
Abstract
Neonatal parenteral nutrition (PN) remains a cornerstone of care for preterm infants and for selected term infants when enteral feeding is not possible or is clearly insufficient. In day-to-day neonatal practice, decisions about when to initiate PN, how quickly to advance macronutrient delivery, which lipid emulsion to use, and how closely to monitor biochemical tolerance are guided by several major documents rather than by a single universally adopted standard. This expert narrative review compares the principal recommendations from ASPEN, NICE, and the ESPGHAN/ESPEN/ESPR/CSPEN pediatric PN guideline series, and interprets them alongside contemporary trials, systematic reviews, meta-analyses, and clinically relevant safety guidance. Across these sources, there is broad agreement on the essentials: start PN early when clearly indicated, introduce amino acids and lipids without unnecessary delay, individualize glucose delivery according to tolerance, provide vitamins and trace elements early, and monitor closely for electrolyte disturbances and catheter- or liver-related complications. The remaining areas of disagreement are narrower but important at the bedside, particularly the upper limits of amino acid provision, timing of PN in critically ill term infants, routine use of standardized versus individualized formulations, interpretation of triglyceride concentrations, and the clinical role of mixed-oil or fish-oil-containing lipid emulsions. A practical reading of the literature suggests that the most workable neonatal PN pathway borrows the operational detail of NICE, the physiologic and subgroup-specific framework of the European guidance, and the evidentiary caution emphasized by ASPEN.
Keywords
Introduction
Parenteral nutrition is one of the defining supportive therapies of modern neonatal intensive care. Its importance is greatest in infants who are born too early, too sick, or too unstable to sustain growth and metabolic adaptation through enteral feeds alone. Yet neonatal PN is never simply a matter of prescribing calories and protein. It sits at the intersection of fluid restriction, organ immaturity, postnatal metabolic transition, vascular access, and the very real risk of biochemical complications.
Over the past decade, guidance has become more detailed, but not fully uniform. ASPEN published a focused guideline for PN in preterm infants in 2023, NICE issued a dedicated neonatal PN guideline in 2020, and the ESPGHAN/ESPEN/ESPR/CSPEN collaboration produced a comprehensive pediatric PN guideline series in 2018 with separate papers on energy, amino acids, lipids, carbohydrates, fluids and electrolytes, vitamins, trace elements, venous access, and complications.1–12 These documents share many core principles, but they differ in tone and emphasis. NICE tends to be operational and bedside-oriented, ASPEN is more conservative and explicitly evidence-weighted, and the European papers are often more physiologic and subgroup-specific in their recommendations.
The research gap is therefore not the absence of guidelines, but the lack of a single clinically usable synthesis that explains how these guidelines should be interpreted together. Existing documents often answer different questions: some prioritize bedside prescribing, some emphasize physiologic principles, and some restrict recommendations to areas with stronger outcome evidence. This creates uncertainty in common NICU decisions, such as how aggressively to advance amino acids in extremely low birth weight (ELBW) infants, how to interpret triglyceride levels, and when term critically ill neonates should receive or defer PN. This review was written as a practical expert narrative synthesis for clinicians and authors who need a usable, manuscript-style summary of neonatal PN. The aim is not only to list recommendations, but to show where the major guidelines truly converge, where they diverge, and how contemporary evidence helps explain those differences. The clinical goal is framed beyond biochemical tolerance alone: PN strategies should ultimately support adequate postnatal growth, head growth, avoidance of cumulative protein-energy deficits, and longer-term neurodevelopmental outcomes, particularly in ELBW and other high-risk infants. 13
Methods
This manuscript is an expert narrative comparative review rather than a formal systematic or scoping review. The principal guidance documents from ASPEN, NICE, and ESPGHAN/ESPEN/ESPR/CSPEN were selected a priori as the core framework because they are the major contemporary international references used for neonatal PN practice.1–12 The review question was practical rather than population-intervention-comparator-outcome driven: how should clinicians interpret and reconcile these major guideline frameworks for bedside neonatal PN prescribing?
To improve transparency, the evidence base was assembled using targeted literature searches in PubMed, guideline repositories, and reference lists of major guidance documents. Search concepts included combinations of neonate, preterm infant, extremely low birth weight, parenteral nutrition, amino acids, lipid emulsion, glucose, triglycerides, cholestasis, micronutrients, standardized parenteral nutrition, venous access, photoprotection, and carnitine. Priority was given to neonatal guidelines, randomized trials, Cochrane reviews, systematic reviews, meta-analyses, and large or practice-informing observational or survey studies. Adult PN literature was not used unless it directly informed a neonatal safety or implementation issue. Studies and documents were included when they addressed neonatal or pediatric PN recommendations, neonatal PN outcomes, substrate dosing, PN-related complications, monitoring, vascular access, standardization, or clinically important implementation controversies. Reports were excluded when they were unrelated to neonatal PN, focused exclusively on adult practice without neonatal relevance, duplicated data already represented in a higher-level synthesis, or were non-data opinion pieces without a clear link to neonatal practice. No formal Cochrane risk-of-bias assessment or meta-analysis was performed because this was not designed as a systematic review. Instead, evidence was weighted pragmatically: guideline recommendations, Cochrane reviews, randomized trials, and meta-analyses were given greatest weight for efficacy and safety; observational studies and surveys were used mainly to describe implementation gaps, practice variability, and unresolved controversies.
Comparison of key operational recommendations across major neonatal PN guidance documents.
Comparison of major macronutrient recommendations in neonatal PN.
Micronutrients, minerals, and monitoring: practical comparison.
When to start neonatal parenteral nutrition
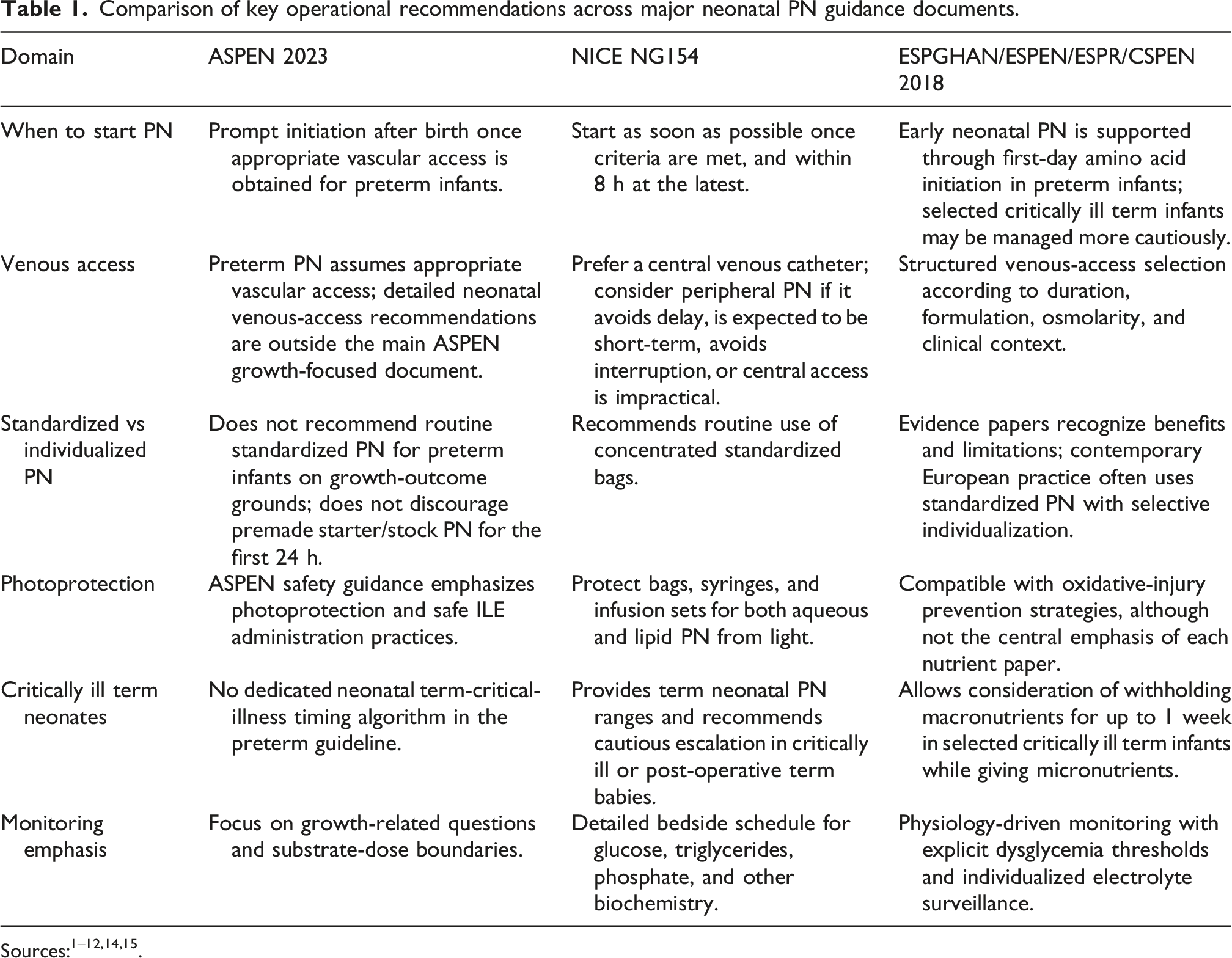
NICE provides the most explicit operational advice on when neonatal PN should begin. For babies who meet criteria for PN, it recommends starting as soon as possible, no later than 8 h, and defines feed-interruption thresholds that should prompt PN in both preterm and term infants. 2 ASPEN supports similarly prompt initiation after birth once appropriate vascular access is available, although its document is directed specifically at preterm infants. 1 The European guidance is also aligned with early nutritional support, but it tends to frame the issue in physiologic rather than workflow terms.3–12 Taken together, the three approaches support an early-start strategy whenever enteral adequacy is unlikely. These operational differences are summarized in Table 1.
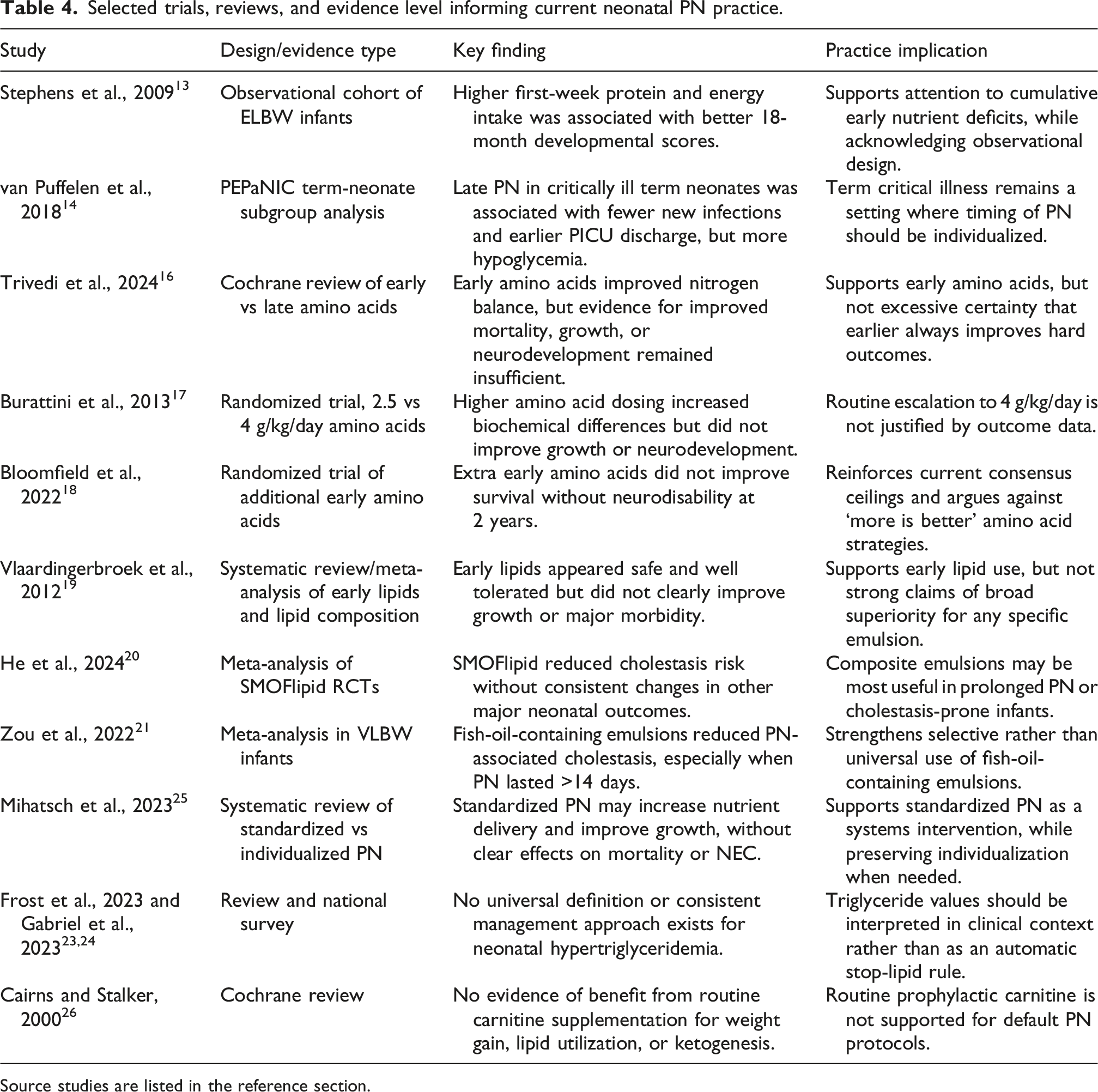
The area that remains genuinely controversial is the critically ill term neonate. NICE takes a distinctly neonatal position and provides nutritional ranges for term infants receiving PN, including those who are critically ill or post-operative, while advising clinicians to stay at the lower end of the energy range when appropriate. 2 The European amino acid guidance is more cautious and allows consideration of withholding PN, particularly amino acids, during the acute phase of critical illness. 5 That caution is supported by the neonatal subgroup analysis of the PEPaNIC trial. In this preplanned subgroup of 209 term neonates enrolled before 4 weeks of age, late PN, started on day 8 rather than on admission, was associated with fewer new infections and earlier discharge from the pediatric intensive care unit, although hypoglycemia was more frequent. 14 The practical implication is that early PN remains standard for preterm infants and many surgical or feed-intolerant neonates, but the acutely critically ill term infant still requires individualized judgment rather than automatic protocolized escalation.
Energy and glucose
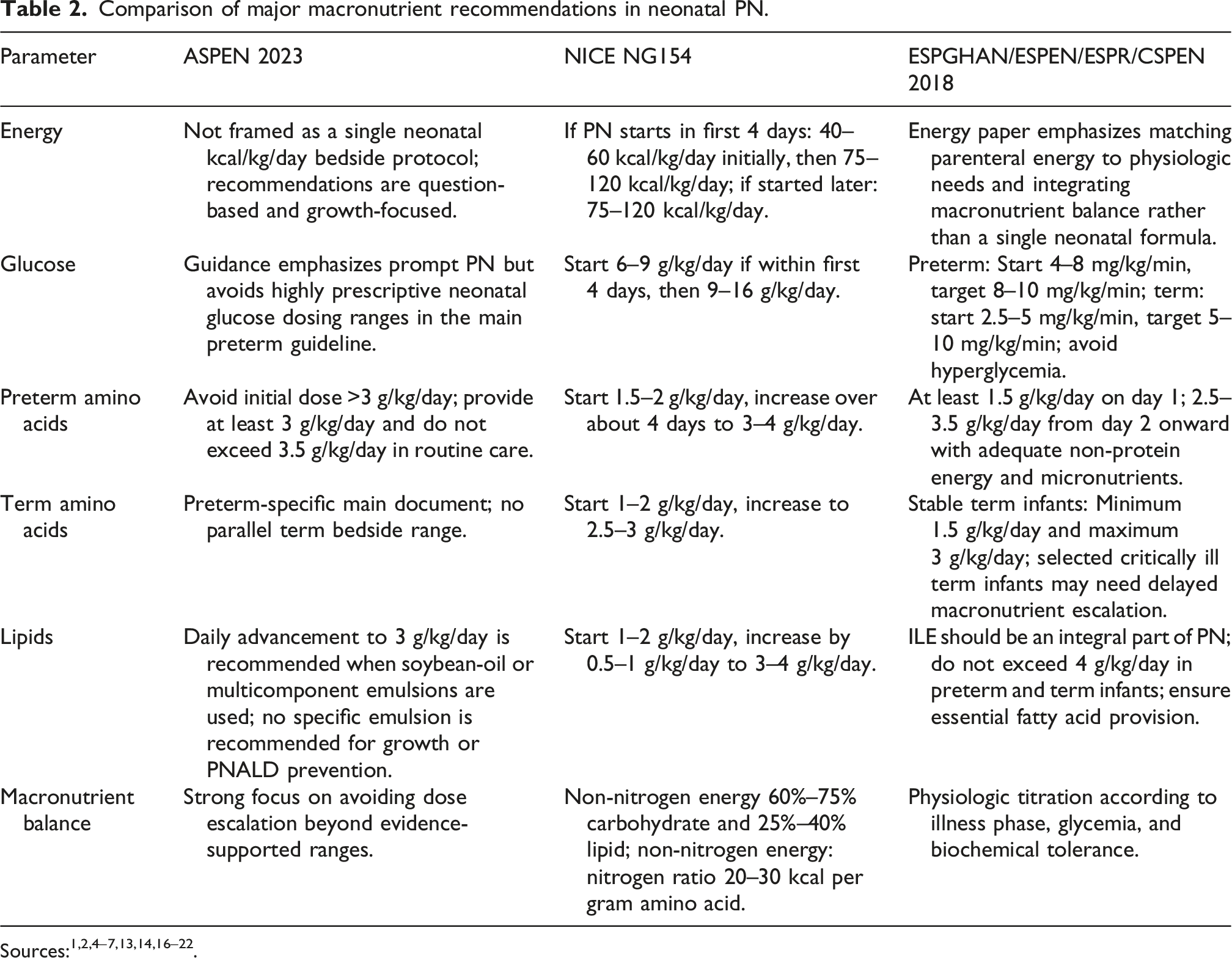
Energy prescription in neonatal PN is constrained by fluid allowance, substrate tolerance, and the infant’s rapidly changing metabolic state after birth. NICE recommends that when PN is started within the first 4 postnatal days, total parenteral energy should begin at 40–60 kcal/kg/day and then increase over roughly 4 days to 75–120 kcal/kg/day; if PN starts after day 4, the maintenance range is 75–120 kcal/kg/day from the outset. 2 These ranges are practical because they are easy to translate into standardized formulations and everyday NICU prescribing. The main numerical ranges across guidelines are compared in Table 2. The European carbohydrate guidance approaches the same problem from a more physiologic angle by expressing glucose supply in mg/kg/min. For preterm newborns, it recommends starting at 4–8 mg/kg/min on day 1 and advancing over 2–3 days to a target of 8–10 mg/kg/min, with an upper maximum of 12 mg/kg/min. For term newborns, the starting rate is lower at 2.5–5 mg/kg/min, increasing to a target of 5–10 mg/kg/min. 7 This framing is especially helpful when bedside decisions are being driven by glycemic tolerance rather than by a pre-composed PN bag.
In practice, NICE and ESPGHAN are more complementary than conflicting. NICE is easier to operationalize in unit protocols and standardized bags, whereas the European guidance provides the metabolic guardrails that matter when infants do not follow an expected course. ELBW infants deserve particular caution because glucose intolerance, insulin exposure, osmotic diuresis, fluid restriction, and concurrent sepsis or steroid exposure may rapidly change glucose tolerance. The shared clinical principle is to avoid both underfeeding and carbohydrate overload, and to adjust glucose delivery to tolerance rather than to formula alone.
Amino acids
Amino acid provision is the most studied and most debated component of neonatal PN. All three major guidance systems now endorse early amino acid delivery, but they differ in how aggressively they escalate it. NICE recommends that preterm infants who start PN within the first 4 days receive 1.5–2 g/kg/day initially, increasing over about 4 days to 3–4 g/kg/day; for term infants, the suggested start is 1–2 g/kg/day with progression to 2.5–3 g/kg/day. 2 ASPEN supports early amino acid initiation in preterm infants but advises avoiding an initial dose above 3 g/kg/day and avoiding routine doses above 3.5 g/kg/day. 1 The European amino acid guideline recommends starting at 1.5–2.5 g/kg/day on day 1 and advancing to a usual target of 2.5–3.5 g/kg/day. 5 These ranges are summarized in Table 2.
Selected trials, reviews, and evidence level informing current neonatal PN practice.
Source studies are listed in the reference section.
A second lesson from the contemporary literature is that amino acid dosing cannot be interpreted in isolation. Phosphate, potassium, magnesium, and adequate non-protein energy all matter. Reviews of protein-related controversies in very preterm infants emphasize that increased amino acid exposure can precipitate refeeding-like hypophosphatemia and related biochemical disturbances when the anabolic drive increases without concurrent mineral support.5,8,12 This is particularly important in ELBW infants, who are most vulnerable to cumulative protein deficits but also to phosphate depletion and glucose intolerance.
Clinically, amino acid strategies should be judged against meaningful neonatal outcomes, not only blood urea nitrogen, acid-base status, or short-term nitrogen balance. Avoiding cumulative protein-energy deficit, preserving head growth, reducing postnatal growth failure, and improving long-term neurodevelopment remain the outcomes that matter most. Observational data link better early protein and energy intake with later developmental scores in ELBW infants, but randomized evidence has not yet defined a universally superior high-dose threshold.13,16–18 A cautious synthesis is therefore to start amino acids early, avoid unnecessary under-provision, but not to escalate beyond contemporary targets unless the rest of the anabolic package and biochemical monitoring are secure.
Lipids and lipid emulsion choice
Early lipid administration is now standard practice in neonatal PN. Lipids are energy-dense, iso-osmolar, and essential for preventing essential fatty acid deficiency. NICE recommends starting lipids at 1–2 g/kg/day and increasing by 0.5–1 g/kg/day to a maintenance range of 3–4 g/kg/day. 2 ESPGHAN treats intravenous lipid emulsion as an integral part of PN and recommends that parenteral lipid intake generally should not exceed 4 g/kg/day in preterm and term infants. 6 Table 2 provides a numerical comparison of lipid dosing recommendations.
The more difficult issue is no longer whether lipids should be used, but which lipid emulsion to prefer. The older meta-analysis by Vlaardingerbroek and colleagues suggested that introducing lipids within the first 2 days of life is safe and well tolerated, but did not demonstrate clear benefits for growth or major morbidity. 19 It also found only limited evidence that newer emulsions outperform pure soybean-oil emulsions across broad neonatal outcomes.
More recent evidence suggests a narrower, but clinically meaningful, advantage for some composite emulsions. A 2024 meta-analysis of randomized trials reported that SMOFlipid reduced the risk of cholestasis compared with other emulsions, but did not significantly affect mortality, sepsis, necrotizing enterocolitis, bronchopulmonary dysplasia, patent ductus arteriosus, retinopathy of prematurity, or length of stay. 20 A 2022 meta-analysis of fish-oil-containing emulsions similarly found a preventive effect against PN-associated cholestasis in very low birth weight infants, especially when PN lasted longer. 21 These findings support considering mixed-oil or fish-oil-containing emulsions in infants at an increased risk of prolonged PN or liver complications.
At the same time, caution remains necessary. Consistent superiority across major neonatal outcomes has not been demonstrated, and lipid composition may influence arachidonic acid, docosahexaenoic acid, and eicosapentaenoic acid exposure in ways that are not yet fully understood.6,22,27 Essential fatty acid content also differs across products; therefore, the lipid dose required to prevent essential fatty acid deficiency may differ by emulsion. ESPGHAN recommends a minimum linoleic acid intake of 0.25 g/kg/day in preterm infants and 0.1 g/kg/day in term infants, but translating this into bedside dosing is not straightforward because products vary in linoleic acid content.6,22
A further operational issue is medication compatibility. There is substantially more accumulated compatibility experience with standard soybean-oil lipid emulsions than with mixed-oil or fish-oil-containing products. Compatibility information for soybean-oil emulsions should not automatically be applied to other lipid emulsions unless supportive data are available; pharmacists and product-specific compatibility information should guide coadministration decisions.15,27 A clearer practical recommendation is therefore: use early lipids routinely, do not assume that one emulsion improves all neonatal outcomes, consider composite or fish-oil-containing emulsions when prolonged PN or cholestasis risk is high, and interpret triglycerides in clinical context rather than as a single automatic trigger for lipid cessation.
Fluids, electrolytes, calcium, phosphate, and magnesium
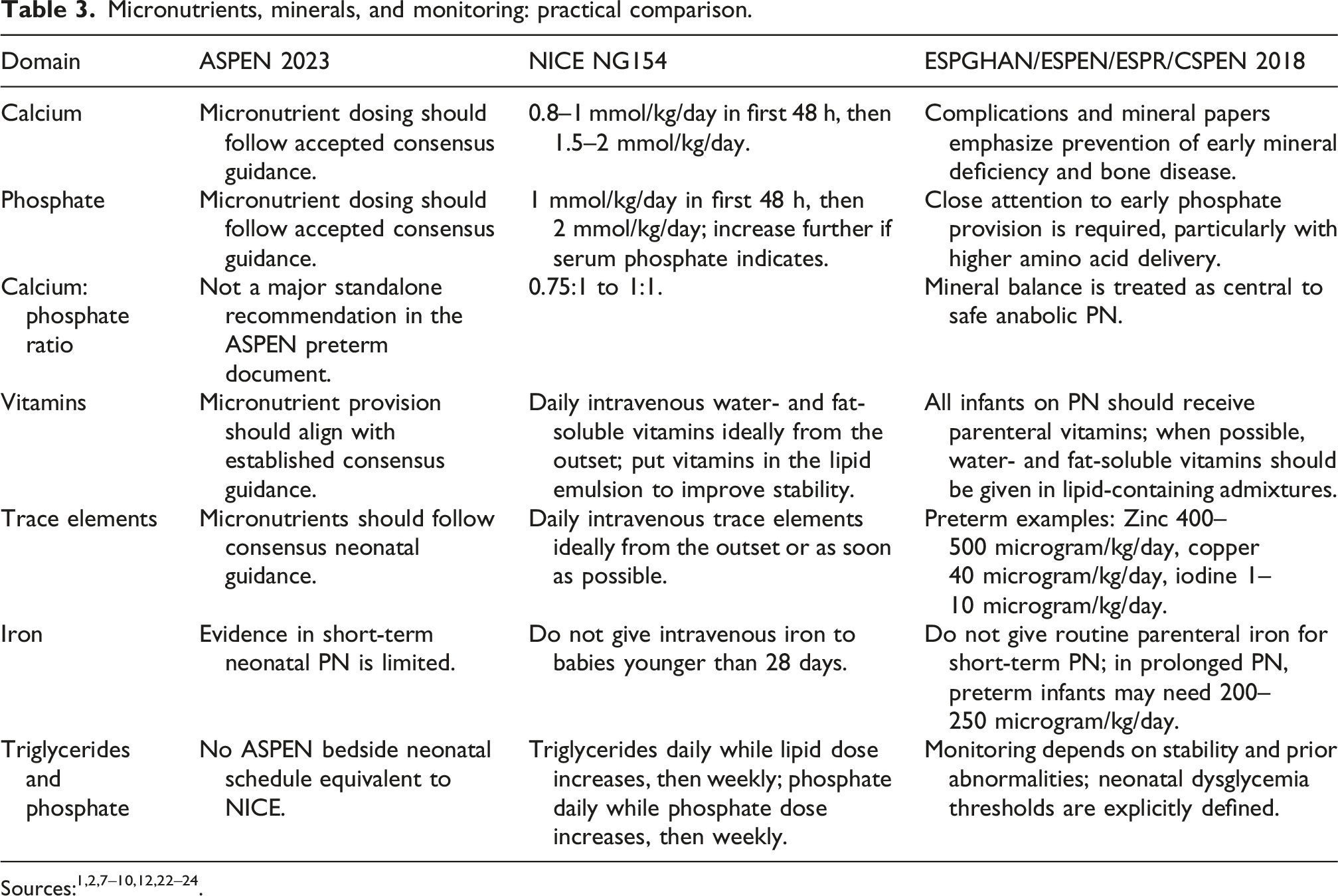
Electrolyte and mineral prescribing is where physiology often matters most. Neonatal PN is delivered during a period of rapid extracellular fluid contraction, renal adaptation, and abrupt interruption of placental mineral transfer. NICE provides practical bedside ranges, recommending calcium 0.8–1.0 mmol/kg/day initially and 1.5–2 mmol/kg/day as maintenance, together with phosphate 1 mmol/kg/day initially and 2 mmol/kg/day as maintenance. 2 These values provide clinicians with a workable framework for early prescribing and are summarized in Table 3.
The European fluid and electrolyte guideline adds an important phase-based perspective. It recommends gradual increases in fluid intake after birth and notes that sodium, chloride, and potassium are often not required during the initial contraction phase associated with early postnatal weight loss. 8 In ELBW and VLBW infants, sodium and potassium may be introduced later depending on clinical status, weight trend, urine output, and laboratory data. This approach is especially useful when early fluid shifts are pronounced and when fixed maintenance targets could be misleading.
Magnesium attracts less debate, but it should not be treated as an afterthought. NICE recommends providing magnesium ideally from the outset, or as soon as possible after PN is started. 2 In current practice, that point has become even more relevant because phosphate deficiency and refeeding-like syndromes rarely occur alone; they are commonly accompanied by hypokalemia and hypomagnesemia.8,12 The key lesson from both guidelines and recent clinical practice is that early biochemical surveillance has to accompany any strategy that promotes anabolism, especially in ELBW, growth-restricted, or severely ill infants.
Vitamins, trace elements, and iron
Micronutrient guidance is one area where the major documents are closely aligned, even though the evidence base is less robust than it is for macronutrients. NICE recommends daily intravenous administration of water-soluble and fat-soluble vitamins, ideally from the start of PN or as soon as possible after initiation, and advises delivering vitamins within the lipid emulsion to improve stability. 2 It also recommends daily trace elements and magnesium when PN is expected to continue for more than a few days. ESPGHAN similarly recommends parenteral vitamins and trace elements for infants receiving PN.9,10 Practical ranges and monitoring considerations are summarized in Table 3.
The European trace element paper is more explicit about dosing. For preterm infants, it recommends zinc 400–500 microgram/kg/day, copper 40 microgram/kg/day, and iodine 1–10 microgram/kg/day, with closer monitoring during prolonged PN or in infants with high gastrointestinal losses. 9 Iron is handled differently from the other micronutrients. NICE advises against intravenous iron in babies younger than 28 days, whereas the European guidance discusses iron mainly in the context of longer-duration PN and special clinical circumstances.2,9 In routine short-duration neonatal PN, early intravenous iron is therefore generally avoided.
The evidence gap is important. Many micronutrient recommendations are based on physiologic plausibility, deficiency prevention, expert consensus, and limited neonatal outcome data rather than large randomized trials. Therefore, prolonged PN, intestinal failure, high stoma losses, cholestasis, renal dysfunction, or unexplained poor growth should prompt individualized review of trace element and vitamin adequacy rather than reliance on a fixed default formulation.
Operational aspects
Venous access
The operational side of PN strongly affects both safety and nutrient delivery. NICE recommends central venous access for neonatal PN, but also allows peripheral administration when doing so avoids delay, is likely to be short-term, prevents interruption of PN, or when central access is impractical. 2 This pragmatic position matters because waiting for the ideal line can lead to avoidable undernutrition in the first days after birth. ESPGHAN provides a more structured venous-access framework according to expected duration, formulation characteristics, and clinical context. 11 These practical differences are shown in Table 1.
Standardized versus individualized PN
The debate over standardized versus individualized PN remains one of the clearest examples of real divergence in guidelines. NICE explicitly supports routine use of concentrated standardized bags because they are immediately available and help keep the nutritional prescription within the infant’s total fluid allowance. 2 ASPEN is more cautious and does not recommend routine standardized PN for preterm infants, reflecting concern that standardized formulations may not adequately address the substantial variability seen in this population. 1
Recent evidence helps bridge that gap. A 2023 systematic review suggested that standardized PN may improve growth by increasing early nutrient delivery, particularly protein, while showing no clear effect on mortality, necrotizing enterocolitis, or PN duration. 25 Smaller studies have generally found standardized PN to be at least non-inferior to individualized PN and, in some settings, more consistent in achieving early nutritional targets.28–30 A reasonable synthesis is that standardized PN works well as the default starting point in many units, provided clinicians maintain a low threshold for individualized modification when biochemical or clinical needs diverge. This is especially relevant for ELBW infants, surgical infants, infants with renal dysfunction, and those with evolving electrolyte disturbances.
Photoprotection and compatibility
Photoprotection has moved from being a theoretical concern to a practical recommendation. NICE advises shielding bags, syringes, and infusion sets for both aqueous and lipid PN solutions from light. 2 The rationale is to reduce light-induced degradation products and peroxide generation, which is especially relevant in premature infants exposed to prolonged PN. Even though the direct neonatal outcome data are not exhaustive, the intervention is low-risk and easy to implement.
Medication compatibility should be treated as a safety issue rather than as a routine nursing workaround. This is particularly important when lipid emulsions are infused separately or when mixed-oil and fish-oil-containing products are used. Product-specific compatibility data, institutional pharmacy review, and line-access planning should be incorporated into PN protocols rather than left to ad hoc bedside decisions.15,27
Monitoring and discontinuation
Practical monitoring and discontinuation summary for neonatal PN.
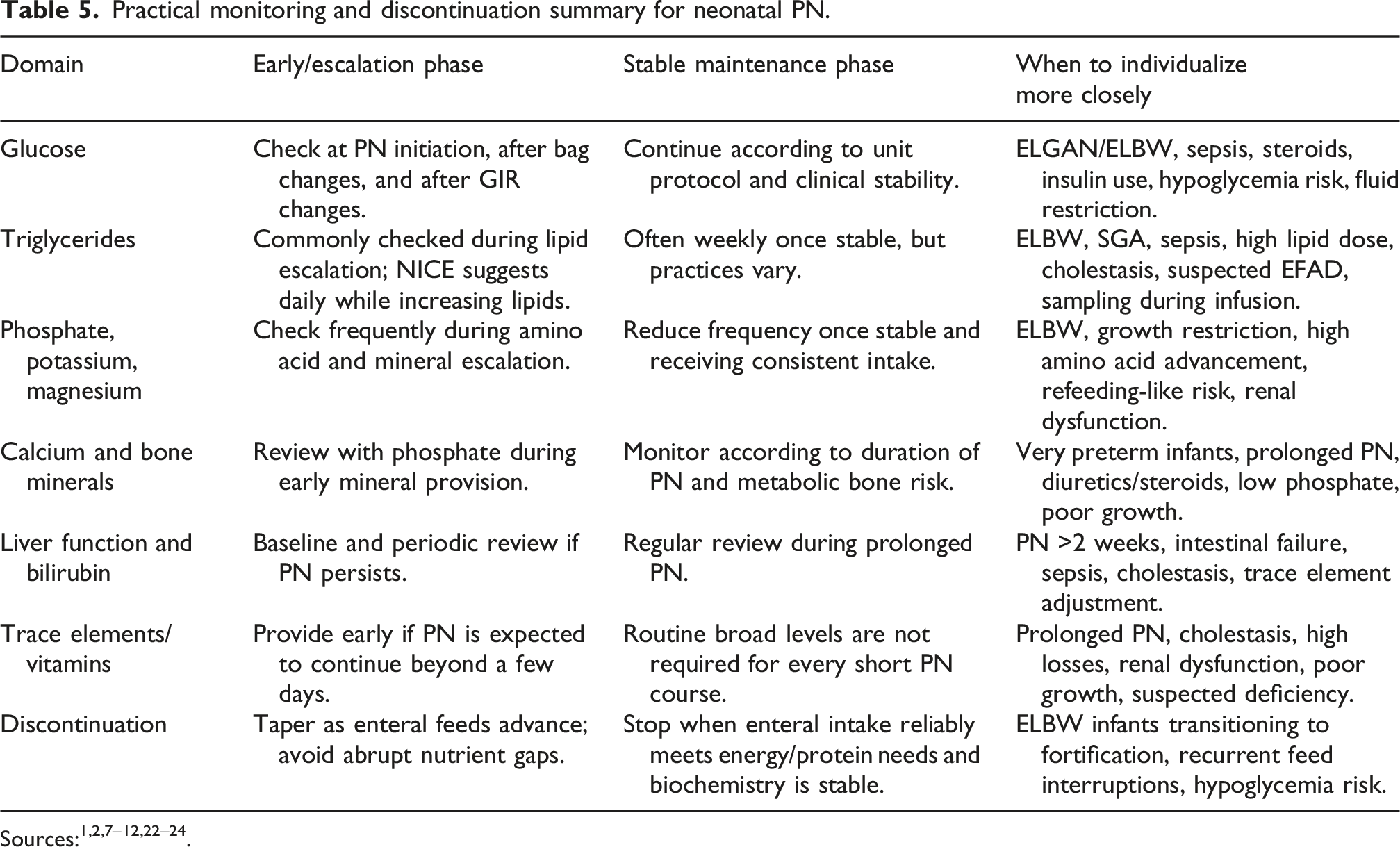
A sensible neonatal monitoring bundle includes daily assessment of fluid balance and weight trend; close glucose surveillance during initiation and whenever dextrose concentration changes; frequent review of triglycerides, calcium, phosphate, magnesium, and potassium during early advancement; and continued monitoring of liver function and trace element status in infants who remain on PN for longer periods. ELBW, growth-restricted, septic, steroid-exposed, renal-impaired, and cholestatic infants require closer individualized review than stable larger preterm infants.
Stopping PN is much less contentious. As enteral nutrition advances, PN should be tapered progressively rather than withdrawn abruptly, especially in infants who still depend on PN for a meaningful proportion of energy or protein intake. The safest transition is usually staged, with biochemical stability and enteral tolerance improving together. During this transition, clinicians should avoid creating a protein-energy gap by stopping PN before enteral feeds and fortification can meet nutritional targets.
Special clinical situations
Several situations deserve explicit mention because they are common sources of protocol drift. First, the critically ill term neonate remains a special case in which guidance does not fully align. In these infants, bedside decisions should balance the European allowance for delaying macronutrients during acute critical illness against the more proactive neonatal framework used by NICE, while keeping in mind that the strongest trial evidence available in this subgroup does not support indiscriminate early PN.2,5,14 Second, ELBW and high-risk preterm infants require more than simple weight-based extrapolation. Fluid shifts, phosphate depletion, glucose intolerance, sodium management, lipid tolerance, and cumulative protein-energy deficit all vary substantially by gestational age, birth weight, illness severity, and growth-restriction status. Protocols should therefore include ELBW-specific safeguards: early phosphate and potassium review when amino acids are advanced, cautious glucose escalation, explicit GIR adjustment rules, and early review of growth and head circumference trends.
Third, prolonged PN and intestinal failure are qualitatively different from short early-transition PN. In infants expected to need PN beyond 2 weeks, prevention of cholestasis, preservation of trace element balance, surveillance for liver disease, and prevention of essential fatty acid deficiency become more prominent priorities. In that setting, composite or fish-oil-containing lipid emulsions may be reasonable, not because they have demonstrated broad superiority across all outcomes, but because their potential benefit in preventing cholestasis becomes more relevant.20,21
Fourth, any aggressive macronutrient strategy must be paired with equally aggressive biochemical surveillance. The current literature does not support routinely escalating amino acid dosing beyond contemporary targets, and any protocol that increases amino acid delivery should specify phosphate, potassium, magnesium, and glucose monitoring from the outset rather than only after abnormalities appear.5,8,12,16–18
Current controversies and areas without full agreement
Current controversies and practical synthesis.
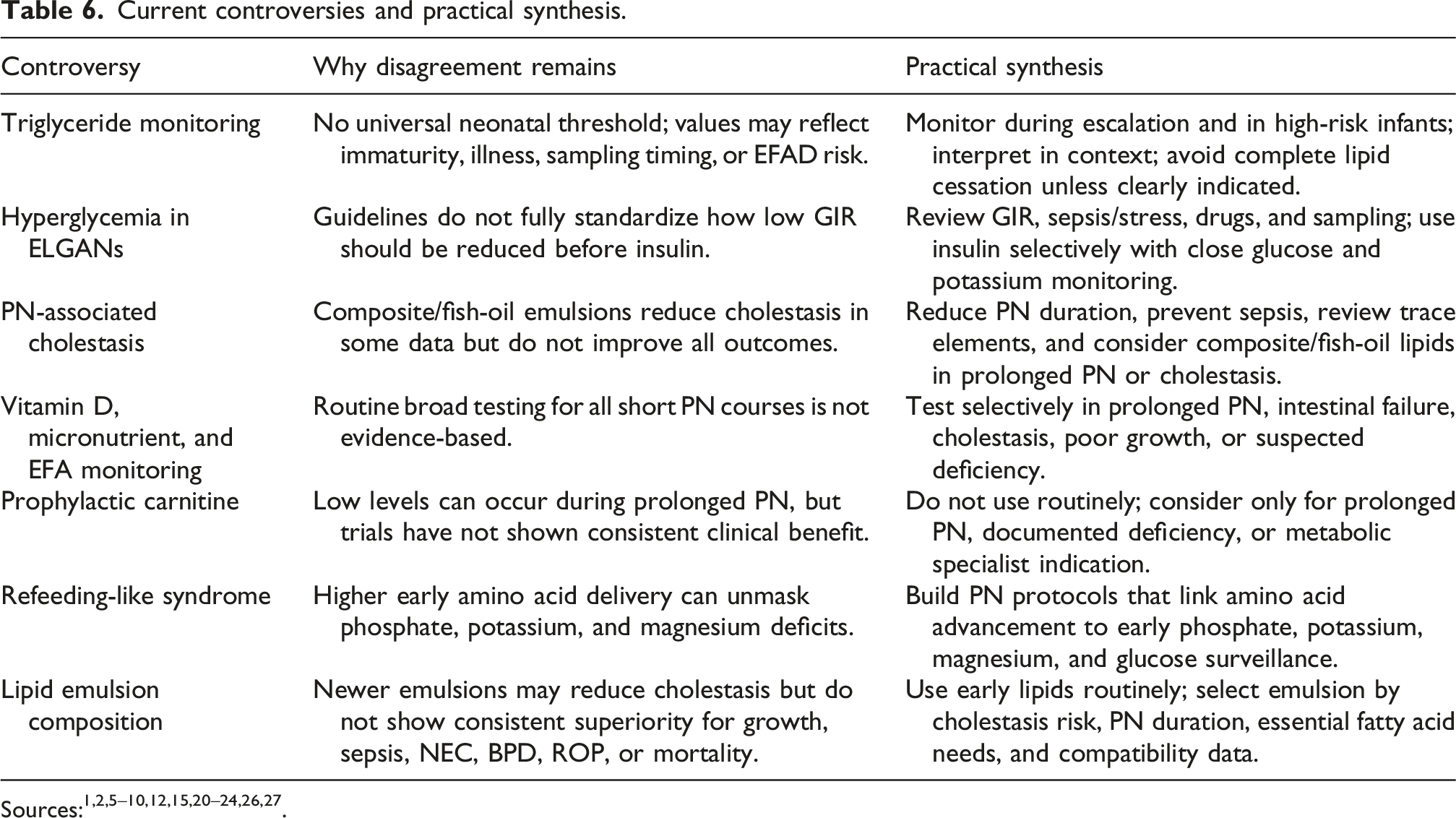
The second controversy is hyperglycemia in ELGANs. Guidelines agree that glucose should be titrated to tolerance, but they do not fully standardize how far to reduce glucose infusion rate before insulin is used.1,2,7 In practice, the first steps are to confirm the glucose value, review GIR and concurrent medications, assess sepsis or stress physiology, and avoid excessive carbohydrate delivery. Insulin may be appropriate for persistent clinically significant hyperglycemia when adequate calories cannot otherwise be provided, but it should be used with careful monitoring because hypoglycemia and potassium shifts can be harmful. The third controversy is PN-associated cholestasis. Strategies include minimizing PN duration, advancing enteral feeds when safe, preventing catheter-related sepsis, cycling PN in selected longer-term patients, reviewing copper and manganese exposure in cholestasis, ensuring adequate zinc in infants with high losses, and considering composite or fish-oil-containing emulsions when PN is prolonged or cholestasis has developed.6,9,12,20,21 The evidence supports selective use rather than a universal claim that newer lipid emulsions improve all neonatal outcomes.
The fourth controversy is micronutrient, vitamin D, and essential fatty acid monitoring. Routine frequent measurement of all micronutrients is not feasible or evidence-based for every short-term PN course. However, prolonged PN, intestinal failure, cholestasis, poor growth, unusual skin findings, recurrent infections, or restricted lipid dosing should prompt individualized testing, including consideration of fatty acid profile or triene:tetraene ratio when essential fatty acid deficiency is suspected.9,10,22 The fifth controversy is prophylactic carnitine. Preterm infants may develop low carnitine levels during prolonged PN, but a Cochrane review found no evidence that routine supplementation of parenterally fed neonates improves weight gain, lipid utilization, or ketogenesis. 26 Therefore, prophylactic carnitine should not be embedded as a routine default in neonatal PN protocols; it may be considered selectively in prolonged PN, documented deficiency, or specialist-directed metabolic contexts.
Where the guidelines agree and where they differ
The major documents agree far more than they disagree. They agree that PN should not be delayed when enteral intake is clearly inadequate; that amino acids should start early; that lipids are a routine component of neonatal PN; that glucose must be titrated to tolerance rather than prescribed reflexively; that vitamins and trace elements need deliberate attention; and that careful biochemical monitoring is essential.1–12 The differences become most visible in three domains. The first is philosophy: NICE translates evidence into highly operational neonatal instructions, whereas ASPEN more often limits itself to recommendations that are directly supported by growth-oriented evidence and is therefore more conservative in areas such as standardized PN.1,2 The second is subgrouping: the European guidance explicitly addresses the critically ill term infant and frames several recommendations by physiologic phase.3–12 The third is tone around escalation: European documents often present a broader physiologic range, while NICE tends to provide a more direct prescribing pathway.
From a practical standpoint, neonatal units do not need to choose one document and ignore the rest. A more useful approach is to build a local PN pathway that combines the operational clarity of NICE, the physiologic nuance of ESPGHAN, and the evidence-discipline of ASPEN. That pathway should explicitly identify where the unit will individualize care for ELBW infants, critically ill term neonates, surgical infants, infants expected to require prolonged PN, and infants with evolving biochemical instability.
Clinical synthesis
A balanced neonatal PN strategy can therefore be summarized in a few pragmatic steps. Do not delay PN when enteral adequacy is unlikely in the short term. Use central access when PN is expected to continue or when the formulation requires it, but do not let line logistics postpone early support if safe peripheral PN is feasible. Start with moderate substrate delivery and advance thoughtfully rather than reflexively. Pair amino acid advancement with phosphate, potassium, and magnesium surveillance. Use early lipids routinely, while considering composite emulsions in infants at higher risk of prolonged PN-associated liver disease. Introduce vitamins and trace elements early. Use standardized PN as a systems tool when it improves timely nutrient delivery, but preserve rapid individualized adjustment for ELBW infants and clinically unstable neonates. The most important clinical shift is to view PN as a bridge toward meaningful neonatal outcomes rather than a biochemical prescription alone. Growth velocity, head circumference trajectory, avoidance of postnatal growth failure, duration of PN exposure, liver health, catheter complications, and neurodevelopmental follow-up should be incorporated into quality review. Future studies should address long-term neurodevelopment, optimal protein dosing thresholds, triglyceride interpretation, ELBW-specific refeeding prevention, lipid emulsion composition, and real-world implementation of standardized PN protocols.
Limitations of the current evidence and of this review
The evidence base has several limitations. Many neonatal PN recommendations are supported by physiologic reasoning, consensus, and short-term biochemical outcomes rather than by large trials powered for survival, growth, head growth, liver disease, and neurodevelopment. Trials differ in gestational age, birth weight, illness severity, baseline enteral feeding practices, lipid products, amino acid formulations, and outcome timing. ELBW and extremely preterm infants are often the patients most affected by PN decisions, but they are also the most difficult subgroup in which to generate definitive evidence.
This review also has limitations. It is a narrative expert review, not a systematic review. Although the methods have been made more transparent, no formal risk-of-bias assessment, certainty grading, or pooled meta-analysis was performed. Selection bias is possible, and the interpretation emphasizes clinically relevant evidence rather than exhaustive inclusion of all publications. The review should therefore be used as a practical synthesis to guide protocol development and bedside reasoning, not as a substitute for local multidisciplinary guideline development.
Conclusion
Neonatal PN has evolved from a rescue measure into a structured, evidence-informed component of routine neonatal care. The major contemporary guidelines no longer differ on the fundamentals: timely substrate delivery, careful escalation, proactive micronutrient replacement, and close monitoring form the common ground. The remaining controversies are narrower but still clinically important: how high amino acid delivery should go, when PN should be withheld in critically ill term neonates, how strongly standardized bags should be favored, how triglycerides should be interpreted, and whether newer lipid emulsions offer benefits beyond cholestasis reduction.
The most clinically useful approach is not strict allegiance to one guideline, but thoughtful integration of complementary perspectives. Integrating these guideline frameworks into unified, context-adapted NICU protocols may represent the most effective strategy to optimize neonatal growth, biochemical safety, liver health, and longer-term outcomes.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.