
Abstract
This study assesses the extent of “first-cost green building construction premiums” in the healthcare sector based on data submitted by and interviews with 13 current LEED-certified and LEED-registered healthcare project teams, coupled with a literature survey of articles on the topics of actual and perceived first-cost premiums associated with green building strategies. This analysis covers both perceived and realized costs across a range of projects in this sector, leading to the following conclusions: Construction first-cost premiums may be lower than is generally perceived, and they appear to be independent of both building size and level of “green” achievement; projects are using financial incentives and philanthropy to drive higher levels of achievement; premiums are decreasing over time; and projects are benefiting from improvements in health and productivity which, although difficult to monetize, are universally valued.
Keywords
Calculating the capital first costs and associated benefits of green healthcare facilities is a challenging yet important undertaking. This study assesses the extent of first-cost green building premiums in the healthcare sector based on data submitted by and interviews with 13 current Leadership in Energy and Environmental Design (LEED®)-certified and LEED-registered healthcare project teams, coupled with a survey of articles and studies on the topic of the actual and perceived first-cost premiums associated with green building strategies in the broader construction industry This analysis reveals both perceived and realized costs across a range of projects in this sector. The findings are summarized as follows:
There is no single industry standard for defining first-cost green building premiums, yet there is widespread presumption that a consistent definition exists. Each project was asked to identify which design and construction elements were tracked and reported as a “premium”; the survey reveals little consistency in both the strategies and elements included or in calculation methodology.
Projects are achieving a broad range of reductions in energy demand; a limited subset of projects is using projected reductions in operating costs as a component of a business case for increased capital spending.
First-cost green building premiums may be lower than is generally believed, and they appear to be independent of both building size and level of “green” achievement as determined by the U.S. Green Building Council (USGBC) LEED Rating System.
Projects are benefiting from a wide range of financial incentive programs and private philanthropy that contribute to higher levels of sustainable building achievement, as measured by LEED, across a broad range of strategies.
Benefits attributed to green building include human health and productivity, staff recruitment/retention, and improved community perception; however, these benefits are difficult to quantify and are beyond the scope of this analysis.
Unlike the commercial office building sector, the healthcare sector priorities of human health and patient, workplace, and environmental safety are nested within a broad organizational mission focused on healing and stewardship (Guenther, Vittori, & Atwood, 2006). This important distinction leads to significant challenges in defining consistent first-cost green building premiums and benefits among the projects studied. This values-laden context blurs the distinction between design elements that add costs to the construction budget and those that are increasingly acknowledged as standard practice for the healthcare sector. Contributing to the challenge to conduct a statistically significant first-cost green building premium analysis is the reality that the pool of completed green healthcare facilities (particularly green hospitals) is still relatively small, albeit growing at an impressive rate. Finally, there is wide variation in the marketplace regarding the interpretation of the question: “Does green building cost more?”
A prevalent notion in today's market is that green buildings cost more. “More than what?” is the first question that should be carefully framed. Does a green hospital cost more than the exact same building without the green features? More than the available capital budget? Or more than a neighboring comparable building of the same size and complexity? A related question is, of course, just how much does a hospital cost to construct? And, finally, what is the cost of not constructing a green hospital? Already, it is clear that this is a complex question requiring careful analysis (Guenther & Vittori, 2008).
One of the most common methods to establish the first-cost green building premium is to compare the final cost of a building to the established budget of the project; this was the methodology employed by 4 of the 13 subject projects that reported no first-cost premium. A 2004 study noted that more than 50% of the subject projects in their survey applied this methodology (Matthiessen & Morris, 2004). An alternative methodology suggests that projects enumerate specific sustainability enhancements by isolating individual elements and estimating the difference between a non-green baseline material or system and the green option, regardless of the impact on the project budget. Nine of the subject projects applied this methodology in various forms to arrive at a first-cost green building premium. In no instance did project teams derive the definition of green building premium by comparing their overall construction cost to other programmatically similar but non-green facilities in their region.
More importantly, for the mission-driven healthcare sector there is understandable concern that isolating the subject of first-cost green building premiums from a broader discussion of benefits does not serve the healthcare sector well. This is because it is a sector that applies triple bottom line thinking (that is, a commitment to occupant health and safety, financial efficiency, and community benefit) to its core business—the provision of healthcare services—so dissociating benefit from cost places unwarranted emphasis on the first-cost capital component (Guenther & Vittori, 2008; Guenther, et al., 2006). In this survey many of the subject teams studied expressed this concern openly and passionately. Therefore, following a presentation of the core data is a discussion of both the operational savings and additional associated “benefits” articulated by our subjects.
Summary of Findings
This research focuses on the first-cost green building premiums estimated from 13 green healthcare construction projects in the United States, ranging in size from 28,000 square feet (SF) to 470,000 SF. Eleven of these projects were completed between 2003 and 2008; two are to be completed in 2009. Owing to differences in size, energy intensity, and program complexity among the sample projects, this research distinguishes among three related but distinct medical building types—acute-care hospitals, outpatient buildings, and mixed-occupancy facilities. Participants completed a standardized information matrix, which was followed by a telephone interview.
The subject projects reveal the complexity of estimating first-cost green building premiums in the healthcare sector. Overall findings include:
First-cost green building premiums reported by the subject projects range from 0% to 5% before financial incentives are accounted for, and from 0% to 3.8% after financial incentives are included. In this study, financial incentives include philanthropic gifts, grant programs, and public or utility incentive programs.
First-cost green building premiums do not correlate directly with the LEED certification level of a project. Indeed, consistent with other studies (Matthiessen & Morris, 2004; Matthiessen & Morris, 2007), healthcare facilities that achieve LEED-Gold or -Platinum certification do not bear higher first-cost green building premiums than those that achieve LEED-Certified or -Silver.
Projects that achieved LEED certification early in this decade indicated higher first-cost green building premiums than those that achieved it later. In general, and consistent with other studies (Kats, 2003a; Kats, 2003b; Kats, 2005; Kats, 2006), projects are trending toward reduced first-cost premiums over time.
A closer analysis reveals a range of factors that contribute to the variability of reported first-cost green building premiums; these are examined at length later in this article:
Definition of strategies included in the calculation of the premium
Methodologies used to calculate the premium
Total amount of grants or incentives (including utility rebates) awarded to projects.
In all instances, projects that received financial incentives used them to “buy down” or reduce the reported first-cost premium. A summary of findings is presented in Exhibit 1.
Summary of Findings
Projects that reported no first-cost green building premium described a design process in which the building budget was established and the team integrated sustainable strategies successfully into the overall construction budget—essentially a basis-of-design approach—thereby eliminating the need for line item premiums and savings. Three of the 13 projects reported zero first-cost green building premiums based on the assessment of delivering a project within the established budget; one project did not track or report first-cost green building premium data.
The availability of grants, financial incentives, and/or philanthropy influences the choice of sustainability strategies. In the projects studied, the availability of financial incentives to offset a portion of increased first-costs enabled increased expenditures. This coupling of incentives to increased first-costs led projects to offset overall first-cost green building premiums by the amounts of the incentives received.
The actual building components included in the first-cost green building premium vary widely, yet overall aggregate premiums fall within a fairly narrow range.
The baseline of healthcare design is changing. Consistent with the broader construction industry, as more sustainable materials enter the marketplace, the first-cost premium associated with these materials lessens (Green Buildings, 2007). A comparison of study projects revealed that green design strategies identified as components of first-cost green building premiums in early projects—because of either a lack of market-available alternatives or the perception of “above standard” solutions—had become embedded in the definition of a baseline healthcare building in later projects.
The data further suggest that an owner's motivation for undertaking a green building process is key to determining the elements included in the first-cost green building premium reported. Subject projects that prioritized occupant health and safety, for example, were more likely to exclude healthier material selection from their premium calculation. Project teams that focused on operational efficiency in some instances used the operational savings expected to accrue from energy and water efficiency measures to justify green strategies with capital cost premiums that do not offer a direct quantifiable financial payback, such as enhanced indoor air quality or outdoor places of respite. These trends and attitudes are examined in the sections that follow.
Background: What Makes Green Healthcare Unique?
Healthcare is the largest single service sector in the U.S. economy; the U.S. Department of Commerce International Trade Administration (2008) estimates that it represented 16% of the gross domestic product (GDP) in 2007, and this is projected to grow to 19.5% of GDP by 2017. The sector also acts as an economic driver through job creation—the U.S. Department of Labor Bureau of Labor Statistics (2008b) estimates that the sector employed approximately 13.28 million people as of May 2008. In many regions, healthcare is the dominant employment sector (Bureau of Labor Statistics, 2008a); in 2007, hospitals were the second largest source of private sector jobs in the United States (American Hospital Association, 2009).
Healthcare construction is experiencing its largest building boom in decades (McGraw Hill, 2007). This reflects, in part, the fact that many healthcare facilities constructed in the 1950s and 1960s have reached the end of their useful life and need to be replaced (Carpenter, 2008). In some regions, changes in regulatory standards—such as seismic regulations in California (Office of Statewide Health Planning and Development, 2005)—are further accelerating the healthcare construction boom. According to the U.S. Census Bureau (2008), healthcare invested $47.4 billion in construction between April 2007 and March 2008, a 7% increase over the previous year. The investment banking firm FMI Corporation projects annual healthcare construction spending to reach $60.1 billion by 2010 (Kure, 2007).
Although healthcare was initially slower to embrace green building principles and practices than other sectors, such as commercial office buildings (Green Buildings, 2007), McGraw-Hill Construction and Research Analytics (2007) projects a substantial increase in green building projects in the healthcare sector in the coming years; the percentage of healthcare organizations that projected that more than 30% of their projects would have a green building focus jumped from 4% in 2006 to 6% in 2007 to 19% of building starts in 2008. The steady increase of Green Guide for Health Care registered projects from 2005 to 2007 (Figure 1) is another indicator of the increasing engagement of the healthcare sector in sustainable building.
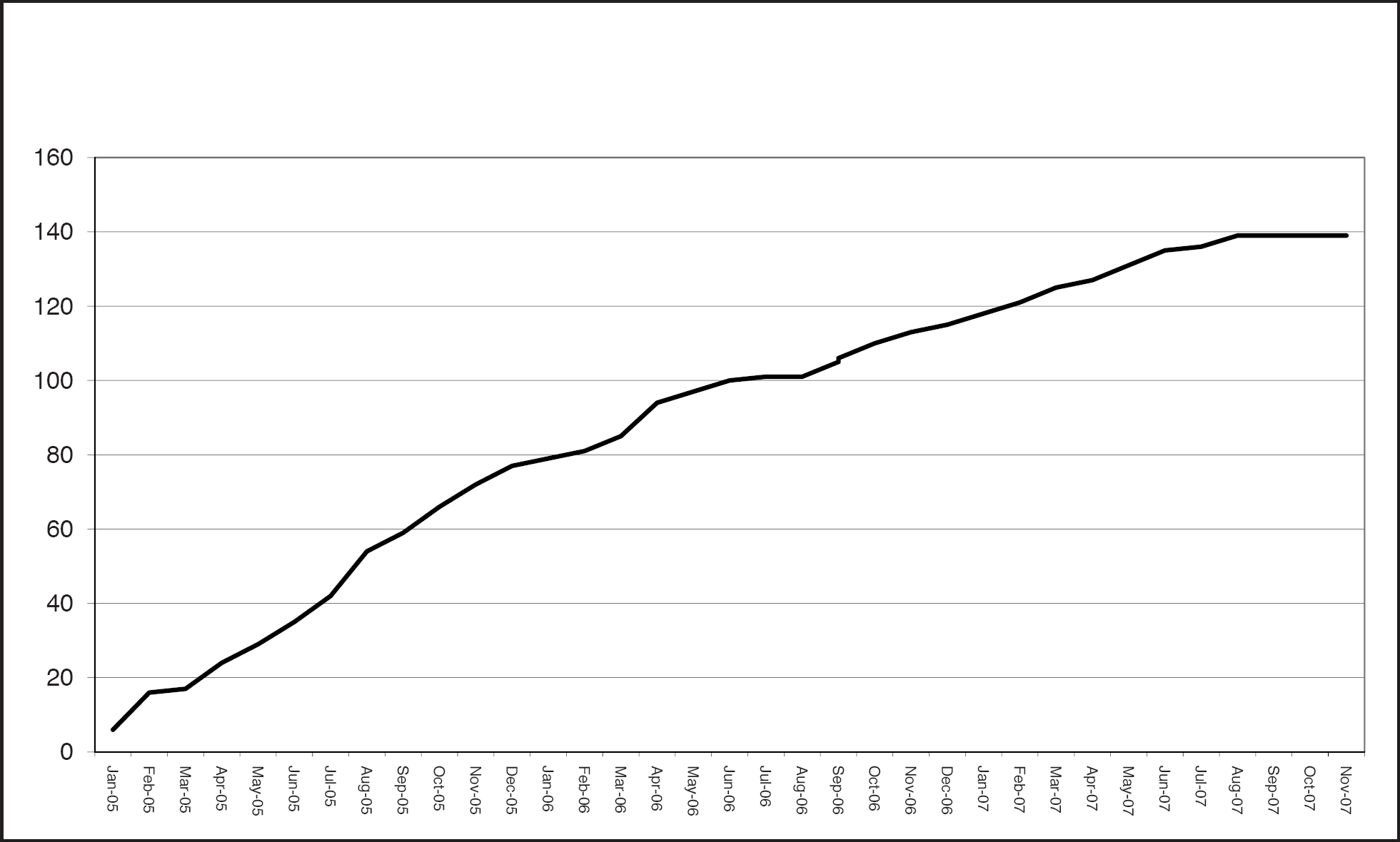
The growth of Green Guide registered projects held steady throughout 2007.
The healthcare sector spans a range of building types including hospitals, outpatient clinics, medical office buildings, and labs (Joint Commission, 2009). According to the U.S. Department of Energy Commercial Buildings Energy Consumption Survey, licensed acute-care hospitals represent only 6% of the total number of healthcare facilities, but 60% of total square footage (U.S. Department of Energy, 2003). Acute-care hospitals are on average more than 16 times the size of a typical office building (about 241,400 SF for inpatient healthcare buildings compared to 14,800 SF for office buildings) and operate with more than twice their energy intensity per square foot (187,700 Btu/SF for inpatient healthcare buildings compared to 92,900 Btu/SF for office buildings) (U.S. Department of Energy, 2003). In comparison, outpatient healthcare facilities such as medical office buildings display energy intensity similar to commercial office buildings (94,600 Btu/SF), although on average they are slightly smaller (10,400 SF). Given the range of energy intensity associated with specific types of healthcare facilities, it is essential to differentiate these buildings based on programs and services to establish a relevant basis for comparison.
What drives the energy intensity of acute-care hospitals? Acute-care facilities are stringently regulated, complex buildings operating 24 hours a day, 7 days a week and dependent on multiple tiers of mechanical and electrical health and safety systems (GGHC, 2007). In addition to strict regulations covering mechanical ventilation and air change rates, hospitals contain continuously operating diagnostic equipment that generates substantial cooling loads. As a result, even when maximizing efficiency by means of strategies such as “right-sizing” equipment, redundancies must be accommodated to safeguard critical services and provide for future incremental growth and technology changes.
Defining Green Healthcare Projects
According to the Office of the Federal Environmental Executive (White Paper on Sustainability, 2003), green building is defined as “Increasing the efficiency with which buildings and their sites use energy, water and materials, and reducing building impacts on human health and the environment, through better siting, design, construction, operation, maintenance, and removal—the complete building life cycle” (p. 4). Currently, two tools are in use to support the design and construction of green healthcare projects: the USGBC's LEED® third-party green building rating system and the Green Guide for Health Care (Green Guide), a project of Center for Maximum Potential Building Systems and Health Care Without Harm. The Green Guide is a voluntary, self-certifying, best practices green design, construction, and operations toolkit tailored to the healthcare sector (Green Guide, 2007). Nearly 700 projects are registered with one or both systems. As of April 2009, more than 150 projects were registered with the Green Guide; some of these projects are also among the 480 healthcare projects registered with LEED (USGBC, 2009). To ensure that the projects included in this study had a documentable basis to be defined as green, all the selected projects are either registered or certified with the USGBC LEED program.
As of April 30, 2009, 43 healthcare projects had achieved LEED certification (USGBC, 2009). Of these, 13 are acute-care or specialty hospitals, 5 are ambulatory (mixed-occupancy) buildings, and 25 are medical office buildings/clinics (Figure 2). A graph of the LEED certification levels achieved by the 42 healthcare projects certified from 2003 through April 2009 (Figure 3) demonstrates increased activity in the marketplace in tandem with the earlier referenced growth of the Green Guide registered projects. The anticipated launch of LEED for Healthcare in late 2009 is likely to accelerate this trend (Green Guide, 2008; USGBC, 2009).
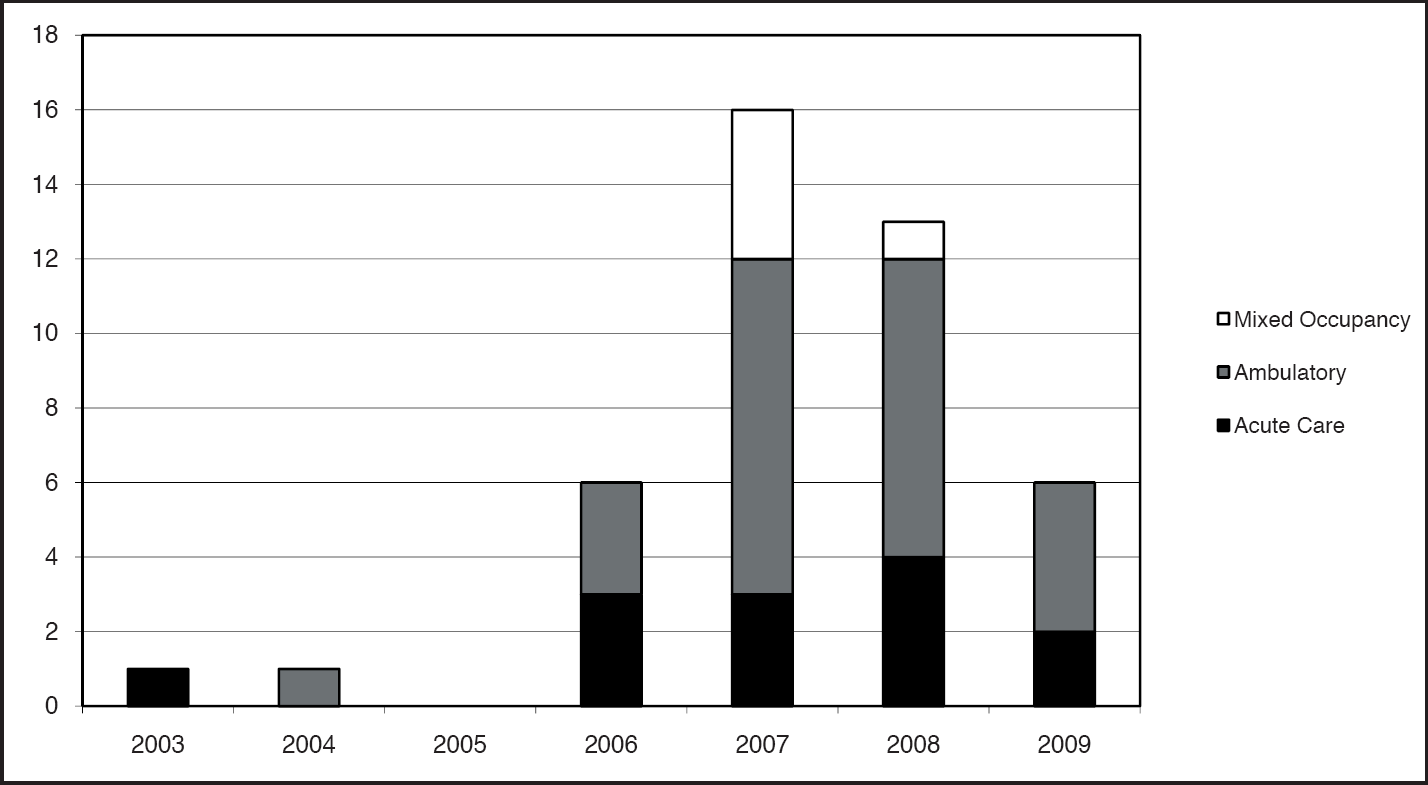
LEED-certified healthcare projects by project type 2003–2009.
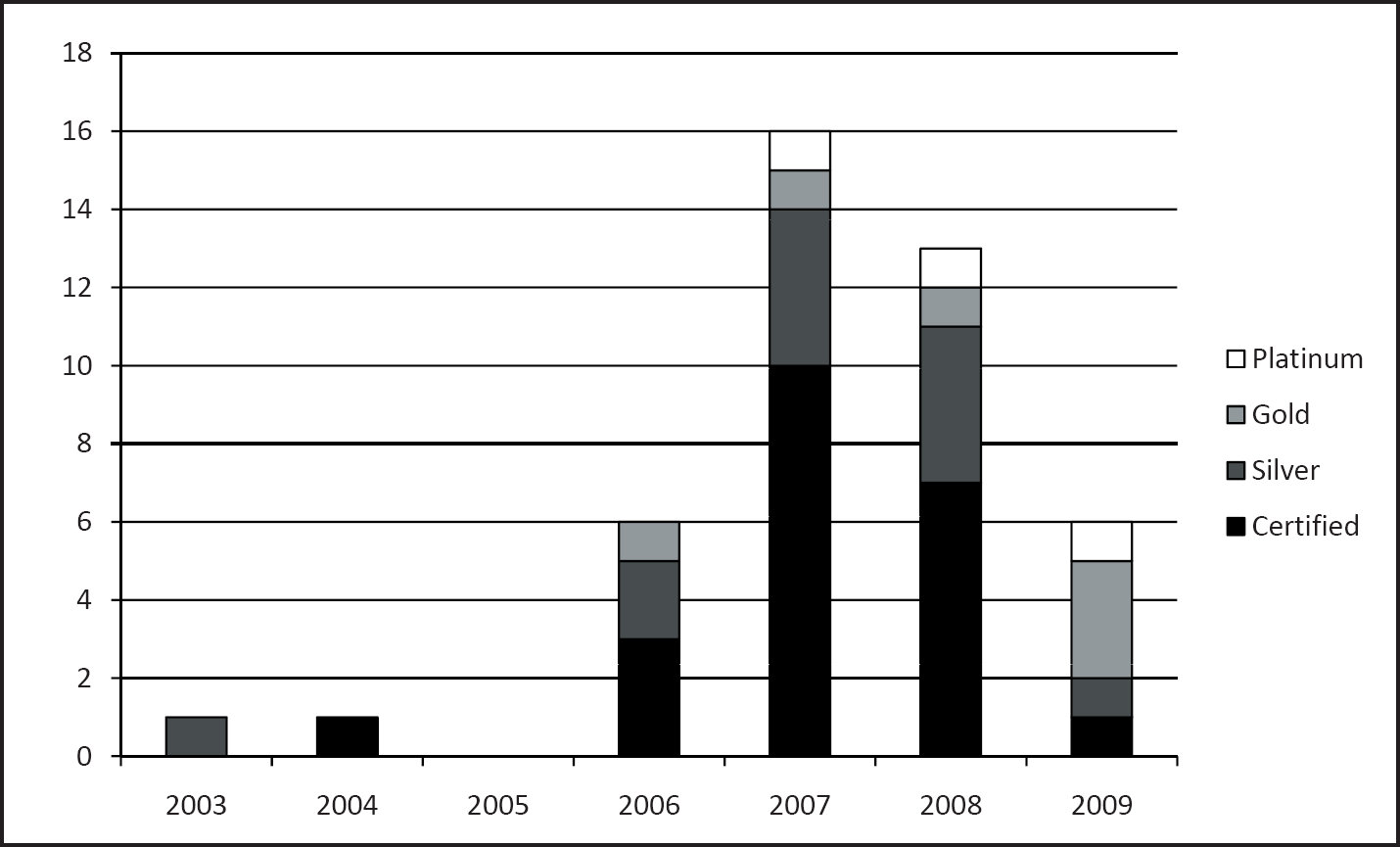
Level of achievement of LEED-certified healthcare projects 2003–2009.
Defining the Study Projects
Of the current 43 total LEED-certified projects, 10 were selected for inclusion in the study: five acute-care hospitals, two large ambulatory (mixed-occupancy facilities), and three ambulatory care facilities. The study excluded specialty hospitals, long-term care facilities, medical office buildings of less than 10,000 SF, and renovation projects. In addition to these 10 LEED-certified projects, the study data set included three additional, completed, registered acute-care projects awaiting LEED certification for which costs are summarized. This enabled the study to increase the number of acute-care hospitals surveyed, as well as include current data associated with recently completed projects (two of these have achieved certification since the completion of the study and are included in the April 2009 total). The projects selected span large to small facilities, including eight acute-care hospitals, two mixed-occupancy buildings, and three ambulatory care projects.
The 13 projects in this study generally fall within the Commercial Buildings Energy Consumption Survey square footage data for either inpatient healthcare facilities or outpatient buildings, although two mixed-occupancy projects—the Oregon Health and Science University (OHSU) Center for Health and Healing (400,000 SF) and St. Mary's Duluth Clinic (208,000 SF)—bridge the inpatient and outpatient building types in terms of both size and building program. (See Figure 4.) These buildings do not include beds, nor do they operate continuously; however, they do house surgical facilities and extensive diagnostic equipment. OHSU provides ambulatory surgery, while St. Mary's Duluth Clinic offers extensive oncology radiation and diagnostic imaging, chemotherapy, and oncology beds. Hence, their energy intensity profile approaches that of acute-care hospitals.
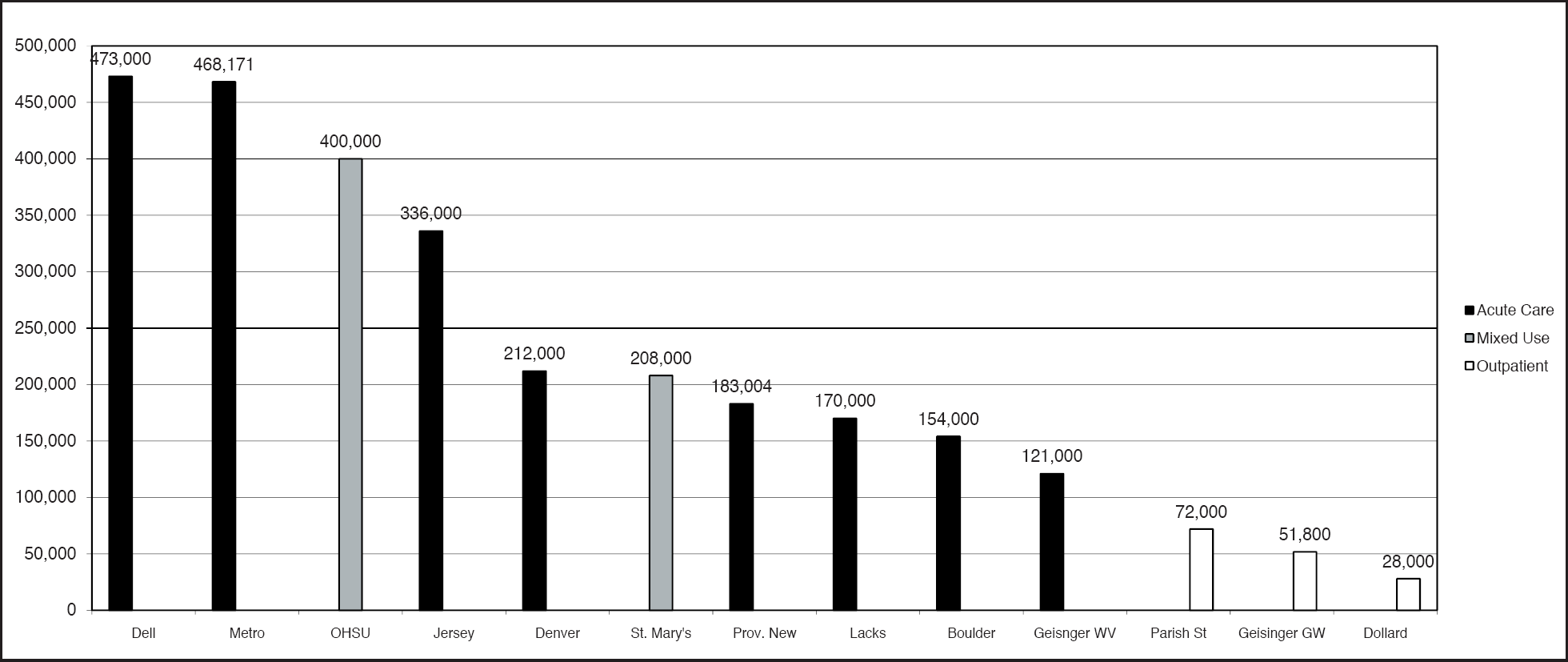
Healthcare projects in this study, organized by size and type.
The Business Case for Green Healthcare
A growing body of literature seeks to quantify green building costs and benefits across multiple building sectors. Beginning as early as 2000, published surveys anticipated the construction cost premiums associated with green building; at this writing, those have largely been superseded by studies examining the actual costs of completed buildings. At the same time, particularly in market sectors with a limited data set of completed buildings, there are multiple market surveys of perceived costs and benefits. This section summarizes the state of the surveys to date; it is not intended to be an exhaustive review of each survey or its findings.
The David and Lucile Packard Foundation commissioned one of the earliest studies projecting the anticipated green building cost premium related to the construction of a new headquarters building (Packard, 2002). The study concluded that the cost differential between a certified LEED facility and a conventional building was less than 1%. A unique aspect of the study monetized the costs associated with pollution: when the cost of environmental pollution was taken into account, the LEED-certified building cost less over 20 years. At the same time, the study projected a relatively linear relationship between increasing levels of sustainability and first cost, a finding that has continued to inform subsequent studies. However, when the costs of pollution are included, the life-cycle costs dramatically decrease with greater reductions in fossil fuel energy use. The study concludes that the lowest life-cycle cost correlates with the highest level of sustainable building (i.e., LEED-Platinum or beyond). Few, if any, subsequent studies have recognized the generally externalized life-cycle costs of pollution.
As the data set of completed green buildings expanded, several later studies quantified the actual construction cost performance of green buildings. Few have specifically addressed healthcare, though key conclusions from more general green building cost studies are relevant to healthcare:
Many green buildings can be built for no premium over traditional construction. In two separate studies, construction cost consultants Davis Langdon (Matthiessen & Morris, 2004; Matthiessen & Morris, 2007) compared data on particular building types in the same region over a similar time period. They confirmed: “There is no significant difference in average costs for green buildings as compared to non-green buildings” (Matthiessen & Morris, 2007, p. 3).
On average, the premium for green office buildings (all LEED levels of achievement) is about 2%. Operational energy savings alone more than offset the increased first costs associated with green building (Kats, 2003a; Kats, 2003b).
The factors that affect costs have been isolated as follows:
The earlier green building objectives are incorporated into the design, the more likely it is that the project will stay on budget (Matthiessen & Morris, 2004).
The climate where the building is to be constructed influences whether or not the project can achieve particular points, and it can affect the cost of achieving particular LEED certification levels (Matthiessen & Morris, 2004).
Often, higher first costs can be avoided by employing a design team experienced in green building (Matthiessen & Morris, 2004).
Relative to healthcare, a study by construction cost consultants Matthiessen and Morris (2007) compared the costs of 17 green and nongreen ambulatory care buildings (9 LEED and 8 non-LEED) in their extensive construction cost database to determine whether green buildings cluster in the upper ranges of cost per square foot. Buildings in the sample included cancer treatment centers, ambulatory surgery centers, and ambulatory care centers. Medical office buildings were not included. Although the authors of the study admit that the sample size is insufficient to develop robust statistical data, it was evident that the green buildings fall well within the range of overall sector costs.
Consistent with data from other market sectors, the Matthiessen and Morris survey (2007) found no statistical correlation between increased construction costs and green buildings, reconfirming the earlier Matthiessen and Morris (2004) conclusions:
There is a very large variation in the cost of buildings, even within the same building program category. Cost differences between buildings are primarily attributable to program type.
Factors such as the local construction economy, level of design, and regulatory issues often influence total first cost as much as or more than sustainable design strategies.
There are low- and high-cost green buildings; there are low- and high-cost nongreen buildings (Matthiessen & Morris, 2004).
Few studies have examined the association between first-cost green building premiums and LEED certification level. Early studies projected a relatively straight-line increase in the construction cost premium based upon certification level (Kats, 2003a; Kats 2003b; Packard Foundation, 2002; Turner Green Buildings, 2005). For example, Turner Green Buildings (2005) projected premiums ranging from 0.8% for LEED-Certified buildings to 11.5% for LEED-Platinum achievement. Although the limited initial data seemed to support this notion (Kats, 2003a; Kats, 2003b), Amory Lovins and the Rocky Mountain Institute proposed a powerful countervailing cost model. Lovins (2004) postulated that, although capital costs would increase initially as sustainable building features were added to conventional buildings, an integrated design process would ultimately lead to synergies between building systems that would ultimately drive initial construction costs lower than conventional construction (Figure 5). In fact, the LEED-Gold and -Platinum certified buildings in this study realized some level of synergy that reduced their first-cost premiums.
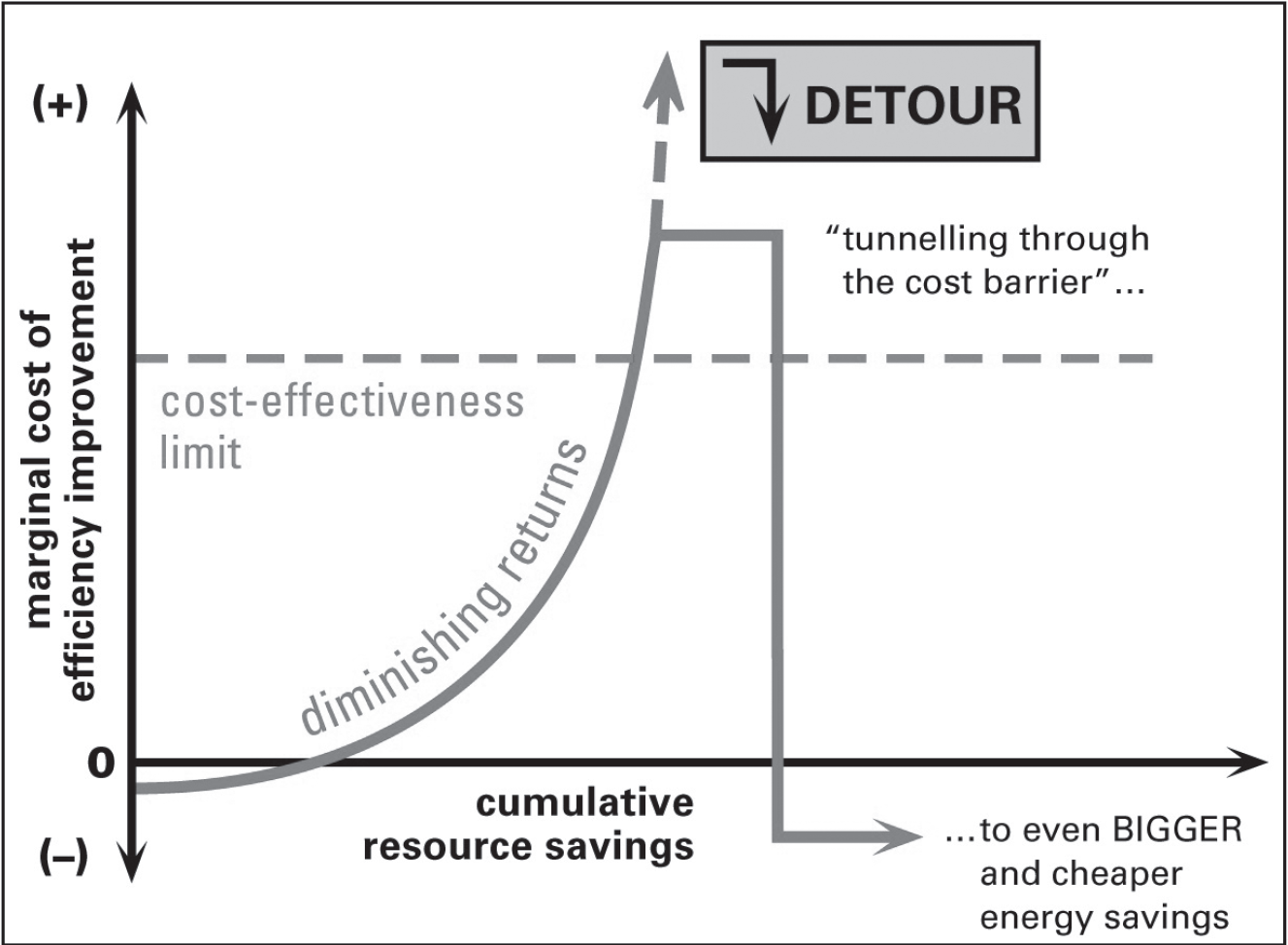
Tunneling through the cost barrier.
At the same time, anecdotal evidence is accumulating that refutes the notion of substantial first-cost green building premiums at all levels of LEED certification. Gerding Edlen, the LEED developer of the OHSU Center for Health and Healing, a LEED-Platinum certified building included in this study, confirms that LEED-certified projects should cost only slightly more than traditional projects:
“Cost depends on project specifics and the LEED level targeted,” said Dennis Wilde, senior project manager at Gerding Edlen. “Gold ratings can increase hard construction costs between 1% and 2%,” he said, “while attempts at Platinum can be upward of 5%. But LEED-Certified or -Silver projects should see no increase, especially if the participants have experience. If you've been to this party before, there should be no material cost increase,” Wilde said. (Ryan, 2005)
Survey participant Bill Gladish, Director of Construction for Geisinger Health, confirmed that specific factors contributed to keeping first-cost green building premiums within a manageable range:
We were fortunate [with the Wyoming Valley Critical Care Building] in hiring construction managers with LEED experience. We looked for people who knew the ropes, so to speak. Consequently, everyone was on board early. [Wyoming Valley] is a difficult project. The daily operational and logistic requirements of owning and maintaining emergency department and operating room environments places rigorous demands upon the design that are not present with less complex building types such as office buildings. There's not a lot of latitude in this kind of building. (Bill Gladish, personal communication, July 16, 2008)
On the topic of benefits accrued from green building, the early Capital-E study of completed office buildings in California concluded the following:
Green buildings offer benefits that conventional buildings (also known as “brown buildings”) do not, including improved indoor air quality, worker recruitment, retention and performance benefits, and enhanced public image.
The largest financial benefits may be improved worker health, performance, and retention. Staffing costs dwarf the operating costs of buildings; therefore, even modest increases in worker health and productivity provide significant benefits. For the purposes of his analysis, Kats conservatively assumes a 1% increase in productivity for green buildings compared to non-green buildings. Several subsequent studies support this estimate (while confirming its conservatism) (Kats, 2003a).
In Greening America's Schools, Capital-E (Kats, 2006) documented the costs and benefits associated with green school buildings. A national review of 30 green school projects demonstrated that the first cost of green schools averaged 2% more than conventional school buildings (or $3/SF). Financial benefits ranging from energy and water conservation to health improvements (reductions in the incidence of asthma, cold, and flu) to improved teacher recruitment and retention total $74/SF. Kats summarized his findings as follows: “Building healthy high-performance school buildings is now far more fiscally prudent and lower risk than building conventional, inefficient, and unhealthy school buildings” (Kats, 2006, p. 4).
Two recent surveys of healthcare executives focused on the perceived costs and benefits of green building in healthcare. Building Design + Construction (BD&C) magazine's “Green Buildings Research White Paper” (2007) includes a survey of Green Guide users. When asked how much of a premium they expected to pay for a green hospital, 17% of respondents assumed the premium would exceed 10%; 19% expected a 6–10% premium. The largest single group of respondents (43%) identified the range found in this study: 0–5%. More importantly, 90% of the BD&C survey respondents identified their organizations as incorporating or planning to incorporate green concepts into their capital projects despite the perception of increased capital costs.
The McGraw-Hill Construction and Research Analytics Health Care Green Building SmartMarket Report (2007), based on a survey of healthcare and hospital administrators, reported a lack of consensus around the value of perceived first-cost premiums associated with green building. When asked whether green building burdens construction projects with an unjustifiable cost premium, 36% responded that green building benefits do not justify a cost premium; 24% disagreed with that position; and 40% of respondents were neutral. However, almost 50% of SmartMarket Report respondents expressed the perception that green buildings do not live up to the promise of a return on investment. The report concludes that “lack of knowledge about green techniques” is the most significant barrier to green design in healthcare (McGraw-Hill, 2007, p. 21), indicating that some of the negative responses to their survey may have reflected perceived, rather than real, cost differentials between green and conventional buildings.
More importantly, these survey responses stand in stark contrast to the reported experiences of owners and design teams that engage in and complete green building projects. Respondents in this study believe that green building strategies have become embedded in the definition of a “better healthcare building”; they report that their firms and/or healthcare systems are continuing to raise the level of sustainable design on subsequent projects. Brian Toevs, a partner with the environmental building consultant 7group, describes the transformation of Geisinger Health: “It has gone from ‘Can we get LEED certification?’ to ‘Not only can we get it, but we can get Silver and beyond’” (Brian Toevs, personal communication, July 16, 2008).
Several surveys have focused on the perceived operational benefits associated with green building in healthcare, such as operational efficiency, staff recruitment and retention, and occupant health. Although a growing number of evidence-based studies have established correlations between specific design features such as daylighting and improved patient recovery, evidence for health and operational benefits from green healthcare building practices remains largely anecdotal. Interestingly, findings from the Turner Construction Market Barometer (2005) confirm this anecdotal trend: more than half of the respondents, regardless of whether the respondent worked at a firm with green building experience, expected green buildings to increase building value, and to improve occupant health and well-being, worker productivity, and return on investment.
A University of California at Los Angeles Anderson School study on the diffusion of green building practices reports: “Casual observation and anecdotal evidence indicate a few promising nonmonetary/secondary benefits:
Faster completion with fewer delays and more on-time deliveries
Faster sales and absorption rates of green product
Greater overall satisfaction and quality of construction
Higher worker satisfaction and productivity” (Cryer et al., 2006, p. 9)
The McGraw-Hill Construction and Research Analytics SmartMarket Report (2007) survey identified the three most common perceived benefits of green building in healthcare:
Lowering life-cycle costs such as energy efficiencies and productivity increases
Being part of an industry that values the environment
Perceived benefits of green building in healthcare
Values-Driven Design and Construction: Enriching Community Benefits Through Green Hospitals, a white paper sponsored by the Robert Wood Johnson Foundation, concludes that healthcare facilities have begun to identify green building as aligning with their mission to provide healing and community stewardship (Guenther et al., 2006). Although these institutions set goals of improved performance to justify their adoption of green building principles, their executives report that embedding a health-based focus in their approach to green building has positioned them as leaders in their communities, boosted patient satisfaction survey scores, and improved staff recruitment and retention in addition to building performance (Guenther, et al., 2006).
In conclusion, both empirical and anecdotal evidence in the existing body of literature overwhelmingly contradicts healthcare executives' perception that green buildings cost significantly more than traditional buildings. Moreover, research suggests that the benefits derived from direct operational cost savings (e.g., energy, water), productivity, and health gains more than offset the modest first-cost premium required to build green healthcare facilities.
The First-Cost Green Building Premium
Because no industry standard that defines the components of a first-cost green building premium exists, survey participants were given the following working definition to guide their responses: First-cost green building premiums are defined as the additional construction costs associated with design and construction elements included in a project primarily due to their environmental performance, including strategies where additional costs were offset by financial incentives. Project teams were asked to identify both “soft costs” (e.g., commissioning fees, energy modeling, registration and certification fees) and “hard costs” (i.e., premium construction costs associated with the use of a particular material or system). For projects located on designated brownfields, environmental remediation was excluded from first-cost premium calculation because it is a legal requirement. After receiving this basic guidance, each project team was asked to identify the full range of soft and hard costs that were tracked during the project as a first-cost green building premium, both in actual dollars and as a percentage of total construction cost.
The methodology of reporting first-cost green building premiums as percentages of total construction cost has a number of objectives: It attempts to standardize data across buildings of varying size and complexity located in divergent construction markets over a period of 7–10 years, during which the construction industry exhibited significant, albeit geographically uneven, growth (Green Buildings, 2007; McGraw-Hill, 2007). The range of sizes and reported construction costs of the 13 projects in this study is significant—leading to far greater variances in the total dollar amount of first-cost green building premiums than the percentage differences suggest. Nonetheless, this methodology prevails in similar studies conducted in other sectors (Kats 2003a, 2003b, 2005, 2006; Matthiessen & Morris, 2004; Matthiessen & Morris, 2007).
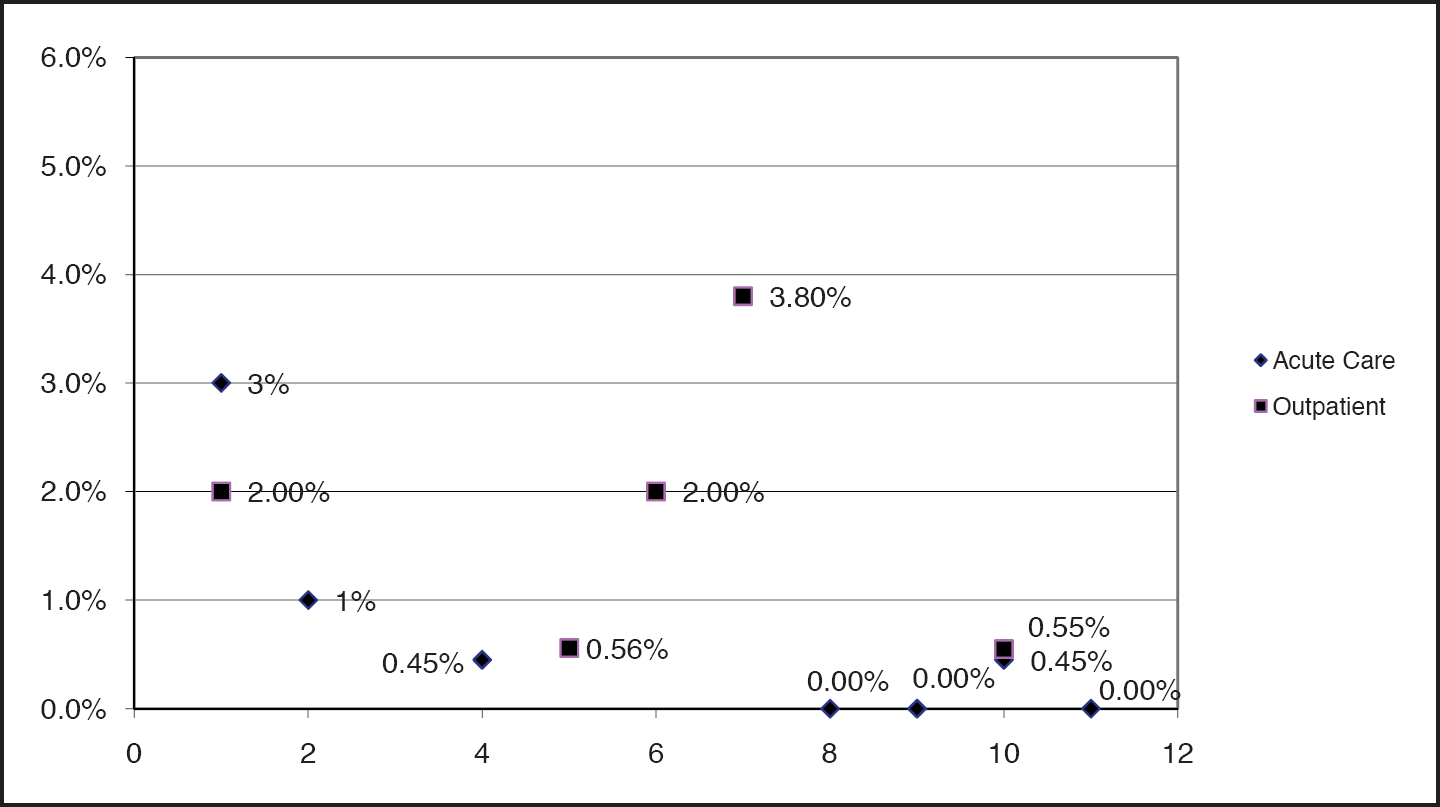
This study reveals variation both in the total amount of first-cost green building premiums identified for each of the 13 projects, as well as the components of the premium. Three of the 13 projects report no first-cost premium after grants and incentives are taken into account; five report premiums of less than 2%; four report premiums in the range of 2–3.8%; and one project, Denver Health Women's and Children's Pavilion, did not calculate a premium (Figures 6A and 6B). Eight projects received utility incentives or dedicated funding that, in each case, was applied to reduce projected premiums. Data in Figures 6A and 7A compare first-cost premiums before the application of funding or incentives. Data in Figures 6B and 7B are based on the net premium numbers, after the application of funding or incentives. Jersey Shore University Medical Center, as of the interview date, predicted that incentives would result in a net savings in construction costs (Michael Pavelsky personal communication, June 30, 2008).
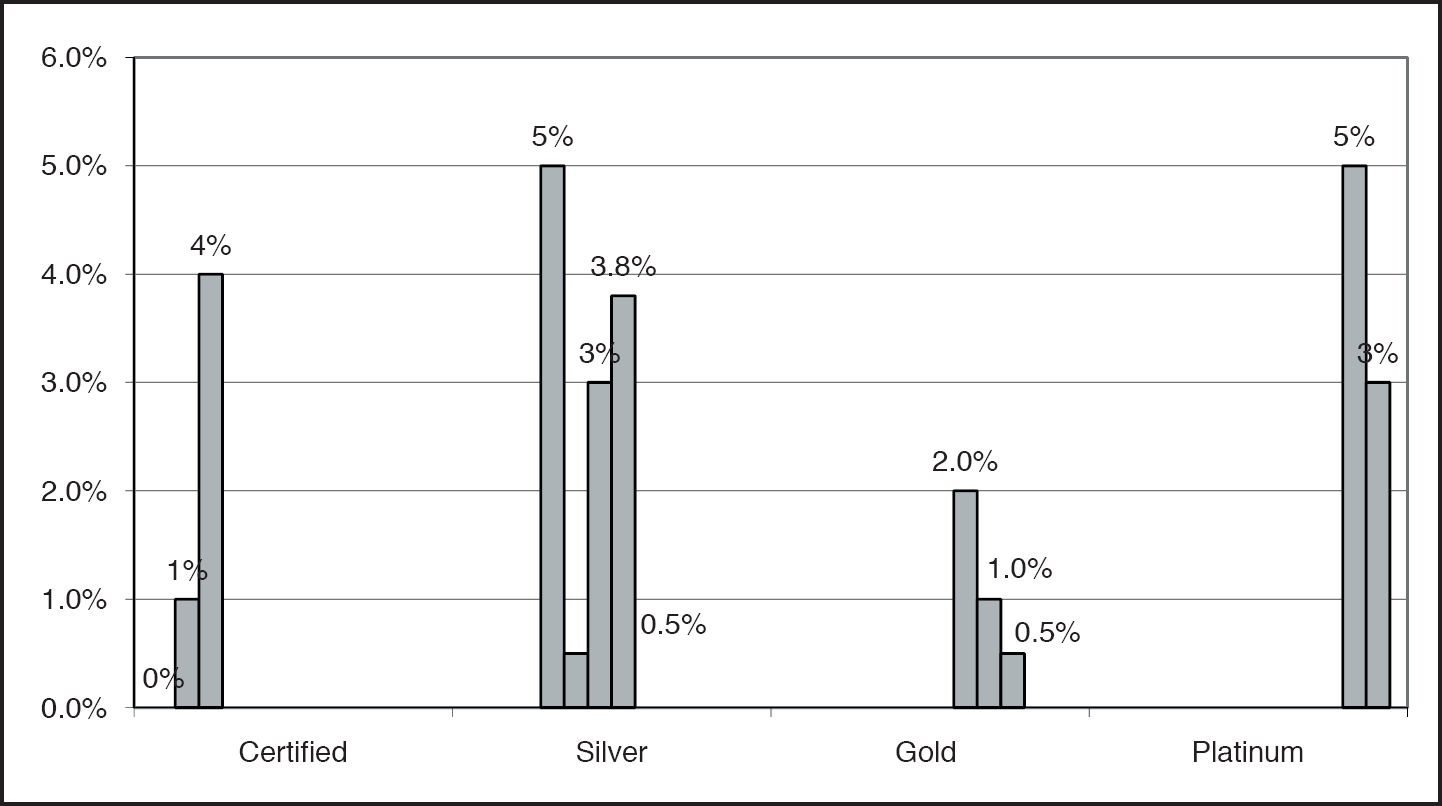
First-cost premiums before incentives by actual or anticipated LEED certification level.
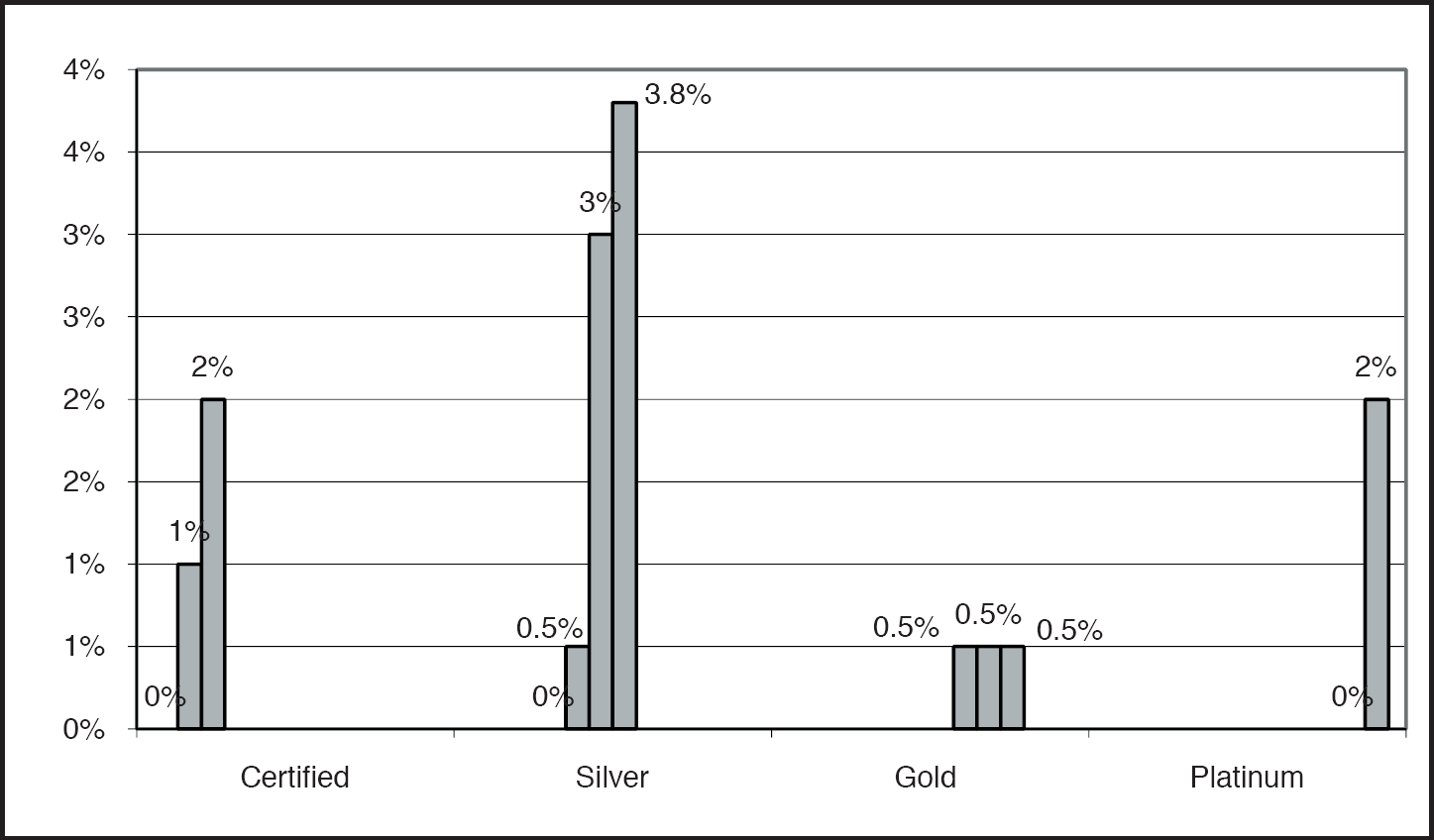
First-cost premiums after incentives by actual or anticipated LEED certification level.
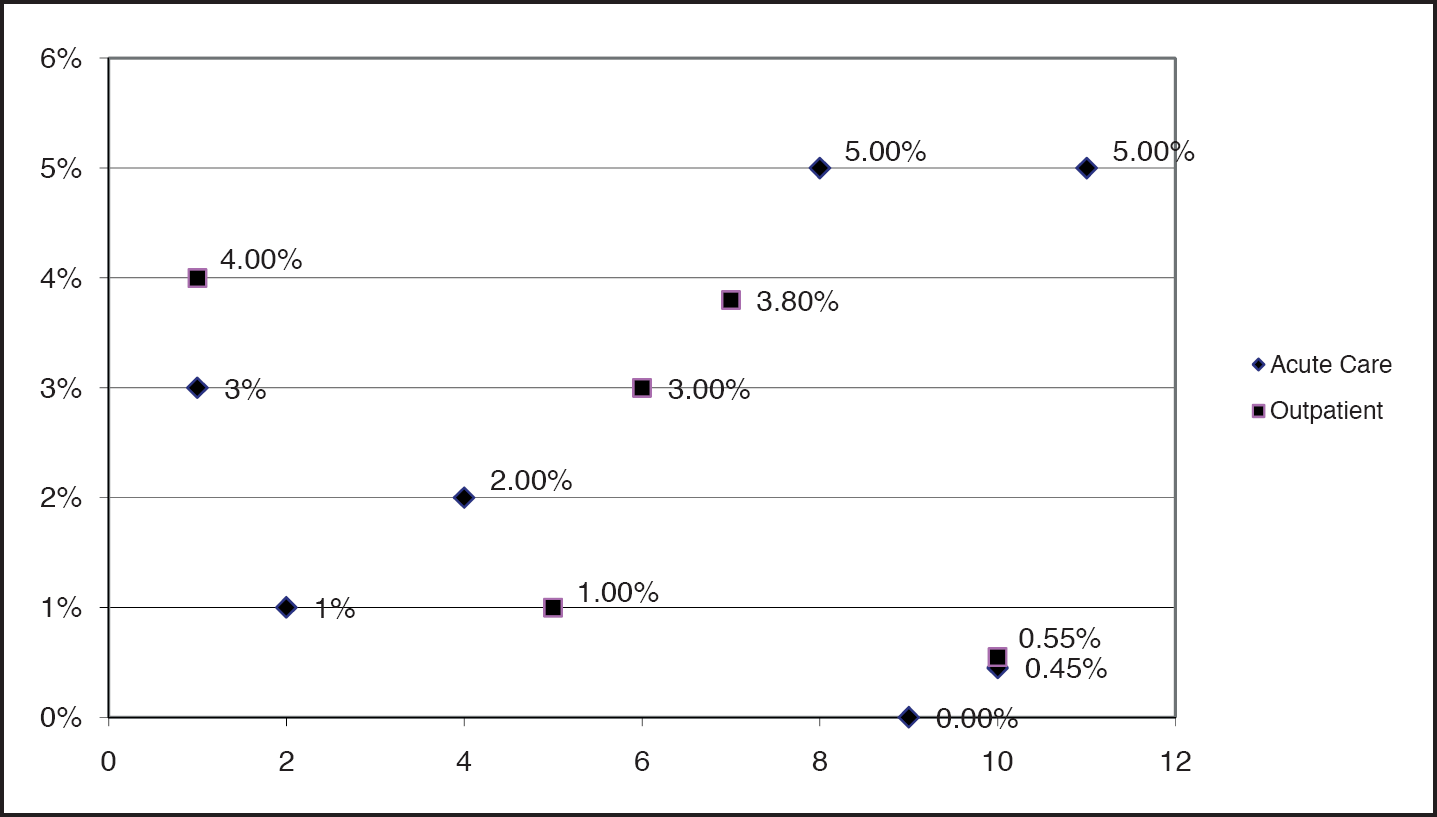
First-cost premiums before incentives by year.
First-cost premiums after incentives by year.
Why did the LEED-Silver projects exhibit the highest first-cost green building premiums? A number of the LEED-Silver certified subject project teams reported relatively late entry into the LEED certification process; they achieved LEED-Silver instead of-Certified by simply adding strategies to the project (and budget). The surveyed LEED-Gold and -Platinum certified projects, on the other hand, entered the LEED process earlier in design, established aspirational goals, and applied astute business strategies to achieve a high certification level at more modest first-cost green building premiums.
Components of the First-Cost Green Building Premium
In the aggregate, the 13 projects demonstrate significant variability in the set of hard and soft cost elements identified as contributing to a project's first-cost green building premium. In summary, the elements isolated by project teams for inclusion in the reported premium derive from the following sources:
Strategies linked to financial incentive programs, ranging from energy efficiency measures that qualify for utility rebates to green roofs and bio-swale installations that garner environmental grants. Some of these strategies would have been incorporated in the project with or without grant funding, but the existence of the incentive placed them in the category of “first-cost green building premium.”
Components that go above and beyond what owners considered to be “baseline” green building practice. The wide variability of these measures supports the idea that this definition is both subjective and a moving target (Green Buildings, 2007; White Paper on Sustainability 2003). These items include green material substitutions that carry first-cost premiums, ranging from flooring to cabinet substrate to certified wood, as well as 100% outside air or enhanced filtration systems.
Measures that carry first-cost premiums but deliver operational savings, ranging from energy efficiency measures such as enhanced control systems and enhanced building envelope components to higher first-cost finishes that require less ongoing maintenance. In general, these enhanced components are compared with a more conventional baseline; only the cost differential between the baseline and the enhanced system is considered part of the first-cost green building premium.
The case study examples that follow demonstrate the range of interpretation regarding elements that are included in the first-cost green building premium; even within this study, projects were inconsistent in the elements included in these calculations. For example, St. Mary's Duluth Clinic adopted a “Healthy Building Vision” to highlight its emphasis on improved human health through green building design (James Brew, personal communication, July 2, 2008). This approach led to including the premium for Forestry Stewardship Council-certified wood, the difference in cost for linoleum in lieu of vinyl composition tile (VCT), and indoor air quality testing as the major contributors to the project's reported 0.5% first-cost premium (St. Mary's calculated a 1% premium before incentives) (James Brew, personal communication, July 2, 2008). In contrast, Denver Health Pavilion for Women and Children included similar strategies within the project baseline and did not isolate them as a first-cost green building premium (Kristi Ennis, personal communication, July 3, 2008).
Project teams indicated that the baseline for green strategies is moving over time—not only are green products moving from premium to standard pricing, but expectations of baseline criteria for building products—or the basis of design—are changing. For example, the earliest subject projects reported first-cost premiums associated with low-volatile organic compound (VOC) materials. Today, such products are routinely incorporated as standard practice (Green Buildings, 2007). Although the urea-formaldehyde-free cabinet substrate specified at Denver Health was not isolated for cost analysis, it was initially identified as an additional cost associated with the LEED certification effort; the contractor began including it in the overall project budget once the decision was made to pursue LEED certification. Kristi Ennis of Boulder Associates, the project sustainability champion and LEED coordinator, reports that it has since become a standard on Denver Health projects (Kristi Ennis, personal communication, July 3, 2008).
Finally, overlapping business decisions can affect how sustainable design measures are accounted for. Dell Children's Medical Center of Central Texas (DCMCCT) is a prime example of the complexity of analyzing these data. DCMCCT prioritized occupant health and safety, leading the project to incorporate low-emitting and healthy flooring finishes to minimize the risk of toxic chemical exposure to its young patients. However, the project team did not report these elements as contributing to the first-cost green building premium. The DCMCCT project also benefited from the savings associated with the combined cooling, heating, and power plant (CCHP), constructed on site by the local utility. The CCHP plant essentially removed $6 million from the project budget that would have been used for central plant infrastructure. In turn, that $6 million was redirected for $2.5 million in energy efficiency measures and $3.5 million in additional green enhancements—culminating in a building with a construction cost equal to a building with on-site plant infrastructure. The project identified additional measures such as exhaust heat recovery, high-performance window glazing, concrete paving (instead of asphalt), high-efficiency lighting and daylighting controls, and electronic air filters as the major elements of its 5% first-cost green building premium before incentives (2% after incentives) (Phil Risner, personal communication, July 10, 2008).
Despite the wide array of elements included in the calculation of first-cost premiums, the range of reported premiums remains modest at 5% or less before financial incentives. However, it is important to understand the level of variability among projects with regard to the role of incentives and calculation methodologies.
The Role of Financial Incentives
Eight of the 13 projects in the data set received grants and/or financial incentives to offset the direct costs of green strategies (Figures 8 and 9). OHSU, a LEED-Platinum certified building, reported the highest amount of financial incentives (Yudelson, 2005). DCMCCT, another LEED-Platinum certified building, also reported receiving a significant financial boost through the CCHP plant partnership with the local municipally owned utility (Phil Risner, personal communication, July 10,2008). Thus the two LEED-Platinum certified buildings both benefited from an aggressive approach to energy management, incentives, and rebate programs. This indicates that a combination of incentive availability and astute business decisions can increase a project's LEED certification level while simultaneously reducing its out-of-pocket first-cost premium by maximizing business opportunities, available grants, and incentives.
This analysis does not recognize the impact of private philanthropy consistently. (Figure 8 categorizes the Center for Discovery Kresge Grant as a green building incentive, but other projects did not necessarily report all philanthropic gifts as impacting their green building premium.) A number of philanthropic foundations now require green buildings as a prerequisite for capital project funding, even for grantees that do not focus explicitly on green building (Jensen, 2008). In fact, the Kresge Foundation (2009) announced in early 2009 that its Green Building Initiative grant program has been so successful in incentivizing green building practices in the nonprofit sector that it will retire the initiative as a stand-alone grant opportunity. Instead, environmental stewardship has been incorporated into the set of nine core values governing all grants awarded by the foundation. Within the subject projects, incentives ranged from a modest $20,000 High-Performance Design Grant from the Colorado Governor's Office of Energy Management and Conservation Rebuild Colorado Program (now of the Colorado Governor's Energy Office) for the Denver Health Pavilion for Women and Children, to $1.6 million for the OHSU Center for Health and Healing from multiple energy efficiency and renewable energy incentive programs.
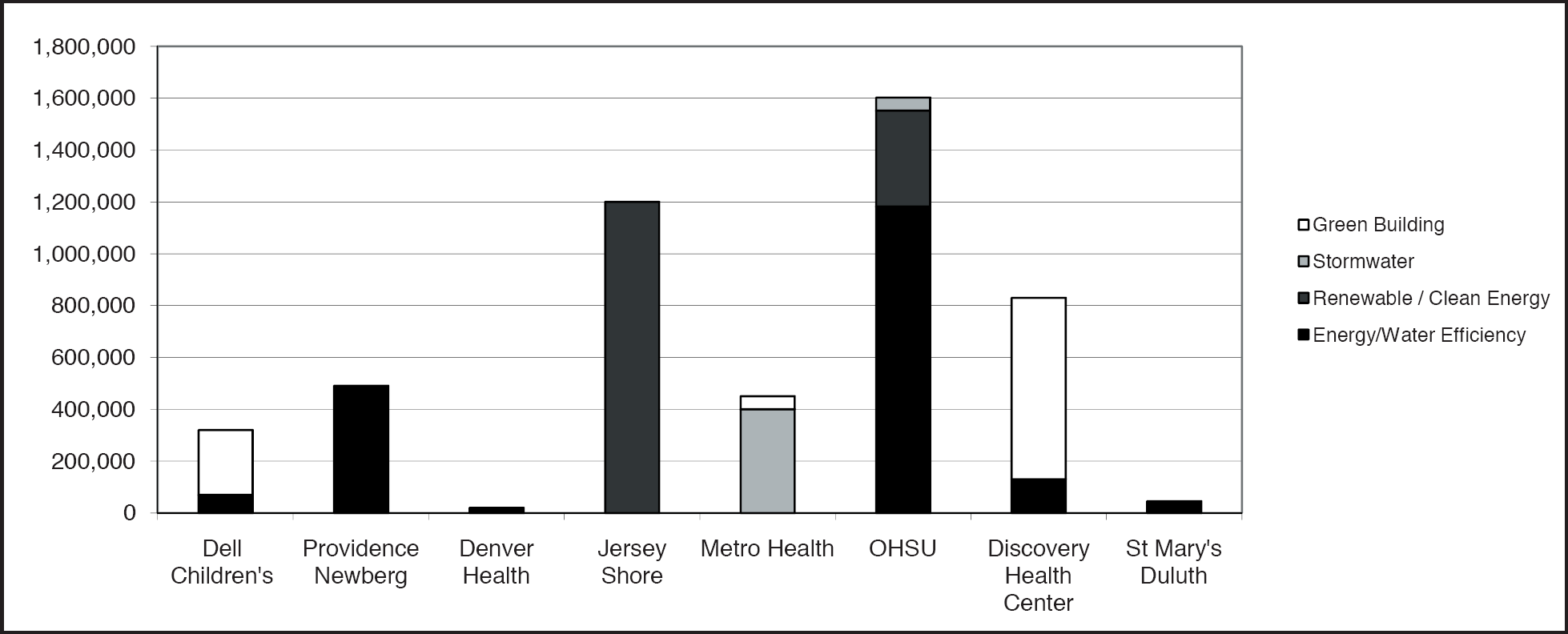
Grants and incentives by category.
For the eight projects that received grants and/or financial incentives, incentive packages often served as a basis for including subject elements as first-cost green building premiums:
Metro Health in Wyoming, MI, identified its green roof and bio-retention swale as the major elements included in the first-cost premium because of the $400,000 Non-Point Source Pollution Grant awarded to the project by the Michigan Department of Environmental Quality (John Ebers, personal communication, July 8, 2008).
OHSU Center for Health and Healing in Portland, OR, also calculated the first-cost premium and payback period for green strategies in relation to grants and incentive programs (Renée Loveland, personal communication, July 7, 2008). The project received over $1.5 million in incentives and tax credits tied almost exclusively to the implementation of energy efficiency, water efficiency, and renewable energy strategies (Yudelson, 2005). OHSU did not ask for a line item cost assessment of premiums associated with other green elements, such as rapidly renewable finish materials. These elements were incorporated into the project as integral to the design goals. However, the project contractor estimates a 1% premium for all green material upgrades (Robert Miller, personal communication, July 2, 2008). Overall, OHSU estimates that grants and incentives reduced its total first-cost green building premium from 3% to 2% (1% associated with energy efficiency, water efficiency, and renewable energy strategies and an estimated 1% associated with green product and material upgrades (Robert Miller, personal communication, July 2, 2008).
Lacks Cancer Center in Grand Rapids, MI, responded to the general green building requirements tied to the philanthropic gift that supplied a substantial portion of the project budget. In particular, the seed funding from local philanthropist Peter Wege that stipulated LEED certification provided both the public support and budgetary flexibility necessary to become the second hospital to achieve that distinction. The holistic approach to designing a green hospital resulted in a calculated first-cost green building premium of less than 1% of total budget.
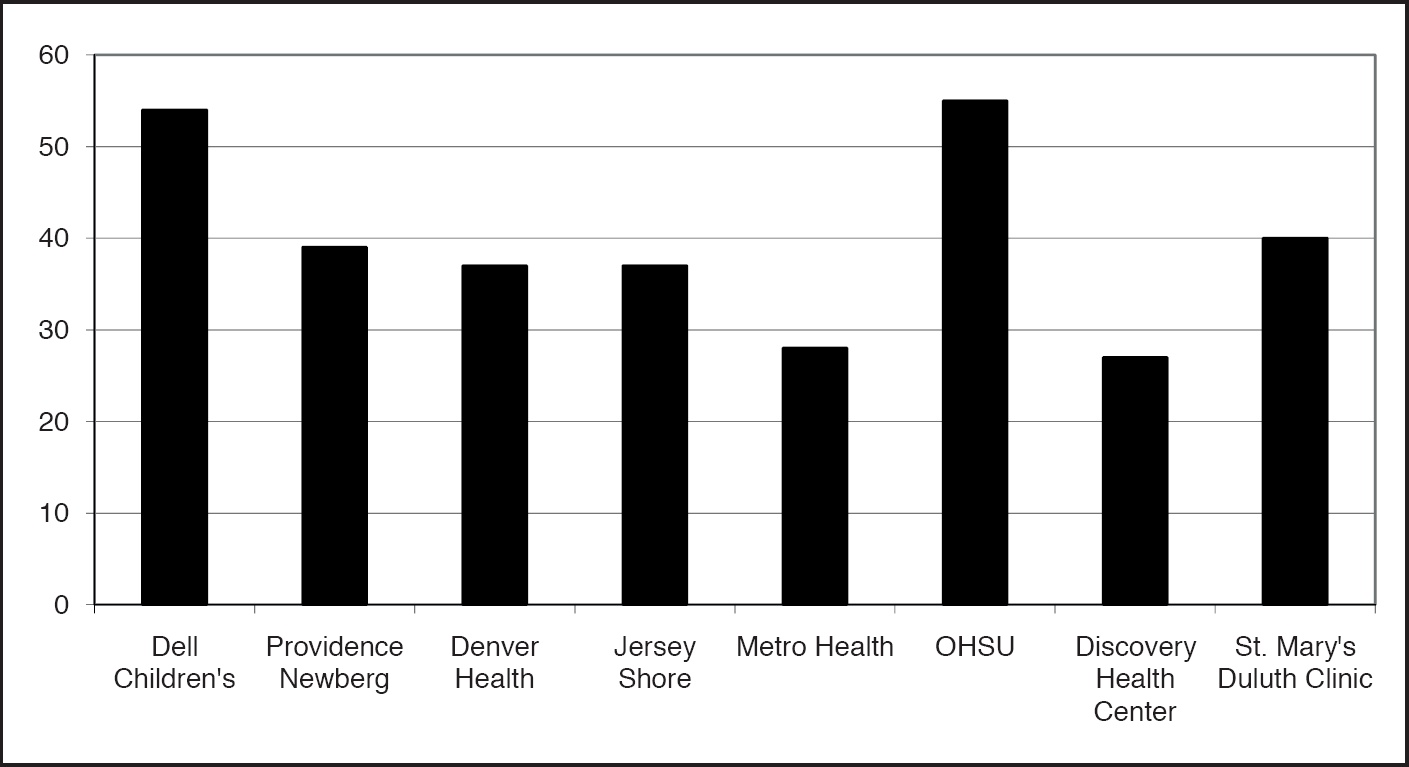
Overall LEED point achievement of projects that received incentives.
First-Cost Green Building Premium Calculation
Another important variable of the first-cost green building premium is the method of calculating capital cost differences. Rarely, if ever, did subject design teams report designing two alternative systems or solutions to perform detailed cost estimates to define the “difference” or “premium” related to the enhanced solution. In most instances, the contractor or construction manager conceptually estimated the relative first-cost premium associated with a green strategy. In summary, the study uncovered little to no detailed documentation to support the calculation of first-cost green building premiums.
At the Center for Discovery in Harris, NY, the methodology for calculating the first-cost implications of an efficient building envelope is summarized by Perkins + Will Associate Principal Peter Syrett:
There were certainly first-cost premiums associated with the envelope, but the owner did not view it that way. There was not a single element that went beyond standard practice and captured their attention or was the topic of cost justification. The building has an exposed wood deck ceiling roof structure with insulation on top of it and metal roofing. I think there was some question about whether the wood decking was a cost premium. But when you subtracted the $5/SF for suspended ceiling systems you did not have to use, the savings more than paid for the roof upgrade. That is the kind of exchange we calculated rather than considering these elements as a green premium. (Peter Syrett, personal communication, July 2, 2008)
In projects with incentives linked to specific energy-conserving technologies, the first-cost green building premium is often carried forward from the grantor's assessment of the difference in construction cost associated with a specific strategy.
The Center for Discovery, for example, estimated the first-cost green building premium associated with ground source heat pumps by using New York State Energy Research and Development Authority cost premium data; the design team did not design a conventional boiler/chiller system for the purpose of comparison (Peter Syrett, personal communication, July 2, 2008).
Aligning the First-Cost Green Building Premium With Project Objectives
The survey of 13 green healthcare projects included a prioritization exercise. Teams were asked to rank six sustainable design objectives in order of importance to their project: (1) occupant health and safety; (2) climate change impacts; (3) mission/leadership: (4) community benefit; (5) public relations; and (6) operational efficiency. Occupant health and safety, operational efficiency, and community benefit emerged as the three highest-priority objectives (Figure 10); however, most survey participants noted that climate change impacts have a higher level of priority in projects that are initiated today. All projects identified green building as aligned with health system priorities and mission. Likewise, the high-priority objectives often influenced the elements included in the first-cost green building premium. An analysis of these priorities reveals that several elements commonly identified in other sectors as specific to green projects are more likely to be incorporated as standard practice if they fall within the owner's overall project goals and objectives. These findings are supported by the Davis Langdon study: “Many projects can achieve sustainable design within their initial budgets, or with very small supplemental funding. This suggests that owners are finding ways to incorporate the elements important to the goals and values of the project, regardless of budget, by making choices and value decisions” (Matthiessen & Morris 2004, p. 25).
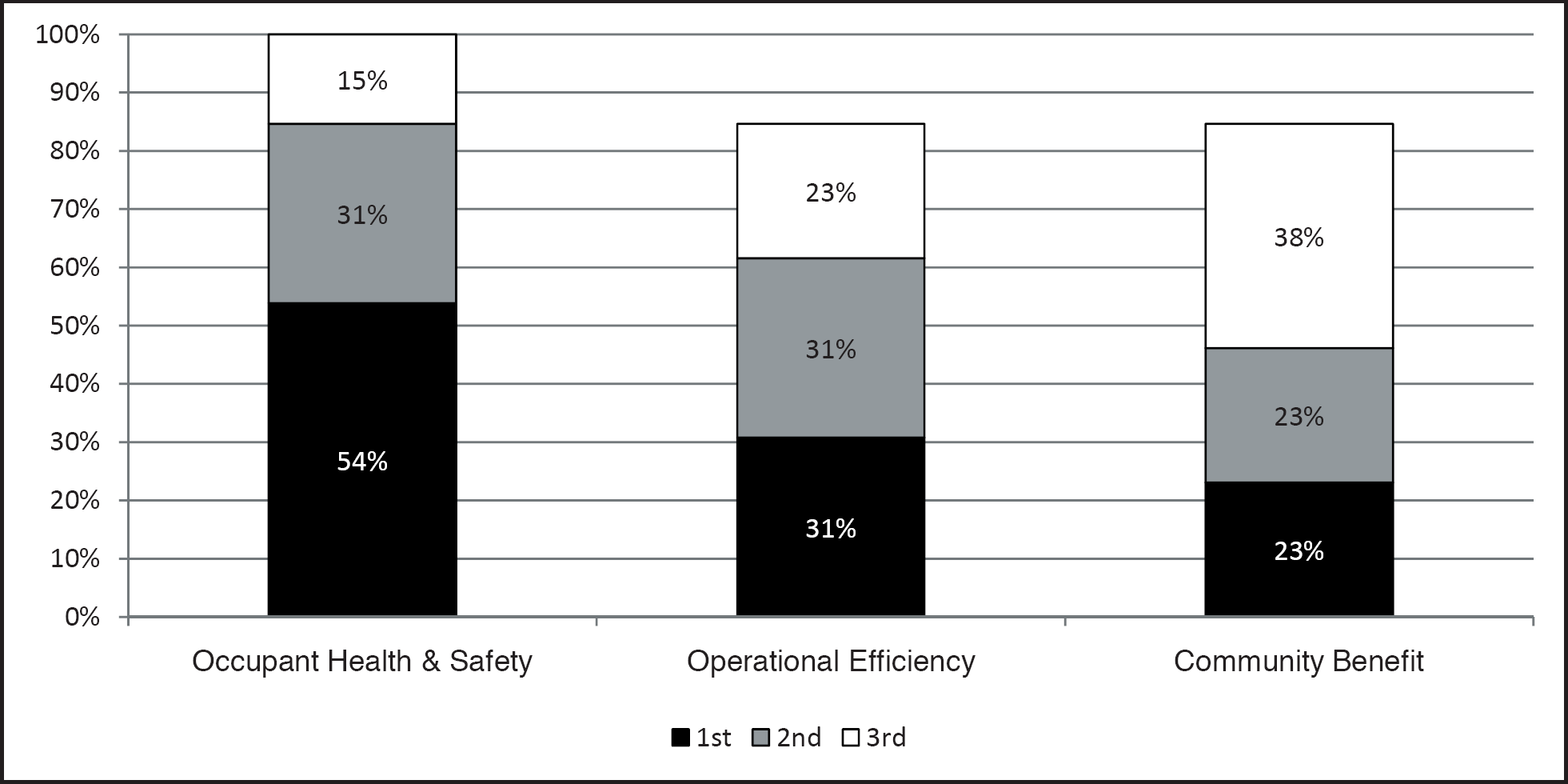
Green building priority objectives.
Occupant Health and Safety
Each project in the data set listed occupant health and safety as its first, second, or third priority (Figure 10). Reflecting the growing trend among healthcare organizations to prioritize strategies that support occupant, community, and global health (Guenther et al., 2006), subject projects that prioritized healthy, healing environments for their patients and staff often identified indoor environmental quality strategies such as low-emitting materials; improved ventilation strategies; persistent, bioaccumulative, and toxic chemical and formaldehyde avoidance; and green cleaning as key elements in the delivery of improved occupant health and safety.
Attributes that are common to green buildings and that promote healthful work environments include the following:
Energy efficiency (lower greenhouse gas emissions)
Much lower source emissions from measures such as better siting (e.g., avoiding locating air intakes next to outlets such as parking garages, avoiding recirculation); better building material source controls (i.e., low VOCs associated with building products); and improved zoning of indoor chemical and pollutant sources (i.e., isolating copiers and sterilizers)
Significantly better lighting quality, including: more daylighting, better daylight harvesting and glare control, greater occupant control of lighting
Generally improved thermal comfort and better ventilation
Commissioning, use of carbon dioxide monitoring, use of measurement and verification to ensure better performance of heating, ventilating, and air conditioning systems (Kats, 2003b)
The Carnegie Mellon University Center for the Built Environment compiled findings from studies correlating improved indoor environmental quality and occupant health. Indoor air quality is associated with asthma, allergies, colds, Sick Building Syndrome, respiratory problems, and headaches. These studies reveal health improvements (i.e., a reduction in the prevalence of symptoms) ranging from 13.5% to 87%, with an average improvement of 41%). In addition to summarizing these studies, Kats determined that four attributes associated with green building design—increased ventilation control, increased temperature control, increased lighting control, and increased daylighting—have been correlated positively and significantly with increased productivity (Kats, 2003b).
The earlier subject projects often included improved indoor environmental quality strategies as components of first-cost green building premiums, while more recent projects tend to consider these elements part of the baseline design. For instance, recognizing the increased vulnerability of children to the effects of exposure to toxic chemicals, DCMCCT prioritized low-emitting and healthy flooring finishes to minimize exposure of their young patients to toxic chemicals (Phil Risner, personal communication, July 10, 2008). This demonstrates how market transformation alters the definition of a “baseline building.”
Two of the study projects illustrate different positions on including healthy materials in the first-cost green building premium versus regarding them as part of the baseline budget.
St. Mary's Duluth Clinic in Duluth, MN, articulated three strategic goals embedded in its “healthy building” vision: (1) Addressing the life-cycle effects of the building design, materials, and systems; (2) tracking the project's level of achievement using nationally recognized guidelines; and (3) avoiding materials and products known to have negative consequences on human health or the environment (James Brew, personal communication, July 2, 2008). “One of the more obvious examples from the list of strategies is avoiding the use of vinyl as much as possible. St. Mary's paid a premium for linoleum over VCT flooring” (James Brew, personal communication, July 2, 2008). These strategies are components of St. Mary's reported first-cost green building premium.
The Center for Discovery in Harris, NY, serves adults and children with severe disabilities. Given the Center's focus on a very vulnerable population, healthy materials and healthy indoor environmental quality quickly became a priority. As architect Peter Syrett explained, “The environmental health issues and material palettes that we incorporated into the design coincided so heavily with their mission that the owner considered healthier materials and green maintenance intrinsic to the design and budget” (Peter Syrett, personal communication, July 2, 2008). Any additional costs related to these substitutions were not included in the reported first-cost green building premiums.
Operational Efficiency—Energy and Water
Subject projects that prioritized operational efficiency (Figure 10) were more likely to incorporate strategies with direct financial payback, such as energy and water efficiency measures. Energy efficiency is generally the first place that building owners—including healthcare executives—look for a measurable return on investment in green building strategies (Green Buildings, 2007; McGraw-Hill Construction, 2007). Collectively, the projects in this data set report a range of projected energy savings from 0–50% among acute-care hospitals, and 15–58% among outpatient and mixed-occupancy facilities (compared to an American Society of Heating, Refrigerating and Air-Conditioning Engineers [ASHRAE)] 90.1 baseline) (Figure 11). Because many jurisdictions exempt healthcare facilities from local energy codes based on ASHRAE 90.1, these facilities may outperform their sector by a higher margin than these projections.
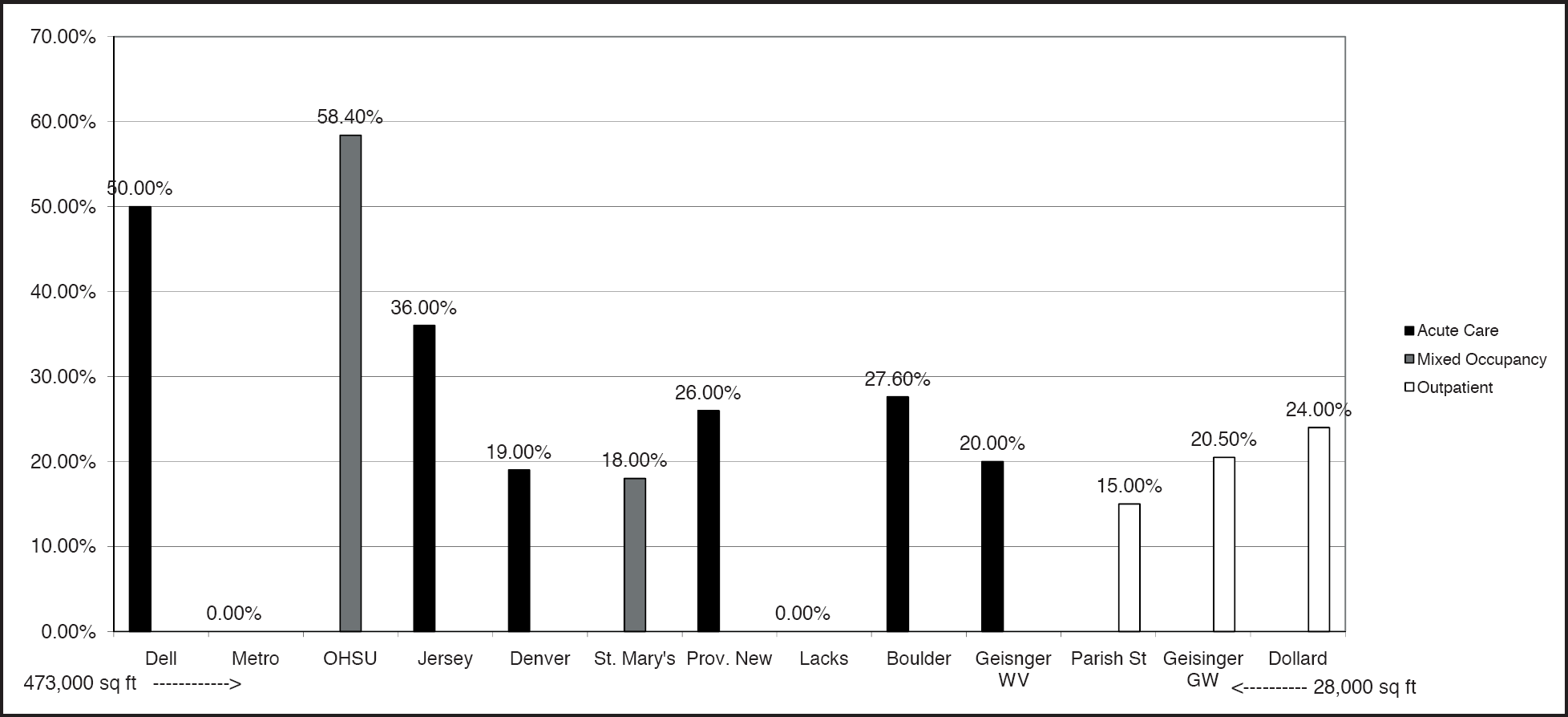
Modeled energy savings of study projects (arranged by size of facility).
In general, the subject projects predicted energy demand reductions of less than 30%. For the most part, projects achieved this by optimizing conventional mechanical system design. DCMCCT in Austin (50%) and OHSU Center for Health and Healing in Portland, OR (58.4%) incorporated CCHP systems, displacement ventilation, and other emerging technologies to achieve even greater reductions (Phil Risner, personal communication, July 10, 2008; Renée Loveland, personal communication, July 7, 2008). Examples of energy reduction strategies include:
Both Geisinger Health System projects in the study demonstrate the proven benefits of energy efficiency measures aimed at optimizing conventional system technologies. Both the acute-care facility and an outpatient facility, when compared to a baseline building, achieved an estimated 20% reduction in energy use through an enhanced thermal envelope, increased insulation, high-performance windows, variable-air-volume ventilation system with optimized air flow during off-peak times, high-efficiency variable-speed chillers in the chiller plant, variable frequency pumps for chilled water, reduced lighting power density (a 15% electrical savings by itself), and high-reflectance roof systems (Bill Gladish, personal communication, July 16, 2008). Geisinger Health System has established as standard practice investment in energy efficiency water efficiency, and commissioning strategies with demonstrated benefits to the health system over time. “We're a cost-driven organization; if we're going to spend money, we're going to spend it wisely on strategies that provide benefits for the people we serve” (Bill Gladish, personal communication, July 16, 2008).
Parrish Healthcare Center at Port St. John in Cocoa, FL, a LEED-Silver certified project, projected a 15% reduction in energy use attributable in part to a 5-year “Guaranteed Performance Agreement” with a mechanical systems consultant. This approach allowed Parrish to use life-cycle cost accounting to achieve system upgrades that otherwise may have been considered too high a first-cost premium (Chris Male, personal communication, July 24, 2008).
Acute-care hospitals, generally designed for long life spans (40–50+ years) (Office of Statewide Health Planning and Development, 2005), are more likely to be owner-occupied than are speculative commercial office buildings (U.S. Department of Energy, 2003). As a result, hospital owners should be receptive to longer payback periods for design elements that reduce energy consumption. However, the projects in this study were divided in their ability to couple additional capital dollars with potential operational savings; some organizations were able to manage this financial model, while others reported difficulty converting operational savings to funding for additional capital. This remains an important and provocative issue that profoundly impacts the ability of the healthcare sector to implement advanced technologies and energy demand reduction strategies. Providence Health and Services, one of the subjects in this study, has developed an intriguing approach to crossing the capital-operations chasm (see case study). Many of the projects in this study used some aspect of life-cycle cost calculation to justify investments in energy efficiency measures:
Boulder Community Foothills Hospital in Boulder, CO, accepted a 12-year estimated payback period for key green design elements such as a remote central utility plant. Because of rising energy prices, however, the hospital estimates that its actual payback period has been significantly shortened (Kristi Ennis, personal communication, July 3, 2008).
Oregon Health and Science University in Portland, OR, challenged its Center for Health and Healing project team to deliver an operationally efficient building at a cost savings. As Renée Loveland of Gerding Edlen Development explains:
When we put out the request for proposal for the mechanical engineering design, we asked to achieve 60% energy efficiency at 25% less first cost. The message was that we were looking for efficiency on a grand scale and we were looking for the engineer to be thoughtful and creative, because we felt it didn't need to cost us more. We actually wanted it to cost us less, and we were convinced that if we integrated things well, over the long term, it would prove to be a better operational strategy. (Renee Loveland, personal communication, July 7, 2008)
Although ultimately the project did not realize the 25% first-cost savings on the mechanical, electrical, plumbing budget (it ended up costing about 10% less), after incentives and accounting for trade-offs from standard design practice, the first-cost green building premium hovered at 1% of the construction cost for mechanical elements.
CASE STUDY
Crossing the Capital-Operations Chasm: Providence Health and Services
Providence Health and Services employs life-cycle costing methodologies to make the case for using operational savings to fund the additional capital necessary to purchase energy conservation technologies. After much experimentation, Richard Beam, the Director of Energy Management Services for the Providence Office of Supply Chain Management, developed this simple graphic to convey the impact of reducing energy consumption on the overall margin of the system (Figure 12). After all, healthcare executives are keenly aware that margin propels mission in the nonprofit healthcare community.
The amount of revenue needed for the same bottom line impact as $50,000 in operating cost savings given the operating margins of different hospitals.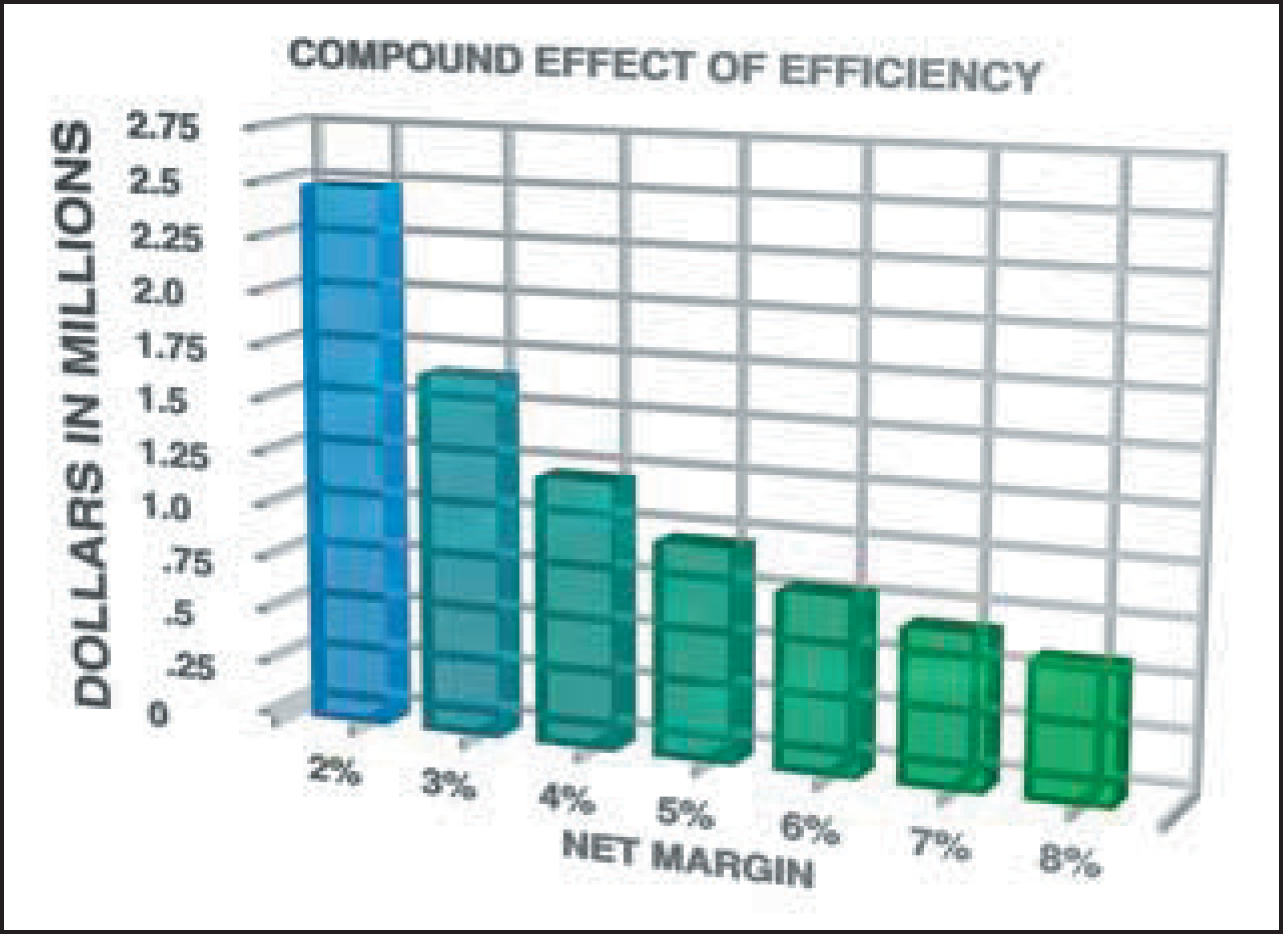
Simply stated, $50,000 of energy savings delivers $50,000 to the bottom line. Figure 12 illustrates the range of healthcare business revenue that must be generated to deliver the same $50,000 revenue to the bottom line. In essence, the lower the net operating margin of a hospital, the more healthcare service delivery revenue is necessary to deliver a given amount to the margin. At a 2% net operating margin, for example, a hospital must deliver nearly $2.5 million in services to return $50,000 to the margin; in contrast, at an 8% net operating margin, $600,000 of revenue is required. By comparing operational savings to the business revenue required to produce it, the value of operational savings becomes more pronounced.
Using this tool and the energy modeling data, Beam projects the dollar savings associated with proposed energy efficiency measures and applies the corporate hurdle rate of 22% return on investment (roughly a 5-year payback). For example, if the energy model projects a $500,000 per year energy savings, it generates approximately $2.3 million in available capital dollars to use for sustainable design measures. Beam explains,
What the corporation is saying is, if you can initiate energy conservation measures that give us a 22% internal rate of return or better, we will fund them. … We can spend dollars for sustainability and efficiency items up to whatever will fit under that 5-year simple payback. (Richard Beam, personal communication, July 2, 2008)
To perform the analysis, Providence created a Business Opportunity Assessment Team to review all capital projects in excess of $5 million for opportunities to realize operational improvement. Once these assessments began, Beam and his team realized that the energy efficiency measures often were financially achievable for less than the additional first-cost budget generated by the 5-year utility savings (particularly with rising energy costs). He asked to be able to tap the additional capital dollars to pay for elements with no easily measurable operational payback. He continues, “So, if the energy elements pay back in 3 years, we can pay for other elements until we've reached that hurdle limit” (Richard Beam, personal communication, July 2, 2008).
For their LEED-Gold certified hospital in Newberg, OR, Providence Health and Services initially accepted a 5-year payback on green strategies. However, the organization was able to reduce the final return on investment to 14 months by securing a variety of state and utility incentives and a pass-through tax credit. Additionally, as Beam explains, “At Providence, there's always a major effort to include as much energy efficiency into a project as we can afford to do. We model our construction design to see what the potential energy conservation measures might be that we could employ to drive our energy costs down” (Richard Beam, personal communication, July 2, 2008).
To calculate the energy savings and evaluate the use of additional capital that could be generated, Providence instituted a standard design practice—the energy eco-charrette. According to Beam:
Anytime we build a project whose value is $5 million or more, it automatically triggers an energy eco-charrette and an energy modeling exercise. We've proven to ourselves that by paying more capital for enhanced energy systems, on a life-cycle cost basis, we create an energy savings value stream of dollars over the operational life of the equipment, or the operational life of the building. However you measure it, that value stream provides a solid return on investment.
To succeed, you need to recognize life-cycle costing as a valid approach, and consider it equivalent to first cost. And so, when you make a decision about whether you're just going to put in code-compliant energy equipment or something better, you need to do a life-cycle cost analysis as part of the energy modeling exercise. That tells us what we can afford to put in the project that'll drive us the maximum amount of operational savings over the life of the building, which is what we try to then implement in the construction plan. (Richard Beam, personal communication, July 2, 2008)
The topic of commissioning produced variable responses with regard to inclusion in first-cost green building premiums. Few if any subject projects included fundamental commissioning in their first-cost green building premiums, indicating that commissioning has become standard practice. Conversely, several design teams identified enhanced commissioning as a premium. For example, Jersey Shore University Medical Center in Neptune, NJ, isolated only portions of enhanced commissioning as a green building first-cost premium (Michael Pavelsky personal communication, June 30, 2008). As Michael Pavelsky, Sustainability Director with the She-ward Partnership, explains,
The owner's baseline requirements for fundamental commissioning were far above the LEED requirements and protocols. Every single variable-air-volume box is tested. Every single connection is tested. It is a 4-month process. So, the contractor had an entire staff in place for the commissioning from the beginning. In addition, we brought in a third party to both oversee all of their activities and serve as the enhanced commissioning representative.
Finally, additional costs associated with renewable-energy or “green power” electrical utility purchases were not universally treated as part of the first-cost green building premium by subject projects. In some instances, projects excluded “green power” purchases from the premium calculation because they viewed it as a contract above and beyond the bricks-and-mortar building. In other instances, particularly where achieving green power-related LEED points elevated projects to a higher LEED certification level, the cost of the green power contract was included in the reported first-cost green building premium calculation.
On-site renewable energy often carries significant capital cost. Its cost, however, was generally included in reported first-cost green building premium calculations unless it was substantially offset by utility incentives or when it was achieved through lease-back arrangements, as demonstrated by the following projects surveyed:
The OHSU Center for Health and Healing in Portland, OR, isolated its 60 kW photovoltaic array as a first-cost premium element that required grants and incentives. The project successfully offset most of the cost of the array by means of the State of Oregon Business Energy Tax Credit, the Oregon Energy Trust, and the sale of renewable energy credits generated by the system. The array, generating 50,000 kWh net per year, comprises building-integrated photovoltaic electric panels mounted in the sunshades located on the south façade of the building. According to developer Gerding Edlin, the sunshades actually save as much energy as the photovoltaic panels produce (Renée Loveland, personal communication, July 7, 2008).
Four years after achieving LEED-Gold certification, Boulder Community Foothills Hospital in Boulder, CO, installed two photovoltaic solar arrays on its medical campus totaling 75.35 kW and offsetting 103,888 kWh of electricity, representing less than 5% of the total annual electricity use of the hospital. By engaging in a power purchase agreement with the solar installer, whereby the installer “rents” space on the roof in exchange for the hospital agreeing to purchase the power generated by the photovoltaic arrays, the premium associated with this installation was negligible (Kristi Ennis, personal communication, July 3, 2008).
Nine of the 13 projects studied achieved 20% or more potable water reduction in fixtures such as sinks and toilets. The OHSU Center for Health and Healing instituted a comprehensive water use reduction strategy, including an in-building membrane bioreactor that treats all gray- and blackwater on site and routes it for reuse in toilet flushing, irrigation, and cooling tower make-up to achieve a reported reduction of more than 50% in total potable water usage (Yudelson, 2005). Although a reduction in domestic water usage (i.e., in fixtures) is laudable, it may not produce as significant a water savings in acute-care healthcare facilities, where roughly 60% of water is used for building processes such as the mechanical system and to cool sterilizer equipment (Massachusetts Water Resources Authority, 1996).
Currently, the most cost-effective large-scale water efficiency strategy is to recycle process water through a closed-loop system and reuse it for limited irrigation and in cooling towers (Massachusetts Water Resources Authority, 1996). Providence Newberg Medical Center in Newberg, OR, achieved a reported 20% reduction in fixture water use compared to a conventional building by installing low-flow fixtures, and an estimated 30% reduction in process water use by means of strategies such as dishwashers that recycle final rinse water as pre-rinse water for the next cycle.
All of the subject projects reduced potable water use for landscape irrigation by at least 50%, with a 100% reduction for all of the outpatient projects.
Metro Health in Wyoming, MI, the only project to include captured rainwater landscape irrigation systems in its reported first-cost green building premium calculation, received a $400,000 Non-Point Source Pollution Grant from the Michigan Department of Environmental Quality to install a vegetated roof, to dredge stormwater retention ponds for irrigation water, to upgrade stormwater controls, and to monitor the effectiveness of stormwater retention ponds in filtering pollutants (John Ebers, personal communication, July 8, 2008). As John Ebers of Metro Health explains, the retention ponds that supply water for irrigation were actually viewed as a cost savings:
The hospital sits on a 170-acre development called the Metro Health Village. One of the things that we looked at early on was putting in rain vaults underneath the hospital for a cost of approximately $575,000. Instead, we constructed two ponds at the entrance of the Village that receive runoff from 50% of the site, paid $45,000 for pumps that provide irrigation water to both the hospital and the rest of existing tenants and future tenants in the Village. … In the deed restriction for the site, all of the buildings have to achieve minimum LEED certification. So this is something they can check off their checklist and say, “Alright, we already have that credit.” (John Ebers, personal communication, July 8, 2008)
Community Benefit
Community benefit is a high priority for many hospitals and health systems that are pursuing LEED certification or green building. To maintain their tax-exempt status, nonprofit healthcare organizations are required to provide community benefit. Although customarily this requirement has been satisfied by providing uncompensated care to the uninsured, hospitals are beginning to emphasize a broader range of community health programs, thereby providing important avenues to strengthen relationships with the surrounding community. Benefits of this approach can include reduced public resistance to campus expansion, expedited project review and approval processes, and opportunities for the philanthropic support of elements such as roof gardens that may be considered difficult to justify in other sectors (Guenther et al., 2006). No project in the study included in its green building premium calculations strategies considered to be community benefits.
Boulder Community Foothills Hospital—the first LEED-certified acute-care hospital—chose to pursue LEED certification as an expression of community stewardship. Although the hospital had a strong environmental track record before the new facility, achieving LEED certification provided an opportunity to spur market transformation in the healthcare sector. Kristi Ennis of Boulder Associates notes,
They opted for a green project because they believed that was the next logical step for them, considering their environmental track record. They have been a member of the community for over 100 years, and they believed that a green building would continue their status as a good citizen. (Kristi Ennis, personal communication, July 3, 2008)
The Lacks Cancer Center in Grand Rapids, MI, committed to a green building from the inception of the project in response to community expectations. As Robert Miller of HKS Architects explains,
Western Michigan is a hotbed of green development. Steelcase and Herman Miller both have built significant green structures. … and the community has recognized sustainable building as being the right thing to do. (Robert Miller, personal communication, July 2, 2008)
Located on a tight site surrounded by a residential area, a school, and a 50-unit senior housing facility, Jersey Shore University Medical Center in Neptune, NJ, prioritized building massing, orientation, and site elements as benefits for the surrounding community. Consistent with the survey direction, the mitigation costs for the brownfield site were excluded from the reported first-cost green building premium because they were identified as a condition of the site, not as sustainability goals (Michael Pavelsky personal communication, June 30, 2008).
Parrish Healthcare Center at Port St. John in Cocoa, FL, expanded habitat for a native endangered species, the scrub jay, by protecting a 6.2-acre swath of the project site with a federal easement awarded by the U.S. Department of the Interior. The easement prohibits development on the protected land in perpetuity. On-site retention ponds further enhance the site's natural habitat by means of low-impact stormwater mitigation measures and native and adaptive plantings cared for by a local environmental scientist sensitive to the needs of local wildlife. (Chris Male, personal communication, 2008)
These project examples did not include the costs associated with the LEED registration and certification processes in their reported first-cost green building premiums, but other project teams did. DCMCCT, Denver Health Pavilion for Women and Children, Metro Health, and the Center for Discovery received (or anticipate receiving) grants or incentives tied to achieving LEED certification that were applied to reduce project registration and certification fees. The USGBC, for example, refunds certification fees for projects that achieve LEED-Platinum certification (USGBC, 2009), and a number of private foundations and utility rebate programs boost grant amounts for LEED-certified projects (Jensen, 2008; Kresge Foundation, 2009; USGBC, 2009). In most cases, the grants cover soft costs such as registration, eco-charrettes, the integrated design process, energy modeling, and commissioning.
Related Operational Benefits
Research suggests a correlation between green healthcare design and reduced patient length of stay, a reduced medical error rate, improved staff retention, and competitive advantage (as measured by patient satisfaction surveys) (Ulrich et al., 2008). A growing body of evidence-based research has begun to identify specific sustainable design decisions as contributing to these health and financial outcome indicators. For example, data such as staff turnover rates, average length of patient stay, patient satisfaction surveys, medical error rates, and workplace injury reports are routinely tracked and can be correlated with financial performance. For example, research has consistently shown that daylighting and access to views of nature provide beneficial effects for patients and staff. Patients with views of nature have been shown to heal faster and use less pain medication than patients looking out at an uninspiring view such as a brick wall (Beauchemin & Hays, 1996; Ulrich, 1984; Walch et al., 2005).
These benefits translate directly to the bottom line of a healthcare facility through increased market share, the avoidance of liability, and the costs associated with staff turnover, including recruitment and training. More than 20 healthcare providers in the United States are currently gathering data on the health benefits of green building strategies through evidence-based research programs, in particular The Center for Health Design's Pebble Project® (Center for Health Design, 2009).
Many benefits of green building, such as energy and water efficiency savings, are realized only after a facility is operational. Study participants reported that strong ties between the design team and the facility operations team increase the likelihood that the desired benefits will meet or exceed expectation. Green healthcare projects benefit from integrating operational priorities advanced by the facility's “green team” during the integrated design process. Additionally, projects can pilot design initiatives and green cleaning and maintenance programs in existing buildings before breaking ground on a new facility (Guenther & Vittori, 2008).
Several projects in this study are tracking operational benefits to build a body of evidence linking green building strategies to both financial and performance improvements:
Geisinger Health System identified the operational savings associated with LEED projects as its primary motivation for pursuing LEED certification. Brian Toevs with 7group explained,
Geisinger's asking for [green design elements] because they know they work, and they know they're saving money. So the strategies that Geisinger has incorporated into these projects are because they work and because they save money, and, oh, by the way, they also are very helpful towards the LEED process. (Brian Toevs, personal communication, 2008)
Providence Health and Services retained the University of California Berkeley Center for the Environment to conduct a post-occupancy evaluation of the LEED-Gold certified project in 2008, 2 years after opening its doors. As Richard Beam of Providence Health explains,
The report's findings provide hard evidence that the Newberg LEED-Gold building is the new standard for healthcare operations. … It's telling us that all these things we hoped would happen—that we would have higher employee satisfaction, higher patient satisfaction, better retention of clinical employees and nurses, better physician recruitment—have scored higher due to the nature of this building.
Conclusion
As evidenced by this survey study, the question of first-cost green building premiums in healthcare is complex and challenging and deserves continued study and tracking. The complexity of the undertaking resists simple categorization and conclusions. The data in this study corroborate the findings of earlier, well-regarded industry business case efforts (Kats, 2003a; Kats, 2003b; Kats, 2005; Kats, 2006; Matthiessen & Morris, 2004), with the exception of predicting increased first-costs related to the level of LEED certification.
Many of the healthcare organizations in this study did not decide to pursue green building based on financial calculations; instead they were motivated by the values of leadership and community benefit. However, one healthcare-specific lesson learned stood out in reports from the vast majority of projects: the more emphasis an owner placed on the connection between the benefits of green building and occupant health and safety, the more sustainable building elements were integrated into the project as basic building features.
First-cost green building premiums appear to be lower than industry expectations (Green Buildings, 2007; McGraw-Hill, 2007) and may be decreasing over time. Certainly, study projects demonstrated that green elements previously viewed as above-standard are being incorporated into projects as a new baseline definition of best practice healthcare construction.
Ultimately, however, the topic of first-cost green building premiums, although useful for comparing industry data, presents a one-dimensional view of a complex, multilayered topic. Kristi Ennis of Boulder Associates explained that the integrated design process for Boulder Community Foothills Hospital disregards any attempt to calculate a first-cost premium specific to green design elements: “Because of the integrative design process, elements of the project were incorporated if they met several criteria: they might be green, but they were also low maintenance or met criteria for infection control, etc.” (personal communication, 2008). Peter Syrett of Perkins + Will, referencing the Center for Discovery in Harris, NY, agrees:
The concept of a first-cost premium inherently presents an item as a premium when it isn't necessarily an add to the budget—and in a process where we are not asked to analyze the subtractions. If orienting a building to optimize passive solar gain in winter reduces heating load with no impact on construction cost, where is that “savings” tracked? (Peter Syrett, personal communication, 2008)
Clearly, the work ahead is to develop a more comprehensive model for tracking cost and savings using an integrative design model. As this model emerges, it will be necessary to continue to reference the healthcare sector's triple-bottom line values and their commitment to occupant health and safety, operational efficiency, and community benefit (Guenther, et al., 2006). The healthcare sector deserves no less in a continuing analysis of this topic.
Footnotes
Acknowledgments
The authors would like to acknowledge the assistance of Breeze Glazer, Perkins + Will, New York, and Rachel Dewane, CMPBS, Austin, TX, in the development of the graphics and interviews. Portions of survey data (Figures 6, 7, and ![]() ) are reprinted here with permission of Greg Kats and Island Press. The Health Care Without Harm Research Collaborative sponsored this research, with funding provided through the Kresge Foundation and Merck Family Fund.
) are reprinted here with permission of Greg Kats and Island Press. The Health Care Without Harm Research Collaborative sponsored this research, with funding provided through the Kresge Foundation and Merck Family Fund.