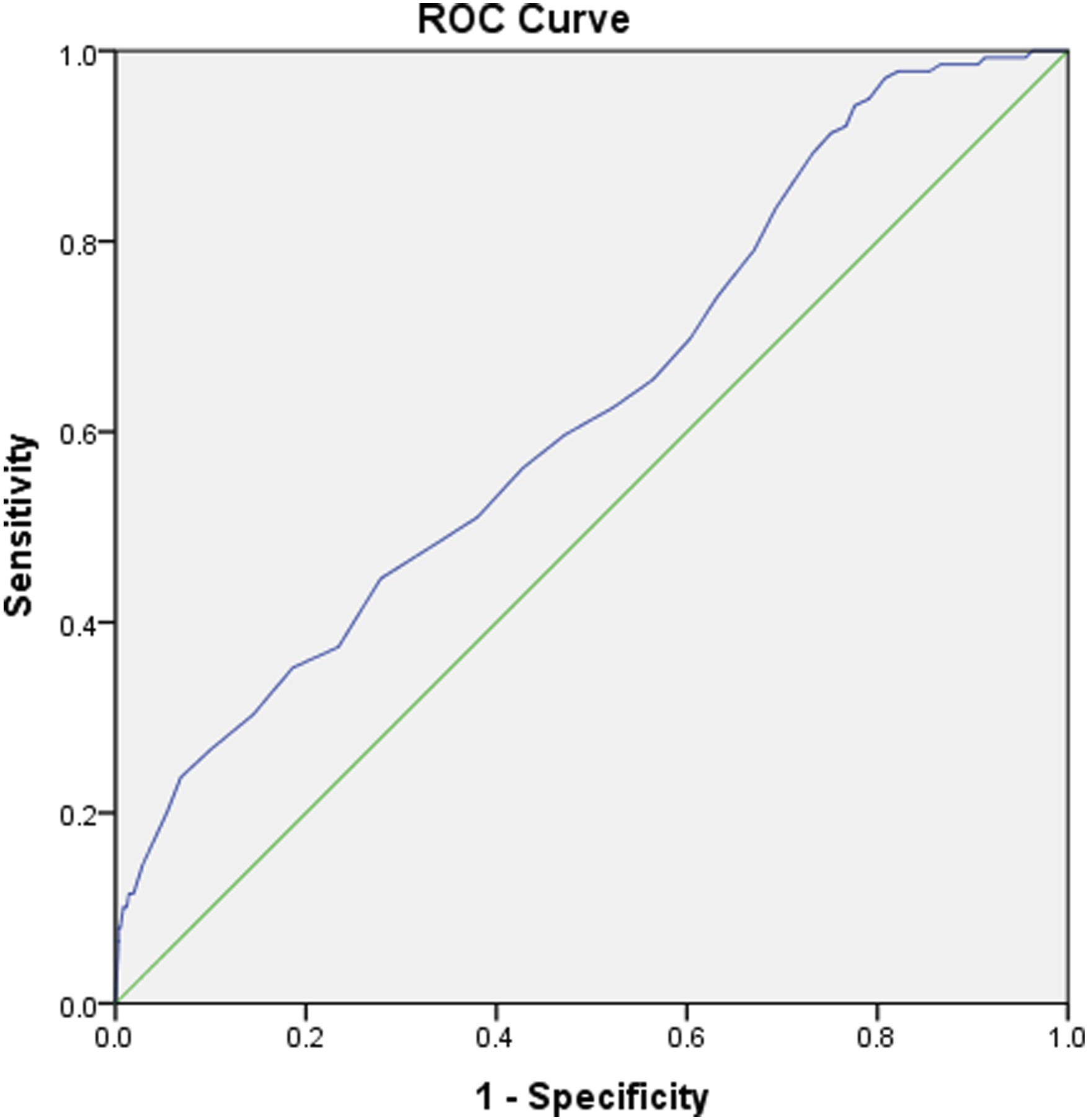
Prevalence-dependence of NPV: With sensitivity 0.266 and specificity 0.900 (MAP < GA), expected NPV declines as prevalence increases (approximately 92% at 10% prevalence; 83% at 20%; 74% at 30%; 65% at 40%). With sensitivity 0.266 and specificity 0.937 (MAP <30 mmHg), NPV similarly falls (about 92% at 10%; 84% at 20%; 75% at 30%; 66% at 40%), Table S3. This indicates that high NPV in our cohort is prevalence-driven and should not be interpreted as a reliable exclusion of hypotension in higher-risk settings.
Discussion
The current study aimed to investigate the agreement between NIBP measurements and IBP measurements in infants with VLBW and to assess the reliability of NIBP in different clinical scenarios. The findings of this study indicate significant differences between NIBP and IBP measurements. Moreover, the NIBP levels of infants, especially in the first 72 h of life and in infants with lower gestational ages and birth weights, were significantly higher when compared to IBP.
Overall, the study findings revealed that NIBP values recorded were consistently higher when compared to IBP in all categories. This was consistent with the findings of previous studies, where the NIBP was found to be higher than the IBP.9,10 This difference in the values of IBP and NIBP was more evident when different classifying factors were involved, such as gestational age and body weight.11,12 For example, the infants who weighed less than 1000 g had higher NIBP as compared to IBP, and similarly, infants with a gestational age of less than 29 weeks had a similar trend. These findings were in accordance with the previous studies, which had shown there might be an overestimation in BP when taken through the cuff method in infants with VLBW. 11
Furthermore, the analysis of MAP variability over the first 3 days indicated significant differences between NIBP and IBP measurements. However, it is important to mention that in both methods, MAP over time was increased in both techniques. A similar trend was found in this case as well, where the invasive MAP was lower as compared to the non-invasive MAP. This consistently increased non-invasive MAP indicates a limitation of the method, specifically in the early transitional period of infants, where accurately measuring the blood pressure of infants is highly critical. 13
The consistent increase in the value of NIBP that has been observed in this study was consistent with the previous findings. Moreover, the overestimation of NIBP can have a critical impact on the clinical implications. This overestimation accounts for the limitation of the method, which indicates the inaccuracy of the technique.12,14 Accurate measurement of blood pressure, especially in VLBW infants, is very crucial to assess the hemodynamic status and its management.14,15
The overestimation of blood pressure by NIBP can have critical clinical implications. Accurate blood pressure measurement is crucial for assessing the hemodynamic status and guiding therapeutic interventions in critically ill infants. Misinterpretation of low NIBP readings may lead to unnecessary treatment with inotropes or fluid boluses, which can have adverse effects, including fluid overload and potential cardiovascular complications.15–17 Conversely, relying solely on NIBP measurements may mask true hypotension, delaying necessary interventions and increasing the risk of morbidity and mortality, including IVH.5,13
Various factors are associated with inaccuracies in NIBP measurement in infants. One of the factors that contributes to inaccuracies is the use of oscillometric devices, as these devices completely rely on cuff inflation and deflation. That is because these devices cannot detect the changes in small and fragile infants with low body weight and lack sensitivity to the patient age group. Additionally, the cuff size is not universal; therefore, selection of the appropriate size is necessary for accurate measurement, along with the correct position. 18 A slight inaccuracy of the deviated decision can significantly impact the measurement through NIBP. 19
IBP could be prioritized during the critical first days of life, when hemodynamic instability is most pronounced, and especially in infants requiring inotrope or vasoactive support. 20 Furthermore, IBP is strongly indicated in the most vulnerable subgroup of infants with birth weight less than 700 g, where accurate titration of therapy is essential and the risks of mismanagement due to NIBP inaccuracy are highest. In these scenarios, IBP remains the gold standard, despite its procedural risks, because it provides reliable continuous monitoring that is indispensable for guiding clinical decisions in critically ill VLBW infants. 14
In the present study, NIBP demonstrated only modest discriminative ability for detecting hypotension in VLBW infants, with low sensitivity and poor positive predictive value despite high specificity and negative predictive value. These findings emphasize that NIBP should not be used to exclude hypotension and is unreliable for confirming the diagnosis, underscoring the continued importance of invasive monitoring when accurate blood pressure assessment is required. The high NPV observed for MAP < GA reflects low prevalence (4.3%) rather than strong test performance; when prevalence was higher (MAP <30 mmHg, 21.7%), NPV was notably lower (82.2%).
It is important to mention that IBP measurements are still a gold standard for measuring the blood pressure in infants, especially those with VLBW who are in the early days of life. However, due to complications associated with IBP, NIBP may be utilized. Therefore, the clinician or physician must be aware of the fact that there might be an overestimation in the value of BP that has been recorded by NIBP, and this overestimation is accounted for in case of making a clinical decision. Furthermore, there is a need to refine and advance the measurement of BP through NIBP devices using technological advancements, especially in the case of cuff design and size selection, so that more accurate readings can be taken with lower differences between NIBP and NIBP.
Novelty of the Study: Our findings demonstrate that the trend of NIBP overestimating IBP is consistently present in VLBW infants, and importantly, that NIBP shows low sensitivity and poor positive predictive value for diagnosing hypotension when compared to invasive measurements. This extends the literature beyond simple agreement analyses by directly testing the diagnostic performance of NIBP in a high-risk cohort.7,14 By framing NIBP as a diagnostic tool rather than merely a surrogate measurement, our study provides new evidence that normal or borderline NIBP readings cannot be used to exclude hypotension in VLBW infants. This distinction is clinically significant: in practice, clinicians often rely on NIBP for convenience and safety, yet our results show that such reliance may lead to missed episodes of hypotension and delayed interventions. Thus, the novelty of this study is in demonstrating that NIBP is inadequate as a diagnostic test for hypotension in VLBW infants, reinforcing the need for invasive monitoring when accurate hemodynamic assessment is required.
Limitations
The limitation of this study is that this is a single-center design with a relatively small sample size. Repeated measures per infant (clustering) that may affect precision; bedside acquisition could not be blinded to IBP display (standard care), although analyses used de-identified data. We did not prospectively track eligible but non-enrolled infants with arterial lines, which may limit generalizability. However, further studies that include multiple centers and large sample sizes can provide data that is more acceptable and validated, so that the results of this study can be validated. Another aspect that can provide valuable insight into the inaccuracies is to explore the impact of different cuff sizes, placement techniques, and device calibration on NIBP accuracy. This way, the findings of this study are not only validated but also can improve clinical practice.
Conclusion
In conclusion, this study highlights significant discrepancies between NIBP and IBP measurements in VLBW infants, with NIBP often overestimating blood pressure by approximately 7–11 mmHg, most pronounced in extremely premature and lowest birth weight infants. Accurate blood pressure monitoring is essential for the management of critically ill infants, and the observed systematic overestimation argues against using NIBP to exclude hypotension. NIBP demonstrated low sensitivity for detecting hypotension (26.6%), and the majority of NIBP readings (58%) differed from IBP by more than 15%, indicating substantial discordance. Accordingly, NIBP may provide false reassurance in critically ill infants and should not be considered dependable for ruling out hypotension. Clinicians should prioritize IBP measurements for precise hemodynamic assessment, particularly during the early postnatal period and whenever hypotension is suspected or vasoactive therapy is being considered. IBP remains the gold standard for accurate hemodynamic assessment. Further research and technological advancements are needed to enhance the accuracy and reliability of non-invasive blood pressure monitoring in this vulnerable population.
Supplemental Material
Supplemental Material - Reliability of non-invasive blood pressure monitoring in sick very low birth weight preterm infants
Supplemental Material for Reliability of non-invasive blood pressure monitoring in sick very low birth weight preterm infants by Mohamed Abdelmaw, Enshrah Radwan, Adeeb Khawaji, Maan Abuzaid, Raniah Aljeaid, Ahmed Elkordy, Ahmed Abuelnour, Nisreen Kafi, and Ahmed Dohain in Journal of Neonatal-Perinatal Medicine.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.