
Abstract
Background
Coronary artery dilatation (CAD) in neonates is an uncommon but clinically important finding on echocardiography. Reported associations include multisystem inflammatory syndrome in the newborn (MIS-N) following COVID-19 infection, congenital cardiac malformations, and perinatal inflammatory states. In the post-COVID era, CAD has been reported more frequently.
Methods
This retrospective, record-based case series conducted at a Government Medical College in South India describes the clinical profile of neonates with CAD who were admitted between January 2023 and December 2024.
Results
A total of 24 neonates with CAD were identified during the study period. They were admitted in NICU for different conditions like respiratory distress syndrome, congenital pneumonia, sepsis, or perinatal asphyxia. The mean (SD) gestational age was 35.5 (2.2) weeks, and the mean birth weight was 2557 (646) g. Respiratory distress was the most common presenting feature (95.8%) followed by shock (75%). CAD was detected incidentally during echocardiography which was performed to evaluate persistent pulmonary hypertension of the newborn (PPHN), assess ventricular dysfunction during shock, and exclude congenital heart disease, particularly in those with an unexpected clinical course. One-third of the neonates (n = 8) met the diagnostic criteria for MIS-N and all of them responded to intravenous immunoglobulin therapy, with no mortality. Mortality was 31.25% (n = 5) among the others. Complete resolution of coronary dilatation was observed in all infants within 3–6 months.
Conclusion
Assessment of coronary arteries for dilatation should be considered in any sick neonate with an inadequate response to conventional management. It may be a pointer for MIS-N.
Introduction
Coronary artery dilatation (CAD) is defined as focal or diffuse enlargement of a coronary artery segment exceeding 150% of the adjacent normal segment diameter. 1 CAD is well recognized in Kawasaki disease and multisystem inflammatory syndrome in children (MIS-C) and in the conditions characterized by systemic inflammation and immune-mediated vascular injury.2–4 However, CAD in the neonatal period remains infrequently reported, despite reports of multisystem inflammatory syndrome in neonates (MIS-N) during the COVID-19 pandemic. MIS-N was defined as an inflammatory syndrome in neonates following birth to mothers with SARS-CoV-2 infection during late pregnancy or secondary to neonatal SARS-CoV-2 infection. 5 Emerging data suggest that maternal SARS-CoV-2 infection during antenatal period and antibody transfer, as well as maternal comorbidities such as preeclampsia and gestational diabetes, may predispose neonates to inflammatory endothelial injury.6–8 Maternal antibodies following COVID-19 vaccination can also pass trans placentally. Whether neonatal CAD represents a transient post-inflammatory phenomenon or a marker of severe systemic illness remains uncertain, as does the need for treatment in asymptomatic cases.
Although MIS-N received attention during the COVID-19 pandemic, data on long-term outcomes and follow-up of neonates with CAD are limited. This case series describes the clinical profile and short-term outcomes of neonates with CAD admitted to a tertiary-care neonatal intensive care unit.
Materials and methods
This retrospective, record-based case series was conducted in the neonatal intensive care unit (NICU) of a Government Medical College in South India. All neonates (both inborn and out born) who were admitted in NICU over a 2-year period (January 2023 to December 2024) with echo cardio graphically confirmed CAD were included. CAD was defined as a coronary artery Z-score >2. Gender-specific, body surface area adjusted z-scores of internal diameter of the proximal coronary arteries (LMCA, LAD, LCX, RCA) were calculated based on Lambda-Mu-Sigma method by software. 9 Two well experienced pediatric cardiologists were doing the echo cardio grapy for the suspected cardiac cases. The neonatology resident was doing bedside ECHO for all the sick neonates during an emergency situation if cardiologist was not available. Video of the echocardiography was then sent to the cardiologist through WhatsApp and the cardiologist used to repeat the ECHO next day in all suspected cases.
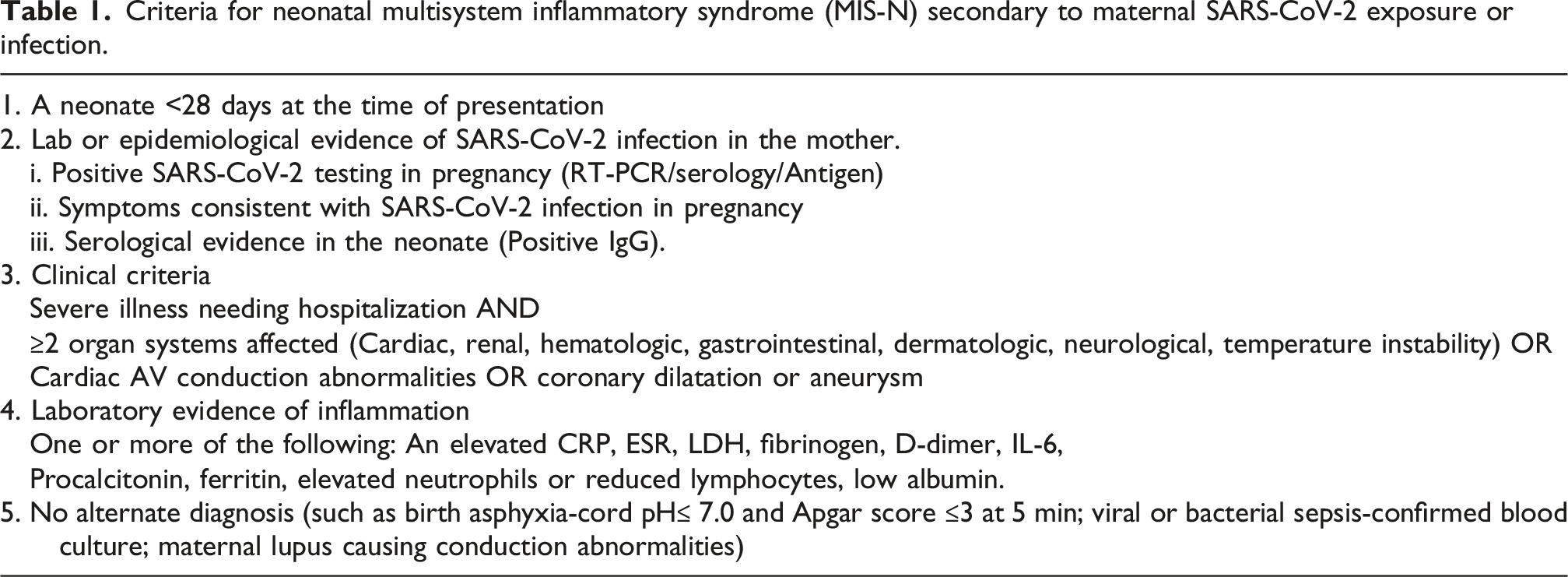
Criteria for neonatal multisystem inflammatory syndrome (MIS-N) secondary to maternal SARS-CoV-2 exposure or infection.
Statistical analysis
Data were analyzed using descriptive statistics. Continuous variables are presented as mean (standard deviation (SD)), and categorical variables as frequencies and percentages.
Results
A total of 24 neonates with CAD were identified during the study period from the monthly statistical report. The mean gestational age was 35.5 (2.2) weeks and mean birth weight was 2557 g (646 g). Majority were preterm (70.8%, n = 17) and of whom 54.2% (n = 13) were late preterm. There was no gender predominance (54.2% males). Nine neonates (37.5%) were delivered by lower segment cesarean section. Maternal diabetes was present in 37.5% (n = 9) and pregnancy-induced hypertension in 54.2% (n = 13). A history suggestive of antenatal viral illness was reported in 29.2% (n = 7) of mothers. Three neonates (12.5%) required resuscitation at birth. All mothers had received COVID-19 vaccination.
Respiratory distress was the most common presenting symptom, observed in 95.8% (n = 23) of neonates; one infant presented with fever from day 1 of life. Invasive ventilation was required in 79.1% (n = 19). The working diagnoses at admission included respiratory distress syndrome (RDS) (45.8%), congenital pneumonia (29.2%), sepsis (16.7%), meconium aspiration syndrome (4.1%), and perinatal asphyxia (4.1%). Shock requiring inotropic support developed in 75% (n = 18) during the course of illness. Hepatosplenomegaly was noted in 20.5% (n = 5). Echocardiography was performed for various clinical indications. CAD was detected incidentally during echocardiography which was performed to evaluate persistent pulmonary hypertension of the newborn (PPHN), assess ventricular dysfunction during shock, and exclude congenital heart disease, particularly in those with an unexpected clinical course.
MIS-N subgroup
One-third of the cohort (n = 8) fulfilled diagnostic criteria of MIS-N (Table 1). Among these, three representative cases are summarized below.
The first was a term male neonate (birth weight 3100 g) referred on day 2 of life with fever from day 1, without any other symptoms. Initial evaluation suggested suspected sepsis; however, cultures and cerebrospinal fluid analysis were normal, and fever persisted beyond day 5. Echocardiography performed to exclude infective endocarditis revealed left main coronary artery (LMCA) dilatation (1.8 mm). Secondary inflammatory markers were markedly elevated (Serum ferritin level 1650 mcg/L, fibrinogen level 132 mg/dl, LDH level 1914 U/L, D-dimer 2.8 mcg/ml and pro-BNP of >35,000 pg/ml). Maternal and neonatal COVID-19 IgG were positive. A diagnosis of MIS-N was made, and treatment with intravenous immunoglobulin (IVIG, 2 g/kg over 2 days) and intravenous methylprednisolone was initiated as per the treatment protocol of MIS-N. Fever subsided after the first IVIG dose, LMCA size reduced within 1 week, and coronary dimensions normalized by 3 months while on follow-up.
The second case was a late preterm female neonate (35 weeks, 2100 g) with respiratory distress from birth. She was initially managed as congenital pneumonia. Baby was referred to this hospital on day 6 in view of multiple extubation failures. Initial ECHO at admission was normal. As the baby was progressing to features of chronic lung disease, echocardiography was repeated at 3rd week of life and revealed dilatation of the right, and left main coronary arteries. Inflammatory markers supported MIS-N, and the infant responded to IVIG followed by methylprednisolone, with successful extubation shortly thereafter. Aspirin was continued for a short period, till normalization of coronaries.
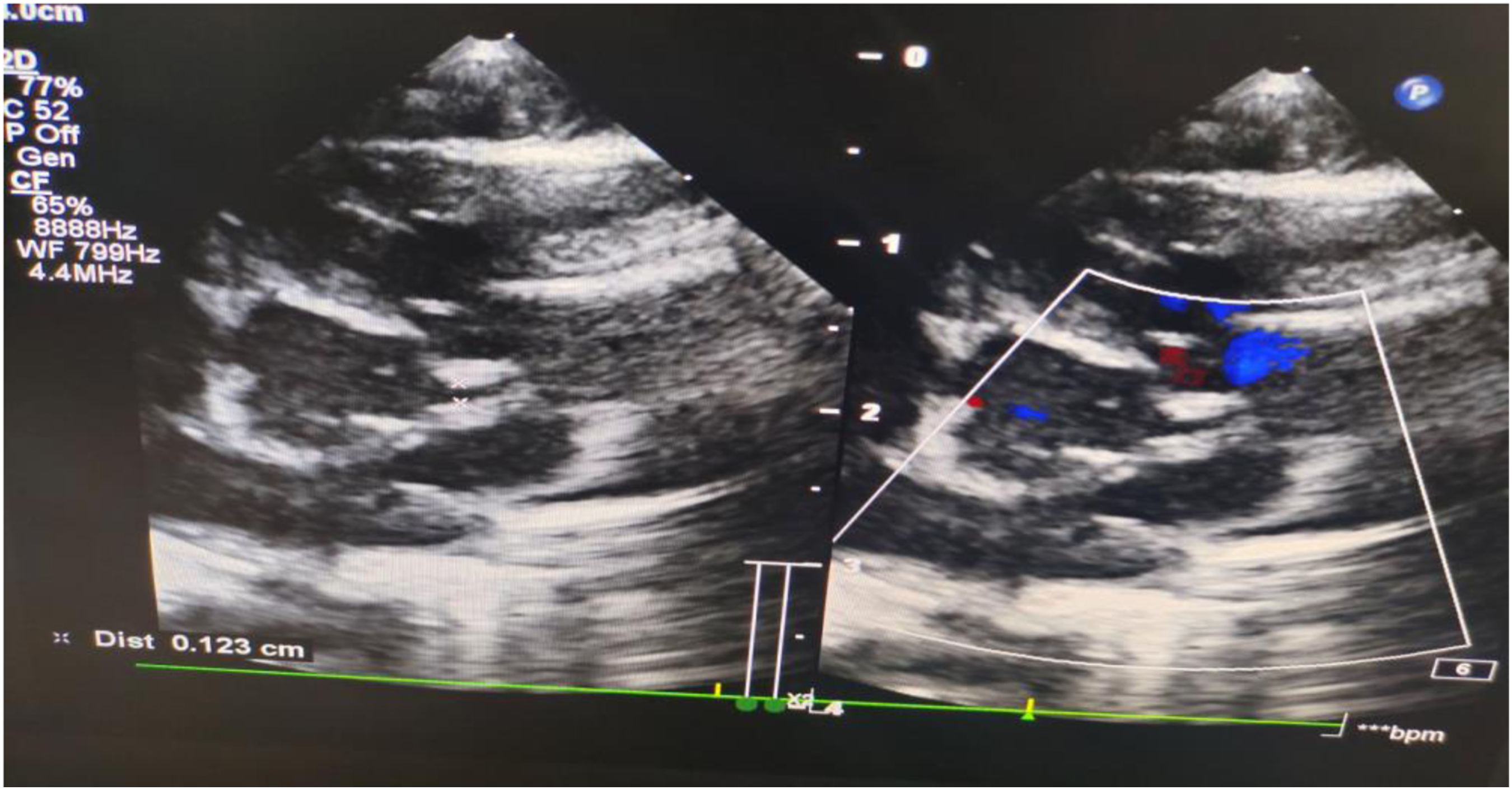
The third case was a late preterm neonate (35 weeks, 2100 g) who initially presented with mild respiratory distress on day 1 but subsequently developed encephalopathy and compensated shock on day 2. Sepsis evaluation was negative. Echocardiography revealed CAD on second day (Figures 1 and 2 ). Inflammatory markers were favoring the criteria for MIS-N and the infant showed a dramatic clinical response to IVIG. Shock was corrected on the very next day. Baby was given corticosteroids and aspirin. Coronary dimensions normalized on follow-up between 3 and 6 months.
The rest of the five babies have almost similar clinical course. They presented with features of RDS or congenital pneumonia needing either NIV or invasive ventilation. As they developed shock, ECHO was done and incidentally detected CAD. Among the MIS-N group, three infants had severe pulmonary arterial hypertension (PAH), two had moderate PAH, two had mild PAH, and one had no PAH. Left ventricular ejection fraction was <55% in 75% of cases. Aspirin was continued at discharge in 87.5% (n = 7). All infants with MIS-N survived to discharge, and all had complete resolution of coronary dilatation by 3–6 months.
For those who have satisfied the clinical criteria of MIS-N, therapy was done as per MIS-N treatment guidelines. IVIG was given at 2 gm/kg as single or two divided doses over 2 days. Then intravenous methyl prednisolone was given at 1–2 mg/kg/day as two divided doses, followed by oral prednisolone to get it tapered over 2–3 weeks. Aspirin was given at 3–5 mg/kg/day once daily after steroids or along with steroids depending on the opinion from cardiologist. It was continued for 6–8 weeks or till the resolution of coronary abnormalities as per cardiologist’s advice. Echocardiographic images showing severe left main coronary artery dilatation (LMCA) with proximal diameter 2.07 mm (bigger arrow) and distal diameter as 1.32 mm (small arrow) before giving IVIG and steroids. Echocardiographic images of same patient shown in Figure 1 shows significant decrease in diameter (1.23 mm) of LMCA after 1 week of receiving IVIG and steroids.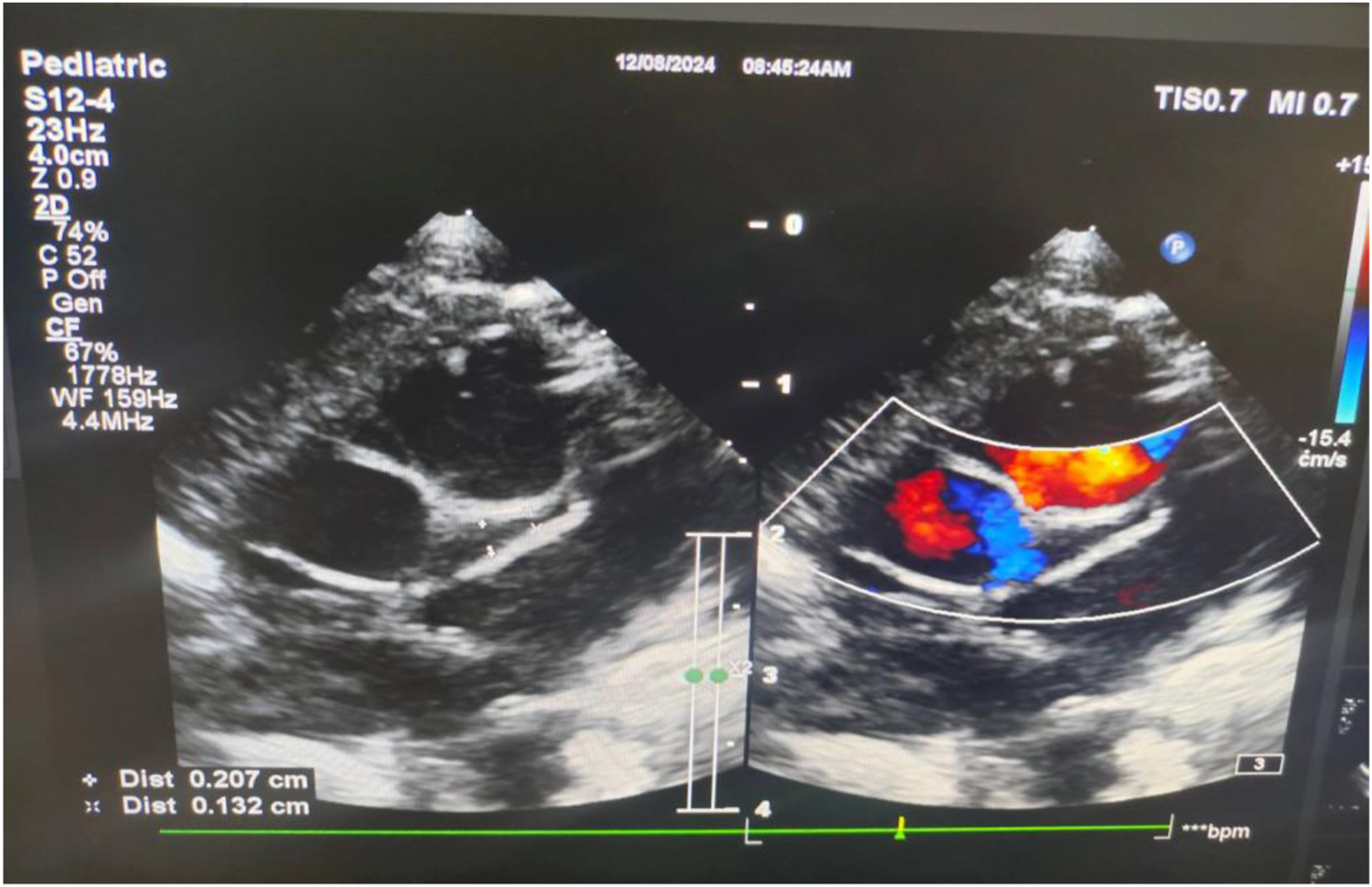
Non–MIS-N group
The remaining 16 neonates had coronary artery dilatation (CAD) but did not fulfill the full diagnostic criteria for MIS-N, as alternative diagnoses were more strongly favored. Eight infants (50%) had respiratory distress syndrome, four (16.7%) had sepsis (three culture-positive and one probable sepsis), three (12.5%) had congenital pneumonia, and one (4.2%) had perinatal asphyxia. In these cases, MIS-N was not suspected clinically. Intravenous immunoglobulin (IVIG) was administered empirically to four critically ill neonates while awaiting inflammatory marker results; however, corticosteroids were not initiated due to lack of clinical response to IVIG and concern for alternative diagnoses. These four cases included one neonate with enterococcal sepsis, one preterm infant with meconium aspiration syndrome (who died within 72 h), and two infants with respiratory distress syndrome complicated by persistent pulmonary hypertension. The latter two infants showed gradual clinical improvement.
As CAD appeared to be an incidental finding in these neonates and there was a strong likelihood of alternative diagnoses, immunomodulatory therapy was not routinely initiated. Additionally, the presence of systemic signs of sepsis in most infants contributed to reluctance in starting steroid therapy. Pulmonary arterial hypertension was observed in eight cases (four severe, three mild, and one moderate). The mortality rate in this group was 31.25% (n = 5).
Echocardiographic and laboratory findings
Comparison of secondary inflammatory markers between MIS-N and other cases.
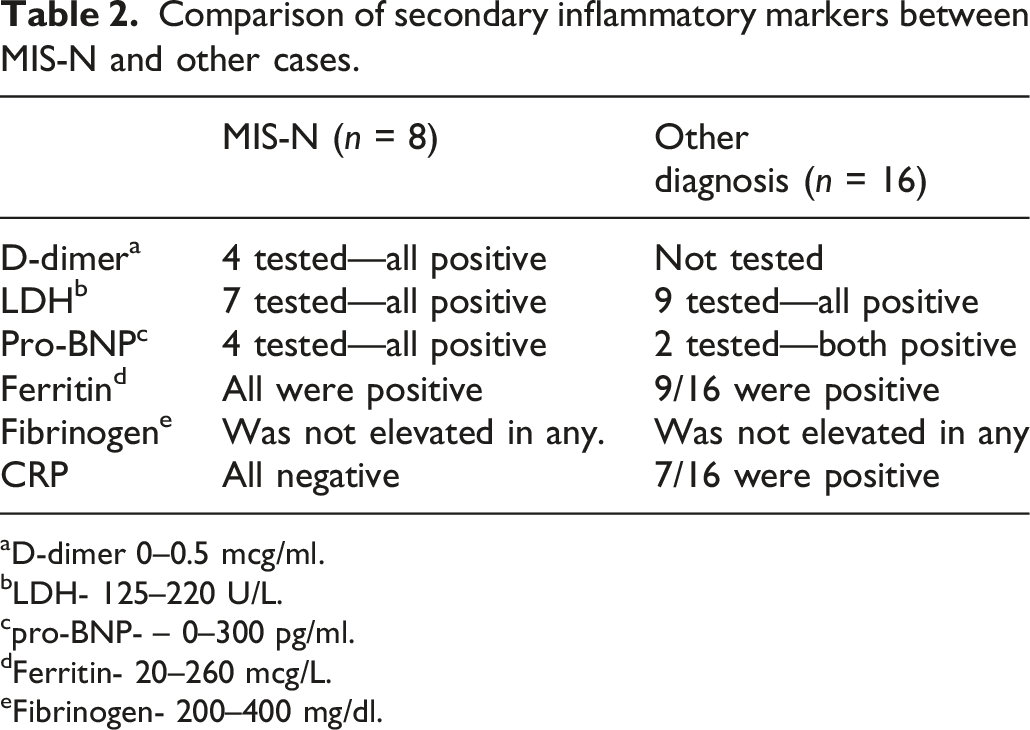
aD-dimer 0–0.5 mcg/ml.
bLDH- 125–220 U/L.
cpro-BNP- – 0–300 pg/ml.
dFerritin- 20–260 mcg/L.
eFibrinogen- 200–400 mg/dl.
Comparison of coronaries affected between MIS-N and other causes.
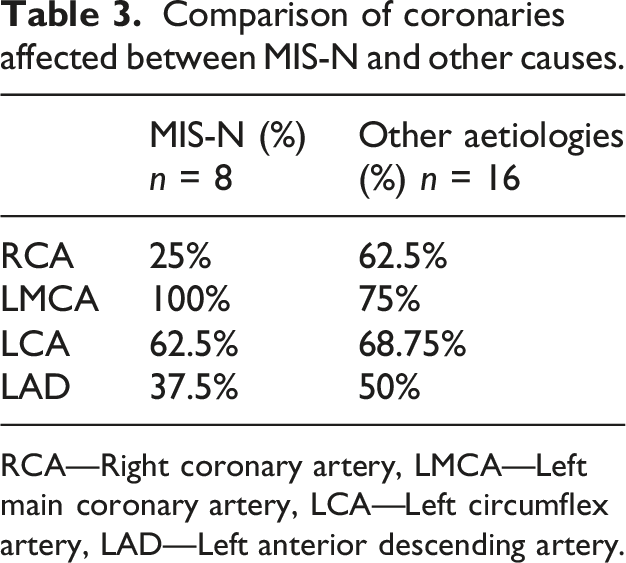
RCA—Right coronary artery, LMCA—Left main coronary artery, LCA—Left circumflex artery, LAD—Left anterior descending artery.
Discussion
This case series highlights coronary artery dilatation (CAD) as an important and often under-recognized finding in critically ill neonates. One-third of cases were attributable to MIS-N, while the remainder were attributed to other inflammatory or critical illness states, suggesting that CAD may represent a transient post-inflammatory vascular change. Whether CAD represents a marker of illness severity may need further comparative studies. Approximately half of the affected neonates were late preterm, emphasizing the vulnerability of this subgroup.
Respiratory distress was the predominant presenting feature, and the majority of neonates developed shock requiring inotropic support. In late preterm neonates with poorly responsive respiratory distress and shock, targeted evaluation of the coronary arteries may provide a critical diagnostic clue. In one notable case, a neonate with presumed congenital pneumonia and PPHN who remained ventilator-dependent into the third week of life showed a dramatic clinical response to IVIG after CAD prompted consideration of MIS-N; this infant also had a coronary aneurysm and responded despite delayed initiation of immunomodulatory therapy. Although fever is not a mandatory criterion for MIS-N, unexplained or persistent fever should raise suspicion and prompt evaluation in appropriate clinical contexts.
Inflammatory marker patterns in this cohort highlight important diagnostic challenges. Fibrinogen levels were not elevated in any case, while LDH, D-dimer, and pro-BNP were frequently elevated, and CRP was largely negative. Given that many biochemical markers are nonspecifically elevated in critically ill neonates and that optimal neonatal cut-offs—particularly in preterm infants—are not well established, these markers may have limited discriminatory value for MIS-N. Consequently, clinical course and echocardiographic findings may be more reliable for diagnosis. In the post–COVID-19 vaccination era, universal maternal–infant antibody positivity further limits the utility of serology in distinguishing MIS-N from other inflammatory conditions.
Consistent with observations in Kawasaki disease and MIS-C, coronary dilatation in our cohort resolved completely within months. Prior pediatric studies attribute coronary involvement in hyperinflammatory states to cytokine-mediated endothelial injury and immune complex deposition. Our findings extend this paradigm to the neonatal period, potentially influenced by antenatal inflammation, maternal SARS-CoV-2 exposure, antibody transfer, or vaccination. Whether neonatal CAD represents a distinct Kawasaki-like process, infection-related inflammation, or a COVID-19-associated immune phenomenon remains unresolved. The need for immunomodulatory therapy with IVIG and steroids also may need expert discussion on case to case basis.
A key therapeutic implication of this study is the potential role of early immunomodulation. IVIG, with or without corticosteroids, appeared beneficial in neonates with MIS-N, CAD, shock, or myocardial dysfunction, paralleling treatment strategies in Kawasaki disease and MIS-C. Aspirin and corticosteroids were used selectively. Importantly, all neonates underwent echocardiographic follow-up through discharge and up to 6 months, confirming complete resolution of coronary abnormalities.
The study is limited by its retrospective design, small sample size, lack of a control group, incomplete availability of inflammatory and virological testing due to resource constraints and absence of long-term follow-up. Additionally, the relative contribution of maternal infection versus vaccination to neonatal antibody positivity could not be delineated.
Whether IVIG is beneficial in neonates with CAD who do not meet MIS-N criteria warrants further investigation. Larger, multicenter studies are needed to define the prognostic value of CAD and guide immunomodulatory therapy in this population.
Conclusion
Coronary artery dilatation should be actively searched in critically ill neonates with an atypical clinical course, poor response to conventional management, or sepsis-like presentation without supportive laboratory evidence. MIS-N should be considered, particularly in late preterm neonates presenting with respiratory distress and shock. However, not all cases of coronary dilatation represent MIS-N, and lack of response to immunomodulatory therapy should prompt reconsideration of the diagnosis. Secondary inflammatory markers have limited discriminatory value in neonates, whereas echocardiographic findings may provide an important diagnostic clue. Bedside echocardiography thus plays a crucial role in the evaluation and management of sick neonates in the post–COVID-19 era.
Footnotes
Acknowledgment
We sincerely thank Dr Sobhakumar S, Emeritus Professor, Dr Radhika.S, Professor and Dr Anupama.S.Pillai, Assistant Professors in Neonatology department for their constant mental support and scientific suggestions offered throughout the study. We also thank Dr Lekshmi S, Professor of Paediatric Cardiology for her scientific support.
Ethical considerations
Human Ethics Committee, Medical College, Thiruvananthapuram, India. Permission Number: HEC NO: 01/20/2025/MCT.
Consent to participate
The authors certify that we have obtained all appropriate patient consent forms. The parents understood that their baby’s name would not be published and due efforts would be made to conceal their identity on publishing the data.
Author contributions
All 6 authors have contributed to the concept and design of the work, analysis, and interpretation of data, drafting of the article, and approval of the version to be published. The first author has done the acquisition of the data. Each author has participated sufficiently in the work to the public responsibility for appropriate portions of the content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings of this study are available with the corresponding author and can be made available on reasonable request.