
Abstract
Breast cancer remains the most commonly diagnosed malignancy among women worldwide. Standard treatment often involves mastectomy, followed by chemotherapy and/or radiation. Approximately 40% of patients undergo breast reconstruction to address the physical and psychological effects of tissue loss. Since the first autologous breast reconstruction described in 1887, both autologous and alloplastic techniques have evolved significantly to improve patient outcomes. However, current approaches are limited by issues such as the inability to restore biological breast function, suboptimal tissue integration, and concerns over long-term implant viability. Tissue engineering has emerged as a promising field capable of overcoming these limitations. Since the 1990s, advances in biomaterials, stem cell research, and regenerative strategies have enabled the development of vascularized, patient-specific constructs with potential applications in both structural and functional breast reconstruction. This review provides a comprehensive overview of the evolution of breast reconstruction techniques and the integration of tissue engineering into the field. Particular emphasis is placed on tissue engineering’s role in enhancing breast cancer treatment and diagnosis while also exploring future directions toward functional restoration, including lactation.
Impact Statement
Breast cancer is a disease with a multifaceted impact, affecting physical health, emotional well-being, sexual health, and overall quality of life. The continuous evolution of breast reconstruction methods is driven by the critical need to address all of these aspects, with breast tissue engineering focusing on developing new, accessible, biologically compatible, and durable solutions. By compiling the advancements and challenges in this field, this review serves as a valuable resource for clinicians and researchers, helping to understand the current state of the field and guiding future progress.
Keywords
Introduction
Breast cancer (BC) is now the most commonly diagnosed cancer in the world. The global cancer burden estimates that there were 2.26 million new cases of BC in 2020, and the disease is the leading cause of cancer mortality among women worldwide. According to the World Health Organization’s findings in an article published by Elsevier (Arnold et al., 2022), the data presented indicates that by 2040, BC is predicted to increase to over 3 million new cases and 1 million deaths annually, globally.1–3 Mastectomy remains a cornerstone in the surgical management of BC. However, the physical and psychosocial consequences of breast loss can be profound. Up to 40% of patients pursue breast reconstruction (BR) to restore not only body image but also psychological well-being, self-esteem, and quality of life. 4
Despite significant advances in both autologous and implant-based techniques, current BR methods face limitations, particularly in patients with prior radiation, poor skin flap vascularity, or insufficient donor tissue. Complications such as fat necrosis, capsular contracture, and volume loss remain prevalent.5,6 These challenges underscore the need for novel, regenerative strategies that go beyond traditional surgical approaches. Tissue engineering (TE) has emerged as a promising field offering biological and technological innovations to create constructs that can replace native tissues or to aid tissue regeneration. 7 TE seeks to overcome the limitations of conventional BR by enhancing vascularization, promoting tissue integration, and enabling patient-specific regeneration. By bridging advances in BC diagnosis and treatment, TE not only improves current reconstruction techniques but also opens new avenues for comprehensive care and potential functional restoration.
This review provides a concise overview of emerging concepts in breast TE. The objective of this article is to examine the full spectrum of TE in breast tissue and bioengineering applications in BR and to outline how these emerging technologies can be leveraged to improve surgical outcomes.
Current Techniques in Breast Reconstruction: Progress and Limitations
BR has progressed significantly from the era of radical mastectomy to modern autologous and implant-based techniques. Landmark developments include the introduction of pedicled flaps from donor areas such as thoraco-epigastric, flank, contralateral breast, and gluteal regions in the first half of the 20th century.8–11 With the advent of free tissue transfer, silicone implants, and reappraisal of vascular territories in the 1970s and 1980s, a new era in reconstructive surgery began with the emergence of contemporary techniques including a variety of donor sites including abdominal wall, buttocks, lumbar region, and thigh region, depending on the available donor tissue.12–19
Free tissue transfers and silicone implants collectively constitute the foundation of modern BR. Among autologous options, the deep inferior epigastric artery perforator (DIEP) flap has become the workhorse, offering favorable aesthetic outcomes and reduced donor site morbidity by using only the vascularized skin and subcutaneous tissue of the anterior abdominal wall. 14 Implant-based approaches—with or without flap coverage—offer less invasive alternatives with shorter recovery times and have been widely adopted, particularly as ablative BC surgeries have become increasingly conservative. 20 Fat grafting is increasingly used for breast volume restoration in both reconstructive and aesthetic procedures. 21
Despite these advances, current methods remain limited by several factors. Autologous techniques require extensive operative time, specialized expertise, and suitable donor tissue-constraints that may exclude some patients. 5 Implant-based reconstruction, while more accessible, is associated with complications such as capsular contracture, infection, and implant failure, particularly in irradiated tissue beds and poorly vascularized mastectomy flaps. 6 Fat grafting with traditional techniques can also be limited by variable volume retention, often requires multiple staged procedures to achieve the desired outcome and has a relatively high complication rate with the most common being fat necrosis. 22 In addition to volume restoration, reconstruction of the nipple-areolar complex often entails further surgical interventions and may require cartilage grafts, adding to patient morbidity and procedural complexity. 23 These persistent challenges underscore the need for novel approaches in BR.
TE and regenerative medicine offer the potential to overcome existing limitations by enabling the regeneration of vascularized, patient-specific soft tissue with minimal donor site morbidity. Such approaches can support BR in multiple ways, for example, by improving the skin envelope, enhancing fat graft retention, or directly facilitating the creation of a new breast mound or nipple-areolar complex. For instance, acellular dermal matrices (ADMs) are a widely adopted adjunct in clinical practice, particularly useful in implant-based reconstructions allowing better placement and cover for implants. 24 Also, current BR methods are primarily focused on reducing complications of mastectomy by minimizing chest wall deformities and improving the psychosocial well-being of patients, but they are unable to restore its biological function of the breast such as lactation and endocrine signaling. 25 This highlights a critical gap in regenerative strategies that aim for true functional restoration rather than cosmetic reconstruction alone. TE offers a transformative approach in this regard, with the potential to preserve or restore breast tissue and its biological functions. 26 Furthermore, engineered breast tissue models can play a pivotal role in BC diagnosis and treatment by providing more accurate in vitro platforms for studying tumor biology, drug screening, and personalized medicine. These models closely mimic the native microenvironment, allowing researchers to investigate tumor-stroma interactions, hormone responses, and metastatic behavior in a more representative setting.27–29
Overall, integrating TE into BR bridges the gap between structural restoration and biological function, and offers a more comprehensive solution for patients undergoing mastectomy.
Breast Tissue Engineering
TE methods for BR started to be actively explored in the 1990s as part of the broader development of regenerative medicine. 30 TE has the potential to revolutionize rehabilitation for patients with BC by providing a practical solution that can restore the breast after mastectomy and address the limitations of current reconstructive surgery techniques. 31 Breast TE has enabled new treatment options for tissue loss in patients with BC, by creating different types of substitutes in the laboratory. 28 In addition, TE has made significant advances in the broader field of BC research and recovery. Innovations are driving more effective approaches for understanding tumor biology, improving drug delivery, and facilitating tissue regeneration following cancer treatments, ultimately enhancing both patient outcomes and quality of life. 28
The following sections describe the key applications of breast TE. The first section focuses on innovative TE strategies for the diagnosis and treatment of BC. The second section explores its role in aesthetic BR, aiming to restore a natural appearance and chest wall deformities. The final section highlights approaches to functional BR, emphasizing the restoration of both anatomical structure and physiological function. Together, these sections illustrate the broad potential of TE to improve outcomes for patients with BC.
Tissue engineering for breast cancer diagnosis and treatment
Animal models have long been considered the gold standard in studies of tumor physiology and cancer treatment. However, the vast majority of drugs (90%) that successfully passed preclinical testing failed in clinical trials.32,33 While there has been an increase in the use of in vitro models focused on BC physiology and treatment, two-dimensional models do not accurately replicate all aspects of breast tumors. These models cannot mimic the complexity of the entire organism, nor can they simulate the critical cell-cell and cell-stromal interactions necessary for normal tumor growth, nor do they replicate the tumor-like microenvironment.27–29 Tumor heterogeneity is a major challenge for BC researchers, and one of the most promising applications of TE in cancer diagnosis is the creation of 3D cell cultures. 34 Researchers are developing three-dimensional (3D) BC models to replicate human breast tumor (BT) environments in vitro. These models are created by engineering 3D tissues that mimic the structure and behavior of tumors. By simulating how cancer cells interact with their microenvironment, these models can identify tumor-specific markers or genetic changes that signal the early stages of cancer. 33 Studies are focusing also on creating patient-specific tumor models using TE to replicate individual tumor characteristics. These models can be used to test biomarkers or identify early molecular changes that might indicate the presence of cancer, potentially leading to more accurate, personalized diagnostic tests. 35
The extracellular matrix (ECM) also plays a crucial role in cancer progression, and engineered ECM models are being developed to identify early tissue changes that may indicate the presence of cancer. By creating bioengineered ECM models that closely mimic the tumor microenvironment (TM), researchers can explore how cancer cells modify their surroundings, offering the potential for novel diagnostic approaches to detect tumors at an early stage. Furthermore, the stromal components of breast tumors, such as immune cells, fibroblasts, adipose tissue, endothelial cells, and tissue-derived stem cells, play a pivotal role in cancer progression by secreting factors, altering cell phenotypes, and reorganizing themselves. TM models that recreate the intricate interactions between cancer cells, stromal cells, and immune cells are increasingly used to study tumor growth and metastasis and to identify biomarkers for diagnostic purposes. For instance, engineered models can be used to investigate the interactions between circulating tumor cells and surrounding tissue, shedding light on potential biomarkers that could signal the spread of cancer.36,37
Due to concerns about the side effects associated with traditional BC treatments, recent research has focused on developing alternative approaches for targeted drug delivery in cancer therapy, such as the use of plant extract-loaded scaffolds in BC treatment. 38 Another emerging area of research is immunoengineering. 39 By creating artificial immune systems, researchers can identify better model BC diagnoses. 40 Additionally, TE is exploring the use of nanoparticles combined with TE methods to create advanced imaging technologies. 41 Biosensors are also being developed to detect cancer-related biomarkers in blood, urine, or other bodily fluids, while high-throughput screening and predictive models for tumor behavior, such as artificial neural networks, are being employed to enhance diagnosis and treatment strategies.42–44
All TE approaches used in BC diagnosis and treatment are summarized in Figure 1.33,45–48
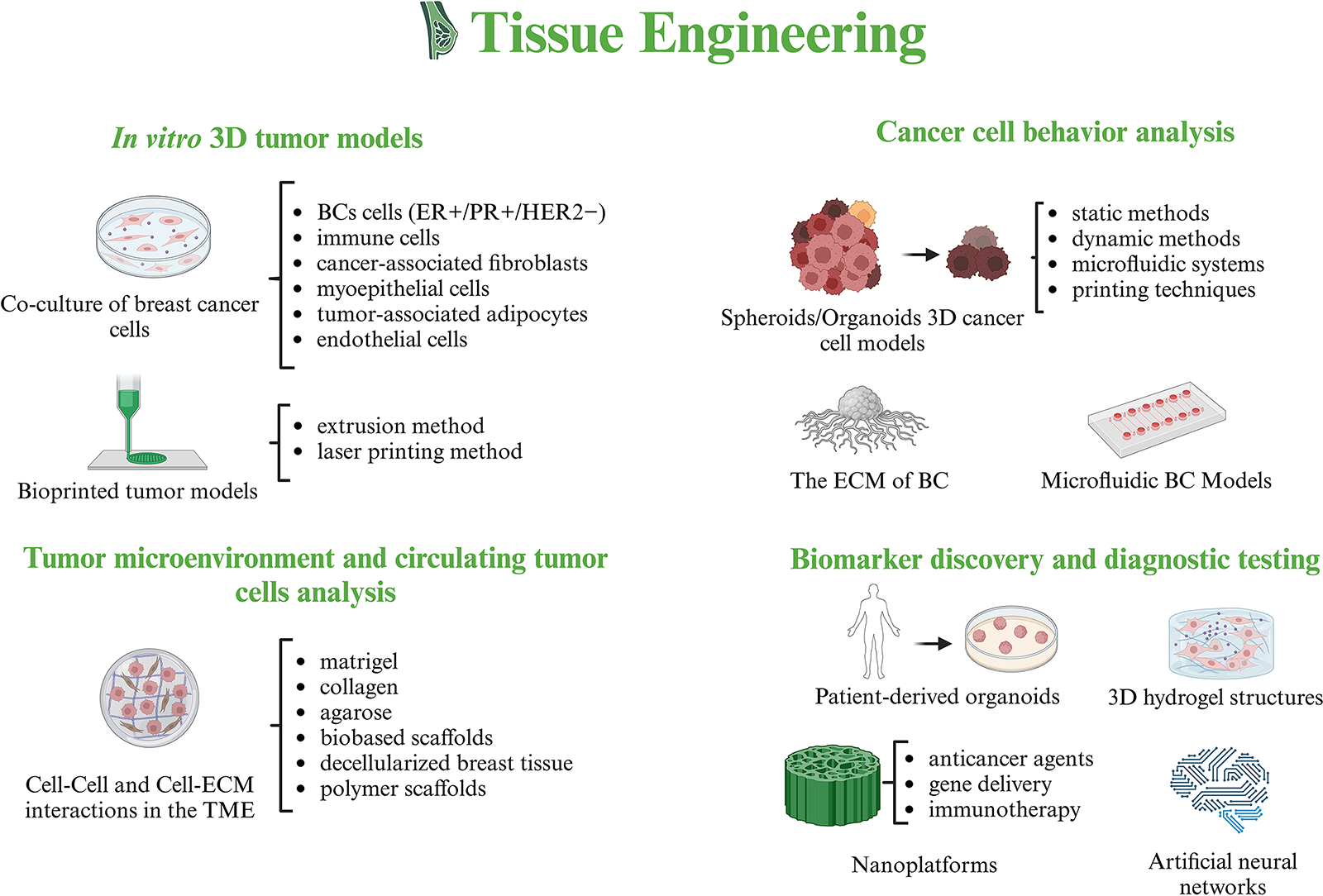
Tissue Engineering Approaches in Breast Cancer Diagnosis and Treatment.
Tissue engineering for aesthetic breast reconstruction
BR after mastectomy involves both skin and volume restoration. The primary goal is to rebuild the patient’s breast mound while preserving tactile sensation when possible. Breast function, however, is not typically a primary objective at this stage. 31 There are several areas of TE that have begun to significantly advance BR methods.
3D printing in BR
3D printing has emerged as a transformational technology that makes it possible to create scaffolds that are patient-specific and are controlled precisely in terms of their structure, material properties, and intended purpose. 3D printing, or computer-aided manufacturing, has revolutionized reconstructive breast surgery by providing patient-specific solutions that enhance recovery after mastectomy. Stereolithography files are used to convert computer-aided design models into printable objects. According to the design specifications, the 3D printer constructs an object layer by layer, precisely depositing the selected material, known as “bioink.” Furthermore, this technology has been successfully applied to implantable scaffolds designed to repair specific tissue defects.49–51
The development of a 3D-bioprinted scaffold for BR has substantial clinical relevance. Innovations in 3D printing enable autologous tissue integration, which can improve patient outcomes. In BC surgery, poly-4-hydroxybutyrate scaffolds have been used to fabricate more natural-looking nipples. In contrast to conventional methods, these scaffolds gradually degrade while supporting natural tissue formation, maintaining the nipple’s shape and projection over time. According to animal studies, the body’s natural healing mechanisms fill the spaces with vascularized and fatty tissues characteristic of nipples as the scaffold degrades. Furthermore, 3D-printed scaffolds can be manufactured in various sizes and shapes to accommodate individual patient needs or custom-designed to replicate the remaining nipple in cases of unilateral mastectomy. 52 In a recent study, the authors used a 3D-bioprinted scaffold designed and fabricated by additive biomanufacturing to deliver delayed fat injections into custom-designed scaffolds. A well-established additive biofabrication platform was used to fabricate patient-specific, multilayer reticulated hemispherical scaffolds from polycaprolactone (PCL). An invasive ductal carcinoma patient was diagnosed using medical imaging techniques, such as CT scanning and laser scanning. The imaging data were utilized to construct a 3D model of the breast, which guided the fabrication of a 100 cm³ patient-specific porous breast scaffold. These 3D-printed scaffolds were implanted into subglandular pockets in immunocompetent minipigs to evaluate their functionality. Implants demonstrated promising results, including angiogenesis and adipose tissue regeneration. According to histological analyses, the group receiving a combination of prevascularization and lipoaspirate displayed the most significant percentage of adipose tissue, closely resembling native breast tissue. Based on this study, 3D-bioprinted scaffolds can support adipose tissue integration and vascularization during BR, thus improving outcomes. 53
In 2019, Luo et al. developed an innovative multifunctional scaffold made from dopamine-modified alginate and polydopamine (PDA) using 3D printing to promote tissue repair following BC surgery. Due to their powerful photothermal effect, alginate-PDA (Alg-PDA) scaffolds are suitable for cancer treatment. Additionally, the scaffold showed excellent flexibility and an elastic modulus, similar to normal breast tissue. Furthermore, Alg-PDA scaffolds displayed excellent adhesion to and proliferation of human breast epithelial cells. Combining photothermal efficiency and enhanced cell proliferation could be a promising option for BC therapy and tissue repair after surgery. 54 Tytgat et al. used extrusion-based 3D printing to fabricate scaffolds with methacrylamide-modified gelatin (Gel-MA) and methacrylated κ-carrageenan (Car-MA). The 3D-bioprinted scaffolds demonstrated long-term durability, high water absorption capability, and mechanical properties similar to those of natural breast tissue. Gel-MA and Car-MA-based scaffolds exhibit these characteristics, illustrating their potential for applications in breast TE. 55
In 2016, a pioneering study in Australia explored 3D-printed TE for human BR. Five postmastectomy female patients aged 35 to 49 participated in the trial. The procedure involved harvesting a pedicled thoracodorsal artery perforator fat flap (6–50 mL) and transposing it onto the chest wall. Morrison developed a perforated acrylic dome-shaped chamber implant with 3 mm holes that range in size from 140 to 360 mL. Findings revealed the formation of new blood vessels, fibrous tissue, and adipose tissue in the subject. As a result of this study, large, well-vascularized tissue-engineered constructs were generated using this technique. However, their texture was hard, and their cosmetic outcome was poor, emphasizing the need for further refinements to improve patient satisfaction. 56 A customized breast form was created using 3D printing technology with polypropylene copolymer bioink. BR was performed using a single-pedicle flap or double-pedicle flap combined with a 3D-printed mold. In this study, the method was demonstrated to be adaptable, which allowed it to be used for BR in patients with breast ptosis with only minor modifications. Using 3D surface imaging and 3D-printed molds, Tomita et al. reported effective and efficient methods for restoring breast symmetry using DIEP flap reconstruction. By using this approach, surgeons with less experience may be able to reconstruct symmetrical, nonptotic breasts in a shorter period of time.57,58 Another study conducted by Stefan et al. produced a 3D-bioprinted breast prosthesis replicating a mirror image of the contralateral breast from which the 3D-bioprinted prosthesis is derived. The prosthesis is created using Polylactic acid as the printing material. 3D stereophotogrammetry images were used to create patient-specific templates, which were then printed. A printed template guided the surgeon in shaping and sizing the autologous flap during reconstruction. 59 Likewise, 3D printing was used in another study to create a porous PCL implant for BR. In the study, PCL was demonstrated to be biodegradable and biocompatible as a breast implant. With 3D printing, implants and molds can be customized to the patient’s specific anatomy, enhancing symmetry and aesthetic results, especially in unilateral mastectomies that must match the contralateral breast. 60
A summary of studies based on 3D printing in BR is represented in Table 1.
Three-Dimensional Printing in Breast Reconstruction
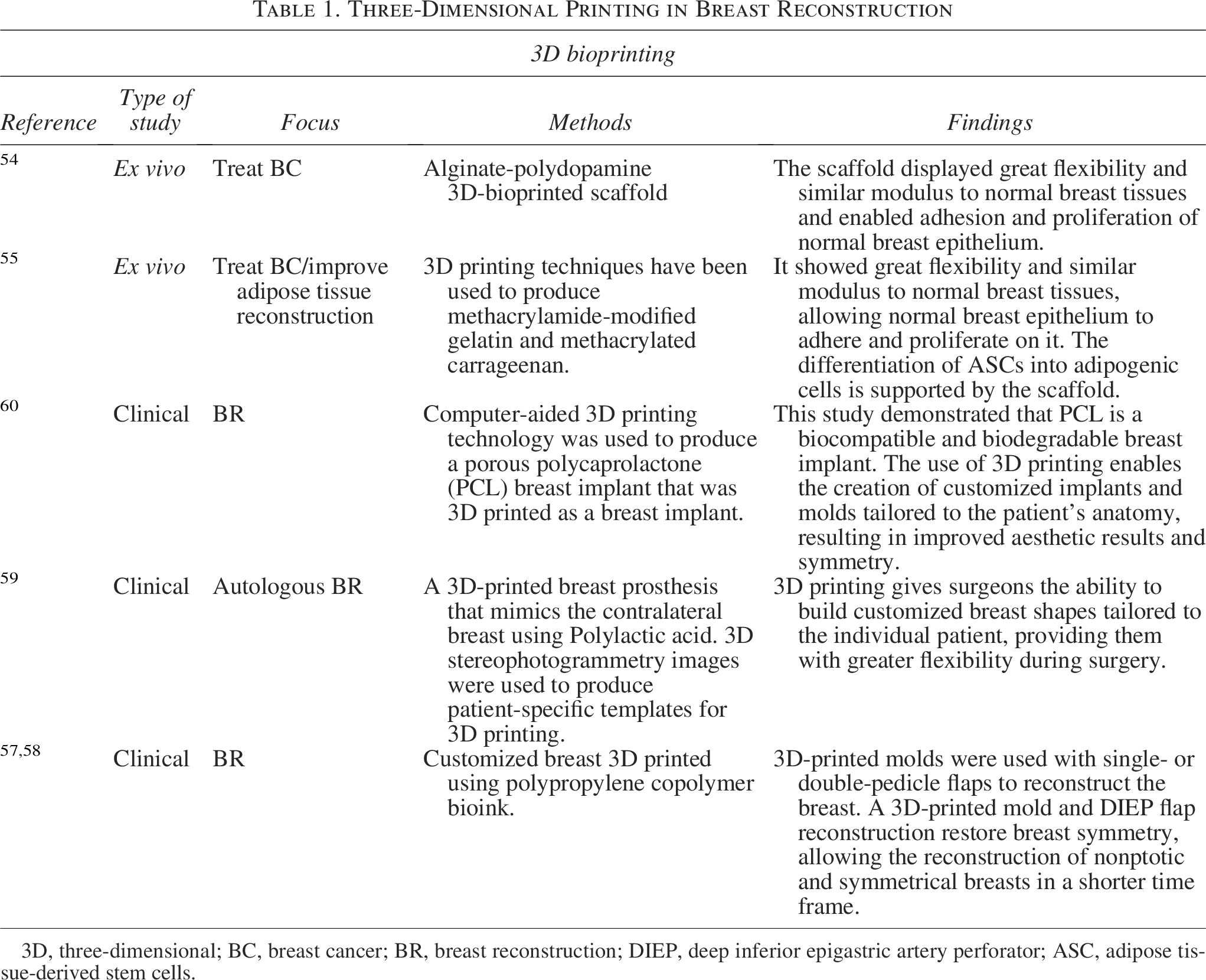
3D, three-dimensional; BC, breast cancer; BR, breast reconstruction; DIEP, deep inferior epigastric artery perforator; ASC, adipose tissue-derived stem cells.
Decellularization
Decellularization began to be used in BR in the 2000s, when ADM started to be used for this purpose. 24 Currently, decellularization is also employed to obtain acellular bovine pericardium and porcine peritoneal matrix, which are used as meshes for dual-plane and prepectoral BR.61,62
Decellularized and delipidated breast tissue can be used to develop 3D BC models. Blanco-Fernandez et al. developed a method for obtaining decellularized porcine breast tissue rich in glycosaminoglycans and collagen to recreate the complex composition of breast tumors using bioprinting. 63 Jin et al. used a decellularized breast matrix as a bioactive microenvironment for in vitro cancer culture. The authors believe that these can be powerful tools for future preclinical research in breast development. 64 Caronna et al. (2021) presented their results on the viability of acellular biological grafts for nipple-areolar complex reconstruction in a nonhuman primate model. The authors mention that the human-derived decellularized nipple-areolar complex (dcl-NAC) is safe and supports recellularization as well as the presence of nerves at 6 weeks postengraftment. No adverse systemic responses were detected. 65 Maistriaux et al. used human NACs to obtain decellularized ECM. The authors described in vitro cytocompatibility of the ECM by seeding human fibroblasts, as well as its in vivo biocompatibility and immunogenicity through subcutaneous implantation in recipient rats for 30 days. 66 Another study presenting tissue-engineered NACs using decellularization is by Pashos et al., who confirmed that decellularized nonhuman primate NAC grafts can promote neovascularization as well as re-epithelialization in vivo. 67
A summary of studies based on decellularization in BR is represented in Table 2.
Decellularization in Breast Reconstruction
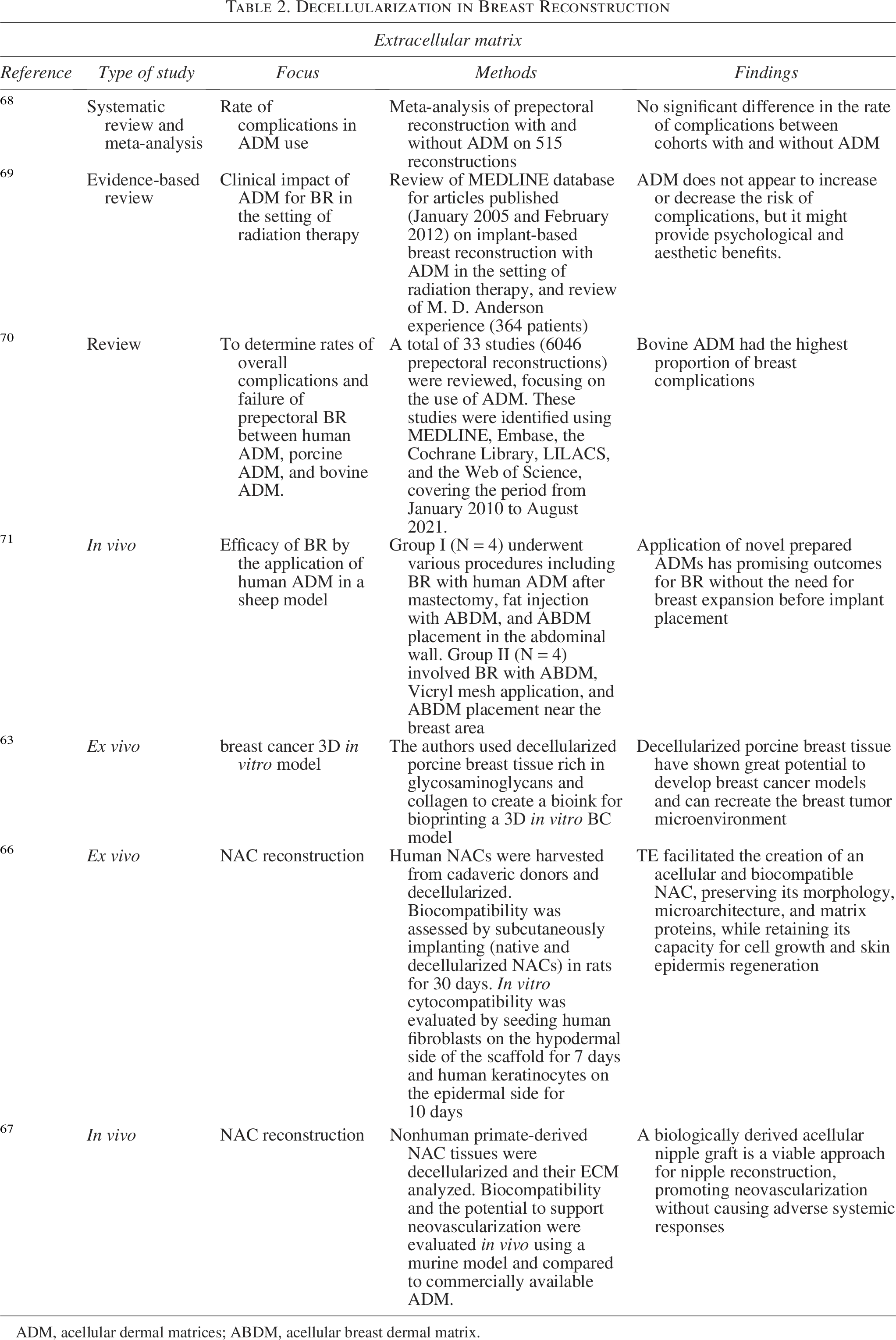
ADM, acellular dermal matrices; ABDM, acellular breast dermal matrix.
Cells
Undifferentiated progenitor cells, such as adipose-derived stem cells (ADSCs) have become increasingly important in BR, demonstrating significant advantages in both autologous and implant-based approaches. These cells enhance breast contour and restore a natural sensation, leading to improved cosmetic and emotional outcomes. 72 The role of ADSCs has garnered considerable attention due to their ability to secrete a variety of growth factors. These factors play a crucial role in promoting vascular growth, cell migration, and differentiation through a paracrine mechanism. Consequently, increasing the number of ADSCs per unit volume, a technique known as cell-assisted lipotransfer, has been shown to enhance fat graft survival and optimize clinical outcomes in lipotransfer procedures.73–75
In 2019, Gentile et al. assessed the effectiveness and safety of engineered fat grafts enhanced with ADSCs for BR. Their findings indicated that, after 12 weeks, 72.8% of patients treated with ADSCs experienced restored breast contour and a 12.8 mm increase in 3D volume, compared to only 27.3% in the control group treated without cells. The study concluded that the addition of ADSCs to autologous fat grafts significantly enhanced breast soft tissue volume. Furthermore, the authors suggested that this approach promoted neoangiogenesis, driven by stromal vascular fraction cells (SVFs), ADSCs, and the release of growth factors. 76
One of the advantages of engineered fat grafts enhanced with ADSCs is their reduced rate of fat graft reabsorption compared to nonenhanced fat grafts. Studies have shown that, over the first year, the reabsorption rate is significantly lower for SVF-enhanced fat grafts (37%) compared to nonenhanced fat grafts (61%). 76 Additionally, ADSCs release proangiogenic factors, including vascular endothelial growth factor (VEGF), which interact perivascularly with blood vessels and provide physical ECM cues to support and enhance endothelial sprouting. 77 In this context, Koellensperger et al. demonstrated that coculturing ADSCs with BC cell lines (BRCAs) enhances the angiogenic potential of both ADSCs and BRCAs across all tested cell lines. 73 Although, concerns have been raised about the use of ADSCs in fat grafting due to their potential role in increasing cancer risk or recurrence.
Theoretically, ADSCs could contribute to this risk by enhancing cell proliferation and angiogenesis through endocrine, paracrine, and autocrine pathways. 72 While some studies indicate that even with a higher concentration of ADSCs in cell-assisted lipotransfer (CAL), there is no significant impact on rates of local tumor recurrence or metastatic cancer, CAL may offer longer-lasting outcomes and a lower likelihood of cancer recurrence compared to traditional fat transfer. 78 However, other studies suggest that coculturing ADSCs with BC cells in vitro leads to significant alterations in key malignancy-related parameters. This suggests a possible increased oncological risk in vivo, emphasizing the importance of caution when considering the clinical use of cell-assisted lipoaspirates in BC patients. 73
A summary of studies based on cells in BR is represented in Table 3.
Cells in Breast Reconstruction
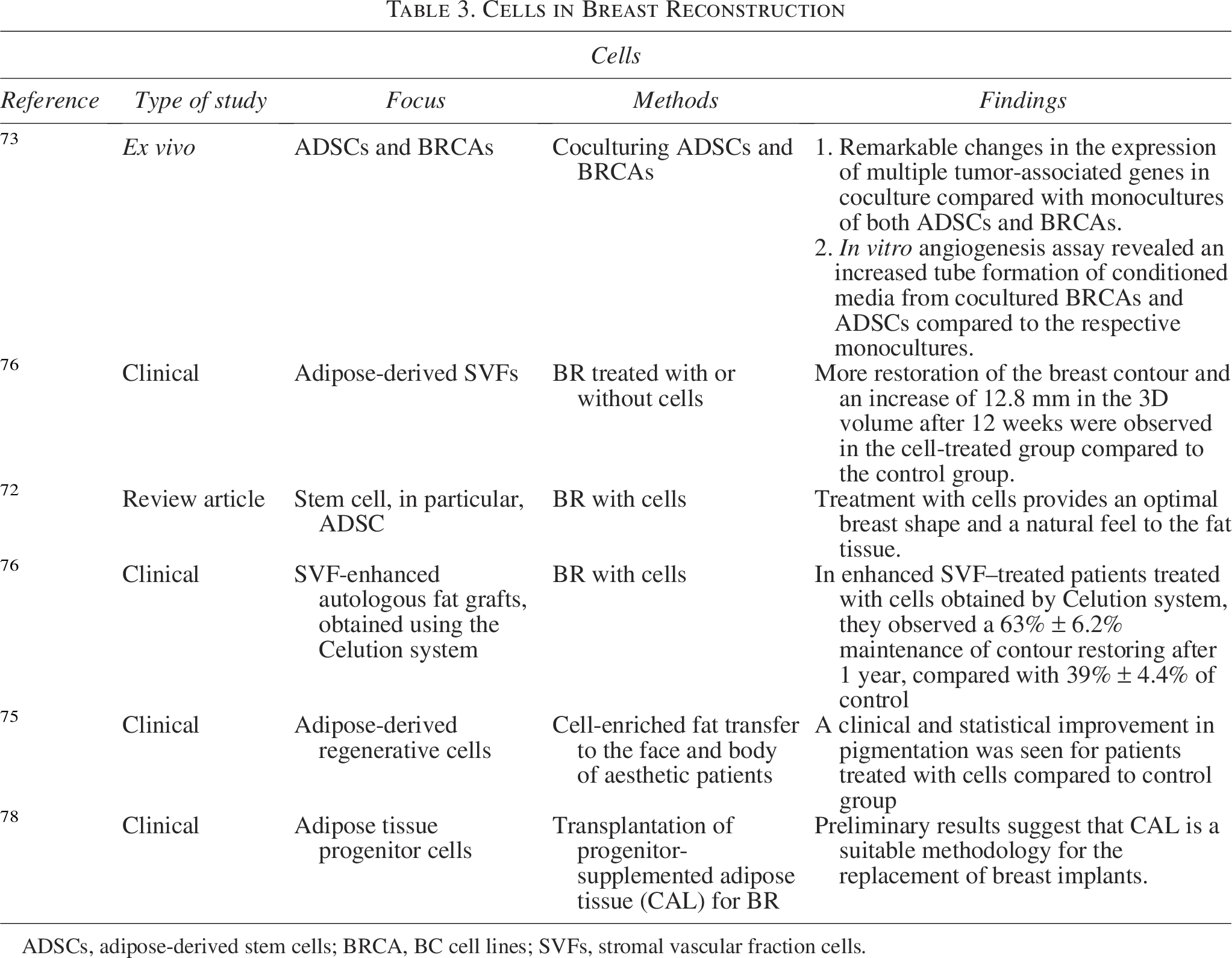
ADSCs, adipose-derived stem cells; BRCA, BC cell lines; SVFs, stromal vascular fraction cells.
A summary of TE approaches used in aesthetic BR is presented in Figure 2.54–58,63,66–72,76,78
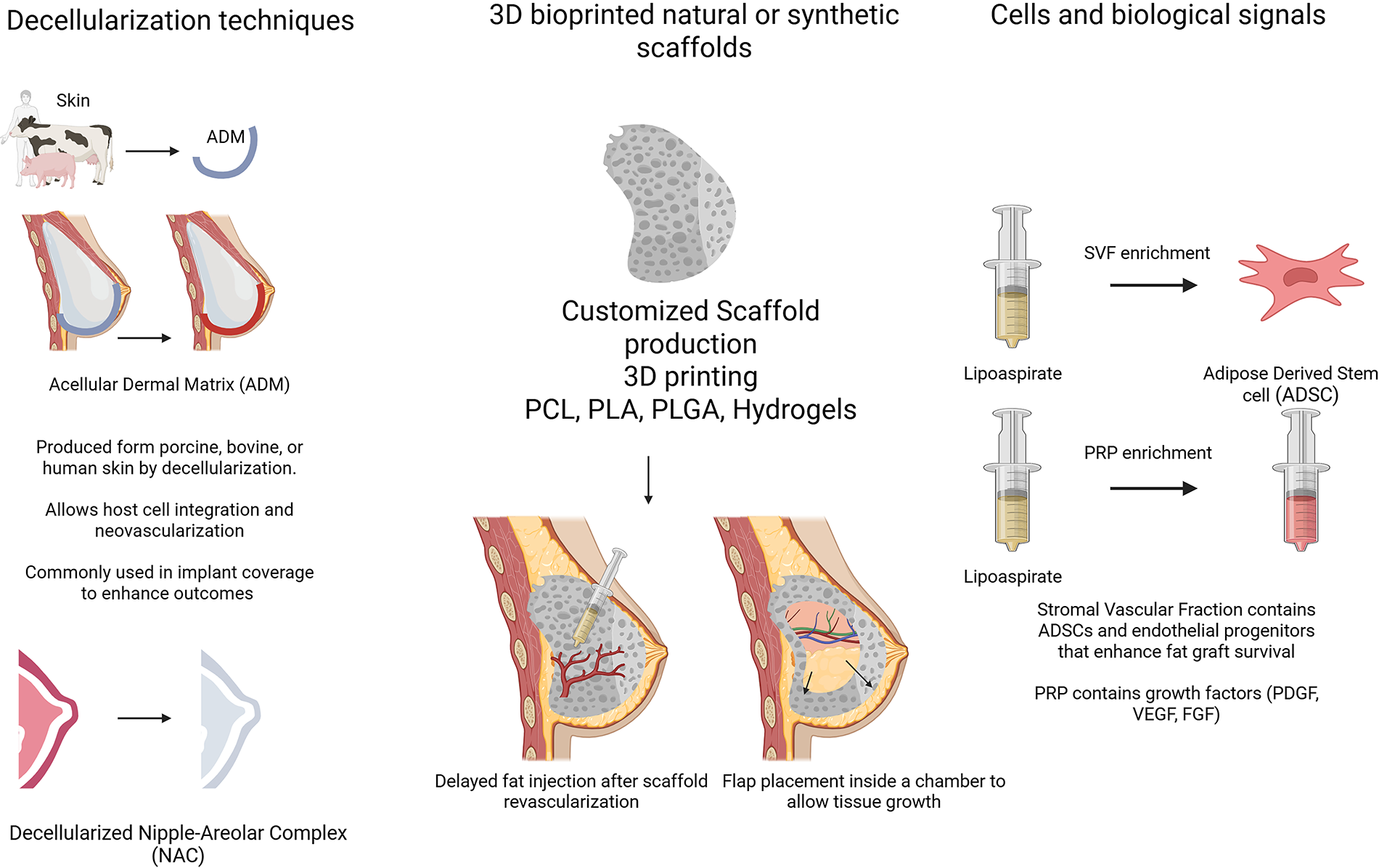
Tissue Engineering Applications in Aesthetic Breast Reconstruction.
Tissue engineering for functional breast reconstruction
To date, the literature reports relatively few studies involving mammary glands (ducts and/or alveoli). Building on this, Sumbal et al. reported in 2020 an in vitro organoid model capable of maintaining long-term lactation. In this study, the authors documented sustained milk production and stable morphology of lactating organoids over a 14-day culture period. 79 Later, Jia et al. were the first to publish a mammary organoid culture system that models mammary gland development and the lactation process in ruminants. 80 Another direction of research involves human breast organoid models. These 3D organoids replicate key features of human mammary tissue, enabling research on milk production, hormone response, and breast biology. They are derived either from induced pluripotent stem cells or patient breast tissues and are cultured within specialized ECM to form structures that closely resemble human breast alveoli and ducts. 81 Hasenauer et al. were the first to publish an in vitro mammary duct/alveoli model. The authors described a printed model based on mammary ECM seeded with human milk-derived mammary epithelial cells (MECs). As a result, the MECs formed stable epithelial layers on the printed surfaces and secreted β-casein and milk fat globules. These results hold great promise for advancing both basic research in mammary gland biology and lactation. 26
Together, these studies highlight the growing potential of bioengineering to more accurately replicate mammary gland structure and function. Such models offer valuable platforms for advancing research in lactation biology, breast development, and are used to replicate or regenerate breast tissue in a controlled, functional way.
Discussion
Despite significant advances, breast TE still faces several critical limitations that hinder its clinical application. One major challenge lies in replicating the complex architecture of the breast, which includes adipose tissue, connective tissue, vasculature, nerves, and functional glandular components such as ducts and alveoli. Although TE provides tools for generating the breast’s ECM, no studies to date have successfully engineered the entire organ. Nevertheless, the literature offers foundational insights that could support such developments, for example, the anatomical dissection described by Lartizien et al., which outlines a vascularized porcine abdominal flap encompassing the full breast structure and may serve as a platform for future studies in this direction. 82
Another key obstacle is achieving sufficient vascularization, as engineered tissues require a stable blood supply to survive and integrate after implantation. Promoting angiogenesis within ECM scaffolds or other 3D-printed structures remains one of the greatest challenges in TE overall. 83 Additionally, while most current efforts focus on aesthetic reconstruction, restoring breast functions such as lactation and hormonal responsiveness has proven challenging. The development of scaffold materials that accurately mimic the mechanical and biochemical properties of the native ECM also remains challenging.
Furthermore, immunogenic responses, including inflammation or rejection of implanted materials, further complicate clinical translation. Finally, the lack of long-term data remains a significant barrier to bringing engineered breast tissue solutions into clinical use.
Conclusion
BR after mastectomy remains a complex challenge due to limitations in available donor tissues, complications associated with adjuvant BC treatments, and the need for more biologically compatible and durable solutions. Current methods, such as implant-based reconstruction, use of autologous tissue, and allogeneic methods, offer promising outcomes but still present limitations, including donor site morbidity, prolonged treatment periods, and limited tissue integration. TE, including the development of decellularized matrices, 3D-printed scaffolds, and stem cell-based therapies, offers an exciting avenue to address these limitations. These methods aim to create aesthetically pleasing textures, achieve symmetry, withstand radiation, provide the option for immediate reconstruction (single surgery), eliminate the need for donor sites, reduce the risk of rejection, and ensure oncological safety. Future perspectives in BR lie in the advancement of tissue-engineered solutions that offer improved biocompatibility, reduced rejection, and enhanced regenerative capabilities. Further work is needed to optimize the “off-the-shelf” bioengineered breast. Moreover, surgical innovation is not only dependent on technical and scientific progress but is also closely linked to the psychosocial evolution of society and medical professionals. It is important to stimulate the creative minds that contribute to this field.
Authors’ Contributions
A.S. contributed to the literature search, writing the original draft, and design of in-house figures and tables. C.D., F.C., F.B., B.T, and G.K. contributed to the literature search and design of in-house figures. S.H. contributed to supervision. All the authors read and approved the final article.
Footnotes
Disclosure Statement
All the authors have read the article and declare no conflict of interest. No writing assistance was utilized in the production of this article.