
Abstract
Background
Traditional diagnostic criteria for hypoxic-ischemic encephalopathy (HIE) rely heavily on documented fetal acidemia, which may be missing or unavailable in resource-limited settings. This study evaluated the diagnostic utility of multi-organ biomarkers in identifying neonates with HIE who do not meet classic acidemic criteria (“non-classic HIE”).
Methods
This clinical population study analyzed 416 full-term and late-preterm neonates over 3 years at a tertiary neonatal intensive care unit (NICU). Participants were categorized into “classic HIE” (acidemia present) and “non-classic HIE” (no acidemia but presenting with clinical encephalopathy). Cardiac (Troponin-I), renal (urea/creatinine), hepatic (ALT/AST), and hematological (neutrophil-to-lymphocyte ratio [NLR]) biomarkers were evaluated to predict HIE severity and short-term outcomes.
Results
Of the cohort, 54.8% (n = 228) were classified into the non-classic HIE group. Within this group, 49.1% presented with mild, 43.4% with moderate, and 7.5% with severe clinical features, confirming systemic hypoxia despite “normal or near-normal” initial blood gases. Significant elevations in cardiac Troponin-I and AST were observed in the mild-to-severe classic HIE groups compared to the non-classic cohort (p < 0.001). Troponin-I showed high performance (AUC = 0.711) in predicting moderate-to-severe HIE across both cohorts. The NLR was significantly higher in all infants with clinical evidence of moderate-to-severe hypoxic insult.
Conclusions
Multi-organ biomarkers, particularly Troponin-I and NLR, offer valuable adjunctive metrics reflecting the severity of systemic hypoxic insults. They assist in identifying asphyxiated neonates when early blood gases are inconsistently captured or fail to show fetal acidemia.
Impacts statements
1. This study provides a comprehensive three-year analysis of the diagnostic utility of multi-organ biomarkers in a large cohort, offering a practical framework for identifying asphyxiated neonates in resource-limited settings where advanced neuro-monitoring is not constantly available. 2. The current investigation analyzes various degrees of HIE using existing clinical and laboratory indicators. This might assist clinicians in early identification and assessment of the severity of asphyxiated infants. 3. The research identifies the “Non-classic HIE” group as a substantial category of asphyxiated neonates who fail traditional biochemical criteria but still exhibit neurological and laboratory manifestations of hypoxia. Despite lacking classic acidemia, these infants experience significant hypoxic insults resulting in measurable multi-organ involvement. Most of these patients are clinically and physiologically comparable to the mild HIE group. 4. The duration of ventilation is the most important predictor of mortality in asphyxiated neonates.
Introduction
Hypoxic ischemic encephalopathy (HIE) affects 2 million infants annually worldwide, with a global burden of 50.2 million disability-adjusted life years. 1 The clinical criteria used in diagnosis of HIE indicated for hypothermia based on early neuro-clinical criteria, early blood gases and aEEG are widely practiced worldwide. 2 These criteria might miss patients with mild-to-moderate brain damage and provides no alternatives in situations where time window of early blood gas and early clinical assessment were missed, as well as unavailability of aEEG. 3 MRI can be helpful in providing objective criteria for early diagnosis of HIE albeit, their use might be hampered by expenses, unavailability, transportation constrains. 3 Cerebral oxygenation metrics and Doppler ultrasound of cerebral vessels might also be helpful in early identification of asphyxiated neonates. However, their benefits are still under investigations and depend on availability of the devices.4–6
Biomarkers induced by hypoxia serve as early, valuable inexpensive complementary indicators of systemic end-organ involvement, hypoxic-ischemic injury to the heart, the liver, the kidneys, and hematological and the immune systems. Hypoxic injury of those organs might precede hypoxia induced brain injury. 7 While they do not replace definitive neurological staging or electrophysiological monitoring, tracking these multi-organ parameters provides an objective reflection of the total hypoxic burden suffered by the neonate. The severity of HIE can vary depending on the intensity, duration, and timing of the hypoxic event. 8 Assessing the severity is a key factor in predicting future outcomes for children with HIE. Biomarkers can help in identification of severity of hypoxic insult, more precisely, alongside with the neurological assessment.8,9 This can guide immediate management strategies and provide important prognostic information regarding potential neurological outcomes.
Subjective diagnosis of asphyxiated patients and sticking to the present diagnostic criteria for HIE might miss important large category. 10 For our knowledge, no study showed before the magnitude of problem of another subcategory, which is patients with evidence of hypoxia without fetal acidemia that are neither indicated for TH by the classic criteria or classified as “classic HIE” according to the diagnostic clinical criteria in the first 12 h of lives and then they experience hypoxia-related neurological manifestations, after exclusion of other causes of brain damage.
Therefore, the current study aims to determine the significance of multiple laboratory biomarkers in the early detection and assessment of severity of HIE. We hypothesized that distinct panels of systemic biochemical and hematological markers can accurately differentiate neonates with moderate-to-severe HIE from those with mild injury, and that these biomarkers can identify a critical subcategory of neonates with perinatal depression who experience neurological manifestations despite the absence of initial fetal acidemia. Furthermore, we sought to determine the prevalence of these subcategories within our intensive care unit admissions and evaluate the clinical factors influencing overall neonatal mortality.
Methods
This study utilized a retrospective cohort design. All records of asphyxiated patients admitted to NICU of Alexandria University Maternity Hospital (AUMH) and diagnosed as perinatal asphyxia in the time period from January 1st 2020 to the 31st of December 2022 were included in the study. The study was approved by the ethics committee of the Alexandria University with, ID number 0107549, IRB number 00012098, and FWA number 00018699.
Study population and enrollment
The study included asphyxiated late preterm and full-term neonates (gestational age ≥34 weeks). 11 Patients were classified into mild, moderate, or severe encephalopathy using the modified Sarnat staging, as well as a distinct “non-classic HIE” group.
Classification criteria
Classic HIE criteria
Neonates were classified under “classic HIE” if they met traditional biochemical thresholds for therapeutic hypothermia: • Evidence of fetal acidemia: Cord blood or blood gas within the first 60 min of life revealing a pH < 7.0 and/or a base deficit >−12. • Evidence of perinatal hypoxia: Evidence of deteriorating intrapartum monitoring (CTG, Doppler US), obstructed labor, meconium-stained amniotic fluid, or an Apgar score <5 at 5 min. Apneic, flaccid neonates requiring intermittent positive pressure ventilation (IPPV) for more than 10 min in resuscitation. • Biomarker Alterations: Evidence of multi-organ involvement, including elevated Cardiac Troponin-I, AST, ALT, or serum creatinine. • Neurological Manifestations: Symptoms such as altered muscle tone, absent reflexes, or convulsions, and/or Abnormal Thompson score.
Non-classic HIE criteria
This group included neonates who exhibited clinical evidence of hypoxic exposure despite the absence of traditional acidemia. Blood gas analysis within the first hour of life demonstrated neither a pH < 7.0 nor a base deficit >−12 mmol/L. However, these infants still demonstrated objective biomarker alterations and neurological manifestations.
All patients were classified into mild, moderate, and severe encephalopathy according to modified Sarnat staging, 12 as well as “Non-classic HIE.”
To maintain the integrity of the cohort, specific exclusion criteria were applied during the enrollment process. Infants were excluded if their neurological symptoms were attributed to alternative etiologies, such as primary neuromuscular diseases (using nerve conduction and EMG studies), congenital brain malformations (using cranial sonography), sepsis (negative blood/CSF cultures) or underlying metabolic disorders (Normal ammonia and screening for inborn errors of metabolism). Additionally, the study was restricted to late preterm and full-term neonates, meaning any infant born at a gestational age of less than 34 weeks was ineligible for participation.
Data collection and biomarker assays
Clinical data and laboratory results were retrieved from patient files. To ensure objectivity, laboratory staff performing biomarker assays were blinded to the clinical Sarnat stage of the infants.
Timing of investigations: • Blood Gases: Collected within the first hour of life. • Early Enzymes: LDH and CK-MB were tested once within the first 6 h of life (pre-therapeutic hypothermia). • Troponin-I: Recorded once between 6 and 24 h of life. • Serial Biomarkers: Complete Blood Count (CBC), liver function, and CRP were recorded twice: within the first 6 h (before TH) and between 48 and 72 h of life (during TH). Electrolytes, renal function, and coagulation profiles were recorded twice: at age of 24 h of life and between 48 and 72 h of life (during TH).
All data used in the current work were collected from patients’ files and printed laboratory results in patients’ files.
Statistical analysis
Data were entered into the computer and analyzed using IBM SPSS software version 27.0. The Kolmogorov-Smirnov test was applied to assess the normality of the distribution. Continuous variables following a normal distribution are presented as Mean ± SD and compared using one-way ANOVA, while non-normally distributed variables are presented as Median (IQR) and compared using the Kruskal-Wallis test. To control the family-wise error rate associated with multiple subgroup assessments, a Bonferroni correction was applied to all post-hoc pairwise calculations (p1 through p6). For these specific matrices, the threshold for statistical significance was strictly adjusted to p < 0.0083. The prevalence of patients exposed to hypoxia among admitted patients was calculated. Binary logistic regression analysis (univariate and multivariate analysis) was used to identify independent risk factors for mortality. For the multivariate logistic regression model, a “complete case analysis” approach was utilized; consequently, only the 142 neonates with a full dataset for all selected predictors, including Troponin-I and duration of mechanical ventilation, were included in the final model, while cases with any missing values for these variables or those who did not require mechanical ventilation were excluded from this specific analysis. Statistical significance was determined at the 5% level. Multicollinearity was assessed by evaluating correlation coefficients and VIF. While expected correlations were found between sequential APGAR scores and between Troponin and ventilation duration, all VIF values remained below the threshold of 5, confirming model stability. Receiver operating characteristics (ROCs) were generated to demonstrate sensitivity of different biomarkers in detection of Sarnat 2 and 3 in each group, “Non-classic HIE” and “classic HIE,” as well as in the whole studied patients.
Results
Among all total admissions (n = 4474 neonates) to NICU of AUMH, 416 full term and late preterm newborns were diagnosed as perinatal hypoxia including “classic HIE” and “Non-classic HIE.” The prevalence of asphyxiated patients was estimated to be 9.3% of all admitted patients to NICU of AUMH. One hundred and eighty-eight cases were diagnosed as “classic HIE,” in addition to, two hundred and twenty-eight patients had “Non-classic HIE,” after exclusion of other causes of neurological diseases. “Classic HIE” group is classified according to the scoring system into mild (n = 88), moderate (n = 72), and severe HIE (n = 28), in addition to “Non-classic HIE” group (n = 228), supplement-1. Among the 228 patients with “Non-classic HIE,” 49.1% presented with mild (Stage 1) symptoms, 43.4% were classified as moderate (Stage 2), and 7.5% exhibited severe (Stage 3) clinical features.
Comparison between the studied groups as regards socio-demographic data and maternal risk factors.
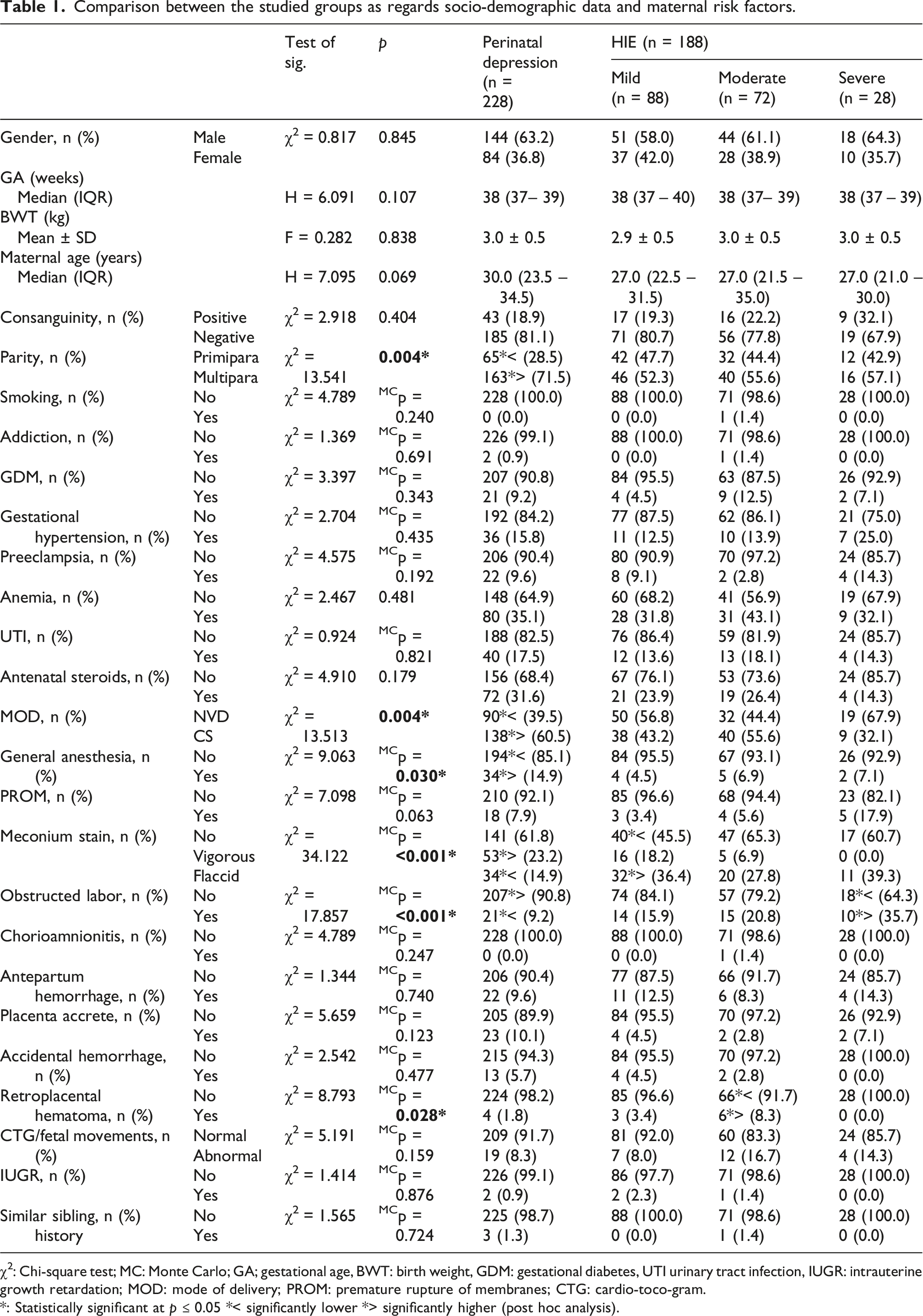
χ2: Chi-square test; MC: Monte Carlo; GA; gestational age, BWT: birth weight, GDM: gestational diabetes, UTI urinary tract infection, IUGR: intrauterine growth retardation; MOD: mode of delivery; PROM: premature rupture of membranes; CTG: cardio-toco-gram.
*: Statistically significant at p ≤ 0.05 *< significantly lower *> significantly higher (post hoc analysis).
Comparison between studied groups as regards perinatal data.
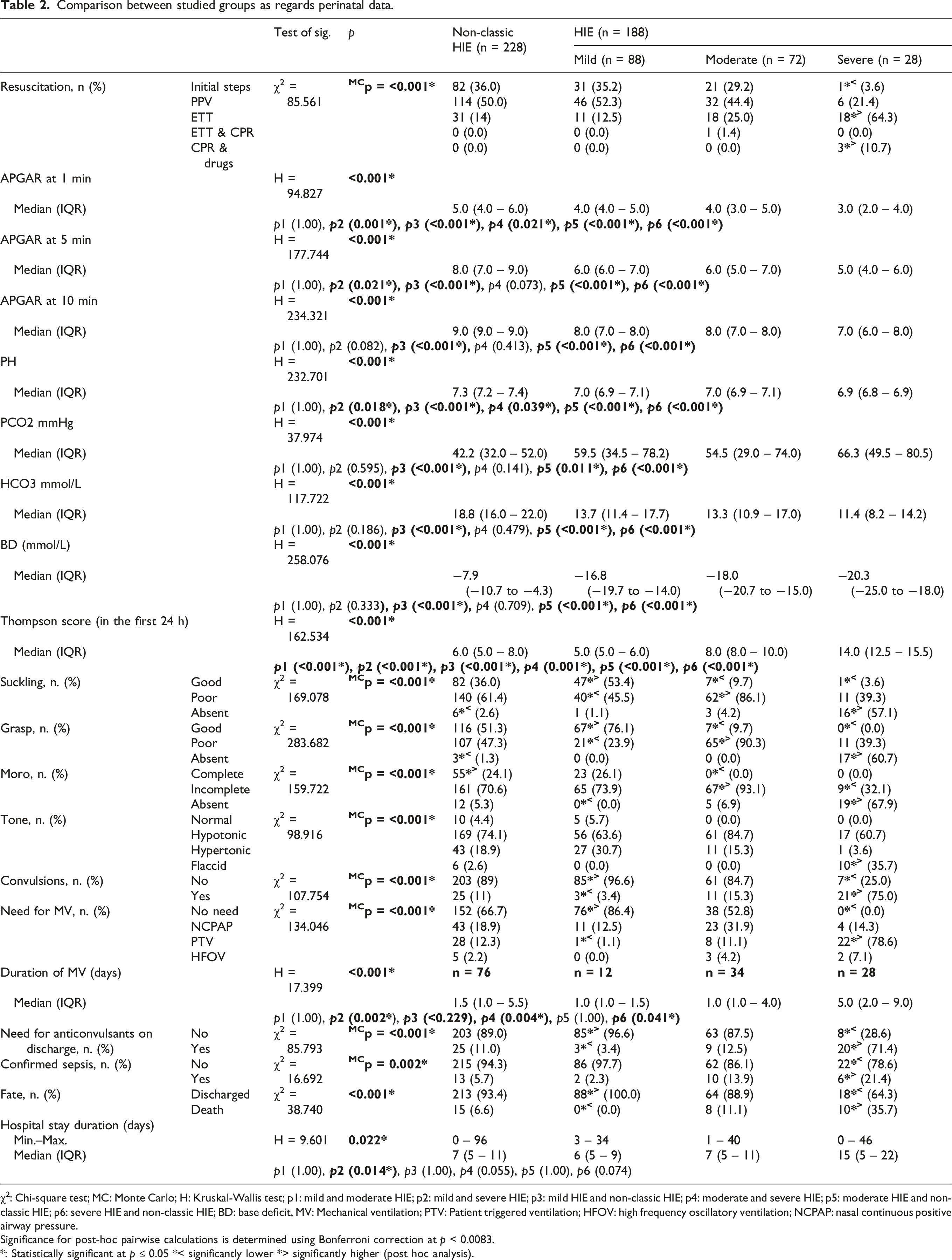
χ2: Chi-square test; MC: Monte Carlo; H: Kruskal-Wallis test; p1: mild and moderate HIE; p2: mild and severe HIE; p3: mild HIE and non-classic HIE; p4: moderate and severe HIE; p5: moderate HIE and non-classic HIE; p6: severe HIE and non-classic HIE; BD: base deficit, MV: Mechanical ventilation; PTV: Patient triggered ventilation; HFOV: high frequency oscillatory ventilation; NCPAP: nasal continuous positive airway pressure.
Significance for post-hoc pairwise calculations is determined using Bonferroni correction at p < 0.0083.
*: Statistically significant at p ≤ 0.05 *< significantly lower *> significantly higher (post hoc analysis).
Comparison between studied groups as regards hematological, coagulation, and chemistry profiles initially.
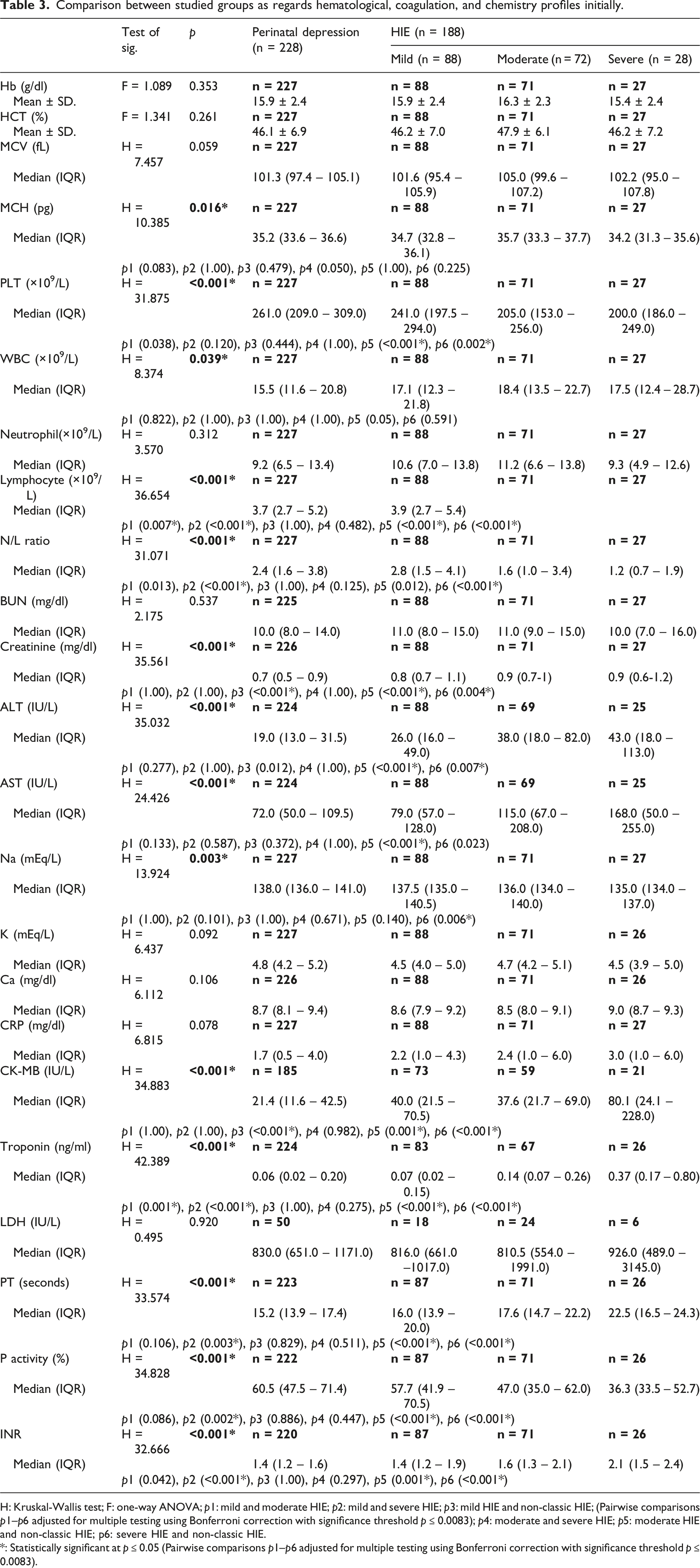
H: Kruskal-Wallis test; F: one-way ANOVA; p1: mild and moderate HIE; p2: mild and severe HIE; p3: mild HIE and non-classic HIE; (Pairwise comparisons p1–p6 adjusted for multiple testing using Bonferroni correction with significance threshold p ≤ 0.0083); p4: moderate and severe HIE; p5: moderate HIE and non-classic HIE; p6: severe HIE and non-classic HIE.
*: Statistically significant at p ≤ 0.05 (Pairwise comparisons p1–p6 adjusted for multiple testing using Bonferroni correction with significance threshold p ≤ 0.0083).
Comparison between studied groups as regards hematological, coagulation, chemistry profiles during TH.
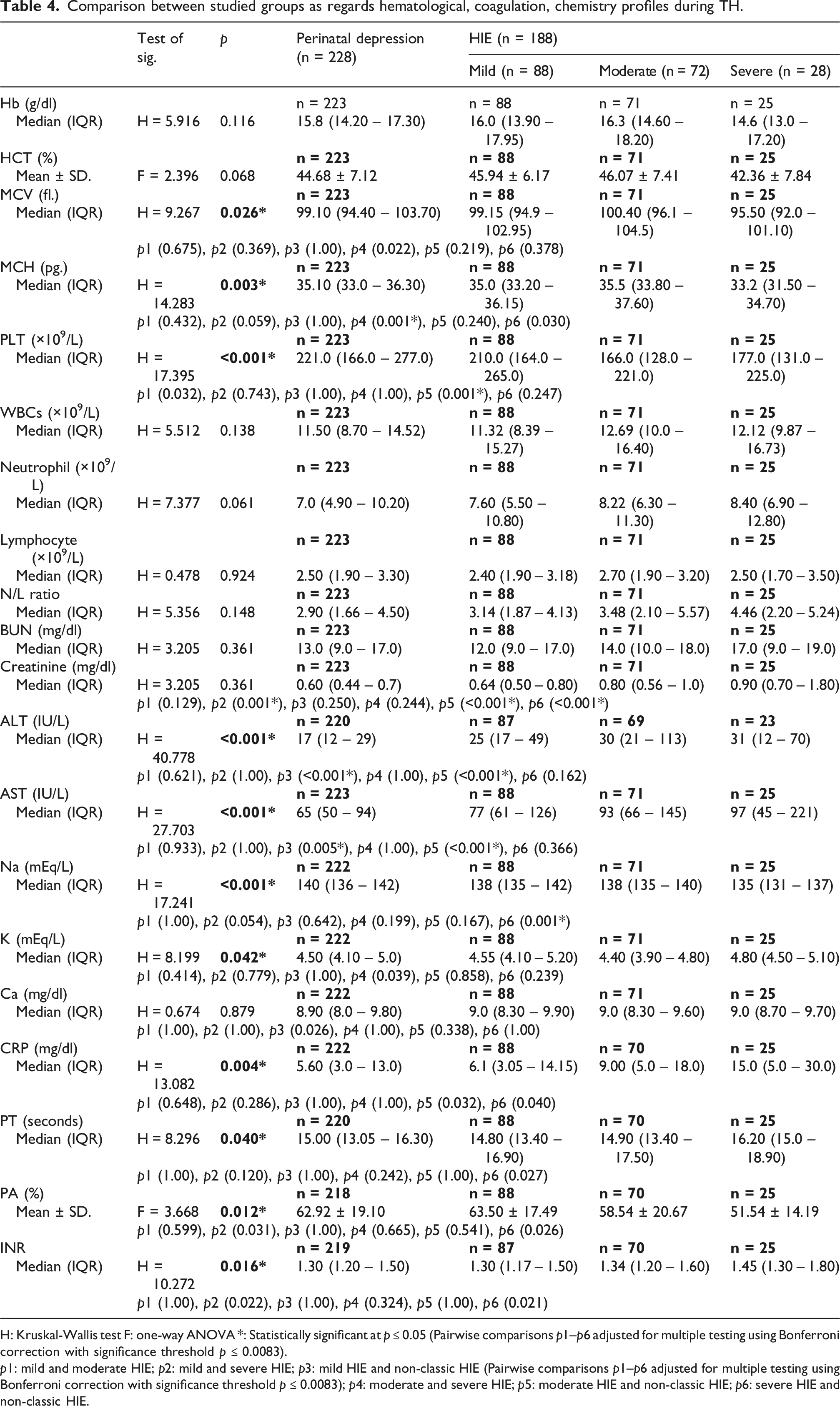
H: Kruskal-Wallis test F: one-way ANOVA *: Statistically significant at p ≤ 0.05 (Pairwise comparisons p1–p6 adjusted for multiple testing using Bonferroni correction with significance threshold p ≤ 0.0083).
p1: mild and moderate HIE; p2: mild and severe HIE; p3: mild HIE and non-classic HIE (Pairwise comparisons p1–p6 adjusted for multiple testing using Bonferroni correction with significance threshold p ≤ 0.0083); p4: moderate and severe HIE; p5: moderate HIE and non-classic HIE; p6: severe HIE and non-classic HIE.
Multivariate logistic regression analysis for the parameters affecting fate of asphyxiated patients.
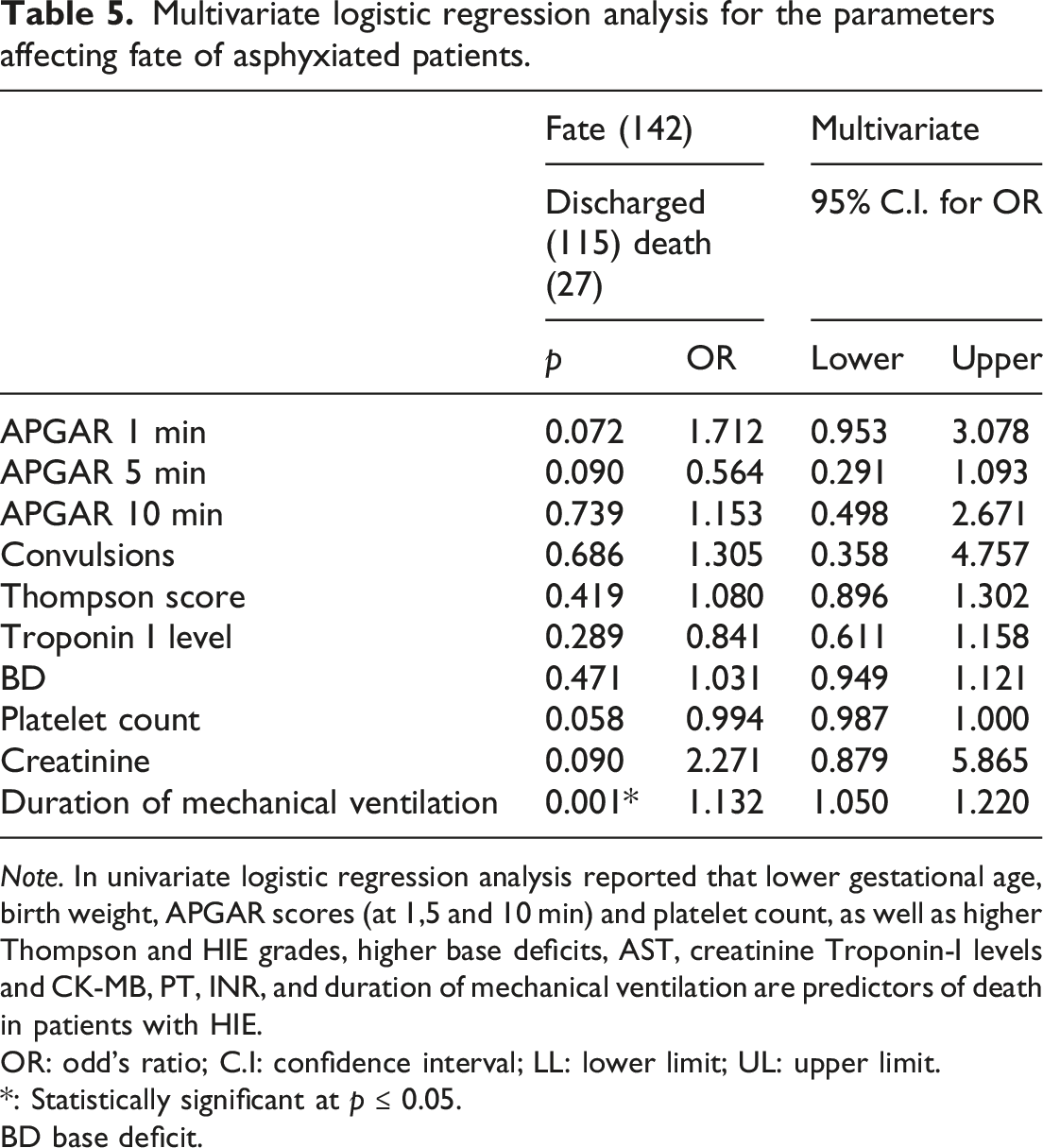
Note. In univariate logistic regression analysis reported that lower gestational age, birth weight, APGAR scores (at 1,5 and 10 min) and platelet count, as well as higher Thompson and HIE grades, higher base deficits, AST, creatinine Troponin-I levels and CK-MB, PT, INR, and duration of mechanical ventilation are predictors of death in patients with HIE.
OR: odd’s ratio; C.I: confidence interval; LL: lower limit; UL: upper limit.
*: Statistically significant at p ≤ 0.05.
BD base deficit.
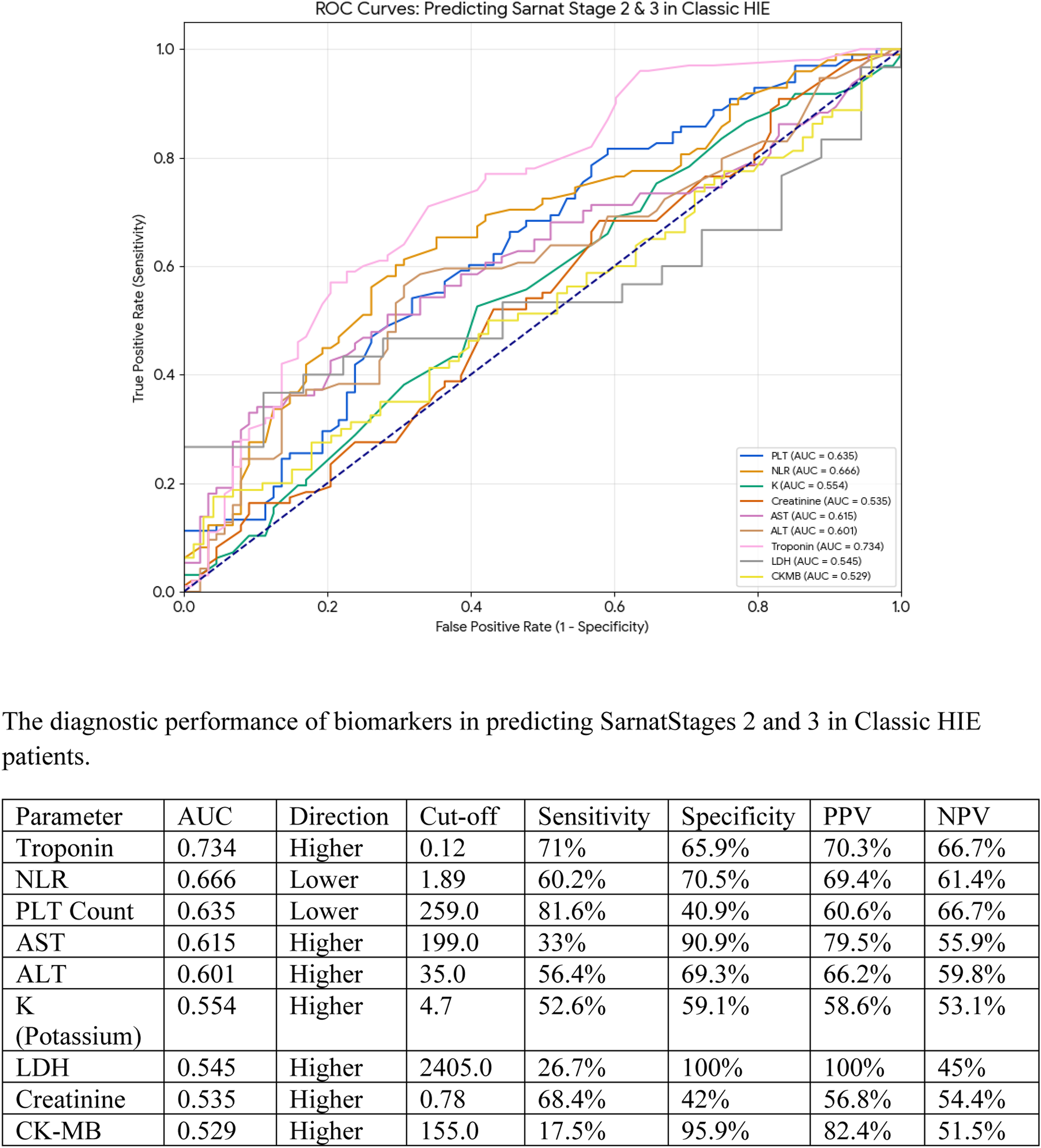
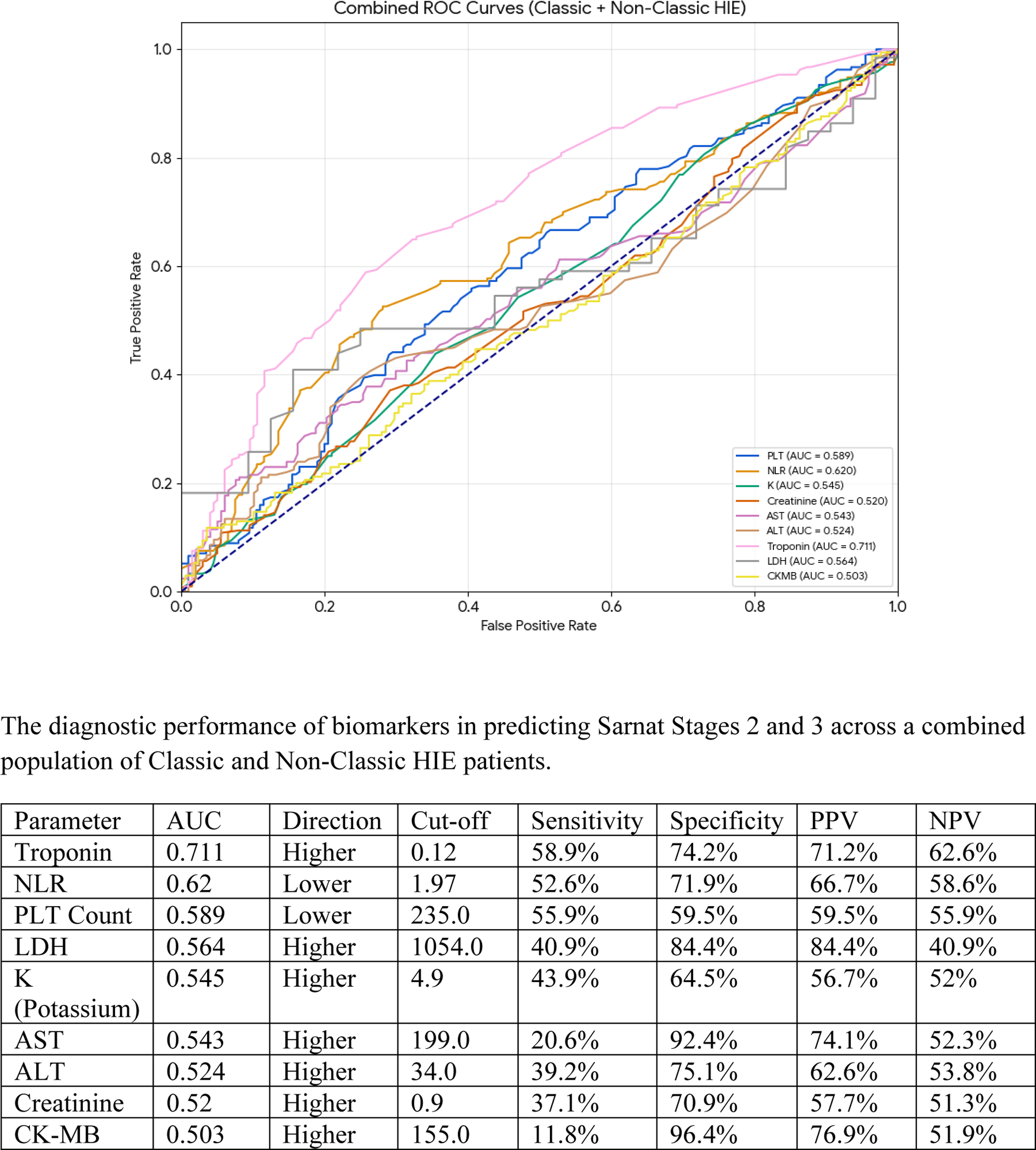
Based on the ROC analysis results in Figures 1–3, Troponin consistently emerges as the most effective biomarker for predicting Sarnat Stages 2 and 3, achieving its highest diagnostic performance in “Classic-HIE” patients demonstrating an AUC of 0.734, a sensitivity of 71%, and a specificity of 65.9%. While other markers like LDH show exceptionally high specificity (up to 1.0 in Classic HIE), their clinical utility is limited by low sensitivity. Across all groups “Non-classic HIE,” “Classic HIE,” and combined populations biomarkers generally demonstrate superior predictive accuracy in the Classic HIE cohort compared to “Non-classic HIE” group, where several parameters like creatinine and AST exhibit AUC values near the 0.50 line of no discrimination. ROC curve of the diagnostic performance of biomarkers in predicting Sarnat Stages 2 and 3 in non-classic HIE patients. ROC curve of the diagnostic performance of biomarkers in predicting Sarnat Stages 2 and 3 in classic HIE patients. The ROC of diagnostic performance of biomarkers in predicting Sarnat Stages 2 and 3 across a combined population of classic and non-classic HIE patients.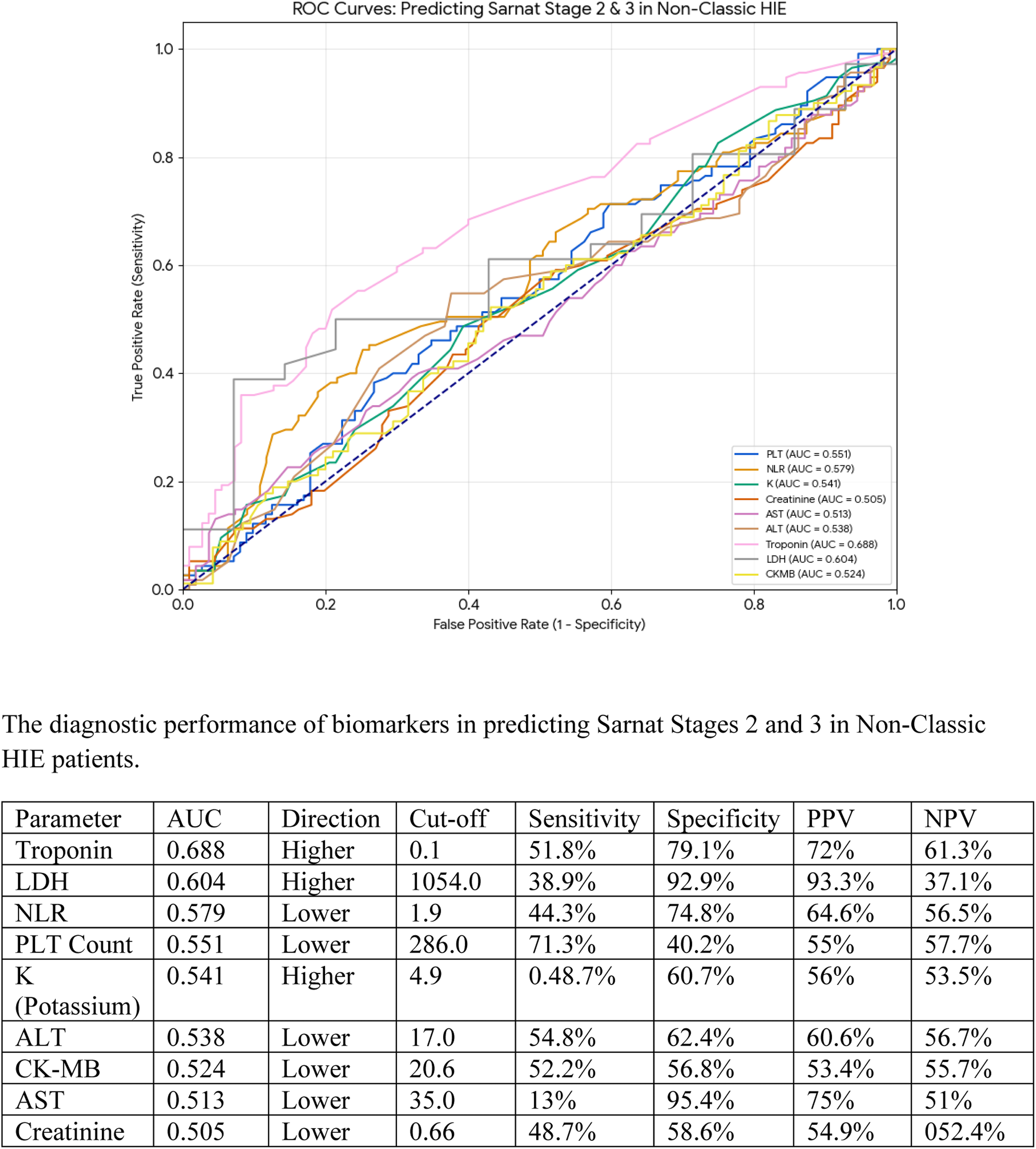
Discussions
Brain injury caused by hypoxia is a significant health issue in low- and middle-income nations. The treatment of newborns suffering from asphyxia is challenged by the subjective nature of clinical criteria and the lack of access to MRI and aEEG in most NICUs in developing countries. TH is the standard treatment for moderate to severe HIE, while the neuroprotection of mild HIE is still being researched. In this study, we focused on a crucial subgroup of asphyxiated newborns classified as “Non-classic HIE.” Additionally, we examined various clinical and laboratory criteria for this subgroup and compared them with different HIE grades. Both “classic HIE” and “Non-classic HIE” patients received TH, provided they exhibited neurological symptoms linked to hypoxia during the perinatal period, and other causes of neuronal injuries were ruled out. Among the patients in the “Non-classic HIE” group, some exhibited notable neuronal symptoms. Of the 228 individuals with “Non-classic HIE,” a high Thompson score was observed as follows: 16 (n = 2), 15 (n = 4), 14 (n = 1), 13 (n = 4), 12 (n = 5), 11 (n = 4), 10 (n = 15), 9 (n = 15), and scores ranging from 3 to 8 (n = 178).
Notably, two patients within the “Non-classic HIE” group initially presented with a Thompson score of 16 and were diagnosed with HIE grade III according to the modified Sarnat score, despite lacking sufficient evidence of fetal acidemia in blood gas analysis within the first 60 min. The first patient was a female neonate, born at 36 weeks of gestation, weighing 2100 g, to a 35-year-old mother who presented to the emergency room with accidental hemorrhage. The mother underwent an emergency cesarean section under general anesthesia. The neonate was intubated during resuscitation, with Apgar scores of 3, 6, and 8 at 1, 5, and 10 min, respectively. Venous blood gas analysis within the first 60 min revealed a pH of 7.3, a PCO2 of 35 mm Hg, a HCO3 of 17 mmol/L, and a BD of −9 mmol/L, while Troponin-I was measured at 0.6 ng/ml. The patient exhibited an initial Thompson score of 16, with absent primitive reflexes and hypotonia. The patient was ventilated for 1 day and discharged after 13 days. The second patient was a male neonate, born at 38 weeks of gestation, weighing 3.6 kg, to a 28-year-old, G6P6 mother with gestational hypertension. This patient was also intubated during resuscitation, with Apgar scores of 5, 8, and 8 at 1, 5, and 10 min, respectively. Venous blood gas analysis within the first 60 min showed a pH of 7.27, CO2 of 54 mm Hg, HCO3 of 20.7 mmol/L, and BD of −6.2 mmol/L, while Troponin-I was 11.7 ng/ml. The patient required ventilation for 52 days and was discharged after 96 days.
For the previously detailed patients, we acknowledge that while MRI imaging was limited by the retrospective/resource-constrained setting, the biochemical evidence (Troponin, ALT, AST) strongly suggests these infants suffered a true hypoxic insult that the initial blood gas missed.
At the cellular level, hypoxia cause anaerobic metabolism and causes fetal/neonatal acidemia; however, the absence of fetal acidemia in our cohort likely reflects late-stage presentation or a chronic-on-acute hypoxic event where the initial metabolic derangement had partially compensated by the time of birth. In addition, hypoxia can cause damage to almost every tissue and organ. In response to hypoxic-ischemic insult to the fetus, a series of protective reflexes, collectively termed the “diving reflex,” get initiated to prevent damage to more vital organs (brain, heart, and adrenals) at the expense of lesser vital organs (kidney, lungs, gastrointestinal tract, liver, and spleen) by an attempt to redistribute available blood flow. 13
Kidneys are highly sensitive to hypoxia or reduced renal perfusion. Early recognition of renal failure is important in babies with HIE to facilitate appropriate fluid and electrolyte management as a stable biochemical milieu is vital. 14 Renal function tests such as S.Cr, BUN, Na, and K are monitored to assess kidney functions. Hepatic involvement is often found in asphyxiated patients as it highly involved in so many metabolic processes. About 40–60% of newborns who diagnosed with HIE experience ischemic hepatic damage. Increased ALT and AST values might be a sign of hypoxic hepatocellular damage, that can indirectly represent the severity of the hypoxic insult and its influence on the prognosis. 13
In the current work, initial creatinine, ALT, AST, and Na showed significant difference among the four groups. Compared to the “Non-classic HIE” group, the mild to severe HIE groups had substantially higher levels of creatinine and ALT. Compared to the “Non-classic HIE” group, the moderate to severe HIE groups had substantially higher AST levels. Baseline serum sodium was significantly lower in the severe HIE group compared to the “Non-classic HIE” group, a finding primarily stemming from hypoxia-induced AKI or secondary to SIADH.
CK-MB and Troponin levels are associated with hypoxic cardiac muscle damage. They are indirect markers of HIE. Among those markers, troponin is generally more specific to hypoxic myocardial injury as it is present in cardiac myocytes, but CK-MB and LDH are found also in other body organs.
The current study showed no significant difference in LDH among the four groups. CK-MB showed higher significant difference in mild, moderate, and severe HIE groups than “Non-classic HIE” group. On the contrary, troponin was significantly higher in moderate to severe HIE than mild HIE and “Non-classic HIE.”
Counter to the present results, Lee et al. 15 showed no significant differences between mild and moderate to severe HIE regarding CK-MB. However, LDH was significantly higher in the moderate to severe group compared to the mild HIE group. Michniewicz et al. 16 showed that troponin was statistically significant higher in the severe HIE group. Beken et al. 17 found that serum CK-MB was much higher in infants who died due to severe HIE and that biomarker changes occurred before the clinical presentation. Furthermore, they found that while LDH significantly increases during the progression of HIE, they do not have strong predictive value in advanced stages (stages 2 and 3) of the condition.
It’s well noticed that platelets, WBC, lymphocytic counts, as well as NLR respected the severity among the four compared groups. Platelet count and NLR were of the least values in severe HIE and of the highest values in “Non-classic HIE” group. While, WBC and Lymphocytic counts were higher in moderate to severe HIE groups than mild HIE-perinatal hypoxia groups. These significant differences were also present during TH. In accordance, Lee et al. aimed to recognize early diagnostic blood biomarkers linked to neonatal HIE and found that only WBC count was significantly greater in moderate and severe HIE. 15 PA is one of the common causes of thrombocytopenia due to hypothermia, hypoxia, sepsis or even catheter associated thrombocytopenia.18,19 Boutaybi et al. reported that neonates with HIE have thrombocytopenia as a result of hypothermia treatment. 20 Kurt et al. discovered that prior to hypothermia, patients with HIE had elevated WBCs, lymphocyte, and neutrophil counts and the values of those markers were subsequently reduced during hypothermia. 21
Severe hypoxia that hindered clotting factor production or function as a result of liver disease or DIC may have an indirect impact on coagulation measures including extended PT and activated partial thromboplastin time (aPTT). 22
In our study, whenever initially and during therapeutic hypothermia, PT and INR showed higher significant difference in moderate to severe HIE groups than mild HIE and “Non-classic HIE,” while Prothrombin activity was significantly lower in moderate to severe HIE than mild HIE and “Non-classic HIE.”
Michniewicz et al. 16 demonstrated that PT and INR were statistically significantly higher in the severe HIE group, which is consistent with the current findings. In contrast to the present findings, Lee et al. 15 found no discernible variations in PT between the two groups.
The current study showed that severe HIE, flaccid tone, absent Moro reflex, absent suckling, absent grasp, convulsions, Thompson score, need for mechanical ventilation (MV) especially PTV and HFOV, duration of MV, need for anticonvulsants, confirmed sepsis, long hospital stay, increased laboratory levels of troponin, CK-MB, PT, INR, Creatinine and AST and are significantly higher in death group than discharged group. BE, platelets count and PA were significantly lower in death group than discharged group.
However, in the logistic regression model only duration of mechanical ventilation was retained and significant. There is correlation between the duration on MV and the prognosis of neonates; the longer the duration, the worse the prognosis. Several factors are attributed with prolonged ventilation including neurological affection, sepsis predisposition, hemodynamic instability and multi-organs affection.
Basiri et al. 23 conducted a study to identify the factors that predict mortality in babies with HIE undergoing selective head cooling. The authors found that the risk of death was increased by significant abnormalities in aEEG, a lower 1-min Apgar score, the need for mechanical ventilation, and advanced neonatal resuscitation. Kutman et al. 24 found that inotropic score and Troponin I are good predictors of mortality in patients with moderate to severe HIE. According to the study by Shankaran et al., 25 hypothermia appears to be less protective in infants with the most severe HIE. Similarly, in our study, all cases of neonatal death involved severe HIE (stage 3).
That is a critical clinical consideration, as the narrow 6-h window for initiating therapeutic hypothermia is the primary challenge when using delayed biomarkers. While the ROC analysis confirms that Troponin has the strongest diagnostic performance in identifying Sarnat Stages 2 and 3, its utility as a “gatekeeper” for cooling depends entirely on the kinetics of its elevation. Troponin levels peak or significantly rise only after the 6-h, therefore, it may be more effective as a confirmatory tool for the “Non-classic” HIE cases rather than a primary trigger for immediate intervention. The physiological rise of troponin occurs as a result of cardiomyocyte injury secondary to prolonged hypoxia and the “diving reflex,” where blood flow is redistributed away from the heart to the brain. This systemic response often means that detectable levels of troponin reflecting significant organ damage may not be fully realized within the critical first few hours after birth.25,26 Troponin I acts as a cumulative marker of cellular injury, making it more reliable for catching these “Non-classic HIE” cases, rather than Ph that represent a snap shot of a moment.
Strength points of the study
The study is powered by several key factors. It included a large sample size collected over a span of 3 years. The research examined most clinical and laboratory biomarkers both initially and during the process of TH. To our knowledge, this is among the few studies that compared the “Non-classic HIE” group with different stages of classic HIE. Although it is a single-center study, AUMH handles critical deliveries from four government sources, which may make it comparable to multicenter studies.
Limitations of the study
It is important to acknowledge several limitations. The study’s retrospective nature, the absence of a control group, and lack of current data about long-term follow-up. However, we have initiated a follow-up phase currently recruiting these patients for neurodevelopmental assessment using the Bayley Scales. This will allow for a comprehensive evaluation of long-term outcomes in future studies, building upon the clinical framework established here. A significant limitation of this study is the lack of early MRI and the unavailability of amplitude-integrated electroencephalography (aEEG) during the study period. While these tools are gold standards for evaluating neonatal encephalopathy, their absence reflects the pragmatic clinical realities of low-resource settings. Furthermore, the retrospective nature of this study may introduce selection bias regarding biomarker data, such as LDH and CK-MB; as these tests were not part of a universal screening protocol, they were more likely to be ordered for the most critically ill neonates based on clinical suspicion and when test is available, which may affect the generalizability of these specific laboratory findings, selection bias.
ROC curves were to differentiate Sarnat Grade 1 from Grades 2 and 3 rather than comparing to healthy controls, reflects the real-world challenge of deciding whether to initiate neuroprotection, especially with emerging evidence that infants with Sarnat grade 1 (mild HIE) are still at risk for neurodevelopmental delays.
Conclusion
Perinatal hypoxia inherently triggers a systemic cascade that extends beyond central neurological injury to affect multiple organ systems, a phenomenon clearly reflected by the checked biomarker dynamics. Crucially, these biochemical and hematological alterations represent the systemic manifestations of generalized perinatal distress rather than direct, localized neurological damage. Our findings indicate that the magnitude of these biomarker aberrations correlates directly with the severity of the initial hypoxic insult. Consequently, these parameters should be viewed as valuable adjunctive tools, rather than diagnostic substitutes, to complement traditional clinical assessments, assist in identifying asphyxiated neonates who may benefit from TH, and anticipate the clinical trajectory of affected patients. Furthermore, ROC analysis demonstrates that Cardiac Troponin-I and NLR serve as robust, objective markers across both classic and non-classic encephalopathy cohorts, potentially functioning as biological bridges to validate an underlying hypoxic burden when early umbilical or neonatal pH levels are deceptively reassuring.
From previous clinical and laboratory results, it is obvious that the majority of patients within the “Non-classic HIE” group remain highly comparable to the mild HIE group. “Non-classic HIE” is considered a huge group of neonates who do not fulfill the criteria for HIE, but are exposed to hypoxic insult and manifest clinical (neurological) and laboratory features similar to “Classic HIE.” Previous research on mild HIE was rather thorough and revealed that it has neurodevelopmental consequences such as learning impairment, speech, and motor delay. Hence, new trends have encouraged the use of TH in the management of mild HIE. 27 Therefore, “Non-classic HIE” might be included in this strategy.
Some concomitant factors affect the course and prognosis of perinatal hypoxia and response to TH. The duration of mechanical ventilation was the most significant factor, with longer hospital stay, and poorer outcomes.
Supplemental material
Supplemental Material - Multi-organ biomarkers for the identification of neonatal encephalopathy in the absence of traditional fetal acidemia: A three-year clinical cohort study
Supplemental Material for Multi-organ biomarkers for the identification of neonatal encephalopathy in the absence of traditional fetal acidemia: A three-year clinical cohort study by M. M. Farag, M. H. Gouda, A. S. M. El-Hadidi, and E. W. Abd-El-Aziz in Journal of Neonatal-Perinatal Medicine.
Footnotes
Acknowledgements
We extend our heartfelt gratitude to all the staff members of the NICU at Alexandria University who assisted in managing the patients whose records were part of this study. Additionally, we are thankful to the filing team in the NICU, as their tremendous efforts were crucial to the completion of this work.
Consent for publication
Written informed consents were waived as anonymous data were extracted from files. The protocol of the research was approved by Research Ethics Committee of Alexandria faculty of medicine on its monthly regular meeting on 19th January 2023 and the need for ethical consent from participants was accepted to be waived as the study of retrospective design and the used patients’ data is anonymous (approval no. is 0107549).
Author contributions
MMF conceived of the presented idea. EWA collected the data. MMF, EWA, and ASME verified the analytical methods. MMF contributed in interpretation of results. MMF and EWA wrote the manuscript. MHG supervised the findings of this work. All authors provided critical feedback and helped shape the research, analysis and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.