
Abstract
Sensorineural hearing loss is a major public health concern, yet its treatment remains limited by the anatomical complexity and biological barriers protecting the cochlea. Among these, the round window membrane (RWM) constitutes a key interface for local drug delivery to the inner ear. However, passive diffusion via intratympanic injection is often insufficient, particularly for hydrophilic, large, or negatively charged molecules such as gene therapy vectors. This systematic review aimed to evaluate biomechanical and biochemical strategies to enhance RWM permeability for more efficient and targeted drug delivery to the inner ear, including direct permeability modulation of the RWM properties or indirect enhancement mechanisms increasing drug delivery without altering intrinsic membrane permeability. Following Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines, a comprehensive literature search was conducted using the Scopus, MEDLINE/PubMed, Cochrane, and CINAHL electronic databases. In vivo studies and clinical trials involving biochemical or biomechanical strategies to enhance RWM permeability were included. Risk of bias was assessed using the SYRCLE (Systematic Review Center for Laboratory Animal Experimentation) tool. Out of 1776 screened articles, 89 met the inclusion criteria. Four biochemical approaches and three biomechanical strategies were identified, respectively: (1) hydrogels, thermogels, and emulsions, (2) nanosystems, (3) microsystems, and (4) permeabilizers, and (1′) sonoporation, (2′) acoustic stimulation, and (3′) magnetic systems. Most studies reported improved drug delivery to the inner ear or therapeutic efficacy. While earlier research focused on hydrogels, thermogels, emulsions, permeabilizers, and acoustic stimulation for small molecules such as corticoids and antioxidants, recent studies increasingly explore nanosystems, microsystems, sonoporation, and magnetic methods to facilitate the delivery of larger agents, including gene therapy. This review also highlights that while many strategies are already available and effective in animal models, further research is essential to facilitate the clinical translation of both existing and emerging delivery methods.
Impact Statement
This systematic review highlights the critical role of round window membrane permeability in optimizing inner ear drug delivery for the treatment of sensorineural hearing loss. By synthesizing current biochemical and biomechanical enhancement strategies, it provides the first comprehensive overview of methods designed to improve delivery efficiency, including for large therapeutic agents such as gene therapy vectors. The findings underline that clinical translation of novel inner ear therapies depends not only on pharmacological efficacy but also on overcoming anatomical barriers. This work identifies key research gaps and offers a foundation for developing minimally invasive, targeted delivery systems.
Keywords
Introduction
Hearing loss represents a growing public health concern, affecting an estimated 430 million people worldwide. It is estimated that 2.5 billion people will have some degree of hearing loss by 2050, with more than 700 million requiring hearing rehabilitation (World Health Organization, 2024). Sensorineural hearing loss (SNHL) is the most prevalent form, often caused by irreversible damage to the inner ear’s hair cells or auditory neurons.1–3 Current treatments, such as hearing aids and cochlear implants, mainly address symptoms rather than underlying causes.4,5
Recent advances in gene therapy and regenerative medicine aim to restore hearing by acting on molecular and cellular mechanisms.6,7 However, delivering therapeutic agents effectively to the inner ear remains a major challenge.8–11 The inner ear is an isolated, complex, and fragile organ, and the presence of biological barriers restricts the passage of substances into the cochlea. 9 Indeed, traditional approaches, such as systemic administration, are limited by the blood–labyrinth barrier, resulting in reduced drug penetration and increased systemic side effects. 12 Intratympanic injections, where the drug is administered into the middle ear cavity, have improved local delivery. This conservative approach, in contrast to invasive intracochlear injections, allows passive diffusion through the round window and oval window membranes. However, intratympanic delivery remains limited by variable drug distribution, potential damage to middle ear structures, rapid clearance via the Eustachian tube, and possible contamination of adjacent tissues.13,14 Direct injections through a cochleostomy or through the round window membrane (RWM) are an alternative to increase drug uptake into the cochlea, 15 but they are associated with a significant risk of trauma to the inner ear. These limitations have driven the development of strategies to enhance RWM permeability and improve more efficient and targeted drug delivery to the inner ear.
The RWM is a thin, trilaminar structure providing a direct route from the middle ear to the scala tympani of the cochlea. Histologically, it consists of three distinct layers: an outer epithelium facing the middle ear, a central layer of connective tissue, and an inner epithelium facing the inner ear, which contains the perilymph. It is located in the round window niche, a triangular bony structure. In humans, its thickness averages about 60 µm 16 compared with 10 µm in rodents, 17 with a surface area of approximately 2.08 mm2 (1.90 × 1.54 mm).18,19 Functionally, the RWM acts as a selective barrier, allowing the passage of molecules based on size, lipophilicity, charge, and concentration gradients. Small, lipophilic, and positively charged molecules diffuse passively, while larger molecules require active transport mechanisms. While this selective permeability protects the cochlea, it presents a significant obstacle to the delivery of large therapeutic molecules such as gene therapy vectors. As a result, enhancing RWM permeability has become a critical point in the development of effective, minimally invasive inner ear drug delivery strategies. The ability to modulate RWM barrier properties is crucial to improve treatment precision and efficacy in SNHL and other inner ear disorders.
Permeability enhancement strategies of interest include direct permeability modulation of the RWM properties or indirect enhancement mechanisms increasing drug delivery without altering intrinsic membrane permeability. These strategies are divided into two main categories: biomechanical and biochemical approaches. Biomechanical methods use physical forces to increase drug passage through the RWM. For example, ultrasound coupled with microbubbles (USMBs) generates cavitation, transiently disrupting tight junctions in the outer epithelium. 20 Magnetic microrobots21,22 offer another innovative solution, navigating biological structures to deliver drugs directly to the inner ear.
In parallel, biochemical strategies employ agents such as surfactants, 23 high-osmolarity solutions, 24 or enzymes 25 to disrupt lipid bilayers, loosen tight junctions, or alter the extracellular matrix, increasing RWM permeability, nanoparticles, and nanocarriers, with tunable sizes and surface properties, to enhance drug penetration through the RWM26,27 or biocompatible hydrogels to prolong drug residence time in the middle ear and promote gradual diffusion into the inner ear.9,28
The clinical potential of these strategies is considerable. Overcoming the RWM barrier could enable the delivery of a broader range of therapeutics, including gene therapy vectors currently under development,29–31 directly to the inner ear, opening new perspectives for the treatment of SNHL. However, there is a need to validate the safety and reversibility of these permeability enhancement strategies, as the preservation of hearing and cochlear integrity is essential. In this context, the present study investigates the efficacy and safety of biomechanical and biochemical methods for enhancing RWM permeability. Despite growing demand for safe, minimally invasive drug delivery systems compatible with novel inner ear therapies, no comprehensive systematic review has yet summarized current strategies to enhance RWM permeability and their outcomes, as well as the experimental models used to evaluate them in vivo. Our findings provide a foundation for developing minimally invasive, targeted therapies, in particular gene therapy, for inner ear disorders, advancing the field of inner ear drug delivery.
Materials and Methods
Protocol
The systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines based on the Population, Intervention, Comparison, and Outcome (PICO) method to define the search strategy. The review protocol was registered in the PROSPERO database (CRD42024605251).
Focused question
The question to be addressed by the review was defined as: “What biochemical or mechanical strategies have demonstrated efficacy in enhancing the permeability of the round window membrane for drug delivery to the inner ear in vivo, compared to standard drug deposition in the middle ear?”
Selection criteria
In vivo studies investigating biochemical or biomechanical strategies to improve the RWM permeability for drug delivery to the inner ear were included. Inclusion and exclusion criteria are presented in Supplementary Table S1.
Search strategy
The PICO reporting system was used to develop the search strategy (Table 1). A structured electronic search for articles published in English was conducted using Scopus, MEDLINE/PubMed, Cochrane, and CINAHL electronic databases, up to June 18, 2025. Cited articles of the included studies were also assessed.
Search Strategy Based on the PICO Reporting System
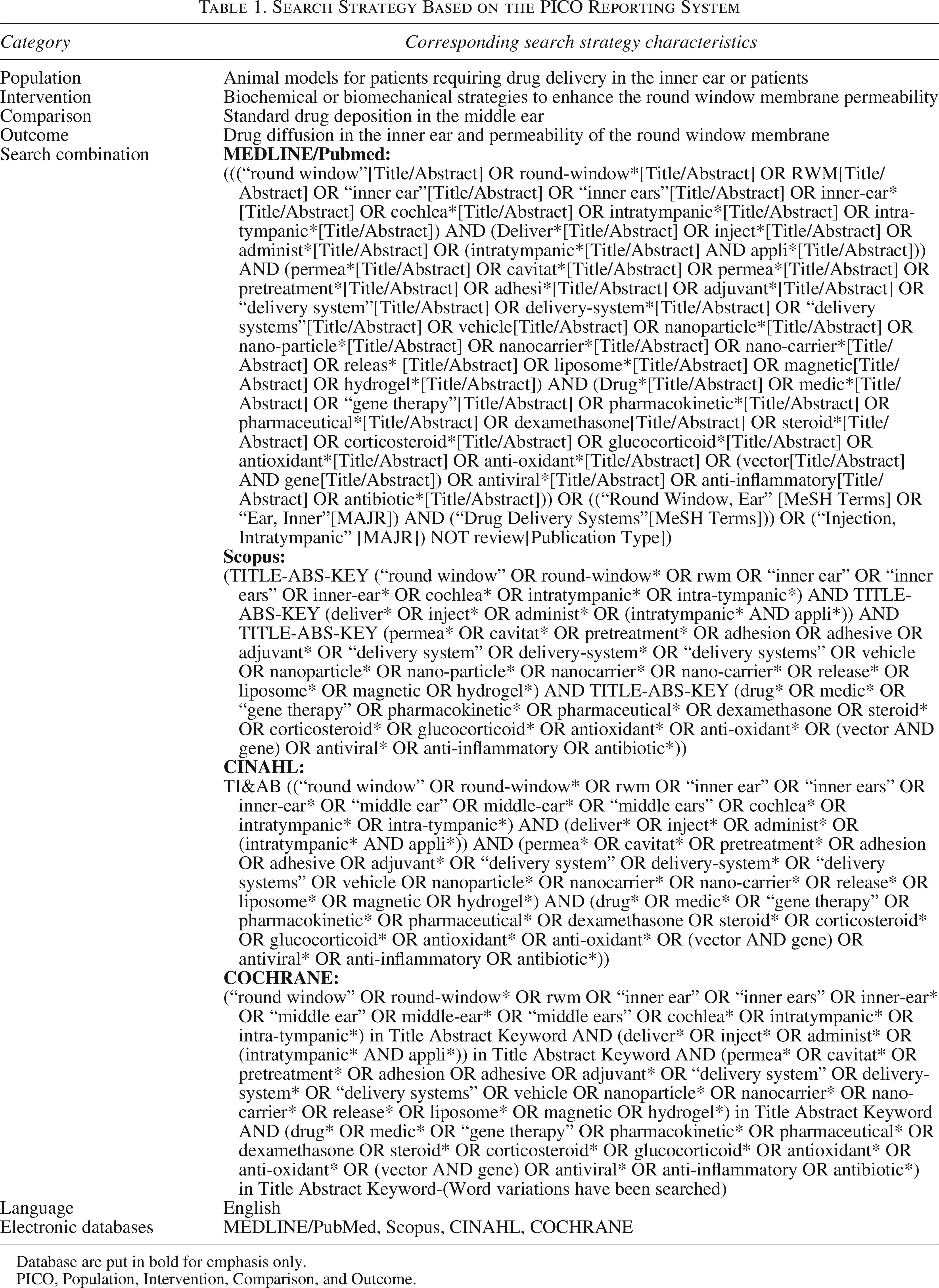
Database are put in bold for emphasis only.
PICO, Population, Intervention, Comparison, and Outcome.
Screening method and data extraction
All references retrieved from the search strategy were imported into the RAYYAN software, a recognized screening system. Duplicates were eliminated, and the articles were screened by two reviewers working independently (A.B. and O.K.). Based on inclusion and exclusion criteria, the selection was conducted in two stages: (1) title/abstract screening and (2) full-text screening. A comparison of selected articles was performed, and all disagreements were resolved by a third reviewer (RD). Exclusion criteria were prioritized as follows: (1) not in English; (2) review, conference abstract, case study, or case report; (3) not an in vivo study on mammalian animal model; (4) no drug delivery to the inner ear, delivery via another route than the RWM, invasive approach (intracochlear injections), or no enhancement strategies of the RWM permeability; (5) no comparison with standard drug deposition in the middle ear; and (6) studies that do not report on drug diffusion or permeability of the RWM or treatment efficacy.
For eligible studies meeting the inclusion criteria, both reviewers conducted a thorough review of the full text using a data extraction form (Microsoft® Excel, Microsoft Corporation, Redmond, WA, USA). Data were extracted from the text, tables, and graphs and then organized into two tables.
The first table included the following elements: authors, year of publication, animal model, method to induce hearing loss, if applicable, type of drug, type of RWM permeability-enhancing strategy, parameter assessed, method of assessment, and results.
The second table contained the following elements: authors, year of publication, outcomes on delivery assessment, outcomes on safety assessment, and outcomes on efficacy assessment.
Science mapping analysis
Science mapping analysis of scientific domains was performed from the list of included articles by using keyword co-occurrence networking on VOSviewer (free software, version 1.6.18, Center for Science and Technology Studies, Leiden University, Leiden, The Netherlands, 2022).
Network analysis of the keywords was generated from the matrix of retrieved papers (threshold value at 4). The term–document matrix allowed the measurement of document similarities between clusters of topics.
Quality assessment and risk of bias
The risk of bias within the included studies was assessed independently by two reviewers. The SYRCLE’s risk of bias tool for animal studies was used to perform the risk of bias. The items evaluated (“yes,” “unsure,” and “no”) were (1) “Was the allocation sequence adequately generated and applied?” (2) “Were the groups similar at baseline or were they adjusted for confounders in the analysis?” (3) “Was the allocation adequately concealed?”, (4) “Were the animals randomly housed during the experiment?” (5) “Were the caregivers and/or investigators blinded from knowledge which intervention each animal received during the experiment?” (6) “Were animals selected at random for outcome assessment?” (7) “Was the outcome assessor blinded?” (8) “Were incomplete outcome data adequately addressed?” (9) “Are reports of the study free of selective outcome reporting?” and (10) “Was the study apparently free of other problems that could result in high risk of bias?”
Reviewers A.B. and O.K. conducted the bias assessment. When no consensus was reached, any discrepancies were resolved by a third reviewer (RD). Formatting was done with the robvis visualization tool.
Qualitative and semiquantitative comparative framework
As a formal statistical meta-analysis is not feasible due to the heterogeneity of the studies in terms of methodologies, a comparison of ranking score is performed, according to the ranking score described in Figure 1, by two reviewers working independently (A.B. and P.R.). All disagreements were resolved by a third reviewer (O.K.). Criteria were selected by the authors to reflect the quality of scientific evidence for delivery, efficacy, and safety assessment, based on extracted results. The objective is to determine which strategies are closest to human applicability. The heterogeneity of the studies also originated from the large possibilities in methodology, whether for delivery, efficacy, and safety assessment. Therefore, a qualitative ranking is performed for each type of outcomes, to summarize the usefulness of outcomes for delivery evidence, spatial distribution information, safety evidence, degree of applicability, risk of misinterpretation, and based on this information, whether it is recommended as primary outcome. Key strengths and main limitations are also summarized.
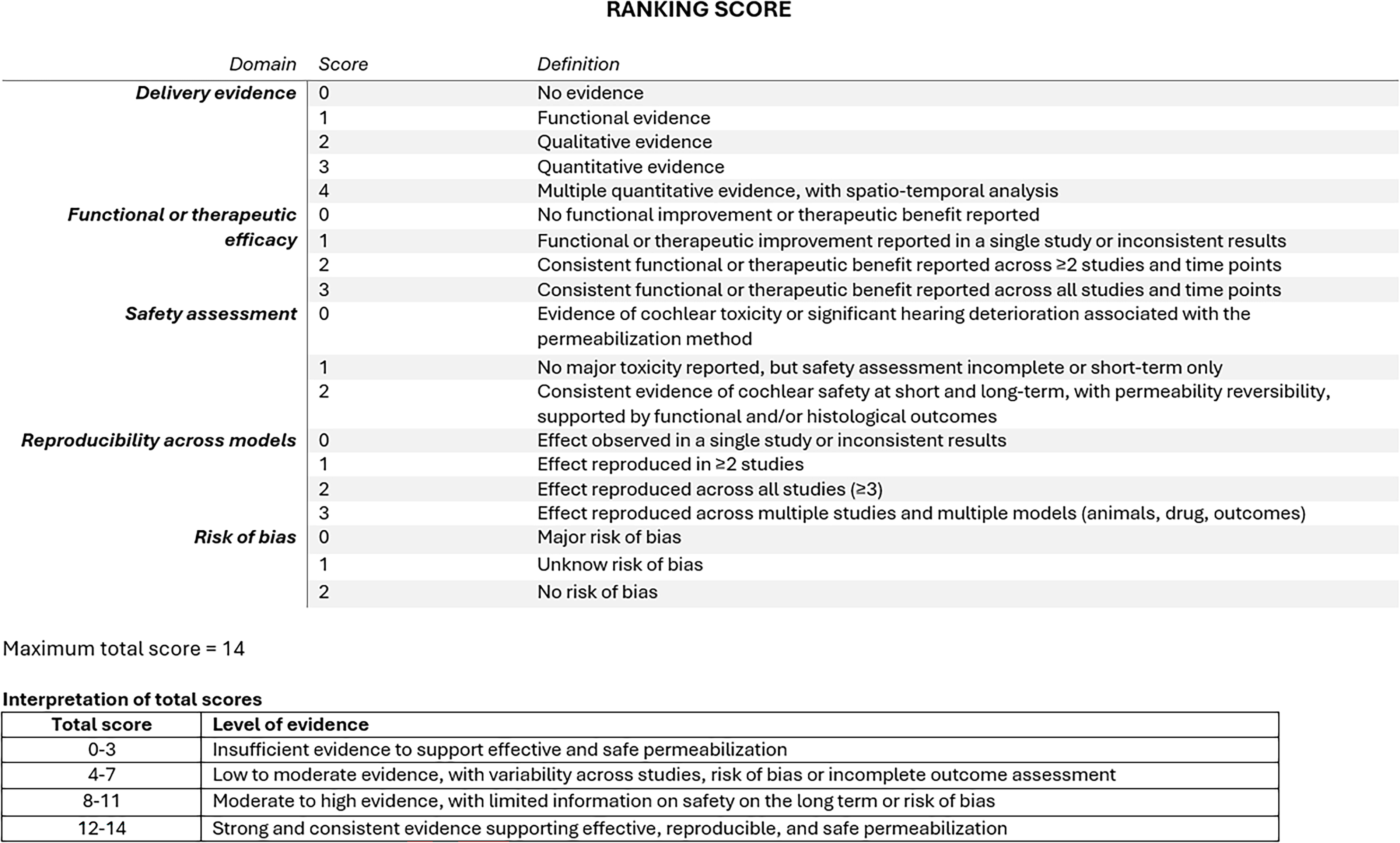
Semiquantitative scoring system used to rank and assess the level of evidence of strategies for enhancing RWM permeability. RWM, round window membrane.
Results
Systematic review following PRISMA guidelines
The database search using the PICO model yielded 2621 articles: 822 articles from MEDLINE/PubMed, 1646 articles from Scopus, 104 articles from Cochrane, and 149 articles from CINAHL. After removal of duplicates and screening of titles and abstracts, 283 articles were selected for full-text analysis and evaluation. Following this stage, 195 articles were excluded, and 2 could not be retrieved. Ultimately, 86 articles were included and supplemented by 3 additional studies identified through reference screening, resulting in a total of 89 included articles (Fig. 2).
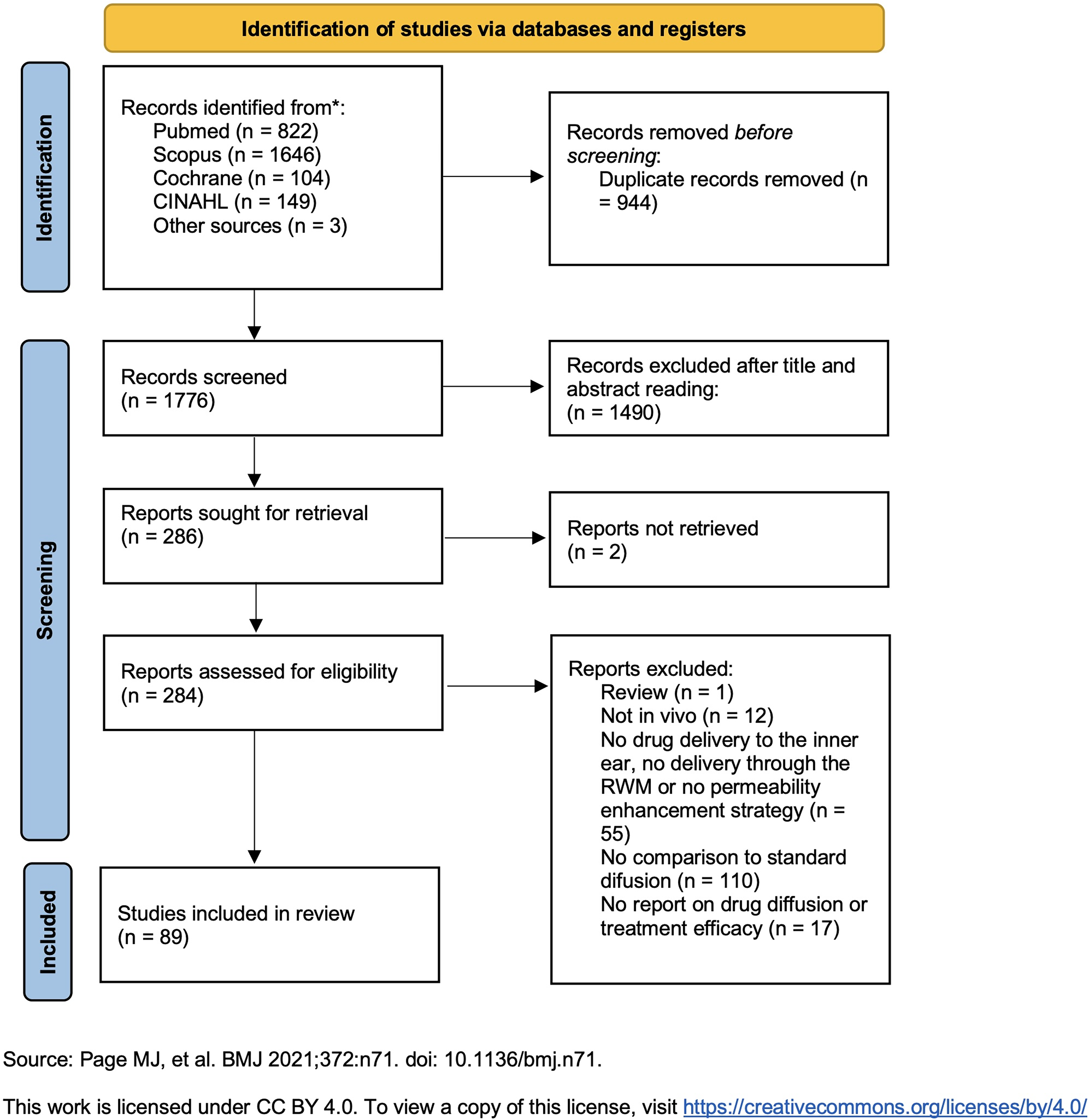
Flow diagram of studies selection according to PRISMA guidelines. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
A scientific map displayed the spatial representation of keyword relationships (Fig. 3), with keywords depicted by nodes of various colors and sizes. Each color corresponds to a thematic group, and the connections between them are illustrated by lines. The size of each node is proportional to its degree. 32 The most recurrent keywords included animals, guinea pigs, dexamethasone, male, drug delivery, mice, hearing loss, drug liberation, and inner ear. These keywords highlight the major areas of research related to inner ear drug delivery and RWM permeability enhancement.
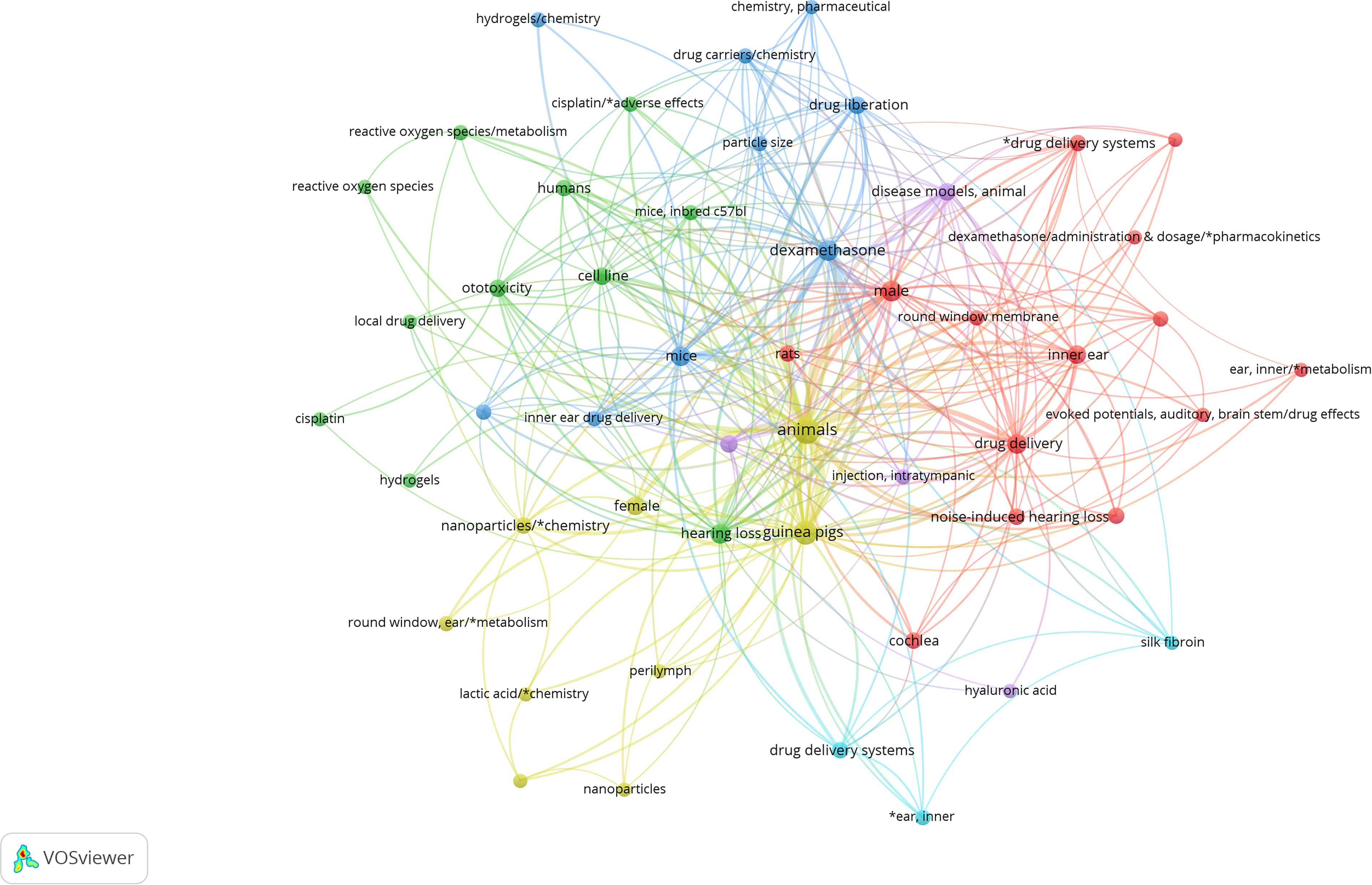
Science mapping analysis of scientific domains: keyword co-occurrence networks among the included articles. Each node size is proportional to its degree, and the link’s thickness represents the tie strength.
A quantitative meta-analysis was not feasible due to the important heterogeneity in experimental models (animal model, drug classes, enhancement protocols, and outcomes). Therefore, a qualitative analysis and semiquantitative ranking were performed by extracting study characteristics, methodology, and outcomes. Specific attention was given to enhancement strategies allowing gene therapy delivery.
Quality assessment and risk of bias
The quality assessment results are presented in Figure 4. Risk of bias was evaluated using the SYRCLE tool. Most studies did not mention blinded assessment or randomization; however, they reported that the experiments were conducted in accordance with local ethical guidelines and were apparently free of other problems that could result in high risk of bias. Only three studies33–35 were associated with a high risk of bias regarding data acquisition or data analysis.
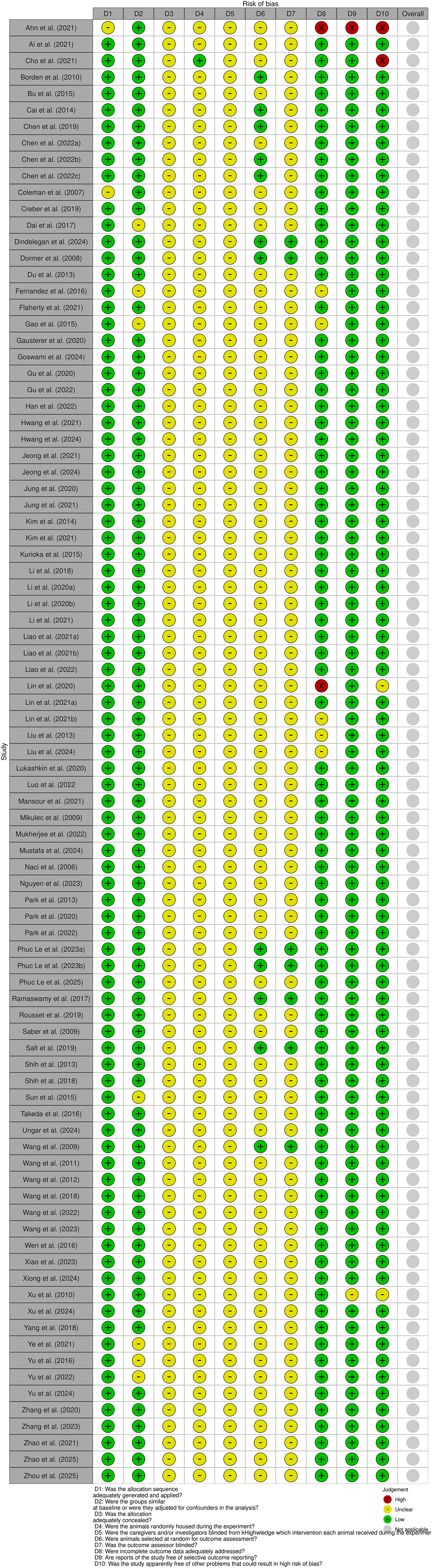
Quality assessment of selected studies using the SYRCLE method. SYRCLE, Systematic Review Center for Laboratory Animal Experimentation.
Study characteristics and methodology
Main characteristics
The main characteristics of the included studies are summarized in Table 2. The selected articles were published between 2007 and 2025. Among these, 19 studies34,35,37–53 explored biomechanical strategies, while 69 focused on biochemical approaches.23–25,28,33,36,54–116
Summary of Study Characteristics

ABR, measurement of ABR thresholds or ABR threshold shifts; CM (agent), confocal microscopy marking the agent to perform a qualitative assessment; qCM (agent), confocal microscopy marking the agent to perform a quantitative assessment; DIHL, drug-induced hearing loss; fluorescence (fluorophore), use of fluorescence to visualize the delivery of a fluorophore; ELISA, Enzyme-Linked Immunosorbent Assay; GFP, Green Fluorescent Protein; HC, hair cells; H&E staining (tissue), histological analysis using hematoxylin and eosin staining of the tissue of interest; IHS: immunohistochemical staining; LC–MS regroups, HPLC–MS, UHPLC–MS, IGF-1, Insulinlike Growth Factor 1; LC–MS/MS, LC, and MS techniques to quantify drug concentration in the perilymph and/or the amount of drug in cochlear tissues; MicroCT, microcomputed tomography to quantify the residence time of the drug in the middle ear; NIHL, noise-induced hearing loss; OC, organ of Corti; PLGA, Poly(lactic-co-glycolic acid; RTqPCR, Reverse Transcription Quantitative Polymerase Chain Reaction; RWM, round window membrane; SGN, spiral ganglion neuron; SNHL, sensorineural hearing loss; SV, stria vascularis; USMB, ultrasound microbubbles; WB, Western blot.
Guinea pigs were the most commonly used animal model (62%),24,25,28,35–41,43,44,46,47,50,51,53,57,61–64,66,69–73,75–78,81,84,85,87–90,92,93,95–100,102,103,105–108,111,112,114,117 followed by mice (22%)34,42,48,52,65,67,68(p202),74,75,80,82,83,86,91,93–95,101,104 (p201),110,113 rats (13%),23,33,45,49,54–56,60,74,79,93,109,115 and, more rarely, rabbits,81,116 chinchillas, 59 and humans (one clinical study) 53 (Fig. 5).
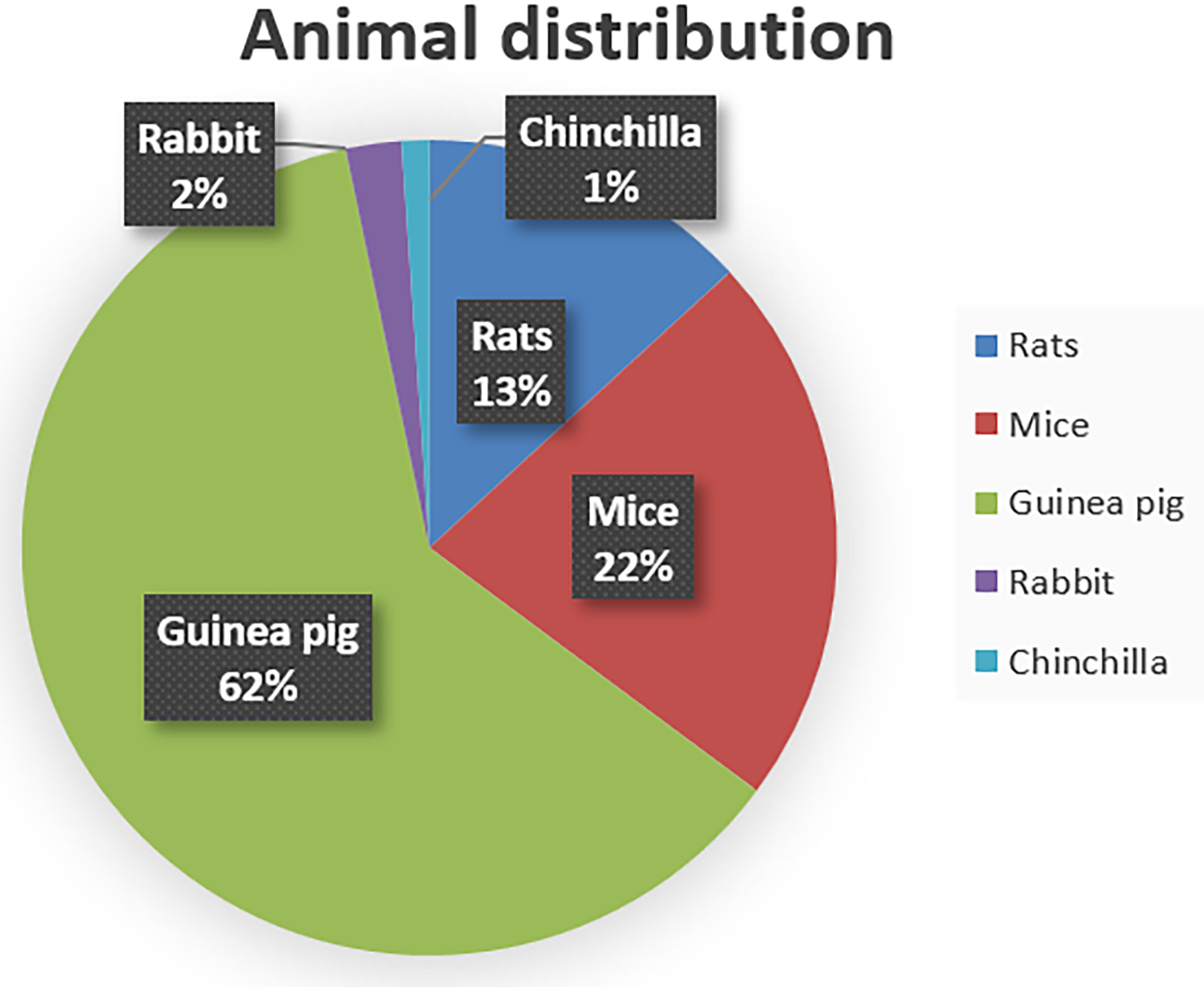
Distribution of the animal models used in the selected articles.
In terms of therapeutic agents, corticosteroids were the most studied (50% of articles),23,33,37,38,45,48,50,52–57,62–64,67,69–80,82,84–86,91,92,97,101,105–107,109–112,114,116 followed by antioxidants (16.3%)28,36,68,77,81,88,89,93–96,98–100,118 (Fig. 6). Other studies focused on delivery of dyes (fluorophore, dye, contrast agent, etc.),24,35,43,60,99,103,104 ototoxic agents,40,45–47,58,65 gene therapy vectors,25,44,49,61,113 growth factors,33,39,41,83,87,102 nanoparticles,42,51 or other agents.34,59,66,90,115 Ototoxic agents have the particularity to induce hearing loss and inflammatory responses, allowing to quantify their efficacy by assessing hearing loss or vestibular defects.
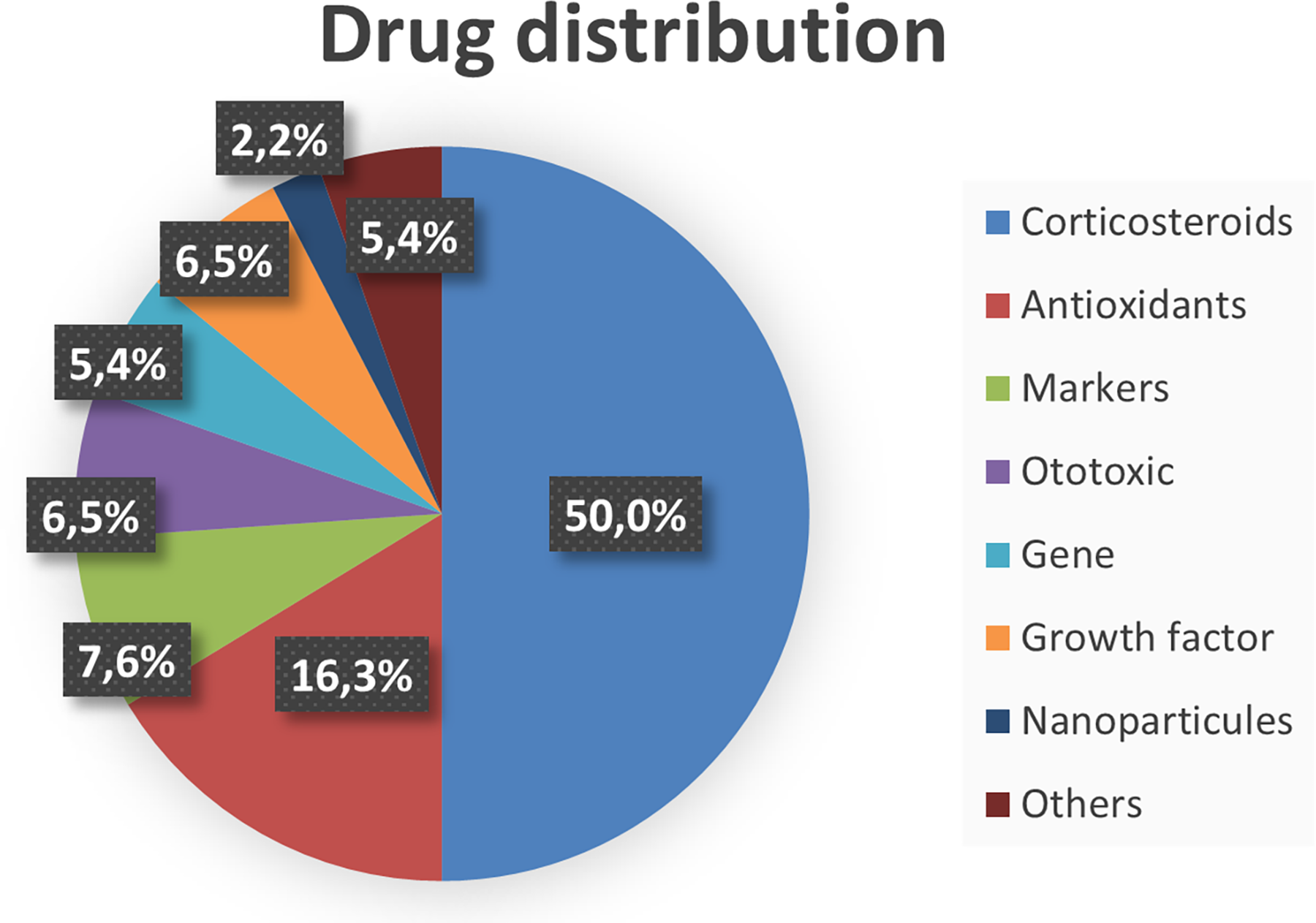
Distribution of the drug delivered in the selected articles.
A model of hearing loss was used in 58% of the selected studies, induced mainly by ototoxic agents (34%),34,36,37,46–48,52,54,55,58,68,73–75,79,82,84–86,88,91,92,96,98,100,109,114,115 acoustic trauma (22%),23,33,38(p201), 41,49,56,59,62,69,83,87–90,93–95,97,105,110 irradiation (1%), 80 or sudden SNHL (1%). 53 Chemically induced models included cisplatin, kanamycin, sodium salicylate, gentamicin, or neomycin (Fig. 7).
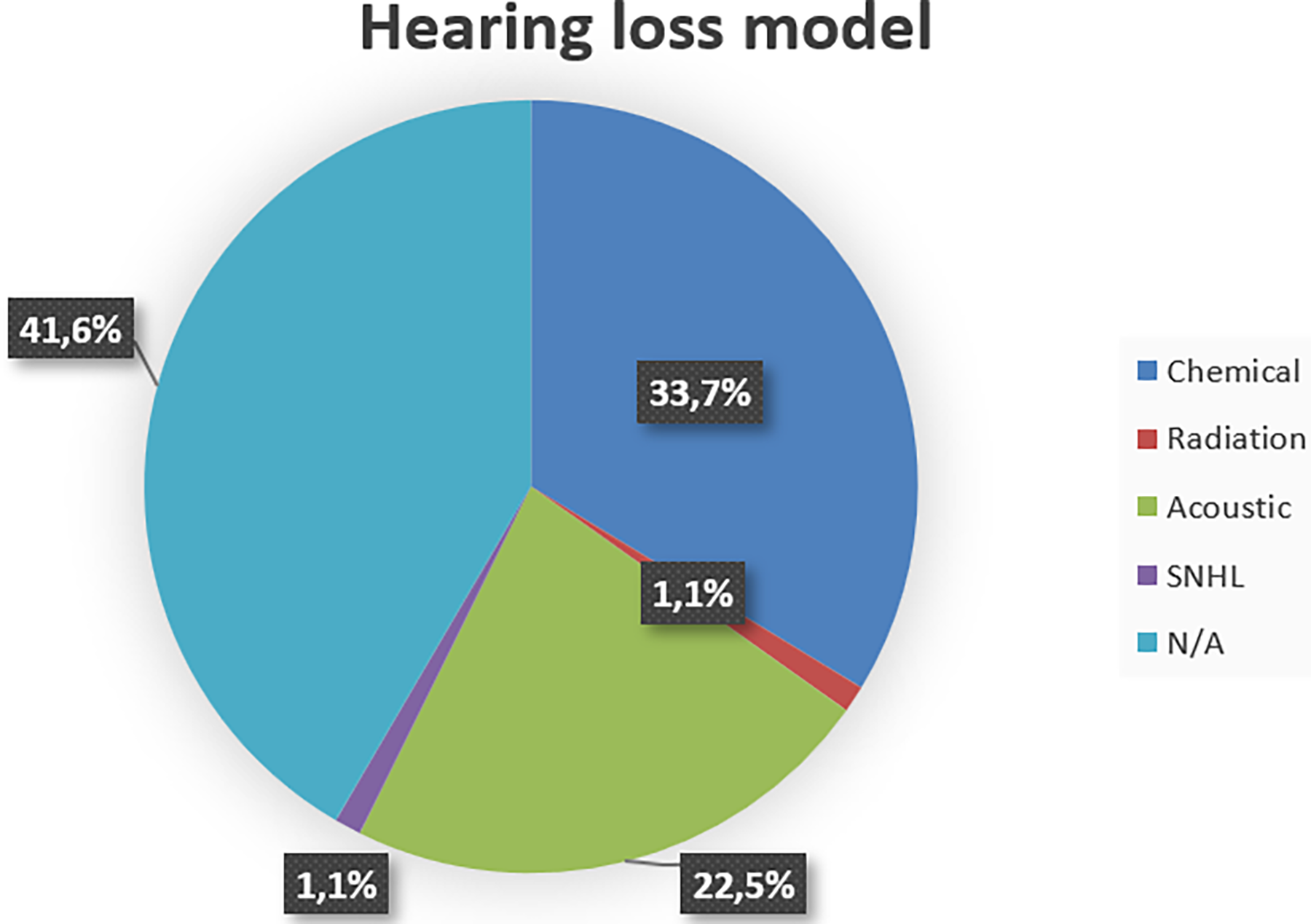
Distribution of the hearing loss model used in the study (N/A: not applicable, no hearing loss model was used in the study).
Delivery, safety, and treatment efficacy assessment
To assess agents’ delivery, the main method relied on the quantification of drug concentration in the perilymph and cochlear uptake using liquid chromatography-mass spectrometry (LC–MS) techniques.23,28,36,45,50,53,54,62–65,67–72,74–78,81,82,85,89,95,99,100,102,106,107,110,111,114 To validate drug penetration into the cochlear, 25 studies delivered fluorophore into the perilymph,33–36,40,42,43,50,67,68,74,78,85,86,88,89,91–93,95,96,98,103,112,115 and 11 used confocal microscopy of the organ of Corti to quantify or visualize drug uptake in the inner ear cells.25,40,41,43,44,49,61,87,104,113,115
For safety assessment, histological analyses were mostly employed (26 studies).34,63,64,66,67,74,77,78,80,86,87,89,92,96,97,99,100,102,105,107,108,110,111,114,115 Mean auditory brainstem response (ABR) threshold and ABR threshold shift measurements, as well as confocal microscopy of the organ of Corti, were the following most used methods (12 studies).25,35,37,39,40,42,43,61,69,71,76,78
Treatment efficacy was mostly determined using mean ABR threshold and ABR threshold shift measurements (47 studies),23,25,33,36,38,41,48,49,52–54,59,62,65,68,69,73,75,79,80,82–94,96–98,100–102,105,110,114,115,118 as well as qualitative and quantitative assessment of hair cell survival (34 studies). Several articles used transcription or protein (immunohistochemical staining, five studies36,38,41,79,83; ELISA, three studies82,87,89; Western blot, six studies68,82,83,87,101,115; RT-qPCR, four studies41,82,91,115) analysis to quantify expression of genes or proteins involved in cellular growth, protection, or antioxidant activity.
Qualitative ranking of outcomes
A qualitative ranking of outcome reliability as indicators of effective delivery was performed based on extracted results (Table 3). As described in the section above, outcomes were highly variable from one study to another and used in various contexts. This table aims to summarize the reliability and scope of application of these outcomes for future studies. This qualitative ranking also highlights that while specific outcomes (LC–MS, ABR, histology, and quantitative immunofluorescence) are highly reliable, a combination of different outcomes is necessary to validate delivery, safety, and treatment efficacy.
Qualitative Ranking of Outcomes Reliability as Indicators of Effective Delivery
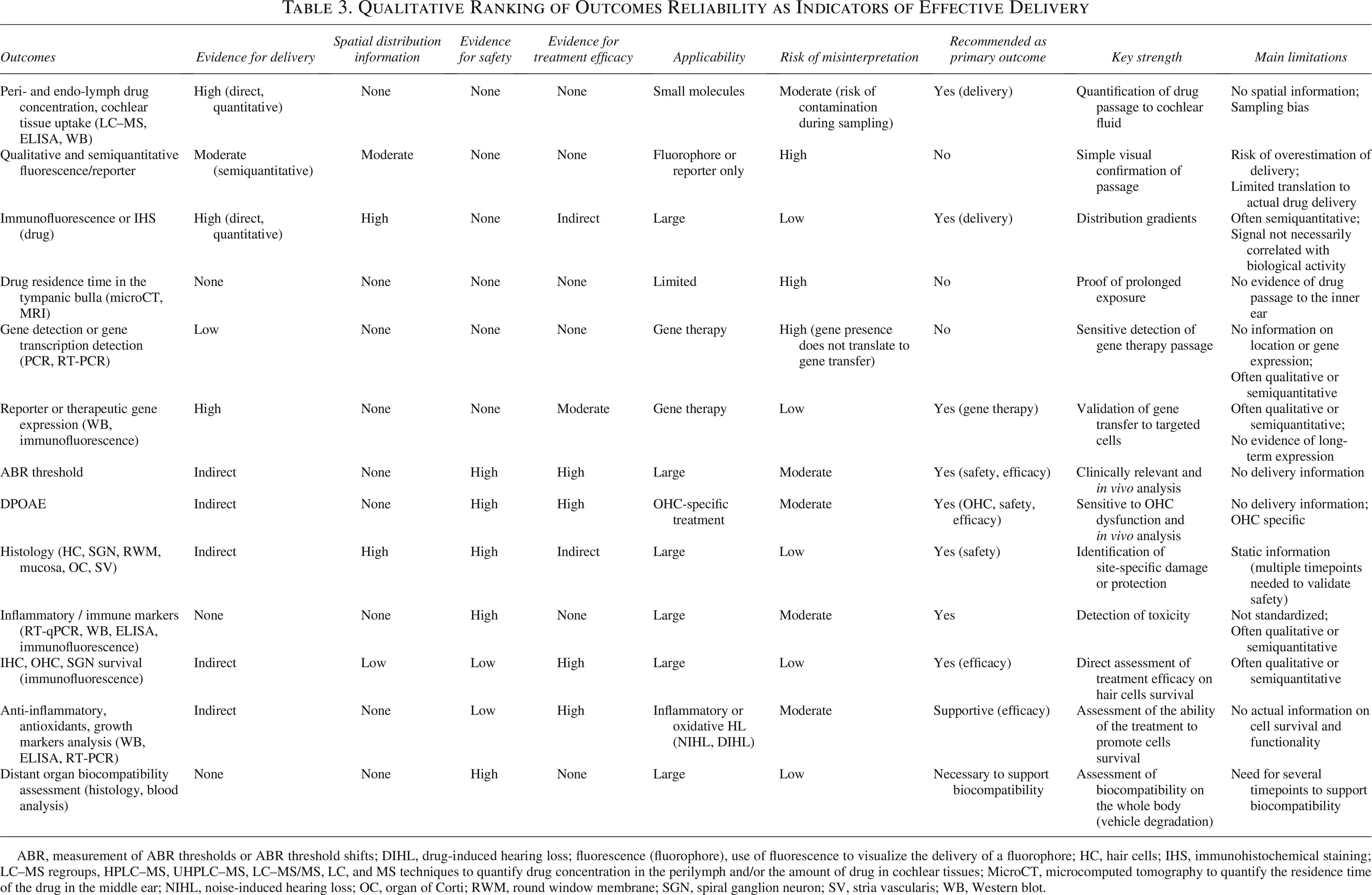
ABR, measurement of ABR thresholds or ABR threshold shifts; DIHL, drug-induced hearing loss; fluorescence (fluorophore), use of fluorescence to visualize the delivery of a fluorophore; HC, hair cells; IHS, immunohistochemical staining; LC–MS regroups, HPLC–MS, UHPLC–MS, LC–MS/MS, LC, and MS techniques to quantify drug concentration in the perilymph and/or the amount of drug in cochlear tissues; MicroCT, microcomputed tomography to quantify the residence time of the drug in the middle ear; NIHL, noise-induced hearing loss; OC, organ of Corti; RWM, round window membrane; SGN, spiral ganglion neuron; SV, stria vascularis; WB, Western blot.
Study outcomes
Biochemical strategies
Biochemical strategies were categorized into four main groups: hydrogels, thermogels, and emulsions (32 articles)28,54–68,70–83,107,113; nanosystems (22 articles)36,68,84–93,95–100,102–104,114; microsystems (8 articles)33,94,105–107,109,115,118; and permeabilizers (7 articles)23–25,110–112,116 (Table 4). These strategies primarily relied on indirect enhancement strategies, focusing on increasing residence time28,54–68,70–83,107,113 or improving transport through the RWM using carriers,11,36,84–93,95–100,102–104 except for permeabilizers,23–25,110–112,116 which directly increase permeability through weakening of the membrane integrity.
Summary of Study Outcomes

The assessed biological phenomena (for instance, Cochlear uptake, Hair cell count) are put in bold for emphasis and separation of corresponding results.
ABR, measurement of ABR thresholds or ABR threshold shifts; Dex, dexamethasone; IHC, inner hair cells; n.c., not communicated; n.s., not significant; OC, organ of Corti; OHC, outer hair cell; RWM, round window membrane; SGN, spiral ganglion neuron; SNHL, sensorineural hearing loss; SPL, sound pressure level; SV, stria vascularis; USMB, ultrasound microbubbles. Italics and underlines are used to distinguish the three different types of in vivo assessment: delivery, safety and efficacy assessement.
Among the first category, eight studies54–61 used hyaluronic acid-based hydrogels. Drug delivery assessment demonstrated prolonged retention and/or increased drug concentrations in the perilymph when using drug-loaded hydrogels compared with free drug alone (six studies).54–57,60,61 Safety assessment revealed no adverse effects or hearing sensitivity changes, except in one study 58 using neomycin, an ototoxic drug, which caused similar toxicity when administered alone. Of the five studies assessing treatment efficacy, four reported hearing improvement,54–56,59 with a significant protective effect in two,54,55 and one study 58 found no difference in hair cell count (Table 4).
Five studies62,64–66,113 investigated chitosan-based hydrogels. Prolonged residence time and/or higher perilymph drug concentration versus free drug were reported in four articles,62,64–66 with significant improvement in three.62,64,65 In one study, 66 peak concentration was higher with free drug, but overall exposure (area under the curve [AUC]) was greater with the chitosan hydrogel. No adverse effects were reported.64,113 Regarding efficacy, one study 65 reported significant vestibular impairment after gentamicin (ototoxic agent) delivery using chitosan hydrogel. One study 113 employed a polyplex-loaded glycol chitosan thermogel to deliver GFP-pDNA to inner ear hair cells, reporting significantly higher transcription efficiency compared with both pDNA alone and hexanoyl glycol chitosan thermogel (Table 4).
Ten studies28,63,67–74 explored poloxamer-based thermogels for enhancing residence time in the tympanic bulla. Four63,70–72 reported lower perilymph concentrations during the first hours postdelivery compared with free drug, although higher concentrations were observed after 24 h in two studies.71,72 Three studies63,71,72 reported prolonged residence time, yet only one 71 demonstrated a higher AUC. In contrast, five studies28,67,69,74,101 consistently reported higher concentration or fluorescence in the cochlea or perilymph when using poloxamer-based hydrogels at all measured timepoints. Regarding safety, temporary ABR threshold elevation was noted in two studies,69,71 and transient inflammation in one, 71 while two others reported no adverse reactions63,67 (Table 4).
Three studies75–77 tested silk-based hydrogels. Two reported prolonged dexamethasone detection in the perilymph, although with lower concentrations and absorption rates in the third. None demonstrated significant differences in drug delivery compared with free drug. One study reported temporary ABR threshold elevation 76 with no associated inflammatory responses, suggesting conductive hearing loss due to the surgical procedure and no inner ear damage; the other two did not report on this aspect (Table 4).
The last six studies78–83 investigated functionalized hydrogels, emulsions, vitrogels, or nanoparticle- or microsphere-loaded hydrogels. All reported increased perilymph concentrations, enhanced cochlear uptake, or improved therapeutic outcomes, including hearing improvement or hair cell preservation (Table 4).
All evaluated nanosystems increased cochlear drug uptake, perilymph concentrations, and/or therapeutic efficacy on induced hearing loss. These nanosystems included peptide-functionalized nanoparticles (7 studies),84–90 acide poly(lactique-coglycolique) (PLGA) and/or poly(ethylene glycol) (PEG) nanoparticles (5 studies),91,92,96,98,99 DNA nanostructures (2 studies),93,95 solid–lipid nanoparticles (1 study), 97 polymersomes (2 studies),100,104 P407 nanoparticles (1 study), 68 self-assembled conjugates (2 studies),36,114 or cubosomes (2 studies).102,103 Peptide-functionalized nanoparticles were particularly associated with therapeutic efficacy, as all studies reported ABR threshold improvement and hair cell preservation, with significant protective effects in six.84–88,90 PLGA/PEG-loaded nanoparticles significantly protected against cisplatin- and kanamycin-induced hearing loss in four studies.91,92,96,98 The fifth study 99 reported higher concentration, AUC, and bioavailability when delivering coumarin-6, Ginsenoside Rg1, and Rb1 with PLGA nanoparticles; however, lower concentration, AUC, and bioavailability when delivering salvianolic acid B and tanshinone IIA. Entrapment in tetrahedral DNA allowed enhanced epigallocatechin gallate (EGCG) delivery and improved hearing preservation against noise-induced hearing loss, although no statistical comparison with free EGCG was reported. Only one study 90 reported an adverse effect: increased RWM thickness after delivery of a fusion protein (XIAP-9R), with preserved ABR threshold and structure of the inner ear (Table 4).
Microsystem-based approaches included silk-coated or silk-based microparticles (3 studies),106,107,118 microgel particles (4 studies),33,94,105,115 and microcubosomes (1 study). 109 Microgel particles extended drug residence time in three studies33,94,115 and improved treatment efficacy in studies using GelMA microparticles.94,105,115 However, it did not induce hearing improvement or hair cell survival in one study using cross-linked hyaluronic acid and PLGA microcapsules, which also induced a higher rate of inflammatory reactions in treated animals. 33 For silk-coated or silk-based microparticles, two studies106,107 evaluated dexamethasone delivery without showing significant improvement over free drug, although encapsulated Dex exhibited longer residence time but lower AUC. No adverse effects were noted. One study 118 using silk fibroin polydopamine-composited microcarriers demonstrated significant hearing improvement and reduced synaptic damage compared with free NAC. Dex-loaded microcubosomes 109 improved distortion product otoacoustic emission (DPOAE) levels at all frequencies and increased overall recovery rates (Table 4).
Among the seven studies assessing permeabilizers, two evaluated histamine,110,111 two sodium caprate,23,112 two benzyl alcohol (BA),24,112 one collagenase, 25 and one buffered papaverine. 116 Histamine enhanced drug delivery in both studies,110,111 although 4% histamine induced significant inflammation of the middle ear. 110 Sodium caprate significantly increased drug concentration in one study but had no effect in the other. N-Méthyl-2-pyrrolidone, saponin, 4% BA, suction-induced drying, and high-osmolarity solutions significantly enhanced fluorescent dexamethasone delivery, while dimethylsulfoxide had no effect. Finally, while adeno-associated viruses (AAVs) did not cross the RWM without treatment, partial digestion of the RWM with collagenase (30 mg/mL) enabled AAV transfection into outer and inner hair cells. 25 However, higher concentrations (over 40 mg/mL) led to permanent ABR threshold elevation 4 weeks posttreatment (Table 4).
Biomechanical strategies
Biomechanical strategies were grouped into three main categories: sonoporation (9 studies),37–44 acoustic stimulation (4 studies),45–47,53 and magnetic systems (6 studies)34,48–52 (Table 4). These strategies relied on direct modulation through sonoporation, targeted transport using magnetic systems, or passive diffusion enhancement via acoustic stimulation.
In all studies, USMBs enhanced drug delivery by inducing cavitation and transient surface disruption of the RWM. Applications included dexamethasone,37,38 gentamicin, 40 IGF-138,41 gold nanoparticles, 42 fluorophore,35,43 and viral vectors. 44 RWM disruption resolved within 3–7 days. For viral vectors, transfection was achieved in inner hair cells with efficiency comparable to cochleostomy. No adverse effects or hearing impairment were observed (Table 4).
Acoustic stimulation significantly improved apical cochlear delivery and global perilymph concentrations. No significant impact on hearing was observed46,47 (Table 4).
Magnetic delivery, using external magnet to trigger passage of magnetite nanoparticles across the RWM, was investigated in six studies.34,48–52 While magnetic targeting did not enhance mesenchymal stem cell (MSC) delivery 34 and led to off-target organ distribution, it improved delivery of viral vectors, 49 prednisolone, 52 and dexamethasone 48 to the cochlea. However, safety assessments for magnetic strategies were lacking across the included studies (Table 4).
Semiquantitative ranking of enhancement strategies
A semiquantitative ranking of the different enhancement strategies was performed based on a score assessing delivery evidence, reproducibility across models, safety of the methods, functionality or therapeutic efficacy, and risk of bias (Fig. 1, Table 5). In general, the level of delivery evidence is high (score of 3–4) except for microsystems. Nanosystems, microsystems, permeabilizers, sonoporation, and magnetic systems had a moderate-to-high level of evidence for functional and therapeutic efficacy; however, only sonoporation and nanosystems were associated with consistent evidence of cochlear safety, supported by functional and histological outcomes. For each strategy, risk of bias and reproducibility across models were insufficient and limit cross-study analysis. Hyaluronic acid-based hydrogels, sonoporation, and nanosystems had the strongest global scores, illustrating that these strategies are closest to human applicability.
Semiquantitative Ranking of RWM Permeability Enhancement Strategies
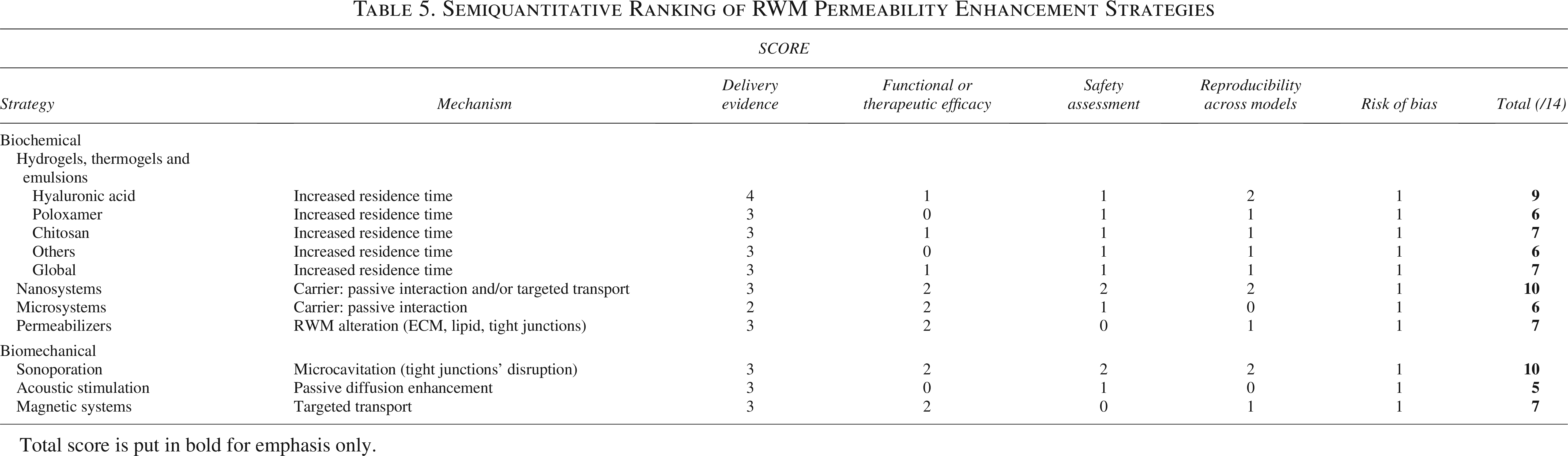
Total score is put in bold for emphasis only.
Gene therapy delivery
The number of studies demonstrating successful gene transfer following RWM permeabilization is limited. Among the studies included in this review, only five assessed gene therapy delivery using hyaluronic acid-based hydrogel, 61 chitosan-based hydrogel, 113 collagenase, 25 sonoporation, 44 or magnetic targeting, 49 demonstrating the exploratory nature of this field (Table 6). All studies reported passage of viral or nonviral vectors across the RWM; however, only one study reported efficient gene expression and functionality of gene therapy by assessing treatment efficacy on induced SNHL. What is more, all studies reported outcomes on the short-term, which do not necessarily translate into durable gene expression.
Enhancement Strategies for Gene Therapy Delivery to the Inner Ear
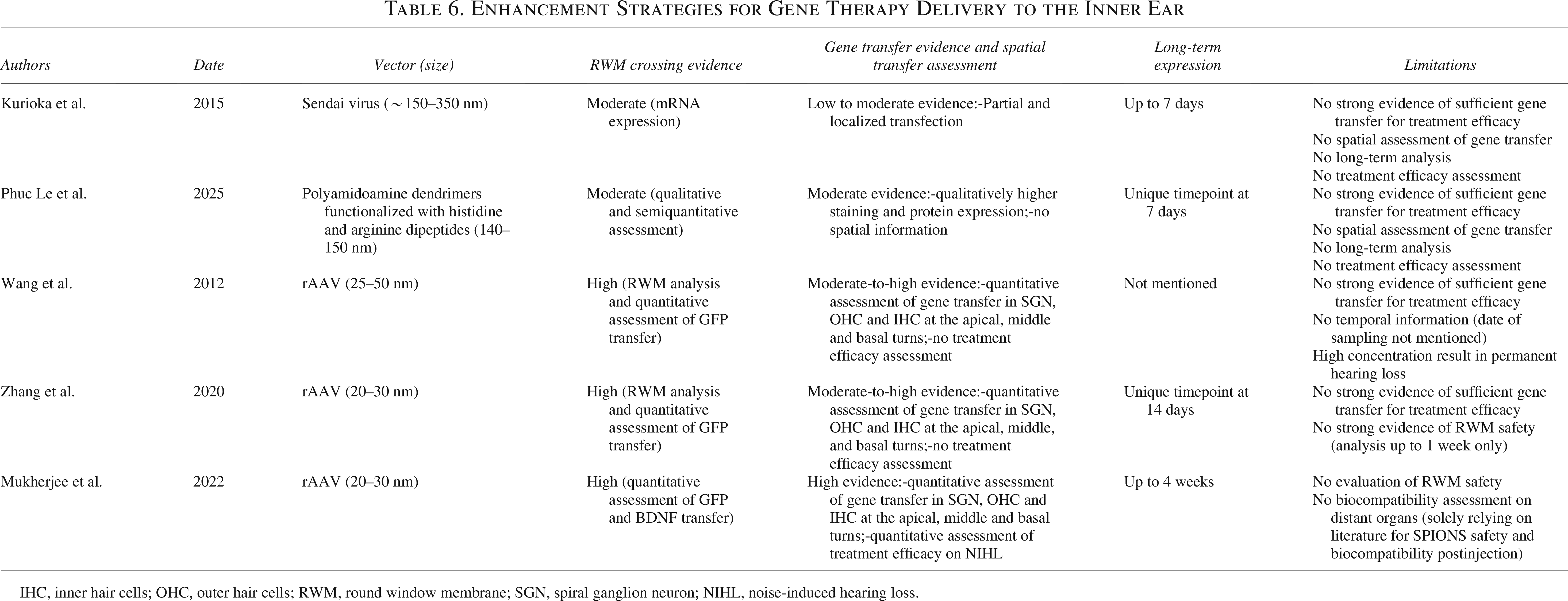
IHC, inner hair cells; OHC, outer hair cells; RWM, round window membrane; SGN, spiral ganglion neuron; NIHL, noise-induced hearing loss.
All extracted results are detailed in the supplementary material (Supplementary Table S2).
Discussion
This systematic review aimed to identify and evaluate biomechanical and biochemical strategies developed to enhance drug delivery through the RWM, focusing on their potential to improve diffusion into the cochlea and treatment efficacy for inner ear disorders. Seven categories of enhancement strategies were identified during the review and are represented in Figure 8, respectively: (1) hydrogels, thermogels, and emulsions, (2) nanosystems, (3) microsystems, and (4) permeabilizers, alongside (1′) sonoporation, (2′) acoustic stimulation, and (3′) magnetic targeting. Not all strategies included in this review directly modify the intrinsic properties of the RWM. Indeed, true permeability modulation refers to approaches that alter the RWM structure itself, such as disruption of the tight junctions (sonoporation), extracellular matrix modification, or lipid bilayer alteration (permeabilizers), while pharmacokinetic strategies (hydrogels, thermogels, and emulsions) increase residence time or rely on transport mechanisms through diffusion enhancement, carrier–membrane interactions, endocytosis, or direct transport mechanism (nanosystems, microsystems, magnetic targeting, and acoustic stimulation). This distinction is critical as different mechanisms are required depending on the characteristics of the delivered drug, and multiple strategies may be combined to enhance delivery. Most studies reported increased intracochlear drug detection, extended middle ear residence time, longer detection periods, or improved treatment outcomes, with only a few negative or neutral results involving poloxamer-based,70–72 hyaluronic acid-based, 56 chitosan-based hydrogels, 66 silk-coated microcrystals, 106 buffered papaverine, 116 and magnetic targeting of MSCs 34 (Fig. 9). Sonoporation and nanosystems demonstrated the most consistent evidence of enhanced cochlear delivery across multiple models. Both strategies provided quantitative delivery data and associated functional improvement. However, this moderate-to-high level of evidence is associated with limited long-term safety data. Microsystems and magnetic targeting showed moderate evidence of benefit, supported by fewer studies and limited reproducibility across models. Finally, increasing the residence time through hydrogels, thermogels, or emulsions provided little evidence of membrane permeability modulation. Indeed, their primary effect appears to be pharmacokinetic, and they should be interpreted as facilitators rather than permeabilization techniques, especially for large, hydrophilic, negatively charged molecules.
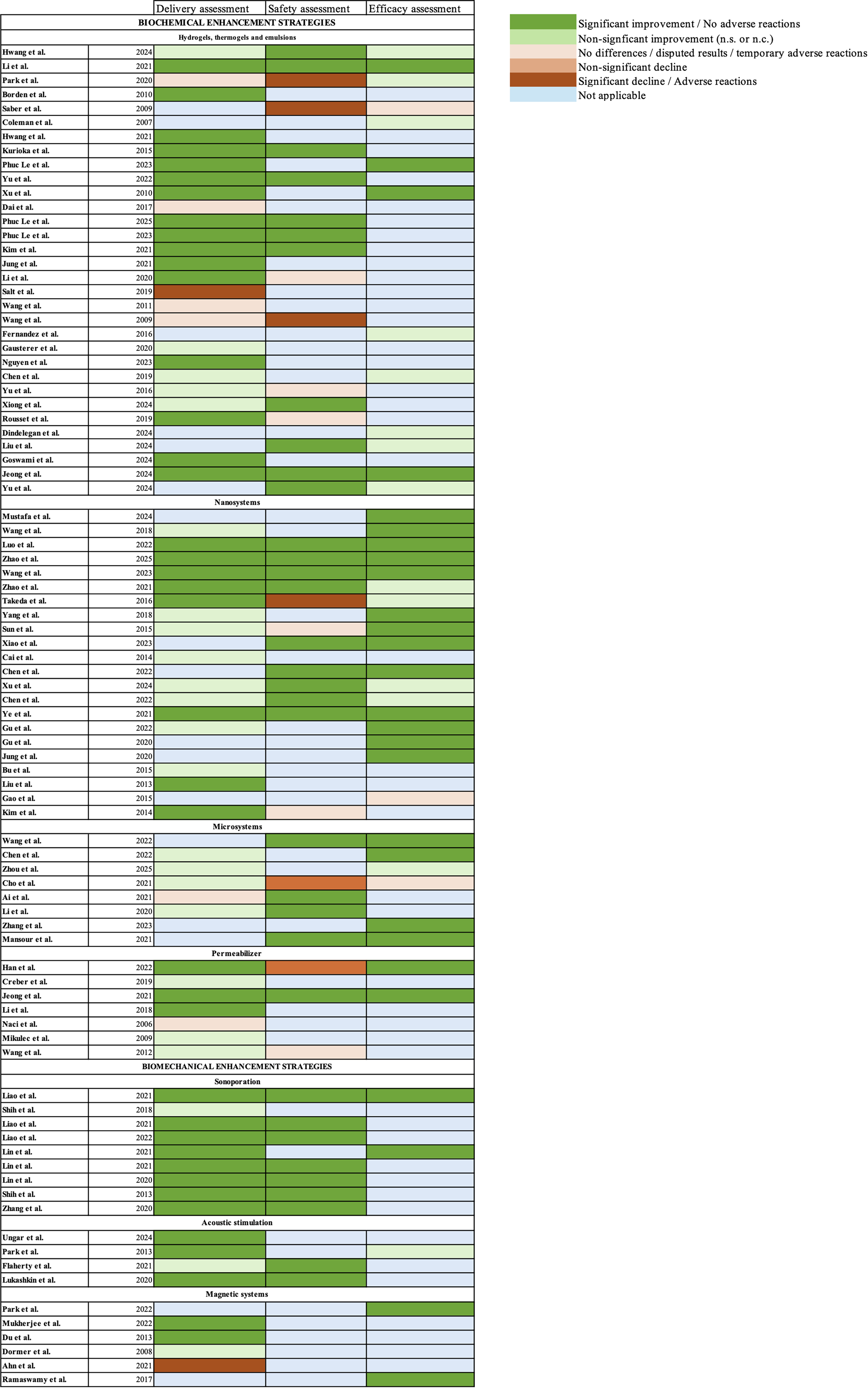
Visualization of the study outcomes.
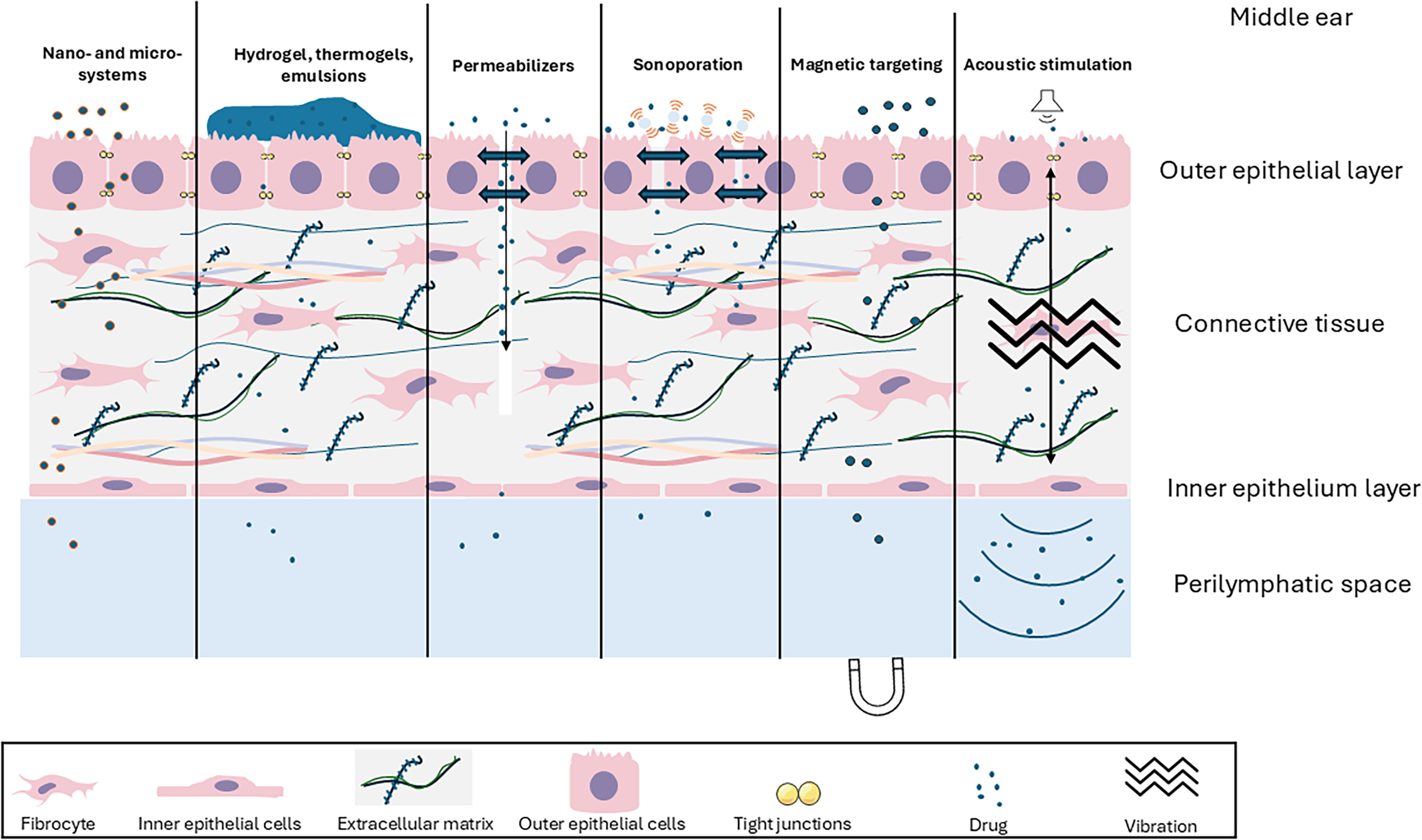
Schematic representation of included RWM permeability enhancement strategies. RWM, round window membrane.
Globally, reproducibility across species, disease models, and therapeutic agents remains insufficient for most strategies, as they were not validated in more than one experimental context. What is more, heterogeneity in selected outcomes represents a major source of variability and limits cross-study analysis. Direct quantification of perilymphatic drug concentration using LC–MS techniques constitutes robust evidence of intracochlear delivery, if performed without sampling bias or contamination risk, but provides no or limited spatial information. Immunohistochemical or spatial mapping provides spatial information but should be quantitatively assessed. Delivery assessment should be combined with functional assessments such as ABR and DPOAE to evaluate safety and therapeutic efficacy and to provide both direct evidence of RWM crossing and treatment efficacy. A key implication of this review is that standardization of primary endpoints, combining quantitative delivery measurements with functional and safety validation, would significantly increase translational relevance. Guinea pigs, the most used animal model in the included articles, offer distinct advantages due to their hearing frequency range overlap with humans, similar cochlear structure, and a larger, thicker RWM compared with mice and rats. 119 Perilymph sampling and RWM histological analysis are also easier in these animals due to their size. Mice remain a gold standard for genetic hearing loss due to available transgenic models and ease of genetic manipulation.120–122 However, differences in therapeutic efficacy between preclinical and clinical studies may originate from the overestimation of drug diffusion through the RWM in rodents and emphasize the need for intermediate animal models, anatomically closer to humans, or for in vitro or ex vivo three-dimensional models of the human RWM. Another methodological limitation is that most included studies presented unclear or moderate risk of bias, mainly due to insufficient reporting of randomization, allocation concealment, blinding, and sample size calculation, restricting confidence in these preclinical studies. Future studies should clearly adhere to standardized reporting of bias to strengthen the validity of conclusions.
Over the past two decades, a clear chronological shift in strategies to enhance RWM permeability has emerged. Early research focused primarily on hydrogels and permeabilizers to improve local delivery of dexamethasone, a corticosteroid widely used to treat inner ear inflammation, Ménière’s disease, and sudden SNHL. Hydrogel-based systems remain the most clinically applicable in terms of safety, biocompatibility, and ability to prolong drug residence time in the tympanic cavity. Numerous studies included in this review confirm that such systems significantly increase perilymph concentrations over time and reduce ABR thresholds compared with dexamethasone alone, supporting their therapeutic potential. However, clinical outcomes remain inconsistent: a systematic review and meta-analysis of intratympanic dexamethasone for sudden SNHL found insufficient evidence to recommend this approach over systemic administration. 123 When combined with hyaluronic acid hydrogels, intratympanic dexamethasone yielded variable outcomes, ranging from hearing improvement in low-frequency idiopathic sudden SNHL 124 to improvement in vertigo without hearing gain in patients with Ménière’s disease 125 or selective frequency improvement in sudden SNHL. 126 These observations do not only reflect on delivery limitations but also on the variability in drug effectiveness across pathological contexts.
Whether in animal models or humans, the hydrogel-based strategies remain largely restricted to small molecules such as antioxidants, corticosteroids, or growth factors. Meanwhile, gene therapy is rapidly advancing, with several vectors entering clinical trials.30,127 These new treatments introduce additional complexity beyond small-molecule diffusion, as it requires active transport mechanisms. Current delivery techniques, used in preclinical studies and clinical trials, are invasive, involving surgical perforation of the RWM, OWM, or semicircular canals and associated with risks of fibrosis and permanent hearing loss. In this review, only five investigations studied gene therapy delivery through the RWM, with limited quantitative transgene expression, and long-term expression beyond four weeks was not documented. Current evidence suggests that RWM-mediated gene delivery is feasible but remains insufficiently validated for translational progression. No matter the delivered drug, long-term safety remains one of the most critical issues, as most studies assessed hearing thresholds and histology within 1–4 weeks. Chronic RWM alterations, fibrosis, persistent inflammation, or delayed hearing deterioration were not investigated. This limitation represents a major translational barrier, as inner ear disorders are often chronic and require repeated administration. Based on this systematic review, a translational roadmap is suggested in Figure 10, and it is advised that no strategy should advance toward clinical translation without fulfilling all five domains.
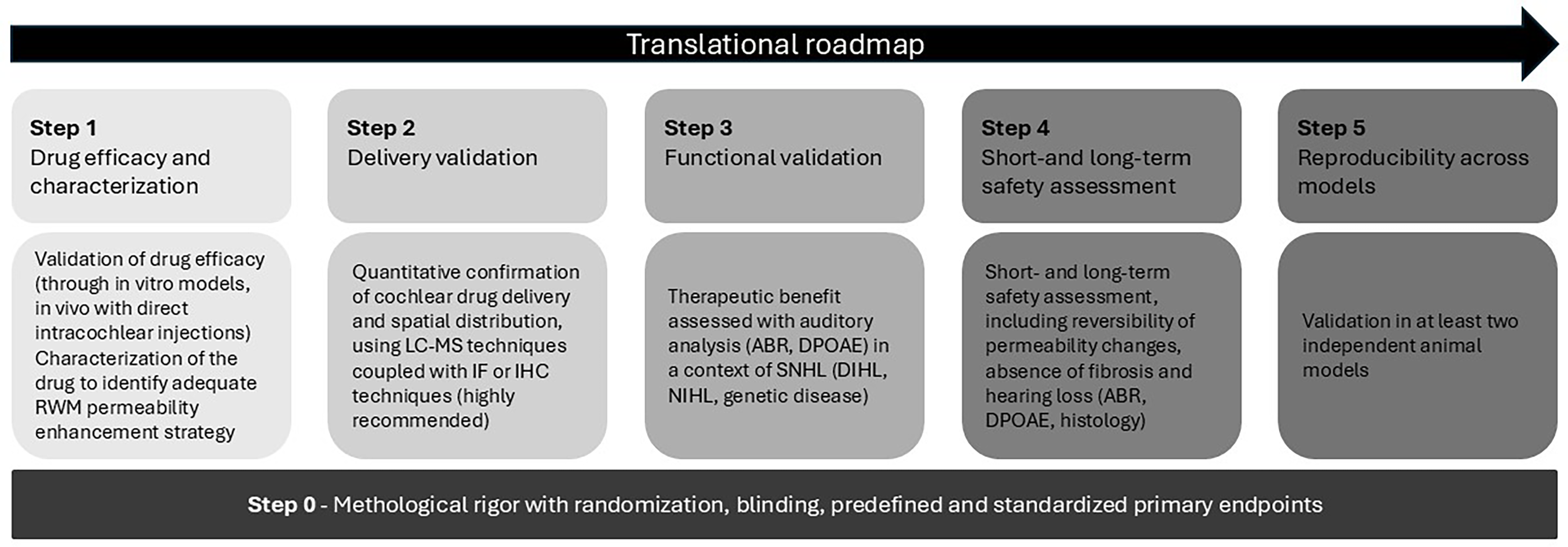
Translational roadmap toward clinical application.
Even though surgical approaches were not considered enhancement strategies in this review due to the focus on RWM permeability, they remain critical for effective drug delivery to the inner ear. Techniques such as a microendoscopy, 128 microcatheters, 129 micropumps, 130 round window niche drilling, 131 or other microdevices132,133 can optimize drug application to the RWM, improve delivery consistency, and address potential anatomical obstructions. Emerging in situ bioprinting techniques, which enable direct printing of biological materials in vivo using extrusion, jetting, or laser-assisted methods, are also promising. A recent proof-of-concept study demonstrated the potential of laser-assisted bioprinting for inner ear drug delivery, combining laser deposition with a poloxamer-based hydrogel to deliver dexamethasone directly into the perilymph. 134 Similarly, combining nanocarriers with mechanical enhancement methods such as ultrasound or magnetic targeting could facilitate controlled, targeted drug application, improving both spatial precision and therapeutic outcomes, particularly valuable for large macromolecules such as viral vectors, CRISPR-Cas systems, or monoclonal antibodies. A promising direction for future research lies in the combination of multiple enhancement strategies and standardization of preclinical protocols.
Conclusion
Despite the effectiveness of current drug formulations in animal models, translation to human application remains a major challenge. Local delivery onto the RWM represents a promising and minimally invasive approach for targeting the inner ear. In this review, a summary of biomechanical and biochemical strategies to enhance the RWM permeability in vivo is presented, along with efficacy and safety assessments. However, the human RWM is thicker and structurally more complex than that of rodents, limiting extrapolation of permeability results. 135 In this context, the development of minimally invasive, reproducible, and clinically adaptable delivery methods is crucial. The review emphasizes that while many drug delivery strategies are already available for various pharmacologically effective treatments, their clinical success and reliability rely on optimized delivery protocols to ensure safety, reproducibility, and sufficient drug concentrations reach the human cochlea. Further research is essential to facilitate the clinical translation of both existing and emerging delivery methods. Importantly, for all strategies, long-term side effects such as fibrosis or progressive hearing loss remain poorly described and should be further investigated to ensure safety for clinical translation.
Authors’ Contributions
A.B.: Conceptualization, investigation, data curation, writing—original draft, writing—review and editing, and visualization. P.R.: Data curation, writing—review and editing, and visualization. Y.B.: Writing—review and editing. D.B.: Supervision and writing—review and editing. R.D.: Supervision, writing—review and editing, and funding acquisition. L.G.: Supervision and funding acquisition. O.K.: Conceptualization, supervision, writing—review and editing, and visualization.
Footnotes
Acknowledgments
The authors would like to thank Hélène Plouseau-Guédé from the Life and Health Sciences Library at the University of Bordeaux for her help in defining the search strategy.
Author Disclosure Statement
The authors declare no conflict of interest. No AI-assisted writing or text-generation tools were used.
Funding Information
This systematic review is part of Agathe Bedoux’s doctoral thesis project. This PhD program was made possible through the CIFRE dispositive, carried by the ANRT (Association Nationale Recherche Technologie) and through ALPhANOV (Optics and Laser technological center). The project is also supported by funding from SPARK (Université de Bordeaux).
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.