
Abstract
Traditional approaches to tissue-engineered small intestine (TESI) require implanting a construct in the omentum of the abdominal cavity to allow for vascularization of the construct and tissue maturation. A second operation is then needed to implant the construct in continuity with the intestine. The timing of the second operation has historically been chosen based on predetermined biological endpoints. Currently, no well-validated method has been used to noninvasively monitor for vascular maturity which would better inform when the second operation should be performed. We hypothesized that photoacoustic imaging (PAI) could serve as a tool to noninvasively monitor regional and temporal changes in vascular maturity in scaffolds implanted in the omentum. For this pilot study, tubular scaffolds used for TESI were fabricated with electrospinning and implanted in the omentum of Sprague–Dawley rats for 1 and 2 months. Scaffolds were imaged with PAI and tissue oxygenation and hemoglobin concentration were quantified. PAI was then correlated with gross observations of vascularization at each time point. PAI was able to determine regional and temporal changes in tissue oxygenation and hemoglobin concentration. Specifically, the oxygenation and hemoglobin concentration of the top wall of the construct showed better vascular maturity compared with the bottom wall. In addition, vascular maturity seemed to improve in the top wall from 1 to 2 months. The bottom wall was not well covered by the omentum and thus did not vascularize as well as the top wall. The PAI findings were confirmed on gross examination of the scaffolds and upon quantification of the histological analysis of endothelial cell density. Thus, PAI may serve as a critical tool for monitoring vascular maturity in TE, specifically within the abdomen. This will be a critical tool in the preclinical development and clinical translation of TESI.
Impact Statement
Imaging methods to track functional changes in tissue-engineered constructs are need. These critical tools will be essential for tissue-engineered small intestine (TESI) development and clinical translation. In particular, understanding when a TESI construct has achieved vascular maturity is required prior to placing the TESI in connection with native intestine. In this proof-of-concept study, we have shown that photoacoustic imaging can be used to noninvasively track construct vascular maturity and that the imaging correlates with end-point histology. In addition to TESI, this tool is broadly applicable to all tissue-engineered constructs.
Introduction
Intestinal failure (IF) is the inability to absorb adequate nutrients or fluids to grow and sustain life.1,2 The prevalence of IF in the United States, including children and adults, is estimated to be 79 patients per million inhabitants. 3 IF is managed by intravenous calories given through a central venous catheter (parenteral nutrition [PN]), enteral feeds through feeding tubes, and multidisciplinary teams that can oversee the treatment of these complex patients with the hope of promoting intestinal adaptation such that the native intestine will eventually be able to absorb all nutrition through the gut (i.e., enteral autonomy).4–6 Treatment is expensive with costs in the United States in 2014 estimated to be $2.3 billion.4,7,8 More importantly, these therapies have numerous morbidities such as central venous catheter complications, sepsis, diarrhea, intestinal-failure-associated liver disease, and death.4,5,9,10 The all-cause mortality of IF ranges from 7% to 16% and is primarily driven by central venous access complications and liver failure from chronic PN.5,11–14 Tissue-engineered small intestine (TESI) has emerged as a potential treatment strategy for IF.
Previous efforts to create a TESI have focused on the epithelium and nutrient absorption with less attention on the critical requirement of peristalsis, which is vital for nutrient absorption.15–29 We have focused our initial work on the intestinal muscular layer and have successfully created a tubular scaffold with aligned fibers that induces human intestinal smooth muscle cell (hiSMC) alignment in vitro, which is a good candidate for developing a tubular tissue construct with organized muscle that may be capable of peristalsis once implanted in vivo. 2 In the rodent animal model to test TESI for tissue formation and function, the seeded construct is first implanted in the omentum to allow the muscle cells to form tissue and to obtain a blood supply. Four to six weeks after initial implantation, the constructs are placed in continuity with the intestine. This fixed interval time point is chosen based on convenience and general assumptions of the time course of inflammation without any direct knowledge of how each individual construct has matured prior to the second operation. The inability to functionally query the changes of an implanted construct over time thus represents a significant gap in the TESI field and is limiting to the advancement of tissue-engineering and regenerative medicine in general.
Novel noninvasive imaging modalities are required to enable in vivo assessment of implanted constructs, particularly to evaluate vascularity, a critical determinant of construct viability and success. Photoacoustic imaging (PAI) has emerged as a promising technique to address this need. PAI generates image contrast through the ultrasonic detection of optical absorption events. When combined with spectrally selective near-infrared imaging, PAI enables differential visualization and quantification of oxyhemoglobin and deoxyhemoglobin via computational spectral unmixing, permitting spatial assessment of tissue perfusion and oxygen saturation. Although PAI has been applied to the monitoring of scaffolds in tissue engineering, its utilization has remained limited.30–34 Moreover, to date, PAI has not been employed to evaluate vascular maturation of scaffolds within the abdominal cavity, a specific requirement for TESI. We hypothesized that PAI could be used to noninvasively quantify functional vascular maturation of TESI constructs in vivo over time, thereby informing the optimal timing for anastomosis with native intestine. In this pilot study, we demonstrate the feasibility of noninvasive functional vascular imaging using PAI to monitor temporal changes in tissue oxygenation and hemoglobin content as indicators of vascular maturation within TESI constructs (Fig. 1).
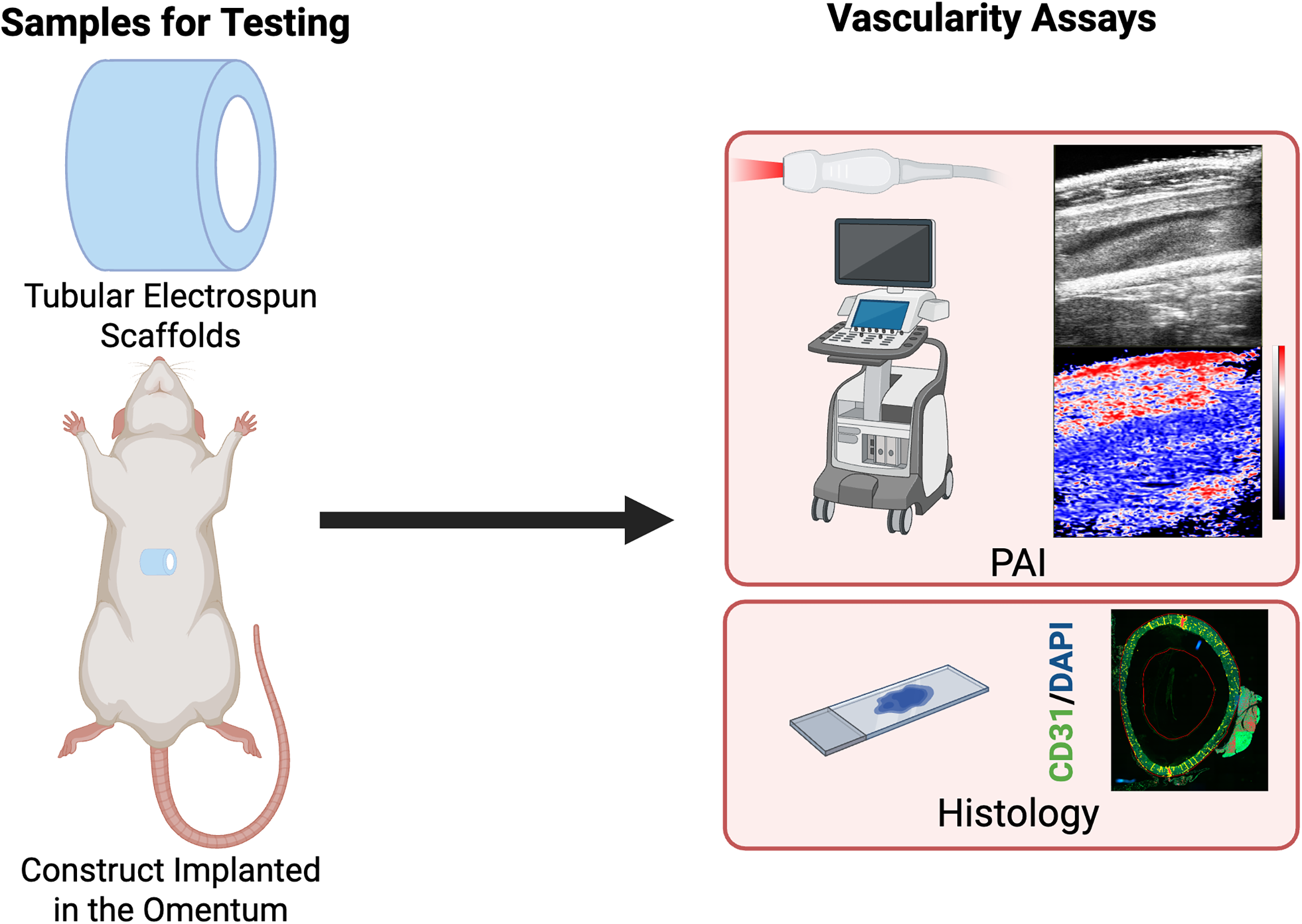
Study design and overview. Tubular scaffolds are fabricated with electrospinning using a combination of polycaprolactone and type I collagen. The constructs are then implanted into the omentum of Sprague–Dawley rats. At 1- and 2-month, the vascularity of the constructs is evaluated using photoacoustic imaging and correlated to end-point histological staining for CD31, a vascular endothelial marker. Created in BioRender. Ladd, M. (2025) https://BioRender.com/0t80o07.
Methods
Materials list
Pluronic F-127 (Sigma Aldrich, cat# P24434), Polycaprolactone (PCL, Evonik/Lactel absorbables, cat# B6003-2 and Sigma 24980-41-4, cat# 24980-41-4, inherent viscosity range 1.0–1.9 dL/g cat# 900820), calf skin type I collagen (Elastin Products Company, cat# c857), hexafluoroisopropanol (HFIP, Sigma Aldrich, cat# 105228), 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC, Thermofisher Scientific, cat# 22981), N-Hydroxysuccinimide (NHS, Sigma Aldrich, 130672).
Scaffold fabrication
Scaffolds were fabricated as previously described in Ladd et al. 2 In brief, tubular scaffolds consisting of a one-to-one blend of PCL and type I collagen (with inner diameter of 6 mm were fabricated using electrospinning. The polymer/collagen solution was 18% wt/vol and dissolved in HFIP. Prior to electrospinning the polymer solution, 3 mL of a 20% wt/vol Pluronic F-127 solution in deionized water was used to coat the mandrel so that the final scaffold would be easier to remove from the mandrel. Then, the PCL/collagen solution was spun at a flow rate of 10 mL/hr through a 16-gauge blunt tip needle, with a needle to mandrel distance of 15 cm and needle tip voltage of 20 kilovolts. The mandrel rotation speed was 11,000 RPMs to promote alignment of electrospun fibers in the circumferential direction. The scaffolds were allowed to dry and then crosslinked with EDC and NHS for 24 h. After crosslinking, the scaffolds were rinsed in deionized water, submerged in 100% ethanol to wet the Pluronic and remove the scaffold from the mandrel, frozen at −80ºC for 2 h, and then lyophilized. After lyophilization, scaffolds were stored at −80ºC until use. These scaffolds were previously characterized in Ladd et al. 2
Scaffold omental implantation
All animal surgeries and imaging studies were approved by the Institutional Animal Care and Use Committee (Protocol A24-063). Sprague-Dawley rats between the ages of 8 weeks and 6 days and 9 weeks and 1 day old at the time of scaffold implantation were used for all studies.
Prior to implantation, the scaffolds were cut to 4 cm in length. The day prior to surgery, the scaffolds were sterilized by placing them in 70% ethanol for 2 h followed by three 20-minute rinses in sterile PBS under a laminar flow hood. The constructs were then left under UV light for at least 2 h after which they were placed in the 37°C incubator overnight to acclimate to body temperature prior to implantation. After sterilization, animals were appropriately anesthetized after which a midline laparotomy was performed. The scaffold was then wrapped in the omentum and the omentum was secured in place on the right aspect of the construct using a simple 4-0 Vicryl suture. The abdomen was then closed in layers in the usual fashion. Animals were then survived until their time point at 1- or 2-months postsurgery. At each time point, the rats were anesthetized for PAI and then were euthanized. After euthanasia, gross images were taken of the constructs to compare with imaging and then the constructs were explanted for histological analysis.
Photoacoustic imaging
Prior to the animal study, we performed PAI on scaffolds embedded in psyllium husk agar phantoms to verify that the scaffold itself did not produce photoacoustic signal. High-frequency anatomical ultrasound (US) images were acquired with coregistered PAI images acquired at 750 nm and 850 nm spectral excitation wavelengths using a Vevo F2 LAZR-X (FUJIFILM VisualSonics, Inc., Toronto, ON, Canada). Specifically, Images were acquired using a UHF29x linear array ultrasound transducer with 15–29 MHz bandwidth and 20 MHz center frequency. Laser excitation was delivered via a Q-switched neodymium-doped yttrium aluminum garnet (Nd:YAG)-pumped Optical Parametric Oscillator (OPO) laser with 5 ns pulse width, 20 Hz repetition rate, 45 ± 5 mJ pulse energy using the medium (24 mm) Vevo Optical Fibers. These preliminary studies demonstrated that the scaffold did not have signal at 750 or 850 nm (Supplementary Fig. S1).
For the in vivo study, rats were anesthetized using isoflurane delivered in 100% oxygen (100% FiO2) and PAI was performed as described above. This enabled high-resolution measurements of oxyhemoglobin and deoxyhemoglobin concentration throughout the abdomen of the rats. 2D images were centered at the construct midplane with the construct oriented in the transverse direction. 3D images were acquired based on stacked 2D slices acquired at multiple locations perpendicular to the imaging plane over a range of 10.5 mm with image step size of 0.15 mm and used to build a 3D volume (23 mm by 24 mm by 10.5 mm) with US imaging transducer location controlled automatically via a motorized controller. Construct oxygenation was assessed based on the calculation of oxygen saturation using PAI measurements of oxyhemoglobin and deoxyhemoglobin concentrations. Oxygen saturation (sO2) was calculated as the ratio of oxyhemoglobin to total hemoglobin (HbT), performed using vendor-supplied analysis tools. Regions-of-interest (ROIs) were drawn to indicate both the top and bottom walls of the construct within the abdomen and used to measure average construct blood oxygen saturation and HbT in the top half of the scaffold compared to the bottom half for each rat. Mean sO2 and HbT measurements were recorded for ROIs drawn from the anatomical US images to designate the top and bottom walls of the construct in 2D analysis of the construct midplane. Following initial imaging assessment under 100% FiO2, a breathing gas challenge was used in which the carrier inhaled gas was changed to medical air (21% FiO2) and imaging measures were repeated.
Histological analysis
At the time of euthanasia, gross images were obtained, and the constructs were removed from the omentum. A center section of the construct was excised for histology and placed in 10% neutral-buffered formalin and fixed for 2–3 days. Then it was transferred to 70% ethanol until it was further processed and paraffin-embedded. The constructs were embedded to obtain both cross-sections. Sections were cut at 5 microns and then stained with hematoxylin and eosin (H&E). These slides were imaged on the E1000 Dx Digital Pathology Solution at 200X with the entire tissue sections being captured allowing for digital changes in magnification (Epredia).
Sections also underwent immunostaining to evaluate for vascular endothelial cells using an antibody for CD31 (rabbit anti-CD31 [EPR17259, Abcam, ab182981, 1:1000 dilution). The slides underwent antigen retrieval with EDTA at pH 9 prior to staining. The secondary antibody used was donkey anti-Rabbit IgG 488 (Biotium, 20015, 1:1000 dilution) and the slides were counterstained with DAPI. Afterwards, the slides were imaged on the Evident Slideview VS200 (Evident) at 200X. The entire tissue section was imaged at 200X, which then allowed for digital changes in magnification. The images were then analyzed using QuPath. 30 Specifically, the images were opened, and the tissue area was manually outlined to designate a region of interest. Positive fluorescent area was designated above a threshold of 2500 within the tissue region of interest. The threshold was chosen as the value at which QuPath was selecting the true positive staining. The percent positive area was then calculated as the positive threshold area divided by the total tissue area. This percentage was then taken as the approximate value of positive CD31 staining with a higher percent area positivity denoting higher microvascular density.
Statistical analysis
All data are shown as a mean with standard deviation. All data were analyzed with unpaired or paired two-tailed t-tests (as specified) or one-way ANOVA with post hoc Tukey’s test as appropriate with significance taken as a p value <0.05. Data were analyzed using GraphPad Prism software.
Results
Scaffold implantation
Surgeries for a total of 12 animals, 6 animals each in the 1-month and 2-month time points, were without issues. Three total animals had to be euthanized due to humane endpoints and at necropsy were found to have bowel obstructions where the bowel slipped into the lumen of the scaffold. This was thought to have occurred because of the 4 cm length of scaffold used and the relatively young (approximately 9-weeks old) age and low weight (approximately 250–300 g) of the rats used, with a less developed omentum that was not quite large enough to fully wrap the entire scaffold. Thus, there were 4 rats for the 1-month time point and 5 rats for the 2-month time point. All remaining rats survived until their planned time point.
Photoacoustic imaging
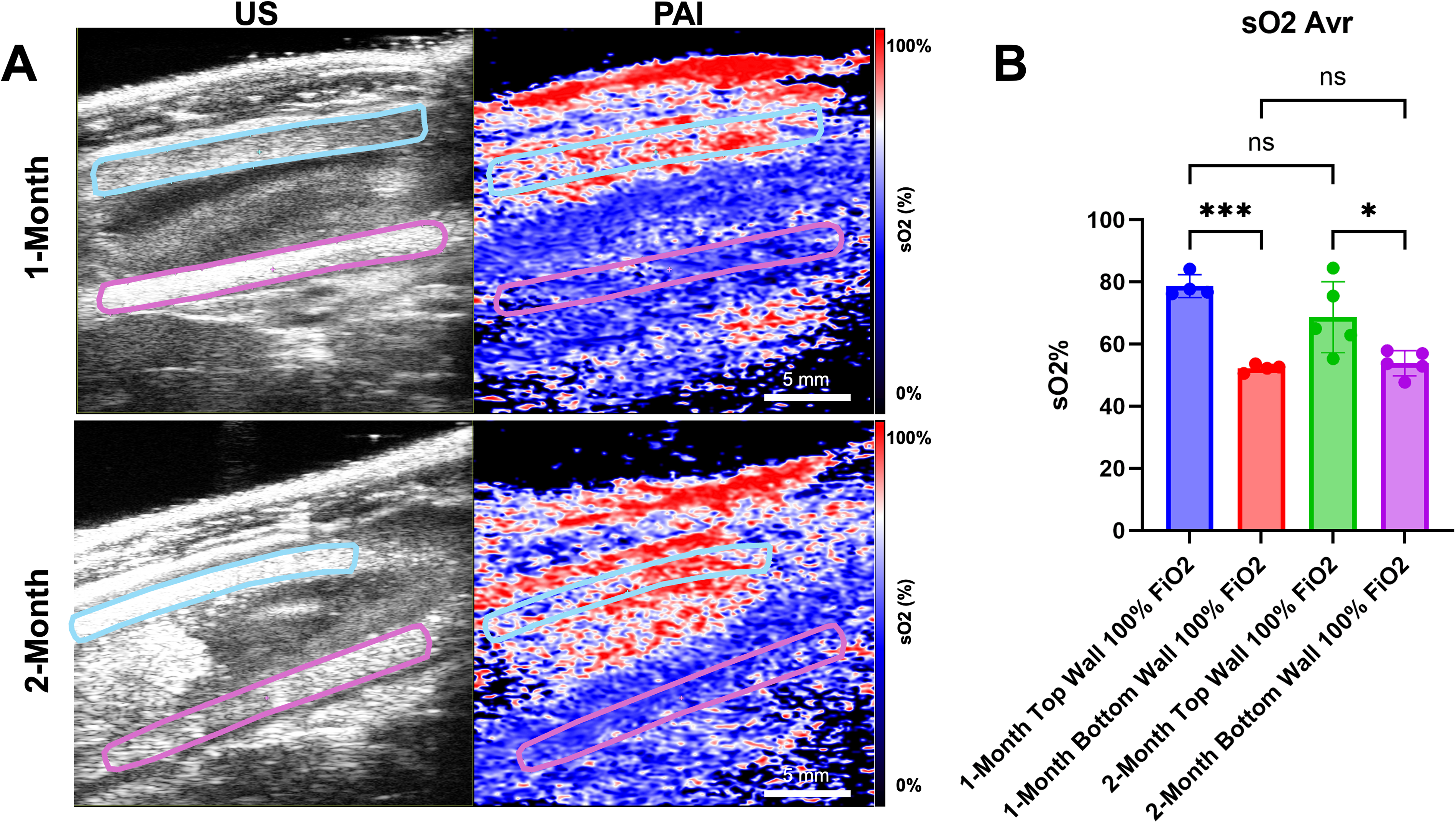
At the 1- and 2-month time points, PAI demonstrated that the regions of the implanted scaffold were well-oxygenated (Fig. 2). Of interest, the top wall of the implanted scaffolds at both 1- and 2-months were found to have more oxygen saturation compared with the bottom wall of the scaffold. When quantifying the oxygen saturation from PAI at 100% inhaled oxygen concentration between 1- and 2-months, there was a significantly higher oxygen concentration in the top wall at both time points compared to the bottom wall (Fig. 3). There was no increase in tissue oxygen saturation in the top wall of the scaffolds from 1- to 2-months. Similarly, there was no increase in tissue oxygen saturation in the bottom wall of the scaffolds from 1- to 2-months.
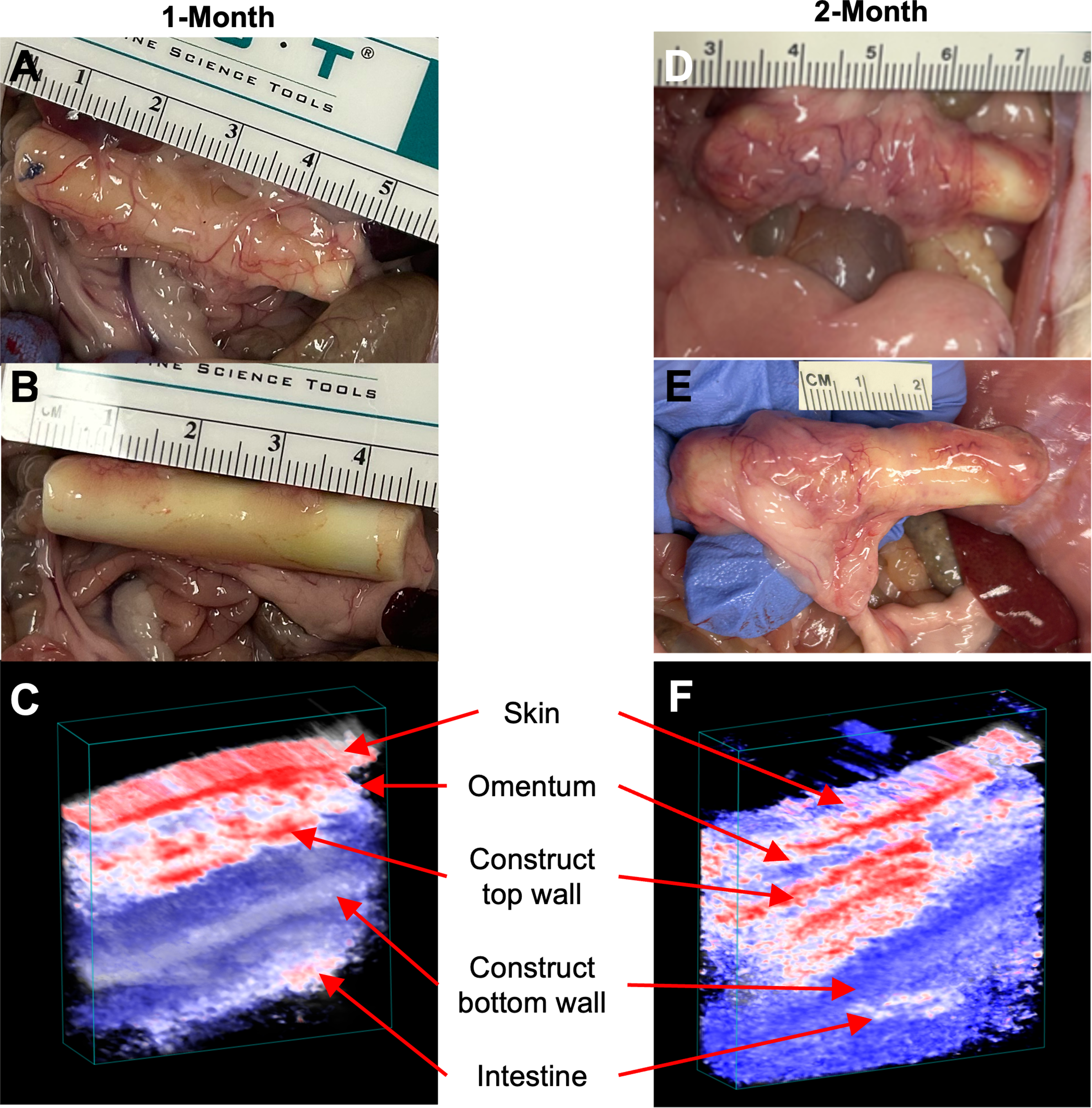
Gross evaluation of implanted scaffolds and correlation to photoacoustic imaging reconstructions at 1- and 2-month time points.
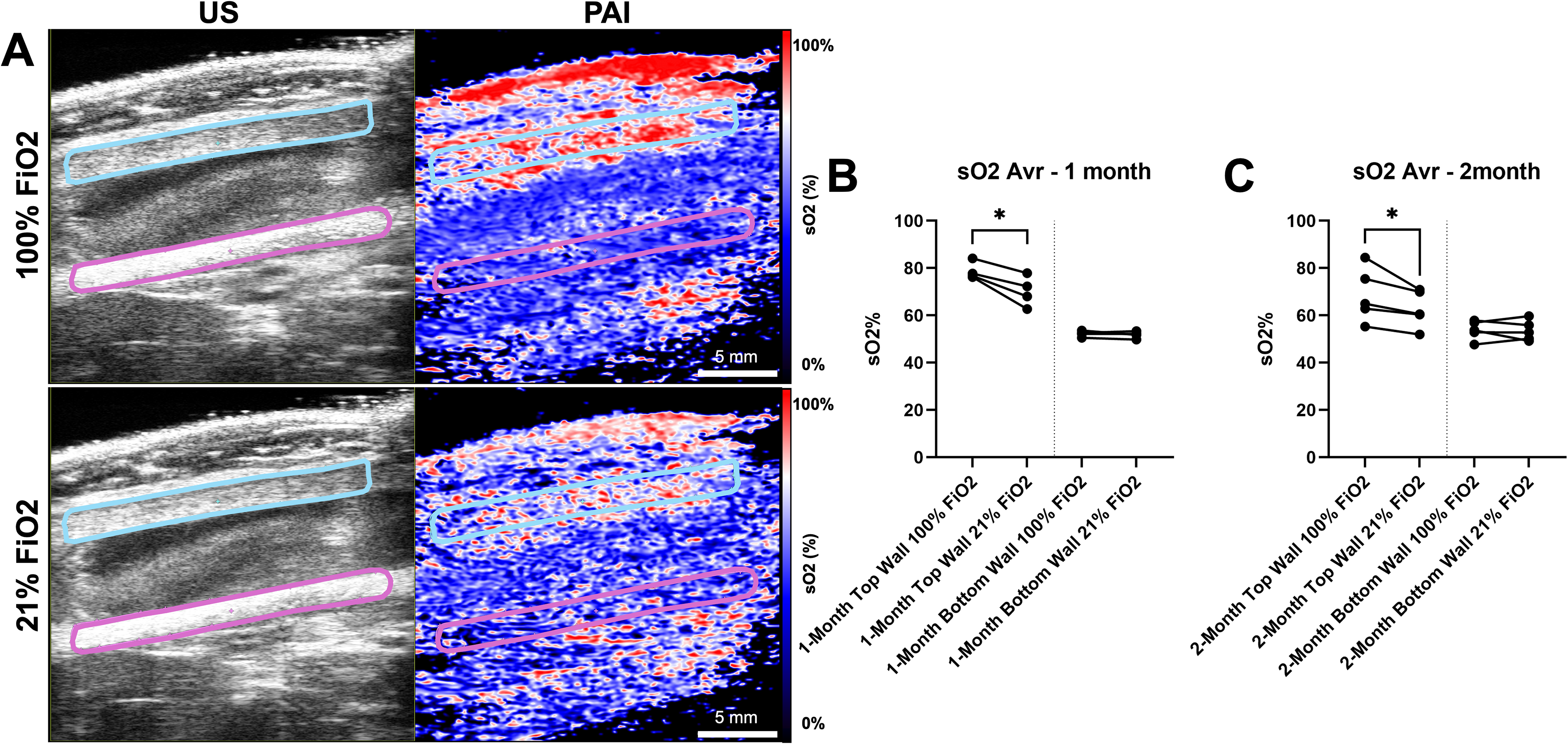
Next, the concentration of inhaled oxygen was changed from 21% FiO2 to 100% FiO2 in a breathing gas challenge to further validate PAI detection of oxygen saturation changes within the construct responsive to systemic oxygen saturation changes (Fig. 4). In doing this, there was a clear visual difference overall in the amount of oxygen saturation within the construct at 100% FiO2 as compared to 21% FiO2 (Fig. 4A). This was specifically apparent within the top wall at 1- and 2-months, which showed a statistically significant decrease in oxygen saturation in the top wall of the scaffold when decreasing in inhaled oxygen concentration from 100% to 21% (Fig. 4B and C). Because the bottom wall was less vascularized, a similar reduction in oxygen saturation was not seen in the bottom wall of the construct when decreasing from 100% to 21% oxygen. This confirmed the ability of PAI to detect functional vasculature within the scaffold when present, with changes in inhaled oxygen concentration leading to changes in the oxygen concentration in the scaffold on PAI.
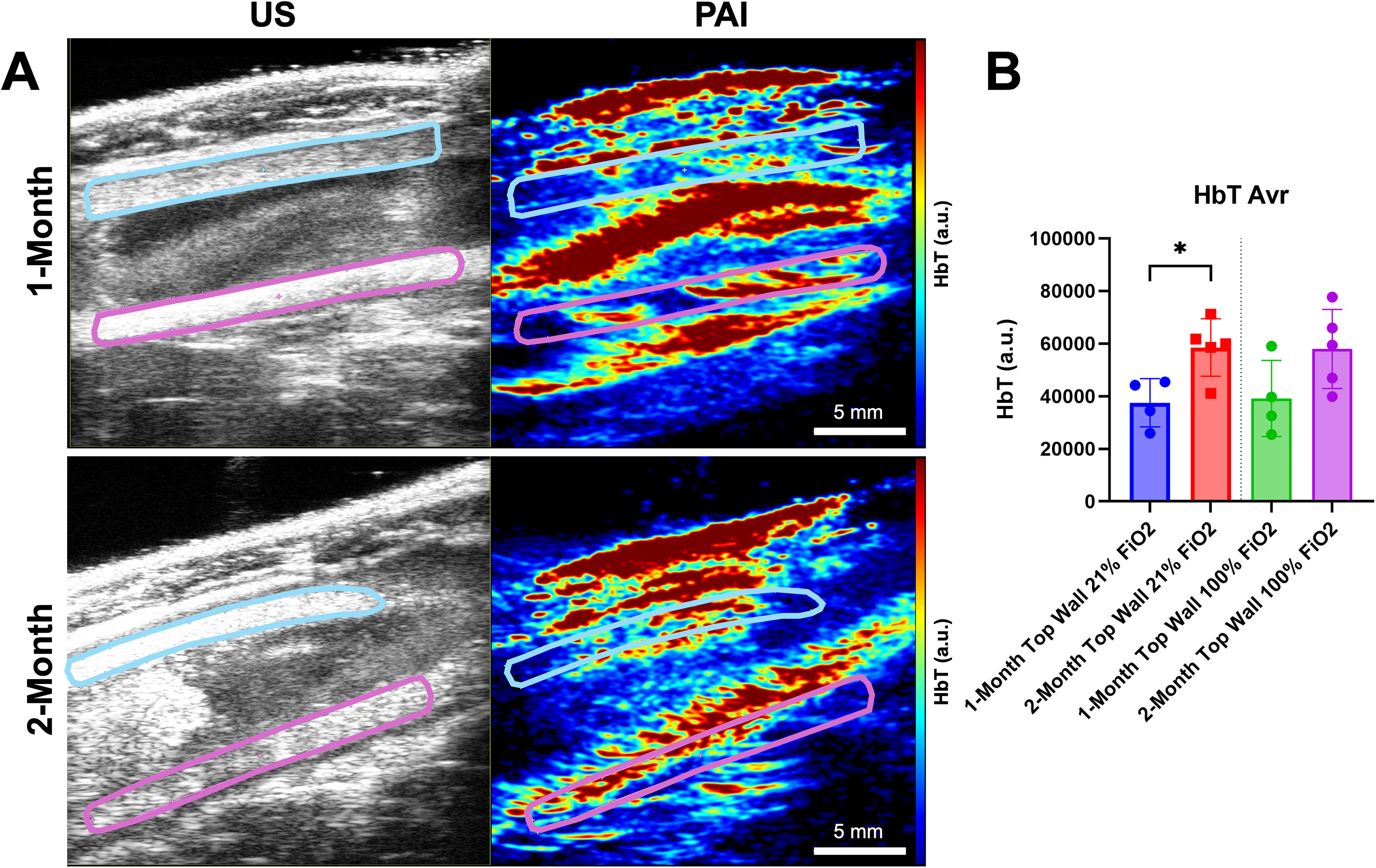
Finally, we examined HbT content in the implanted scaffolds at both 100% and 21% inhaled oxygen using PAI (Fig. 5). Given the relatively low amount of oxygen saturation and thus vasculature in the bottom wall of the scaffold, we evaluated only the top wall of the scaffold. There was an increasing trend in HbT content in the top wall from 1- to 2-months, both at 21% and 100% inhaled oxygen; however, only the increase at 21% FiO2 was statistically significant (Fig. 5B). This was consistent with our gross observations which revealed increased vascularization of the 2-month scaffolds in general compared to the 1-month scaffolds. Again, this demonstrated the ability of PAI to detect regional and temporal changes in not only tissue oxygen saturation, but also HbT content, which is a surrogate measure for vascularization.
Gross examination
Gross observations at necropsy revealed that the omentum was covering the top or anterior surface of the scaffolds better than the bottom or posterior side of the scaffold. This was consistent with the PAI findings. Because of this, each animal served as an internal control demonstrating that we could differentiate the vascularization seen on the top where it was better compared with the bottom. When carefully examining the gross surfaces, there seemed to be more vascular ingrowth and angiogenesis at 2 months compared with 1 month on average. In addition to the vascularization of the scaffold, we could easily identify the other layers of the abdomen including the skin and omentum, and the underlying intestines (Fig. 2).
Histology
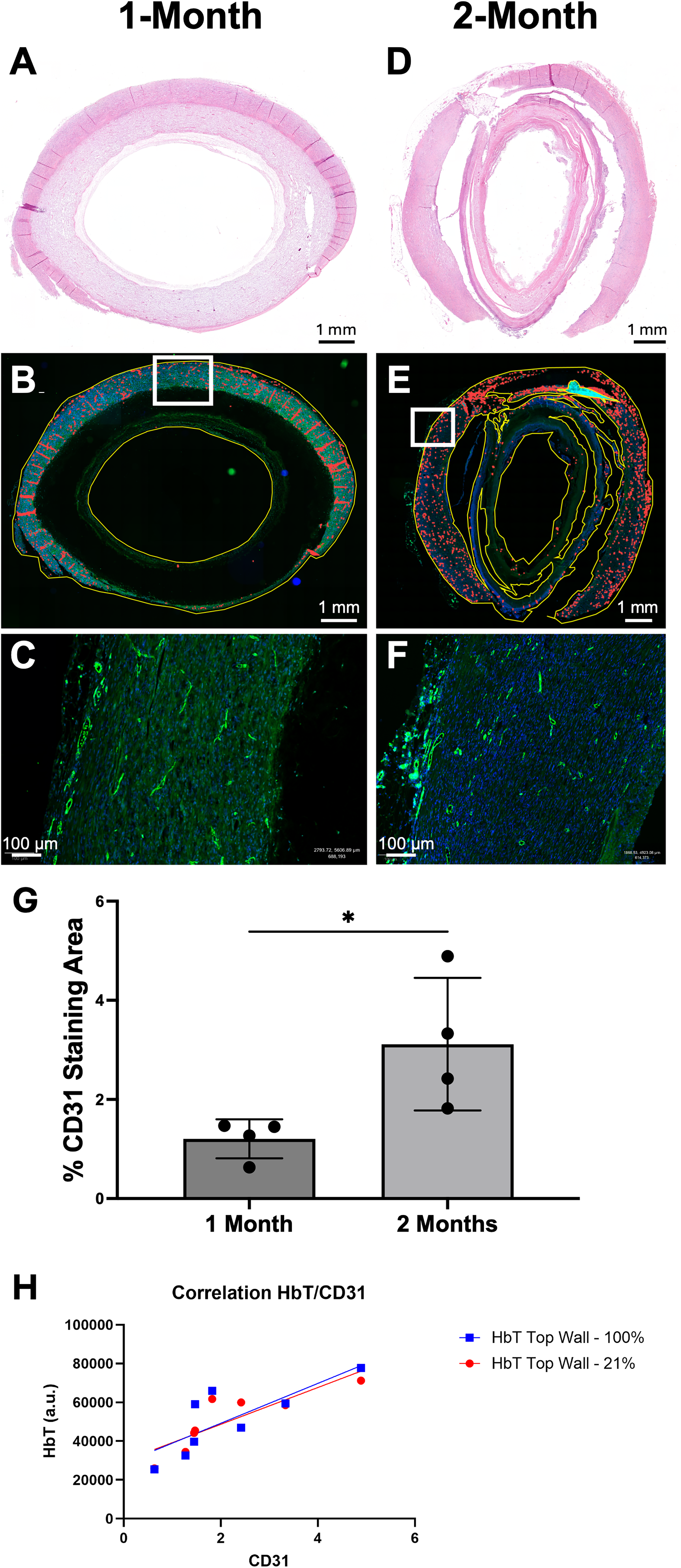
Staining and analysis of the scaffolds after explantation from the omentum demonstrated surrounding omental and inflammatory tissue. In addition, there were areas of vascular ingrowth noted on H&E (Fig. 6). The CD31 staining showed that endothelial cells were contained within the surrounding tissue as well as within the scaffold (Fig. 6B,C, E, and F). Of note, the amount of CD31 positive staining was found to be more prevalent and deeper into the scaffold in the 2-month samples as compared with the 1-month samples. When the samples were quantified, there was an increase in positive staining area of CD31 at 2-months compared with 1-month.
Discussion
This pilot study demonstrates the feasibility of PAI to monitor TE scaffold or construct vascular maturity over time. We show that PAI can detect changes in both tissue oxygenation and hemoglobin content. We internally validated our findings through the use of a breathing gas challenge wherein we changed the inhaled oxygen concentration from 100% to 21% and detected a clear decrease in tissue oxygenation, confirming that PAI detects functional vasculature within the wall of the scaffold. Moreover, the differences detected by PAI correlated well with our observations both grossly and histologically. The top wall of the implanted constructs was found to have more oxygenation and hemoglobin than the bottom wall on PAI and this difference in vascular ingrowth was evident on necropsy of the animals. In addition, PAI measured HbT concentration increased from 1-month to 2-months in the top wall of the scaffold suggesting an increase in vascularity. This was confirmed histologically with staining of vascular endothelial cells with CD31 and quantification of microvessel density. To our knowledge, this is the first report of using PAI to monitor changes in vascularization of TE scaffolds in the abdomen over time. PAI is feasible and reliable in detecting tissue oxygenation and hemoglobin content in implanted constructs within the abdomen and can distinguish the scaffold wall from surrounding tissues such as the omentum and intestine. Finally, histological quantification of microvessel density correlates well with PAI imaging, validating imaging findings.
While PAI was able to detect functional vasculature within the wall of the scaffold, the lack of increase in tissue oxygenation within the top wall from 1 to 2 months was initially surprising, as we observed on gross inspection that there appeared to be more vascular ingrowth at 2 months. For the bottom wall, the lack of increase in vascularity was consistent with our gross observations of the scaffolds at both time points. However, upon analysis of HbT, we deduced that vascularity was increasing and that tissue saturation was generally the same as saturation is not dependent on HbT but is the percent of oxygenated hemoglobin. Regardless, the results demonstrated that PAI can detect regional differences and changes in scaffold tissue oxygenation over time. The breathing gas challenge indicated that the scaffolds had developed blood flow, presumably through angiogenesis, and that these vessels were responsive to changes in inhaled oxygen concentration. Histological analysis confirmed that there was an increase in microvessel density from 1- to 2-month time points validating the PAI findings of HbT increase from 1 to 2 months.
Depth- and wavelength-dependent attenuation of optical fluence, known as spectral coloring, can bias estimates of sO2 and complicate comparisons of regions located at different depths. Therefore, direct quantitative comparisons between the top versus the bottom wall should be interpreted with caution. That said, the intention of this technique is to evaluate regions of the same depth over time. However, future studies incorporating fluence compensation methods will be needed to minimize these effects to enable more accurate regional comparisons when those comparisons are of interest.31–33
It is important to note that the bottom wall sO2 values were close to 50% and remained 50% during the breathing gas challenge. Thus, an alternative explanation for the observation within the bottom wall of the construct of reduced sO2 and lack of dynamic response to the breathing gas challenge is that the bottom wall experiences insufficient optical fluence due to depth-dependent attenuation and therefore produces minimal PA signal from hemoglobin. However, PAI data should be interpreted in combination with gross anatomical observations, shown in Figure 2 that validate minimal omental vascular integration. Moreover, we note that the bottom wall was at a depth of approximately 12.8 mm, which is within the commonly accepted penetration depth range for Vevo PA imaging within the literature, with commonly implemented depth ranges up to 15–20 mm (Supplementary Fig. S2). Combined, our data reflect that the likely explanation for the regional differences in the top wall and bottom wall are due to true differences in oxy- and deoxyhemoglobin.
While the development of PAI began in the 1960s, the modern use of PAI for in vivo imaging did not begin until the 1990s. 34 The first use of PAI in tissue engineering was reported in 2009 by Nam et al., who evaluated the vascularization of hydrogels that were implanted subcutaneously in rats. Prior to imaging, however, Nam et al. removed the constructs and performed PAI ex vivo. Since then, others have used PAI to evaluate implanted scaffolds or constructs, but these have been implanted subcutaneously or in the abdominal wall and not within the abdominal cavity.35–37 Despite this early work, the use of PAI has not accelerated in TE and seems underutilized.
The motivation to use PAI in TESI was born out of experience with the in vivo model. Specifically, TESI constructs are placed into the omentum to mature and develop a blood supply. Then, after a predetermined time point based on the known time course of inflammation and angiogenesis, the construct is then placed into continuity with the intestine during a second surgery using the omental flap as the blood supply for the construct. However, in our experience, there are times upon performing the second operation that the construct is not yet well-vascularized or is incompletely wrapped by the omentum. This problem spurred the motivation for this work. Non-invasive monitoring of the implanted constructs would allow us to monitor construct vascular maturity to avoid this situation. Alternatively, in the case of a construct in which the omentum had separated from the construct, combining the use of US and PAI would allow early identification of this problem and alert to the need to perform a reoperation to better wrap the omentum around the construct.
The study did have several limitations. First, the overall sample size was small as this was a proof-of-concept pilot study. Second, the sample size was further decreased due to early mortality in the animal model. As discussed, this mortality was likely due to the use of younger rats with less robust omentum in combination with scaffolds that were too long. In future work, we will use older rats with better-developed and larger omentum along with shorter length scaffolds for implantation. Third, we did not orient scaffolds with ink or other landmark fiducials when they were removed from the omentum. This limited direct histological correlation to imaging results as we are unable to conclusively comment on top versus bottom wall from a histology perspective. Fourth, we performed staining of single sections to perform histological validation assessment; however, this could be improved by performing serial sectioning with subsequent quantification. Lastly, we examined only two relatively short time points in this pilot study, but future work will examine more and longer construct maturation time points.
While this pilot study shows significant promise, we used a scaffold with a single material composition. Future work will investigate scaffolds composed of short- and long-term biodegrading materials to determine differences in vascularization between material types and further validate the imaging assessment method. In addition, as we progress in developing TESI, we will begin to include cell-seeded constructs and will monitor them for vascular maturity.
Conclusions
PAI represents a promising imaging modality for the noninvasive assessment of in vivo vascular maturation in tissue-engineered scaffolds and constructs. In this study, we demonstrated the feasibility of PAI to monitor both regional and temporal changes in vascular maturity of tubular scaffolds implanted within the omental region of the abdominal cavity. PAI findings were corroborated through gross examination and quantitative histological analysis of vascularization. Future investigations will build upon this pilot work by incorporating larger sample sizes, extended implantation durations, and diverse biodegradable scaffold materials with varying degradation profiles. Collectively, these findings highlight the potential of PAI as a valuable tool in preclinical tissue engineering research and in advancing the clinical translation of tissue-engineered technologies.
Authors’ Contributions
J.A.W.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, visualization, writing original draft, writing review and editing. M.R.K.: Data curation. N.C.D.: Data curation. M.Z.S.: Conceptualization, resources, writing review and editing. A.A.: Conceptualization, funding acquisition, writing review and editing. M.R.L.: Conceptualization, funding acquisition, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing original draft, writing review and editing.
Footnotes
Acknowledgments
The authors would like to thank the Wake Forest Institute for Regenerative Medicine for its ongoing support. The authors would like to acknowledge the Preclinical Ultrasound and Photoacoustic Imaging Core of Wake Forest School of Medicine supported in part by the Wake Forest Clinical and Translational Science Institute (NIH NCATS
Author Disclosure Statement
The authors report no conflicts of interest related to the work in the article.
Funding Information
Research reported in this publication was supported by a grant from the state of North Carolina and the
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.