
Abstract
Background
Neonatal early onset sepsis [EOS] continues to impact the neonatal morbidity and mortality rates worldwide. The diagnosis of suspected EOS in the neonatal intensive care unit (NICU) remains an important challenge for clinicians as the signs of sepsis are often nonspecific and the laboratory investigations may be unreliable or not routinely available.
Presepsin (P-SEP) or soluble clusture of Differentiation 14 Subtype (SCD14-ST) is generated as a part of the body’s response to bacterial infection, being effective in the early phase of inflammation and detected as an early marker of neonatal sepsis.
This study aimed to evaluate the diagnostic value of presepsin in early-onset sepsis, and its prognostic value regarding disease severity, and duration of hospital stay. Moreover, the study aimed to assess the possible predictive ability of presepsin in identifying the type of bacterial organism causing early-onset sepsis in preterm neonates.
Materials and methods
The study recruited 36 preterm neonates with risk factors for early onset sepsis. Control group included 20 sepsis free neonates. Serum Presepsin levels, CRP and blood culture were tested in all studied neonates.
Results
The predictive performance of presepsin levels between 640 and 970 ng/L was evaluated, and the associated clinical implications were analyzed. The serum baseline presepsin was significantly elevated in Sepsis group (p < 0.001). Moreover, it showed the best diagnostic performance at a cutoff value ≥640 ng/L.
Day 3 Presepsin levels demonstrated better performance than day 1 levels in gram negative infections with the best Predictive performance at a cutoff value ≥970 ng/L.
Conclusion
Presepsin evaluation in preterm neonates may serve as a valuable early marker in detection of early onset sepsis and in distinguishing gram-negative bacteria.
Keywords
Introduction
What is known, what is new?
Presepsin has been recognized as an effective early diagnostic marker for both early and late onset sepsis.1,2 Presepsin appears in blood earlier than some other markers, potentially allowing for faster diagnosis and treatment. 3 Moreover, it has been reported to be higher in infections caused by gram negative bacteria. 4
Neonatal sepsis is one of the leading causes of neonatal mortality and morbidity. 5 The vital and major challenge remains the identification of newborns at high risk for early onset sepsis before the appearance of clinical symptoms, in order to guide appropriate antibiotic therapy. 6
Although CRP is the most extensively studied acute-phase reactant, it has several limitations as a diagnostic marker because its sensitivity is lowest during the early phase of infection7,8 and peaks after 2–3 days, making it less reliable in early onset neonatal sepsis. 9
Presepsin (P- SEP) is a promising early biomarker for neonatal sepsis, showing high sensitivity and specificity in diagnosis. It is a fragment of the Soluble CD14 Subtype (SCD14ST) released by-immune cells upon encountering pathogens as part of the host response to bacterial infection, thereby promoting a systemic inflammatory response.10,11
Presepsin levels increase significantly in the bloodstream during the early stages of sepsis and inflammation. It is less influenced by Perinatal factors irrelevant to infection (as mode of delivery, birth stress and maternal complications). In addition, higher levels of Presepsin have been associated with more severe sepsis. Previous studies have demonstrated its high diagnostic accuracy for neonatal sepsis, suggesting that it may serve as a valuable biomarker in neonates with suspected sepsis.12,13
The aims and objectives in this study is to evaluate the efficacy of presepsin as a marker in the early diagnosis of early-onset sepsis in preterm neonates and correlate it with routine sepsis markers. This may help to appraise it as a possible prognostic marker for severity, progression of EOS and mortality outcome. Moreover, to assess the possible efficacy of presesin in identifying the type of bacterial organism.
Methodology
This research was a Prospective observational study. The study was conducted from October 2021 to October 2022 at NICU of Pediatrics Hospital, Ain Shams University Cairo, a tertiary referral center.
The study was approved by the Research Ethical Committee of Ain Shams University no MS619/2021. Informed consent was obtained from the Parents of each patient recruited in the study.
The present study included 56 newborn preterm infants; 36 cases (further divided into proven and suspected sepsis) and 20 controls.
All enrolled neonates underwent routine sepsis screening, including C-reactive protein (CRP) measurement, and were followed for 72 h. A CRP value <6 mg/L at enrollment represented the baseline measurement to ensure assessment during the early phase of suspected sepsis, before the rise of conventional inflammatory markers. The CRP testing and blood cultures are routinely performed in neonates with suspected sepsis as part of Standard NICU practice.
Neonates included were preterms with gestational age <37 weeks (assessed by 2 clinicians using the New Ballard Score).
Cases: Preterm neonates who fulfilled predefined maternal or neonatal risk factors for early-onset sepsis were consecutively recruited during the study period.
Controls: were selected from preterm neonates without clinical or laboratory evidence of sepsis and were matched as closely as possible for gestational age and birth weight.
Neonates with major congenital anomalies likely to affect survival or inflammatory markers were excluded.
Classification of infants according to infection definitions was made by two clinicians and samples were included as septic or free only if both clinicians agreed; the treating physicians were blinded to the laboratory results. All neonates received empirical antibiotics therapy according to protocol in children hospital’s NICUs until culture and sensitivity results appeared.
The neonates comprised in the study were divided into 3 groups: Group 1 (proven sepsis): Diagnosed in case of positive blood culture in the presence of neonatal clinical signs of infection and/or maternal risk factors for sepsis. Group 2 (probable sepsis): Considered in the presence of neonatal clinical signs of infection and/or maternal risk factors for sepsis, in addition to increased CRP >6 mg/dl at follow up on day 3 of life, despite negative blood culture Group 3 (controls): enclosed healthy preterm babies matched for GA and weight who did not show any clinical, radiographic or laboratory findings attributable to sepsis (CRP <6 mg/dl), no maternal risk factors for sepsis, negative blood cultures and no altered serum parameters. All controls were monitored clinically for 72 h by clinical examinations and laboratory assessments to ensure they remained free of sepsis. Any neonate who subsequently developed signs suggestive of sepsis was excluded from the study.
The neonatal clinical indicators of sepsis included: Respiratory distress starting more than 4 h after birth, need for mechanical ventilation; seizures, signs of shock, altered behavior or responsiveness, altered muscle tone; feeding difficulties or intolerance (including vomiting excessive gastric aspirates and abdominal distension); abnormal heart rate, hypoxia (as central cyanosis or reduced oxygen saturation level); Jaundice within 24 h of birth; apnea, signs of neonatal encephalopathy, need for cardiopulmonary resuscitation, temperature abnormality (<36°C or >38°C), unexplained excessive bleeding, thrombocytopenia or abnormal coagulation (International Normalized Ratio >2.0), oliguria persisting beyond 24 h after birth, altered glucose homeostasis, metabolic acidosis (base deficit of 10 mmol/L or greater); in addition to local signs of infection.
14
Maternal risk factors for sepsis included: Suspected or confirmed invasive bacterial infection at anytime during labor or in the 24 h before and after birth, infection in another baby in case of multiple pregnancy, in addition to group B streptococcal infection in a previous baby or colonization of maternal group B streptococci during the current pregnancy; premature delivery after spontaneous labor (before 37 weeks gestation), suspected or confirmed rupture of membranes >18 h in a preterm birth, high intrapartum fever, confirmed or suspected chorioamnionitis; procedures used during pregnancy as cervical circlage and amniocentesis.14,15 Laboratory evidence suggestive of sepsis: Initial Rodwell’s hematological scores: The severity of the illness was graded according to the score for Neonatal Acute Physiology (SNAP II) as: mild (1–20), moderate (21–40), and severe >40.
16
Neonates with serious or major congenital malformations, fetal hydrops, perinatal asphyxia and confirmed intrauterine infections were excluded from the study.
The preterm neonates underwent the following assessments and investigations:
Complete history taking (antenatal, natal, postnatal), gestational age, sex, birth weight, and mode of delivery were recorded. A comprehensive general examination was performed, including assessment of vital signs, level of consciousness, activity tone, and evaluation of major congenital anomalies which may independently affect clinical status and inflammatory markers. The local examination comprised: Respiratory assessment included documentation of respiratory rate and signs of respiratory distress as tachypnea, grunting, chest retractions, nasal flaring, and cyanosis. Cardiovascular assessment included heart rate, peripheral perfusion, capillary refill time, and blood pressure. Respiratory and heart rates were included among the recorded vital signs; Abdominal examination (abdominal girth and signs of feeding intolerance); Central nervous system (head circumference, fontanelles, muscle tone, reflexes, posture and any convulsions observed).
The laboratory investigations included: Blood culture (BACTEC), complete blood count (CBC), and CRP which was measured using a highly sensitive C-reactive protein (hsCRP).
CRP was selected for its wild availability, cost effectiveness and routine use in neonatal sepsis evaluation within our institution.
Presepsin (PSEP) was measured using the enzyme-linked immunosorbent assay (ELISA) technique. The test kits supplied one original standard reagent, and dilution occurred according to instructions provided.
Blood samples were withdrawn from all cases prior to starting antibiotic therapy for culture, CBC with differential, CRP, and P-SEP at day 1 of life. The biomarkers were measured again at 72 h of life. Samples were withdrawn by the most skilled personnel in the facility and no samples were stored to be used in any further research.
Neonates who remained hospitalized beyond 28 days continued to receive standard NICU care and follow up until discharge or transfer. Their final clinical outcomes were documented accordingly.
Statistical analysis
Data were initially entered and organized using Microsoft Excel software and subsequently imported into the Statistical Package for the Social Sciences (SPSS), version 28.0, for statistical analysis. Categorical variables were represented as number and proportions; Quantitative continuous variables were represented as mean and standard deviation (SD) for parametric data, while non-parametric data were presented as median and interquartile range.
The following tests were used to ascertain differences and associations for significance: Normality of data was assessed by visual inspection of their histograms, skewness and kurtosis statistics, and standard errors.
The student’s t-test was used for comparison of independent continuous variables of parametric data between the sepsis and control groups.
The Mann–Whitney U test and Kruskal–Wallis H test were used for independent continuous variables of non-parametric data.
Data distribution was assessed using the one-sample Kolmogorov-Smirnov test and/or Shapiro-Wilk test, variables are not normally distributed if (p value <0.05). Levene’s test was used to verify equality of variances in the samples (homogeneity of variance), variances are not equal if (p value) <0.05. The probability (p value) was set at <0.05 for statistically significant results and <0.001 for those highly significant.
The odds ratio (OR) and 95 percent confidence interval (95% CI) values were displayed where deemed relevant. Receiver Operating Characteristic (ROC) curves were analyzed for P-SEP, CRP values; Area Under Curve (AUC) estimation and the most accurate cut-off values. Furthermore, these were used for calculations of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), likelihood ratio positive (LR+) and likelihood ratio negative (LR−) for all the studied parameters for sepsis prediction. The exact 95% CI were calculated for all parameters.
The AUC 1.0 suggests optimal test index; AUC of a diagnostic test with no significance is 0.5. Generally, a diagnostic test is of low value when its ROC-AUC is between 0.5 and 0.7, medium value between 0.7 and 0.9, and great value when higher than 0.9.
Survival distributions between the studied groups were compared using the log-rank test following Kaplan–Meier survival curve analysis.
Results
Demographic data and anthropometric measures among total sepsis cases and controls.
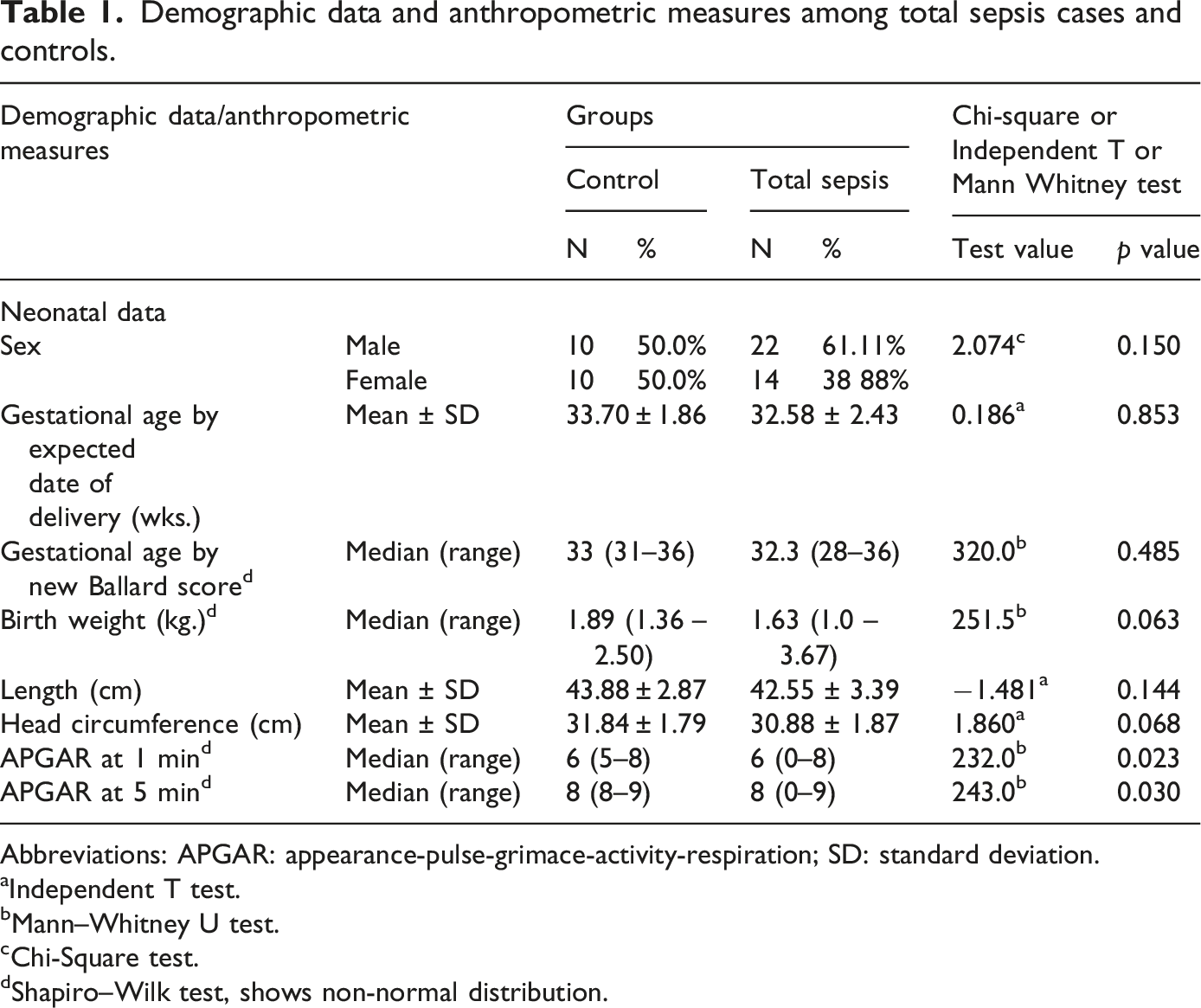
Abbreviations: APGAR: appearance-pulse-grimace-activity-respiration; SD: standard deviation.
aIndependent T test.
bMann–Whitney U test.
cChi-Square test.
dShapiro–Wilk test, shows non-normal distribution.
Hematological laboratory investigations at baseline (day 1).
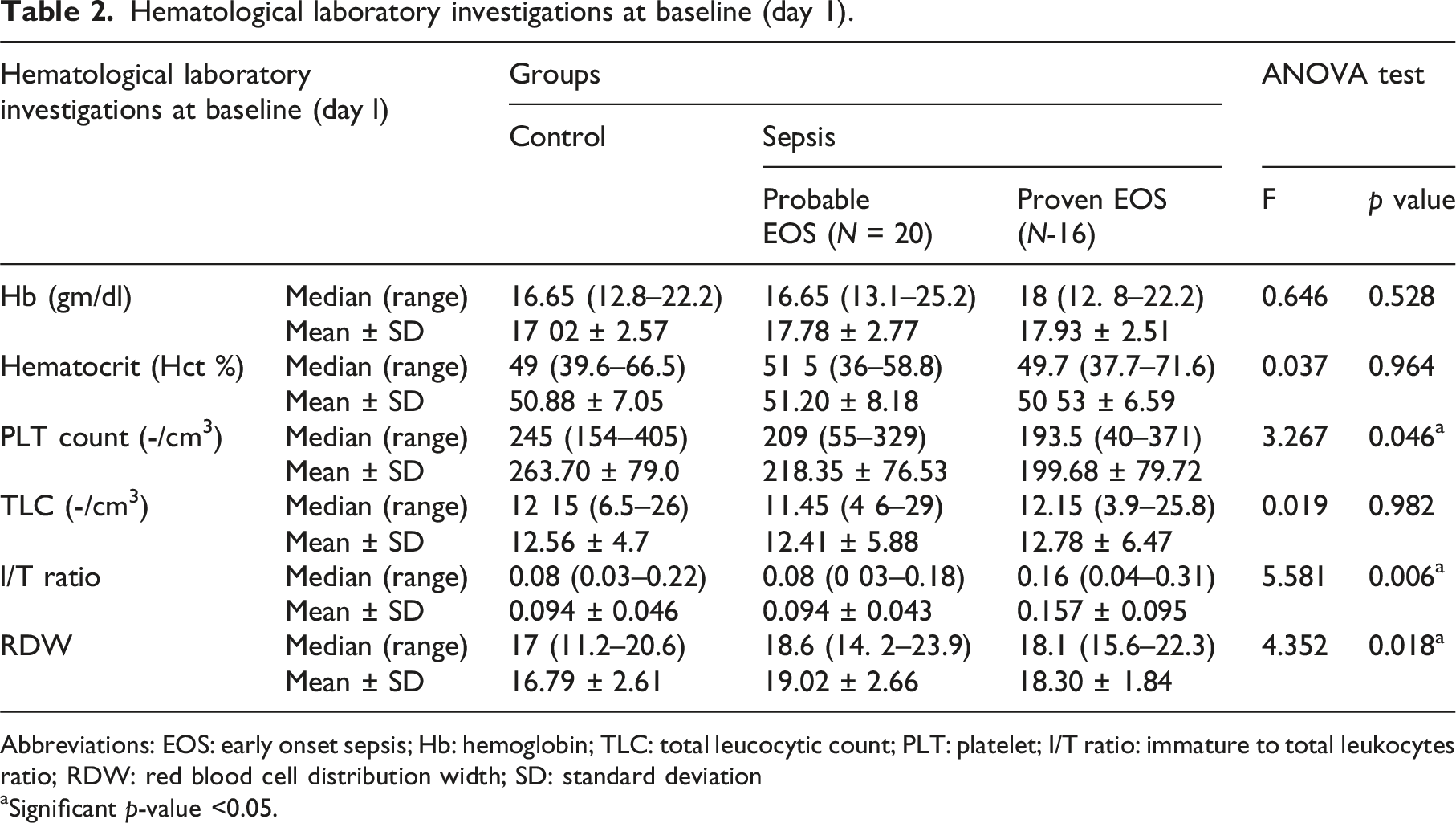
Abbreviations: EOS: early onset sepsis; Hb: hemoglobin; TLC: total leucocytic count; PLT: platelet; I/T ratio: immature to total leukocytes ratio; RDW: red blood cell distribution width; SD: standard deviation
aSignificant p-value <0.05.
Follow up (day 3) revealed only significant difference in hematocrit level (lower in proven than probable sepsis groups).
Regarding the clinical scores and sepsis markers at baseline, Presepsin, SNAP II score and Rodwell score were significantly higher in both probable and proven sepsis than control groups. However, proven sepsis group was significantly higher than probable sepsis group in presepsin and Rodwell score. Moreover, concerning the clinical score and sepsis markers on follow up day 3, proven sepsis group showed higher significance in presepsin levels than probable sepsis group. There was no significant difference regarding CRP.
Diagnostic performance of P-SEP in early detection of EOS at various cut-offs.
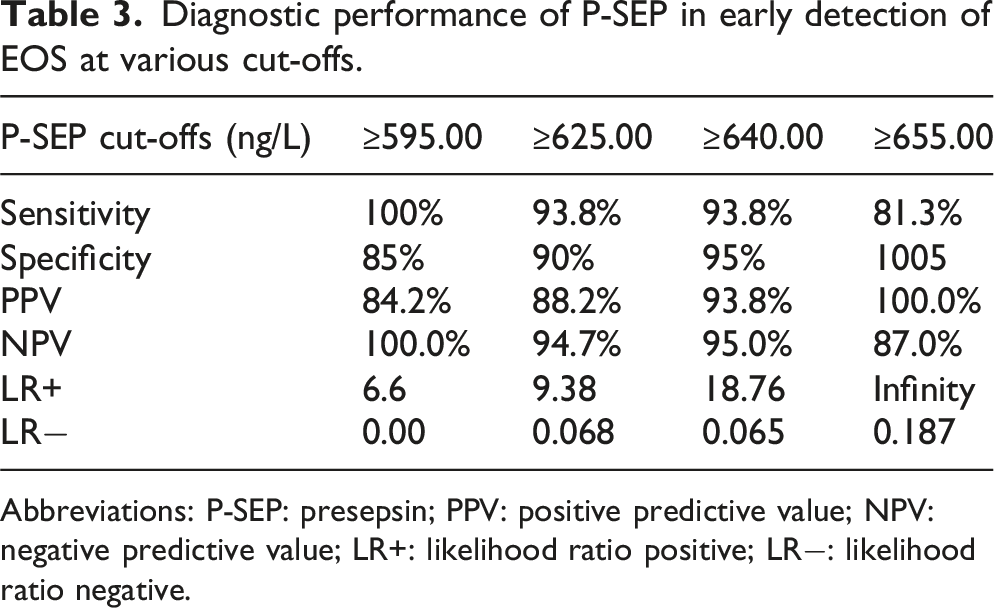
Abbreviations: P-SEP: presepsin; PPV: positive predictive value; NPV: negative predictive value; LR+: likelihood ratio positive; LR−: likelihood ratio negative.
Blood culture results were positive in 44.4% of all sepsis cases. The gram-negative bacteria were detected in 8 of 16 cultures proven early onset sepsis (50%). However, the gram-positive bacteria were detected in 7 of 16 cultures proven EOS (43.7%).
Coagulase negative staphylococcus was the most prevalent organism (n = 4; 25%), followed by Klebsiella (n = 3; 18.7%), Enterococci (n = 2; 12.5%), Acinetobacter (n = 2; 12.5%). Staphylococcus aureus, MRSA, Enterobacter aerogenes, Candida parapsilosis and a mix of Klebsiella and Acinetobacter were similar regards number and percentage (n = 1, 6.3%).
P-SEP level according to blood cultures result in proven EOS group.
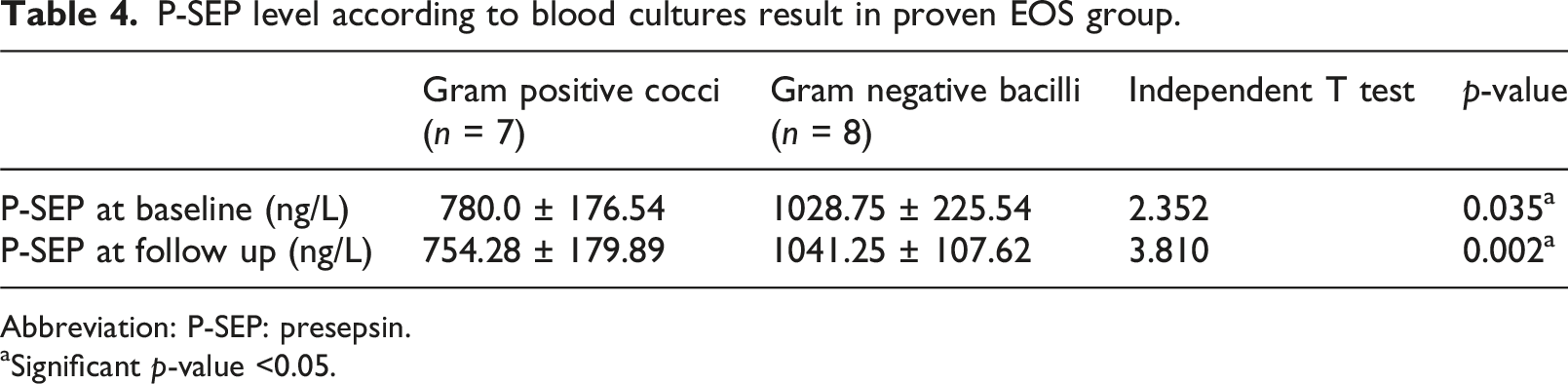
Abbreviation: P-SEP: presepsin.
aSignificant p-value <0.05.
The result values of P-SEP at a cutoff value ≥920 ng/L on day 1 and at a cutoff value ≥970 ng/L on day 3 revealed: 75% sensitivity, 85.7% specificity, 85.7% positive predictive value (PPV) and 77.4% negative predictive value (NPV)) on day 1; While 87.5% sensitivity and 100% specificity, 100% PPV and 88.8% NPV) on day 3. It is apparent that P-SEP on day 3 achieved better performance in prediction of gram-negative infections in EOS.
The ROC curve for prediction of gram-negative infections in patients with EOS is shown in Figure 1. Receiver-operating characteristics (ROC) curve for prediction of gram-negative infections in patients with EOS.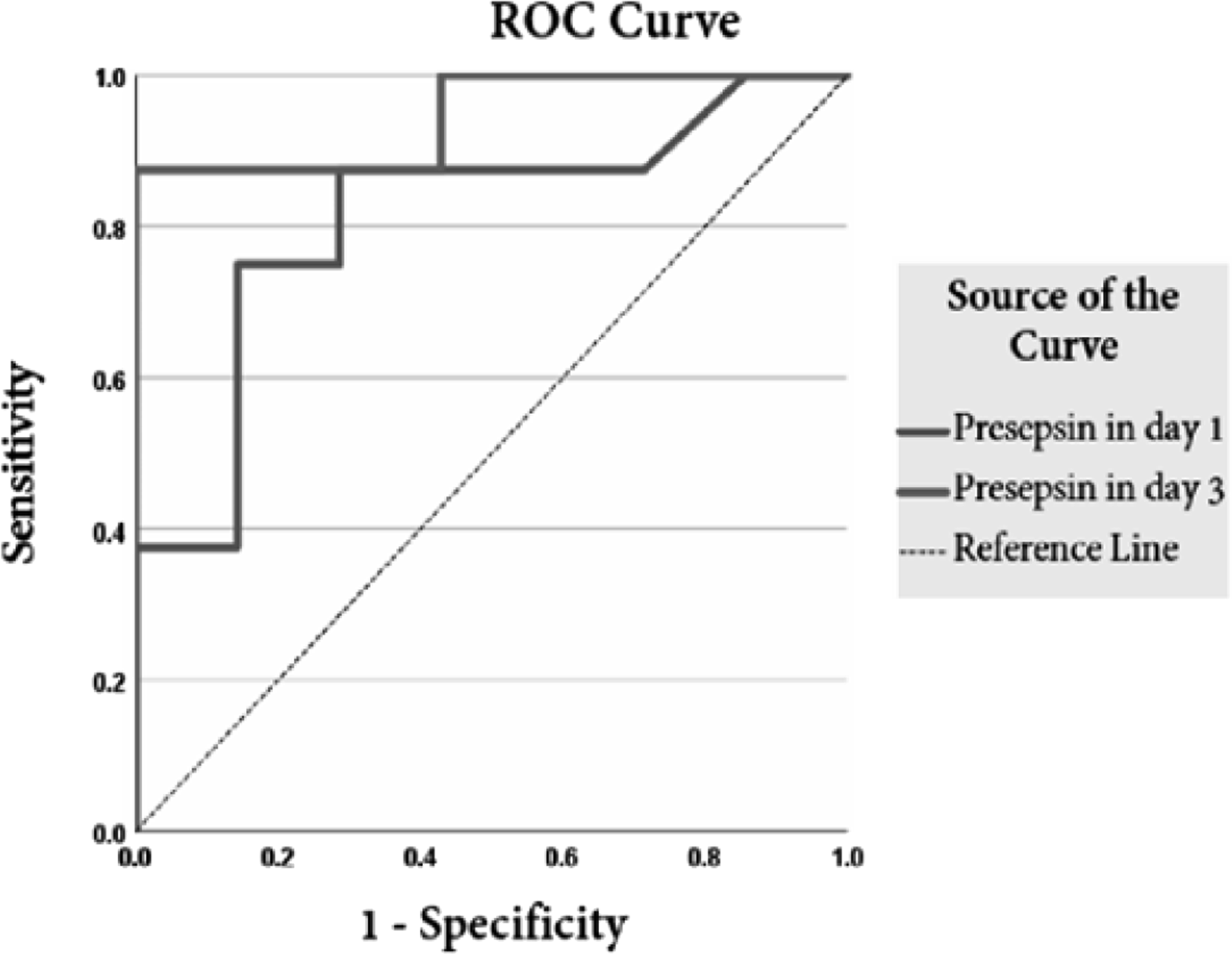
Discussion
Premature newborns in the NICU are more vulnerable to systemic infections due to the immaturity of their immune system. In addition, complications associated with prematurity may further compromise their ability to combat infections. The diagnosis of neonatal sepsis in the NICU is one of the most common and challenging diagnoses due to the nonspecific signs of sepsis. The poor diagnostic performance of currently used laboratory markers and the delay in bacterial culture data (the gold standard), made it crucial to explore other markers that can detect a high likelihood of sepsis in neonates who require antimicrobial therapy soon after birth.17,18
Although studies have shown that traditional diagnostic tools as (total white blood cell count, absolute neutrophil count, immature-to-total neutrophil ratio (I/T) ratio and platelet count) have limited reliability in the diagnosis of early onset sepsis, these parameters continue to be widely used in clinical practice. 19
In the last decade, the human P-SEP level began to emerge as a diagnostic tool for early and late onset sepsis. 20 The present study aimed to investigate the potential diagnostic and prognostic value of P-SEP for early onset sepsis in preterm neonates with initial negative routine sepsis marker (CRP <6).
The relation between the type of causative organism and various sepsis biomarkers has not been extensively studied. Moreover, we aimed to explore this aspect using P-SEP as a potential indicator.
Laboratory results in the present study revealed positive blood culture results in 44.4% of proven sepsis cases, while 55.6% of probable sepsis cases were negative (probable sepsis).
Gram-negative bacteria were isolated in 8 of 16 culture-proven EOS (50%), while gram positive bacteria were identified in 7 of 16 cultures proven EOS (43.7%). One case (6.3%) yielded Candida species. These findings are consistent with previous studies reporting a predominance of gram-negative early onset sepsis among preterm neonates. 21
Despite the fact that gram negative infections in this study were the most frequent, the most common organism was Coagulase negative staphylococcus (CONS) (25%), followed by Klebsiella and Acinetobacter (18.8%, 12.5%), respectively. These findings agree with those reported by Lee et al., who found that CONS represented the most common bacteria isolated from blood. 22 Similarly, Iskandar et al. stated that the most prevalent bacteria in patients with EOS were CONS and Enterobacter gergoviae, while Klebsiella Pneumonia was the most prevalent bacterium in patients with late onset sepsis followed by CONS. 23
In contrast with our results, Hornik et al., found that Escherichia coli and group B streptococci were the most isolated pathogens in preterms with early onset sepsis. 24
Although the platelet count in this study was significantly lower in the proven sepsis group, our findings do not support the use of platelet count in the early diagnosis of EOS [AUC: 0.308; 95% CI (0.133–0.483), (low sensitivity = 1%, specificity 99%). Bayoume et al., found no significant difference in platelet count between culture proven EOS, probable EOS and healthy groups. 25
In addition, hemoglobin, hematocrit and total leucocytic count, showed no significant statistical difference between the 3 groups. On the contrary, Adane et al. reported that anemia and leucopenia were more common in EOS patients than LOS patients. 26
The RDW in our study was significantly higher in the probable sepsis group compared to controls. The cutoff value for sepsis detection was 18.55%; however, our findings do not support the use of RDW in diagnosis of EOS [AUC = 0.659, 95% CI (0.478–0.841), sensitivity 56.3%, specificity 90%.
Regarding CRP in the present study, all preterms included had initial CRP <6 mg/dl. The diagnostic accuracy of initial CRP showed less sensitivity and specificity at a cutoff >2.75 mg/dl. These findings agree with Montaldo et al., who reported lower sensitivity for initial CRP level on admission. 27 Moreover, most CRP results in our study showed elevation >6 mg/dl at follow up but with non-significant statistical difference between proven and probable early onset sepsis. These findings agree with Rashwan et al., who reported no statistical difference in CRP levels between probable and proven sepsis group. 28
The 13 KDa, subtype of the soluble CD14 on the N-terminal segment, is the Presepsin we measured in our study (P-SEP). The P-SEP levels at baseline were significantly higher in both proven and probable sepsis groups than the control group (p < 0.001) and P-SEP on days 1 and 3 were significantly higher in proven sepsis compared to probable sepsis. These findings are in accordance with Rashwan et al.; who reported significantly higher P-SEP means in the proven sepsis compared to the probable sepsis groups. 28
Concerning the statistical correlations with P-SEP in our study, a strong positive correlation was found with the SNAP-II and the Rodwell scores at baseline (r = 0.667, p < 0.001; r = 0.585, p < 0.001), respectively.
SNAP II is a general neonatal illness severity score, it was used in our study as a general neonatal illness severity score including sepsis and we acknowledge that factors as prematurity, respiratory distress and hemodynamic instability may also influence the score.
In comparison to the P-SEP on day 1, the P-SEP on day 3, showed better results having a positive predictive value of 100% versus 85.7%, and a sensitivity of 87.5% versus 75%.
In the present study, P-SEP at follow up showed very good performance for prediction of gram negative infections at a cutoff value of >970 ng/L (Sensitivity 87.5%, specificity 100%, PPV 100%, NPV 88.8%]. However, at the cutoff value >920 ng/L, the P-SEP level at baseline on admission had (sensitivity 75%, specificity 85.7%, PPV = 85.7%, NPV = 77.4%).
These results were in line with those of Masson et al., who found that patients with gram negative bacterial infections had greater baseline P-SEP levels (946 ng/L) than patients with gram negative infections. 15
Inconsistent to our results, Mahmoud Zayed et al., found that gram positive infections had greater P-SEP level at days 1, 3 and 6 of life than gram negative infections. 29 These findings may be related to differences in study population, gestational age distribution, timing of sampling, or diagnostic criteria.
The CD14 is expressed on the membrane of phagocytic cells and serves as a pattern recognition receptor (PRR) for lipopolysaccharide (LPS)/LPS-binding protein (LPS-LBP) complexes. The presence of LPS, a characteristic part of gram-negative bacteria, may help explain why Presepsin levels are higher in gram negative than gram positive infections. 30
Moreover, the present study showed excellent diagnostic performance for culture proven EOS at a cutoff value ≥640 ng/L with sensitivity 93.8% and specificity 95%.
Montaldo et al. evaluated 32 preterm newborns with EOS and compared them with non-sepsis preterms. They found the best cutoff value of P-SEP level in the first 12 h was >653 and >788 ng/L in the first 24 h. 27
In concordance, Miyasawa et al. found P-SEP at cutoff value 795 pg/ml, when they evaluated 13 preterm newborns with EOS and compared them with 18 non-sepsis preterms. 31
The results in our study are in line with several studies suggesting promising results for P-SEP as an early diagnostic sepsis biomarker, but with different cutoff values ranging from 304.5 ng/L to 1442 ng/L. A meta-analysis attributed this discrepancy to the different monitoring time points (from birth to 72 h), different studied populations and different measurement techniques. 32
Regarding the severity of EOS detected by the SNAP II score in the present study, P-SEP level at follow up showed higher cutoff values than P-SEP levels at baseline in prediction of sepsis severity. These findings are consistent with an interesting study by Pietrasanta et al., who reported that P-SEP levels correlate with the severity of the disease. 33
In comparison to the Rodwell score, which had the second-best model quality for EOS detection in our study, the P-SEP showed better sensitivity and positive prediction value (93.8% vs 87.5%), (93.8% vs 87.5%), respectively. In line with our results, Ashraf et al. reported that Presepsin is an accurate diagnostic biomarker for early diagnosis of sepsis compared to other acute phase reactants and inflammatory markers. 34
Based upon the present results, our study supports the previous research results, which conclude that P-SEP levels were significantly higher in early onset preterms compared to healthy preterms. The P-SEP AUC is greater than the AUC of Rodwell, SNAP II, and CRP scores.
Although P-SEP and CRP on day 3 demonstrated relatively comparable sensitivity and negative predictive values in our study, P-SEP showed superior overall diagnostic performance through earlier elevation, higher specificity and better discriminatory ability in detecting neonatal sepsis.
To summarize, Presepsin may improve antibiotic usage in NICUs by enabling earlier and more accurate identification of neonatal sepsis. Its rapid rise during bacterial infection and relatively high sensitivity may help clinicians distinguish infected from non-infected neonates sooner than conventional markers alone. This could support earlier decisions regarding initiation, or reduce unnecessary antibiotic exposure in neonates with suspected early-onset sepsis.
Finally, it is important to take into account a number of noteworthy limitations of this research. The study we conducted was carried out in a single center with a small sample size, limiting the generalizability of our samples. The limited number of culture-positive cases, limits the statistical power for robust ROC curve deviation and subgroup analysis. In addition, variability in assay techniques and cutoff values between institutions and its routine implementation in resource-limited settings may be affected by the cost all of which may affect the widespread applicability.
Conclusion
Presepsin evaluation in preterm neonates with early onset sepsis can serve as a valuable early marker and a good predictor for gram negative infections, 28 days mortality and sepsis severity.
Footnotes
Acknowledgments
The authors would like to acknowledge the parents of the patients and medical staff of Ain Shams University who accepted to participate in the current study.
Ethical considerations
The study was approved by the Research Ethical Committee of Ain Shams University no. MS619/2021 and was conducted in accordance with the ethical standards of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from the parents of each patient recruited in the study.
Author contributions
D.F., M.I.: conceptualization, data curation and supervision. A.N., H.I.: data curation, investigations and analysis. Authors read the final version and editing draft. All wrote the final paper and accepted it.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
It was conducted at NICU of Pediatrics Hospital, Ain Shams University, Cairo, Egypt.