
Abstract

Implementing evidence-based design (EBD) may be desirable and—arguably—even necessary, but is it affordable? I would like to bring to your readers' attention exciting new research findings on ways to reduce the first cost of better-quality design.
During the HealthCare Design ′09 conference held in Orlando, Florida, from October 31—November 3, the question of affordability sat squarely at the fore. A larger-than-usual number of session leaders and panelists addressed the apprehension and financial uncertainty that healthcare decision makers are now facing. The Baby Boom generation is retiring; how will we afford to pay for their—and our—basic healthcare needs, let alone the design recommendations being made by the EBD community of researchers?
It has been suggested that EBD pays for itself, thanks to reductions in medical errors and patient falls, and increases in staff retention and philanthropy, among other metrics. These claims are not without support; the EBD community has begun estimating the benefits and costs associated with EBD implementation, basing its figures on observations from Pebble Project® case studies. The now well-known Berry et al. (2004) article entitled “The Business Case for Better Buildings” suggests that EBD interventions not only pay for themselves within 1–3 years, they offer the potential for long-term cost savings once the payback period has been attained. This line of reasoning falls into a research territory called life cycle cost analysis. It is the argument made by the environmentally sustainable design community as well. The message of life cycle cost analysis researchers is this: scrimping and saving is good to a point, but when an inferior environment is created, a false economy may ensue. The EBD community argues that spending a bit more for better quality up front can lead to long-term cost benefits.
It is difficult to find fault with such an argument. In fact, the question is not so much whether or not EBD interventions make long-term financial sense (they almost certainly do—at least in some areas), but whether or not a conscientious owner can afford the first-cost premium sometimes associated with a better-quality building. Owners fear that the answer is “no.”
Interestingly, those who wish to develop environmentally sustainable buildings face similar concerns. Yet first-cost data on U.S. Green Building Council LEED®-certified buildings suggest something surprising. Matthiessen and Morris (2004) of Davis Langdon compiled first-cost values from 138 non-LEED- and LEED-certified buildings; they found there was no statistically significant cost difference between the two. This begs the question: if the material value of LEED buildings is higher than that of non-LEED buildings, how can there be little difference in cost?
There is mounting evidence that first cost can be substantially affected by the type of delivery process used. In fact, the authors of the Davis Langdon report (Matthiessen & Morris, 2004) suggest that, unlike costly LEED buildings, the least expensive LEED-certified buildings incorporate environmentally sustainable design features early in the delivery process, ensuring that sustainability is embedded in the building fabric early on, when its influence is greatest and the cost to incorporate it changes least. This logic is suggested by the MacLeamy Curve (Figure 1). The graph makes intuitive sense if the reader compares the cost of deciding to include single-patient rooms or a south-facing building early during concept design instead of during design development. The implication of the curve is that shifting the involvement of architecture, engineering, and construction (AEC) consultants from the traditional, temporally linear route to a collective, integrated, large-meeting format ensures that the early stages of design are maximally informed.
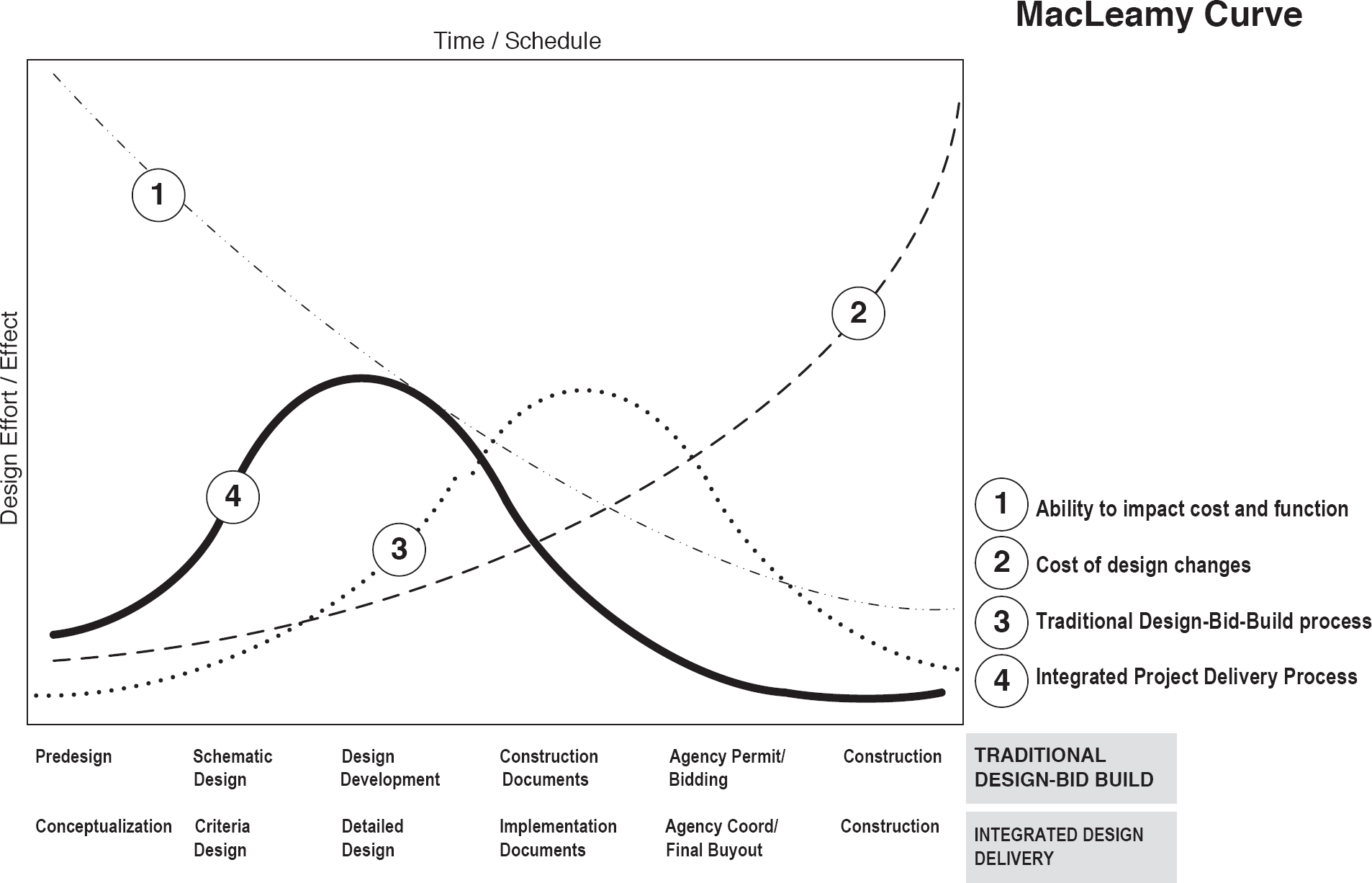
The MacLeamy Curve.
To emphasize, the way a building is designed can significantly influence first cost. By way of illustration, think of an architect who specifies for a building low-e glass, which blocks infrared rays from entering windows and heating the building. In a traditional design-bid-build process, a cost premium would be associated with the low-e glass. However, if the AEC team is present during early design, the mechanical engineer might discover that, because low-e glass is included, he or she can down-size the chiller and shrink overhead duct sizes. If a structural engineer is also present during early design, he or she can lower the floor-to-floor heights, as appropriate, to accommodate the adjusted, smaller duct sizes. Had the building been developed using a traditional, linear design-bid-build process, the addition of low-e glass would likely have added a first-cost premium to the building (Barnett, 2004). By contrast, thanks to integrated design, waste is removed from the building process during design, enabling the addition of value for the same price.
Target Value Design and Lean Construction
Early AEC-team design collaboration on a project is only one part of the cost reduction puzzle, however. The Lean Construction Institute, founded by Gregg Howell and Glenn Ballard in August 1997, works with industry to identify opportunities for waste removal and value addition during the construction process. Lean construction is an application of the Toyota Production System's Lean Production; its pioneers apply the Lean mantra of kaizen—or continuous improvement—to transform a low-value “fat” project into a high value “lean” one, as diagrammed in Figure 2. The PDCA cycle is an acronym for Plan-Do-Check-Act—the processes used during continuous improvement. The PDCA cycle really represents the scientific process: a modification is proposed (plan) and implemented (do); measurement data are recorded and assessed (check); and the change is either adopted or rejected (act) based on whether the proposed change actually reduced waste and added value.
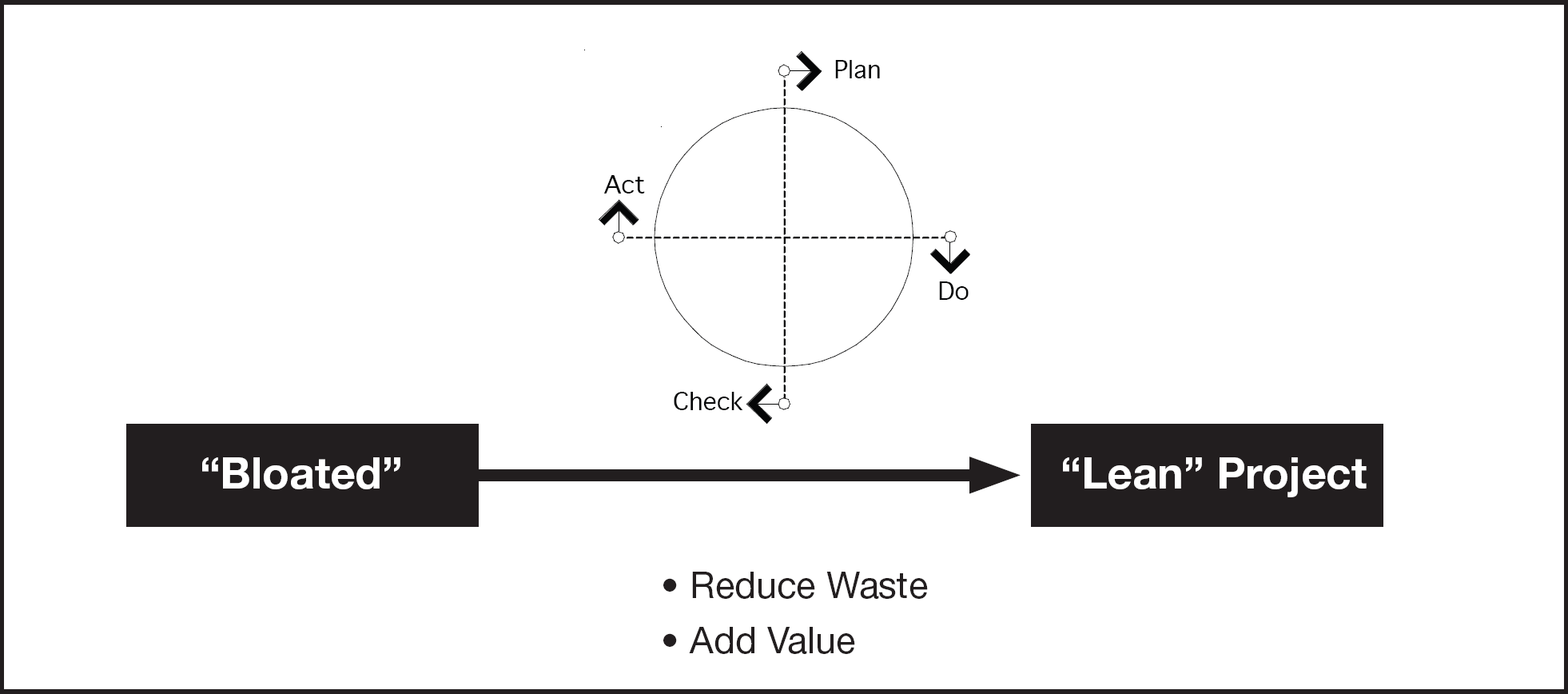
Lean construction process and objective.
Lean construction shares some similarities with the Lean supply chain, such as the preference for pull processes, just-in-time delivery, one-piece flow, low inventory, and low variability. An explanation of each of these concepts—and the proof of their effectiveness—lies beyond the scope of this letter, but suffice it to say, Lean thinking is developing a rapidly increasing following because it works.
Lean consultants introduce Lean thinking by asking employees to engage in a 3-minute assembly activity called the Airplane Game. In this game, players assemble a Lego airplane, first using the old way, and then again using the Lean way. Collected metrics, such as time-to-first-plane, work-in-progress, and the total number of assembled planes convincingly demonstrate to players that a Lean pull system, low-batch-size process results in less waste and greater value than a business-as-usual push process. We verified this finding using a computer simulation and discovered that it aligned with the results of actually playing the game (Rybkowski, Wong, Ballard, & Tommelein, 2008).
Target Value Design (TVD) is a subprocess of Lean thinking that challenges the integrated team to address financial constraints collectively and creatively by reducing waste and adding value. An application of target costing, TVD begins with the price an owner is able and willing to pay for a facility (the allowable cost) and works with an integrated team to systematically design to this price. It is critical that the entire project be cancelled if the allowable cost cannot be met, because such a project would not be financially viable. This is different from a traditional design-bid-build process that begins with a design and then sets a price; this price is usually too high for many facility owners and leads to unfortunate cost-cutting measures that can hurt the functional capabilities of the facility. By contrast, with TVD, an experienced estimator continually revises the project price as waste is incrementally removed and value added to the project design over time. An especially successful TVD exercise may result in surpassing the allowable cost to design to an even lower target cost. Imagine an EBD-quality design emerging even as cost continues to drop over time.
Lean construction practices such as TVD represent more than theoretical musings. They have been and continue to be tested using the PDCA cycle on case study projects. In fact, results from a 912,000-square-foot acute care women's and children's medical facility in San Francisco suggest that TVD can help a project reduce its first-cost per square foot to 15–20% below market cost (Figure 3).
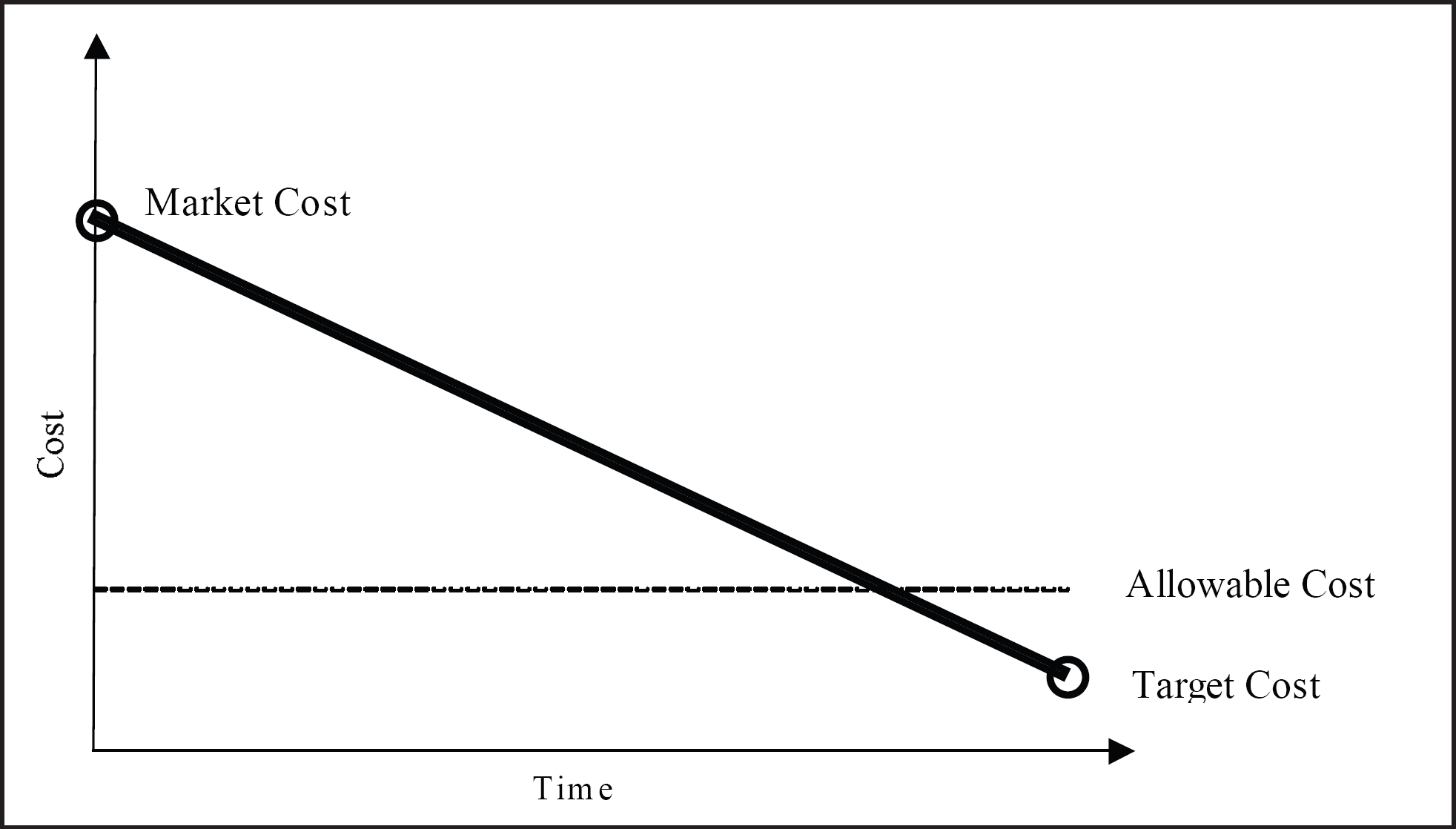
Estimated project costs over the course of TVD meetings.
These are exciting findings, because they suggest that TVD is the type of process that can cause the first-cost premium associated with EBD to partially or completely disappear. They mean that, contrary to some fears, the enhanced value demanded of EBD interventions can be financially feasible.
Lean Construction is a label that appears more frequently these days, and it has demonstrated significant benefit in the California healthcare market. The concept is popping up across the country and is proving to be valuable on projects large and small. Why would a hospital owner want to consider Lean construction methodologies?
Predictability: the single biggest concern in a construction project is to be able to count the costs before building. Business feasibility and funding decisions typically must be made long before a project is fully defined. Without a framework for this definition, the needs and wants of many different constituents will drive program requirements—and thus the cost of the program—well beyond the original concept. In a traditional delivery methodology, designers interact with users to define the size and nature of the space, make materials decisions, and unilaterally establish quality levels and make maintainability decisions with limited regard for the detailed costs associated with each decision. Often these decisions are made in individual silos without regard for their impact on the overall program. On bid day or when a contracting partner is engaged, many of these decisions come to light and the owner must face the fact that they add up to much more than anticipated. The owner is left with the decision either to spend the extra money, which might significantly change the business equation, or to value engineer systems, adding rework costs, schedule delays, and the perception of a downgraded program.
One Lean method called target value design calls for a team approach in which builders and designers work together from the beginning of concept development. Having the builders at the table with the designers allows the team to start with a detailed cost estimate of what it will take to deliver the project. Each decision can then be measured against this estimated benchmark. If a decision is made to spend more money on one line item, it has to be taken from another.
An engaged owner will participate in this process and help facilitate these decisions based on organizational values. This means that the owner drives the value decision-making process, has a far better understanding of the end product, can manage expectations during the process, and is continually aware of the cost of the program. This methodology requires many things from an owner. First, the owner must be willing to dedicate the time and energy to participate in the process and make decisions in a timely manner. There are many decisions to make, most of which can affect cost. Second, the owner must create a team atmosphere of trust and reliability. All parties must be willing to share openly the cost data, their mutual needs, and their ignorance of certain aspects of the program. Parties must also make reliable commitments to each other and live up to those commitments willingly. To effect this process, an owner must choose his partners carefully, trust that they understand the project goals, encourage the team to seek project value over individual benefit, and empower team members to openly challenge any and all preconceived rules or concepts derived from previous experience. By means of this collaborative team process, owners can expect to adhere to predicted program costs, have a strong understanding of the product to be delivered, understand the value of each building system, and learn a significant amount about the Lean process and all partners.
In 1997, the Governing Board of Intermountain Healthcare (IHC) approved a major capital program of $1.3 billion to improve and enhance the healthcare environments and safety of all of their major hospital facilities. Over the past 12 years, 10 hospitals were either replaced or significantly remodeled, and three new hospitals were constructed in new service areas. While planning a system effort of this proportion, it was recognized and understood that a mechanism for value optimization and facility environmental evaluation would have to be created and integrated into the project development process and culture. Knowing this was necessary, many “value assessment” steps were created and instituted in the planning and design process.
Although the work had been carefully planned, as with most major capital projects, our conceptual cost estimates for each respective project rarely—if ever—were adequate to cover the scope of work. We knew that as planning and design progressed on each project, a great deal of team interface time and creative energy would be expended. We knew from past experience that the local project teams would feel vested and take intense ownership of their design solutions. We also anticipated that the mindset of the physicians and other healthcare professionals who had participated in this design process would be, “We have finished the plan; so when do we move in and begin treating patients?”
In past projects, we had experienced the frustration and disappointment of these dedicated local teams—especially the physicians—when project cost estimates, which were based on completed design development drawings, almost always exceeded the conceptual budget. At this point, without exception, the project development process was discontinued or sidetracked, and doubt about the project and a lack of direction crept into the team process. Pressure mounted from various internal and external sources to proceed with the design and to keep the project on schedule. Administration and other vested parties often began to suggest random cost-cutting ideas and alternatives in an attempt to solve the budget problem as quickly as possible. Some began to question all of the prior assumptions and solutions used by the design team, and old ideas that had been discarded began to return to the process.
Unfortunately, these random ideas often were not studied and well thought out. They had the potential to lead to compromises in work environments, produce barriers to operational performance, eliminate life-cycle cost advantages, and even affect clinical process efficiency. In some projects, even the vision and mission of the project were forgotten for the sake of finding a budget solution. These unfortunate, random cost-cutting ideas were often introduced in the name of “value engineering.” Because of their service orientation, even design and engineering professionals, along with the construction management team, would begin to respond to random cost-cutting requests from the owner and other users. They began to perform isolated cost-reduction evaluations on ideas and concepts suggested by the owner and the team.
In anticipation of these events occurring in a multiproject capital program, many value assessment steps were created and implemented in the planning process. Perhaps the most effective and impactful value optimization step was the inclusion of a value-engineering workshop at the conclusion of the design development phase of the project.
This interdisciplinary design review workshop was organized and conducted by the system's central office, the Facility Planning and Development Department. From the beginning of the project, a placeholder for this 2- or 3-day workshop and the 2- or 3-week follow-up period was formally written into the schedule. All team members, including the physicians and other healthcare professionals, were instructed in advance regarding the content and format of this planned value engineering development step. The workshop model was incorporated into the culture of the project development process and all project team members were instructed in the goals and possible outcomes of this event. The goals of the IHC value-engineering workshop included the following:
Obtain optimum value for every dollar spent.
Provide alternative design solutions that result in initial and long-term value without reducing clinical and service functionality and safety.
Enhance operational performance and the human experience.
Maintain the concept of life-cycle cost in the evaluation of alternatives.
Value engineering begins with the discipline to ask a set of simple questions regarding any suggested change to a project. These questions may include: What is it? What does it do? What must it do? What does it cost? What other material or method could be used? What is the alternative cost?
These questions are used as the core of a study process that will evaluate and attempt to further optimize the plans and specifications of a project at the point of design development. The study will bring into question all of the prior assumptions and solutions used by the original design and engineering team.
Methodology
The workshop utilizes the concept of a peer review mechanism, using a “Cold Team” and a “Hot Team” to analyze and optimize the project plans and specifications. A Cold Team of professionals is approved, selected, and prepared for the workshop. The Cold Team consists of two to four members in each of the following disciplines: administrative, design, engineering, and construction management. The administrative Cold Team members usually consist of hospital executives from two other hospitals in the IHC system. The other Cold Team members, including architectural, engineering, and construction management professionals, are principals in their respective firms. The firms selected must be located in a state other than the one in which the project is located. These principals must not have been involved in the project previously in any way and have not seen the design development drawings.
The Cold Team participants not employed by IHC are paid a per diem consulting stipend plus expenses. We have found that principals from other firms are enthusiastic about participating for the experience and the learning process that occur. As preparation for their role in the workshop, each member of the Cold Team is sent a complete design development set to study 2 to 3 weeks prior to the workshop.
The Hot Team consists of similar professionals who have developed the project, including all of its concepts, assumptions, plans, and specifications. The Hot Team usually is paid only expenses; their compensation for workshop time is included in their initial design fee.
The workshop is structured using seven study groups, one for each professional discipline involved. Each study group includes members of the Cold Team and Hot Team with similar specialty training. Various representatives of the owner, including hospital department leaders, physicians, and clinical users, are also invited to meet with each of the study groups. The seven study groups include:
Administration
Architecture
Mechanical engineering
Electrical engineering
Structural engineering
Civil/geotechnical engineering
Construction management/contractor
For example, the mechanical engineering study group is made up of the mechanical engineers who designed the project (Hot Team) and the mechanical engineers who are completely new to the project (Cold Team) as well as members of the hospital engineering department and others.
The introduction and overview to the workshop with all group members present includes an explanation of the motto that governs these sessions, which reads, “To see what everyone else has seen and to think what no one else has thought.” The introduction also includes a detailed discussion of the five phases of the workshop and the expected outcomes. The workshop then proceeds to carry out the five phases as described.
Information phase. During this phase, all study teams are presented with the vision, mission, and objectives of the facility and the project. A complete project design overview including site, architecture, and engineering is provided by the Hot Team along with a design development budget and cost estimate based on the current drawings.
Creative phase. The seven specialty study groups meet individually during this phase. The Hot Team in each group discusses with the Cold Team the assumptions used in their part of the design and brainstorms alternatives that may improve function and value. Every alternative and idea is considered without initial reaction or judgment. Each idea is written on a separate form and categorized by the group. This phase also includes alternatives that will improve life-cycle costs, which may or may not be a cost reduction.
Evaluation phase. During this phase, each study group evaluates every alternative or idea generated to determine the extent to which it will improve value, function, or safety. The groups identify the highest-priority alternatives to be developed further into complete proposals for additional study and cost estimating.
Development phase. In this phase, each “highest priority” idea or an alternative selected as the highest priority is recorded on a separate description and evaluation form. The description of the proposed change may be accompanied by sketches and a preliminary cost. The proposed alternative may also have a list of advantages and disadvantages for consideration. Comments regarding the effect of the idea on facility operations and clinical function also may be included. At the conclusion of this phase, all study groups reconvene to give all workshop participants a brief overview and preliminary report on their findings.
Master report/estimating phase. Within 2 to 3 weeks following the actual workshop, a master report containing all suggested alternatives and related working papers is developed and presented to the owner. It is not uncommon to have 100–150 ideas listed in this report. We have been able to objectively evaluate alternatives for significant building components such as elevator configurations, parallel double corridors, window wall systems, roof structures, patient room layouts, and hundreds of other design elements. The report contains a summary listing of all alternatives that have been formally included and a researched cost and/or cost reduction figure accompanies each item suggested on the list. The amount of possible savings and/or value improvement is summarized at the conclusion of the report.
The master report is then presented to the owner's project executive committee, and each item is analyzed and reviewed by those most affected. The owner may use various approaches to come to a decision on each item listed in the report. These approaches may include review by other standing clinical and operational committees of the facility.
Conclusion
The workshop approach using Cold and Hot Teams has proven to be an effective, orderly method to optimize value and reduce cost. It provides a process for stakeholders to evaluate their design assumptions professionally and to consider alternatives. Over the past 12 years of designing and building new hospitals and multiple major remodeling projects in the IHC system, this process has reliably proven to accomplish the stated value engineering objectives. We have been able to demonstrate how to obtain optimal value for every dollar of the budget; to provide constructive, well thought-out alternatives to enhanced environments; and to ensure that life-cycle costs are considered in the decision-making process. By using this methodology, the construction cost of all projects over this 12-year capital program has been reduced by approximately 8%, or roughly $52 million.
Results
This peer review method has been an effective tool in developing optimal project scope, priority, and operational value. The accuracy and credibility of project costs have also improved. By using the interdisciplinary format of Cold and Hot Team study groups, and by including owners' representatives and clinical leaders, the entire project team gains an understanding of the cost elements of a project. They learn the value and cost of the major elements of their project from its configuration down to various products and requested equipment. All project team members gain an appreciation of project assumptions and the resulting detailed design. They also gain a deeper understanding of the “where and why” of project costs and alternative solutions. Thus, they are better prepared to make informed “true value-” engineered changes and trade-offs. They then have the tools to bring the project back within budget, yet still achieve the clinical and operational goals of the facility. I believe this method is transferrable and, if more organizations used this approach or something similar, major project costs could be reduced and better value achieved for every dollar spent.