
Abstract
Alternative therapies are needed for heart failure following myocardial infarction (MI), as ischemic cardiomyopathy remains a major global health concern despite advances in acute MI management. Platelet-rich plasma (PRP), which is enriched with cytokines and growth factors, holds therapeutic potential in ischemic cardiovascular diseases. However, its clinical application remains unrealized due to the absence of a reliable delivery approach. An epicardial patch provides a spatially stable delivery system on the heart surface. This approach becomes particularly attractive when combined with biodegradable controlled-release hydrogels that prolong and localize factor release. Therefore, combining these two modalities into an epicardial hydrogel patch offers a novel and efficient strategy for targeted PRP delivery. This study evaluated the feasibility and therapeutic efficacy of a biodegradable gelatin hydrogel patch, incorporating PRP and designed for epicardial use, in a rat MI model. PRP was prepared via double-spin centrifugation and activated with calcium chloride. In vitro, cytokine and growth factor levels (transforming growth factor-beta 1 [TGF-β1], platelet-derived growth factor-BB [PDGF-BB], insulin-like growth factor-1 [IGF-1], vascular endothelial growth factor [VEGF]) were quantified using enzyme-linked immunosorbent assay. PRP contained TGF-β1, PDGF-BB, and IGF-1; VEGF was undetectable. Release kinetics were measured under nonenzymatic and collagenase conditions. The hydrogel provided controlled release, especially of TGF-β1, for 5 days in vitro. In vivo, MI was induced by ligating the left anterior descending artery in rats. The epicardial hydrogel patch was placed at the infarct center, covering a fibrin–collagen sealant patch. The patch remained in place for 10 days and degraded by day 20. Cardiac function was evaluated via echocardiography through day 28, after which hearts were harvested for histological infarct analysis. Serial echocardiographic evaluations revealed that the PRP group demonstrated less decline in systolic function (fractional area change) from the hyperacute phase (day 1) to the chronic phase (day 28). Morphological assessments demonstrated that the PRP group had smaller left ventricular end-diastolic dimensions from day 7 onward. Histological evaluation confirmed greater infarcted wall thickness and myocardial area within the infarcted region compared with controls. Therefore, the epicardial delivery of PRP via a controlled-release hydrogel patch attenuated cardiac dysfunction from the hyperacute to the chronic phases and mitigated adverse ventricular remodeling.
Impact Statement
This study highlighted the cardioprotective effects of platelet-rich plasma (PRP) after myocardial infarction (MI) using a novel epicardial delivery system. A biodegradable hydrogel patch was specifically designed for stable and controlled PRP release from the cardiac surface. In a rat MI model, PRP attenuated systolic dysfunction during the hyperacute phase of MI and prevented adverse left ventricular remodeling in the chronic phase. A significant finding of this study was that PRP exerted a rapid cardioprotective effect as early as day 1 after MI. This PRP delivery platform may be an alternative therapy for ischemic heart disease.
Introduction
In the clinic, the “state-of-the-art” therapy at the hyperacute stage of myocardial infarction (MI) is timely reperfusion therapy. As adjunctive therapies, antiplatelet agents, anticoagulants, and vasodilators can support reperfusion and prevent further thrombus formation in the coronary artery. However, heart failure following MI remains a major global health burden. 1 Although clinical advances in hyperacute-phase management, such as timely reperfusion therapy, have improved survival outcomes, current therapeutic strategies, including adjunctive treatments such as antithrombotic therapy and pharmacological agents, remain insufficient in preserving the myocardial structure and preventing adverse ventricular remodeling. 2 Therefore, novel adjunctive therapies represent an urgent clinical priority.
Platelet-rich plasma (PRP), a blood-derived product enriched with cytokines and growth factors, has demonstrated healing potential through anti-inflammatory and tissue-reparative mechanisms. 3 Despite the growing recognition of its therapeutic potential in the setting of MI, clinical application of PRP remains limited, partly due to the reliance on the limitations of current PRP delivery systems, such as intramyocardial injections, 4 which carry risks of mechanical injury, limited local retention, and volume restrictions.5,6 To address these limitations, epicardial patch-based delivery systems have emerged as a promising alternative. 7 This approach has the advantage of having a high volume and potential for minimally invasive delivery of bioactive substances directly to the infarcted myocardium. 8 Biodegradable controlled-release hydrogels developed by Tabata et al. represent a promising material for drug delivery systems. These hydrogels function by forming polyion complexes in response to electrical charges and are gradually degraded by collagenase in vivo, thereby enabling the controlled release of bioactive substances incorporated into the hydrogel matrix. 9 Incorporating PRP into these hydrogels has been reported to prolong the availability of cytokines and growth factors, 10 reduce their rapid degradation, 11 and be associated with therapeutic effects.12,13
Based on these findings, it was hypothesized that this approach would allow the localized and controlled release of bioactive factors included in PRP directly over the infarcted myocardium, thereby mitigating adverse ventricular remodeling and attenuating the decline in cardiac function. Specifically, the present study aimed to evaluate the feasibility and therapeutic efficacy of a biodegradable gelatin hydrogel patch, designed and optimized for epicardial application, incorporating donor-derived PRP in a rat model of MI.
Materials and Methods
All animal procedures were conducted in accordance with the Principles of Laboratory Animal Care and the NIH Guide for the Care and Use of Laboratory Animals (NIH Publication No. 86-23, revised 1985). The protocol was approved by the President of the Animal Experiments Ethical Review Committee of Nippon Medical School (Approval No. 2021-001). Female Sprague–Dawley rats (280–320 g; Tokyo Laboratory Animals Science Co., Tokyo, Japan) were used as both PRP donors and recipients. Female rats were selected to minimize variability in body weight and behavioral aggression, which can affect postoperative management and echocardiographic measurements.
Preparation of biodegradable gelatin patches
Pig skin gelatin, with a weight-average molecular weight of 100,000 and an isoelectric point of 5.0, was kindly supplied by Nitta Gelatin Co. (Osaka, Japan). Gelatin (500 mg) was dissolved in 5 mL of double-distilled water and rapidly frozen in liquid nitrogen, followed by freeze-drying for 72 h to obtain gelatin sheets. The sheets were cross-linked via dehydrothermal treatment at 140°C for 48 h in a vacuum oven and sterilized with ethylene oxide. The resulting hydrogels were molded into 1-mm-thick sheets and punched into 8-mm-diameter discs (Fig. 1A, B).
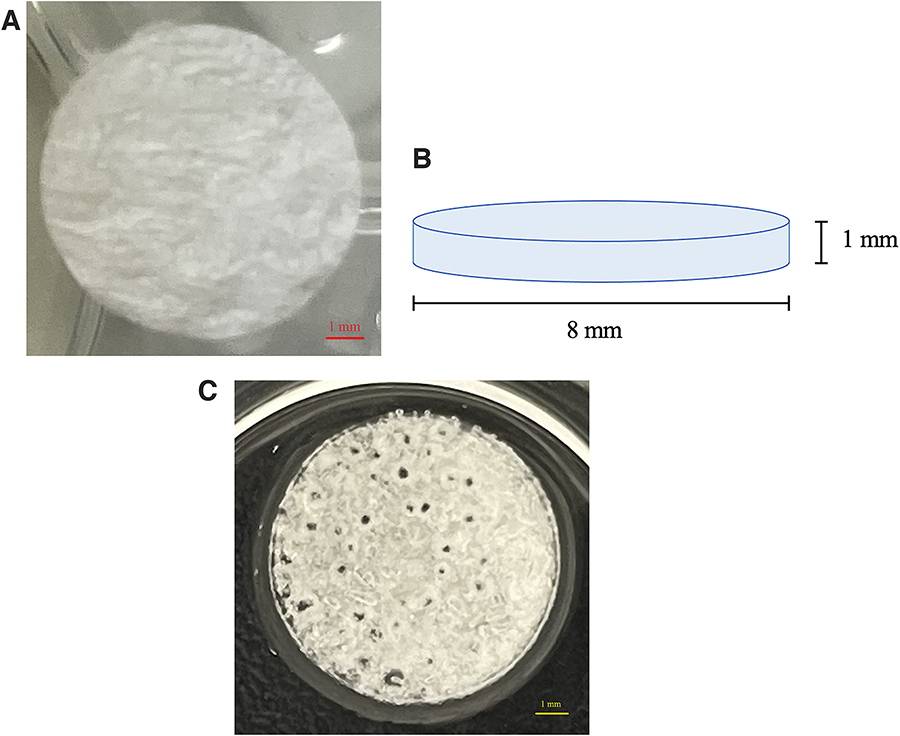
Biodegradable gelatin hydrogel patch.
Preparation of PRP
Allogeneic PRP was prepared from donor rats of the same strain. Briefly, whole blood (7–10 mL) was collected via cardiac puncture under general anesthesia with 4.0–5.0% isoflurane using an 18G needle, placed into tubes containing 1.5 mL of Acid Citrate Dextrose Solution A (ACD-A; Becton, Dickinson and Company, Franklin Lakes, NJ, USA), and centrifuged (Kubota 2700; Kubota Corporation, Tokyo, Japan). The first centrifugation was performed at 1,700 rpm (470 g) for 10 min. The plasma and buffy coat were transferred to a new tube and subjected to a second centrifugation at 2,300 rpm (850 g) for 15 min. After the second spin, the supernatant (platelet-poor plasma) and platelet pellet were separated. The pellet was resuspended in the platelet-poor plasma to a final volume of 300 μL, yielding PRP. 12 Blood cell counts were performed using an automated hematology analyzer (Celltac α; Nihon Kohden Corporation, Tokyo, Japan). In this study, PRP was defined as having a platelet concentration exceeding 300 × 104/μL and achieving ≥7-fold enrichment compared with whole blood. 3
Preparation of PRP-gelatin hydrogel patches
Each hydrogel disc was impregnated with 120 μL of a PRP-CaCl2 mixture (105 μL PRP and 15 μL 10% CaCl2; 7:1 ratio 10 ) and incubated at 37°C for 2 h with gentle stirring (Fig. 1C).
In vitro evaluation
Quantification of cytokines and growth factors in PRP
The concentrations of transforming growth factor-beta 1 (TGF-β1), platelet-derived growth factor-BB (PDGF-BB), insulin-like growth factor-1 (IGF-1), and vascular endothelial growth factor (VEGF) in the PRP were quantified using commercially available enzyme-linked immunosorbent assay (ELISA) kits, following the respective manufacturers’ protocols. Kits for TGF-β1, PDGF-BB, and IGF-1 were sourced from R&D Systems (Minneapolis, MN), whereas the VEGF kit was obtained from Abcam (Cambridge, UK). All assays were conducted in duplicate, and the concentrations were determined based on standard curves generated from known concentrations of each cytokine.
Temporal release profiles of PRP-loaded gelatin hydrogels
To evaluate the release kinetics, PRP-loaded hydrogels (n = 3) were immersed in 500 μL of phosphate-buffered saline (PBS)(+) at 37°C under gentle agitation. Under nonenzymatic conditions, samples were collected at 1 and 12 h. Thereafter, enzymatic degradation was initiated with 10 μg/mL collagenase D (Roche Diagnostics, Basel, Switzerland), 10 and additional samples were collected at 18, 24, 36, 60, 84, and 132 h. At each time point, hydrogels were retrieved using a cell strainer and secured with a monofilament suture for consistent handling. Supernatants were collected for cytokine quantification using the ELISA kits mentioned above.
In vivo evaluation
Surgical procedures for a rat MI model and epicardial patch implantation
All animals were randomly allocated into three groups (n = 6 per group) before surgery: a PRP patch group that received a PRP-loaded hydrogel patch, a PBS patch group that received a PBS-loaded hydrogel patch, and an MI-only group that received no patch application.
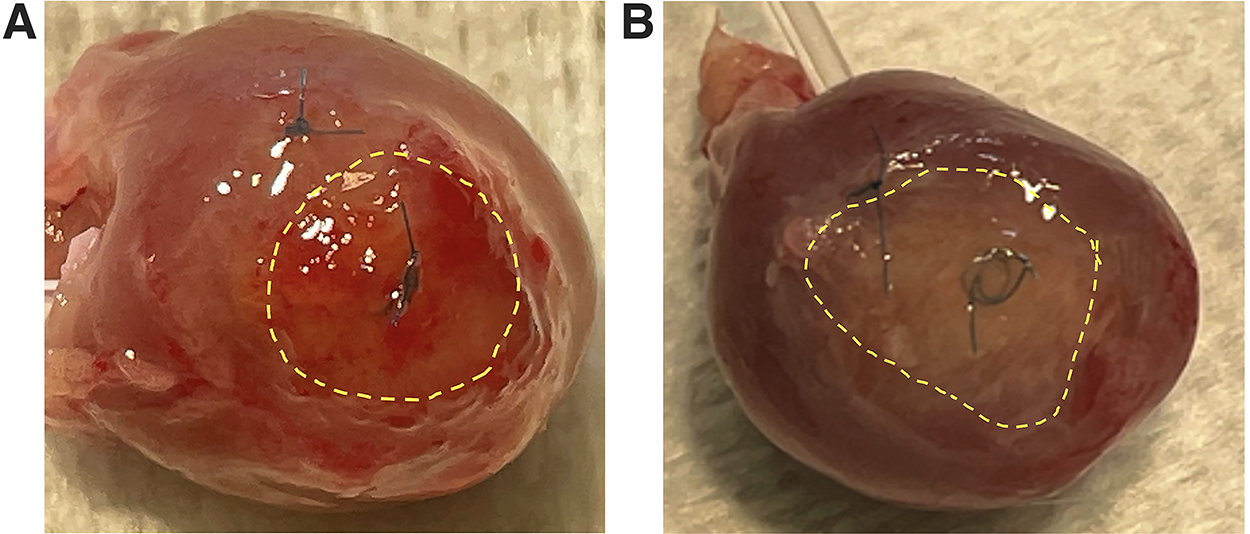
The implantation procedure is illustrated in Figure 2A. Briefly, rats were anesthetized with 2.0–3.0% isoflurane and intubated. Following left thoracotomy, MI was induced via permanent ligation of the left anterior descending coronary artery (LAD; Fig. 2B). 14 The hydrogel patch was sutured to the infarct center with a single 7-0 Prolene suture (Fig. 2C). A fibrin–collagen sealant patch (TachoSil®; 12 × 12 mm; CSL Behring, Marburg, Germany) was placed over the hydrogel, and an adhesion barrier film (Seprafilm®; 20 × 20 mm; Baxter International Inc., Deerfield, IL) was layered on top for reinforcement (Fig. 2D).
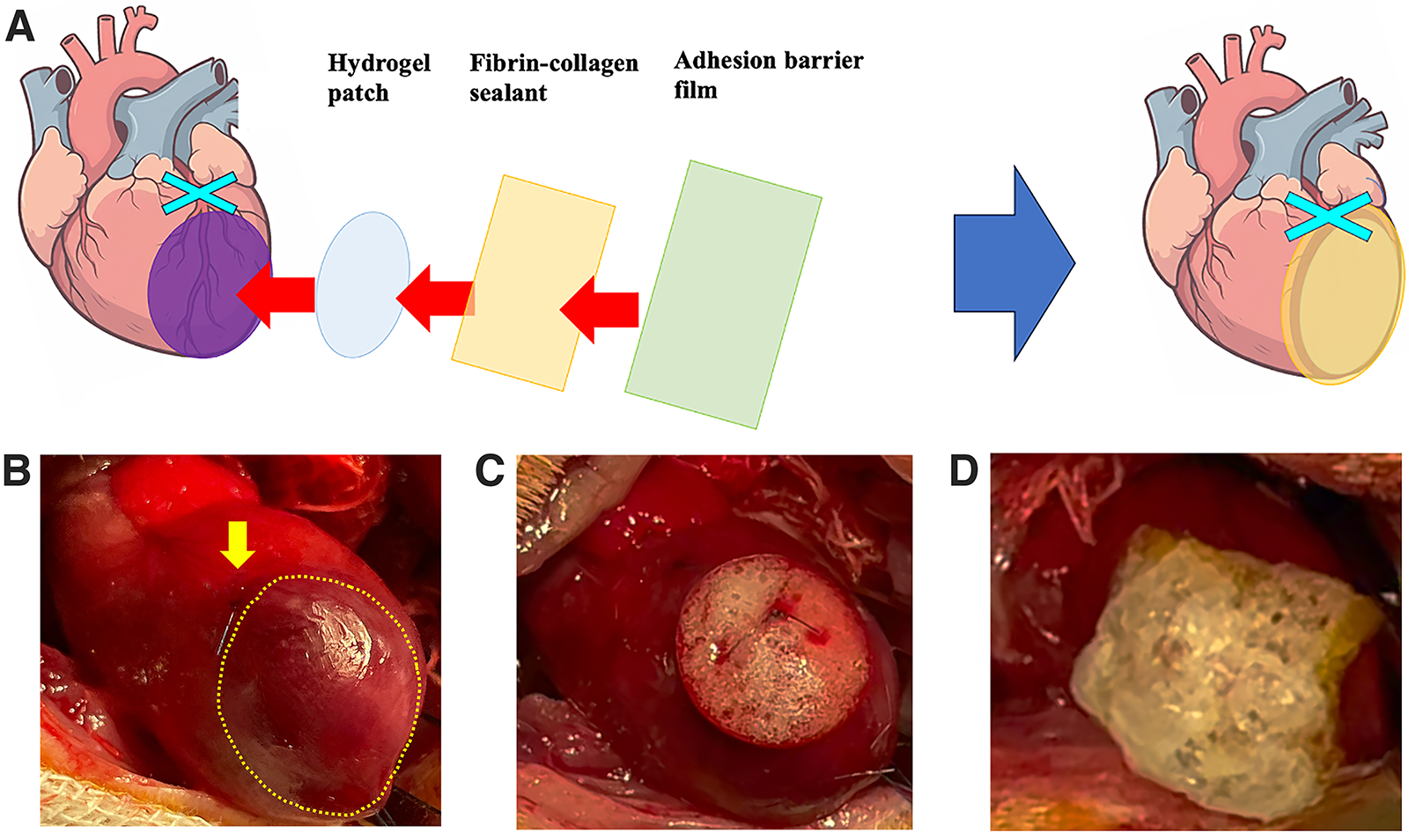
Implantation of the gelatin hydrogel patch on the heart.
Evaluation of patch retention and degradation in vivo
To assess in vivo degradation, the PRP-loaded hydrogel patch was evaluated at 10 and 20 days postimplantation (n = 3 per time point). Diastolic arrest was achieved via intravenous injection of KCl before harvesting the hearts.
Functional evaluation of the PRP patch in an MI model
Therapeutic efficacy was evaluated in three groups (n = 6 per group): (1) the PRP patch (PRP-loaded hydrogel patch), (2) PBS patch (PBS-loaded hydrogel patch), and (3) MI-only groups (no patch application). Serial echocardiographic and histological assessments were performed per group.
Cardiac Function via Echocardiography
Echocardiography was conducted preoperatively and on postoperative days 1, 3, 5, 7, 14, 21, and 28. Contrast-enhanced imaging was performed preoperatively and on postoperative days 1, 7, 14, and 28 using perflubutane microbubbles (0.04 μL microbubbles per session; Sonazoid®, GE Healthcare Japan, Tokyo, Japan),14,15 administered via tail vein injection. Imaging was performed using a diagnostic ultrasound system (ACUSON Sequoia 512; Siemens Healthineers, Erlangen, Germany) equipped with an 8V5 pediatric probe under 1.0–2.0% isoflurane anesthesia. This concentration range has been widely used in previous studies, including our own, and does not adversely affect cardiac function.14,15 The midportion view of the left ventricle was obtained from the short axis of the echocardiograph. The fractional area change (%FAC) was calculated using the formula %FAC = [(LVEDA − LVESA)/LVEDA] × 100, where LVEDA and LVESA represent the left ventricular end-diastolic and end-systolic areas, respectively. Echocardiographic assessments were performed independently by three investigators who were blinded to the treatment allocations.
Histological Evaluation
At 28 days postsurgery, the rat hearts were arrested in diastole via KCl injection, excised, and fixed. Patch degradation beneath the fibrin–collagen sealant was also confirmed. Each heart was sectioned transversely at 2-mm intervals, yielding six slices. From these, an optimal midventricular section corresponding to the papillary muscle level observed in the echocardiographs was selected for analysis. Paraffin-embedded sections (5 μm thick) were stained with Masson’s trichrome and α-SMA to evaluate fibrosis and vessel number in the infarcted lesions, respectively. Imaging and quantification were conducted using a fluorescence microscope (BZ-X800; Keyence Corporation, Osaka, Japan). The infarct region, defined as approximately 50% of the infarcted area, was designated as the border zone and was subdivided into five equal segments for measurement. The wall thickness was measured within each segment, and the region of interest (ROI) was automatically determined using imaging software (BZ-X Analyzer, Keyence Corporation, Osaka, Japan) using standardized threshold and morphology parameters. These parameters were applied consistently across all specimens to ensure objective and reproducible quantification. Histological analyses were conducted by three independent investigators who were blinded to the treatment groups.
Statistical analysis
Statistical analysis was performed using R (version 4.5.0; R Foundation for Statistical Computing, Vienna, Austria) and EZR (version 1.68; Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R. Data are presented as the mean ± standard deviation (SD). For longitudinal echocardiography data, a repeated-measures analysis of variance (ANOVA) was conducted using one between-subject factor (Groups: MI, PBS, PRP) and one within-subject factor (Time: preoperative and postoperative days 1, 3, 5, 7, 14, 21, and 28). When the assumption of sphericity was violated, the Greenhouse–Geisser correction was applied. Post hoc pairwise comparisons were performed using the Bonferroni adjustment to control for multiple testing across time points. For histological quantitative analyses and other independent group comparisons (PRP, PBS, and MI), one-way ANOVA followed by Tukey’s post hoc test was performed. Cohen’s d and the detectable effect size (Δ), derived as the half-width of the 95% confidence interval obtained from Tukey’s test, were calculated to estimate the magnitude of pairwise differences.
Results
PRP profile evaluation using ELISA
The platelet concentration in PRP (387.1 ± 47.3 × 104/μL) represented a 7.7 ± 0.6-fold enrichment compared with those in whole blood (50.3 ± 2.6 × 104/μL). In contrast, the white and red blood cell counts were markedly reduced in the PRP (WBC: 3.1 ± 2.4 × 102/μL; RBC: 5.0 ± 4.3 × 104/μL) relative to that in whole blood (WBC: 23.4 ± 5.6 × 102/μL; RBC: 677.0 ± 24.8 × 104/μL), as summarized in Table 1. Because the PRP obtained in this study contained only a small amount of leukocytes, it was classified as leukocyte-poor PRP (LP-PRP). 16
White and Red Blood Cell Counts in the PRP Relative to That in Whole Blood

PRP, platelet-rich plasma; SD, standard deviation.
The concentrations of TGF-β1, PDGF-BB, IGF-1, and VEGF are summarized in Table 2. The IGF-1 concentration in the PRP was 556.8 ± 40.8 ng/mL, whereas VEGF was not detected (<0.82 pg/mL). Fibrinogen content was not specifically measured in this study, but its presence may have contributed to the observed gelation behavior of the hydrogel.
The Concentrations of Various Growth Factors (TGF-β1, PDGF-BB, IGF-1, and VEGF)
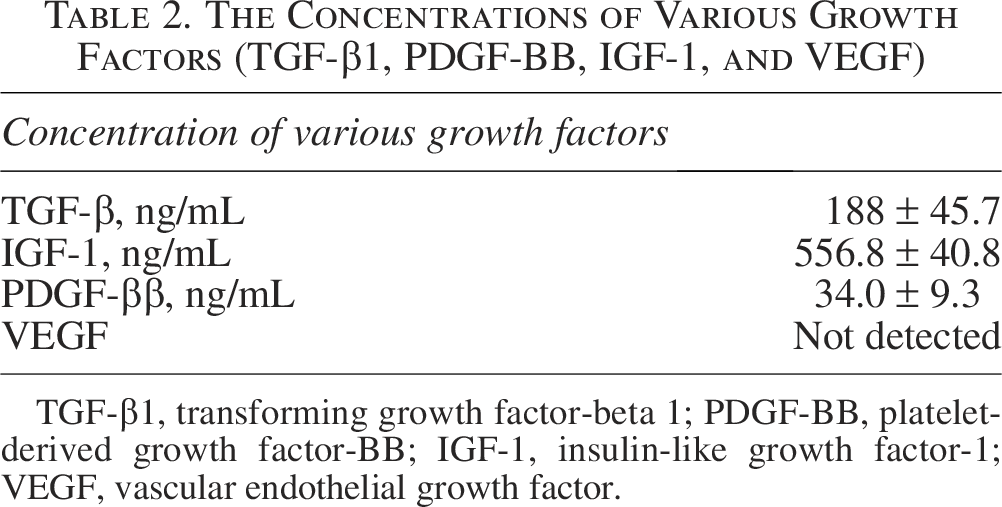
TGF-β1, transforming growth factor-beta 1; PDGF-BB, platelet-derived growth factor-BB; IGF-1, insulin-like growth factor-1; VEGF, vascular endothelial growth factor.
Evaluation of gelatin hydrogel degradation before and after collagenase treatment
Figure 3A illustrates the degradation behavior of the gelatin hydrogel before and after administration of collagenase, as observed under a stereomicroscope. In the absence of enzymatic activity, the hydrogel remained structurally intact throughout the observation period. In contrast, the administration of collagenase led to progressive hydrogel degradation. By the end of the release study (132 h), the hydrogel had largely dissolved, leaving behind a residual lumpy mass composed of PRP-derived components and remnants of the hydrogel matrix. The dry weight of the hydrogels used across all in vivo and in vitro experiments was 3.4 ± 0.2 mg.
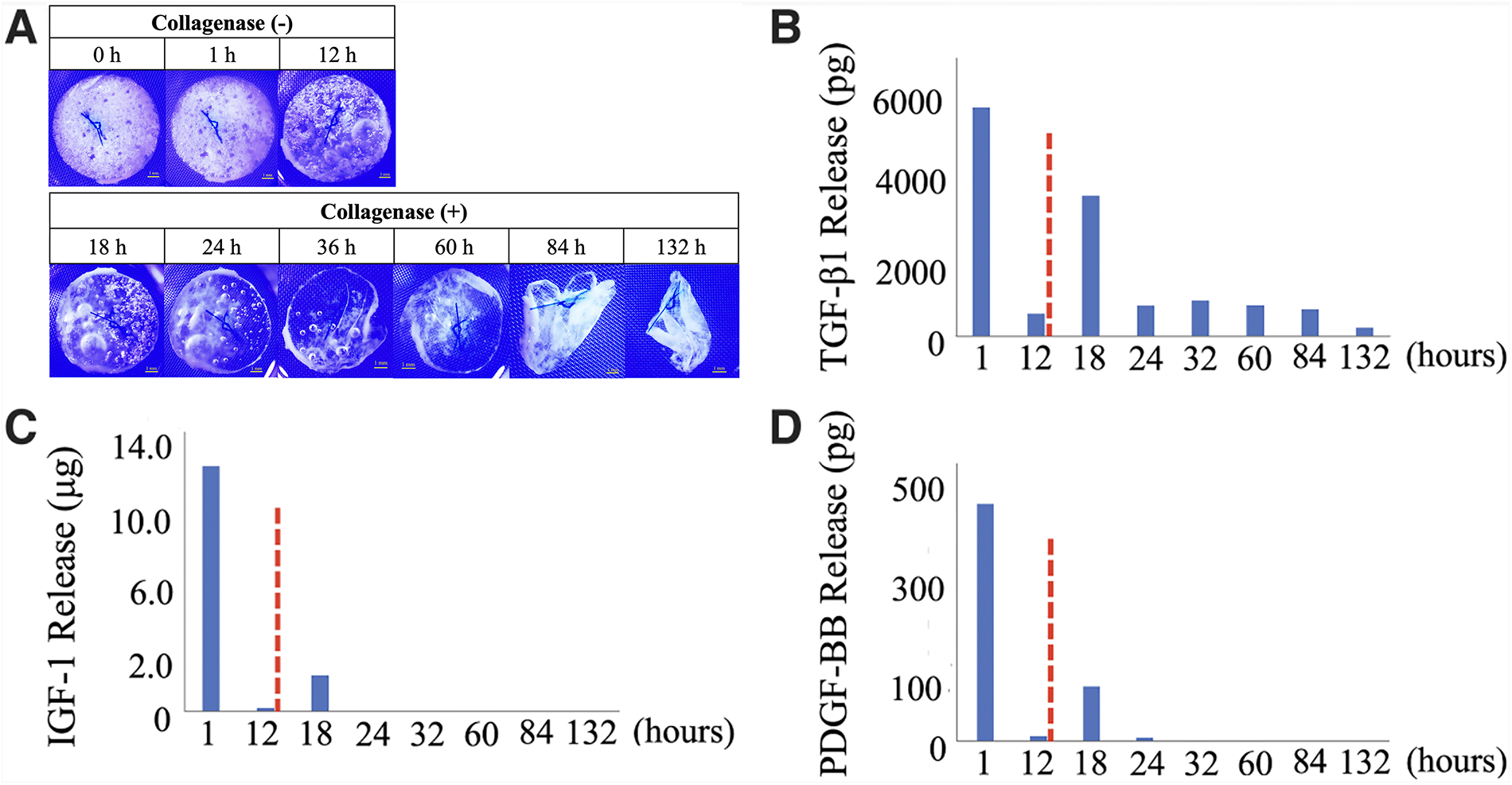
In vitro properties of the gelatin hydrogel patch.
Temporal release profiles of the biodegradable gelatin hydrogel incorporating PRP
A fast burst release of cytokines and growth factors was observed under nonenzymatic conditions, followed by a progressive increase upon exposure to collagenase D, resulting in a biphasic release profile (Fig. 3B–D). Among these, TGF-β1 exhibited controlled release lasting up to 5 days following collagenase administration (Fig. 3B), while IGF-1 and PDGF-BB showed gradual release patterns (Fig. 3C, D).
In vivo evaluation of patch properties
In the retention and degradation assessment, both the fibrin–collagen sealant and the hydrogel remained localized over and fully covered the infarcted area on postoperative day 10 in all specimens (Fig. 4A). By day 20, although the fibrin–collagen layer had diminished in size, it continued to provide sufficient coverage of the infarct region, whereas the hydrogel was no longer detectable beneath it in any specimen (Fig. 4B). The PRP-impregnated biodegradable hydrogel persisted for more than 10 days but was completely degraded by postoperative day 20. In the functional evaluation, at the time of tissue harvesting on day 28, remnants of the fibrin–collagen sealant were still observed over the infarcted area, while no visible hydrogel remained in any specimen. The adhesion barrier film was also no longer identifiable at this point. The combination of the fibrin–collagen sealant and the adhesion barrier film demonstrated stable localization on the heart surface for up to 28 days. Histological analysis using Masson’s trichrome staining revealed that although residual material was present on the surface of the infarcted area, no hydrogel components were detected. These findings confirmed complete hydrogel degradation in all specimens, consistent with the macroscopic observations.
In vivo degradation profile of the gelatin hydrogel patch.
Evaluation of the PRP patch in a myocardial infarction model
One death occurred in each of the MI and PRP groups on the day following the procedure. In the PBS group, one animal was excluded due to the absence of MI, as confirmed by echocardiographic and pathological evaluation. As a result, six animals per group initially underwent the procedure; five animals per group met the study criteria, survived until day 28, and were included in the final analysis (Fig. 5).
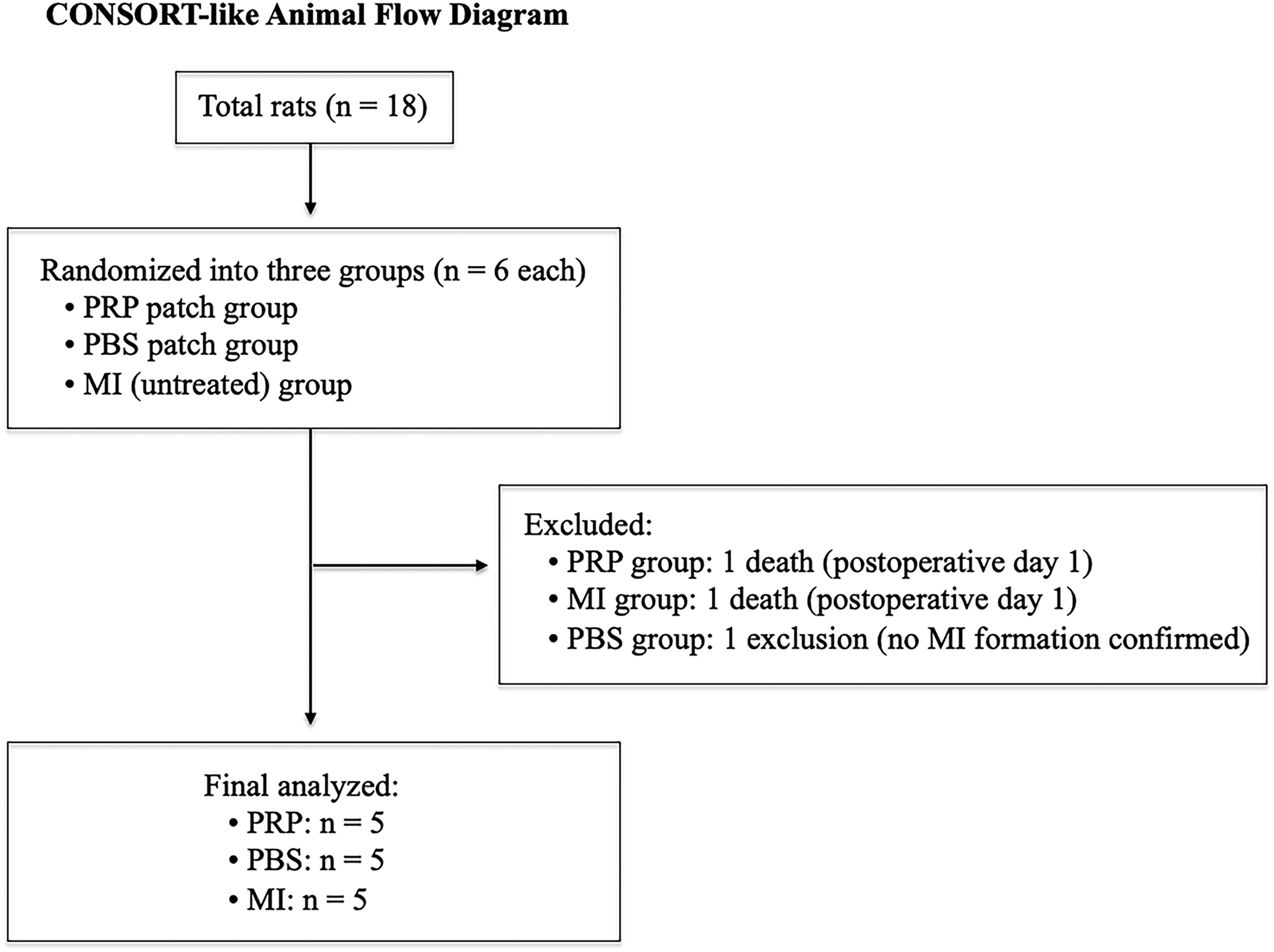
CONSORT-like animal flow diagram. This diagram summarizes the allocation, exclusions, and final number of animals included in the analysis. A total of 18 rats were initially included and randomly assigned to three groups (n = 6 per group): the PRP patch, PBS patch, and MI-only groups. One rat each in the MI and PRP groups died on the day following the procedure. Similarly, one rat in the PBS group was excluded due to the absence of myocardial infarction, as confirmed via echocardiographic and pathological evaluation. Consequently, five animals per group met the study criteria, survived until day 28, and were included in the final analysis. PRP, platelet-rich plasma; PBS, phosphate-buffered saline; MI, myocardial infarction.
Serial cardiac function via echocardiographic evaluation
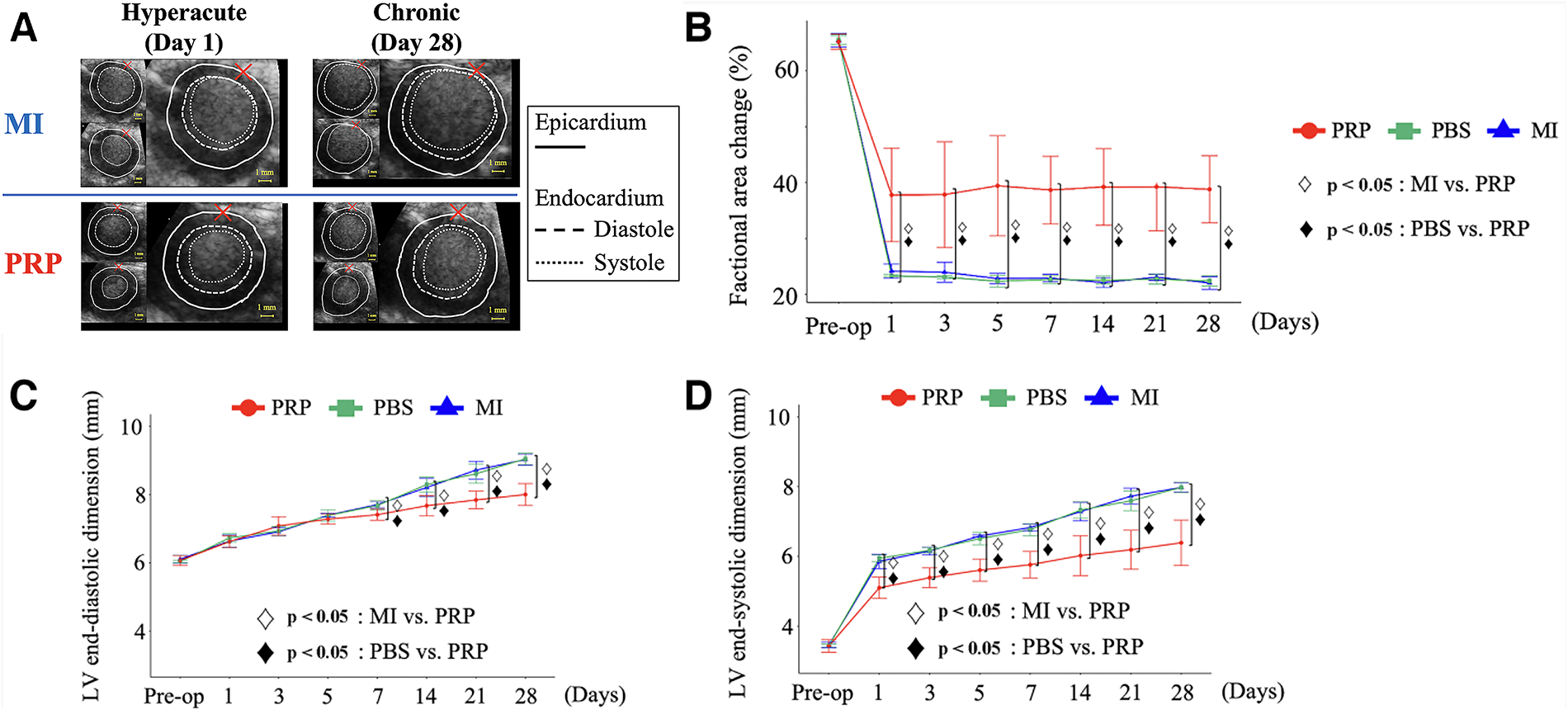
Echocardiographic measurements were successfully obtained under 1.0–2.0% isoflurane anesthesia, without resulting in excessive bradycardia or respiratory suppression that could influence cardiac function. Figure 6A shows representative echocardiography images comparing the PRP and MI groups. In the MI group, the infarct area exhibited reduced wall motion, whereas the PRP group displayed less reduced wall motion, indicating less severe impairment. In the PRP group, systolic function, as assessed by the %FAC, was moderately reduced in the acute phase but remained relatively stable thereafter. Ventricular remodeling was attenuated during the chronic phase, as reflected by changes in left ventricular end-diastolic dimension (LVDd) and left ventricular end-systolic dimension (LVDs). Although all groups exhibited asynergic wall motion in the LAD infarct region, the degree of wall motion abnormality appeared reduced in the PRP group (Fig. 6A).
Evaluation of cardiac function using serial contrast-enhanced echocardiography.
Fractional Area Change
The %FAC, a key index of systolic performance, decreased in all groups following MI. On day 1 (hyperacute phase), the reduction in %FAC was significantly less pronounced in the PRP group (37.8 ± 8.4%) compared with the MI (24.1 ± 1.1%) and PBS (23.3 ± 0.2%) groups (overall p < 0.05). Similarly, the %FAC was significantly greater in the PRP group than in the MI and PBS groups (both p < 0.05), whereas no significant difference was observed between the MI and PBS groups (p = 0.96). Notably, in the PRP group, the %FAC remained stable with no further decline on days 3 and 5. Although slight fluctuations were noted thereafter, the %FAC remained relatively high through day 28 (p < 0.05; Fig. 6B). At day 28, the %FAC in the PRP group (38.8 ± 6.0%) remained significantly higher than in the MI (22.0 ± 1.2%) and PBS (22.4 ± 0.9%) groups (overall p < 0.05). Pairwise comparisons showed greater %FAC in the PRP group compared with the MI and PBS groups (both p < 0.05), whereas no significant difference was observed between the MI and PBS groups (p = 0.99) (Supplementary Data; Table 1).
Left Ventricular End-Diastolic and End-Systolic Dimensions
The LVDd and LVDs were measured to evaluate the morphological changes in the heart following MI. On day 1, no significant differences in LVDd were observed among the groups (MI: 6.6 ± 0.1 mm; PBS: 6.7 ± 0.1 mm; PRP: 6.6 ± 0.2 mm). However, from day 7 onward, LVDd dilation was gradually suppressed in the PRP group, with values significantly smaller than those in the MI and PBS groups (PRP: 7.4 ± 0.2 mm; MI and PBS: 7.7 ± 0.1 mm; both p < 0.05). On day 7, pairwise comparisons showed significantly smaller LVDd values in the PRP group compared with the MI (p < 0.05) and PBS (p < 0.05) groups, while no significant difference was found between the MI and PBS groups (p = 0.95) (Supplementary Data; Table 1).
This difference became more evident by day 28, when the LVDd reached 8.0 ± 0.3 mm in the PRP group, compared with 9.0 ± 0.2 mm in both the MI and PBS groups (p < 0.05; Fig. 6C). Pairwise comparisons demonstrated significantly smaller LVDd in the PRP group compared with the MI and PBS groups (both p < 0.05), whereas no significant difference was found between the MI and PBS groups (p = 0.96) (Supplementary Data; Table 1). LVDd dilation was comparable among groups at baseline and on day 1; however, from day 7 onward, it was gradually suppressed in the PRP group, with this difference becoming more pronounced by day 28 (p < 0.05; Fig. 6C).
In contrast, significant differences in the LVDs were already apparent on day 1. The PRP group exhibited smaller LVDs (5.1 ± 0.3 mm) compared with the MI (5.9 ± 0.2 mm) and PBS (5.9 ± 0.1 mm) groups (overall p < 0.05). Pairwise comparisons showed lower LVDs in the PRP group compared with the MI and PBS groups (both p < 0.05), whereas no significant difference was observed between the MI and PBS groups (p = 0.80). By day 28, the LVDs in the PRP group remained significantly lower (6.4 ± 0.7 mm) than in the MI (8.0 ± 0.1 mm) and PBS (8.0 ± 0.2 mm) groups (overall p < 0.05; Fig. 6D). Pairwise comparisons showed smaller LVDs values in the PRP group compared with the MI and PBS groups (both p < 0.05), whereas no significant difference was found between the MI and PBS groups (p = 1.00). From day 1, this difference was consistently maintained throughout the observation period (p < 0.05; Fig. 6D), with the corresponding data provided in the Supplementary Data; Table 1.
Histological evaluation
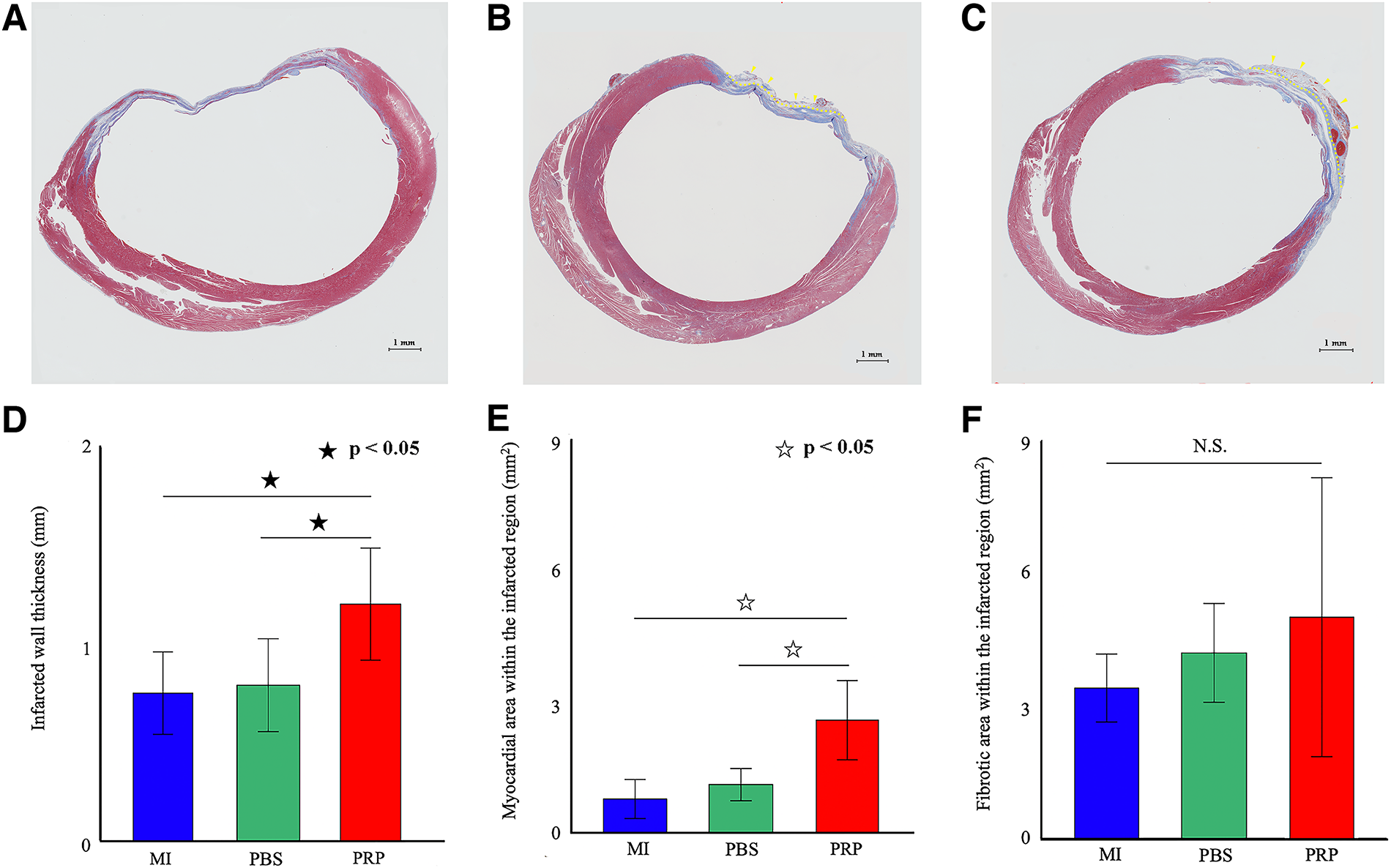
Masson’s trichrome staining of whole-heart specimens harvested on day 28 was used to evaluate cardiac tissue structure. Representative stained sections are shown in Figures 7A (MI), 7B (PBS), and 7C (PRP). The infarcted wall was significantly thicker in the PRP group (1.3 ± 0.3 mm) than in the MI (0.8 ± 0.2 mm) and PBS groups (0.8 ± 0.2 mm) (both p < 0.05 vs. the PRP group; Fig. 7D). The myocardial area within the infarcted region was also significantly greater in the PRP group (2.7 ± 0.9 mm2) compared with the MI (0.8 ± 0.5 mm2) and PBS (1.1 ± 0.4 mm2) groups (both p < 0.05 vs. the PRP group; Fig. 7E). In contrast, no significant differences were observed in the fibrotic area within the infarcted region, which measured 3.4 ± 0.8 mm2 in the MI group, 4.2 ± 1.1 mm2 in the PBS group, and 5.1 ± 3.2 mm2 in the PRP group (Fig. 7F). α-SMA staining of whole-heart specimens harvested on day 28 was performed to evaluate the vessel number in the infarcted region. Representative stained sections are shown in Figures 8A (MI), 8B (PBS), and 8C (PRP). The vessel number showed no significant difference among the three groups, which measured 87.4 ± 26.9 in the MI group, 70.8 ± 28.6 in the PBS group, and 74.8 ± 32.6 in the PRP group (Fig. 8D).
Quantitative histological analysis on postoperative day 28.
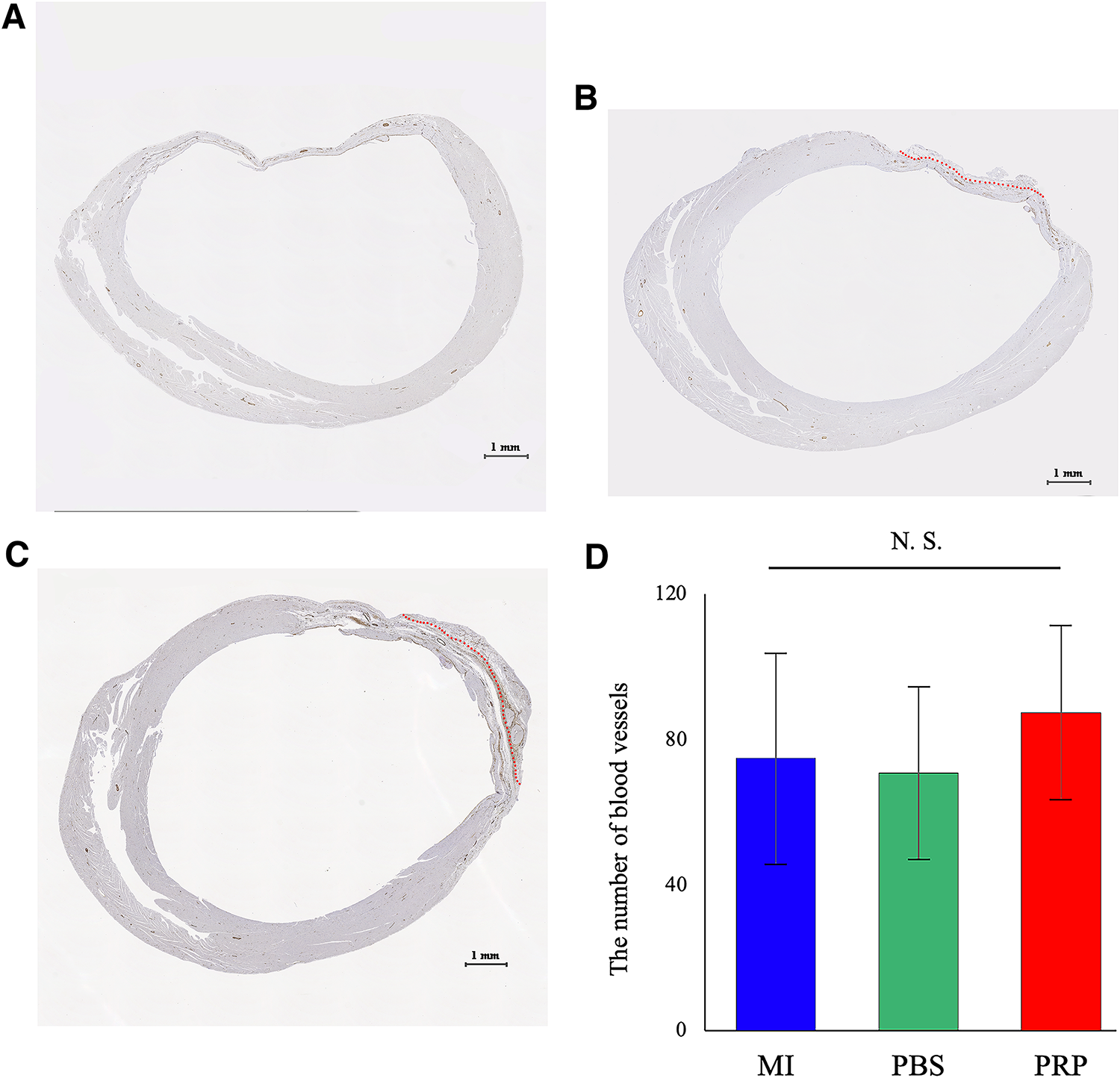
Quantitative histological analysis using α-SMA staining on postoperative day 28.
Discussion
This study focused on the cardiac function and histological findings after PRP epicardial hydrogel patch intervention. The biodegradable hydrogel patch was able to incorporate high-dose PRP and demonstrated controlled release of cytokines and growth factors in vitro. In vivo, this patch degraded on the epicardium until 3 weeks after implantation. In a rat MI model, echocardiographic analysis showed that the epicardial PRP hydrogel patch attenuated the decline in systolic function 1 day after MI induction. Until the chronic phase, systolic function was preserved, and the adverse remodeling was prevented in the PRP group. In our histological study, the PRP group had a significantly greater infarct wall thickness and a larger myocardial area within the infarcted lesion compared with the MI and PBS groups.
The epicardial controlled-release hydrogel patch fabricated in this study could provide some advantages for PRP delivery in an MI model. First, it could contain high-dose PRP (over 100 μL of PRP). Regarding the dose-dependent manner of PRP release, further study is needed to investigate the proper dose of PRP after MI. 17 Second, the epicardial patch demonstrated broad coverage of the infarcted area. Previous studies have reported that epicardial patch-based delivery systems enable effective drug delivery from the cardiac surface.7,8 This spatial advantage became possible through consistent PRP delivery from the epicardial hydrogel patch to the extensively injured myocardial tissue. Third, the gelatin-based hydrogel used in this study exhibited a controlled release profile—a fast burst followed by sustained cytokine delivery. Considering the pathological changes after MI, therapeutic interventions should start in the hyperacute phase to salvage the injured ischemic myocardium. 18 In addition, continuous therapy is required to prevent adverse cardiac remodeling. 19 The fast burst and controlled release of the hydrogel patch may provide PRP not only at the hyperacute phase but also for up to 2 weeks after implantation.
In this study, specific cytokines and growth factors (TGF-β1, PDGF-BB, and IGF-1) were observed after the controlled release of the PRP patch. It is believed that these factors modulate fibroblast activity, promote tissue repair, and exert anti-inflammatory effects. 3 These PRP-derived effects may contribute to the cardioprotective outcomes observed in injured cardiac tissue following MI. Previous studies have also demonstrated that PRP possesses intrinsic anti-inflammatory properties, 20 which may further contribute to its cardioprotective effects. 21 In this study, we observed a suppression in the decline of cardiac systolic function in the hyperacute phase and the prevention of cardiac remodeling in the chronic phase. These outcomes might be caused by the multiple cardioprotective effects of PRP.
Furthermore, this study demonstrated that the epicardial PRP application attenuated cardiac deterioration due to myocardial injury from the hyperacute phase, as early as day 1 after acute MI. To our knowledge, this is the first report of the effect of PRP onset in the hyperacute phase of MI. 3 The hyperacute period after MI is characterized by abrupt hemodynamic decline, severe myocardial ischemia, and activation of inflammatory signaling cascades. 18 Notably, serial echocardiographic evaluation showed that the preservation of cardiac pump function in the PRP group was achieved without the use of cardiotonic agents or cardiovascular agonists. The functional cardioprotective effects observed in this study can be interpreted through a mechanistic framework that links the biological properties of PRP, the temporal dynamics of epicardial drug delivery from a hydrogel, and the known pathophysiology of early myocardial injury. The LP-PRP used in this study suppressed the expression of proinflammatory cytokines and retained those of anabolic factors. 16 In the temporal release study, the PRP epicardial gelatin hydrogel released TGF-β1, PDGF-BB, and IGF-1 in a fast-burst manner corresponding to the hyperacute phase of MI, followed by a sustained controlled-release phase. This timing is critical because the hyperacute inflammatory wavefront determines the severity of downstream myocardial salvage and long-term cardiac remodeling. 18 The early epicardial delivery of anti-inflammatory and cytoprotective cytokines may contribute to the observed functional cardioprotective effect by reducing cardiomyocyte edema in the hyperacute phase after MI. 22 Nonetheless, further investigations are required to clarify the underlying mechanisms. Our findings may provide novel insight by directly demonstrating the efficacy of PRP therapy for myocardial ischemic injury.
Histological analysis in the chronic phase demonstrated that the hydrogel was no longer found in the PBS and PRP groups. These findings suggested that the epicardial hydrogel biodegraded completely at 4 weeks. Due to complete hydrogel degradation, all incorporated PRP was released on the epicardium. Regarding the fibrin–collagen sealant patch covering the hydrogel patch, some patches remained on the epicardial surface until 4 weeks after implantation. However, all residual fibrin–collagen sealant patches occupied a small area of the heart surface. Histological examination at 4 weeks consistently demonstrated that the residual sealant fragments were markedly smaller than the infarcted region in all specimens, as indicated by the arrows in Figure 6B, C. Nonetheless, the most important histological finding was that the left ventricular wall thickness was preserved in the PRP group. Moreover, the myocardial area in the PRP group was also significantly greater compared with the MI and PBS groups. Furthermore, both myocardial and fibrotic tissue were observed within the infarcted left ventricular wall in the PRP group.
Considering the mechanism underlying the structural cardioprotective effects of PRP from the epicardially controlled-release gelatin patch, early cytokine exposure may attenuate acute myocyte loss and stabilize the border zone, consistent with prior reports demonstrating the PRP-mediated suppression of oxidative stress, inflammatory signaling, and early cardiomyocyte apoptosis.23,24 TGF-β signaling is often associated with fibrosis; mild and localized fibrosis in the infarct border zone can provide structural cardioprotection and prevent excessive wall thinning and rupture.25,26 Additionally, VEGF was undetectable in our PRP preparation, and the vessel density did not differ among groups, suggesting that angiogenesis was not the primary driver of the functional or morphological benefits observed in this study. Further research is needed to determine the functional and structural cardioprotective effects of PRP. Collectively, our histological findings suggest that PRP treatment contributed to the structural preservation of the infarcted myocardium.
Study limitations
Several limitations should be acknowledged. Regarding the PRP profile, PRP contains a diverse mixture of cytokines, growth factors, and extracellular vesicles. In this study, only four major factors, such as TGF-β1, PDGF-BB, IGF-1, and VEGF, were quantified, leaving the roles (and levels) of other components unclear. Given the multifactorial nature of PRP, evaluating its overall biological activity may provide more meaningful insight than isolating its individual constituents. In addition, this study is limited by the mismatch between short in vitro cytokine release profiling and 28-day functional assessment. Although early cytokine exposure may initiate cardiac repair, longer release studies are needed to confirm this, and the discrepancy between kinetics and efficacy should be recognized.
Regarding the study protocol, this study did not include a cover-only control group. Because the PRP and PBS patches used the same gelatin hydrogel, material-related effects are likely negligible. Furthermore, adding another control group was not feasible due to limited animal availability, making additional comparisons impractical for both ethical and logistical reasons.
With regard to the animal model, this study was conducted exclusively in female rats, and sex-specific biological differences were not assessed. Therefore, the generalizability of these findings to male animals remains limited. Besides, species-specific differences in lifespan and remodeling rates may limit translation. Although rats show human-like acute responses, the 28-day period corresponds to several human years, potentially complicating the interpretation of long-term outcomes. 27
Conclusion
An epicardial controlled-release hydrogel with PRP demonstrated a cardioprotective effect from the hyperacute through the chronic phases in a rat MI model. Additionally, the PRP patch attenuated adverse ventricular remodeling after ischemic heart injury. Overall, our results suggest that the PRP epicardial delivery platform we generated may be a feasible alternative therapy for MI.
Authors’ Contributions
Study conception: T.M., Y.M., R.A., Y.T., Y.I.; Data curation: T.M., Y.M.; Formal analysis: T.M., Y.M., R.A., T.O., Y.M.; Investigation: T.M., Y.M., R.A.; Methodology: T.M., Y.M., R.A., Y.T., Y.I.; Project administration: T.M., Y.M.; Resources: T.M., Y.M., R.A., Y.T., Y.I.; Supervision: Y.M., T.O., Y.T., Y.I.; Validation: Y.M.; Visualization: T.M.; Writing—original draft: T.M.; Writing—review and editing: all authors; Final approval of the article: all authors; Accountability for all aspects of the work: all authors.
Footnotes
Acknowledgments
The authors used ChatGPT (OpenAI) to assist with English language refinement during the preparation of this article.
Funding Information
This work was supported by JSPS KAKENHI Grant Number JP22K08927.
Disclosure Statement
The authors declare no conflict of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.