
Abstract
The Coronavirus Disease of 2019 (COVID-19) pandemic caused by SARS-CoV-2 resulted in widespread mortality, economic strain, and healthcare system disruption, highlighting the need for effective strategies to address viral threats. Tissue engineering and biomaterials can contribute significantly in advancing our understanding and treatment of respiratory viral infections by developing physiologically relevant in vitro models, controlled and targeted drug delivery systems, and effective next-generation vaccine platforms. Over the last 5 years, tissue-engineered cell-based models, including organ-on-a-chip systems, have improved our understanding of viral entry, immune response, and therapeutic efficacy in pulmonary, cardiac, neurological, and vascular tissue. Biomaterial-based delivery systems have enhanced the targeting, bioavailability, and sustained delivery of therapeutics such as antivirals, monoclonal antibodies, nucleic-acid-based vaccines, and anti-inflammatory drugs, while also reducing or eliminating system toxicity and our reliance on intravenous administration. Advancements in vaccine platforms using lipid nanoparticles, protein scaffolds, and vesicular or cell-based platforms are in different phases of development to stimulate more robust responses against emerging SARS-CoV-2 variants. Collectively, these advancements highlight the influence of tissue engineering and biomaterials in SARS-CoV-2 research and treatment. This review provides an overview of recent developments in in vitro modeling, drug delivery systems, and vaccine platforms, highlighting their future role in improving clinical outcomes, managing variants, and preparing for potential future pandemics, including addressing challenges in infrastructure such as limited access to high-containment biosafety facilities used to study emerging infectious pathogens.
Impact Statement
During the COVID-19 pandemic, we introduced basic tenets of virology to a tissue engineering audience and proposed different areas in which the field could contribute to developing diagnostics and therapeutics for respiratory viral infections. In this 5-year update, we highlight how tissue engineers and biomaterial scientists contributed tools to dissect virus pathophysiology and deliver therapies such as mRNA vaccines to prevent mortality during the pandemic. With the emergence of new variants and the threat of new respiratory viral pandemics, tissue engineers can continue to play important roles in virology.
Introduction
The Coronavirus Disease of 2019 (COVID-19) pandemic caused by the virus SARS-CoV-2 resulted in an estimated 7.08 million deaths globally. 1 The pandemic also disrupted global supply chains, strained labor markets, and contributed to the global loss of 62 million jobs in 2020 with a 2.57% shrinkage in the global gross domestic product (GDP). 1 Healthcare systems experienced pressure at multiple levels. From September 2020 to February 2021, approximately 63% of U.S. hospitals reached their critical intensive care unit capacity for at least 2 weeks.2,3 Nursing homes were among the worst impacted, with more than 40% of total COVID-19-related deaths among residents or staff by August 2020. 3 Physicians were also impacted, with burnout rising from 45% to 60% and intent to leave rising from 30% to over 40% from 2019 to 2021. 4
Amid the pandemic in the late spring of 2020, we described the potential roles of tissue engineering and biomaterials in responding to viral pandemics. 5 This work summarized key aspects of virology for a tissue engineering audience and highlighted potential areas for bioengineering contributions. These included the design of in vitro cell/tissue assays for therapeutic screening, controlled drug delivery systems to decrease reliance on intravenous (IV) medications/need for hospitalization, and novel vaccine platforms. We noted in our prior review that “Work [was] already underway to develop vaccines effective against SARS-CoV-2…” Later that year, messenger ribonucleic acid (mRNA) vaccines delivered from lipid nanoparticles (LNPs) developed by biomaterials scientists were released to the public. Vaccination has since been estimated to have saved over 1.5 million lives, demonstrating the invaluable role of our field in response to pandemics.6,7
In this review, we will give an update on the landscape of COVID-19, including contributions from tissue engineering/biomaterial and new challenges pertinent to our field. We will discuss viral pathophysiology and current therapies, including the emergence of variants with new drug resistance. We will then examine work done by tissue engineers/biomaterials scientists in tissue models, controlled drug delivery, and novel vaccine platforms over the past 5 years (Fig. 1). This is not intended to be an all-inclusive review but rather a narrative review aimed at highlighting overall trends in the field. For context, a PubMed search using the terms “COVID” and “engineering” since 2020 yields over 32,000 results, 8 reflecting the scope of research literature. Papers were not systematically screened and selected.
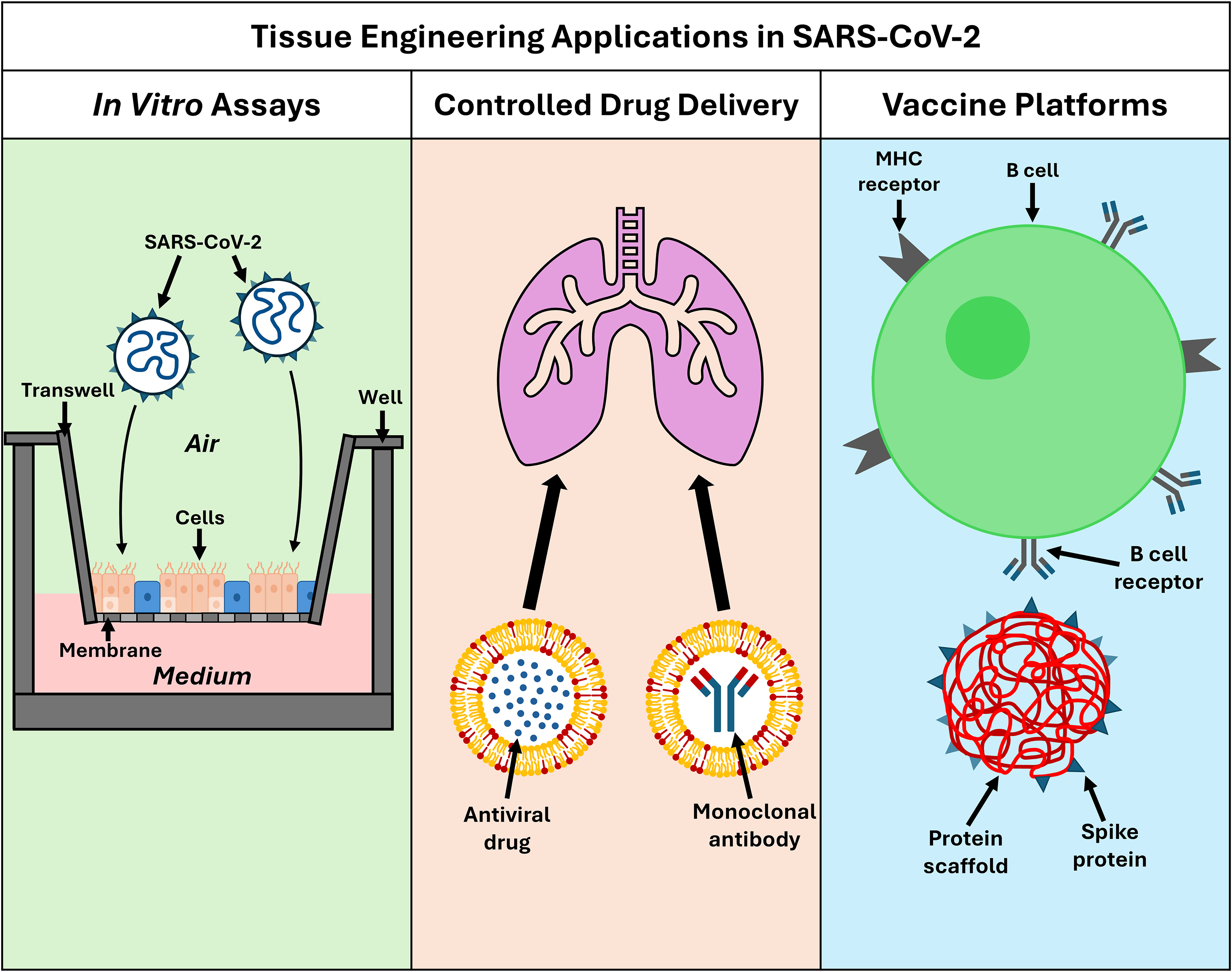
Overview of tissue engineering applications in studying and treating SARS-CoV-2, including in vitro assays, controlled drug delivery systems, and vaccine platforms.
SARS-CoV-2 pathophysiology
SARS-CoV-2 is composed of a positive-sense single-stranded RNA genome surrounded by a protein capsid. The complete virion consists of four structural proteins: spike, envelope, membrane, and nucleocapsid. Viral entry into a host cell is mediated by the spike protein. Specifically, the spike protein receptor binding domain (RBD) interacts with angiotensin-converting enzyme 2 (ACE2) on a host cell surface to induce entry. This initiates membrane fusion, requiring cleavage of the spike protein by furin.9,10 Conformational changes in the spike protein further expose the RBD, which enhances its accessibility to ACE2. Like the hemagglutinin protein used as an antigen in influenza A vaccines, SARS-CoV-2 spike protein is the most common vaccine target due to its importance in viral entry. 5 The spike protein and its RBD are critical in the ability of a virus to transmit, with many variants accumulating mutations in these regions that increase ACE2 binding affinity and ability to adapt to treatment. The Omicron variant has emerged as the most genetically diverse of all strains, with more than 50 mutations dispersed among its genome.11,12 Researchers studying SARS-CoV-2 have used spike protein alone, pseudovirus (constructs containing certain components of SARS-CoV-2 but unable to replicate), or actual authentic SARS-CoV-2 to better understand host/viral interactions. While studying intact SARS-CoV-2 allows for the most complete understanding of its behavior, the culture of SARS-CoV-2 requires Biosafety Level 3 containment facilities which adds expense, limits bandwidth, and may not be accessible to all tissue engineering groups.
SARS-CoV-2 primarily spreads through mucociliary droplets released during coughing, sneezing, talking, or breathing. The respiratory tract is the most dominant route of transmission.13,14 Disease presentation ranges from mild symptoms such as fever, cough, and shortness of breath to more severe including pneumonia, acute respiratory distress syndrome (ARDS), respiratory failure, sepsis, multiple organ failure, and death. 15 Beyond the respiratory system, SARS-CoV-2 has been detected in lymphocytes, intestinal mucosa, renal epithelial cells, and neurons. 16 The adaptable nature of the virus and its ability to infect multiple tissue types highlight the need for utilizing tissue engineering to develop more relevant in vitro models, drug delivery systems, and vaccine platforms to improve diagnostics and therapeutics.
Therapeutics update
In the past 5 years, vaccines have played a central role in reducing COVID-19 severity and mortality. There are four World Health Organization–approved vaccine platforms: mRNA, DNA-based viral vector, inactivated whole pathogen, and protein subunit. 9 The most widely used mRNA vaccines, Pfizer-BioNTech (Comirnaty) and Moderna (Spikevax), use nucleoside-modified mRNA encoding full-length spike protein in LNPs for improved delivery and stability. DNA-based viral vector vaccines use recombinant, nonreplicating adenoviruses that encode a stabilized spike protein. Inactivated whole pathogen vaccines use chemically inactivated SARS-CoV-2. Protein subunit vaccines present recombinant or purified antigens to the immune system. 9 Across the successive waves of emerging variants, increased vaccination rates and coverage in combination with immunity acquired through natural infection have been associated with fewer deaths, resulting in the significant decline in COVID-19-related mortality since its peak in 2021.2,17
In addition to vaccine technologies, therapeutics such as small-molecule antivirals and monoclonal antibodies (mAbs) have also emerged. Small-molecule antivirals, including remdesivir and molnupiravir, are inhibitors of the RNA-dependent RNA polymerase of SARS-CoV-2, while nirmatrelvir/ritonavir inhibits the main protease of SARS-CoV-2 and limits viral replication.18,19 These antivirals have resulted in reduced mortality and decreased hospitalization rates, though benefits may vary with antiviral and patient population.18,19 Monoclonal antibodies neutralize the virus by binding the spike protein and promoting antibody-dependent phagocytosis, cell-mediated cytotoxicity, and complement activation. However, the rapid emergence of new variants with spike protein mutations has reduced the efficacy of mAbs, raising concerns about treatment effectiveness. 20
Following the initial pandemic, several SARS-CoV-2 variants emerged between 2020 and 2023, including Alpha, Beta, Gamma, Delta, and Omicron. Each variant has different mutations of the spike protein or other regions that affect virulence, transmissibility, and/or effectiveness of public health measures.9,11 The rise of the Omicron strain and its lineages continues to pose challenges to economic recovery and established public health strategies. 11 Tissue engineering and biomaterial approaches allow for the creation of next-generation models and platforms capable of studying variants and their changes that allow for immune evasion.
Cell/Tissue Models
Following the outbreak of SARS-CoV-2, tissue engineers and virologists developed new in vitro models that have furthered our understanding of viral infection, replication, and biomarker production. Earlier studies relied heavily on two-dimensional (2D) Vero cell monolayers, which lack key human entry pathways and are derived from nonhuman cells. Since the start of the pandemic, engineers have created more advanced 2D models using immortalized human cell lines that better replicate viral entry and proliferation. These 2D models do not capture tissue structure. The next evolutions were simple three-dimensional (3D) culture systems, such as transwell air–liquid interface (ALI) cultures and more complex microphysiological and organ-on-a-chip models that better mimic human infection and native tissue architecture. 21
2D immortalized cell lines
Previously, the gold standard for coronavirus infection modeling had been 2D monolayer growth of Vero cells, a line of kidney epithelial cells isolated from the African green monkey. 22 While these models are still widely used, they have proved limited in modeling severe disease and drug effects.22–24 Newer models utilizing human-cell-based platforms retain key proteins required for viral entry, better representing infection. One example is the use of Calu-3 lung epithelial cells derived from human pulmonary adenocarcinoma, which have gained popularity for their ability to recapitulate infection and preserve genomic accuracy. 25 Their ability to express a serine protease-mediated entry pathway (TMPRSS2) used by the spike protein to enter human cells more accurately models cell entry.26–28 From these advancements, engineers leveraged immortalized 2D models to study viral entry and test therapeutics like an ACE2-mimetic peptide that reduced SARS-CoV-2 infection.29,30 These models have been used to evaluate antiviral agents such as main protease (Mpro) inhibitors across multiple cell-based assays with maintained activity against variants. 31 Separately, alveolar carcinoma cell lines like A549 cells have been engineered to express ACE2 to further study viral entry and replication in the pulmonary system. 32 Additionally, these models have been used to study entry pathways independent of TMPRSS2 that use metalloproteases ADAM 17 and ADAM 10, as well as the use of therapeutics such as rimantadine, amantadine, and tromantadine to show inhibition in the growth of SARS-CoV-2.32,33 The use of cell lines derived from other human organ systems, such as ACE2-expressing HEK-293T, Huh7, MCF7, and Caco-2 cells (derived from kidney, liver, breast, and intestinal cells, respectively), has all shown to be promising models due to their high levels of TMPRSS2 mRNA and SARS-CoV-2 replication capacity.34,35 Ultimately, randomized controlled trials in patients revealed that ACE2 inhibitors and amantadine were not found to prevent mortality in COVID-19—this may speak to the limitations of 2D culture in capturing the complexity of human disease.36,37
Simple 3D culture systems
3D models offer several advantages over 2D models in recapitulating physiology relevant to viral infection, including differences in proliferation rates, cell morphology, gene expression, and drug responsiveness. 38 Among cell-based infection models, pulmonary tissues are important due to the prevalence of COVID-19 pneumonia and the susceptibility of respiratory tissues to infection and injury. 23 Bronchial, nasal, and airway epithelial cells have been seeded onto transwells to create ALI culture models that expose the apical and basal sides of a cell layer to an air-rich and nutrient-rich medium, respectively, to better represent the human respiratory tract as depicted in the leftmost schematic in Figure 1.29,39–41 These ALI models differentiate into relevant cells such as ciliated cells, goblet cells, and basal cells and have been successful at recapitulating key events during infection such as the early targeting of ciliated cells, extensive viral shedding, the activation of the Hippo signaling pathway, and the rapid spread of newer variants like Omicron.29,39,42,43 More advanced ALI models incorporating immune components like neutrophils cocultured with airway epithelial cells allow the study of inflammation in the airway during infection. 44 Through these models, it was discovered that SARS-CoV-2 can generate relatively weak airway interferon responses despite the activation of pathways such as PKR and RNase L. 45 These models have also enabled the study of cellular responses at a mechanical level, including changes in cytoskeletal organization, mitochondrial dysfunction, and actin remodeling as a result of infection in epithelial cells. 46 More complex transwells have been created using multiple cell types such as tracheobronchial tissue and bronchial epithelial tissue, which differentiate into a variety of relevant cells such as ciliated cells, goblet cells, and alveolar type I- (AT1) and type II-like cells (AT2) capable of recreating key upper airway features such as mucus production and cilia movement.24,40 Infection was established with both SARS-CoV-2 and Influenza A, and treatment was successful using drugs, such as remdesivir and IFN-beta–remdesivir has been validated to improve outcomes in clinical trials.24,47 Other human lung organoid-derived ALI systems have been responsive to interferon treatment, making them potential models for drug screening. 48 Finally, models other than ALI have been used, such as alveospheres (3D spherical structures that mimic the alveoli) created from autopsied lung tissue from patients with severe COVID-19 made of primary human AT2 cells capable of abnormal host responses such as cellular senescence and weak interferon-I and -III signaling. 49
3D microphysiological systems/organs-on-chips
For COVID-19, organ-on-a-chip models are among the most widely used 3D models and involve culturing cells in channels that can provide nutrients, oxygen, and drugs at controlled gradients to better mimic a human tissue environment. These systems can recapitulate key physiological features inside microfluidic devices, such as the tissue–tissue interfaces, fluid shear stress, and concentration gradients to create environments that are not possible with conventional 2D models or simpler 3D models. 50 Bronchial-airway and alveolar chips derived from human epithelial basal and pulmonary endothelial cells or human-induced pluripotent stem cell (hiPSC)-derived lung progenitors can be engineered to recreate mucociliated airway structures for the study of SARS-CoV-2 pseudovirus infection and drug efficacy.51,52 These models demonstrated that amodiaquine, toremifene, and clomiphene block viral entry in 3D chips at lower drug concentrations compared with 2D culture. Investigators have additionally been able to observe immune responses such as cytokine secretion, neutrophil recruitment, interferon production, and endothelial activation, with more advanced high-throughput microfluidic platforms like the Draper PREDICT96-ALI with real-time output of infectious and antiviral responses.51–54 Alternative 3D models use whole tissue obtained from surgical resections that maintain tissue architecture and cellular heterogeneity by embedding the tissue in a collagen and Matrigel extracellular matrix perfused with media. This facilitates the modeling of T and B cell dynamics, including immunoglobulin A plasma cells and effector memory cells, if lymphoid tissues are captured during surgical resection. 21 In this example, infection was modeled using SARS-CoV-2 antigens (M, N, and S proteins) rather than authentic virus.
While SARS-CoV-2 first infects the respiratory system, damage to other organs such as the heart and brain can also occur. 55 Cardiomyocytes are important targets because of complications such as heart failure and myocarditis. hiPSC-derived models have been engineered to produce cardiomyocytes for infection models that enable time-series analysis over the course of infection, revealing different patterns of gene upregulation and downregulation. 22 These studies used authentic replicating SARS-CoV-2 to establish infection. Heart-on-a-chip models using hiPSC-derived cardiomyocytes and fibroblasts in collagen-based hydrogels also recapitulate phenotypes seen in COVID-19, including impaired contractile functioning, apoptosis, and sarcomere disarray when exposed to authentic virus. 56 Other engineered heart tissue models derived from hiPSC cardiomyocytes using collagen/Matrigel as extracellular matrix can also support viral replication and recreate key features seen in infected myocardial tissue, including reduced contractility and cell death. 57 Similarly, human microvascular endothelial cells cultured into 3D pulmonary microvessels show immunoglobulin M-mediated effects after exposure to SARS-CoV-2 spike protein, while hiPSC-derived endothelial progenitors embedded in 3D hydrogels create capillary-like networks suitable for studying vascular dysfunction in response to SARS-CoV-2-associated factors like autoantibodies, though these models lack immune cells.38,58
Brain and CNS models are also important, as roughly 30% of hospitalized patients develop neurological symptoms that may persist, including dizziness, headaches, and even chemosensory abnormalities in smell and taste.55,59,60 Models derived from hiPSC-brain capillary endothelial-like cells and neutral stem cell-derived astrocytes mimic brain vasculature and astrocyte metabolism. These models suggest that proteins like NRP1 may have a higher contribution to viral cell entry than ACE2 in neurological tissues; using authentic virus discoveries such as these from tissue-engineered models may lead to new therapeutic targets.55,59 Human embryonic stem cell-derived peripheral neuron models have identified olfactory neurons as direct infection targets, though it should be noted that models using single populations are limited by their lack of innervation recipients such as epithelial and immune cells. 60 Multiorgan engineered models have also been developed, such as a lung alveolus chip and a blood–brain barrier chip, to better understand the link between lung and brain infection. 61
In summary, in vitro models of SARS-CoV-2 infection have progressed from using Vero cells to human 2D immortalized cell lines, simple 3D systems, and more complex 3D microphysiological platforms. Each model has new advantages in providing more relevant platforms to study infection dynamics, tissue damage, and therapeutics across multiple organ systems although adds complexity in methodology. Additional advancements include in vitro modeling of adipose tissue, gastrointestinal organs, blood, and musculoskeletal cells that utilize human adipocytes, erythroid precursor cells, and myogenic cells, respectively.60,62–65 Important limitations remain, specifically capturing the full complexity of the immune system and its systemic interactions. Future developments in in vitro models should focus on integrating more immune components and creating more multiorgan systems to better recapitulate the body’s larger response to SARS-CoV-2 infection.
Drug Delivery Systems
Biomaterial-based nanocarriers and other drug delivery systems for COVID-19 therapeutics may improve outcomes for patients by enhancing tissue-specific targeting, bioavailability, and sustained therapeutic exposure while reducing off-target effects. The following preclinical studies exploring these systems show promise for future clinical applications.
Controlled delivery of antivirals
Antivirals are an important group of therapeutics used to treat COVID-19. The most successful clinically approved antiviral during the pandemic was remdesivir, an adenosine nucleotide analog that inhibits viral RNA synthesis, approved after our prior publication. 5 Remdesivir is effective in treating both hospitalized and nonhospitalized patients. 66 However, the drug is limited by poor aqueous solubility and inadequate oral bioavailability, requiring IV administration. Direct pulmonary delivery via inhaled formulations could increase potency, targeted delivery, and ease of use without the need for IV access. Organic polymer nanoparticles such as 2,2-bis(hydroxymethyl)propionic acid (bis-MPA) hyperbranched dendritic nano-scaffolds have been studied in vitro as carriers of remdesivir for inhaled delivery. These loaded nanoparticles showed similar antiviral potency to free drug and improved aqueous solubility, thereby increasing bioavailability and enabling more effective pulmonary delivery. 67 Similarly, poly (lactic-co-glycolic acid) nanoparticles loaded with remdesivir showed enhanced cellular uptake and sustained remdesivir release under physiological conditions in SARS-CoV-2-infected Vero cells. 68 Furthermore, intranasal phospholipid–cholesterol liposomal nanocarriers for remdesivir have also shown increased survival, decreased viral load, and decreased pulmonary inflammatory response in authentic SARS-CoV-2-infected K18-hACE2 mice compared with IV administration of the standard pharmaceutical formulation of remdesivir. 69 In addition to improving efficacy and offering new routes of administration for remdesivir, there has also been work in improving the efficacy of other antivirals against SARS-CoV-2. For example, molnupiravir is an oral ribonucleoside analog antiviral that induces lethal mutagenesis by causing error accumulation in viral RNA during replication. 70 Delivery with novel systems, such as a copper–cobalt ferrite nanoparticles and self-assembled cellulose and pycnogenol nanoparticles, enhanced molnupiravir delivery by improving drug stability and bioavailability via controlled pH-responsive release and reduced systemic toxicity.71,72 However, in vivo validation of molnupiravir delivery systems remains limited in the current literature and is necessary to assess their clinical applicability.
Controlled delivery of mAbs
Especially in immunocompromised or unvaccinated patients, passive immunity via mAbs is a promising treatment option for COVID-19. Monoclonal antibodies induce their effects by binding to the SARS-CoV-2 spike protein to block viral entry into host cells, providing immediate passive immunity when given early in infection. 73 Traditionally, mAbs are delivered via IV or intramuscular injection. 74 Biomaterial-based controlled delivery may increase both accessibility and efficacy of treatment with mAbs. Lung-selective LNPs have been developed to explore this possibility. The incorporation of permanently cationic lipids into LNPs resulted in lung accumulation due to strong electrostatic interactions with the pulmonary endothelium and capillary entrapment, thereby allowing targeted delivery to the site of infection. This contrasts with mRNA vaccine LNPs, which remain neutral in circulation, enabling prolonged blood residence and hepatic uptake. Lung-selective LNPs delivered mRNA encoding mAbs that showed strong neutralizing activity against most SARS-CoV-2 variants. 75 This form of delivery offers multiple options for administration routes, including aerosol inhalation and intranasal inoculation. Additionally, this system showed efficacy in mouse model studies, generating significantly higher antibody levels in the lungs and bronchoalveolar lavage fluid compared with liver-targeted LNPs. When K18-hACE2 transgenic mice were prophylactically treated with the lung-selective LNPs loaded with mRNA encoding for mAbs and then challenged with SARS-CoV-2 Beta or Omicron BA.2 variants, the treated animals showed a reduction in viral load with preserved lung histology. 75 This strategy also provided protection when applied after infection.
Despite their potential, mAbs have been limited by the rapid evolution of SARS-CoV-2 binding targets, especially spike protein. Newly emerging Omicron variants such as LF.7.2.1, JN.1, and KP.2 have developed mutations of the spike protein, allowing them to decrease the neutralization capacity of mAbs via reduced binding affinity.76,77 Ongoing viral evolution highlights the need for mAbs with broader activity or adaptable strategies to maintain the clinical efficacy of this treatment strategy.
Controlled delivery of other therapeutics
The ability to treat ARDS and other advanced forms of disease is an important challenge in preventing COVID-19-related mortality. In severe disease, the use of anti-inflammatory drugs such as corticosteroids has been shown to reduce mortality by decreasing lung inflammation and improving oxygenation. 78 However, corticosteroid use can be limited by harmful side effects due to nonspecific activity, and targeted delivery systems can be used to improve specificity. To overcome these obstacles, several in vivo studies have explored targeted delivery of corticosteroids via biomaterial-based nanocarriers. In murine models, dexamethasone encapsulated in amphiphilic hyaluronic acid derivatives had superior specificity for lung tissue and anti-inflammatory effects compared with free dexamethasone during acute lung injury. 79 Another method of delivering dexamethasone is the use of cell-derived nanovesicles. In preclinical experiments, neutrophil-derived nanovesicles loaded with dexamethasone delivered intranasally reduced lung inflammation with enhanced retention in a mouse model. Furthermore, studies in nonhuman primates have demonstrated safety, biodistribution, and translational feasibility of this delivery system. 80 The use of biomaterial delivery systems can be applied to other steroid drugs, such as budesonide, a glucocorticoid shown to reduce viral load in COVID-19. 81 A novel method of encapsulating this drug is using vesicles composed of bile acid salts formulated within the bilayer membrane of the nonionic surfactant molecules called bilosomes. In addition to sustained release profiles of the drug, in vivo evaluation of rat models with potassium–dichromate-induced acute lung injury showed reduced levels of inflammatory cytokines in the lungs with treatment. 82 These studies underscore how biomaterial-based delivery systems can enhance the therapeutic index of corticosteroids by enabling localized anti-inflammatory effects while minimizing systemic toxicity in severe COVID-19.
Collectively, these examples demonstrate how biomaterial-based nanocarriers may improve therapeutic efficacy in COVID-19 infections by enhancing tissue specificity, increasing bioavailability, and enabling sustained, localized drug release. It is important for researchers to carefully consider the safety of nanomaterials as they may be metabolized differently than other materials. 83
Vaccine Platforms
As a field, tissue engineers have studied the interplay between cells, signals, and the extracellular environment. Progenitor cells, growth factors, and biomaterial-based scaffolds have often been explored with the goal of tissue regeneration. For COVID-19 and other infectious diseases, similar strategies are now being harnessed using immune populations, adjuvants and/or cytokines, and different biomaterials as scaffolds or delivery systems. Recent vaccine platforms have leveraged biomaterials and tissue engineering principles to control the display of antigens, extend the duration of antigen delivery, target specific aspects of the immune system, and provide a sustained immune response. These platforms include lipid-based delivery systems for nucleic acid and protein antigens, protein and scaffold-based materials that optimize antigen presentation, and vesicular or cellular systems that mimic pathogens and cells to induce robust immunity.
Lipid-based vaccine systems
Nucleic acid vaccines, including mRNA and self-amplifying RNA (saRNA) vaccines, use engineered genetic material to control antigen expression in host cells. Due to their cell-free manufacturing and cost-effective production, they have gained popularity as rapidly developed vaccines against the SARS-CoV-2 virus.84,85 Nucleic acid-based vaccines are commonly administered in LNPs, which protect nucleic acids, promote cytoplasmic entry, and have an innate adjuvant effect through ionizable lipid motifs.86,87 For example, clinically approved vaccines such as BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Spikevax) are LNP-formulated mRNA vaccines, demonstrating how biomaterial-based delivery systems provide real-world protection against severe COVID-19 outcomes.88–90 From a biomaterials/tissue engineering perspective, LNPs can be modified through their material composition or architecture to dictate cellular interactions and immune activation. For example, the adjuvant effects of LNPs have been augmented by incorporating toll-like receptor agonists and squalene-based emulsions, some of which are under clinical development, as well as lipid-like materials such as ssPalm, which have preclinical efficacy.91–93 Some of these biomaterial-driven designs have moved beyond preclinical stages. For example, a Phase 1 clinical study of an LNP-encapsulated saRNA vaccine surrounded by oligonucleotides induced robust and durable neutralizing antibody responses effective against Delta and Omicron variants. 94 In addition to nucleic acid delivery, lipid-based formulations have also been used for protein antigens. For example, Phase 2 clinical studies of RBD–liposome vaccines incorporating monophosphorylated lipid A and cobalt–porphyrin–phospholipid showed more sustained immunogenicity than mRNA vaccines.95,96
Polymer/scaffold-based vaccine systems
Protein-based vaccines can benefit from engineered scaffolds to control antigen display and multivalency through scaffold architecture and material composition. For example, protein antigens can be conjugated onto the surface of poly(ethylene glycol)-b-poly(lactic acid) polymer nanoparticles to create a scaffold with rapidly replaceable antigens that enhances neutralizing responses in preclinical models, particularly in combination with adjuvants. 97 A recent clinical trial demonstrated efficacy of using a poly(lactide-co-glycolide) scaffold as a vaccine for metastatic melanoma, suggesting that similar scaffold approaches may be effective against SARS-CoV-2.98,99 Ferritin-based scaffolds utilize symmetrical octahedral cage structures to provide thermal and chemical stability, displaying enhanced binding affinity of presented viral antigens to neutralizing antibodies in preclinical models.100,101 Multiepitope designs, such as ferritin nanocages in 6-helical bundle spike scaffolds or dodecahedral miniferritin constructs, have been shown in both computational and preclinical models, including mice and nonhuman primates, to induce immune responses that persist across variants.100,102–105 Porosity is another scaffold property that has been exploited to better deliver antigens. Porous scaffolds, including mesoporous silica rods, microporous annealed particles, and hydrogels, have been shown in preclinical murine models to recruit and activate antigen-presenting cells and facilitate greater antigen exposure, highlighting how influencing the porosity and mechanical properties of structures can induce immune responses.99,106,107
Vesicular/cellular-based vaccine systems
Vesicular and cellular vaccine platforms use biomimicry to enhance antigen presentation and induce immune responses. Virus-like particles (VLPs) are nanoparticles mimicking the structure, size, and symmetry of an original virus while presenting repetitive immunogenic surfaces without viral genetic material. VLPs can present spike, RBD, nucleocapsid, membrane, and envelope proteins to stimulate dendritic cells and neutralizing antibody production.108–113 Phase 1/2 clinical trials of various VLP formulations have demonstrated durable antibody responses adaptable to emerging variants.114,115 Extracellular vesicles (EVs) are another platform capable of protecting their cargo and facilitating greater cellular uptake and antigen delivery. Preclinical studies have shown that EVs engineered to carry RBD, nucleocapsid proteins, or mRNA are effective in delivering cargo to antigen-presenting cells and eliciting antigen-specific antibodies.116,117 Bacterial outer membrane vesicles, like synthetic bacterial vesicles derived from Pseudomonas aeruginosa engineered to express spike protein, have been investigated as promising vaccine platforms. These vesicles contain essential molecules recognized by toll-like receptors and have demonstrated antigen-specific immune responses in early preclinical models.118,119 Adeno-associated virus (AAV) capsids are viral vector vaccine platforms that include capsid that can be engineered to display antigens, such as AAV6 expressing RBD, and have been demonstrated to enhance humoral and cellular immunity in mice and rabbits.120,121 Universal vaccine cells developed from human stem cells and engineered to mimic a lytic viral infection to result in apoptosis have been explored as platforms to deliver antigens and have been successful in stimulating host immunity in nonhuman primates. 122 Collectively, these vesicular and cellular systems show how surface organization, nanoscale architecture, and mimicry can be used to modulate immune responses in various preclinical models.
In summary, advances in vaccine platforms highlight how tissue engineering and biomaterials can be leveraged to enhance antigen delivery and immune activation. In addition to improving antigen delivery through the design of novel scaffolds, there are even more exciting future directions for tissue engineering to boost vaccine efficacy. For example, artificial antigen-presenting cells are being engineered and injected in mice to optimize response to activation signals. 123 While rare adverse reactions to COVID-19 vaccine platforms have been reported,124,125 the overall evidence supports the safety and effectiveness of current clinically approved COVID-19 vaccines.17,126 Together, these advancements highlight how biomaterials and tissue engineering are being used to create next-generation vaccines.
Conclusions
Tissue engineering and biomaterials have had a critical role in the response to SARS-CoV-2 during the past 5 years. Our culture models have shifted from monolayers of primate-derived kidney cells to human cells in 3D conformations recapitulating tissue architecture. Our field has contributed to the development of LNPs in mRNA vaccines critical to blunting mortality during the early waves of the COVID-19 pandemic. From physiologically relevant in vitro models to next-generation drug delivery systems and vaccine platforms (Table 1), these approaches are essential for advancing our understanding of the virus and our strategies for treatment.
Summary and Examples of Tissue Engineering Models, Drug Delivery Systems with Examples of Delivered Therapeutics, and Vaccine Technologies Used in SARS-CoV-2 Research
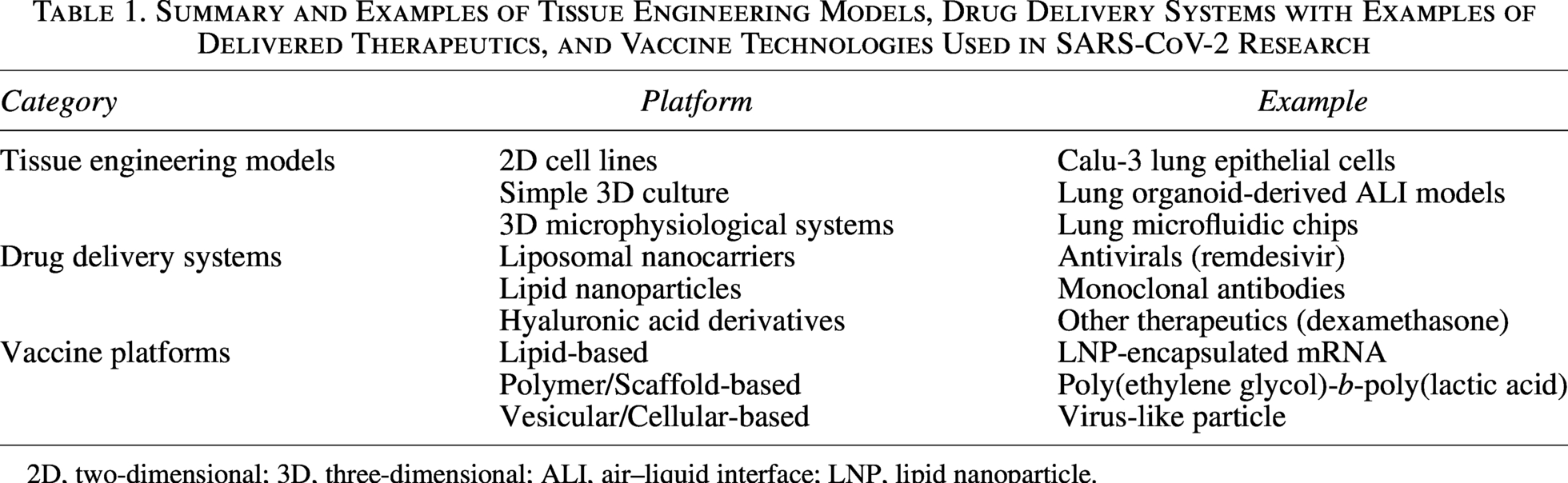
2D, two-dimensional; 3D, three-dimensional; ALI, air–liquid interface; LNP, lipid nanoparticle.
The potential of tissue engineering in contributing to SARS-CoV-2 and broader respiratory pandemic research has not been fully realized. Additional advancements in rapid, patient-derived 3D tissue models will enable more physiologically relevant models of virus pathogenesis and therapeutic responses. Better incorporation of immune populations in 3D tissue models will improve the accuracy of modeled infection. However, limitations in scalability and throughput continue to restrict the widespread use of these. Additionally, limited access to high-containment facilities during the pandemic posed a major barrier to further studying SARS-CoV-2, highlighting the need for foresight in improving infrastructure and policies for continued scientific progress during future outbreaks while maintaining safe environments for researchers. 127 While many different delivery vehicle systems have been studied using preclinical models, tissue engineers and biomaterial scientists need to continue to translate these technologies to clinical trials. Further advancements in simplifying supply chains and storage will further allow for more rapid deployment of treatment. Altogether, tissue engineering and biomaterials are crucial tools in pandemic research and treatment. Continued innovation in these fields will be important for addressing emerging variants and strengthening our response to future pandemics.
Authors’ Contributions
W.K.B. and A.R.M. contributed to the investigation and writing (original draft and review & editing) of this work. A.M.T. contributed to conceptualization, project administration, supervision, and writing (review & editing) of this work. No artificial intelligence was used in the preparation of this article.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No outside funds were sourced for this work.