
Abstract
Objective:
The goal of this project was to create an easy-to-administer and inexpensive tool that can help identify usability issues in a patient room bathroom during the design process so improvements can be made before the final product is constructed and put into operation.
Background:
The bathroom is an essential part of any hospital patient room, yet it is associated with nurse dissatisfaction and patient falls. Minimal literature has examined whether the physical structure of various elements within the bathroom are efficient, safe, and satisfactory for the majority of users. Furthermore, there is a paucity of human factor guidelines for architects and designers to follow to ensure the usability of bathroom space for a wide variety of users.
Methods:
The authors adapted a common technique used in software usability: the heuristic evaluation. A heuristic evaluation is a “discount” evaluation method used to quickly and efficiently evaluate the usability flaws of user interfaces. Three methods were used to provide input for the heuristic evaluation: (1) Review of existing heuristic evaluations, reported hospital bathroom problems, and safety checklists; (2) Interviews with nurses and nursing assistants; and (3) Focus groups with nurses. Analysis of the interview and focus group transcripts enabled the categorization of the types of problems nurses encounter in the patient room bathroom. These categories served as the basis for the heuristics in the heuristic evaluation tool.
Results:
Eleven major heuristics (or categories of problems in the bathroom) were identified initially. The authors then went through several iterations of designing and refining the heuristic evaluation to form parsimonious categories and subcategories. Each of the eventual six major heuristic categories contains a general description as well as specific exemplar questions. These detailed subcategories enable an evaluator to easily gauge whether a bathroom adheres to the guideline, to write any comments about a particular issue, and to rate the severity of any problems.
Conclusions:
The bathroom heuristic evaluation was designed to be a discount usability evaluation tool. It can be used to assess a hospital bathroom during the design process for major usability issues, enabling necessary alterations before a final product is developed.
Introduction
The bathroom is an essential part of any acute care hospital patient room. Patients use the bathroom for toilet activities, showering, and washing at the sink. Nurses and nursing assistants utilize the bathroom when they must help patients perform these activities and when they measure a patient's fluid consumption and urinary output (typically every 4 hours). Patients' family members also spend a significant amount of time in the bathroom assisting their loved ones and using the toilet facilities.
The patient room bathroom has been associated with nurse dissatisfaction and a high percentage of patient falls.
Given the bathroom's importance and frequency of use, it is necessary that the physical structure and layout of the bathroom maximize efficiency, safety, and satisfaction for the majority of users. However, the patient room bathroom has been associated with nurse dissatisfaction and a high percentage of patient falls. Although discussions with nursing subject matter experts revealed that various aspects of the patient room bathroom's design make a nurse's job significantly more difficult and time-consuming than need be, a literature search revealed only one study that explicitly mentioned problems that nurses experience with the patient room bathroom (Tzeng & Yin, 2008). These problems included: a lack of traction on handrails and floors, leading to slippery surfaces; an overall lack of handrails; low toilet height; inadequate storage space; and a need for automatic sinks with preadjusted water temperature.
Several studies have also shown that patient room bathrooms, as well as the path from bed to bathroom, are primary locations where patient falls occur. Such falls often lead to patient injuries, increased length of hospital stay, and associated costs (Boswell, Ramsey, Smith, & Wagers, 2001). One study examined reports of patient falls in a 152-bed acute care hospital over 22 months and found that bathroom-related falls contributed to more than half (129 of 249) of the total falls (Rice & Clemmer, 1985). Fifty-seven of these falls occurred on the way to or from the bathroom, and 72 of the falls occurred within the bathroom. Another study investigating reports of patient falls in a 1,300-bed hospital over a 3-month period found that 92 of 183 documented falls were elimination related (e.g., going to the bathroom, reaching for toilet paper, leaving a soiled bed), and 20 of the falls occurred within the actual bathroom (Hitcho et al., 2004). In a related 42-day examination of fall reports at the same hospital, 46 of 98 falls were toilet related and 12 of those falls occurred within the patient bathroom (Krauss et al., 2005). Furthermore, patients who fell in the bathroom were more likely to suffer an injury than those who fell in the patient room. It is apparent that the patient room bathroom is a safety hazard that contributes to patient falls and injuries.
Bathroom-related fall interventions like lift devices (e.g., Garg & Owen, 1992), nurse training (e.g., Alcée, 2000), and bathroom location (e.g., Gallant & Lanning, 2001) have been studied in the past with mixed results on improving patient safety. However, improving bathroom usability in the design or formative phase has not yet been examined. Using an iterative design process that assesses product usability throughout the initial design phases, rather than after the product has been completely developed, is a pillar of user-centered design and offers many potential benefits, including: identifying flaws early in the design process; saving the team from having to make major (and often expensive) changes at the last minute; streamlining development resources; and ultimately producing a more robust and successful final product (Nielsen, 1993).
Whereas the usability life cycle can be a long and expensive process (because it is iterative), there are modern methods known as “discount usability techniques” that are faster and cheaper than traditional user testing (see Nielsen, 1994, for a thorough overview). Heuristic evaluation is one such quick, cost-effective usability technique that can be used early in the design process without any advance planning. The benefit ratio for improving a user interface compared to the costs associated with executing a heuristic evaluation has been suggested to be approximately 48:1 (Nielsen, 1994).
Essentially, a heuristic evaluation is completed by a small set of evaluators who individually examine a user interface and judge its compliance with a standard set of usability principles, the heuristics. The evaluators then share their findings and rank the usability problems according to severity. It is important to have more than one evaluator, because it is nearly impossible for one individual to detect all of the usability problems of a product. It has been suggested that three to five evaluators provide the highest cost/benefit ratio (Nielsen, 2005a). Heuristic principles should be written in such a way that a usability novice or expert could execute the heuristic evaluation. Nevertheless, research has shown that usability experts identify significantly more usability problems, of greater severity, than do novices (Kirmani, 2008).
Several useful lists of usability principles (heuristics) have already been created (e.g., Gerhardt-Powals, 1996; Nielsen, 2005b; Zhang, Johnson, Patel, Paige, & Kubose, 2003), but all of these lists have focused on evaluating the user interfaces of software devices. There is currently no tool available to evaluate the design of a structural environment and to determine where potential usability problems may arise. To this end, the goal of the current study was to create a heuristic evaluation tool that can be applied quickly and cost-efficiently to determine the usability of a patient bathroom.
Method
To gather a range of appropriate bathroom-specific human factors guidelines, a multistep methodology that incorporated previous literature as well as nurses' opinions on various bathroom designs was utilized. First, a review of existing heuristic evaluations, safety checklists, and reported hospital bathroom problems was completed. Next, interviews were conducted to better understand the range of problems that nurses experience with current patient room bathroom designs. Finally, focus groups were conducted to gather nurses' feedback on a prototype patient room bathroom, designed to be user centered, which had not yet been deployed (see Battisto & Allison, 2008, for more information on how the prototype bathroom was designed).
Review of Existing Material
The literature review began by examining current heuristic evaluations and assessing how they could be applied to physical environments. Although several of the current heuristics were not relevant to physical designs (e.g., help users recognize, diagnose, and recover from errors; Nielsen, 2005a), many could be adapted to relate to physical structures (e.g., consistency and standards; Nielson, 2005b). Next, the authors examined safety checklists from a variety of sources ranging from classrooms (Classroom Safety, n.d.) to chemical laboratories (UW Environmental Health and Safety, 2007). In addition to gaining a detailed understanding of important safety components that buildings should contain, the review of these checklists also helped create the general format for the heuristic evaluation tool, which contains more detailed subcomponents than current heuristic evaluations. Finally, the sparse literature available on patient room bathrooms was reviewed. Most of this information was related to patient falls, yet two articles proved to be especially useful in identifying problems related to the bathroom (Hall, 2003; Tzeng and Yin, 2008). Literature review efforts revealed a lack of available information on the usability of physical spaces, particularly the patient room bathroom. Thus, interviews and focus groups were conducted to gather firsthand input on the bathroom from primary users: nurses.
Interviews
The goal of the interviews was to gather nurses' perceptions of current patient room bathrooms and any problems they had experienced. Six registered nurses and two nursing assistants from a large, acute care hospital were interviewed. Nurses were recruited from five different floors (with different bathroom designs) to increase the variety of responses. The interview was approved by an institutional review board and verbal consent was obtained from each of the participants. All interviewees received $25 for their participation. A graduate student conducted the semi-structured interviews in the actual environments of use (i.e., inside the bathrooms). All interviews were audio-recorded and lasted an average of 24 minutes (range 14:50 to 36:19 minutes).
The semi-structured interview asked nurses about the frequency with which they perform different activities in bathrooms (e.g., empty liquids, help patients use the toilet), particular elements of the bathroom, problems that occur in the bathroom, and possible design solutions. The script focused on the following specific bathroom elements: toilet, shower, sink (if present), toiletries (e.g., towels, soap), flooring, handrails, the nurse call device, lighting, the bathroom entrance, and bathroom cleanability. However, nurses were not limited to the specific topics mentioned and were free to discuss any additional issues.
The interviews were transcribed and analyzed using a grounded approach (Strauss & Corbin, 1998). Parsimonious categories for coding the transcripts were developed through several iterations of segmenting important phrases related to bathroom problems, by generating a list of major categories and subcategories in which the segments could fit and attempting to use the revised coding scheme on another transcript. All data were coded and descriptive results were further analyzed (see results section).
To create a heuristic evaluation that potentially covered a wider range of bathroom-related issues, the data from the interviews were augmented with a focus group, which gathered nurses to discuss opinions and feedback on a prototype user-centered patient bathroom.
Focus Groups
The purpose of the focus groups was to gather nurses' feedback on a full-scale prototype patient room bathroom that had been designed to be patient centered and nurse friendly. Feedback was elicited using a focus group procedure because it was an efficient way to allow nurses to interact with the new bathroom, gather input from multiple people at once, and explore nurses' opinions about various aspects of the bathroom design and potential alternate designs.
The focus group was approved by an institutional review board and written consent was obtained from participants. All nurses received 2 hours of their regular hospital pay as compensation for participating in the study. Two focus group sessions were conducted with nine registered nurses (four in one focus group, five in the other) from a local hospital. The total time required for each session was approximately 1 hour 45 minutes, with an average of 51 minutes (a range of 42 to 60 minutes) spent on the group discussion section. There was a high consensus across both groups and within each group; thus the current sample appeared to be representative of how experienced nurses perceive the prototype bathroom design.
The overall procedure consisted of a role-playing session followed by a group discussion. Focus group participants first completed a demographics questionnaire and an informed consent form. A moderator then explained that the group would have an opportunity to interact with a mocked-up patient room bathroom by role-playing common bathroom tasks. Nurses were given a legal pad and instructed to write down any thoughts they had about the bathroom during the role-playing session. After the role-playing, the nurses participated in a moderated group discussion of what they liked and disliked about specific aspects of the bathroom and any other thoughts or suggestions they had.
The five mock bathroom tasks were selected by consulting a subject matter expert (a nursing instructor with 20+ years' experience) as well as data from interviews with nurses. The tasks were meant to represent typical bathroom tasks:
Assist a patient who is fairly weak and hooked up to an intravenous (IV) line to get from the bed to the toilet and sit down. Then assist the patient to get up from the toilet, wash his or her hands in the bathroom sink, and get back into bed.
Assist a patient who is in a wheelchair to get from the bed to the toilet and sit down. Then assist the patient to get up from the toilet, wash his or her hands in the patient room sink, and get back into bed.
Assist a patient who is in a walker to get from the bed to the toilet and sit down. Then assist the patient to get up from the toilet and get back into bed.
Assist a patient who is able to ambulate with washing his or her face and brushing her teeth.
Assist a patient from the bed to the shower and pretend to assist with the shower.
Before each task began, two participants would volunteer to act as patient and nurse (each nurse had the opportunity to role-play each character). The researcher explained what the specific task was and what materials were available to work with. The “patient” was then set up in the proper position (e.g., with IV on arm lying down in bed) and participants were told to commence when ready. After each task was completed, the researcher would set up for the next task while participants wrote their thoughts on the pads.
After all five tasks were completed, participants and a focus group moderator (a graduate researcher) gathered to discuss their thoughts and opinions about the bathroom tasks. A note taker stood in front of the table and took clearly visible notes outlining what was being discussed. The focus group script was semi-structured and nearly identical to the interview script. Both of the focus groups were transcribed and coded using a coding scheme identical to the one used for the interviews.
Results
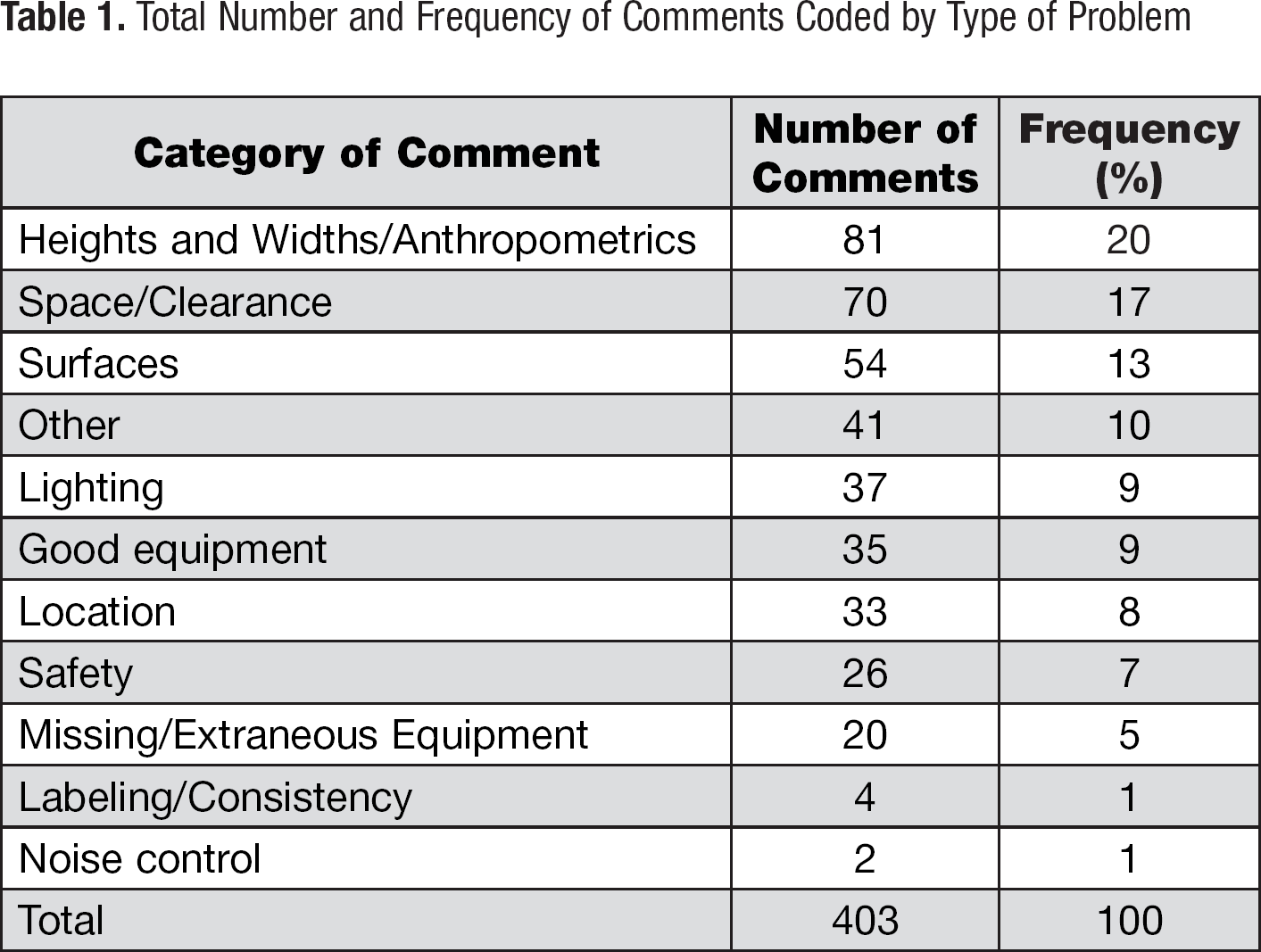
To review, the goal of the project was to capture and organize the full range of usability and human factors-related problems that nurses experience in the patient room bathroom. The general strategy for creating our bathroom heuristic evaluation tool was to identify the problems and categorize them into relevant themes. The interviews and focus groups yielded a total of 403 comments about the bathroom (234 from the interviews and 169 from the focus groups). Each comment was coded along three dimensions: tone of comment (i.e., positive, negative, and neutral); bathroom equipment/element (e.g., sink, bathroom entry); and type of problem (e.g., location, missing equipment). The type of problem category was most useful for this study and will be discussed in further detail. The other categories were less useful for the development of the heuristic evaluation and were not analyzed further.
Table 1 displays the total number and frequency of nurses' comments coded by problem type. These 11 categories formed the foundation of the heuristic evaluation. Following are highlights of some of the kinds of problems nurses experience and prominent themes that emerged from each category.
Total Number and Frequency of Comments Coded by Type of Problem
Heights and Widths
One of the major issues in this category was the height and width of the bathroom toilet. Every single nurse interviewed stated that the toilet seat (which was approximately 15 inches above the ground) was too low. “It's just too low, and these weak patients can't bend that far!” one nurse exclaimed.
Another common theme was that handrails in the bathroom and shower are often at awkward heights that require excessive bending and/or reaching. One of the interview bathrooms, as well as the focus group bathroom, featured a handrail behind the toilet approximately 4 feet up from the toilet seat. In both cases, the nurses commented that the high handrail is not serving any purpose at all, “Because men do not [urinate] standing up in the hospital.”
Multiple participants stated that it is vital to have properly located handrails in the bathroom near the toilet and sink and in the shower (as well as for the walk from bed to bathroom). Nurses revealed that without convenient handrails, patients rely on the nurse to steady themselves. Participants often recommended having handrails next to the toilet and shower seat, on both sides of the patient where they can easily move themselves down and up.
Space/Clearance
A common complaint expressed in both the interviews and focus groups was that the overall size of the bathroom was too small. Nurses said this becomes a problem when they are trying to assist a patient using the restroom, as well as in emergency situations when several staff members must crowd in a tiny bathroom to rescue a patient. Generally, nurses suggested that bathrooms should comfortably accommodate the patient, a nurse (or other helper), and at least one piece of patient equipment (e.g., a walker or an IV pole). Nurses working on floors with bariatric bathrooms liked the size of the bathroom except for the shower. One nursing assistant described how large patients will fit only halfway into the shower, and the whole bathroom gets soaked when washing them with the handheld shower sprayer.
Surfaces
The majority of the comments about surfaces were related to either slippery floors or raised thresholds. A common theme from the interviews was that the bathroom floor often gets slippery when wet and becomes a potential fall hazard. “The tile is just so dangerous when it's wet,” one nurse commented. “I wish that there was maybe some gripper type material on the floor, or at least in the shower, and there is none,” another nurse stated.
Nearly every single nurse in both the interviews and focus groups made a negative comment about the raised threshold (approximately ¼-inch–1 inch) at the entrance of all the bathrooms. While this small bump may seem insignificant to outsiders, nurses experience tremendous difficulty because of it. Walkers, IV poles, and “shufflers” (patients who shuffle rather than lift their feet) all frequently get stuck on the threshold. Some of the showers in the interview bathrooms also contained a high threshold (approximately 6 inches–1 foot), which nurses said makes it difficult for patients to step over.
Good Equipment
The majority of the comments in this section were in reference to the handheld shower sprayer found in both the interview and focus group bathrooms. Participants felt that this was a convenient tool that makes assisting a patient in the shower much easier. Another prominent theme was that nurses like it when the nurse call device has a long string. While one nurse did say that a long string could be involved in an accidental hanging, the majority of the participants preferred having a long string that they could hand to patients using the toilet.
Location
A major theme that emerged was that necessary equipment needs to be located within close reach of the patient. Of particular importance is the location of the nurse call button. Participants said that there should be a nurse call device very close to a patient who is on the toilet or in the shower. Current devices are sometimes located so far away that patients fall trying to reach them. The toilet paper holder was another item commonly mentioned as being located too far away—either behind the patient, or across from the toilet on an opposite wall. These locations require patients to have awkward body positioning and/or to reach too far. As mentioned in the heights and widths category, handrail location was also a common thread among participants.
Safety
Some of the main themes in this category dealt with slippery surfaces, tripping hazards, lack of ventilation, and electrical hazards. The first two of these themes were discussed previously in the surfaces category, so here the focus is on the remaining two. Nearly all of the nurses in both the interviews and focus groups commented on a lack of ventilation in patient room bathrooms. The nurses explained that, without ventilation, the bathroom gets steamy, surfaces get slick, and patients get dizzy and sometimes pass out. Another common finding was that electrical outlets were located very close to the sink, creating a potential electrocution hazard.
To finalize the heuristic evaluation tool, data collected from all three methods (i.e., review of existing materials, interviews, and focus groups) were re-examined and reviewed by four members of the research team who then went through several iterations of designing and refining the heuristic evaluation tool to form parsimonious heuristic categories and subcategories. They found that some of the categories could be combined. For instance heights and widths/anthropometrics was combined with location; noise control was merged into surfaces; and lighting was distributed among labelling/consistency and safety. Other categories, such as good equipment and other, were taken into consideration across the whole heuristic evaluation.
Once the major heuristic principles had been formed, the researchers created a general description of each category. Then, specific exemplars of each heuristic were created in the form of yes/no questions. These detailed subcategories enable an evaluator to easily gauge whether a bathroom adheres to a particular guideline. If the bathroom does not adhere to the guideline, there is a place for evaluators to mark their comments and rate the severity of the problem. The completed heuristic evaluation tool is presented in Appendix A.
Discussion
Many problems experienced by nurses and patients may be traced to ergonomic or human factor-related aspects of a patient room bathroom. However, there is currently no tool available to help identify usability issues for a patient room bathroom. The goal of this study was to create an evaluation tool that would be quick, cost-efficient, and usable by both experts and novices. First, users' perceptions and opinions about current patient room bathrooms were identified. The primary areas of concern were: what tasks do users perform in the patient room bathroom, what problems do they encounter, and how could these problems potentially be mitigated through design? Next, the results from these data were organized around general themes. The themes were then turned back into general design heuristics and used as a basis to create a tool that could be applied by both architects and human factors experts to determine the usability of a given bathroom.
The heuristics identified should serve as guide-posts for potential evaluators when examining an existing or new bathroom. As in Nielsen's (2005a) original heuristic evaluation technique, it is estimated that three to five evaluators individually complete a series of representative tasks in the target bathroom, and then grade the room using these heuristics. Afterwards, the team of evaluators will convene, discuss the problems identified, and rank them by severity. The heuristic evaluation is not meant to be a precise tool; rather, it is meant to identify major usability flaws that can be further examined through user testing.
A key advantage of the heuristic evaluation is that it can be used at any point in the design process to identify usability-related concerns. During the formative design phases, the heuristic evaluation can be applied to either low-fidelity (e.g., blueprints, cardboard prototype) or high-fidelity (e.g., working prototype) mock-ups. When the bathroom is in the final phases of design, the heuristic evaluation can be used to identify serious usability flaws that require attention before the product is released. Finally, existing patient room bathroom designs can be examined to determine what problems currently exist, and how they could be fixed in a renovation or new iteration.
The potential benefits of assessing the usability of a bathroom before it is put into use in a new hospital are increased patient safety and user satisfaction, a reduction in patient falls and the associated costs, and a decrease in future bathroom renovation costs.
The potential benefits of assessing the usability of a bathroom before it is put into a new hospital are increased patient safety and user satisfaction, a reduction in patient falls and the associated costs, and a decrease in future bathroom renovation costs. The proposed heuristic evaluation is currently in the process of being validated by gathering subject matter expert feedback (e.g., from architects and nurses) and testing it on a variety of patient room bathroom designs. The complete heuristic evaluation can be found in Appendix A at the end of this article. It is hoped that the research and design community will adopt and adapt this tool to meet its needs; the authors welcome any feedback.
Incorporating human factors knowledge into the design process can be difficult, especially when personnel with appropriate knowledge are unavailable. Although the heuristic evaluation is by no means meant to replace a human factors expert, it may be useful for situations where a bathroom must be evaluated quickly for major usability flaws. This research represents one way to apply user-centered design techniques to create a physical environment evaluation tool. This study focused on the nurse's perspective, but the method could be applied to other stakeholders as well (e.g., patients). Furthermore, while a patient room bathroom heuristic evaluation was the end result of this research, the general process by which the heuristic evaluation was created may be replicated for other areas of a hospital (e.g., bedside, nursing station, supply room), as well as for other physical structural environments.
Footnotes
Acknowledgments:
This work was supported in part by a grant from the Department of Defense through Spartanburg Regional Health System and NXT Health, Inc. The authors gratefully acknowledge the assistance of Mary-Kate Mclaughlin, Taylor Smith, and Mason Couvillion.
Appendix A: Patient Bathroom Heuristic Evaluation Tool
No.
Issue
Comply?
Comments
Severity
Yes
No
N/A
L
M
H
1.0
1.1
Does the bathroom entrance accommodate large patients, patients in wheelchairs/walkers, and patients attached to a piece of equipment (e.g., IV pole)?
1.2
Does the bathroom door swing open and closed without hitting any other doors or equipment?
1.3
Does the bathroom comfortably accommodate two people (i.e., patient and helper)?
1.4
Can the bathroom door close completely when a person (who may be large or have assistive equipment) is sitting on the toilet?
1.5
Is a large patient able to fit inside the designated shower area?
Other:
Other:
2.0
2.1.0
Handrails
2.1.1
Are handrails present on both sides of the toilet?
2.1.2
Are toilet handrails positioned so patients can easily lower themselves down and then push themselves back up?
2.1.3
Are handrails present on all sides of the shower?
2.1.4
Are shower handrails located in a position that is easy for the majority of standing patients to access?
2.1.5
Do all handrails in the bathroom limit the need to bend, reach, or turn?
2.1.6
Are handrails present on both sides of the shower seat?
2.1.7
Are shower seat handles in a location where patients can easily lower themselves down and then push themselves back up?
2.1.8
If sink is in bathroom, is a handrail located within easy reach for patients to steady themselves on?
2.2.0
Emergency Call Signal
2.2.1
Is the emergency call positioned so a person sitting on the toilet can reach it without excessive bending, reaching, or turning?
2.2.2
Is the emergency call positioned so a person in the shower can reach it without excessive bending, reaching, or turning?
2.2.3
Is the emergency call positioned away from water and/or is it waterproof?
2.3
Is the toilet located at a height so that knees sit at a 90-degree angle or greater?
2.4
Is the toilet paper holder in an easy-to-reach location that minimizes bending, turning, and reaching?
2.5
Is the shower seat located at a height that minimizes bending and allows patients to easily lower themselves down and push themselves back up?
2.6
Are all countertops located at a height that minimizes bending and reaching?
2.7
Are the soap dispenser and paper towel holder located close to each other and within easy reach of the patient at the sink?
Other:
Other:
3.0
3.1
Are light switches located in a typical location (e.g., on the wall to the right or left when you first enter the room)?
3.2
Is light switch operation simple and consistent with everyday operation?
3.3
Are hot/cold assignments on faucets clearly labeled with color (red/blue) or text and color labels?
3.4
Do faucets work in a manner consistent with local customs and mental models (turning on/off and hot/cold)?
3.5
Is the flushing mechanism on the toilet clearly labeled and easy to use?
3.6
Are all bathrooms on a given hospital floor designed the same with all equipment in the same location?
3.7
Is the purpose of every single piece of equipment in the bathroom (i.e., soap dispenser, towel bar) obvious to novices?
3.8
If any piece of bathroom equipment is automated, is it easy for a novice to understand and to operate the equipment correctly?
Other:
Other:
4.0
4.1
Is a smoke detector present and operational?
4.2
Is a sprinkler system present and operational?
4.3
Are there any barriers/ledges on the bathroom floor that may increase the risk of tripping or for machinery (e.g., IV pump) to get stuck?
4.4
Are there any sharp corners or edges that may injure a person?
4.5
Are all shelves, towel bars, etc., securely fastened (even if a person tried to use it as a handrail)?
4.6
Are electrical outlets in proper working order?
4.7
Do electrical outlets have cover plates?
4.8
Are electrical outlets arranged so that cords will not cross the sink (or other water source)?
4.9
Is ventilation adequate to reduce steam buildup?
4.10
Are the mirrors steam-proof?
4.11
Are exits clearly marked?
4.12
Are exits maintained clear and free from obstruction?
4.13
Is there any risk of patients or nurses bumping their heads (e.g., when they are rising from a seated or bent position)?
4.14
Is there enough light in the overall bathroom and shower for nurses to closely examine patients' wounds?
4.15
Are light switches easily accessible in the dark either by convenient location or glowing?
4.16
Is sink water temperature at a controlled setting that prevents water from getting too hot?
Other:
Other:
5.0
5.1
Is the floor made of a nonslip material that will help prevent falls—even when the floor is wet?
5.2
Are the floor and other surfaces made of wear-resistant, easy-to-clean materials?
5.3
Are all sink and shower handles easy to grip when wet?
5.4
Does the bathroom provide proper drainage that prevents excess water buildup?
5.5
Do bathroom surfaces minimize loud noises and provide noise control?
Other:
Other:
6.0
6.1
Is the soap dispenser easy to use, refill, and clean?
6.2
If not automated, does the soap dispenser afford the entire palm to dispense soap comfortably?
6.3
Is the paper towel holder easy to use, refill, and clean?
6.4
Does the paper towel holder prevent paper towels from getting stuck or falling out?
6.5
Is there a shower seat located in the shower that is sturdy (even for large patients), comfortable, and easy to clean?
6.6
If showerhead is hands-free, is it easy for a novice to use, maneuver, and take down/hang up when standing and sitting on a shower seat?
6.7
Is sink deep enough to prevent water splashing with normal hand washing?
6.8
Is there an area in the shower to put basic toiletries (e.g., soap and shampoo)?
6.9
Is there a storage area near the sink for patients (especially long-term) to store essential toiletries (e.g., toothbrush, razor)?
6.10
Is there a place for patients to put a towel while they shower?
Other:
Other: