
Abstract
Objective
To identify variables associated with extubation success in preterm infants undergoing first elective extubation and to determine cutoff values to support clinical decision-making.
Methods
This retrospective cohort study included preterm infants (gestational age ≤36 weeks and 6 days) admitted to a neonatal intensive care unit who underwent first elective extubation after orotracheal intubation. Extubation failure was defined as reintubation within 48 h. Bivariate and multivariate analyses were performed. Discriminant analysis defined cutoff values, and bootstrapping (500 replicates) supported comparisons.
Results
Among 218 eligible infants, 73.9% achieved extubation success. In multivariate analysis, weight at extubation (OR 1.02; 95% CI 1.01–1.04), PaCO2 (OR 0.93; 95% CI 0.89–0.98), and heart rate (OR 0.97; 95% CI 0.94–0.99) were independently associated with success. Cutoff values were 34.7 mmHg for PaCO2 and 156 bpm for heart rate, both with modest sensitivity and specificity.
Conclusions
Weight at extubation, PaCO2, and heart rate were independently associated with extubation success. Although their discriminatory performance was modest, these variables may provide clinically relevant information when interpreted within the context of early extubation. Their integration into a multidimensional assessment may support more individualized decision-making.
Introduction
Mechanical ventilation (MV) provides essential respiratory support for preterm infants who are unable to maintain spontaneous breathing. Although its use, along with technological advances in intensive care, has significantly increased survival rates in this population, it has also been associated with a parallel rise in respiratory complications and impaired neurodevelopment. 1 Given this scenario, the current focus is to reduce ventilatory support and promote early extubation in preterm infants, while minimizing the risk of extubation failure. 2 However, there remains a lack of consistent data to guide clinicians in determining the optimal timing for extubation, thereby reducing the risk of failure. 3
Extubation failure in preterm infants receiving MV is associated with significant adverse outcomes, including prolonged use of MV, increased incidence of bronchopulmonary dysplasia, and extended stays in the neonatal intensive care unit (NICU). 4 Although tests such as the spontaneous breathing trial (SBT) have been used to predict extubation success, recent publications have questioned the routine use of the SBT, citing concerns regarding its low specificity, lack of standardized protocols, and potential to cause hemodynamic instability, particularly in extremely preterm infants.4–6
Preterm infants are particularly susceptible to extubation failure, largely due to the immaturity of their respiratory systems and muscle weakness. 7 The absence of objective criteria to guide extubation further exacerbates this risk. Factors such as pulmonary maturity, birth weight, gestational age, and other clinical parameters have been identified as indicators of successful extubation,8,9 as they provide a more comprehensive assessment of an infant’s capacity to sustain spontaneous breathing.
According to the review, 7 clinical variables such as gestational age, birth weight, and caffeine use, along with physiological parameters including heart rate variability (HRV), may assist in predicting extubation readiness. Similarly, reviews10,11 have reported that higher gestational age, greater birth weight, higher pre-extubation pH, lower FiO2 and PaCO2 before extubation, and a higher Apgar score at 5 min are associated with extubation success in preterm infants, highlighting the importance of a multifactorial assessment in clinical decision-making.
Understanding these clinical predictors is essential for reducing complications related to reintubation. Although several studies have investigated predictors of extubation outcomes in preterm infants, there is still no consensus regarding which readily available clinical parameters should be incorporated into routine bedside decision-making. In addition, clinically applicable cutoff values for these parameters remain poorly established. Therefore, this study aimed to identify clinical variables independently associated with extubation success and to establish objective cutoff values to support extubation readiness assessment in routine neonatal intensive care practice.
Methods
This retrospective, single-center cohort study was conducted through the analysis of medical records as part of a collaboration between academic and tertiary care institutions. Data were collected from January 1, 2019, to December 31, 2020. Ethical approval was obtained from the Research Ethics Committees of both institutions under the following registrations: CAAE No. 47582621.8.0000.5149 (approval No. 4.867.132) and CAAE No. 47582621.8.3001.5132 (approval No. 5.003.612). This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
A proactive attempt was made to contact all parents or legal guardians of the newborns to present the study and obtain written informed consent. Informed consent was successfully obtained from those who could be reached. In cases where contact was not possible—due to outdated contact information, lack of response to multiple attempts (email or phone), or death—a Data Usage Consent Form was used, as authorized by the Ethics Committee, to ensure strict confidentiality and privacy of participant data.
Eligibility criteria
Inclusion criteria
The study included medical records of all preterm infants admitted between January 1, 2019, and December 31, 2020. Eligibility was limited to neonates with a gestational age ≤36 weeks and 6 days who were admitted to the NICU and required orotracheal intubation. Data collection was conducted at the time of the first extubation attempt for each infant; therefore, none of the included neonates had a prior history of extubation failure.
Exclusion criteria
Preterm infants were excluded if they had a diagnosis of congenital heart disease, genetic syndrome, or congenital malformation; underwent unplanned extubation; did not follow the institutional protocol for assessing readiness for extubation; had previous extubation failure; were not born in the hospital; died before extubation or had incomplete medical records.
Potential sources of bias inherent to the retrospective design were considered, including selection bias and incomplete records. Cases with missing data were excluded, and no imputation methods were applied. The sample size was defined by the number of eligible records available during the study period.
Variables
The clinical variables collected were selected based on the available literature at the time of study design and included gestational age, birth weight, sex, mode of delivery, Apgar scores at 1 and 5 min, number of surfactant doses, weight at extubation, postnatal age at extubation, duration of invasive mechanical ventilation, PaCO2 (arterial blood gas measurements), heart rate (HR) and extubation outcome (success or failure).
Protocol
According to the institutional protocol in place at the time of data collection, preterm infants were considered eligible for assessment of readiness for extubation when they met specific clinical stability criteria. These included satisfactory arterial blood gas parameters, hemodynamic stability without the need for escalating inotropic support and favorable chest radiograph findings indicating adequate lung expansion and resolution of acute pulmonary pathology. Following this clinical assessment, they underwent an SBT, which was part of the institutional protocol for assessing readiness for extubation.
The SBT protocol used at the institution involved the ET-CPAP mode, with a PEEP of 5–7 cmH2O, maintaining the same inspiratory flow and FiO2 that the preterm infants had been receiving during mechanical ventilation. The trial was maintained under these conditions for 5 min. Preterm infants were considered to have passed the SBT when they presented no more than one of the following instability criteria: HR <100 bpm or >20% above baseline, bradypnea or respiratory rate >50% above baseline, frequent apnea (>3 consecutive episodes), SpO2 < 90%, blood pressure >20% above baseline, or a Silverman-Andersen score ≥3. Failure of the SBT was defined as the presence of two or more instability criteria. In such cases, mechanical ventilation was resumed using the previous ventilator settings, and a new SBT was not performed for at least 24 h. These criteria were established by the institutional assessment of readiness for extubation protocol in effect during the study period.
Those who successfully passed proceeded to elective extubation within 1 h after test completion. After extubation, all preterm infants were transitioned to nasal intermittent positive pressure ventilation or nasal continuous positive airway pressure, according to the institution’s protocol.
According to the institutional protocol, extubation success was defined as the absence of reintubation within the first 48 h following the procedure. Although time frames for defining extubation failure may vary across studies, the 48h window was adopted to maintain consistency with the unit’s clinical criteria and routine practice during the data collection period.
The clinical criteria used to diagnose extubation failure included the occurrence of apnea (defined as a respiratory pause ≥20 s associated with oxygen desaturation and bradycardia), persistent desaturation (defined as peripheral oxygen saturation <90% for at least 20 consecutive seconds despite adequate oxygen supplementation and positional adjustments), presence of stridor, sustained bradycardia (HR <80 bpm), and signs of increased respiratory effort.
Statistical analysis
The normality of continuous data was assessed using the Shapiro–Wilk test. Continuous variables were summarized as mean (minimum–maximum), whereas ordinal variables, including Apgar scores, were presented as median [interquartile range]. Categorical variables were expressed as absolute and relative frequencies. Corresponding 95% confidence intervals were reported when appropriate.
To evaluate the variables that influenced extubation success (categorical outcome), bivariate association analyses were performed using Spearman’s correlation test or Pearson’s chi-square test, according to the type of variable. A Generalized Linear Model (GLM) was used to construct the prediction model for extubation success in neonates. Variables with p < 0.10 in the bivariate analysis, as well as those that, based on theoretical assumptions, could also influence extubation success or failure, were included in the model. However, only the independent variables that remained statistically significant (p < 0.05) were retained in the final adjusted model. A logit link function and binomial probability distribution were used. Predictive factors identified in this analysis were expressed as odds ratios (OR) with their respective 95% confidence intervals (95% CI). The statistical quality of the model was verified by the absence of multicollinearity, 12 the presence of homoscedasticity, and the normal distribution of residuals. Missing data were present for pre-extubation PaCO2 (30 cases, 13.8%) and HR (2 cases, 0.9%). No imputation procedures were performed. Multivariable logistic regression analyses were conducted using complete-case analysis. For continuous variables identified as independent predictors in the final model, a univariate discriminant function analysis was applied to establish clinical cutoff values for classifying neonates according to the likelihood of extubation success. This approach was chosen because, in the present sample, it yielded clinically meaningful cutoff values and superior classification performance compared with ROC-based methods, which demonstrated limited discriminatory ability (AUC <0.70). To enhance the robustness of comparisons between the extubation success and failure groups, particularly given the unequal sample sizes, bootstrapping was performed with 500 simple random sampling replicates. Group comparisons were conducted using independent Student’s t-tests, Mann–Whitney U tests, or chi-square tests, as appropriate according to variable distribution.
Infants who failed the spontaneous breathing test and therefore were not extubated were classified in the unfavorable outcome group for analytical purposes, as they were considered not ready for extubation based on predefined clinical criteria. All analyses were performed using SPSS version 23.0 and Minitab version 16.0. As this was a retrospective study, no a priori sample size calculation was performed. The final sample size was determined by the number of eligible infants available during the study period.
The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational research. 13
Results
A total of 568 preterm newborns were assessed for eligibility (Figure 1). Of these, 350 were excluded due to incomplete medical records (n = 115), death before extubation (n = 143), never having been intubated (n = 20), birth outside the hospital (n = 17), congenital malformation or genetic syndrome (n = 8), unplanned extubation (n = 8), or not undergoing the SBT (n = 21). The final sample comprised 218 preterm newborns who underwent extubation readiness protocol as part of their first extubation attempt. Among them, 161 (73.9%) achieved extubation success and 57 (26.1%) were classified as extubation failures, including 23 neonates who failed the SBT and were not extubated (for statistical purposes, infants who failed the SBT were included in the extubation failure group). Flowchart of participant selection.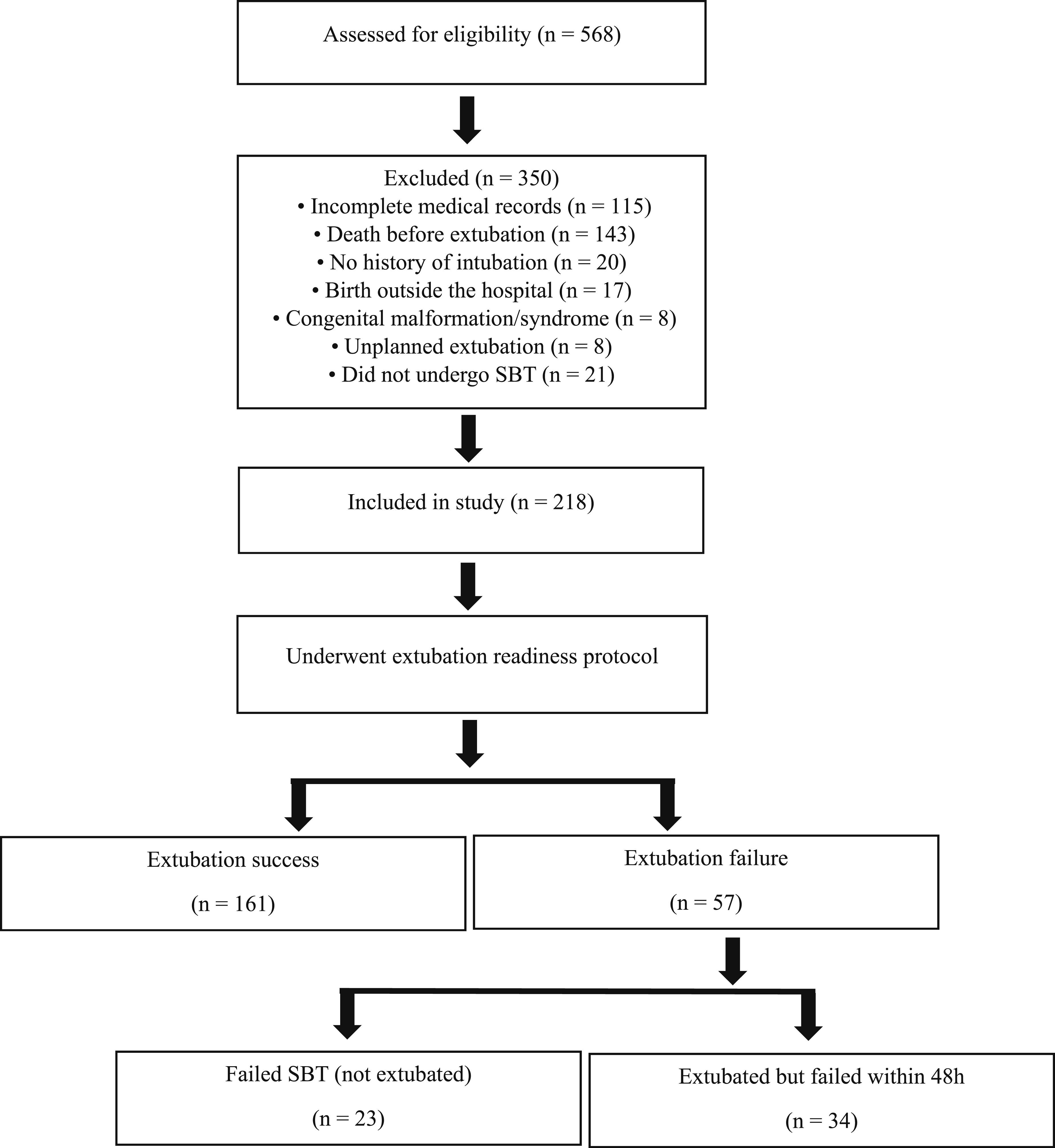
Sociodemographic and clinical characteristics of preterm infants according to extubation outcome.
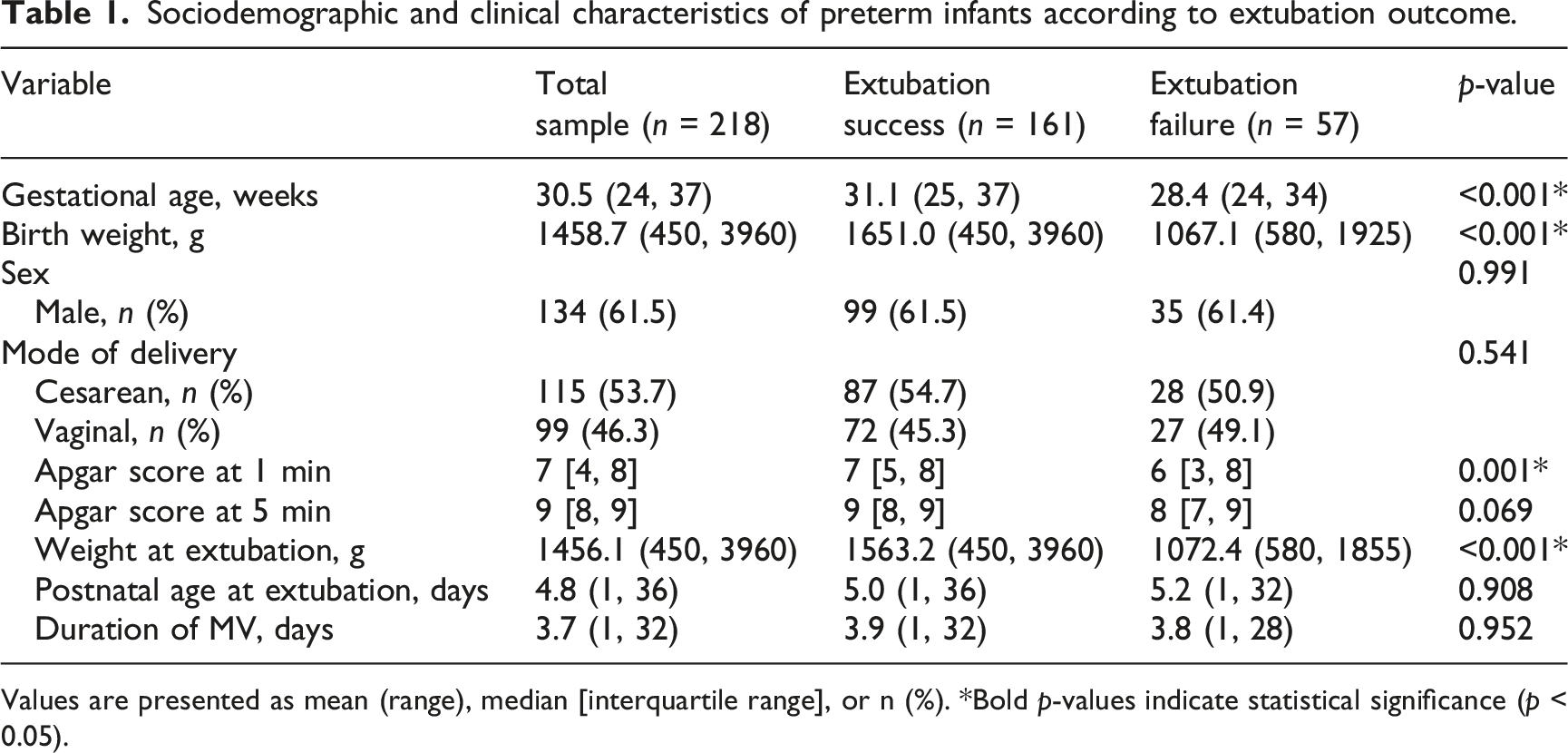
Values are presented as mean (range), median [interquartile range], or n (%). *Bold p-values indicate statistical significance (p < 0.05).
Bivariate analysis of clinical variables associated with extubation success.
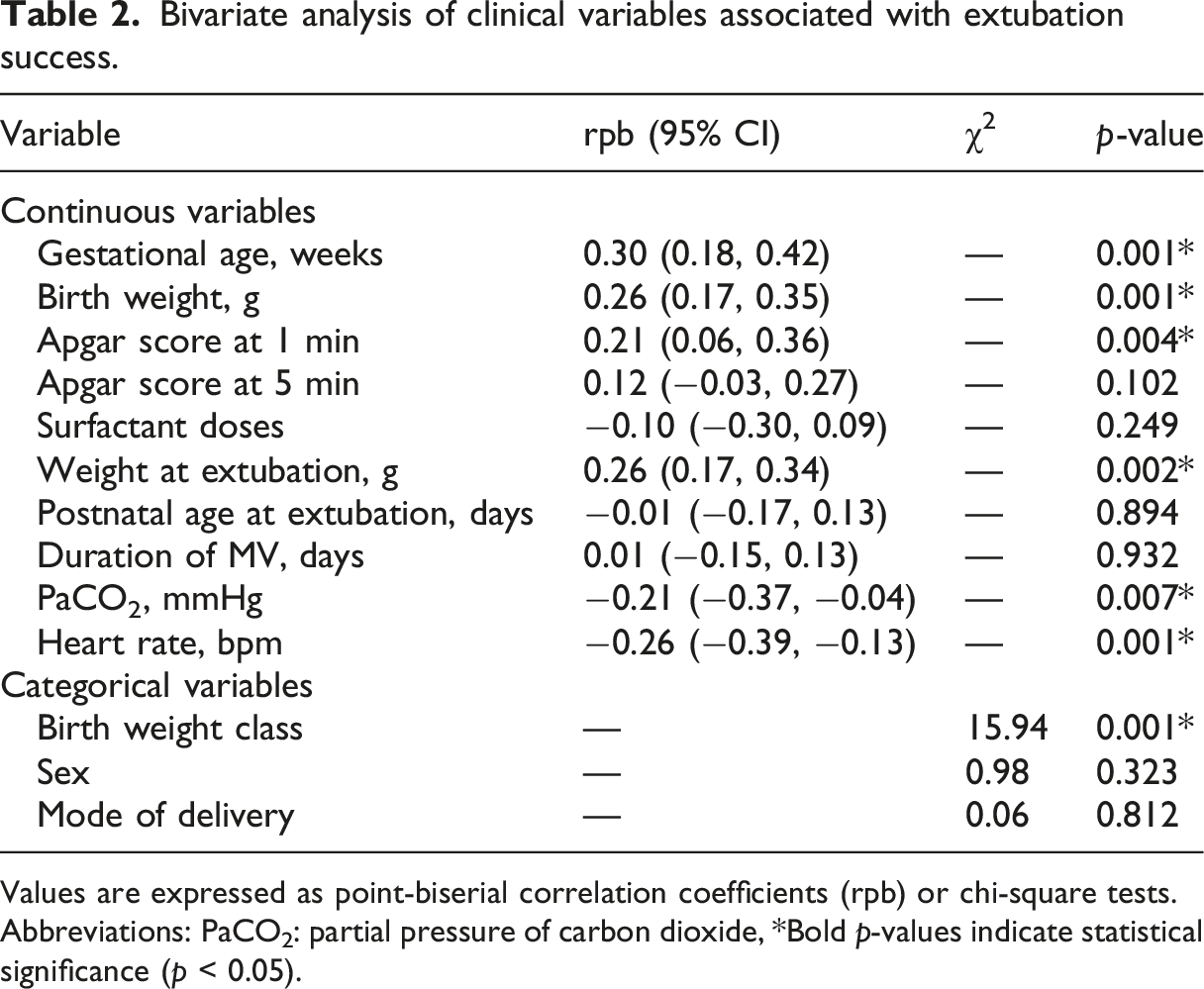
Values are expressed as point-biserial correlation coefficients (rpb) or chi-square tests. Abbreviations: PaCO2: partial pressure of carbon dioxide, *Bold p-values indicate statistical significance (p < 0.05).
Multivariate binomial logistic regression analysis of factors associated with extubation success in preterm infants.
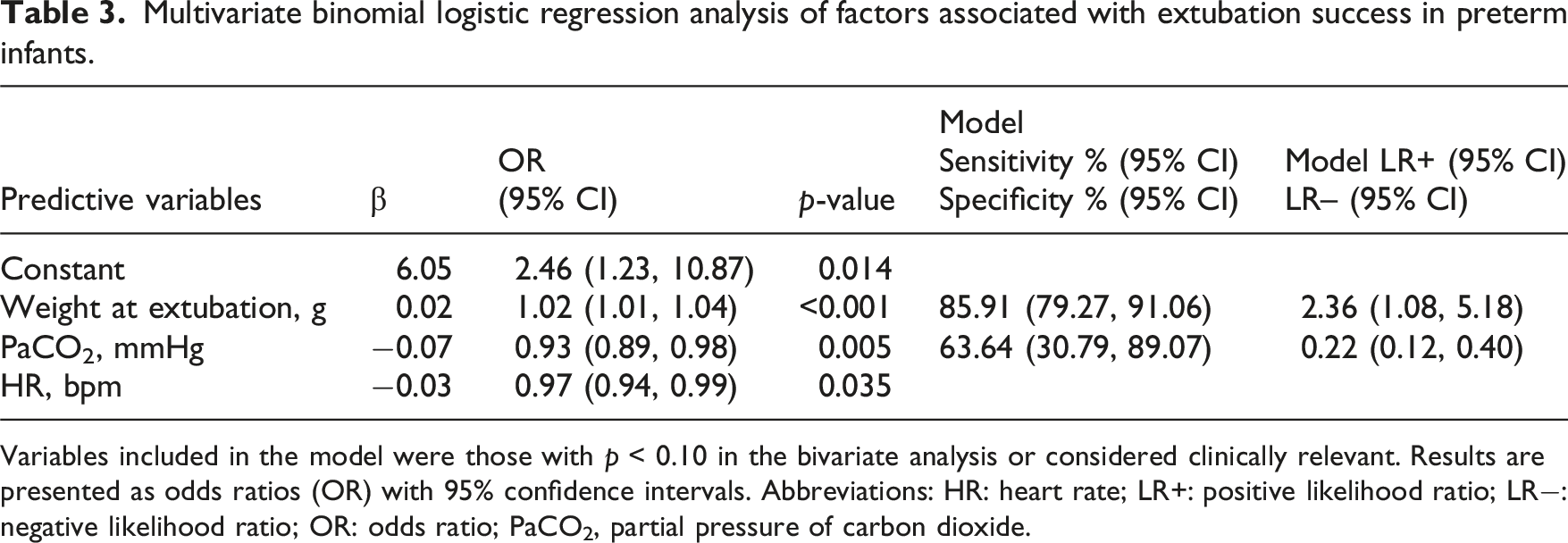
Variables included in the model were those with p < 0.10 in the bivariate analysis or considered clinically relevant. Results are presented as odds ratios (OR) with 95% confidence intervals. Abbreviations: HR: heart rate; LR+: positive likelihood ratio; LR−: negative likelihood ratio; OR: odds ratio; PaCO2, partial pressure of carbon dioxide.
Cutoff values for PaCO2 and heart rate to predict extubation success in preterm infants, derived from univariate discriminant analysis.
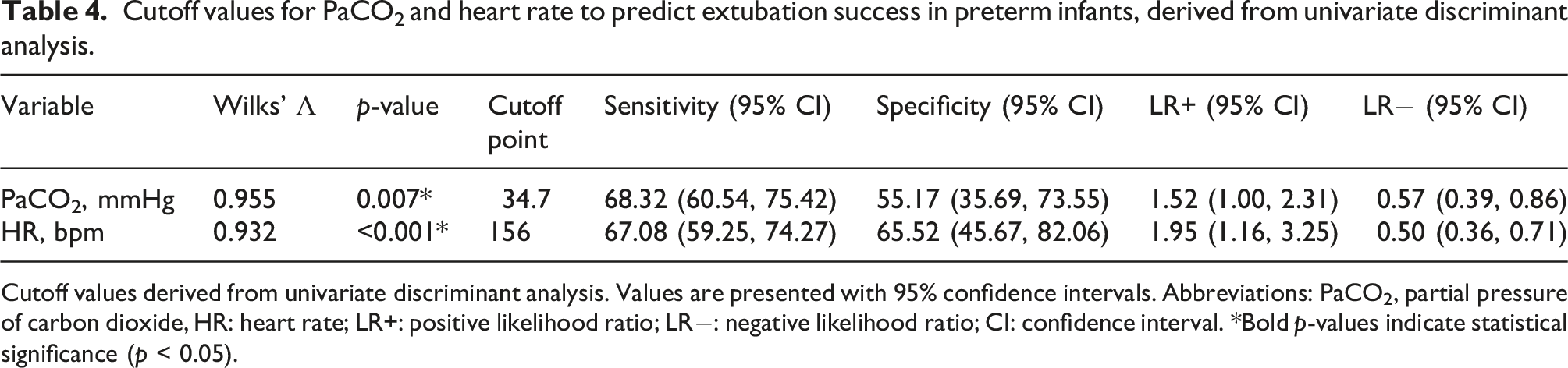
Cutoff values derived from univariate discriminant analysis. Values are presented with 95% confidence intervals. Abbreviations: PaCO2, partial pressure of carbon dioxide, HR: heart rate; LR+: positive likelihood ratio; LR−: negative likelihood ratio; CI: confidence interval. *Bold p-values indicate statistical significance (p < 0.05).
Discussion
This study, involving preterm newborns undergoing their first extubation attempt, identified weight at extubation, PaCO2 and HR as predictors of extubation success. Higher pre-extubation weight was associated with a greater probability of success. Previous studies corroborate this relationship, indicating that greater body weight before extubation reflects more advanced pulmonary maturity and a greater capacity to sustain spontaneous breathing after the procedure.4,8,9 A review has also emphasized that the optimal timing for extubation in preterm infants is influenced by variables such as weight. 7 Conversely, lower weight at extubation is associated with failure, particularly in extremely preterm newborns, in whom pulmonary immaturity, unstable respiratory drive, respiratory muscle weakness, and reduced energy reserves increase the risk of failure. 3 Therefore, body weight may serve as a clinically relevant marker of physiological readiness for extubation.
PaCO2 was identified as another predictive variable in the assessment of extubation readiness. Previous studies support this association, demonstrating that PaCO2 values within or close to the physiological range prior to extubation are associated with higher success rates.9,14,15 In our cohort, the cutoff value of 34.7 mmHg that best discriminated between success and failure is lower than the targets often used in permissive hypercapnia strategies, which may reach up to 60 mmHg. This difference may be explained by the characteristics of our population, composed exclusively of preterm infants undergoing their first elective extubation, with a short duration of mechanical ventilation (median of 4 days), a primary diagnosis of respiratory distress syndrome, and no history of bronchopulmonary dysplasia, prolonged oxygen therapy, or previous extubation failures.
In recent years, advances in neonatal care have led to shorter durations of mechanical ventilation and earlier extubation in preterm infants, aiming to minimize ventilator-associated lung injury. In this context, a lower PaCO2 cutoff may better represent infants extubated earlier in the disease course, as observed in our sample. In our cohort, lower pre-extubation PaCO2 was associated with extubation success, reinforcing the importance of adequate ventilatory status as a marker of readiness for ventilator withdrawal.
It is important to note that, although the cutoff value identified is low compared with permissive hypercapnia targets, the study population did not exhibit extreme hypocapnia, which is associated with lung injury, increased risk of bronchopulmonary dysplasia, and prolonged mechanical ventilation.16,17 In our multivariable model, higher PaCO2 levels were associated with reduced odds of extubation success, suggesting that even moderate elevations—within conventionally acceptable ranges—may indicate residual respiratory compromise in this specific population. Ventilatory strategies aimed at maintaining PaCO2 within a stable physiological range (typically 35−45 mmHg) and avoiding wide fluctuations have been associated with better clinical outcomes, 18 reinforcing that PaCO2 should be interpreted within a multidimensional assessment of extubation readiness rather than in isolation.
Similarly, HR was associated with extubation success in our study, although the literature has predominantly examined HRV rather than absolute HR values as predictors of outcomes. 19 In our analysis, HR was evaluated as a single measurement obtained within 24 h prior to the spontaneous breathing trial. We acknowledge that this time window may allow for physiological variation; however, it reflects the standardized approach to data collection in our setting and the parameters routinely available to guide clinical decision-making.
We identified an HR cutoff of 156 bpm, with modest sensitivity and specificity. HR is an easily monitored and routinely assessed parameter in the neonatal intensive care unit. The association between HR and extubation success in preterm newborns may be related to autonomic regulation and cardiorespiratory adaptation. Studies on HRV—a related but distinct parameter—indicate that it reflects autonomic nervous system modulation and the body’s ability to adapt to physiological and environmental changes. 20 Higher variability indicates better adaptation and more efficient autonomic control, whereas reduced variability may suggest impaired autonomic function and physiological instability. 21 Although our findings do not directly address variability, they suggest that absolute HR values, when interpreted alongside other clinical parameters, may contribute to a more comprehensive assessment of extubation readiness in preterm infants.
It is important to emphasize that these findings reflect the clinical context of preterm newborns undergoing their first extubation attempt, without prior failures or prolonged mechanical ventilation. Therefore, they may serve as a reference for similar populations but should not be extrapolated to infants with established bronchopulmonary dysplasia, multiple extubation failures, or prolonged ventilatory support, whose physiological responses and optimal readiness parameters may differ.
Taken together, these results highlight that extubation readiness in preterm newborns is influenced by anthropometric, ventilatory, and cardiovascular factors. Weight at extubation reflects maturity and physiological reserve, while PaCO2 and HR are simple, non-invasive, widely available, and easily interpretable parameters in routine clinical practice. Their measurement requires no additional resources beyond standard NICU monitoring and can be readily incorporated into daily assessments. Although the cutoff values identified for PaCO2 and HR showed modest sensitivity and specificity, they may still have practical relevance when interpreted within a broader clinical context. Being objective, rapidly obtainable, and easily interpretable, these variables can complement established indicators in guiding extubation timing. Incorporating them into a multidimensional and individualized assessment may help optimize decision-making, reduce the risk of failure, and improve outcomes in preterm infants. Nevertheless, given their moderate discriminatory performance, these cutoff values should be considered exploratory and require validation in independent prospective cohorts before routine clinical implementation.
Limitations
This study has several limitations. As a single-center retrospective analysis, the findings may not be generalizable to other neonatal units with different ventilation and weaning protocols. The main clinical diagnosis at admission was not systematically collected, limiting detailed characterization of the population. However, strict exclusion criteria reduced heterogeneity, resulting in a relatively homogeneous cohort of preterm infants with respiratory distress syndrome, without chronic lung disease, major malformations, or prolonged ventilation. In addition, the large number of excluded infants, particularly due to incomplete records and death before extubation, may have introduced selection and survivor bias, limiting the representativeness of the final cohort.
The presence of missing data, particularly for pre-extubation PaCO2, reduced the effective sample size for the multivariable analysis. As complete-case analysis was used without imputation, the possibility of selection bias cannot be excluded. The modest sensitivity and specificity of the PaCO2 and HR cutoff values indicate that these variables should not be used in isolation to guide extubation decisions. In addition, the wide confidence intervals observed for specificity estimates, particularly among infants with extubation failure, suggest limited precision of these measures and may reflect the relatively small size of the failure group. Additionally, HRV and markers of respiratory effort were not evaluated. Adverse events during the SBT were also not assessed, representing another limitation.
Additionally, the classification of infants who failed the spontaneous breathing test and therefore were not extubated into the unfavorable outcome group may have introduced classification bias. Although the sensitivity analysis excluding these infants yielded results similar to those of the primary analysis, the possibility of residual bias cannot be completely excluded. Furthermore, although we included clinically relevant variables routinely available in neonatal intensive care practice, other potential confounding factors may not have been captured and could have influenced the observed associations, representing an inherent limitation of the retrospective study design. Future studies should explore broader predictive models and validate these findings in diverse neonatal populations.
Conclusion
In preterm newborns undergoing their first extubation attempt, weight at extubation, PaCO2, and HR were independently associated with extubation success. These findings suggest that weight at extubation may be a useful clinical marker when assessing readiness for extubation.
PaCO2 and HR, although demonstrating modest discriminatory performance, may provide additional clinical insight when interpreted within the context of early extubation. In particular, the lower PaCO2 cutoff observed in this study suggests that commonly accepted thresholds may not fully reflect extubation readiness in this specific population.
These findings support the use of a multidimensional approach to extubation assessment, integrating anthropometric, ventilatory, and cardiovascular parameters. Future studies are needed to validate these findings and to further refine clinical criteria for extubation readiness in different neonatal populations.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.