
Abstract
Background
Congenital diaphragmatic hernia is an important cause of neonatal morbidity and mortality, primarily because of pulmonary hypoplasia and pulmonary hypertension. Early postnatal risk stratification may improve prognostication and guide escalation of care. We aimed to identify early postnatal predictors of mortality and to derive a simple bedside mortality risk score for neonates with isolated congenital diaphragmatic hernia.
Methods
We conducted a retrospective cohort study of newborns with isolated congenital diaphragmatic hernia admitted to a tertiary-care NICU within 6 h of life between 2004 and 2025. Clinical and physiologic variables, including Day-1 oxygenation, inotrope requirement and preoperative pneumothorax, were extracted from the medical records. Receiver operating characteristic analysis and Firth penalized logistic regression were performed. A bedside score, the Neonatal Congenital Diaphragmatic Hernia Mortality Risk Score (NCMRS-6), was derived from early predictors and internally evaluated using bootstrap resampling.
Results
66 newborns were included, of whom 52 (78.8%) survived to discharge. Non-survivors had a significantly higher Day-1 oxygenation index than survivors (median 64.0 vs 6.3; p < 0.001) and more frequent inotropic requirement (100% vs 40.4%; p < 0.001). Preoperative pneumothorax was also more common among non-survivors (46.2% vs 7.7%; p = 0.003). Day-1 oxygenation index alone showed excellent discrimination for mortality (area under the curve 0.945). The NCMRS-6, combining Day-1 oxygenation index tiers, inotrope requirement, and preoperative pneumothorax, demonstrated an area under the curve of 0.964 (95% confidence interval 0.894-1.000). A threshold of at least four points yielded 92.3% sensitivity and 90.4% specificity.
Conclusions
Day-1 oxygenation index, inotrope requirement and preoperative pneumothorax are important early predictors of mortality in isolated congenital diaphragmatic hernia. The NCMRS-6 is a simple bedside risk-stratification tool with promising discriminatory ability, but external validation is required before broader clinical application.
Introduction
Congenital diaphragmatic hernia (CDH) is a high-risk surgical anomaly associated with significant neonatal morbidity and mortality.
1
This leads to pulmonary hypoplasia, which in turn leads to pulmonary hypertension of the newborn (PPHN), which are the primary determinants of postnatal morbidity and mortality in these neonates. The left sided CDH also called
In recent decades, there have been significant advancements in neonatal care, of which management of pulmonary hypertension, using gentle ventilation strategies and practices of early surgery post stabilization have led to improved outcomes of CDH neonates. Reported survival rates in developed nations is variable and depends on center load, ECMO availability and other associated anomalies. Contemporary registry and review data suggest survival commonly ranges around 70-80% in many high-income settings, although individual cohorts report wider variation. 2 However, this improvement is not uniform globally, with outcomes differing in developing countries. 3 Furthermore, due to wide variation in care practices across institutions persists, recognized as a significant contributor to outcome disparities. 4 This variability underscores the ongoing challenge in providing optimal care, despite standardized guidelines from consortiums like “CDH EURO.” 5 CDH care relies mainly on seamless collaboration among various multidisciplinary teams including neonatology, surgery and fetal medicine. 6
Given the complex pathophysiology and persistent high morbidity and mortality associated with CDH, there is a continuous need for clinicians to identify effective and easily applicable predictors of outcome. 7 Prenatal assessments, such as Lung-to-head-ratio (LHR) and observed-to-expected total fetal lung volume (O/E TFLV) are crucial for initial prognosis and parental counseling and are routinely used in many specialized fetal medicine centers. However, these measures primarily reflect antenatal anatomic severity and may not fully capture dynamic postnatal cardiopulmonary adaptation, response to ventilation, pulmonary hypertension severity, or early hemodynamic instability after birth. 8
The oxygenation index (OI) is a valuable bedside tool which can be used as a postnatal predictor of mortality in CDH especially when compared to more complicated composite scores. 9 It serves as crucial factor for cardiorespiratory function, widely utilized to assess the severity of respiratory failure 10 and guide decisions regarding interventions such as inhaled nitric oxide (iNO) and extracorporeal membrane oxygenation (ECMO). 11
Hence existing markers often fall short in determination of postnatal outcome in real time clinical settings. Therefore, these lacunae highlight the need for more comprehensive predictions that integrate early postnatal factors to enhance outcome forecasting and optimizing care in CDH neonates. 12 We aimed to develop a postnatal scoring system to predict the mortality and thus be helpful in early escalation of care and prognostication of the condition.
Materials and methods
Study design and setting
This retrospective cohort study was conducted in the level 3 NICU of Sri Ramachandra Medical College (SRMC), Chennai, India, a tertiary-care teaching hospital.
Participants
All neonates diagnosed with isolated congenital diaphragmatic hernia (CDH) within the first 6 hours of life between June 2004 and May 2025 were included. For this study, “isolated CDH” was defined as CDH occurring without a chromosomal or syndromic diagnosis, without major extracardiac congenital malformations, and without hemodynamically significant structural congenital heart disease. Major cardiac anomalies, including cyanotic congenital heart disease, complex structural heart disease, large hemodynamically significant septal defects, or lesions expected to independently affect oxygenation or survival, were excluded. Minor or transitional echocardiographic findings such as patent foramen ovale, patent ductus arteriosus, or small hemodynamically insignificant atrial/ventricular septal defects were not considered exclusion criteria but were reviewed in the context of pulmonary hypertension assessment. Neonates discharged against medical advice prior to survival assessment and cases with incomplete medical records were excluded.
Clinical management
The institutional protocol for CDH management involved elective intubation at birth and initiation of gentle ventilation with conventional mechanical ventilation as the initial mode. Escalation to high frequency oscillator ventilation (HFOV) was considered if mean pressure exceeded 12 cm H2O or inability to maintain target oxygen saturation. Inhaled nitric oxide (iNO) was initiated when oxygenation index (OI) was greater than 20. All the neonates with CDH underwent radial arterial access at the admission to the unit as part of unit policy at par with international guidelines. Surgical repair was deferred until hemodynamic stabilization defined by achieving FiO2 to less than 40% on conventional ventilation preductal saturation above 85% with no requirement of inotrope, serum lactate below 3 mmol/L, and urine output exceeding 1 ml/kg/hr or no further improvement over next 48 h after counseling and shared decision making with parents. Routine screening echocardiography was performed within the first 24 h to assess severity of pulmonary hypertension, ventricular function, ductal/atrial shunt direction where available, and to identify hemodynamically significant structural cardiac anomalies. Severe pulmonary hypertension was defined as echocardiographic evidence of suprasystemic pulmonary arterial pressure, based on estimated right ventricular systolic pressure when measurable, right-to-left or bidirectional ductal/atrial shunting, interventricular septal flattening or leftward bowing, and/or right ventricular dilatation or dysfunction. When individual quantitative parameters were not uniformly available in older records, the severity category recorded in the formal echocardiography report was used.
Inotrope/vasoactive support was initiated for clinical hemodynamic compromise, including systemic hypotension, poor perfusion, rising lactate/metabolic acidosis, reduced urine output, and/or echocardiographic evidence of ventricular dysfunction or pulmonary hypertension-related circulatory compromise, as determined by the treating clinical team. ECMO was not routinely available on-site as rescue therapy for CDH during most of the study period, and no neonate in the analyzed cohort underwent ECMO.
Data collection
Data were retrospectively extracted from medical record department using the ICD-10 diagnostic code Q79.0 (congenital diaphragmatic hernia). The medical records were retrieved in full (case records, daily notes, arterial blood gases, and echocardiography report). Data collected included demographic details, antenatal ultrasound findings, birth weight, gestational age, liver position, deliv mode and APGAR score. Ventilatory parameters, including mean airway pressure (MAP), fractional inspired oxygen (FiO2) and arterial pressure of oxygen (PaO2), were documented from radial arterial blood gas samples to calculate OI. Day-1 OI was defined as the maximum/worst within the first 24 h of life or admission, not the first value or an average. Maximum OI values on day 1, 2 and 3 of life were recorded for further analysis. Additional clinical data such as iNO usage, inotropic support, occurrence of sepsis or pneumothorax and duration of respiratory support were also documented.
Score derivation
The Neonatal CDH Mortality Risk Score-6 (NCMRS-6) was derived from the study cohort using a data-based, additive point-based system. The variables which significantly were associated with mortality in univariate analysis were selected. The points were assigned based on the strength of association (Odds ratios) and biological plausibility. OI was tiered into ordinal levels to capture its dose-response relationship.
Statistical analysis
Data analysis was done using SPSS software. Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR), based on data distribution. Categorical variables were presented as frequencies and percentages. Comparisons between survivors and non-survivors were done using the Mann-Whitney U test for continuous variables and Chi-square or Fisher’s exact test for categorical variables.
Primary prognostic analysis
The primary outcome was in-hospital mortality. The discriminatory ability of the highest Day-1 OI (defined within the first 24 h from birth/admission) to distinguish between those who survived and those who died was determined through ROC curves with AUC and 95% confidence intervals (DeLong method). We also analyzed performance at pre-specified clinically relevant OI thresholds ([e.g., 15, 20, 40]) reporting sensitivity, specificity, Positive predictive value and negative predictive value in addition to the data-derived Youden cutoff (exploratory) analysis.
Regression modeling
The relationship between Day-1 OI and mortality was calculated using penalized logistic regression (Firth correction) to reduce the bias of small-sample size and separation, with odds ratios and 95% CIs reported. Performance was evaluated at clinically relevant OI thresholds and at the data-derived Youden cutoff.
Because CDH is uncommon and the number of deaths was limited, the study was not designed or powered for extensive multivariate modeling. To avoid overfitting, multivariable adjustment was restricted a priori to a limited penalized regression model including only clinically important covariates.
Candidate confounders considered included CDH laterality, liver position, antenatal diagnosis, pulmonary hypertension severity, ventricular dysfunction, iNO use, inotrope requirement, pneumothorax, timing of surgery and era of care. These variables were not entered simultaneously because of limited events per variable, missingness, collinearity with OI/PH physiology, treatment dependence or downstream/post-treatment status. As exploratory sensitivity analyses, ridge-penalized logistic regression models were fitted by adding one candidate covariate at a time to the base model of birth weight and Day-1 OI. These models were interpreted descriptively (supplemental table 3).
Calendar-era adjustment was considered but was not incorporated into the multivariable model because of the limited number of mortality events and the risk of overfitting. Potential confounding by era of care was therefore addressed in the interpretation and limitations.
Missing data
The frequency and pattern of missingness for each variable was assessed. The main analyses were done on a complete-case basis; the number of neonates included in each analysis is stated. To prevent any selection bias, the characteristics of included versus excluded neonates were compared (supplemental table 1).
Results
During the study period neonates with congenital diaphragmatic (CDH) were admitted to the neonatal intensive care unit within 6 hours of birth. After excluding six neonates with major congenital anomalies, chromosomal disorders and incomplete data, 66 neonates with isolated CDH were included in final analysis. Of these, 52 neonates survived (survival 78.8%) to hospital discharge while 14 died (Figure 1). For variables with incomplete documentation, available-case denominators are reported as n/N (%); therefore, denominators vary across variables, particularly among non-survivors who died early. Study cohort flow diagram.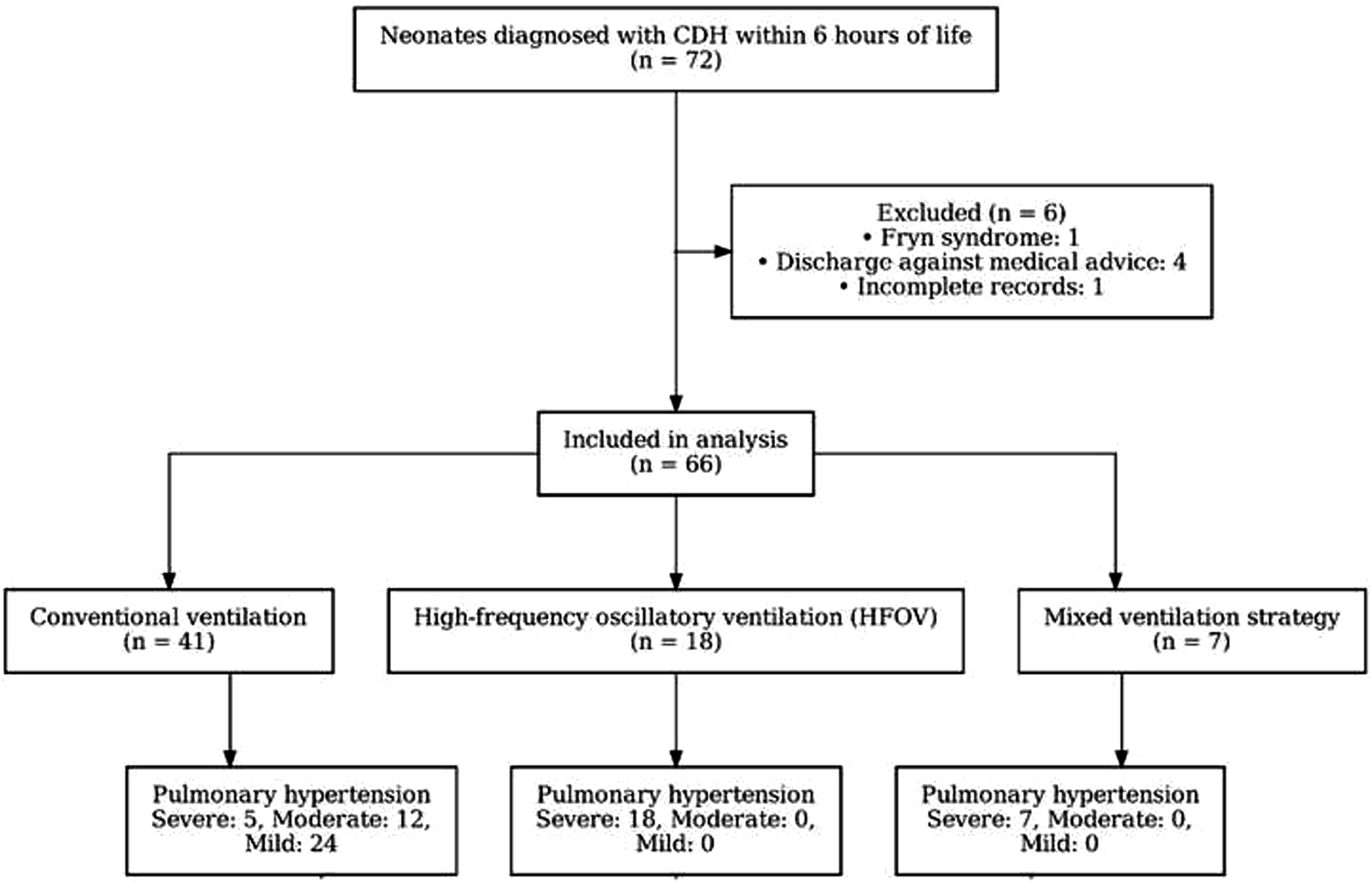
Baseline characteristics, early clinical predictors of in-hospital mortality in neonates with congenital diaphragmatic hernia.
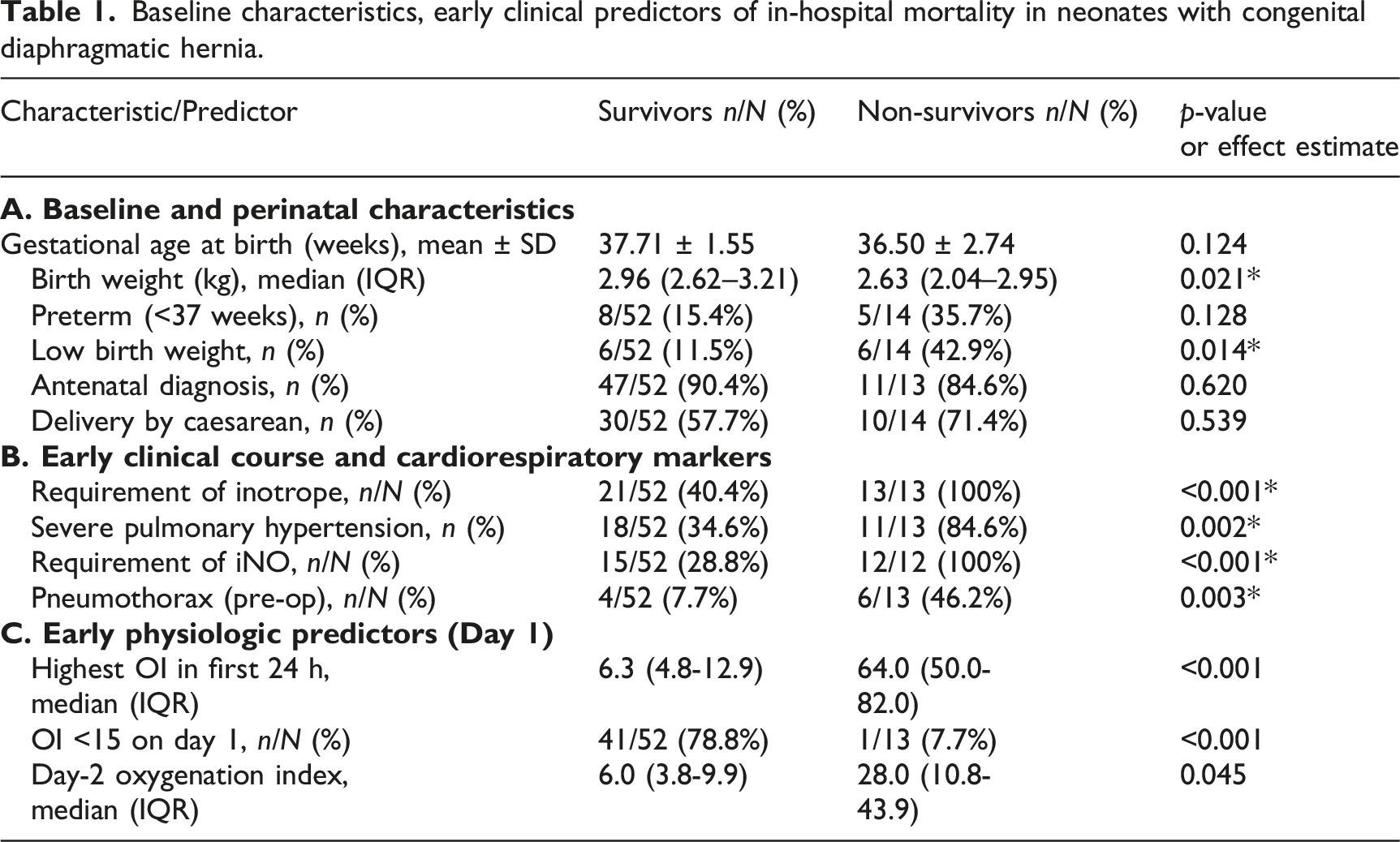
Among the postnatal predictors, early markers of disease severity differed substantially between the two groups. Inotrope requirement was needed in 21/52 survivors, whereas 13/13 evaluable non-survivors required inotropic support (p < 0.001). Preoperative pneumothorax was also more frequently seen among non-survivors than survivors (6/13 [46.2%] vs 4/52 [7.7%]). Inhaled nitric oxide was documented to be required in 15/52 survivors and 12/12 evaluable non-survivors (28.8% vs 100%, p < 0.001).
The maximum OI in the first 24 h was higher in non-survivors (median 64.0, 50.0–82.0) compared to survivors (median 6.3 [4.8–12.9]) showing a tenfold difference (p < 0.001). A day −1 OI <15 was present in 41/52 survivors but only 1/13 non-survivors (78.8% vs 7.7%, p < 0.001). Day-2 OI also remained significantly higher among non-survivors than survivors (28.0 [IQR 10.8–43.9] vs 6.0 [IQR 3.8-9.9], p = 0.045), but later OI values were interpreted descriptively because of informative missingness among early deaths. A clinically useful threshold of 17.4 identified mortality with 92.3% sensitivity and 84.6% specificity, with a positive predictive value of 60% and a negative predictive value of 97.8% for Day-1 OI.
Firth penalized logistic regression analysis for mortality.
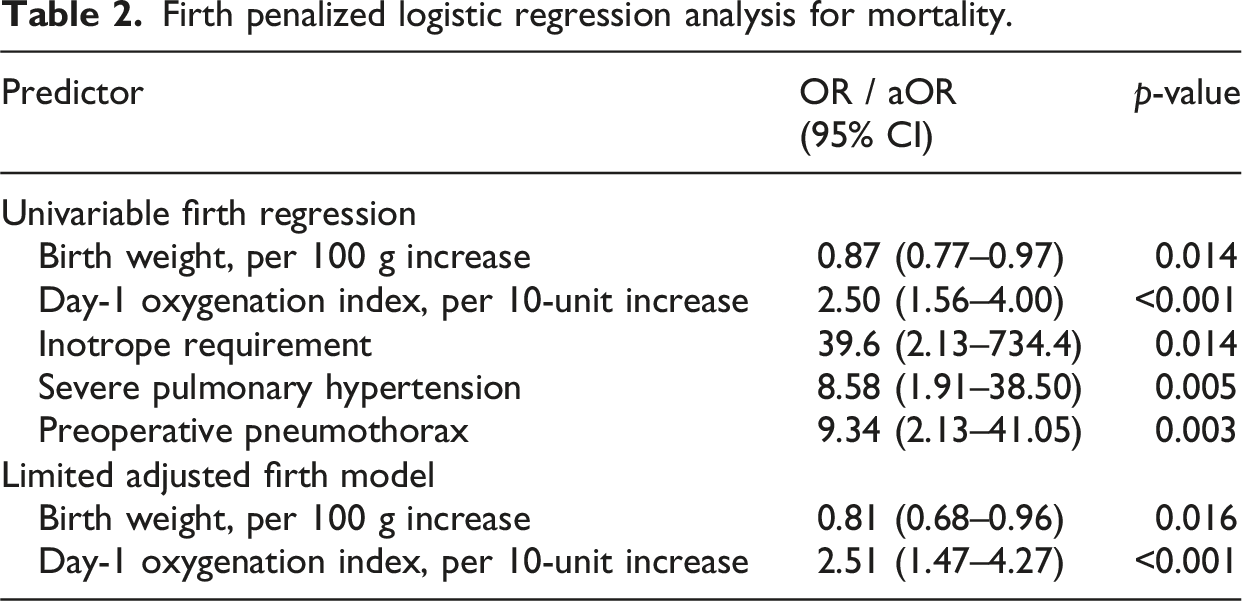
Additional candidate confounders were considered but were not entered simultaneously because of the limited events-per-variable ratio, missingness, collinearity with OI, or downstream/post-treatment status. As a sensitivity analysis, ridge-penalized logistic regression models were fitted by adding one candidate covariate at a time to base model of birth weight and Day-1 OI. These models were interpreted descriptively (supplemental table 3).
Development of a novel bedside mortality risk score (NCMRS-6)
NCMRS-6 Score and Risk stratification.
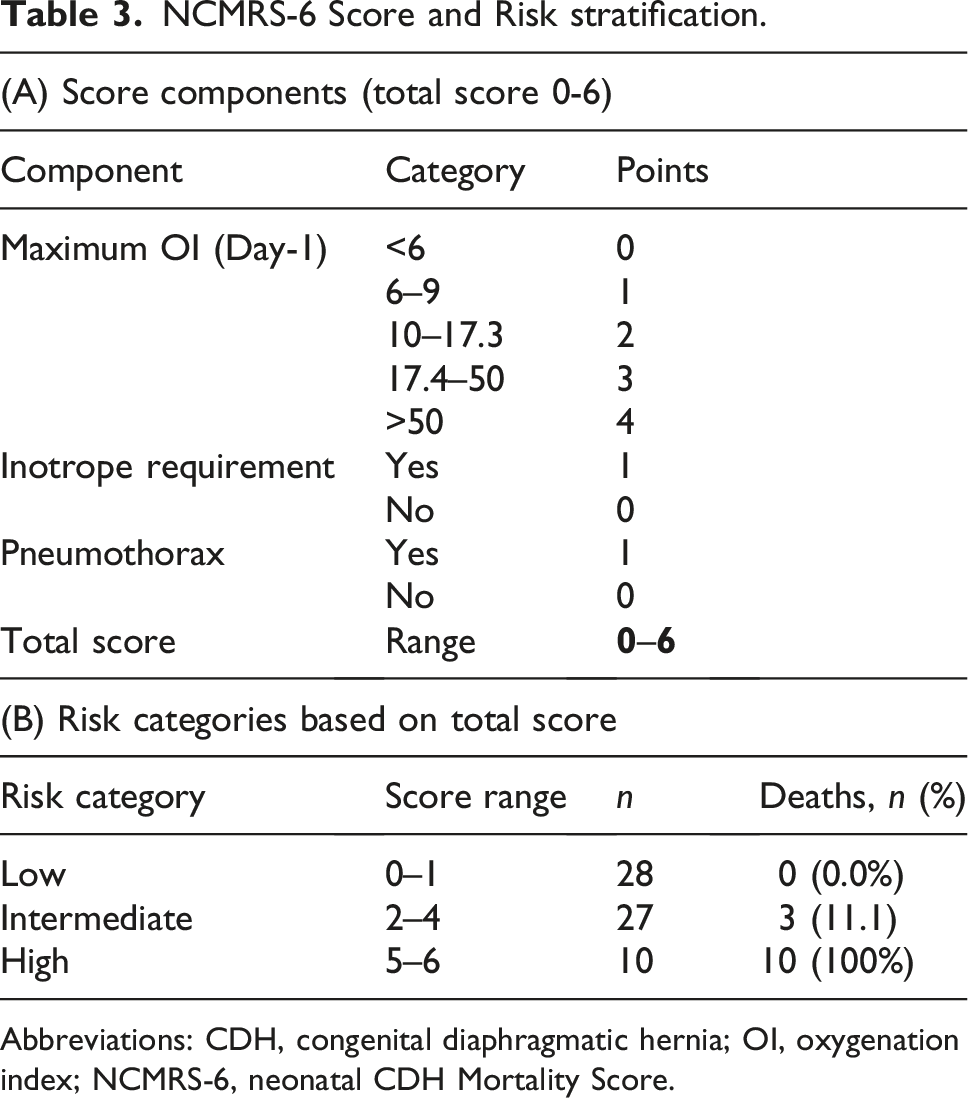
Abbreviations: CDH, congenital diaphragmatic hernia; OI, oxygenation index; NCMRS-6, neonatal CDH Mortality Score.
The final NCMRS-6 was intentionally developed as a simple additive integer score rather than a coefficient-weighted probability calculator, given the limited number of deaths in the cohort. OI was categorized into ordinal tiers to reflect a dose-response relationship with mortality: <6, 6-10, 10–17, 17-50, and >50 contributing 0–4 points, respectively. The threshold of OI 17.4 was derived from the cohort’s ROC Youden analysis and identified mortality with 92.3% sensitivity and 84.6% specificity. The lower threshold of OI <15 was retained as a clinically meaningful low-risk cutoff because it demonstrated a high negative predictive value in this cohort and has been used in prior CDH prognostic literature. Values of 50 were categorized separately because this group showed 100% mortality in the study cohort. Inotrope requirement within the first 24 h and preoperative pneumothorax were each assigned 1 point, yielding a total score ranging from 0 to 6. To support the proposed score structure, a multivariable ridge-penalized logistic regression model was fitted using the three score components: Day-1 OI tier points, inotrope requirement and preoperative pneumothorax. The coefficients were positive for all three components, supporting their inclusion in the score.
Other variables were evaluated but not included in the final score for the clinical and statistical reasons. Birth weight was retained in regression adjustment but was excluded in NCMRS-6 because the score was designed to capture dynamic postnatal cardiorespiratory instability rather than baseline demographic risk. Severe pulmonary hypertension and iNO use were not included because of conceptual overlap and being collinearity with OI. Liver position was not included because of missingness and retrospective documentation variability.
Performance of the NCMRS-6
A total of 65 newborns with complete data for every score component had their score performance assessed (deaths = 13). The NCMRS-6 showed a superior result as compared to Day-1 OI alone in the same subset (AUC 0.964; 95% CI 0.894–1.000) and demonstrated a better discrimination for mortality). A threshold of
Internal validation
Internal Validation Metrics for NCMRS-6 using bootstrap resampling (5,000 resamples).
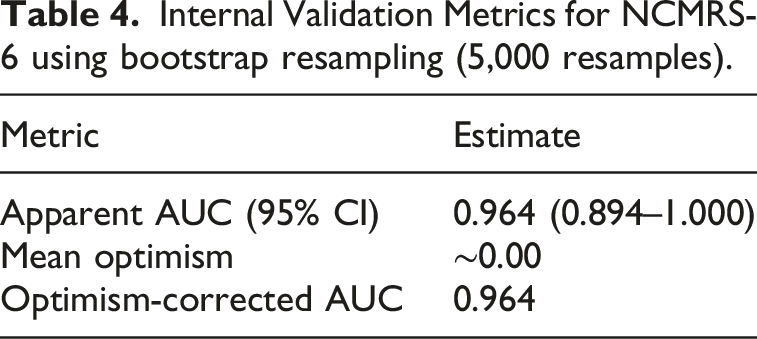
The score showed excellent apparent discrimination for in-hospital mortality, with an AUC of 0.964 and bootstrap derived 95% confidence interval of 0.894-1.000 (Figure 2). This suggests good internal stability of the model within the derivation cohort. Comparison of Receiver Operating Characteristic (ROC) curves for Day-1 Oxygenation Index (OI) and the novel NCMRS-6 Score for in-hospital mortality prediction in neonates with isolated CD.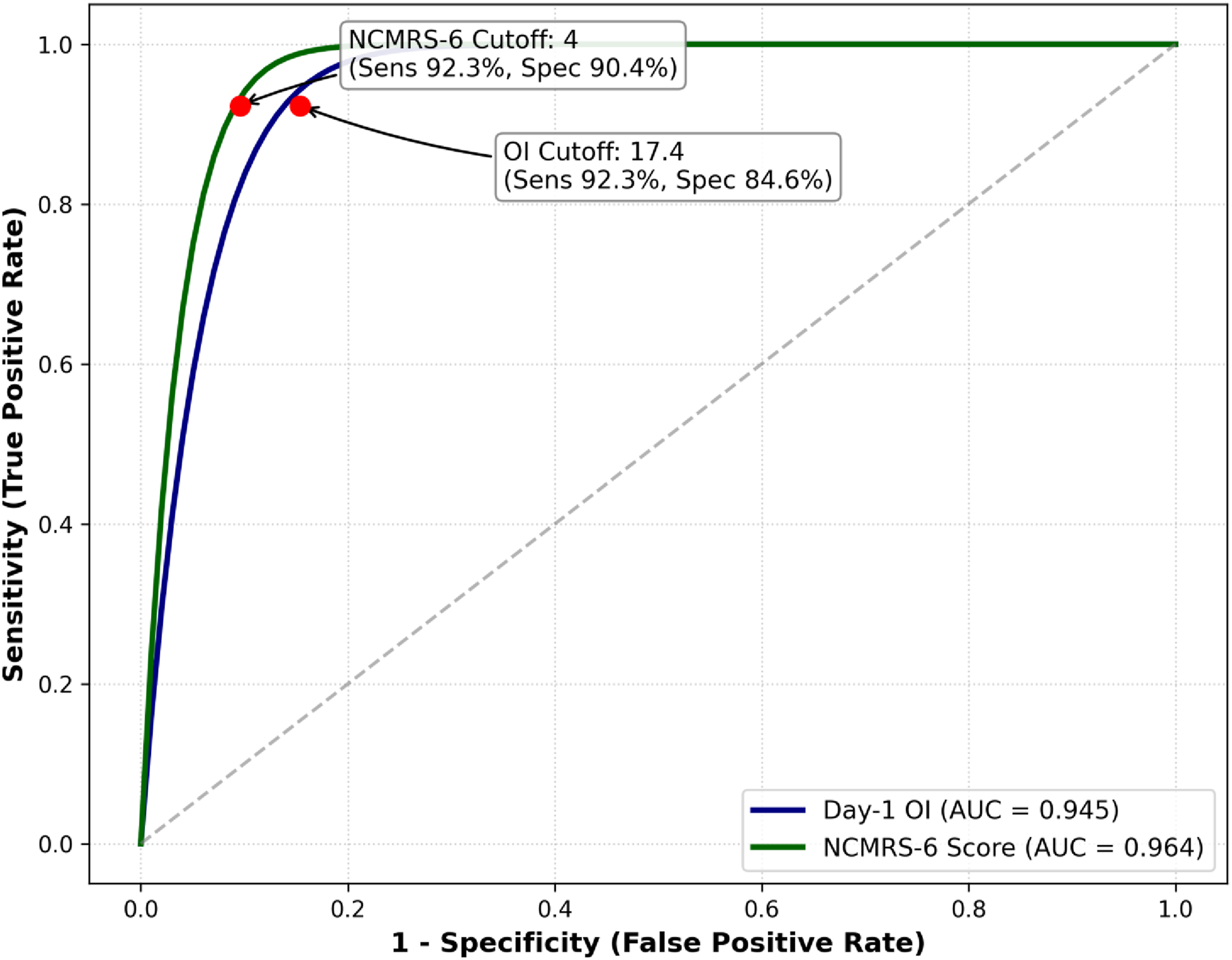
Missing data (Supplemental table 1): In this study, day 1 OI was available for 65/66 (98.5%) neonates (missing 1/66, 1.5%, all in non-survivors). Day 2 and day 3 OI were available for 51/66 (77.3%) and 48/66 (72.7%). The missingness for day 2 and day 3 OI were more frequent with non-survivors consistent with early clinical deterioration/death. No imputation was performed, and all analyses were conducted using available-case denominators. The NCMRS-6 was calculable in 65/66 neonates (98.5%).
Discussion
Our results from a 21-year single-center cohort demonstrate that in neonates with congenital diaphragmatic hernia (CDH), there are several early physiological indicators that are highly predictive of mortality. Specifically, the OI during the first 24 h of life is a reliable predictor of outcome. 10 Those who survived had a significantly lower maximum OI (median 6.3, IQR 4.8–12.9) than non-survivors (median 64.0, IQR 50.0–82.0; p < 0.001) in our cohort’s Day-1 OI. The use of Day-1 OI as a useful bedside tool was supported by prediction for mortality on ROC analysis (AUC 0.945, 95% CI 0.877–1.000; p < 0.001). An objective threshold for early counseling and escalation of care was provided by the ideal Day-1 cutoff determined by Youden’s score (17.4), which showed a sensitivity (92.3%) and specificity (84.6%) in predicting mortality. (1) Also, a Day-1 OI <15 had a very high negative predictive value (97.7%), our study’s role of early OI as a prognostic marker is consistent with findings in various other studies. 13 In a single-center cohort, Chandrasekaran et al. found that a maximum Day-1 OI <15 was a good postnatal predictor of survival, with excellent sensitivity and specificity. 14 Moreover Ruttenstock et al. reported that the best OI on day 1 had an AUC of 0.90 for predicting 28-day survival. 10 Our data also showed that the OI <15 thresholds had a very high NPV, which when incorporated in routine practice serves as a good bedside tool. Although OI continued to be useful after the first day, survivor bias in observational datasets must be taken into account when interpreting later OI trends. In this regard, our findings support the idea that the most reliable prognostic signal is carried by Day-1 physiology and that successive OI values should be interpreted as a dynamic indicator of changing cardiopulmonary status rather than as a predictor of outcome. Feng et al. also found a significantly higher OI in non-survivors as compared to survivors. 15 In practice OI has been used and has also been advocated for escalation of support including as an indication for ECMO. This finding raises the consideration that earlier initiation of therapies such as ECMO could be explored to improve outcomes.16,17
In our study, neonates with severe pulmonary hypertension (PH) and increased cardiopulmonary support in the form of inotropes showed an increased mortality risk. While survivors showed a heterogeneous distribution of mild, moderate, and severe PH, all non-survivors with accessible echocardiographic PH data had severe PH, underscoring the significance of pulmonary vascular disease in predicting early stability. Severe pulmonary hypertension was followed with treatment with iNO which was utilized in all non-survivors (12/12, 100%) but in only 28.8% of survivors (15/52) (p < 0.001), indicating the strong correlation between PH-directed rescue tactics and refractory oxygenation failure.
Although the clinical response to inhaled nitric oxide is variable and depends on underlying vasoreactivity, it is still a widely used modality for the management of pulmonary hypertension in CDH. 18 The results of the study highlight the continued importance of oxygenation index, iNO, ventilatory strategies 19 and other associated complications in predicting mortality in congenital diaphragmatic hernia.
Additionally, we also noted a significant association between mortality and pneumothorax, with 46.2% of non-survivors (6/13) and 7.7% of survivors (4/52) having pneumothorax (p = 0.003). In CDH, pneumothorax which is mostly commonly associated with aggressive ventilation strategies causes a compounding event that can suddenly exacerbate oxygenation and disturb the hemodynamics in an already fragile pulmonary vascular state. 20
Hence, when OI is combined with the need for inotrope and preoperative pneumothorax, the proposed NCMRS-6 demonstrated a strong discrimination (AUC-0.964) in the derivation cohort. More importantly, the high-risk threshold (NCMRS-6
The current concept that CDH is essentially a medical emergency rather than a surgical one and that repair should come after cardiopulmonary stabilization is supported by our surgical results. (8) Our neonates underwent surgery at a mean of 4.77 ± 1.91 days (median 4, IQR 4–6), Out of 52/53 survived, while 13/14 died before surgery, indicating failure to stabilize rather than postoperative collapse. The unit has not reported any postoperative death of CDH since 2017. This indicates advancement of neonatal intensive care over the years. This is consistent with guidelines that encourage early surgery post stabilization. In practical, OI improvement together with improved perfusion and decreasing inotrope requirements can function as an objective measure for timing of surgery.
These findings suggest that a simple composite score may provide a pragmatic tool for early risk stratification, particularly in a resource-limited setting. The most widely used rule, that is, the CDH Study Group (CDHSG) prediction rule, which uses birth weight, APGAR score and presence of anomalies to stratify risk. This model, validated on over 2000 patients, provides three risk categories with associated mortality probabilities and is used for early prognostication and inter-institutional comparison. 22 The SNAP-11 (Score for Neonatal Acute Physiology-II), which was derived from the wider NICU cohort, had also demonstrated predictive value in CDH by capturing physiological derangements in the initial 12 h of life. 23
More recent tools advocate echocardiographic features, severity of pulmonary hypertension or ductal flow patterns. 24
Compared to these, our proposed NCMRS-6 score uses a three variable structure which includes day 1-OI, requirement of inotropes and presence of preoperative pneumothorax. This score improves clinical usability in a resource-limited setting while preserving high predictive power (AUC-0.964). Unlike other scoring systems which are more focused on birth weights or antenatal factors, NCMRS-6 focuses on dynamic cardiorespiratory instability, which may better reflect the prognosis in real time.5,8,25
However, it should be noted that in ECMO-capable centers, neonates with high OI may undergo ECMO rescue where the mortality rate may vary as compared in a resource-constrained setting with no ECMO accessibility. But large ELSO registry studies show that CDH neonates requiring ECMO remain a very high-risk group, with reported mortality of 50.6%, and outcomes appear to vary according to center volume and experience. 26 Therefore, the observed association between Day-1 OI and mortality in our cohort may reflect both underlying disease severity and center-level treatment context. Although ECMO services are available in selected centers in India, published neonatal ECMO data is very limited and is most often associated with high mortality.
Strengths and limitations
The strengths of this study include its two-decade duration, protocol-based management, and convergence of trajectory, continuous (OI) analyses and concordant signal across multiple analytic approaches. The use of OI and categorical risk frameworks (NCMRS-6) shows evidence across multiple analytic approaches, strengthening the reliability of observed association. Moreover, the inclusion of other practical bedside variables, that is, inotropic requirement and preoperative pneumothorax-enhances the clinical applicability of the findings, especially in a resource-limited environment. The model’s stability was further supported by internal validation using 5000 bootstrap resamples.
The principal limitations are the retrospective single-center design, small number of deaths, limited ability to adjust for confounders and lack of external validation. Although Firth penalized regression and bootstrap resampling were used to reduce small-sample bias and estimate optimism in apparent performance, these methods do not eliminate overfitting or establish external validity. The 21-year study period may introduce confounding by calendar time, as ventilation practices, pulmonary hypertension management, echocardiography, surgical timing and rescue options may have evolved. Formal era-stratified AUC analysis was not reliable because of the small number of deaths. The lack of ECMO for a large portion of the era are limitations that could increase the correlation between high OI and mortality in comparison to settings with ECMO capabilities. The NCMRS-6 should be considered as an exploratory bedside risk-stratification framework requiring external validation.
Implications
These findings have important implications in early clinical management and prognostication of infants with CDH. The demonstration that OI on day 1 when combined with requirement of inotrope and pneumothorax can robustly stratify mortality risk, provides a practical tool for clinicians. The proposed NCMRS-6 score is easy to apply and enhances early identification of high-risk neonates who may benefit from timely referral and also in informing individualized care decision. This score could also serve as a standardized severity adjustment metric in CDH research and inter-institutional benchmarking.
Conclusion
In this single-center study which collected data of CDH neonates over 21 years it was seen that maximum OI within the first 24 h emerged as a strong early predictor of in-hospital mortality, with good discrimination on ROC analysis. A day 1 OI cutoff of 17.4 proved high diagnostic accuracy with a sensitivity of 92.3 and specificity of 84.6%, making OI an easy bedside tool for early risk stratification. Moreover when it is clustered with markers of severe early compromise—particularly preoperative requirement and inotrope requirement the prediction of outcome was better.
Hence with the following findings, the
Supplemental material
Supplemental Material - Postnatal predictors of mortality and derivation of a novel risk score in congenital diaphragmatic hernia: A 21-year-single-center cohort study
Supplemental material for Postnatal predictors of mortality and derivation of a novel risk score in congenital diaphragmatic hernia: A 21-year-single-center cohort study by Jaikrith Patil, Prakash Amboiram, Umamaheswari Balakrishnan, Madhu Ramasundram, Ashok Chandrasekaran in Journal of Social and Personal Relationships
Footnotes
Acknowledgments
The authors acknowledge the support of the Neonatal Intensive Care Unit staff, the Department of Pediatric Surgery, and the Medical Records Department of Sri Ramachandra Medical College and Research Institute, Chennai, for their assistance in clinical care and retrieval of case records. The authors also thank their departmental colleagues for academic support during the conduct of this study. The authors are deeply grateful to the neonates and their families, whose clinical journeys form the basis of this work.
Ethical considerations
The study was approved by the Institutional Ethics Committee and informed consent was waived by it because of the retrospective nature of the study. - Ethics approval number:
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.