
Abstract
Osteochondral (OC) defects, involving simultaneous damage to articular cartilage and subchondral bone, remain clinically challenging due to the distinct biological, mechanical, and structural characteristics of each layer. Traditional repair techniques are limited by poor integration and inadequate tissue regeneration. 3D bioprinting has emerged as a promising strategy to fabricate biomimetic OC constructs with precise spatial control over scaffold architecture, cell distribution, and bioactive cues. This review summarizes recent advancements in additive manufacturing techniques and their applications in OC tissue engineering. Scaffold design strategies are discussed, along with the selection of biofunctional materials. Special focus is given to recent progress in bioink development, including the precise incorporation of growth factors, zonal patterning of stem cells to guide region-specific differentiation, and the integration of bioceramics to enhance osteogenic potential while supporting chondrogenic matrix formation.
Impact Statement
Osteochondral (OC) defects present a persistent clinical challenge because of the distinct yet integrated properties of cartilage and subchondral bone. Traditional repair strategies often fail due to poor tissue integration and inadequate regeneration. This review highlights how 3D bioprinting enables precise spatial control over scaffold architecture, cell distribution, and bioactive cues to fabricate biomimetic OC constructs. We present recent advances in bioprinting technologies, bioink innovations, and scaffold design strategies, while identifying remaining challenges and translational barriers. By providing a critical and timely overview, this work offers a roadmap to advance bioprinting approaches toward clinically relevant OC tissue regeneration.
Introduction
According to the World Health Organization, joint pain and limited mobility affect approximately 500 million people worldwide, accounting for about 7% of the global population. Among various joint-related conditions, osteochondral (OC) defects are particularly prevalent, with up to 20.8% of knee arthroscopies detecting such injuries. 1 Current clinical interventions—including microfracture, subchondral drilling, and total joint replacement—fail to fully restore native tissue architecture and function.2–5 These approaches are especially unsuitable for younger patients due to long-term complications associated with implants. Biological grafts (autografts and allografts) also present limitations, such as donor-site morbidity, immune rejection, and poor integration.6,7 Collectively, these shortcomings highlight an urgent need for engineered scaffolds and in vitro models to better understand and regenerate complex joint tissues.
The challenge of OC tissue engineering lies in replicating the intricate composition, mechanical properties, and functional gradients of native tissue. OC tissue comprises three distinct zones—articular cartilage (AC), calcified cartilage (CC), and subchondral bone—each characterized by unique cellular populations, extracellular matrix (ECM) composition, and biomechanical behavior.8,9 Replicating this multizonal structure—with gradients in collagen fiber orientation, matrix composition, and stiffness—poses a significant engineering challenge. Moreover, many current scaffold designs lack the spatiotemporal control needed to mimic the dynamic changes in mechanical properties, degradation, and bioactivity observed in native OC tissue. This often results in poor structural integrity and inadequate cellular differentiation, particularly in maintaining distinct cartilage and bone phenotypes. These limitations stem, in part, from the inadequacies of conventional biomaterials and fabrication methods, as well as challenges in chondrocyte use, including low isolation efficiency, limited proliferative capacity, and rapid phenotypic drift.10,11
To overcome these barriers, stem cell-laden scaffolds have emerged as promising alternatives, offering improved regenerative potential. Achieving functional tissue regeneration, however, requires advanced biomaterial systems and next-generation manufacturing platforms capable of providing precise spatial and temporal control over cell behavior.12,13 In this context, 3D bioprinting offers unique advantages for addressing these complex design criteria and enabling more effective OC repair strategies. 14 This review highlights recent advances in 3D bioprinting for OC defect treatment, with the goal of informing future research and clinical translation.
Native OC Tissue Structure and Function
OC tissue is structurally, biochemically, and mechanically complex, posing a major challenge for regenerative medicine and scaffold design. It is composed of three distinct but integrated layers, each with unique composition, architecture, and mechanical properties (Fig. 1).8,9 The AC is a 2–4-mm-thick, avascular hyaline cartilage primarily made of water, type II collagen, and proteoglycans.17,18 It is subdivided into superficial, middle, and deep zones, with collagen fibril orientation varying to resist shear, tension, and compression. 18 The tidemark defines the boundary between the deep AC zone and CC, marking the transition from nonmineralized to mineralized tissue. 8 CC functions as a mineralized interface that anchors collagen fibrils from AC and facilitates integration with the underlying (subchondral bone) SB. 19 The cement line demarcates the CC-SB boundary, with no continuous collagen fibrils crossing this junction, reflecting a clear structural shift. 20 The vascularized bone matrix primarily consists of type I collagen and hydroxyapatite (HA), providing mechanical stability and load-bearing capacity. 9 Mechanical properties vary significantly across layers: AC shows low stiffness (0.5–0.9 MPa),21–24 CC exhibits a higher modulus (70–600 MPa), 25 and SB reaches the highest stiffness (800 MPa–1.5 GPa).25,26 These gradients enable effective shock absorption and load distribution but create a major challenge for designing biomimetic scaffolds. In summary, the hierarchical architecture, distinct composition, and gradient mechanical properties of OC tissue demand highly specialized material strategies for successful regeneration and functional scaffold development.
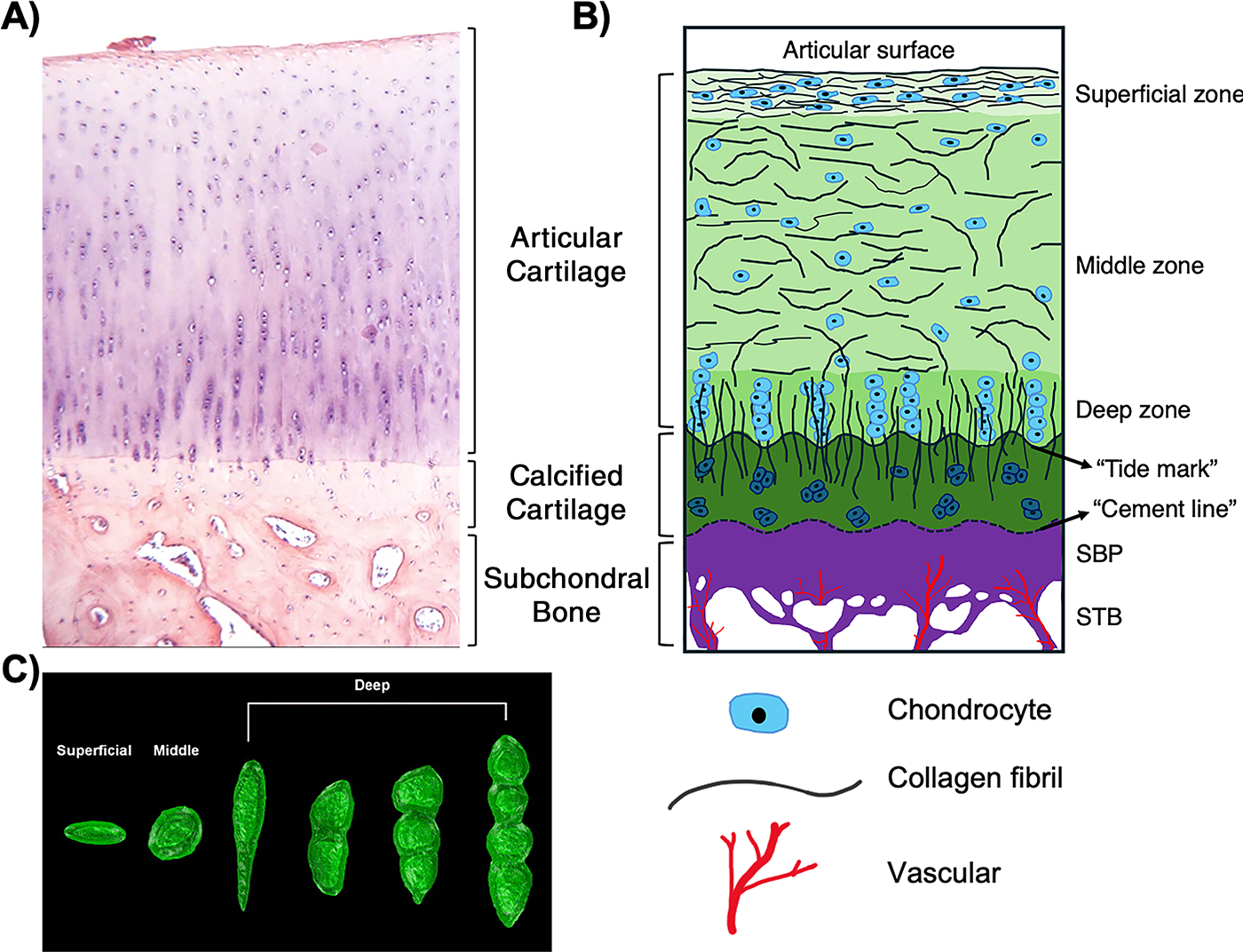
Zonal organization and microstructure of human osteochondral tissue.
With ongoing advancements in biomaterial formulations, bioink development, and bioprinting approaches, 3D bioprinting continues to push the boundaries of regenerative medicine, paving the way for personalized, on-demand tissue and organ replacement as well as disease models for drug screening and development.27–31 Fabricating OC constructs presents challenges due to the structural and compositional complexity of the OC tissue. Designing the OC scaffold involves several key considerations, including scaffold architecture, ink design, cell source, and incorporation of bioactive factors (Fig. 2). Each of these factors plays a crucial role in ensuring the effectiveness and functionality of the scaffold in promoting tissue regeneration and mimicking the native ECM of OC tissue, as discussed in the 3D Bioprinting Technologies for OC Tissue Engineering section below.
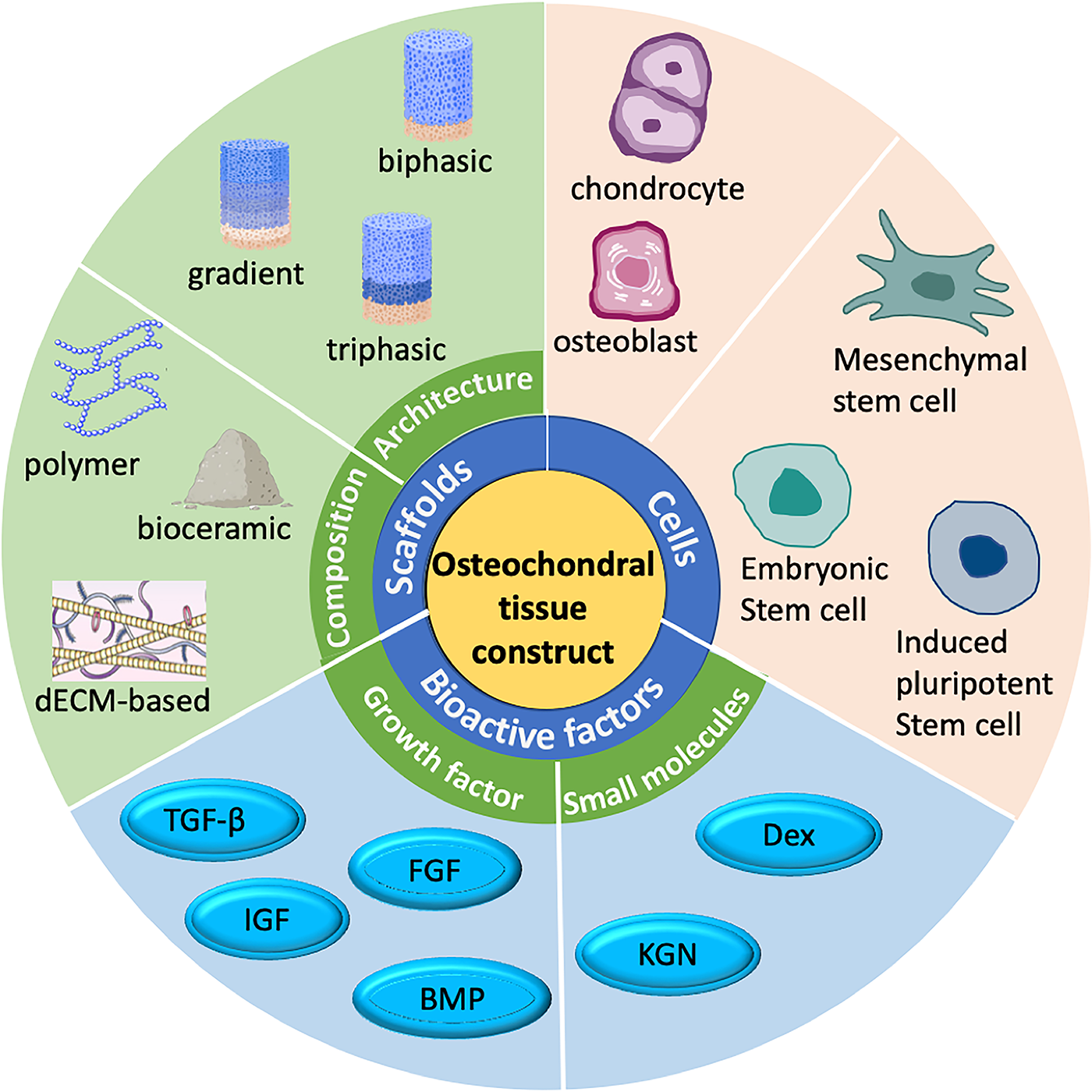
Sketch showing the design criteria for osteochondral (OC) tissue. TGF-β, transforming growth factor-β; IGF, insulin-like growth factor; FGF, fibroblast growth factor; BMP, bone morphogenetic protein; KGN, kartogenin; Dex, dexamethasone.
3D Bioprinting Technologies for OC Tissue Engineering
OC scaffolds were primarily created using manufacturing methods that focus simpler geometries. Freeze-drying, electrospinning, gas foaming, and sol–gel-based fabrication remain highly relevant (Table 1), particularly in commercialized OC implants such as MaioRegen®, Agili-C™, ChondroMimetic®, and TruFit™. Recent studies have also demonstrated the potential of hybrid fabrication approaches that combine multiple scaffold fabrication techniques to overcome the limitations.36,45,48 For instance, electrospinning combined with gas foaming has been used to fabricate integrated 3D scaffolds with a natural and continuous interface between cartilage and bone layers, reducing postimplantation delamination and enhanced cellular infiltration. 49 However, they lack the spatial precision and bioactive patterning capability required for accurate OC biomimicry. Bioprinting’s unique ability to control material composition, cell location, and architectural cues across multiple length scales establishes it as the most promising platform for fabricating hierarchical and functional OC tissue constructs, making it the emerging leader for next-generation OC repair scaffolds.
List of Different Nonprinting Fabrication Methods Used for Osteochondral Scaffolds
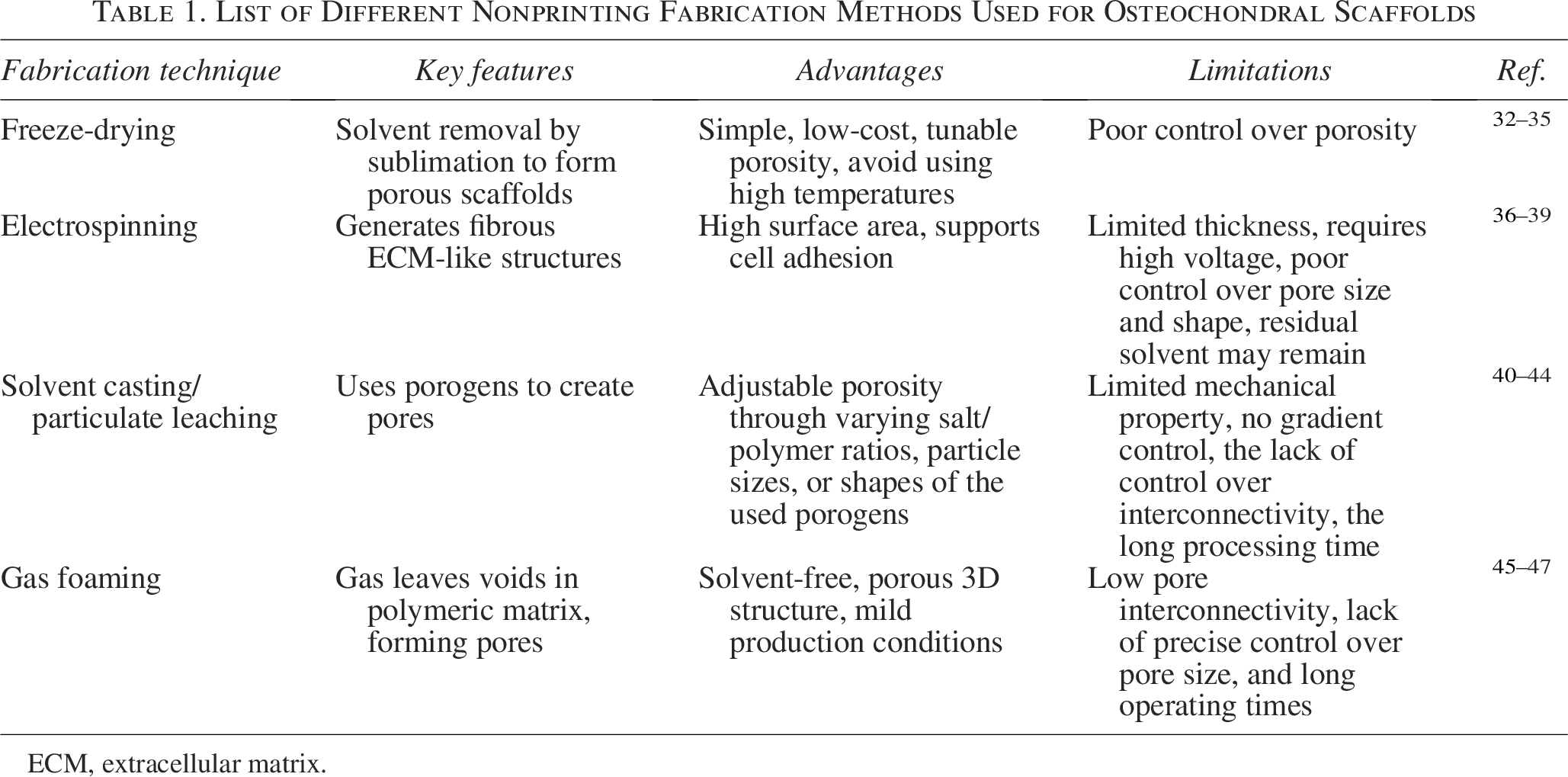
ECM, extracellular matrix.
Bioprinting techniques
3D bioprinting must operate under mild, cell-friendly conditions to preserve viability during fabrication, which restricts the choice of compatible techniques.50,51 For example, fused deposition modeling, a common extrusion-based approach, involves extruding thermoplastic filaments—often combined with ceramics or metals—at elevated temperatures (140–250°C), rendering it unsuitable for cell-laden constructs.52,53 For OC tissue engineering, three major bioprinting techniques—droplet-based bioprinting (DBB), vat photopolymerization-based bioprinting, and extrusion-based bioprinting—are commonly used. Each offers distinct advantages and limitations based on resolution, bioink compatibility, cell loading, and structural requirements (Table 2).
Comparison of Different Bioprinting Techniques

DISW, direct ink writing.
Droplet-based bioprinting
DBB deposits cell-laden droplets with high spatial precision using thermal, piezoelectric, or electrohydrodynamic mechanisms, enabling high-resolution patterning of multiple cellular structures (5–600 μm). 68 It is well-suited for low-viscosity bioinks (3.5–12 mPa/s) yet maintains high cell viability (70–90%, depending on DBB modality).68–71 DBB enables precise patterning of multiple cell types and is capable of fabricating zonally organized OC constructs. For instance, Graham et al. 57 demonstrated high-resolution DBB (≤200 μm) of OC constructs using 1 nL droplets containing ovine mesenchymal stem cells (MSCs) (oMSCs) at densities of ∼107 cells/mL. The oMSCs differentiated into cartilage-like tissue producing type II collagen. Fabrication of layered constructs with oMSC-derived osteoblasts and primary chondrocytes confirmed the potential of the platform for OC tissue engineering.
Despite its precision, DBB faces limitations for OC applications: it requires low-viscosity bioinks, restricting materials that mimic subchondral bone mechanics; discrete droplet deposition hinders the interconnected porosity needed for nutrient diffusion; constructs are prone to swelling or shrinkage; and slow printing speeds limit fabrication of large or clinically relevant scaffolds. 68
Vat photopolymerization-based bioprinting
Vat photopolymerization-based bioprinting, including stereolithography (SLA) and digital light processing (DLP), fabricates 3D constructs by curing liquid resins layer-by-layer without a nozzle, minimizing shear stress and enabling high-resolution printing of bioinks with viscosities from 102 to 104 mPa·s. 55 For example, SLA has been used to create GelMA scaffolds loaded with MSC-derived exosomes and cartilage ECM, promoting chondrocyte migration, cartilage regeneration, and subchondral bone formation in vivo. 72 Similarly, Zhu et al. 73 demonstrated that SLA could preserve cell viability and growth factor bioactivity. By encapsulating TGF-β1-loaded core–shell nanospheres within the GelMA/polyethylene glycol diacrylate (PEGDA) constructs, the authors significantly enhanced MSC chondrogenic differentiation, highlighting the potential of this method for cartilage regeneration. To enable printability across multiple platforms—including extrusion, inkjet, and DLP—rheological modifiers such as xanthan gum and nanofibrillated cellulose were incorporated. Among these, HAMA-based DLP bioinks demonstrated the highest cell viability. 74 This performance was attributed to DLP’s gentle processing conditions, which avoid shear-induced damage common in extrusion and inkjet-based methods.
Although vat photopolymerization offers high resolution and preserves cell viability, its use in OC tissue engineering is limited by narrow bioink compatibility, potential cytotoxicity from photoinitiators, complex handling, and high equipment costs. 75 Advances in visible-light initiators, hybrid biomaterials, and multivat systems are addressing these issues, positioning the technique as a promising tool for creating zonally organized, functional OC scaffolds. 76
Extrusion-based bioprinting (direct ink writing)
Extrusion-based bioprinting, commonly referred to as direct ink writing (DIW), is the most widely used and versatile technique for OC tissue engineering. This method involves the deposition of cell-laden hydrogels or composite inks through a nozzle using pneumatic or mechanical (piston- or screw-driven) force. DIW accommodates a broad range of viscosities (30–6 × 107 mPa/s) and allows high cell loading, making it compatible with numerous bioinks, including reinforced composites. 51 A key advantage of DIW is its capacity to create large, stable constructs with spatially controlled composition, where multimaterial printing enables seamless integration of bioinks with varied mechanical, chemical, and biological properties.77–79 This capability is particularly advantageous for recreating the heterogeneous and hierarchical architecture of native OC tissue, which transitions from soft cartilage to mineralized bone.
DIW enables layered or gradient deposition of hydrogels, ceramics, and reinforcing polymers, replicating stiffness transitions, zonal cell environments, and spatial bioactive cues—key for region-specific stem cell differentiation and scaffold integration.80–83 Bioceramics such as HA or β-tricalcium phosphate (β-TCP) can be incorporated in bone regions, while softer hydrogels (e.g., GelMA, alginate) form cartilage zones. Limitations include shear-induced cell stress, which can reduce viability, and lower resolution compared with droplet- or vat-based methods.84,85 Nevertheless, DIW remains the most practical, scalable approach for producing robust, multimaterial, and functionally zoned OC scaffolds.
Embedded bioprinting
Embedded bioprinting has emerged as a versatile approach for fabricating complex 3D tissue constructs, particularly in OC tissue engineering. In the freeform reversible embedding of suspended hydrogels technique, bioinks are extruded into a temporary support medium, commonly composed of jammed or granular microgels due to their shear-thinning and self-healing behavior, allowing needle motion during printing and rapid solidification afterward.86,87 This enables the creation of soft, delicate, and anatomically relevant architectures with overhanging features, hollow channels, and layer-specific gradients that are otherwise difficult with conventional extrusion printing.88–91 Furthermore, aspiration-assisted bioprinting (AAB) complements embedded printing by enabling precise positioning of spheroids: aggregates are aspirated from a cell media reservoir and deposited into a support medium with high spatial accuracy. 92 This enhances cell–cell interactions and allows the formation of highly organized, multicellular structures. 93 Ayan et al. 94 achieved a scaffold-free OC interface using differentiated adipose-derived stem cell (ADSC) spheroids—chondrogenic on top and osteogenic on the bottom—positioned within a sacrificial alginate matrix using the AAB technique. This approach yielded a bilayer construct with distinct tissue zones and preserved phenotypes. Although AAB provides high precision, its slow printing speed, spheroid preparation requirements, and complex setup limit scalability. Achieving spatially controlled ECM cues in this technique to guide cartilage and bone formation still remains a key challenge.
Recently, Abaci et al. 58 introduced a 3D embedded bioprinting approach using photocurable hydrogels (MeHA, MeAlg) with tunable viscosity to fabricate dense multicellular constructs. Unlike traditional shear-thinning supports, these hydrogels provide long-term structural stability and mimic the ECM, enabling spatiotemporal control of cell-instructive cues. The method allows multimaterial printing with localized variation in hydrogel composition and incorporation of osteoinductive agents such as TCP and BMP-2, directing stem cell differentiation regionally. This strategy effectively modulates cell–matrix interactions and site-specific osteogenesis, offering a versatile platform for engineering heterogeneous OC interfaces.
Design of OC scaffolds
The formation of the OC unit is instructed by the use of a biomaterial scaffold, which acts as a structural foundation and a source of biological cues that mirror the native tissue. Furthermore, designing constructs that closely mimic the native OC architecture is crucial, as it promotes seamless integration between regenerated cartilage and subchondral bone while ensuring stable anchorage to the surrounding native tissue. 95 The necessary layered structure could be achieved by designing the scaffold with multiple phases and incorporating various biochemical factor gradients, and current state-of-the-art design leverages 3D bioprinting to overcome these issues by precisely engineering constructs that directly mimic the native hierarchical tissue structure. Specifically, bioprinting facilitates the fabrication of gradient scaffolds by enabling the gradual blending of bioinks across layers, transitioning smoothly from soft, highly hydrated polymers in the superficial zone to stiff, ceramic-based composites in the subchondral bone, thereby establishing a functional stiffness gradient.96,97 This control extends to creating a depth-dependent porosity gradient as it is a factor in the microenvironment and an impact on cell differentiation, 98 with dense structures at the articular surface to maintain avascularity, progressing to large, interconnected pores in the bone layer to promote vascularization and osteointegration.99,100 The alignment of collagen fibrils is also a factor that contributes to the formation of functional tissue architecture, as studies have shown that a controlled fiber arrangement enhances chondrogenesis101,102 and demonstrated enhanced chondrogenesis using scaffolds with specific fiber alignment fabricated via electrostatic flocking. However, this specific technique is generally limited to fabricating monophasic scaffolds, making direct application to the necessary biphasic OC constructs challenging. Conversely, bioprinting techniques offer the advantage of a controlled, multidirectional fiber alignment,103–105 which shows significant potential for fabricating the complex, hierarchical scaffolds required to accurately mimic the OC interface.
The scaffold design for OC regeneration must combine material selection and structural architecture to replicate native tissue complexity. Native OC tissue features layered organization with biological, biochemical, and mechanical gradients from cartilage to subchondral bone. Over the past two decades, scaffold strategies have evolved from simple monophasic designs to biphasic, triphasic, and gradient-based constructs that better mimic this zonal hierarchy (Fig. 3). Biphasic scaffolds feature distinct cartilage and bone layers, while triphasic designs add a transitional layer mimicking CC to improve mechanical and biological integration.77,106–109 However, interfacial bonding remains a challenge, as mismatched properties can cause delamination. 110 Gradient scaffolds address this by providing continuous transitions to better replicate native architecture and enhance integration with the host tissue.76,111 While 3D bioprinting offers a viable platform, consistent functional outcomes are difficult across studies. Progress will require integrating materials science, bioengineering, and manufacturing to develop scaffolds that accurately replicate native OC structure–function relationships.
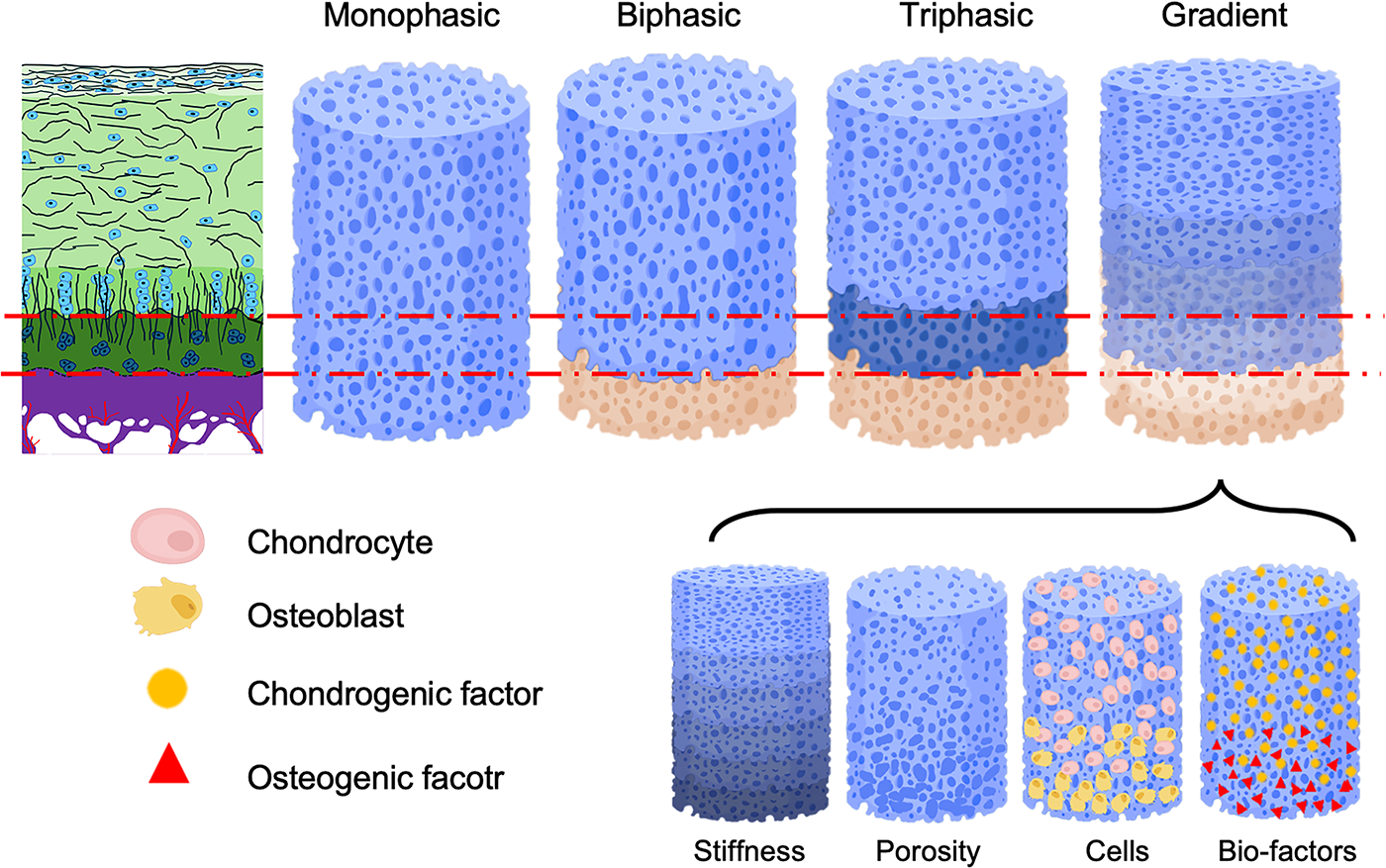
Illustration of scaffold design strategies for osteochondral (OC) regeneration (created in https://BioRender.com).
Bioink design principles
Fabricating functional OC constructs requires bioink formulations that can support the structural, compositional, and cellular complexity of native tissue. An effective bioink design involves several interrelated factors, including scaffold architecture, biomaterial selection, cell sources, and the incorporation of bioactive molecules (Fig. 2). Each of these elements plays a critical role in promoting tissue regeneration, mimicking the native ECM, and enabling spatially controlled differentiation of embedded cells.
Polymers and hydrogels
The choice of biomaterials is a key determinant of bioink performance in 3D bioprinting for OC tissue engineering. Ideal materials must provide sufficient mechanical support, allow for precise printing resolution, and offer a biochemical environment conducive to cell survival, proliferation, and lineage-specific differentiation. Materials used in bioinks can be broadly categorized into four types: natural polymers, synthetic polymers, bioceramics, and decellularized ECM (dECM) (Table 3).
Summary of Bioink in 3D Bioprinting of Osteochondral Construct
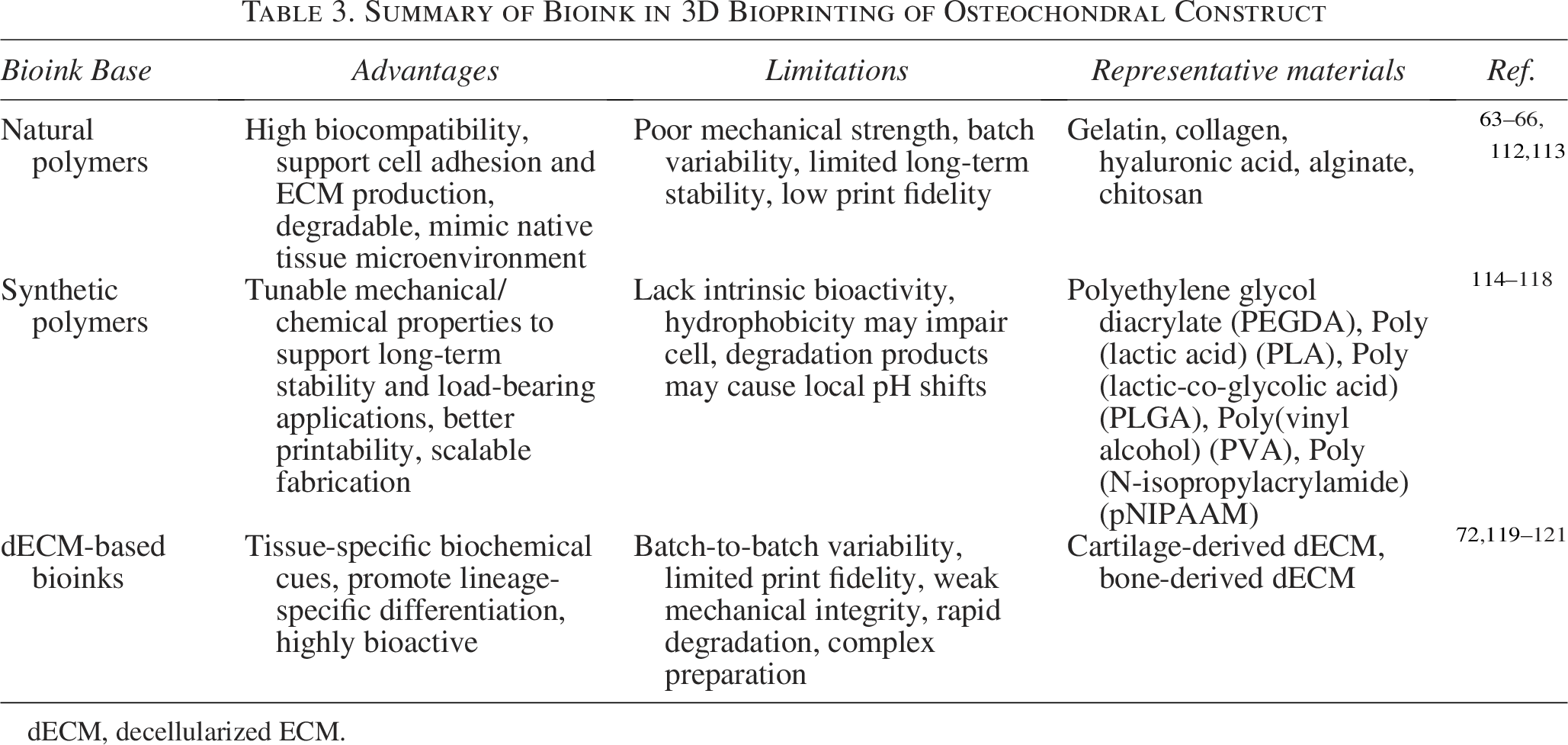
dECM, decellularized ECM.
Natural polymers such as gelatin, collagen, and hyaluronic acid offer excellent biocompatibility and bioactivity but typically suffer from poor mechanical strength and limited print fidelity.114,122–125 Synthetic polymers such as PLGA and PEGDA provide greater mechanical tunability and structural integrity but often lack intrinsic biological signaling.114,115,126 Material choice also depends on scaffold design—zonal layering or continuous gradients—which affects printability, structural fidelity, and the spatial control of stem cell differentiation.
Biological components and additives
Cell selection is critical for OC scaffold function. Commonly used cells include MSCs, induced pluripotent stem cell (iPSC)-derived chondrocytes and osteoblasts, primary chondrocytes, and preosteoblasts. MSCs are favored for their ease of isolation, proliferation, dual chondrogenic–osteogenic potential, low immunogenicity, and minimal ethical concerns.127–130 iPSCs offer pluripotency and long-term expansion but are limited by complex differentiation protocols and tumorigenicity risks.131,132 Primary cells face low yield, dedifferentiation, and poor ECM production.5,86 While MSCs are a versatile choice, achieving spatially distinct chondrogenic and osteogenic differentiation within a single scaffold requires precise control of scaffold architecture, bioink composition, and localized biochemical cues, emphasizing the need for advanced, spatially regulated design strategies.
Growth factors are essential for creating a bioactive microenvironment in OC scaffolds, guiding cell behavior and tissue regeneration. Key factors include TGF-β isoforms for chondrocyte maturation,133–135 BMPs for osteoblast differentiation,136,137 IGF-1 for cartilage homeostasis, 138 FGFs for chondrogenesis, and dexamethasone for both chondrogenic and osteogenic differentiation.139–141 Small molecules such as kartogenin also promote cartilage repair.141–143 However, many of these cues are unstable in vivo, limiting their efficacy, and thus, strategies are being used to improve controlled release, bioavailability, and targeting.
Bioceramics such as HA and β-TCP and bioactive glass are widely used in bioinks. HA provides long-term stability, while TCP degrades faster, releasing Ca2+ and PO4³−, yielding a sustained supply of calcium and phosphate for bone matrix mineralization.144–146 Bioactive glass releases inorganic ion (e.g., Si, Sr) enhancing angiogenesis and osteoconductivity.147,148 dECM-based bioinks, derived from cartilage or bone tissues, retain tissue-specific signaling molecules, native ECM proteins alongside mineral cues, creating a more physiologically relevant environment.58,119,149,150 However, they are typically incorporated into bioinks as reinforcing particle additives rather than used as primary matrix materials. In 3D bioprinting for OC engineering, HA (<200 nm; 1–50 µm),151–153 TCP (1–10 µm),59,153,154 and decellularized bone particles (<500 µm)58,119,149,155 are widely used, where nanoparticles enhance bioactivity through enhancing osteoblast adhesion, proliferation, and protein absorption,156,157 and microparticles provide structural reinforcement and sustained osteoinductive cues. 158
Advances in Bioinks and Bioprinting for OC Tissue Regeneration
In OC tissue engineering, one of the central challenges is achieving coordinated differentiation of stem cells into both chondrogenic and osteogenic lineages within a single construct. Bioink design plays a critical role in overcoming this challenge. Three key strategies have emerged and the section below reviews recent advances in these areas, highlighting innovative approaches, technical challenges, and future directions for enhancing the functional regeneration of OC tissue.
Delivery of biological cues for OC regeneration
One promising approach for promoting dual-lineage differentiation within OC constructs involves the incorporation of biological cues—specifically growth factors—into the scaffold matrix. By carefully selecting and immobilizing these cues within the spatially defined regions of the scaffold, it is possible to create localized microenvironments that direct stem cells toward either chondrogenic or osteogenic lineages, but precise deposition and sustained release remain challenging.
Reversible host–guest interactions have emerged as a robust platform for the sustained and localized delivery of bioactive molecules.80,82 Dai et al. developed a dynamic bioink of dopamine-functionalized GelMA and acrylate β-cyclodextrin that enhances mechanical strength and enables sustained drug release (Fig. 4A). 82 The bilayer scaffold featured a stiff, melatonin-loaded bone layer and a softer, kartogenin-loaded cartilage layer. Encapsulated human ADSCs responded to localized cues, producing the tissue-specific ECM. In vitro (14 days) and in vivo (12 weeks) tests showed effective OC regeneration, although separate layers with differing stiffnesses may reduce interfacial integration.
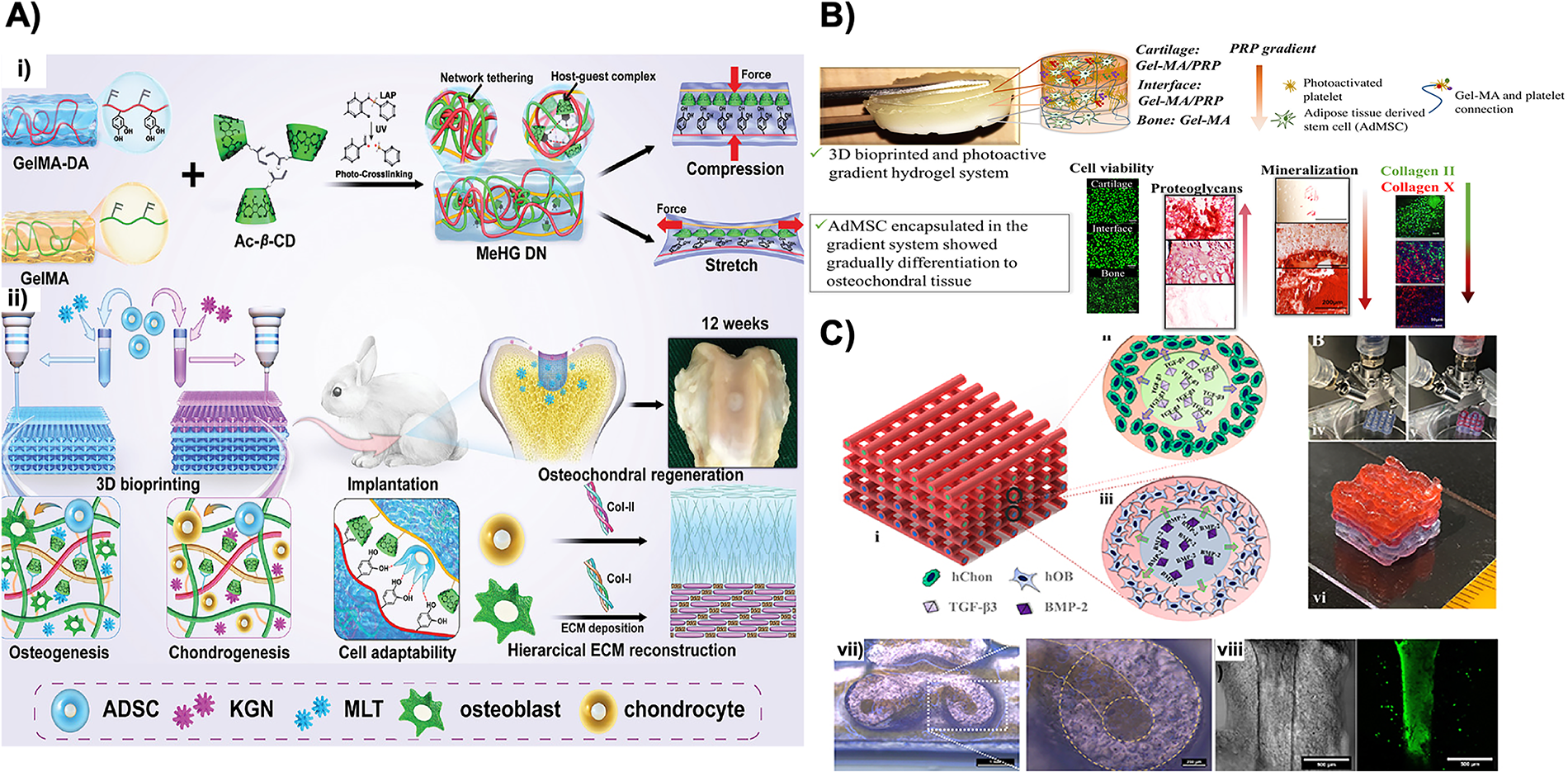
Gradient-based delivery of biological cues is another promising strategy. Irmak et al. 97 created a gradient OC scaffold using ADSCs in platelet-rich plasma (PRP)–GelMA bioinks to form cartilage, interface, and bone regions (Fig. 4B). PRP provided growth factors, activated by near-infrared light to form a fibrin network that enhanced cue retention. The construct supported zonal tissue development in vitro over 21 days, enabling spatial and temporal control of stem cell differentiation. Extrusion-based core–shell bioprinting also enables spatially confined delivery of lineage-specific cues. Kilian et al. 159 fabricated OC scaffolds with compartmentalized hydrogel strands containing human articular chondrocytes and human preosteoblasts in separate layers (Fig. 4C). Alginate–methylcellulose bioinks with laponite enabled shear-thinning and controlled release of TGF-β3 and BMP-2, promoting region-specific chondrogenic and osteogenic differentiation over 21 days in vitro. Challenges remain in interfacial bonding and long-term factor retention.
Matrix-driven spatial control of stem cell differentiation
Spatial control of stem cell differentiation in OC scaffolds is achieved by tuning bioink properties such as stiffness, viscoelasticity, and ligand presentation. Stiffness gradients mimicking native cartilage-to-bone transitions guide MSCs toward chondrogenic or osteogenic lineages, while ligand density and ECM composition regulate cell adhesion, spreading, and migration. This precise control enables scaffolds to direct patterned differentiation and form integrated tissue layers.
Zhang et al. 160 developed a bilayer scaffold using a bioink composed of dECM and silk fibroin to replicate the native architecture of OC tissue (Fig. 5A). The dECM provides a biologically relevant environment that closely mimics the native ECM, supporting MSC adhesion, proliferation, and differentiation. 163 However, dECM-based bioinks typically lack mechanical robustness due to the degradation of native tissue structure during processing. To overcome this limitation, the authors combined dECM with silk fibroin, enhancing mechanical strength and printability.121,164 A PCL frame was printed to reinforce the bone layer, followed by cartilage- and bone-specific hydrogels derived from dECM. MSCs in these zone-specific matrices showed enhanced chondrogenic and osteogenic differentiation, supported by incorporated TGF-β and BMP-2. However, the absence of controlled release posed a risk of burst release, potentially limiting long-term efficacy.
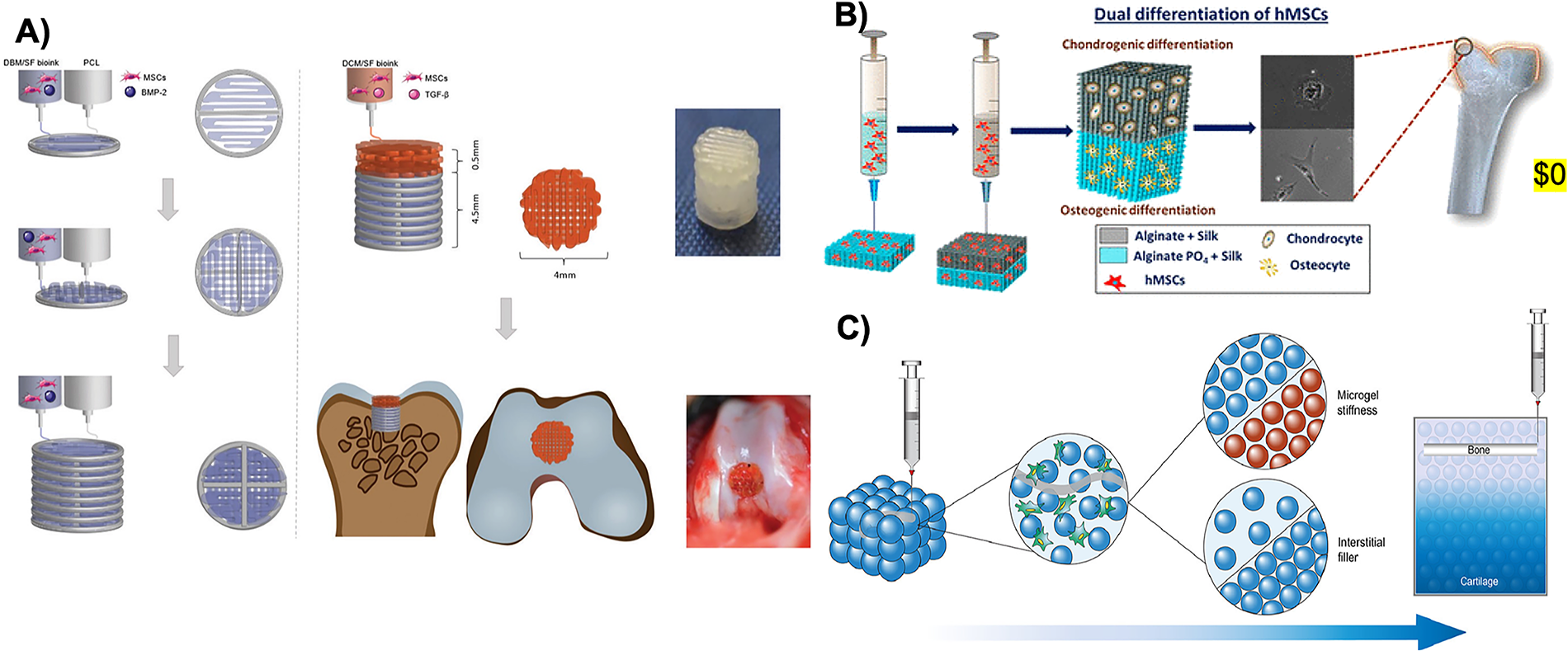
In a related approach, Joshi et al. 161 developed alginate–silk fibroin bioinks for spatially guided hMSC differentiation without exogenous growth factors (Fig. 5B). Phosphate-grafted alginate promoted osteogenesis, while unmodified alginate–silk supported chondrogenesis, enabling dual-lineage differentiation in self-supporting constructs. The bioink showed good printability and cell support, but uniform fiber distribution was challenging, causing mechanical heterogeneity. The phosphate-grafting step could be replaced with bioceramics such as TCP to provide similar osteoinductive effects.
Jalandhra et al. 162 used microgel-based GelMA suspensions to create a biphasic OC scaffold with tunable stiffness (Fig. 5C). Bone and cartilage compartments were optimized separately for osteogenesis and chondrogenesis, with stiffness gradients and interstitial hydrogel volumes mimicking the native OC interface. A jammed microgel bone region promoted osteogenesis, while a softer cartilage matrix supported chondrogenesis. Calcium phosphate ceramic ink added localized mineral content. The scaffold guided ADSC differentiation without growth factors over 21 days in vitro, but printing resolution and interfacial fidelity were not assessed, limiting the evaluation of construct integrity.
Bioceramic-based bioinks for OC applications
Bioceramic-based bioinks offer a promising strategy for promoting dual-lineage differentiation of stem cells within OC scaffolds. Bioceramics closely mimic the mineral composition of native bone and exhibit intrinsic osteoconductive and osteoinductive properties.108,165–167 When incorporated into bioink formulations, these particles can create a favorable microenvironment for osteogenic differentiation. Furthermore, by designing bioceramic-loaded scaffolds with spatially defined architecture and incorporating growth factors, it is possible to simultaneously promote chondrogenesis in the cartilage layer and osteogenesis in the bone layer. Despite these advantages, research on bioceramic-based bioinks for full OC regeneration remains relatively limited.
Yu and colleagues 83 developed a biphasic OC scaffold with a GelMA hydrogel core, incorporating strontium-substituted calcium silicate hydrate (Sr-CSH) nanowires in the subchondral bone layer (Fig. 6A). The Sr-CSH improved mechanical strength and osteoinductivity, supporting BMSC adhesion and osteogenesis. The cartilage layer used unmodified GelMA with cocultured articular chondrocytes and BMSCs, utilizing paracrine signaling to promote chondrogenesis. The scaffold showed good in vitro integration over 7 days and successful OC regeneration in vivo over 12 weeks. Limitations include a cartilage bioink not optimized for chondrogenesis and potential chondrocyte dedifferentiation. Quin et al. 79 bioprinted a biphasic scaffold with bioceramic-integrated bioinks (Fig. 6B). The top hydrogel layer contained chondrocytes for cartilage, while the bottom layer combined MSCs with Lithium-Magnesium-Silicon (Li–Mg–Si) bioceramics to promote osteogenesis. In vitro and in vivo results confirmed osteogenic differentiation and enhanced OC defect repair. A limitation is the reliance on predifferentiated chondrocytes, which introduces donor variability, limited expansion, and phenotypic instability.
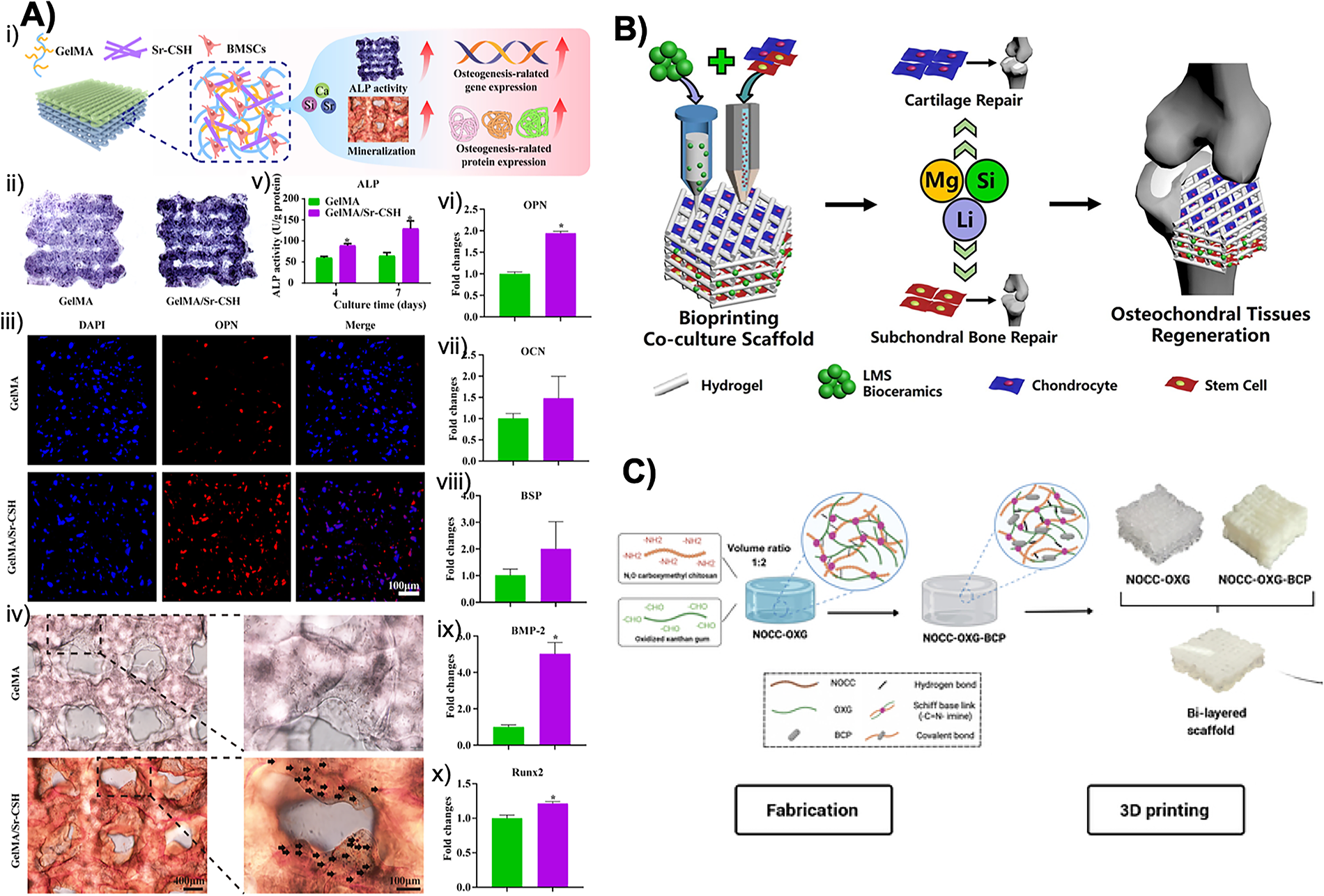
Bioceramic-based scaffolds for OC repair are generally effective in supporting the bone layer due to their osteoconductive properties; however, to induce dual-lineage regeneration without relying on chondrocytes for the cartilage layer, alternative strategies such as mimicking the native ECM porosity can be used to enhance chondrogenesis. To address the need for improved chondrogenic support, Nguyen et al. 107 developed a bilayered OC scaffold with biphasic calcium phosphate (BCP) for bone and a hydrogel of N,O-carboxymethyl chitosan and oxidized xanthan gum for cartilage (Fig. 6C). The cartilage layer featured ECM-like pores (90–300 μm) to support nutrient diffusion and cell interactions, while the bone layer contained 60% BCP to enhance osteointegration and mechanics. In vitro and in vivo tests showed effective OC regeneration. A limitation is the lack of bioactive chondrogenic cues in the cartilage phase, reducing its ability to guide stem cell differentiation without additional factors or predifferentiated cells.
Dense cellular constructs printed within biphasic MeHA support matrices demonstrated tunable osteogenic responses through modulation of matrix composition. 58 Lower MeHA concentrations (5%) promoted enhanced hMSC spreading and aspect ratio, leading to increased local osteogenesis. At a constant 10% MeHA, incorporation of TCP nanoparticles significantly stimulated osteogenic differentiation, with ALP activity increasing ∼1.9-fold and calcium deposition ∼1.6-fold. 58 Similarly, MeHA hydrogels reinforced with bone allograft particles or TCP supported hMSC constructs with high viability and stable mechanics. 59 The addition of bone particles markedly enhanced osteogenesis, as shown by elevated ALP activity and calcium deposition, even in basal media, with effects scaling with particle concentration.
Collectively, bioceramic-based bioinks offer considerable potential for OC, but their ability to support chondrogenesis remains limited unless combined with additional strategies such as growth factor delivery, matrix tuning, or coculture systems. Future studies should focus on integrating bioactivity for both layers, enabling stem cell-based, growth factor-free approaches that better mimic the native OC interface.
Concluding Remarks and Future Directions
3D bioprinting has emerged as a powerful tool for OC tissue engineering, offering precise control over scaffold architecture, material composition, and spatial cell distribution. Recent progress in bioink development, including the incorporation of biological cues, spatial regulation of stem cell fate, and use of bioceramic-based matrices, further supports functional regeneration. Despite notable advances, 3D bioprinting of OC constructs faces several critical challenges. First, achieving high-fidelity replication of the native OC interface is limited by current printing resolution and gradient control. Long-term in vivo data are scarce, hindering validation of tissue integration, remodeling, and function. Vascularization of the subchondral bone also remains unresolved, as incorporating vessels without disrupting the avascular cartilage layer is technically complex. 168 Moreover, while extensive research exists on bone or cartilage regeneration individually, relatively few studies have addressed the fabrication of integrated, full-thickness OC constructs. This gap highlights the need for more comprehensive strategies that consider the functional coupling between these two distinct yet interdependent tissues.
Bioprinted OC scaffolds face major challenges, including maintaining high cell viability and phenotype, stabilizing growth factors with precise spatiotemporal delivery, and achieving reproducible spatial organization of cells, proteins, and mechanics. Scaling up production further complicates translation, while regulatory approval demands extensive validation. Regulatory approval, such as FDA clearance, requires extensive preclinical and clinical validation to demonstrate safety, efficacy, and quality control, making clinical implementation a slow and resource-intensive process. Future work should focus on smart bioinks, controlled bioactive signaling, and dynamic culture systems to enable clinically viable, structurally and functionally integrated OC grafts.
Authors’ Contributions
H.T.: Performed the comprehensive literature search, synthesized the collected data, prepared the figures and tables, and wrote the initial draft of the manuscript. M.G.: Conceptualized the study framework, provided critical intellectual input, and supervised the study.
Footnotes
Funding Information
This study is funded by the National Science Foundation grant (2044479).
Disclosure Statement
No competing financial interests exist.