
Abstract
Background
A controversy exists regarding the efficacy and safety of pigtail catheters (PC) versus classic straight chest tubes (SCT) for treating pneumothorax (PTX) in newborn infants. Our aim is to assess the efficacy and safety of PC compared to SCT in the treatment of PTX in newborn infants.
Methods
We systematically searched Medline, Embase, Cochrane, International Clinical Trials Registry Platform (ICTRP), WHO, ClinicalTrials.gov, and Google Scholar from database inception to December 2024 for randomized controlled trials, quasi control trials, and observational cohort studies. The assessed outcomes were complete radiological resolution, length of hospital stay, total days of placement, recurrence of PTX, drain dislodgment, and mortality.
Results
We included 3 observational studies (138 infants). Regarding the complete radiological resolution of PTX, there was no significant difference between PC and SCT [OR: 2.32; 95% CI (0.29–16.95)]. The length of hospital stay was significantly less in patients treated with PC compared to SCT [MD -14.98; 95% CI (−28.09, −1.87)] while other outcomes including total days of tube placement, recurrence of PTX, drain dislodgment, and mortality were not significantly different between the two interventions.
Conclusions
Our meta-analysis found no statistically significant difference in complete radiological resolution of neonatal PTX between PC and SCT. A statistically significant shorter length of hospital stay was observed with PC; however, this is heavily confounded by multiple clinical factors. Well-designed randomized controlled trials are highly recommended to establish the efficacy and safety of PCs compared to classic SCT for PTX drainage in neonates.
Registration
The protocol for the present systematic review was registered online with PROSPERO, the international prospective register of systematic reviews (CRD42025630790).
What is known?
• Tension pneumothorax is a life-threatening condition requiring prompt drainage. • Two types of draining catheters are available: the traditional straight chest tube and the newly introduced pigtail catheter. However, the optimal choice for neonates remains debatable.
What is new?
• This is the first systematic review evaluating PC versus SCT for neonatal PTX. • No statistically significant difference in radiological resolution was observed; a shorter hospital stay was noted with PC, though this finding is confounded and should be interpreted with caution.
Introduction
Pneumothorax (PTX) is a life-threatening condition that occurs more frequently in newborn infants than in any other age group, with an incidence rate of 0.5–2% among all newborns 1 and up to 9% in very low birth weight infants. 2 In the post-surfactant era, the most common risk factors for PTX in neonates are prematurity, positive pressure ventilation during resuscitation and mechanical ventilation. 1 Recent studies reveal neonatal PTX mortality rates of 12% to 20%. Preterm neonates are particularly vulnerable, as they are more likely to experience recurrent PTX and have a higher mortality rate.3,4 A relatively high mortality rate among neonates with PTX highlights the need to refine and standardize measures for the urgent management of this critical condition.
Management of neonatal PTX includes conservative or invasive treatment such as chest tube drainage and needle aspiration. 5 Other methods, such as nitrogen washout, have been phased out. 6 In contrast to adults, chest tube drainage is the invasive management of choice for neonates. The choice between a pigtail catheter (PC) or a classic straight chest tube (SCT) depends on the skills and preferences of the medical staff in charge of the neonatal intensive care unit (NICU).5,7 Nevertheless, the procedure for inserting an SCT drain is associated with various complications, including recurrence of PTX, hemothorax, subcutaneous emphysema, localized infection, organ laceration, dislodgment, malfunction, scarring of the chest wall, prolonged mechanical ventilation, extended hospital stays, and even mortality. 8
Pigtail chest drains have emerged as an alternative to classic SCT for the drainage of PTX. As a coiled, single-lumen, flexible, polyurethane catheter that ranges in size from 5 to 12 French gauge, its design facilitates easier insertion and positioning without the need for an incision. 9 Beyond the device characteristics, the procedural differences between both modalities are clinically relevant and may influence outcomes. SCT insertion typically requires blunt dissection through the chest wall and a formal incision, and it is included in neonatal training curricula. In contrast, pigtail catheter insertion uses a modified Seldinger technique, requiring a distinct skill set that may not be uniformly available in all NICUs. International guidelines report that small-bore wire-guided (pigtail) chest drains are better tolerated and safer in the treatment of PTX; however, assessing the effectiveness of this approach requires further studies of NICU infants. 8
There is a paucity of data regarding the efficacy and safety of PC compared to traditional SCT in therapy of PTX in newborn infants. Therefore, our meta-analysis was conducted to assess the efficacy and safety of PC in comparison to SCT for treating PTX in this population.
Materials and methods
The study was conducted in concordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 10 Guidelines for the Cochrane Neonatal Review Group were followed. 11 Our meta-analysis was excused from institutional review board approval as it is based on accessible and freely available data.
The protocol for the present systematic review was registered online with PROSPERO, the international prospective register of systematic reviews (CRD42025630790), prior to the start of the literature review.
Search strategy and selection criteria
We systematically searched Medline, Embase, Cochrane, International Clinical Trials Registry Platform (ICTRP), WHO, ClinicalTrials.gov, and Google Scholar for randomized controlled trials (RCTs), quasi control trials, and observational cohort studies published from database inception to December 2024. Searches were independently conducted by (M.E.). The search strategy incorporated both free-text keywords and controlled vocabulary terms (e.g., MeSH in Medline, Emtree in Embase, and Subject Headings) to ensure a thorough retrieval of studies. Boolean operators (AND, OR) were used to combine terms related to the population (neonates, preterm infants), condition (pneumothorax), intervention (pigtail catheter), and comparator (classic chest tube/intercostal drain) (supplementary file). The search was not restricted by publication date, language, or location of the study. A supplemental manual search was done in the references of included studies and by looking at related or cited articles in PubMed and Google Scholar.
The abstracts obtained from the initial search, after removing duplicates, were screened to identify potentially eligible studies. Full texts were obtained and independently assessed by two authors (L.S. and I.N.) for the predefined eligibility criteria. Studies were included if they were RCTs, quasi control trials or cohort studies (prospective or retrospective) that recruited newborns that underwent insertion of either a PC or a classic SCT after diagnosis of PTX. We excluded studies in which insertion of draining catheter was for indications other than PTX, such as intraoperative collection, hemothorax, chylothorax, and pleural effusion, and those that included other populations rather than neonates.
Data extraction
Two authors (L.S and I.N) independently extracted data from the included studies using an Excel spread sheet and a data extraction form designed for this review. Disagreements among the reviewers were settled through discussion.
Outcomes
Our primary outcome was complete radiological resolution of the PTX after drainage (success rate) while secondary outcomes were total days with drains, PTX recurrence, chest tube insertion complications such as hemothorax, local infection, and organ laceration, subcutaneous emphysema and drain dislodgement/malfunction, need for invasive ventilation, length of hospital stay, and mortality.
Risk of bias and quality assessment
Included articles were assessed by two independent authors (N.M and I.N) for risk of bias (ROB) at the outcome level using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) assessment tool Version 2.12,13 This tool evaluates seven possible sources of bias and gives a final overall assessment which varies from low to serious risk of bias. Given the retrospective design of all included studies, all outcomes are vulnerable to the same risk of bias (e.g., patient selection bias and heterogeneity of gestational age). Disagreements were resolved through discussion with a third author (G.S-G).
Similarly, two authors evaluated the certainty of the evidence using the GRADE approach, which considers factors such as the risk of bias, inconsistency, indirectness, imprecision, and publication bias. 14
Statistical analysis
Meta-analysis of pooled data was conducted using Review Manager 5.4.1.3 (Cochrane Collaboration, Nordic Cochrane Centre, Copenhagen, Denmark). We reported odds ratios (OR) with 95% confidence intervals (CIs) for categorical data and mean differences (MD) with 95% confidence intervals (CIs) for continuous data. Heterogeneity among studies was assessed using I2 statistic, and values were interpreted following the guidelines of Cochrane Handbook: 0% to 40%—might not be important, 30% to 60%—may represent moderate heterogeneity, 50% to 90%—may represent substantial heterogeneity, and 75% to 100%—considerable heterogeneity. All analyses were performed using random effects models, and two-sided P values less than 0.05 were deemed statistically significant. For outcomes with zero events in one study arm, Review Manager continuity corrections were automatically applied according to standard Cochrane methodology. Sensitivity analyses were not performed due to the low number of available studies. Assessing for publication bias using funnel plots or Egger’s test was not feasible, as a minimum of 10 studies per outcome is recommended.
Results
The literature search found 382 potentially relevant citations, of which 172 were duplicates, and 210 were screened. After abstract screening and full text selection, 3 observational studies were finally included in the systematic review and meta-analysis. The flow diagram of the study selection process is depicted in Figure 1. Flow diagram of literature search and study selection.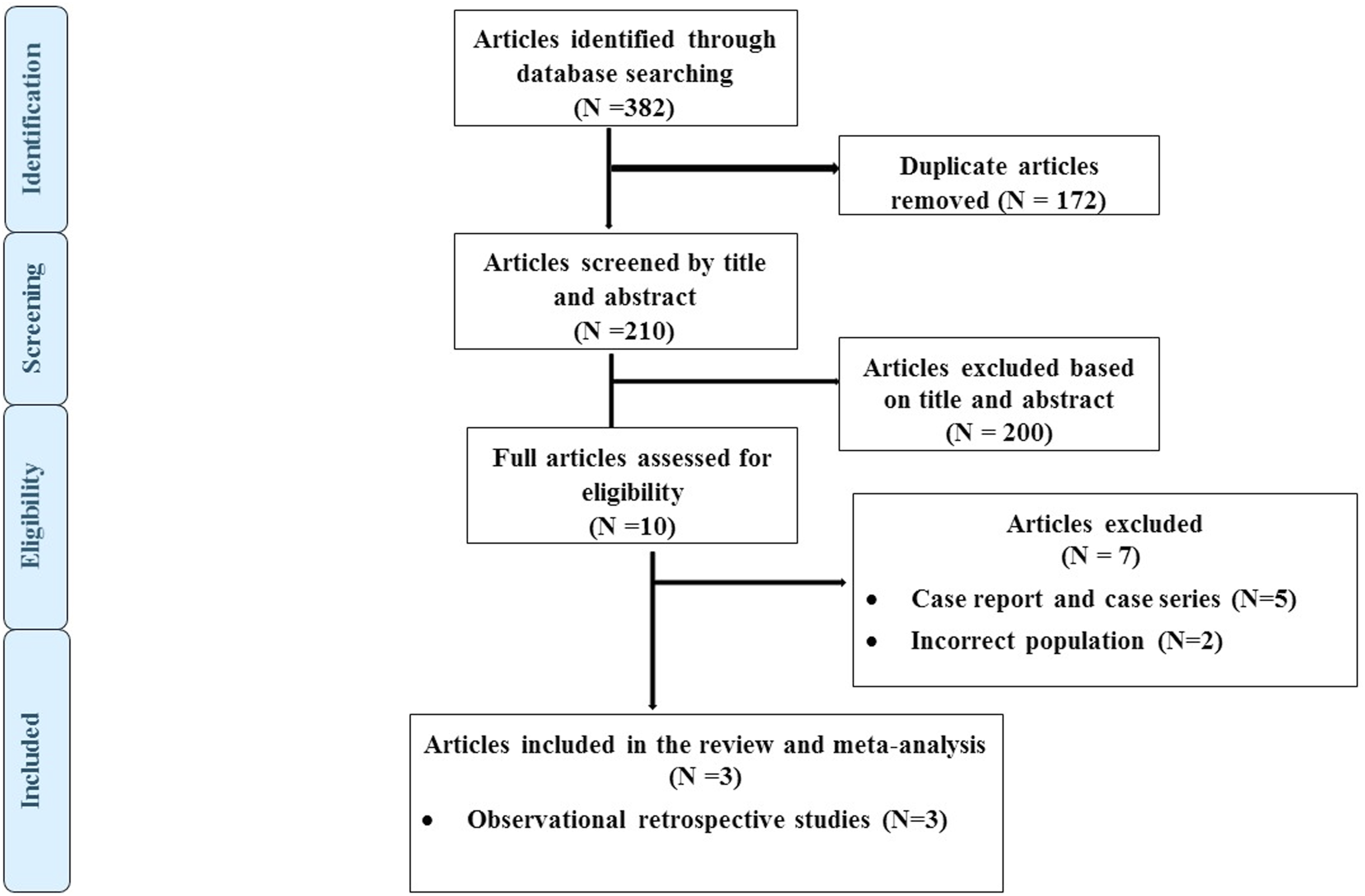
Characteristics of included studies
Characteristics of included studies.
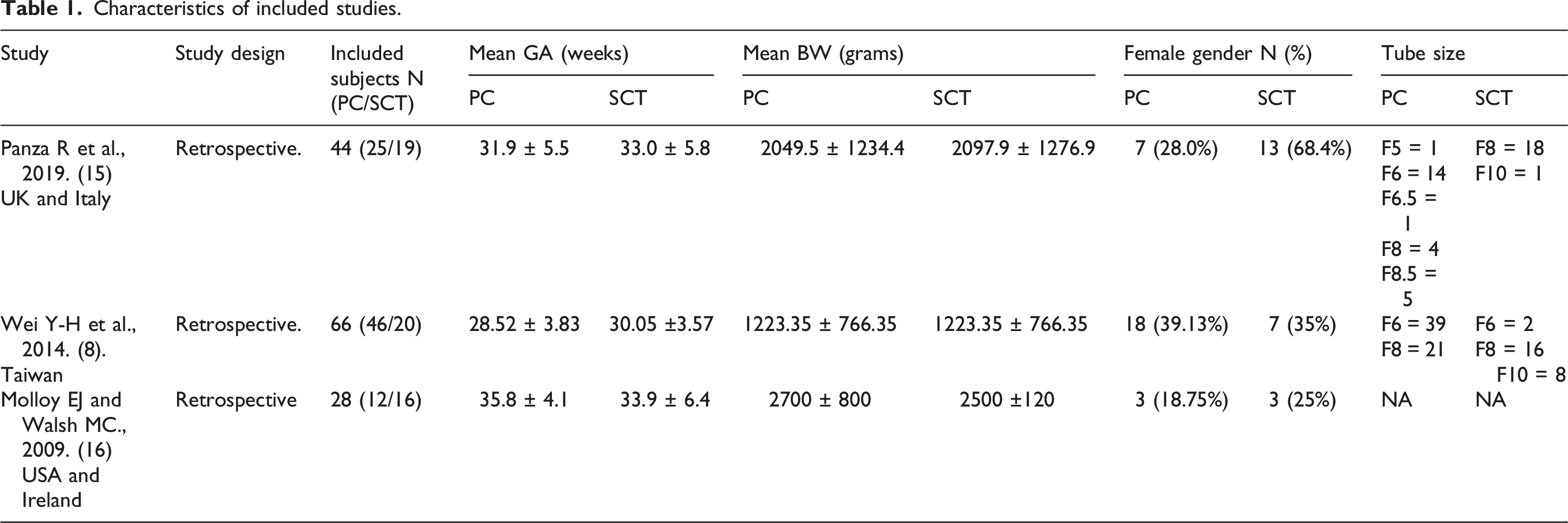
Regarding outcomes, all three studies reported total days of catheter placement, PTX recurrence, and hospital stay, and at least two studies8,15 reported mortality, complete radiological resolution, drain dislodgement, and duration of mechanical ventilation.
Risk of bias assessment
The assessment of risk of bias using Risk of Bias In Non-randomized Studies – of Interventions, Version 2 (ROBINS-I V2).
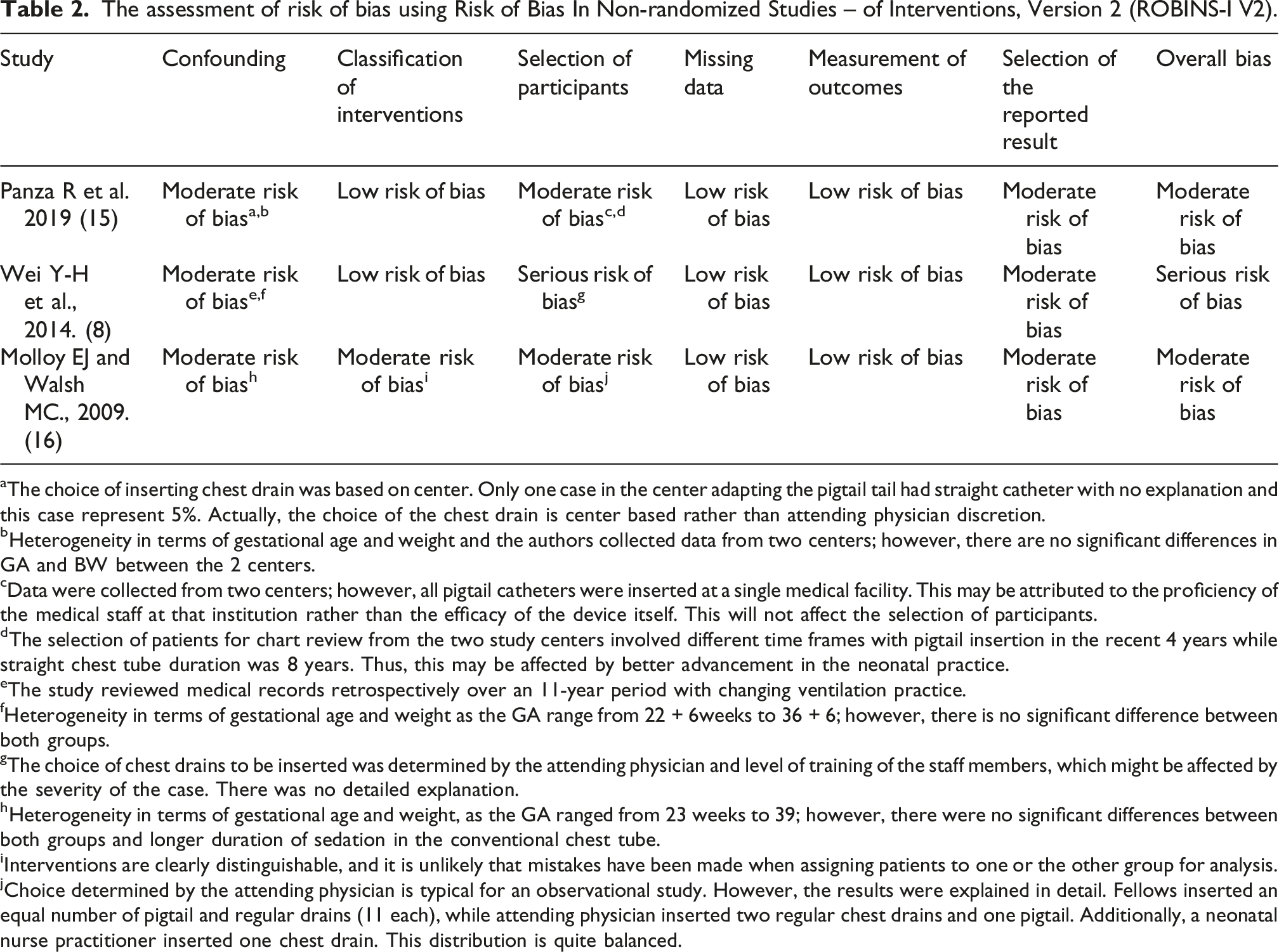
aThe choice of inserting chest drain was based on center. Only one case in the center adapting the pigtail tail had straight catheter with no explanation and this case represent 5%. Actually, the choice of the chest drain is center based rather than attending physician discretion.
bHeterogeneity in terms of gestational age and weight and the authors collected data from two centers; however, there are no significant differences in GA and BW between the 2 centers.
cData were collected from two centers; however, all pigtail catheters were inserted at a single medical facility. This may be attributed to the proficiency of the medical staff at that institution rather than the efficacy of the device itself. This will not affect the selection of participants.
dThe selection of patients for chart review from the two study centers involved different time frames with pigtail insertion in the recent 4 years while straight chest tube duration was 8 years. Thus, this may be affected by better advancement in the neonatal practice.
eThe study reviewed medical records retrospectively over an 11-year period with changing ventilation practice.
fHeterogeneity in terms of gestational age and weight as the GA range from 22 + 6weeks to 36 + 6; however, there is no significant difference between both groups.
gThe choice of chest drains to be inserted was determined by the attending physician and level of training of the staff members, which might be affected by the severity of the case. There was no detailed explanation.
hHeterogeneity in terms of gestational age and weight, as the GA ranged from 23 weeks to 39; however, there were no significant differences between both groups and longer duration of sedation in the conventional chest tube.
iInterventions are clearly distinguishable, and it is unlikely that mistakes have been made when assigning patients to one or the other group for analysis.
jChoice determined by the attending physician is typical for an observational study. However, the results were explained in detail. Fellows inserted an equal number of pigtail and regular drains (11 each), while attending physician inserted two regular chest drains and one pigtail. Additionally, a neonatal nurse practitioner inserted one chest drain. This distribution is quite balanced.
Primary outcome
Pooled analyses of 2 observational studies8,15 (N = 110) showed no significant differences between PC and SCT in complete radiological resolution of PTX (OR: 2.32; 95% CI 0.29–18.95 I2 = 65%) (Figure 2). Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of complete radiological resolution.
Secondary outcomes
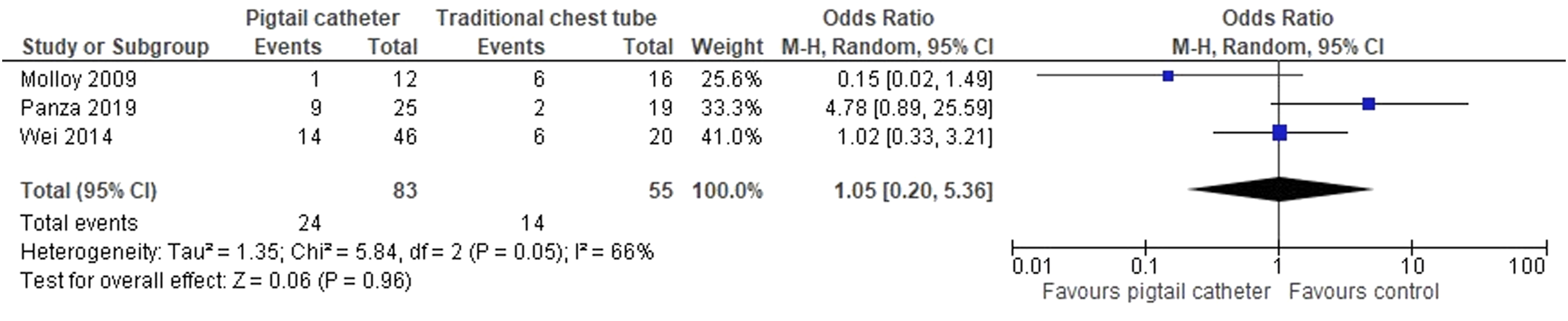
Pooled analyses of all the three studies (N = 138) included in our meta-analysis for the length of hospital stay were significantly less in patients treated by PC compared to SCT (MD -14.98; 95% CI -28.09, −1.87 I2 = 0%) (Figure 3). There were no statistically significant differences between the 2 groups for other pre-specified secondary outcomes (total days of placement, recurrence of PTX, mortality, drain dislodgment, and duration of mechanical ventilation) (Figures 4,5,6,7,8) Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of length of hospital stay. Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of total days of chest drain placement. Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of recurrence of pneumothorax. Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of mortality. Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of drain dislodgement. Forest plot for pigtail catheter versus straight chest drain in neonates for the outcome of duration of mechanical ventilation.




Certainty of evidence (GRADE analysis)
Summary of GRADE assessment.
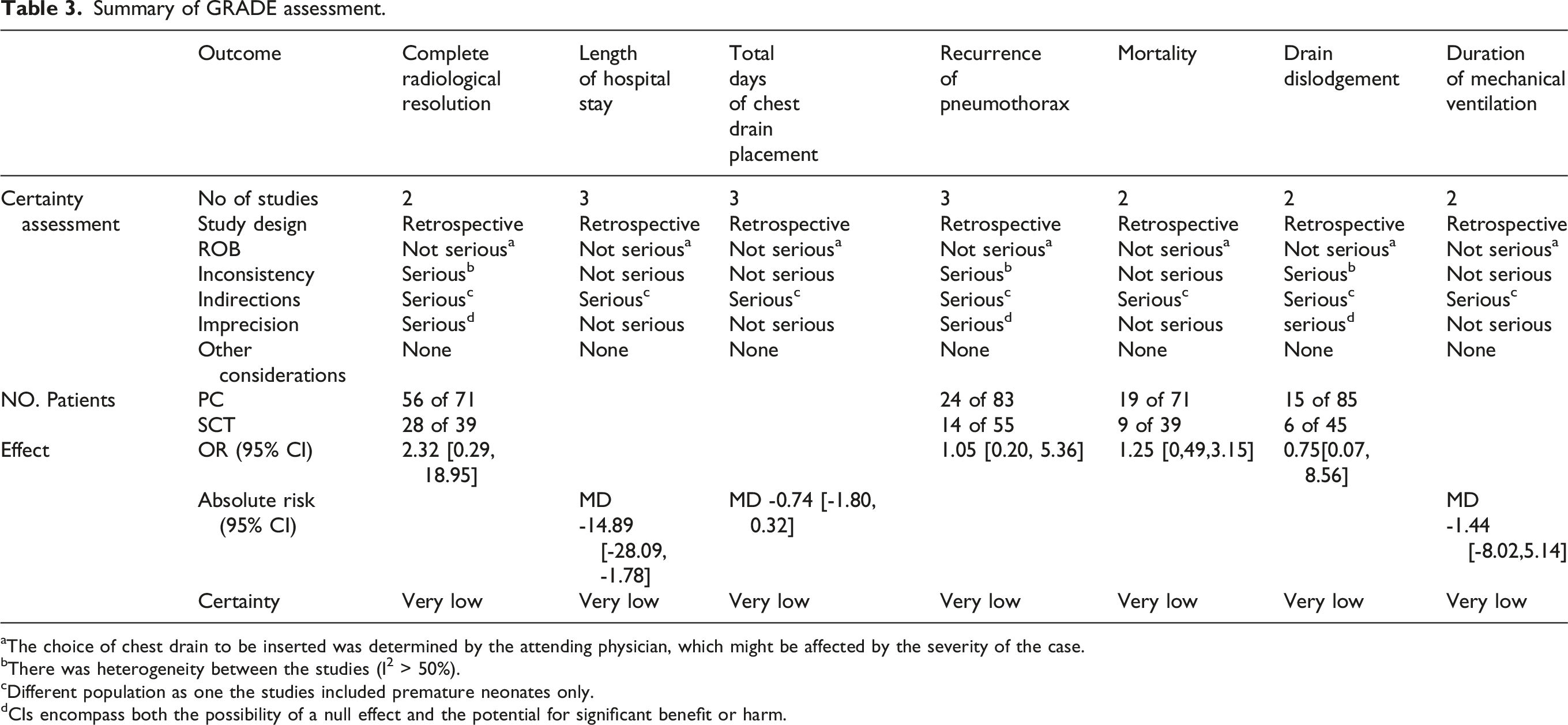
aThe choice of chest drain to be inserted was determined by the attending physician, which might be affected by the severity of the case.
bThere was heterogeneity between the studies (I2 > 50%).
cDifferent population as one the studies included premature neonates only.
dCIs encompass both the possibility of a null effect and the potential for significant benefit or harm.
Discussion
Although the conventional SCT has historically been the most frequently utilized modality for patients with PTX for several decades, recent literature has indicated a growing advocacy among various authors for the more systematic implementation of PC in the management of pneumothorax across a spectrum of severity levels, particularly in neonatal and pediatric cohorts.8,15,17 This shift may be attributed to the minimal air viscosity, making a small-bore PC adequate for most typical cases of PTX, while the traditional SCT can still be reserved for refractory PTX. 18 The advantages of PC include its smaller size, minimal opening, better patient tolerance, cost-effectiveness, and reduced pain; hence, it is considered an acceptable management option for PTX in pediatric patients.16,19 However, a notable drawback of PC is the lower airflow rate. 20 Therefore, our meta-analysis aims to address this debate: which treatment is better for newborns PC drain or SCT for the management of PTX. Despite the growing body of knowledge, evidence regarding neonates remains extremely limited including only three small, retrospective observational studies (total n = 138), with a lack of RCTs. This renders most of our pooled analyses considerably underpowered.
A significant limitation shared by all three included studies is that the drainage modality selection (PC vs SCT) was determined by the attending clinician; hence, it was likely influenced by perceived initial illness severity, pneumothorax size, patient weight, gestational age, and operator training and preference. This introduces a systematic bias in the pooled analysis and substantially limits causal interpretation of the findings. For example, clinicians may have preferentially selected SCT for sicker cases, potentially biasing outcomes in favor of PC. Furthermore, all included studies, being retrospective in design, are vulnerable to unadjusted and unmeasured confounders, including gestational age, severity of respiratory disease, and ventilatory support level. These factors may have substantially biased pooled estimates.
The three included studies exhibited significant clinical heterogeneity. Variability in gestational age (23 to 40 weeks) and birth weight (800 to 3500 g) indicated markedly different patient populations. Catheter sizes varied (5–8.5 French for PC; 6–10 French for SCT), and NICU practices differed across involved hospitals. Furthermore, two studies15,16 collected data from two centers, each potentially having varying management protocols. This clinical heterogeneity may have contributed to the variability in treatment effects and limits the generalizability of the pooled results.
Our systematic review and meta-analysis demonstrated that managing PTX with PC, compared to traditional SCT, did not result in significant differences in the rates of radiological resolution following drainage. We found a shorter duration of hospitalization for patients treated with PC, with no notable differences in other assessed efficacy and safety outcomes.
Our meta-analysis showed no statistically significant difference in complete radiological resolution of neonatal PTX between PC and SCT (success rate). This outcome was reported in two retrospective cohort trials,8,15 while Panza et al. 15 found that the success rate was significantly higher in neonates treated by PC, our pooled analysis did not find this difference; this may be attributed to sample size or study population. Also, Lawlessand his colleagues treated 16 neonates with PCs for PTX and pneumomediastinum. They demonstrated that the PC drain provided a safe, effective alternative to standard tube thoracotomy. 21
In addition, the pooled analysis of all included studies revealed that the length of hospital stay was significantly shorter in neonates who had a PC drain compared to those who had a SCT.8,15,16 Despite this statistical difference, this result should be interpreted cautiously. Within a clinical context, the length of NICU stay is a highly confounded outcome that may be influenced by multiple factors beyond the method of PTX management, including prematurity, birth weight, severity and nature of the underlying lung pathology, feeding challenges, or sepsis. Furthermore, the wide confidence interval (approximately 2 to 28 days) reflects substantial imprecision. In agreement with our findings, another meta-analysis in the pediatric population, including 11 trials, found that patients treated with a PC had a significantly shorter duration of hospital stay compared to those treated with a straight traditional chest tube for different types of PTXs. 17 In contrast, Ricky Le and colleagues 22 conducted a systematic review of adult patients with traumatic PTX to compare PC and SCT methods. Their analysis included 261 cases from two studies23,24 and found no significant difference in the duration of hospital stay between the two management approaches. Both our meta-analysis and their analysis included non-randomized studies that are susceptible to selection bias, as attending physicians may prefer to use PC for less severe cases.
We found that the recurrence rate of PTX was comparable between the patients treated by PC drain and those treated by a SCT. In concordance with our findings, Chang et al. 17 reported that a pooled analysis of four trials of spontaneous PTX in pediatric populations did not find any difference in PTX recurrence in either group.25–28
In our meta-analysis, the total duration of chest drain placement was not significantly different between the two groups in the pooled analysis of all three studies; however, there was a trend for less total duration of tube placement favoring PC drain (95% CI: −1.80–0.32). Similar to our findings, the meta-analysis by Ricky Le et al. (2024) 22 reported no significant difference in the duration of tube placement between the two approaches in adult patients with traumatic PTX. In contrast to our results, Chang et al. reported that the PC group had a significantly shorter drainage duration than the SCT group. 17
Furthermore, our meta-analysis revealed no significant difference in drain dislodgment with either approach to management. Moreover, no significant difference in either mortality or duration of mechanical ventilation in the two groups of our study was found.
There was insufficient data to perform a meta-analysis on analgesia usage, intervention time, and cost of utilization in both interventions, the need for surgical management, exact oxygen requirements, especially in preterm infants, complications related to chest tube insertion like hemothorax and infection.
To the best of our knowledge, this is the first meta-analysis evaluating the optimal drain type for managing PTX in neonates. We acknowledge the following limitations: (1) the total sample size of 138 neonates across only three retrospective studies represents a critically limited evidence; (2) all three included studies have considerable ROB; (3) significant clinical heterogeneity exists across studies; (4) lack of long-term follow-up; (5) the small number of included studies precluded formal subgroup or sensitivity analyses to explore sources of heterogeneity; (6) publication bias could not be formally assessed due to the insufficient number of studies per outcome (n < 10); and (7) unmeasured confounders may substantially bias pooled estimates. Consequently, the results should be interpreted with considerable caution, necessitating the urgent conduction of a larger, multicenter, adequately powered randomized controlled trials. However, performing future RCTs remain challenging partly due to the urgent nature of interventions for alleviating tension PTX, which often leave insufficient time to obtain parental consent for study recruitment, alongside, the limited training that medical staff receive in the use of PCs, unlike the more commonly performed straight chest tube insertion. Furthermore, future RCTs should consider controlling for confounders and heterogonous nature of patient characteristics regarding prematurity and underlying lung pathology.
Conclusion
Our meta-analysis found that there were no differences regarding the radiological resolution of neonatal PTX treated with PCs and classic STCs, which could not be interpreted as evidence of equivalence, given the small sample sizes, wide confidence intervals, and underpowered analyses. The shorter length of hospital stays apparently favoring PC use was likely confounded by multiple clinical factors, including gestational age, severity of underlying lung disease, and physician discretion. In the context of the extremely limited available evidence, all findings should be labeled as preliminary and hypothesis-generating only. An appropriately powered RCT with rigorous methodology is urgently required to establish the efficacy and safety of PCs compared to classic SCTs for PTX drainage in neonates.
Footnotes
Authors’ contributions
I.N., N.M., G.S.-G., L.S., and M.E. conceptualized and designed this meta-analysis. M.E. designed the search strategy and conducted the search. L.S. and I.N. screened and assessed the selected articles for eligibility. L.S. and I.N. extracted the data. N.M., I.N., and G.S.-G. evaluated the included studies for risk of bias. G.S.-G. ran the statistical analysis. L.S. and I.N. wrote the manuscript. All authors reviewed, revised, and approved the final version of the manuscript as submitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Registration
The protocol for the present systematic review was registered online with PROSPERO, the international prospective register of systematic reviews (CRD42025630790).