
Abstract
Bone regeneration presents a significant clinical challenge due to the complex interplay between biological processes and the local mechanical environment. While polymeric scaffolds are widely utilized for their tunable physicochemical properties, traditional designs often fail to replicate the dynamic mechanical cues required for optimal tissue remodeling. This review critically examines the mechanobiological design of bioinspired polymeric scaffolds. We first categorize native bone mechanics and the role of mechanical stimuli—such as stiffness, fluid shear, and stability—in regulating the fracture healing cascade. We then bridge these biological principles with advanced fabrication strategies, analyzing how natural, synthetic, and composite polymers can be engineered to mimic the hierarchical stiffness and bioactivity of native bone. Furthermore, we discuss the role of computational modeling (e.g., Finite Element Analysis) in predicting scaffold performance and highlight emerging technologies, including 4D printing and piezoelectric scaffolds, which offer time-dependent and mechano-electrical adaptability. Finally, we address current barriers to clinical translation and propose future directions for mechanically adaptive systems that actively guide regeneration.
Impact Statement
Current polymeric scaffolds for bone tissue engineering frequently fail to replicate the dynamic mechanical microenvironment required for optimal tissue remodeling. This critical review bridges the gap between foundational fracture healing mechanics and advanced biomaterial design by proposing a “mechanobiological triad”—encompassing fixation mechanics, scaffold architecture, and host biological factors—as a governing framework for clinical success. We systematically evaluate how emerging technologies, including 4D printing, piezoelectric materials, and machine-learning-driven design, can create mechanically adaptive systems that actively guide cellular differentiation rather than serving as passive void fillers. This article serves as a translational roadmap for designing the next generation of bioinspired scaffolds that synchronize mechanical stiffness and bioactivity with the temporal stages of bone repair.
Keywords
Introduction
Bone regeneration has evolved into a critical discipline aimed at addressing complex skeletal defects resulting from high-energy trauma, congenital anomalies, and oncologic resections. Current clinical strategies for osseous restoration typically rely on the procurement and transplantation of autologous bone, either as nonvascularized grafts or vascularized flaps. While autologous bone remains the “gold standard” due to its superior osteogenic integration, its application is severely restricted by limited graft availability, donor site morbidity, and significant associated patient discomfort.
To overcome these limitations, tissue engineering has focused on developing biomaterial scaffolds that can mimic the extracellular matrix (ECM). Ideally, these scaffolds must satisfy a rigorous set of criteria: biocompatibility, bioresorbability, appropriate porosity for vascularization, and specific mechanical qualities that facilitate handling and manufacturing. 1 However, existing biomaterials often require a trade-off between these competing requirements. A fundamental challenge lies in the heterogeneity of native tissue; bone adaptation and resorption rates vary significantly across species, ages, and even specific anatomical regions within the same individual. 2 Despite this biological variability, current surgical approaches frequently utilize a single type of material for a wide spectrum of bone deficiency scenarios, ignoring the site-specific mechanical microenvironment.3,4 In addition to biological and mechanical performance, successful clinical adoption also depends on economic feasibility, including raw material availability, fabrication complexity, sterilization compatibility, shelf stability, and the need for adjunctive components such as exogenous cells, growth factors, or patient-specific manufacturing.5,6
We conceptualize a mechanobiological triad that governs bone repair: (i) fixation mechanics (including fixation stiffness and interfragmentary motion), (ii) scaffold properties (architecture, stiffness, and bioactivity), and (iii) host factors (bone quality, vascularity, and biological milieu). The interaction among these three elements determines whether healing proceeds toward functional regeneration or nonunion. The mechanical environment is a crucial determinant of clinical efficacy. Consequently, we advocate for a biomimetic design strategy that leverages endogenous secondary fracture healing mechanisms to guide the structural architecture of scaffolds. This framework is summarized schematically in Figure 1.
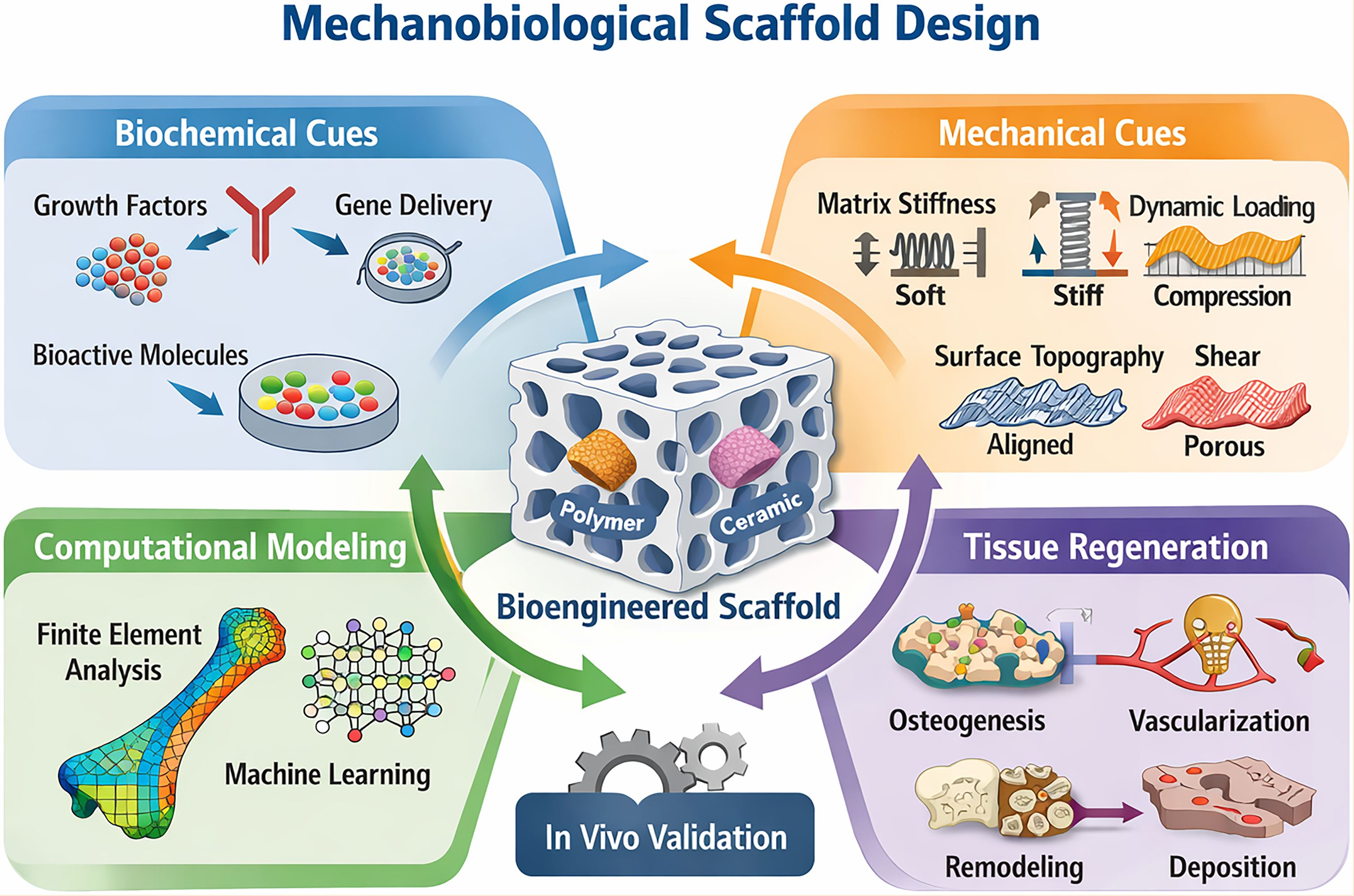
Mechanobiological design framework for bone scaffold development. Scaffold-guided bone regeneration is determined by the interaction among three core determinants: fixation mechanics, scaffold properties, and host biological factors. These inputs collectively shape the local strain environment, vascularization potential, and tissue differentiation outcome. Computational modeling and data-driven optimization serve as integrative design tools to refine scaffold architecture and improve translation predictability.
In this review, we critically examine recent advances in the mechanobiological design of bioinspired polymeric scaffolds for bone regeneration. We focus on how mechanical cues—arising from the defect site, scaffold architecture, and external loading—can be integrated into material design to improve predictability and translational relevance. We also consider the suitability of different animal models for evaluating scaffold mechanics in vivo. Our central premise is that effective scaffolds must not only occupy space but actively support appropriate mechanical conditions to guide cellular differentiation, vascularization, and tissue remodeling.
The Mechanobiology of Bone Repair
Bone repair is a multifaceted biological process that orchestrates the interaction of inflammatory cells, stem cells, and angiogenic factors within a dynamic physical environment. Although biochemical signaling initiates the healing cascade, the mechanical environment—defined by stability, strain, and interstitial fluid flow—plays a decisive role in determining whether repair progresses toward functional regeneration or nonunion. 7 The healing continuum is traditionally categorized into hematoma formation, granulation tissue production, callus formation, and bone remodeling, with each phase exhibiting distinct sensitivities to mechanical stimuli. 8 The sequential and mechanically regulated stages of repair are illustrated in Figure 2.
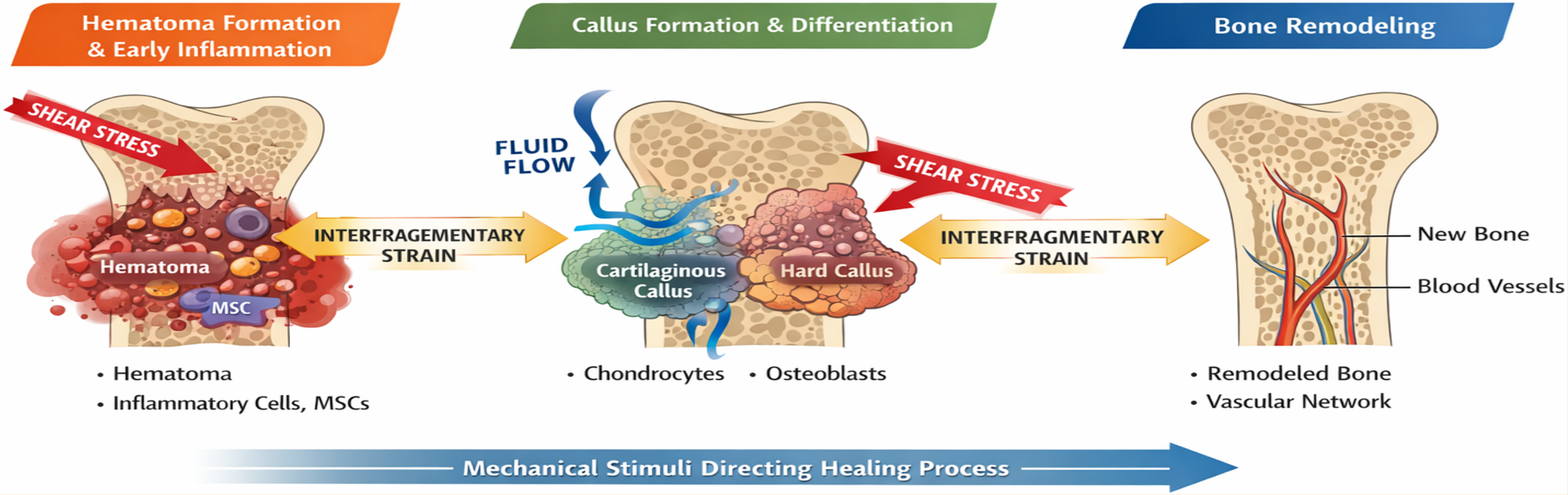
Schematic illustration of the effects of mechanical stimuli on the sequential stages of bone repair. Following fracture, healing begins with hematoma formation and early inflammation, during which inflammatory cells and MSCs are recruited into a fibrin-rich provisional matrix. At this stage, interfragmentary strain and shear stress influence early matrix organization and vascular development. As repair progresses, the soft callus transitions toward cartilaginous and hard callus tissues, with strain magnitude and interstitial fluid flow serving as key regulators of lineage commitment and tissue differentiation. In the final remodeling phase, restored vascularization and mechanical loading promote replacement of provisional repair tissue with mature bone. This schematic highlights the principle that fracture healing is not only biologically regulated but also strongly shaped by the magnitude and timing of local mechanical stimuli. MSCs, mesenchymal stem cells.
Hematoma and early inflammatory response
The bone repair process initiates immediately following fracture, where the disruption of blood vessels results in hematoma formation. 9 This fibrin-rich clot acts as a temporary scaffold, recruiting hematopoietic and mesenchymal stem cells (MSCs) via local and systemic circulation. 10 In addition to initiating inflammation and releasing proinflammatory mediators, this phase represents the earliest stage of mechanical sensing. 11 Mechanical instability, specifically interfragmentary shear or compression, directly affects early ECM formation. For instance, a recent study by Mehl revealed that externally applied shear across a fracture gap delayed hematoma remodeling and altered the morphology of early collagen fiber orientations and microvascular networks, independent of the YAP/TAZ signaling pathway. 12 These findings indicate that mechanical boundary conditions are detected at the very outset of healing and can bias subsequent tissue organization before callus formation.
Callus formation and strain-dependent differentiation
As the hematoma evolves into granulation tissue, progenitor cells differentiate into osteogenic lineages, 13 a process modulated by soluble factors like bone morphogenetic proteins (BMPs), stromal cell-derived factor-1 (SDF-1), 14 and hypoxia-inducible factor-1α (HIF-1α). 15 Importantly, the mechanical history of the defect site strongly influences this differentiation. Mehta et al. demonstrated that interfragmentary strain patterns present during the early soft callus phase (less than 2 weeks) accurately predicted the geometry and patterning of the callus at later stages. 16
The transition from soft cartilaginous callus to hard bony callus is governed by specific mechanical thresholds, as described by foundational mechanobiological theories.
Pauwels’ hypothesis
Suggested that distortional shear stress stimulates collagen fiber formation, while compressive stress induces cartilage formation. 17
Perren’s interfragmentary strain theory
Proposed that healing tissues can only develop within specific tolerance thresholds of strain; for example, bone cannot form in high-strain environments where only fibrous tissue can survive. 18
Prendergast’s mechano-regulatory pathway
Refined these concepts by hypothesizing that differentiation is driven by two stimuli: strain and relative fluid/solid velocity. Under this model, high strain and velocity drive fibrous tissue formation, moderate levels favor cartilage, and low levels favor bone. 19
From a design perspective, these frameworks imply that scaffolds should not simply be stiff or compliant, but should modulate local strain and fluid flow within biologically permissive ranges.
Clinically, these thresholds dictate the mode of healing. Primary bone healing occurs under rigid stability where local interfragmentary strain is typically <2%, whereas secondary (callus-mediated) bone healing occurs under relative stability with strains approximately 2–10%. Strains exceeding ∼10% generally favor fibrous tissue formation and increase the risk of delayed union or nonunion. 20 Conversely, strains exceeding 10% typically result in nonunion or delayed union due to the rupture of bridging tissues. 20
Cellular mechanotransduction and vascular adaptation
At the cellular level, mechanical signals are transduced into biological responses that drive tissue remodeling. 21 MSCs exhibit extreme sensitivity to tissue-level elasticity, specifying lineage commitment based on substrate stiffness. 22 Research by Mao verified that substrate stiffness regulates osteogenesis in MSCs, 23 while Winer et al. showed that MSCs on soft substrates exhibit decreased proliferative activity compared to those on stiffer surfaces. 24 These findings underscore the importance of scaffold substrate stiffness as a primary determinant of MSC fate, providing a direct rationale for tuning polymeric scaffold elasticity in bone tissue engineering.
Crucially, vascularization—a prerequisite for osteogenesis—is also mechanically regulated. Vascular networks are highly sensitive to mechanical conditions.25,26 For example, skeletal fatigue loading has been shown to induce a rapid increase in periosteal vascularity. 27 Recent mechanistic studies reveal that mechanical forces trigger the mechanoreceptor PIEZO1, which modulates the transformation of Type H vessels into Type L vessels to coordinate bone growth with mineralization. 28 Conversely, the stiffness of the scaffold or ECM regulates microvascular stability; stiff ECM enhances endothelial cell integrin phosphorylation and Connective Tissue Growth Factor production, thereby promoting the differentiation of pericytes into myofibroblasts. 29 Furthermore, the timing of mechanical stability is critical: in a large bone defect model, early mechanical loading was found to inhibit vascular invasion, whereas late mechanical loading (after 4 weeks of stiff fixation) significantly stimulated vascular remodeling. 26 Together, these observations suggest that scaffold mechanics must be tuned not only in magnitude but also in timing to support both angiogenesis and osteogenesis.
Computational Modeling and Characterization of the Mechanical Environment
To bridge the gap between in vitro findings and clinical outcomes, computational modeling has become indispensable. Beyond static calculations of stress and strain, contemporary mechanobiological models attempt to incorporate biological feedback—such as tissue growth, matrix deposition or degradation, and transport of nutrients and signaling molecules—under mechanical loading. 30 These models are increasingly used to interpret experimental data and to inform scaffold design, although their predictive accuracy remains context-dependent. 31
Finite element analysis and microstructural characterization
In the context of bone tissue engineering, finite element analysis (FEA) has evolved into an indispensable tool for estimating bone mechanics and predicting scaffold performance. Increasingly, FEA is applied beyond whole-bone models to micro-FE (µFE) simulations of scaffolds within defect sites, enabling the precise prediction of local strain and fluid flow at the scaffold–host interface. 32 By linking imaging-derived microstructures to apparent mechanical competence, these models provide a robust quantitative framework for evaluating novel biomaterials and architectures. 33
Currently, high-resolution µFE, derived from microcomputed tomography (µCT), serves as the in vitro and ex vivo reference standard for correlating trabecular architecture with stiffness and failure modes. 34 However, the intrinsic porosity and heterogeneity of trabecular bone make these models highly sensitive to boundary conditions and material assignments, which can skew mechanical estimations. 35 Translating these microstructural insights to the clinic relies heavily on High-Resolution Peripheral Quantitative CT (HR-pQCT). In vivo, HR-pQCT successfully quantifies site-specific mechanical competence at peripheral sites (e.g., radius or tibia), directly linking microarchitectural metrics to clinical outcomes like fragility fractures. 36 Yet, its inability to fully capture the mechanics of larger, load-bearing bones remains a significant clinical bottleneck.
To overcome the limitations of conventional morphometry 37 and reduce the computational burden of high-resolution models, voxel-based continuum approaches have gained traction. These methods can predict trabecular bone modulus directly from clinical CT images without the need for explicit segmentation. 38 Furthermore, as demonstrated by Oefner et al., µCT-derived morphology can effectively estimate anisotropic elastic properties in osteoporotic bone, offering critical biomechanical insights for interventions such as spinal instrumentation. 39 While these continuum approaches successfully reduce preprocessing complexity, a fundamental challenge remains: their predictive accuracy is still heavily constrained by available imaging resolution and underlying assumptions of tissue homogeneity.
Computational efficiency, platform accessibility, and homogenization strategies
Despite the predictive power of high-resolution FEA, its widespread utility is frequently bottlenecked by the immense computational overhead required to model large, highly porous scaffold-host architectures. Currently, commercial simulation platforms such as Abaqus (Dassault Systèmes) and ANSYS remain the industry standards for high-fidelity bone biomechanics. 32 While these platforms provide robust, user-friendly multiscale modeling environments, their prohibitive licensing fees present a significant barrier to routine clinical integration. 40 Consequently, open-source solvers like FEBio have emerged as vital alternatives. FEBio offers powerful biphasic and multiphasic modeling capabilities at no software cost, 41 though its effective implementation often demands a steeper learning curve and advanced computational expertise. 42
Beyond software accessibility, the feasibility of FEA is heavily dictated by hardware constraints, forcing researchers to navigate the trade-off between model fidelity and computational efficiency. Voxel-based continuum FEA, derived directly from high-resolution micro-CT, provides unparalleled anatomical accuracy but requires massive memory allocation. Processing these patient-specific models typically exceeds the capacity of standard desktop environments, necessitating reliance on high-performance computing clusters or cloud infrastructure to solve the millions of degrees of freedom generated by the highly complex porous network. 43 To circumvent these hardware limitations, the field is increasingly exploring homogenized or reduced-order hybrid FE strategies. Techniques such as the Firm and Floppy Boundary Lattice Element Method offer simplified approximations that can be efficiently solved on standard computational hardware. 44 While homogenization sacrifices localized microstructural detail, it provides a highly pragmatic solution for rapid, large-scale biomechanical screening.
Emerging frontiers: Multiscale modeling and machine learning
Recent modeling efforts extend beyond linear elastic stiffness to capture aspects of bone remodeling. Multiscale frameworks increasingly couple organ-level loading (e.g., musculoskeletal simulations) with tissue-level adaptation algorithms, enabling more patient-specific analyses of how geometry or scaffold architecture may influence bone formation under physiological loads. 45
Furthermore, to better capture crack initiation and age-related changes in toughness, newer computational formulations, such as phase-field approaches, are being employed. 46 Machine learning (ML) is increasingly used to complement FEA. ML surrogates trained on FE outputs can approximate biomechanical quantities (e.g., stresses or failure risk) with substantially reduced computation time, facilitating rapid screening of design spaces. However, their performance depends strongly on the quality, representativeness, and size of the training datasets, and they currently lack the mechanistic transparency of physics-based models. 47
Overall, computational tools are most effective when used in combination with experimental validation, rather than as stand-alone predictors of biological or clinical performance. These trade-offs in spatial resolution, computational burden, and clinical applicability are summarized in Table 1.
Comparison of Major Computational Modeling Modalities in Bone Tissue Engineering
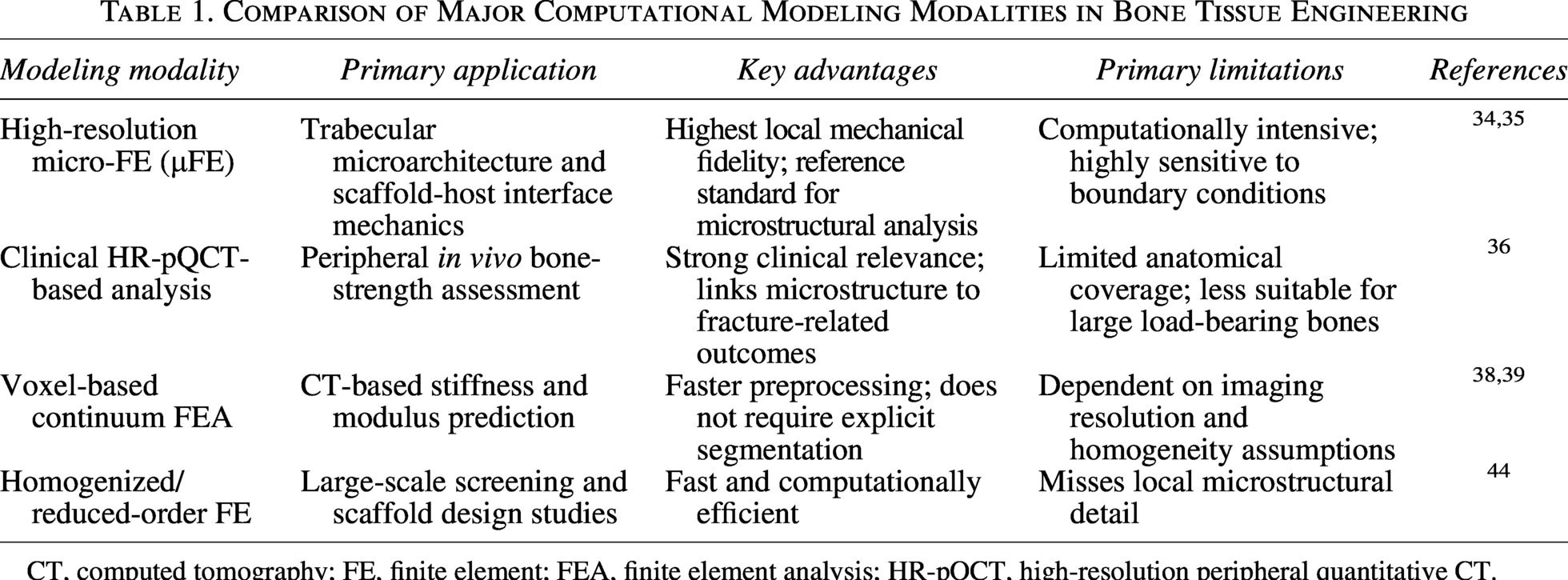
CT, computed tomography; FE, finite element; FEA, finite element analysis; HR-pQCT, high-resolution peripheral quantitative CT.
Material Platforms for Mechanobiological Control
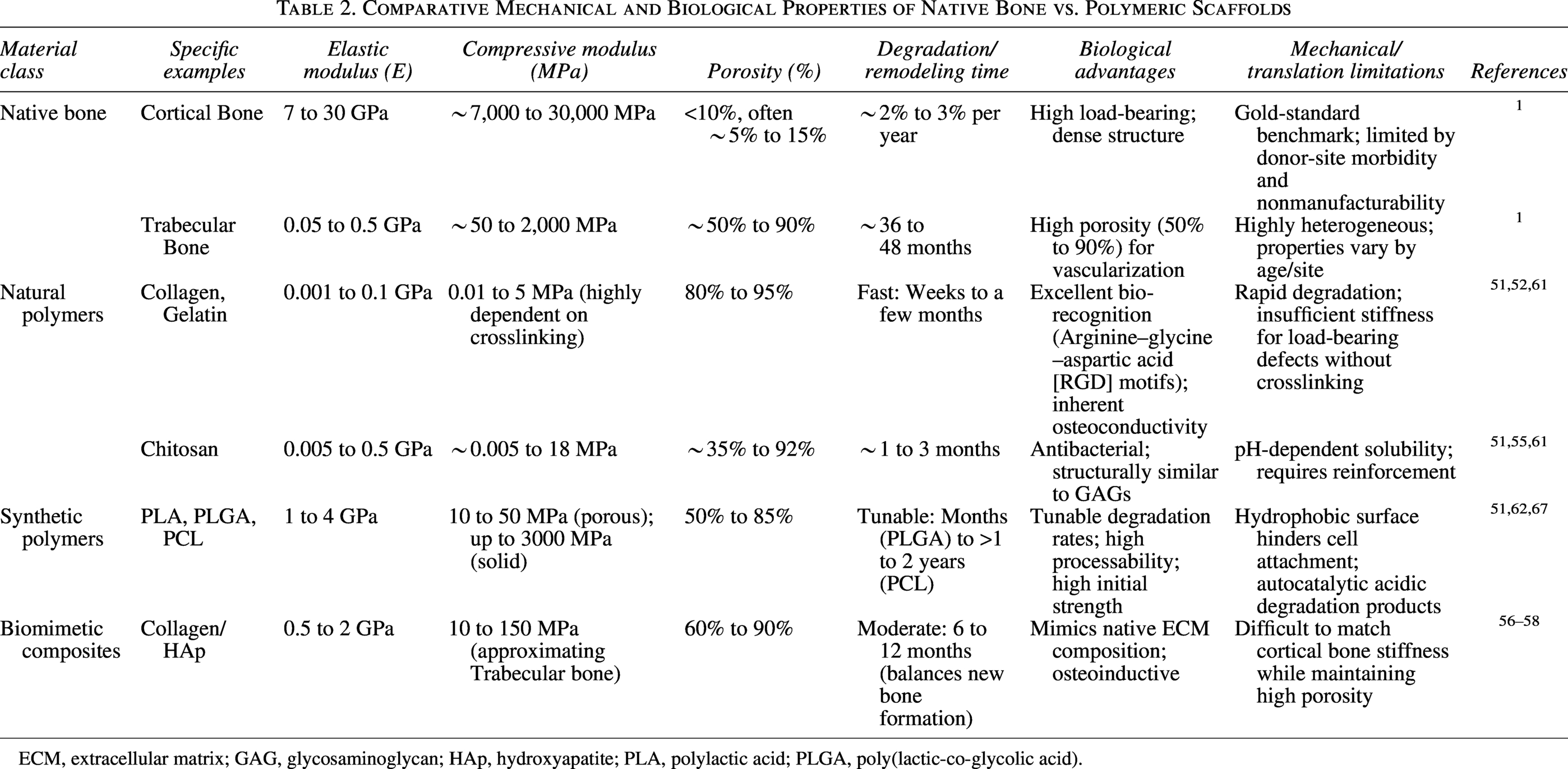
Designing bioinspired polymeric and composite scaffolds for bone regeneration requires a balance between mechanical competence and biological recognition. Depending on their essential components, polymeric scaffolds are categorized into natural, synthetic, and composite systems. Each class offers distinct advantages and limitations in reproducing the mechanical and biochemical features of native bone. 48 In addition to biological activity, quantitative comparison of scaffold platforms requires consideration of fabrication route and production scalability, because these directly influence pore reproducibility, mineral distribution, crosslinking uniformity, sterilization compatibility, storage stability, and batch-to-batch consistency. Accordingly, Table 2 summarizes representative mechanical ranges together with degradation behavior and key translational limitations for major material classes.
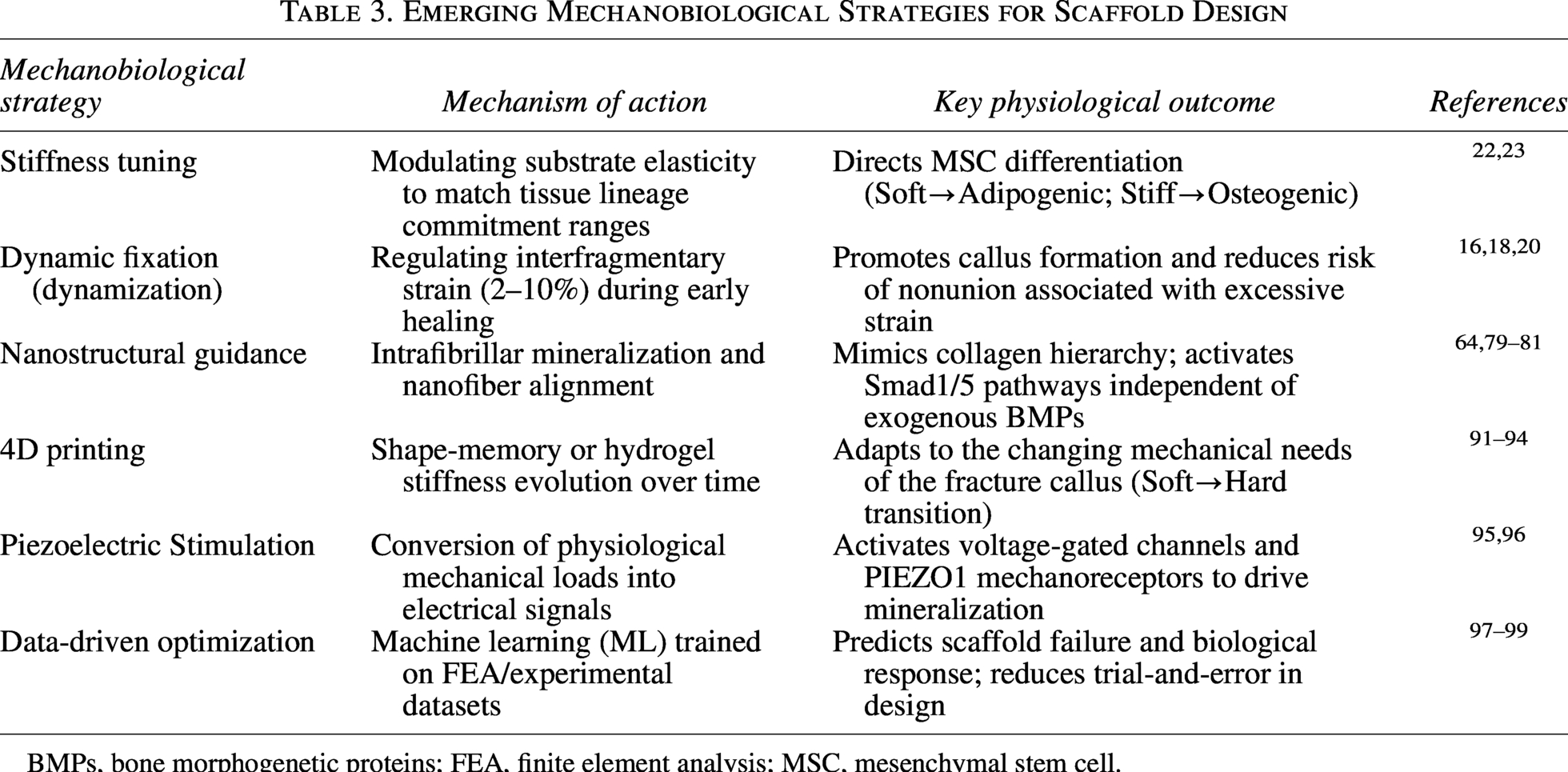
Emerging Mechanobiological Strategies for Scaffold Design
BMPs, bone morphogenetic proteins; FEA, finite element analysis; MSC, mesenchymal stem cell.
Beyond mechanobiological performance, material selection is also shaped by economic and translational constraints. 49 These include the cost and consistency of source materials, processing complexity, scalability of fabrication, compatibility with sterilization and storage, and whether the scaffold requires additional biologics, cell expansion, or patient-specific customization. Accordingly, the translational value of a scaffold platform should be judged not only by its osteogenic potential but also by its likelihood of being manufactured reproducibly and deployed cost-effectively in routine clinical workflows. 50
Natural polymers
Prioritizing Bio-Recognition over Mechanics Natural organic polymers, including collagen, chitosan, and silk fibroin, are inherently hydrophilic and contain bioactive motifs that support cell attachment and differentiation. Chitosan, a derivative of chitin, is widely valued for its biodegradability and biocompatibility. However, its mechanical utility is constrained by pH-dependent solubility and relatively low stiffness. 51 Similarly, collagen, the primary organic component of bone ECM, provides an ideal osteoconductive surface 52 but lacks the compressive strength required for load-bearing defects. While silk fibroin offers improved handling and mechanical properties compared with collagen, its degradation rate is relatively slow. 51
To compensate for these mechanical limitations, natural polymers are frequently incorporated into composite systems. For instance, electrospun chitosan/polyethylene oxide nanofibers have been shown to support osteoblast attachment, 53 while chitosan–gelatin scaffolds significantly enhanced structural properties and healing in rat critical-sized defects. 54 Importantly, these examples illustrate that natural polymers are most effective when combined with reinforcing phases or architectures that improve load-bearing capacity. Chitosan/nanohydroxyapatite composites have demonstrated superior proliferative responses in rabbit tibial defects, 55 and collagen-HAp scaffolds have been shown to commit human MSCs toward osteogenic lineages in vitro 56 and induce spontaneous mineralization in vivo.57,58 Furthermore, crosslinking collagen with chitosan creates tubular scaffolds with desirable porosity and pliability, mimicking the mechanical properties of blood vessels and enhancing nerve affinity.59,60
From a manufacturing perspective, most natural polymer scaffolds are produced by freeze-drying, electrospinning, or hydrogel-based processing. These methods are effective for generating highly porous architectures, but they often suffer from variability in pore size, source-dependent raw material quality, and crosslinking-dependent mechanical performance, which complicate batch standardization and large-scale production. Although natural polymers offer excellent biological recognition and accessible sourcing, their clinical translation is often hindered by batch-to-batch variability, rigorous purification demands, limited shelf life, and the necessity for secondary crosslinking or composite reinforcement to achieve adequate mechanical strength. 61
Synthetic polymers
Tunable Elasticity and Structural Guidance Synthetic biodegradable polymers, including polylactic acid (PLA), polyglycolic acid (PGA), and poly(lactic-co-glycolic acid) (PLGA), offer superior control over mechanical properties. Their processability and tunable elasticity enable fabrication of structures capable of bearing clinically relevant loads. 51 However, their hydrophobic surfaces often hinder initial cell attachment, and their degradation rates can be difficult to control in vivo, potentially leading to autocatalytic acidic environments. 62
In contrast, synthetic polymers are generally more compatible with scalable manufacturing workflows, including melt processing, solvent casting/particulate leaching, electrospinning, and additive manufacturing. Their greater industrial processability is a translational advantage, although this benefit must be balanced against hydrophobicity, acidic degradation products, and the difficulty of simultaneously achieving high porosity and bone-matched mechanics.
From a mechanobiological perspective, the architecture of synthetic scaffolds is as critical as their chemistry. Electrospinning has emerged as a key technology for producing nanofibrous scaffolds that mimic the hierarchical structure of the ECM. 63 The alignment of these fibers provides contact guidance cues that direct cell fate. For example, Rowland et al. demonstrated that aligned polydioxanone scaffolds supported greater adipogenic and osteogenic differentiation of MSCs compared to random orientations or PLGA counterparts. 64 Further reinforcing synthetic matrices with ceramics, such as PLA/HAp composites, has been shown to upregulate BMP-2 and osteopontin expression, 65 while Poly(ε-caprolactone) (PCL)/PLGA composites have successfully induced Alkaline phosphatase (ALP) and Collagen-1 expression in rabbit models. 66 Together, these studies suggest that mechanical reinforcement combined with bioactive additives is necessary to translate synthetic polymers toward effective bone regeneration. Conversely, while synthetic polymers offer superior industrial scalability and batch reproducibility for large-scale manufacturing, their overall translational cost-effectiveness is often compromised by the need for surface modifications, composite reinforcement, and the clinical management of acidic degradation byproducts. 67
Inorganic and composite systems
Mimicking the Native Stiffness Profile To fully replicate natural bone—a composite of organic collagen and inorganic apatite—scaffolds must integrate multiple phases. Inorganic polymers, such as biocalcite, bio-polyphosphate (bio-polyP), and bio-silica, have been identified as potent metabolic modulators. Bio-silica substrates stimulate osteogenic activity and BMP-2 expression, 68 while bio-polyP induces hydroxyapatite formation and inhibits osteoclastogenesis.69,70
In practice, the most effective strategies involve composite materials in which polymers are reinforced with ceramics (e.g., calcium phosphate, bioglass),71–73 silicon, 74 or nanomaterials 75 to better approximate the stiffness of native bone.
Ceramic Reinforcement: Hydroxyapatite (HAp) is the standard for osteoconductivity. Incorporating HAp into chitosan 76 or collagen scaffolds 57 significantly enhances matrix deposition compared with polymer-only controls. 77 Although β-tricalcium phosphate (β-TCP) resorbs 10–20 times faster than HAp, its brittleness often limits its use in high-load regions. 78
Nanomaterial Reinforcement: Nanomaterials like carbon nanotubes, graphene, and nanohydroxyapatite offer exceptional mechanical strength and high surface-area-to-volume ratios. 75 Rather than being used in isolation, these nanomaterials are most effective when integrated into hierarchical composite designs.
For example, our group developed a mineralized collagen-glycosaminoglycan (MC-GAG) scaffold via coprecipitation, creating a nanoparticulate mineralized content that mimics native bone composition.79,80 Mechanistically, these MC-GAG scaffolds induce MSC osteogenesis and constitutive Smad1/5 phosphorylation independent of exogenous BMP-2, 81 autogenously activating the BMP signaling pathway in vivo. 72 This work illustrates how nanoscale mineral organization, rather than bulk stiffness alone, can critically influence osteoinductivity. Composite systems introduce an additional level of fabrication complexity because mineral phase, polymer phase, pore architecture, and crosslinking conditions must all be controlled simultaneously. For example, MC-GAG scaffolds are fabricated through coprecipitation/mineralization followed by freeze-drying and crosslinking, enabling control over calcium phosphate content, pore size, and scaffold stiffness but also requiring tight process control to ensure homogeneous mineral distribution and reproducible mechanical properties across batches. Although composite scaffolds offer superior biological and mechanical matching, their clinical translation is often complicated by the need to simultaneously control multiple structural phases during manufacturing, which inherently increases production costs, quality control demands, and the difficulty of industrial scale-up. 67
Functionalization for signaling and delivery
Beyond structural mechanics, scaffolds act as vehicles for biochemical and genetic cues.
Growth factor delivery
Sustained release systems are critical for prolonged signaling. Chitosan hydrogels modified with fucoidan have been used to protect FGF-2 from proteolysis, 82 while gelatin-coated β-TCP scaffolds have been engineered for the sustained delivery of rhBMP-2. 83 Similarly, microspheres combining chitosan, nHA, and PLGA can effectively release synthetic osteogenic peptides. 84 However, achieving consistent dose control and avoiding ectopic bone formation remain ongoing challenges.
Gene and RNA delivery
Emerging strategies utilize the scaffold as a transfection platform. While collagen matrices delivering polyethylenimine (PEI)-pDNA encoding PDGF-BB showed promise in transfection, they were associated with prolonged inflammation. 85 More recently, RNA nanotechnology has enabled the creation of “biomineral nanomachines.” Shen et al. developed RNA-based structures that direct intra and extrafiber mineralization within collagen scaffolds, creating an osteoinductive microenvironment that accelerates healing. 86 Although innovative, these approaches require further evaluation regarding safety, scalability, and regulatory feasibility.
In addition to safety and regulatory hurdles, these functionalized systems raise important economic questions, because incorporation of recombinant proteins, nucleic acids, or cell-transfection components can substantially increase production cost, analytical testing burden, storage requirements, and reimbursement uncertainty relative to simpler off-the-shelf scaffolds.
Clinical tolerance and host response
While optimizing the mechanobiological properties of scaffolds is a prerequisite for bone tissue engineering, successful clinical translation ultimately hinges on host tolerance and the mitigation of adverse immune responses. The nature of this host response is intrinsically linked to the biomaterial’s origin. Natural polymers, such as collagen and chitosan, are celebrated for their innate biocompatibility and bioactivity; however, their clinical application is frequently complicated by risks of immunogenicity and pathogen transmission if sourced from allogeneic or xenogeneic tissues without exhaustive purification. 87 Furthermore, when these natural matrices are utilized as nonviral gene delivery platforms—such as those incorporating PEI-pDNA complexes—they have been documented to provoke prolonged localized inflammatory cascades and cytotoxic responses. 88
In contrast, synthetic aliphatic polyesters (e.g., PLA, PGA, and their copolymer PLGA) circumvent the risks associated with xenogeneic sourcing, yet they introduce distinct clinical challenges dictated by their degradation profiles. These polymers degrade in vivo primarily via bulk hydrolysis, releasing acidic monomers such as lactic and glycolic acid. If the localized accumulation of these acidic byproducts outpaces the surrounding tissue’s buffering capacity, it induces an autocatalytic degradation cycle. 89 Clinically, this localized acidic microenvironment can precipitate a robust sterile inflammatory response, characterized by foreign body giant cell recruitment, delayed-onset osteolysis, and exacerbated bone resorption—all of which severely compromise the structural integrity of the regenerating site. 90 Consequently, a critical design imperative for both synthetic and composite scaffolds is the precise calibration of degradation rates to align with the host’s metabolic clearance capabilities, thereby preventing acidic accumulation and subsequent postoperative complications. 90
Emerging Frontiers: Mechanobiologically Adaptive and Intelligent Platforms
Traditional scaffold design has largely relied on static architectures that fail to account for the temporal evolution of the healing fracture. Recent efforts are exploring responsive materials that can adapt mechanically over time or convert mechanical loading into secondary biological signals (Table 3).
Comparative Mechanical and Biological Properties of Native Bone vs. Polymeric Scaffolds
ECM, extracellular matrix; GAG, glycosaminoglycan; HAp, hydroxyapatite; PLA, polylactic acid; PLGA, poly(lactic-co-glycolic acid).
4D printing and spatiotemporal adaptation
The concept of “4D printing” extends additive manufacturing by introducing time as the fourth dimension. 91 These systems utilize shape-memory polymers and stimulus-responsive composites to undergo programmable changes in shape or property in response to physiological triggers such as temperature, hydration, or pH. Systematic reviews highlight that these adaptive architectures can enable minimally invasive deployment and improved conformity to irregular defects without compromising baseline physiomechanical properties compared to static controls.91–93
From a mechanobiological perspective, the principal advantage of 4D systems is their potential to better align scaffold geometry and mechanics with the evolving state of the healing tissue. However, the majority of studies remain proof-of-concept, and long-term in vivo performance, reproducibility, and manufacturing scalability are not yet well established.
Beyond shape change, mechanically adaptive hydrogels represent a significant leap forward. In these systems, stiffness and viscoelasticity are engineered to evolve spatiotemporally, matching the mechanical stiffening of the callus during the reparative phase. Several groups have coupled these materials with finite element modeling to guide mechanical design, but standardized metrics for comparing “mechanical adaptivity” across platforms are still lacking. 94
A generic translational workflow integrating clinical assessment, FE-guided design, and adaptive scaffold fabrication is shown in Figure 3. In this generic scheme, patient-specific imaging is first processed via FEA to map the local mechanical environment and determine optimal strain thresholds. These computational outputs directly inform the geometric design and material selection of shape-memory or stimuli-responsive polymers. Following 4D fabrication, the scaffold is deployed via minimally invasive techniques, where physiological triggers (e.g., body temperature or pH) activate its spatiotemporal adaptation. This closed-loop approach ensures the scaffold not only fills the defect but also dynamically shifts its mechanical profile to match the evolving stiffness of the native healing callus.

Generic treatment workflow for mechanobiology-guided scaffold design in bone regeneration. The proposed workflow integrates clinical assessment, imaging-based defect characterization, finite element (FE)-guided structural optimization, and advanced fabrication into a unified translational pathway. Following patient-specific evaluation of defect geometry, anatomical site, fixation requirements, and host bone quality, imaging data are used to reconstruct the local mechanical environment. FE modeling then predicts strain, stress, and fluid-flow distributions to define mechanically permissive design targets for scaffold architecture, porosity, degradation profile, and material composition. These outputs inform fabrication of a patient adapted scaffold, including 4D-printed systems with time-dependent or stimulus-responsive behavior. After implantation, scaffold performance is shaped by fixation mechanics and the evolving stages of repair, including hematoma formation, callus development, and remodeling. Longitudinal follow-up data can then be fed back into future model refinement and design optimization, enabling a closed-loop strategy for scaffold translation.
Mechanoelectrical transduction: Piezoelectric scaffolds
Recognizing that bone is an inherently piezoelectric tissue, researchers are developing biomaterials that convert daily mechanical loading into local electrical stimulation. These bioelectrical signals are thought to influence ion flux, focal adhesion dynamics, and mechanosensitive pathways (e.g., Yes-associated protein [YAP]/Transcriptional co-activator with PDZ-binding motif [TAZ]), although the precise in vivo dose–response relationships remain incompletely defined. 95
Recent translational work has focused on piezoelectric polymer composites, particularly poly(vinylidene fluoride)-based systems reinforced with osteogenic phases like hydroxyapatite (HAp) or barium titanate (BaTiO3). These composites have demonstrated accelerated bone repair in vivo by effectively integrating electrical cues with microtopographical guidance. Mechanistic studies further clarify this effect; for instance, a mechanically tunable fiber-reinforced hydrogel was recently reported to enhance bone repair specifically through the PIEZO1–integrin axis, illustrating how scaffold mechanics and biochemical modulation can be coordinated to sustain osteogenic mechanotransduction. 96 Nevertheless, challenges remain regarding material fatigue under cyclic loading, long-term biocompatibility, and reproducible electrical output in clinically relevant environments.
Data-driven design and closed-loop optimization
Optimizing scaffold microarchitecture—balancing porosity, topology (e.g., triply periodic minimal surface, TPMS), anisotropy, and degradation—remains challenging using purely empirical approaches. As a result, data-driven methods are increasingly being explored. In emerging closed-loop workflows, ML models are trained on experimental or simulated datasets to predict mechanical or biological responses and to suggest candidate architectures that better meet predefined performance criteria.97,98 Importantly, these approaches are most effective when constrained by mechanobiological principles rather than used as purely black-box optimizers. Their generalizability depends on dataset quality, representativeness, and consistency of experimental assays.
Looking forward, integrating mechanobiology-informed descriptors (e.g., predicted strain/strain-rate fields, fluid shear, and electrical potentials) with experimental datasets may further improve generalizability and reduce trial-and-error, especially when coupled to mechanistic simulation (FEA) and standardized reporting.94,99 However, translation of ML-guided designs to clinically manufacturable and regulatory-compliant scaffolds remains a substantial hurdle.
Conclusions
Effective bone regeneration requires more than structural defect filling; it depends on providing a mechanical environment compatible with the biology of fracture healing and subsequent remodeling. Bioinspired polymeric and composite scaffolds that integrate organic matrices with inorganic reinforcements currently represent the most promising strategy to balance bioactivity and mechanical competence. Recent advances in adaptive materials, including 4D-printed systems and piezoelectric composites, offer new opportunities to better match the evolving mechanical and electrical environment of healing bone. However, these approaches remain largely at the preclinical stage and require more rigorous mechanistic validation, long-term safety assessment, and scalable manufacturing strategies. Computational modeling, particularly FEA, has become indispensable for linking scaffold microarchitecture to mechanical performance and biological outcomes. Nevertheless, current models still struggle to fully capture the coupled processes of tissue growth, vascularization, and material degradation in vivo.
Major barriers to clinical translation include insufficient load-bearing capacity in large defects, limited and inconsistent vascularization, variability among animal models, and a lack of standardized testing frameworks. Addressing these challenges will require closer integration of mechanobiology, materials science, and computational modeling, as well as improved alignment between preclinical models and clinical scenarios.
Future progress will depend on developing mechanically adaptive scaffold systems that are not only bioactive but also capable of delivering spatially and temporally appropriate mechanical cues to guide reliable bone regeneration. Future scaffold development should therefore be evaluated not only against mechanobiological benchmarks but also against practical indicators of economic viability, including manufacturability, storage and sterilization burden, requirement for adjunctive biologics, and the anticipated cost of complication management.
Authors’ Contribution
S.L.: Conceptualization, methodology, writing original draft, and funding acquisition. J.W. and P.D.: Visualization and data curation. X.R. and X.L.: Investigation and validation. J.C.L. and Q.Z.: Conceptualization, writing—review and editing, and supervision.
Data Availability
Data sharing is not applicable to this article as no new data were created or analyzed in this study. All data supporting the findings of this review are available within the article and its references.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
This work was supported by the