
Abstract
Background
The effectiveness of phototherapy for neonatal hyperbilirubinemia depends on irradiance and exposed body surface area. In resource-limited settings, suboptimal light delivery may reduce treatment efficiency. Reflective materials such as aluminium foil may improve light utilization during phototherapy.
Objective
To evaluate the efficacy and safety of aluminium foil reflector-assisted phototherapy compared with standard LED phototherapy in term neonates with hyperbilirubinemia.
Methods
In this randomized controlled trial conducted between August 2024 and August 2025 at a tertiary neonatal unit, 90 term neonates requiring phototherapy were randomized to receive either aluminium foil reflector-assisted phototherapy (n = 45) or standard LED phototherapy (n = 45). Total serum bilirubin (TSB) was measured at baseline and at 24-h intervals during phototherapy. Primary outcomes were rate of bilirubin reduction at 24 h and total duration of phototherapy. Secondary outcomes included physiological parameters, weight change, and adverse effects. Analysis of covariance was performed to adjust for baseline covariates.
Results
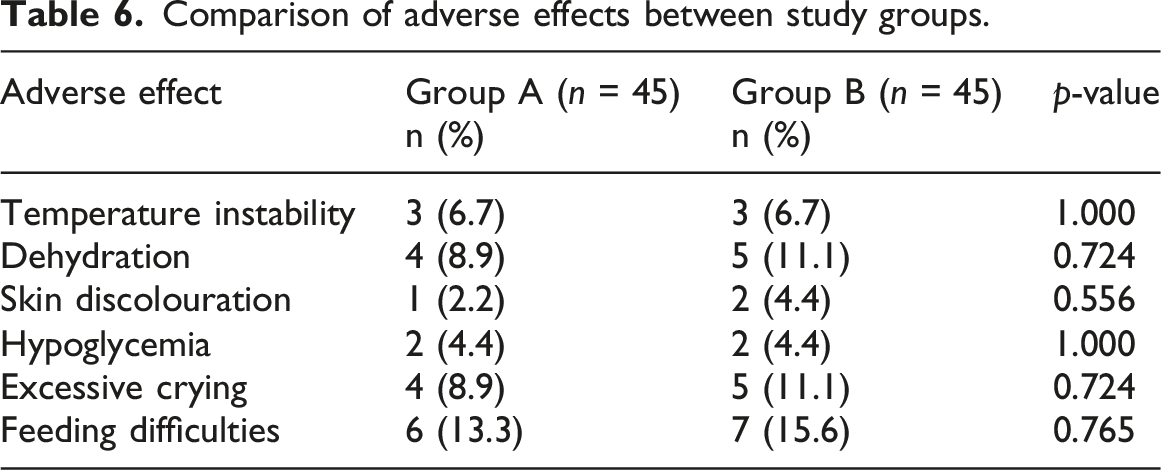
Baseline TSB levels were similar between groups (15.43 ± 1.77 vs 15.85 ± 1.97 mg/dL; p = 0.111). After 24 h, the mean reduction in TSB was greater in the reflector group (3.91 ± 1.96 vs 2.76 ± 1.40 mg/dL; mean difference 1.15 mg/dL; p = 0.006). The total duration of phototherapy was shorter in the reflector group (32.62 ± 7.89 vs 39.04 ± 6.69 h; mean difference 6.42 h; p < 0.0001). The treatment effect remained significant after adjustment for gestational age and postnatal age using ANCOVA. No significant differences in adverse events were observed.
Conclusions
Aluminium foil reflector-assisted phototherapy was associated with faster bilirubin reduction and shorter treatment duration without increased adverse effects. This low-cost modification may improve phototherapy efficiency in resource-limited neonatal care settings.
Keywords
Introduction
Neonatal jaundice is one of the most common conditions encountered during the early neonatal period and remains a frequent cause of hospital admission in the first week of life. Approximately 60% of term and up to 80% of preterm neonates develop visible jaundice due to increased bilirubin production and immature hepatic conjugation.1,2 While most cases are benign, significant hyperbilirubinemia requires timely intervention to prevent acute bilirubin encephalopathy and kernicterus, which are associated with permanent neurological damage and mortality, particularly in low- and middle-income countries. 3 Phototherapy is the standard treatment for unconjugated hyperbilirubinemia. Its effectiveness depends on several factors, including light wavelength, irradiance, duration of exposure, distance from the light source, and the proportion of exposed body surface area. 4 Despite adherence to recommended wavelengths, many neonatal units continue to use phototherapy devices with limited irradiance, resulting in slower bilirubin reduction and prolonged treatment duration.5,6
The use of reflective materials around phototherapy units has been proposed to enhance light utilization by redirecting scattered light back onto the infant’s skin. Aluminium foil is inexpensive, widely available, and highly reflective, making it a practical option in routine clinical settings. Previous studies have explored the use of reflective materials during phototherapy to enhance light utilization and improve bilirubin reduction, although evidence from randomized controlled trials remains limited.7,8 The present study aimed to evaluate the efficacy and safety of aluminium foil reflector-assisted phototherapy compared with standard LED phototherapy in term neonates with hyperbilirubinemia.
Materials and methods
Study design and setting
This randomized controlled trial was conducted in the Neonatal Intensive Care Unit (NICU) of the Department of Paediatrics at Vinayaka Mission’s Medical College and Hospital, Karaikal, Puducherry, India. The study was conducted and reported in accordance with the CONSORT guidelines for randomized controlled trials. The study period extended from August 2024 to August 2025. Approval was obtained from the Institutional Ethics Committee (IEC/VMMCH//2024/DEC/04). Written informed consent was obtained from parents or legal guardians of all enrolled neonates in accordance with the Declaration of Helsinki.
Study population and sample size
The study included term neonates (gestational age ≥37 weeks) admitted to the NICU with clinically significant jaundice requiring phototherapy. A total of 150 neonates were assessed for eligibility; 60 were excluded based on predefined criteria, and 90 neonates were randomized into two study groups: an intervention group (Group A, n = 45) and a control group (Group B, n = 45). The flow of participants through the trial is shown in Figure 1. The sample size was estimated based on expected differences in bilirubin reduction reported in previous studies evaluating reflector-assisted phototherapy. Assuming a two-sided significance level (α) of 0.05 and statistical power of 80%, the required sample size was approximately 40 neonates per group. To allow for potential attrition, 45 neonates were included in each group, resulting in a total sample size of 90 neonates. CONSORT 2010 flow diagram showing participant enrolment, allocation, follow-up, and analysis. A total of 150 neonates were assessed for eligibility. Of these, 60 were excluded (did not meet inclusion criteria = 35, declined to participate = 15, other reasons = 10). The remaining 90 neonates were randomized into two groups: Group A (aluminium foil reflector-assisted phototherapy, n = 45) and Group B (standard LED phototherapy, n = 45). All participants completed the study protocol with no dropouts or loss to follow-up. All 90 participants were analyzed (intention-to-treat analysis).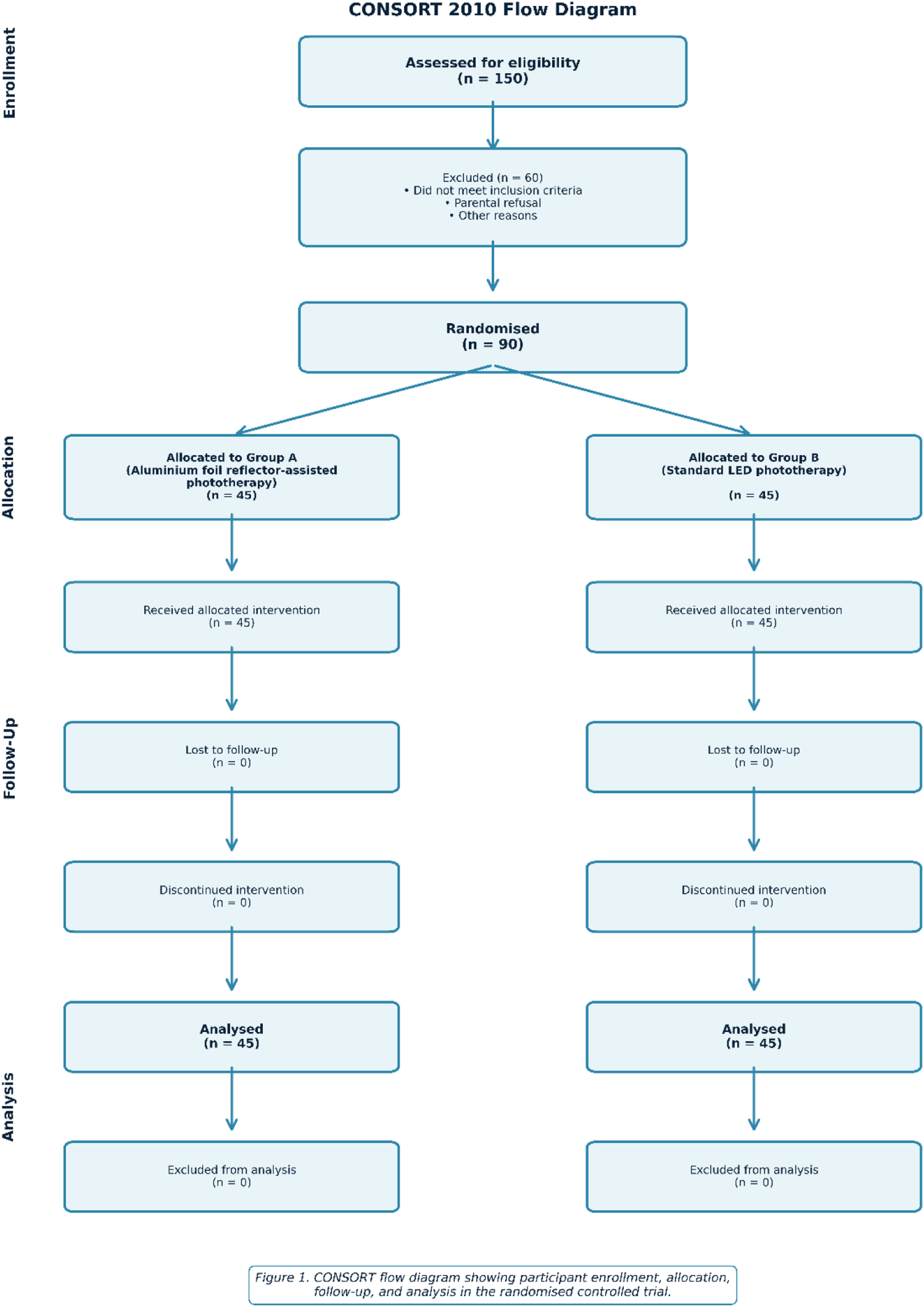
Inclusion and exclusion criteria
Inclusion criteria: (1) term neonates (≥37 weeks gestational age) admitted to the NICU with clinical jaundice and (2) neonates requiring phototherapy based on standard treatment guidelines. Exclusion criteria: (1) neonates with major congenital anomalies, (2) hemodynamically unstable neonates, (3) neonates receiving mechanical ventilation, (4) serum bilirubin levels approaching exchange transfusion thresholds, (5) haemolytic disease such as glucose-6-phosphate dehydrogenase (G6PD) deficiency, and (6) predominantly direct hyperbilirubinemia.
Randomization and allocation
Eligible neonates were assigned to either Group A or Group B using block randomization with a computer-generated random sequence. Allocation concealment was ensured using sequentially numbered opaque sealed envelopes prepared by an independent investigator. Due to the nature of the intervention, caregivers were not blinded to group allocation.
Intervention
All eligible neonates received phototherapy using an overhead LED infant phototherapy unit (SEEFAR Nice 4000 SPOT, Seefar Medical Systems) delivering blue light within the wavelength range of 460–490 nm. Phototherapy initiation and discontinuation were determined according to institutional protocols based on established neonatal hyperbilirubinemia management guidelines considering gestational age, postnatal age, and bilirubin levels. In most cases, phototherapy was initiated when serum bilirubin levels approached the recommended treatment thresholds according to the AAP 2022 guidelines, particularly in the presence of clinical jaundice extending to higher Kramer zones or additional risk factors. In the intervention group, aluminium foil reflector sheets (approximately 18-micron thickness) were fixed along four sides of the radiant warmer frame (two lateral sides, head-end and foot end) surrounding the infant to reflect light toward the exposed body surface. The reflectors were secured using adhesive tape while ensuring adequate ventilation and unobstructed clinical monitoring. The distance between the phototherapy unit and the infant was maintained at approximately 45 cm throughout treatment. Standard eye protection was used for all infants during phototherapy. Infants were monitored regularly for temperature stability, hydration status, and feeding tolerance throughout the treatment period. Intravenous fluids were administered only when clinically indicated according to standard neonatal care protocols. Fresh aluminium foil was used for each patient and discarded as per hospital infection control protocols. Neonates in the control group (Group B) received conventional phototherapy without the use of reflective materials.9,10
Outcome measures
Primary outcomes: (1) rate of reduction in total serum bilirubin levels (mg/dL) at 24 h and (2) total duration of phototherapy (hours). Secondary outcomes included changes in physiological parameters and the occurrence of phototherapy-related adverse effects. Total serum bilirubin levels were measured at baseline and at 24-h intervals during phototherapy as part of routine clinical monitoring. Adverse effects were predefined and monitored using standardized clinical criteria. Temperature instability was defined as axillary temperature <36.5°C or >37.5°C. Dehydration was assessed clinically and supported by weight loss >10% from baseline or reduced urine output. Feeding intolerance was defined as poor feeding or vomiting requiring clinical intervention. Hypoglycemia was defined as blood glucose <45 mg/dL. All adverse events were assessed by treating clinicians during routine monitoring.
Statistical analysis
Data were analyzed using SPSS version 16.0. Continuous variables with normal distribution were expressed as mean ± standard deviation and compared using independent sample t-test; nonnormally distributed continuous variables were compared using Mann–Whitney U test. Categorical variables were expressed as frequencies and percentages and compared using chi-square test or Fisher’s exact test. A p-value of less than 0.05 was considered statistically significant. Analysis of covariance (ANCOVA) was performed with the rate of bilirubin reduction at 24 h as the dependent variable, treatment group as the fixed factor, and gestational age and postnatal age as covariates. This approach was used to adjust for baseline differences between the groups. 11
Results
Baseline characteristics
Baseline demographic characteristics of neonates in the study groups.
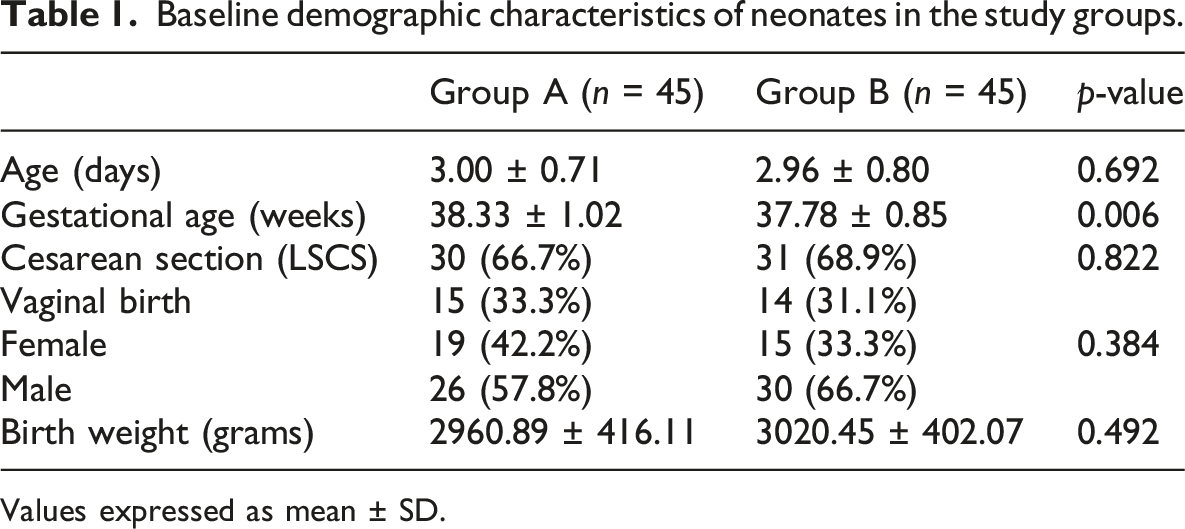
Values expressed as mean ± SD.
Risk factors
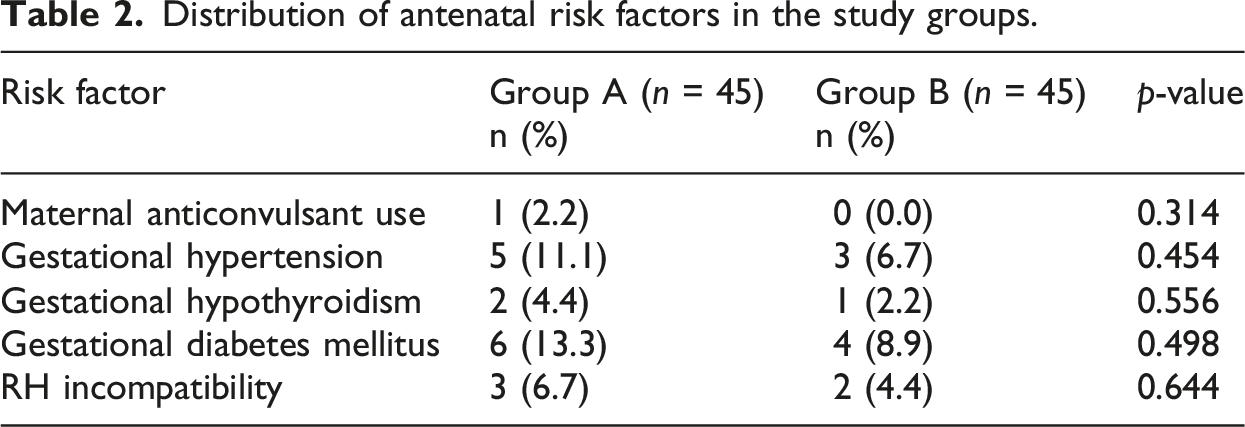
Distribution of antenatal risk factors in the study groups.
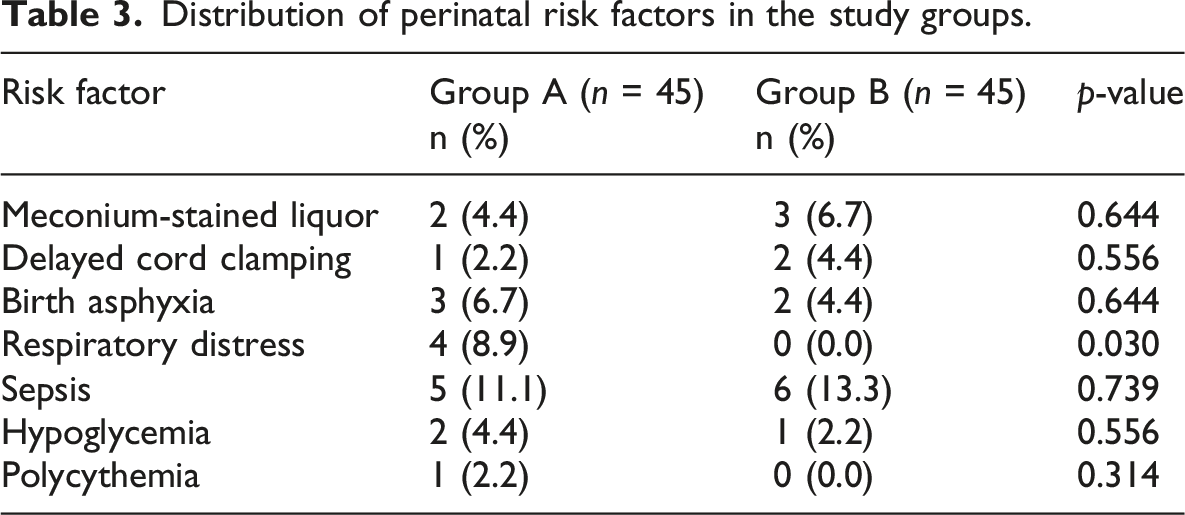
Distribution of perinatal risk factors in the study groups.
Primary outcomes
Comparison of bilirubin levels and physiological parameters between study groups.
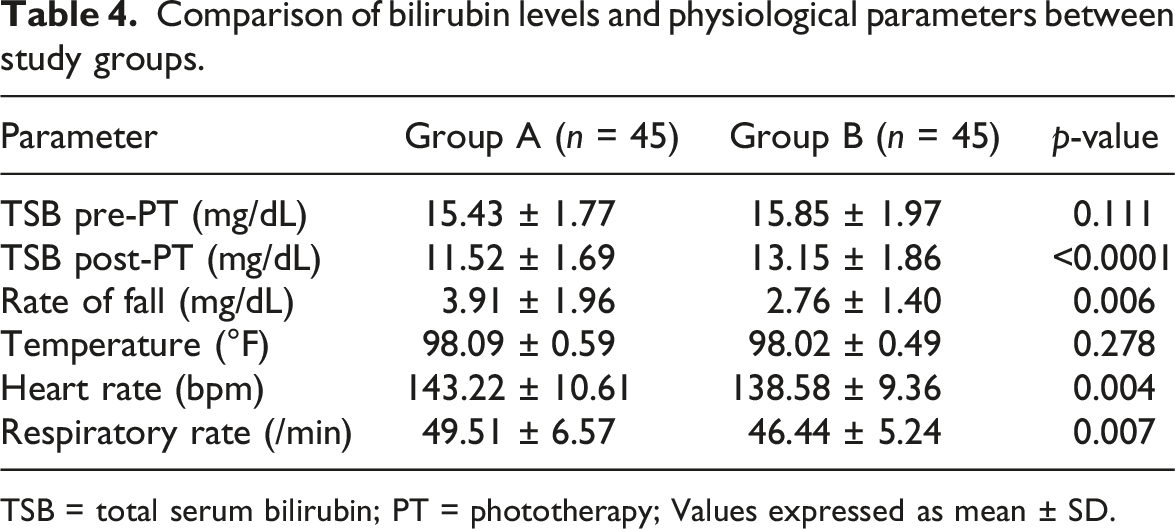
TSB = total serum bilirubin; PT = phototherapy; Values expressed as mean ± SD.
Comparison of total duration of phototherapy between study groups.
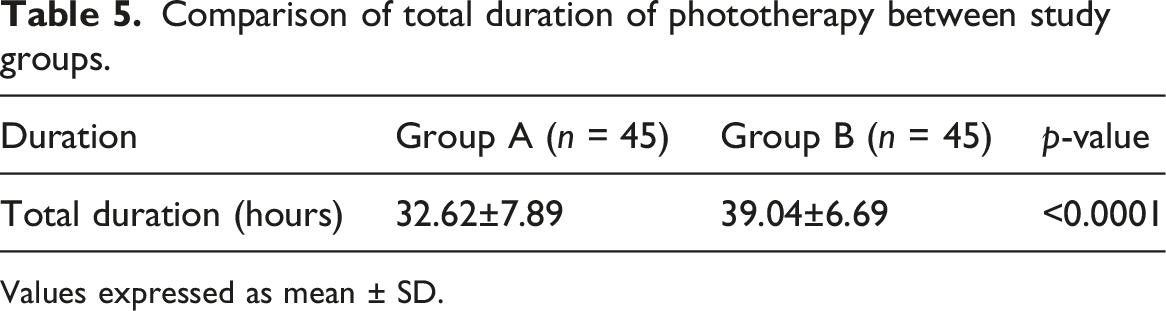
Values expressed as mean ± SD.
Secondary outcomes
Comparison of adverse effects between study groups.
Comparison of weight changes during phototherapy between study groups.
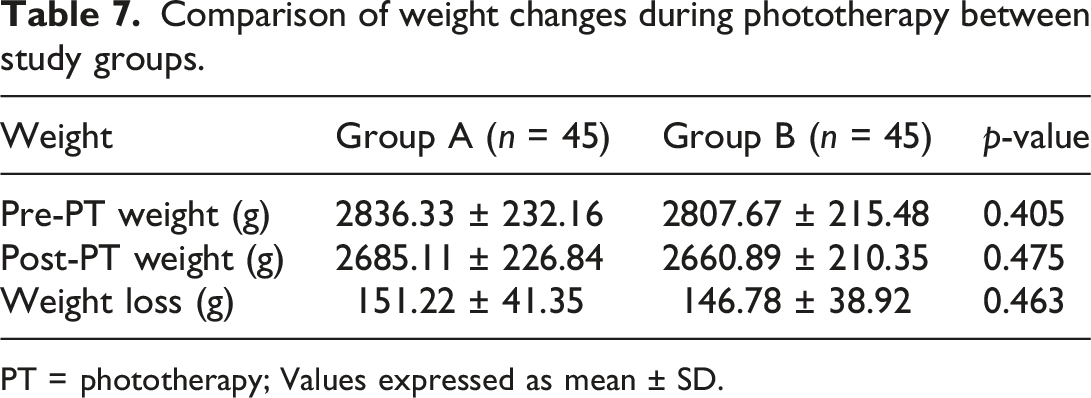
PT = phototherapy; Values expressed as mean ± SD.
Adjusted analysis
ANCOVA analysis for the rate of bilirubin reduction adjusting for covariates (no respiratory distress).

ANCOVA analysis of total duration of phototherapy adjusting for covariates (no respiratory distress).

Discussion
This randomized controlled trial evaluated the effectiveness and safety of aluminium foil reflector-assisted phototherapy compared with standard LED phototherapy in term neonates with hyperbilirubinemia. The findings suggest that the addition of aluminium foil reflectors is associated with a faster reduction in total serum bilirubin levels and a shorter duration of phototherapy compared with standard LED phototherapy, while maintaining physiological stability and a similar adverse effect profile.12,13 The rate of bilirubin reduction over 24 h was significantly higher in the reflector group (3.91 ± 1.96 mg/dL) than in the control group (2.76 ± 1.40 mg/dL), representing a 41.7% greater rate of decline. After adjustment for gestational age and postnatal age using ANCOVA, the treatment effect remained statistically significant, indicating that the observed differences were independent of baseline maturity differences. The results of this study are consistent with earlier clinical trials examining reflective materials during phototherapy. 14 These studies similarly reported faster bilirubin decline and shorter phototherapy duration with reflector-assisted phototherapy. Although the absolute reduction in phototherapy duration was approximately 6.4 h, this difference may still be clinically meaningful. Shorter phototherapy duration can reduce hospital stay, minimize mother–infant separation, decrease nursing workload, and lower healthcare costs, particularly in resource-limited settings. In resource-limited settings where high-intensity LED systems are costly, aluminium foil reflectors are inexpensive and easy to source.15,16 Shortening phototherapy duration may reduce nursing workload, hospitalization time, and healthcare costs. Strengths of this study include randomized allocation with sealed opaque envelope concealment, standardized phototherapy protocols, and objective biochemical outcome measures. Several limitations should be acknowledged.17,18 First, the study was conducted at a single centre, which may limit generalizability. Second, irradiance levels were not measured using a radiometer; therefore, although the reflector intervention improved clinical outcomes, the exact mechanism by which reflectors may enhance phototherapy effectiveness could not be objectively quantified. Third, caregivers were not blinded to treatment allocation, which may introduce potential decision bias in determining phototherapy discontinuation, although standardized bilirubin thresholds were applied.19,20 Finally, the study included only term neonates without severe haemolysis and did not assess long-term outcomes, so further multicentre trials with radiometric measurements and long-term follow-up are warranted. Early bilirubin measurements at 6–8 h were not performed in this study; therefore, early treatment response could not be assessed. Additionally, outcomes such as breastfeeding rates and duration of hospital stay were not systematically recorded and therefore could not be analyzed in this study. 21 The study population primarily consisted of neonates with exaggerated physiological jaundice and common neonatal risk factors such as polycythemia, sepsis, and perinatal stress, which may influence bilirubin kinetics but were similarly distributed between the groups. These findings suggest that aluminium foil reflector-assisted phototherapy may represent a simple and cost-effective strategy to enhance phototherapy efficiency in resource-limited neonatal care settings, although further studies with irradiance measurements are required to confirm the underlying mechanism.22,23
Conclusion
Aluminium foil reflector-assisted phototherapy was associated with faster bilirubin reduction and shortens treatment duration by 16.4% without compromising safety in term neonates with hyperbilirubinemia. This low-cost intervention represents a practical option for improving neonatal jaundice management, particularly in resource-limited healthcare settings where high-intensity phototherapy devices are not readily available.
Footnotes
Acknowledgements
The authors acknowledge the nursing staff of the Neonatal Intensive Care Unit (NICU), Vinayaka Mission’s Medical College and Hospital (VMMC), Karaikal, Puducherry, India for their cooperation and support during the conduct of this study. The authors also sincerely thank the parents and legal guardians of the participating neonates for their trust and consent.
Ethical considerations
This study was approved by the Institutional Ethics Committee of Vinayaka Mission’s Medical College and Hospital, Karaikal, Puducherry, India (Approval No: IEC/VMMCH//2024/DEC/04). The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments.
Consent to participate
Written informed consent was obtained from the parents or legally authorized guardians of all participating neonates prior to enrolment.
Consent for publication
Consent for publication was obtained as part of the informed consent process.
Author contributions
Giraboina Bhavitha contributed to study design, data collection, and initial drafting of the manuscript.
Ravikumar Senthilkumaran contributed to study conceptualization, supervision of the research, statistical analysis, and critical revision of the manuscript for important intellectual content.
Pagadpally Srinivas contributed to data analysis and critical review of the manuscript.
Kokila Manickam contributed to manuscript writing, revision, editing, and submission of the manuscript.
Vanidha Kandasamy contributed to statistical support.
All authors have reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.