
Abstract
The physical facilities in which healthcare services are performed play an important role in the healing process. Evidence-based design in healthcare is a developing field of study that holds great promise for benefiting key stakeholders: patients, families, physicians, and nurses, as well as other healthcare staff and organizations. In this paper, the authors present and discuss a conceptual framework intended to capture the current domain of evidence-based design in healthcare. In this framework, the built environment is represented by nine design variable categories: audio environment, visual environment, safety enhancement, wayfinding system, sustainability, patient room, family support spaces, staff support spaces, and physician support spaces. Furthermore, a series of matrices is presented that indicates knowledge gaps concerning the relationship between specific healthcare facility design variable categories and participant and organizational outcomes. From this analysis, the authors identify fertile research opportunities from the perspectives of key stakeholders.
Healthcare cannot be separated from its built environment (Malkin, 2002). Healthcare buildings, equipment, furnishings, colors, art, landscape, and other elements of the built environment influence the delivery of healthcare and its outcomes and convey multiple clues about the competence and caring of the provider organization (Berry & Bendapudi, 2003; Berry & Seltman, 2008; Ulrich et al., 2008). The field of evidence-based design (EBD) has developed during the last quarter century to apply scientific knowledge and methods to help guide healthcare facility design that reduces the stress of facility users, improves safety and productivity, reduces resource waste, and enhances sustainability (Berry, et al., 2004). EBD offers data on what works and what does not; it brings empiricism to the design process to support imagination, judgment, and evaluation. It makes perfect sense to use the best available evidence to create a healthcare facility that will be used for many years and for which so much is at stake. Yet, as in any field, execution typically lags behind theory and research. In times of economic stress and scarce capital, cost minimization may trump other considerations, including research-based design improvements. EBD has come a long way, as a flurry of new books attests (e.g., Cama, 2009; Guenther & Vittori, 2007; Hamilton & Shepley, 2009; Hamilton & Watkins, 2009; Malkin, 2008; Sternberg, 2009). Much work remains to be done, however, not only in practice but in theory-building and research.
The relevance of EBD to the most pressing challenges of healthcare—cost control, financial stability, avoidable harm, quality improvement, clinical staff shortages, better patient experiences, sustainability—is profound. Improving healthcare buildings is integral to improving healthcare. A quarter century into this fast-evolving, eclectic, interdisciplinary field that draws on research from medicine, nursing, environmental psychology, architecture, and design, among other disciplines, seems like a good time to take stock and reflect on the state of the field. That is the purpose of this article.
The article has two broad purposes. First, the authors present and summarize a conceptual framework intended to capture the domain of EBD as it has evolved up to the present. The goal is to convey visually and in narrative form a broad overview of EBD as a research discipline. In effect, a “picture” of EBD at this point in time is drawn. The picture will change as new subject areas and new relationships emerge over time. The intention is to present an overview of the field, not a comprehensive literature review, which already exists (Ulrich et al., 2008). A conceptual framework for the domain of EBD provides a structure that integrates multiple disciplines, serves as a communications platform for designers and researchers, and visually portrays the complexities, relationships, and pervasive implications of the healthcare built environment.
Second, a series of matrices that indicate knowledge gaps in understanding the relationships between specific healthcare facility design variable categories and participant and organizational outcomes is presented and discussed. A series of priorities for future research is derived from this analysis. It is hoped that this article will stimulate needed empirical research in EBD and contribute to its theoretical development.
Conceptual Framework
The conceptual framework proposed for the domain of EBD in healthcare is presented in Figure 1. The left side of the framework presents built environment design variables. The middle part presents participant outcome variables and demographics that may influence these outcomes. Organizational outcome variables are featured on the right side as are cultural and other organizational factors that may moderate any of the outcomes included in the framework. The lines and arrows indicate the relationships among variables. The authors propose that the healthcare built environment significantly impacts the individuals who use it, including patients, families, physicians, nurses, and other staff. Further, it is posited that the built environment can affect the overall performance of a healthcare organization both directly and—more commonly—indirectly through participant outcomes. The built environment is only one of the multiple influences on participant and organizational outcomes. Facility design plays an important role in healthcare outcomes, but so do clinician competencies, service process design, organizational culture, and a host of other factors.
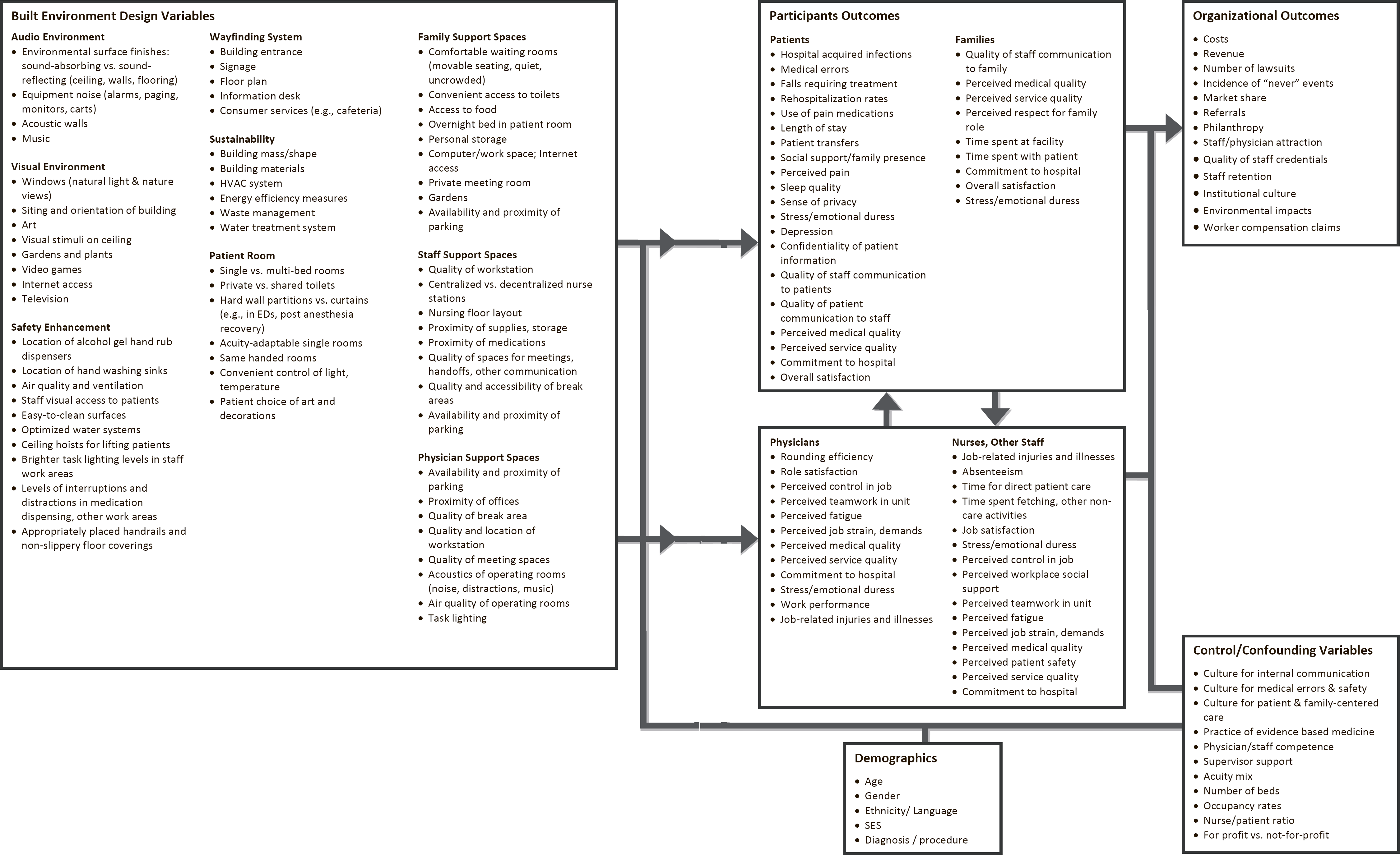
A model of participant and organizational outcomes of the healthcare built environment.
The built environment design variables are grouped into nine categories that reflect the authors' best judgment on how to portray the structure of EBD; they draw, in part, on the literature review by Ulrich et al. (2008). The focus is specifically on the design issues associated with each category. Whereas “sustainability” is a multifaceted societal issue, the specific variables in this category are included as healthcare facility design variables.
The categories and specific variables in this framework are not intended to be mutually exclusive or collectively exhaustive. For example, the variable “single vs. multi-bed rooms,” included in the “patient room” category, also applies to other categories such as “safety enhancement.” Additional topics and specific variables likely will emerge with the continuing growth of this relatively new field of research. The built environment design variables in one category may influence only a subset of the listed participant and organizational outcomes. The design variables in the first six categories are likely to affect multiple participant groups, whereas variables in the last three categories concern a specific participant group.
The following discussion provides a brief overview of each design variable category. Hospitals are emphasized in the discussion of existing research because they are the focus of most EBD research conducted to date. In this respect, EBD research trails practice, because more healthcare is delivered in nonacute care settings. The research cited is illustrative rather than comprehensive. (For a comprehensive review of EBD research, see Ulrich et al., 2008.) The purpose of these overviews is to provide readers a basic grounding in the categories that are proposed as representative of the domain of EBD.
Audio Environment
The audio experience of healthcare can be improved by reducing noise and introducing pleasant sounds, such as music. Noise is a serious problem in healthcare settings. Noise in hospitals (averaging 45–68 decibels [dB] and peaking at 85–90 dB) is a major environmental stressor that negatively influences both patients and staff, contributing to sleep disturbance and deprivation, stress, annoyance and dissatisfaction, detrimental physiological responses (e.g., high blood pressure, high heart rate, and low oxygen saturation), interference with oral communication, and poor staff performance (Topf, 2000; Ulrich et al., 2008).
Environmental noise-reduction measures proven effective in healthcare generally fall into three categories: (1) noise source control, e.g., noise-sensor light alarms (Chang, Pan, Lin, Chang, & Lin, 2006); (2) sound absorption, e.g., acoustic ceiling tiles (Blomkvist, Eriksen, Theorell, Ulrich, & Rasmanis, 2005); and (3) noise blocking, e.g., single-bed rooms with acoustic wall separations (Gabor et al., 2003). Associations have been empirically established between noise reduction measures and improvements in patient outcomes such as stress, sleep, satisfaction, re-hospitalization, and speech intelligibility (Ulrich et al., 2008). Reducing noise may also improve other outcomes such as patient length of stay, perceived pain, and use of pain medications. However, research has not yet directly linked specific noise reduction measures to these outcomes. Similar to noise reduction, other audio interventions including relaxing music and nature sounds (e.g., birds chirping) can reduce stress and pain (Sarkamo et al., 2008). Lee and colleagues (2004) found that combining positive audio and visual stimuli (such as a classical music and a serene nature scenery presentation) is more effective than visual stimuli alone in reducing sedation usage.
Visual Environment
Measures to improve the visual environment of healthcare facilities include positive distraction and natural lighting. Positive distractions provide a moderate level of environmental stimulation that diverts the attention of patients from stressors (e.g., noise, pain), fosters restoration from negative feelings, and improves patients' psychological and emotional well-being (Ulrich, 1991; Ulrich, 2008). Evidence supports the use of nature distractions to reduce stress (manifested as higher blood pressure, increased heart rate, and other negative physiologic responses), reduce pain and pain medication usage, and expedite recovery (Ulrich, 1984). Visual access to nature can be gained directly through outdoor gardens, indoor plants, and window views of nature as well as indirectly through artwork and other visual displays of nature scenes. Direct exposure to nature seems to have a stronger effect than indirect exposure (Kahn et al., 2008). Nature scenes that include soothing elements such as trees and serene water have been found to be more suitable than other types (Nanda, Hathorn, & Neumann, 2007).
The use of natural daylight as a primary lighting source in healthcare facilities is beneficial. Research has linked exposure to daylight (including sunlight) to improved patient outcomes (e.g., less stress, less depression, less pain, less pain medication usage, better sleep at night, faster recovery, shorter length of stay) as well as to higher staff productivity and job satisfaction, although the mechanisms behind the links are not completely clear (Alimoglu & Donmez, 2005; Wakamura & Tokura, 2001; Walch et al., 2005). Moreover, the use of daylight together with proper photoelectric dimming systems reduces electricity consumption for artificial lighting and the ecofootprint of healthcare facilities (Li, Lam, & Wong, 2006). More research is needed to understand the degree of influence of the built environment on the amount, quality, and timing of daylight available to patients and caregivers; how to control possible light pollution (e.g., glare from sunlight); and how different environmental factors interact with each other to influence daylight and healthcare outcomes. Research is beginning to examine the effects of room orientation (e.g., east vs. west, south vs. north) and the size of windows on daylight exposure in patient rooms, but the results are far from conclusive (Pechacek, Andersen, & Lockley, 2008).
Safety Enhancement
The design of the built environment can lower the incidence of nosocomial infections, medical errors, patient falls, and staff injuries (Leape et al., 1991; Zhan & Miller, 2003). Environmental infection control interventions such as high-efficiency air ventilation and filtration, alcohol-based hand-rub dispensers, accessible hand-washing sinks, proper disinfection of inanimate surfaces, optimized water systems, and single rooms with private toilets are effective in lowering hospital-acquired infection rates (Ulrich et al., 2008).
Medication errors can be reduced by controlling interruptions from unexpected peak noises and providing bright illumination in staff work spaces (Buchanan, Barker, Gibson, Jiang, & Pearson, 1991; Flynn et al., 1999). Intrahospital transfers—a source of medical errors—can be minimized by acuity-adaptable rooms that accommodate the different levels of care required by an individual patient during a hospital stay (Hendrich, Fay, & Sorrells, 2004), although acuity-adaptable rooms are controversial because of staffing and other concerns (Evans, Pati, & Harvey, 2008). Decentralized nursing stations, which facilitate close monitoring of patients, have been reported to reduce the incidence rate of patient falls (Hendrich, Bender, & Nyhuis, 2003). The built environment can play an important role in preventing patient falls, but more research is needed to clarify the effectiveness of specific environmental interventions (Gulwadi & Calkins, 2008). Nurses suffer from a disproportionately high rate of musculoskeletal injury attributable to patient handling. The installation of patient lifting devices reduces the incidence of nurse injuries and the consequent costs of workers compensation (Vieira & Miller, 2008).
Wayfinding System
The difficulties of wayfinding in complex healthcare settings can frustrate patients and families, cause stress, result in late or missed appointments, and divert staff time to giving directions (Carpman, Grant, & Simmons, 1990; Huelat, 2007; Zimring, 1990). Wayfinding problems can be addressed effectively by integrating physical environment improvements with organizational and operational changes (Carpman & Grant, 1993). Limited research evidence suggests that the design component of a successful wayfinding system should combine a building structure that is cognitively comprehensible (e.g., perpendicular intersections, main entrance and key facilities positioned close to the main hallway, high visibility of major services for patients and families [Baskaya, Wilson, & Ozcan, 2004; Weisman, 1981; Werner & Schindler, 2004]) with the provision of ample information along the navigating paths (e.g., you-are-here maps oriented in the direction that viewers are facing, a logical signage system that is easily understandable by a lay person, and well-situated information desks [Carpman, Grant, & Simmons, 1983; Levine, Marchon, & Hanley, 1984; Wright, Hull, & Lickorish, 1993]). Enhanced wayfinding features should improve certain participant and organizational outcomes. However, the effects of these features on outcomes have not yet been directly and rigorously evaluated.
Sustainability
The construction and operation of healthcare facilities consumes considerable energy and other resources and generates millions of tons of waste and greenhouse gas emissions each year (Guenther & Vittori, 2007; Kaplan, Orris, & Machi, 2009). Sustainable design represents a significant opportunity to reduce building operating expenses and environmental impact. Design variables that affect healthcare sustainability include building mass, shape, and orientation (e.g., self-shading); building envelope (e.g., double-glazing, green roof); the heating, ventilation, and air-conditioning system (e.g., displacement ventilation, heat recovery); selection of materials and equipment (e.g., occupancy sensors, energy-efficient imaging machines); and waste management and water treatment systems (Guenther & Vittori, 2007).
Research in healthcare and other settings that supports the effectiveness of certain sustainable design interventions is limited but encouraging. For example, computer simulation studies reveal that building energy consumption could be significantly reduced by double-glazed façades, exterior wall insulation materials, and self-shading (Capeluto, 2003; Hien, Wang, Chandra, Pandey, & Wei, 2005; Khodakarami, Knight, & Nasrollahi, 2008). Post-occupancy evaluations of Leadership in Energy and Environmental Design-certified buildings have documented energy savings due to sustainable design (Fowler & Rauch, 2008; Newsham, Mancini, & Birt, 2009). Far more work is needed to consolidate the knowledge base of sustainable design through the empirical evaluation of design innovations (Kaplan et al., 2009; U.S. Green Building Council Research Committee, 2008).
Patient Room
Accommodating patients in single-bed rooms instead of traditional multibed rooms or open bays can improve numerous healthcare outcomes, including hospital-acquired infection rates, sleep quality, stress level, number of privacy breaches, communication between patients and staff, satisfaction of patients and families, number of patient transfers, and patient length of stay. A growing body of research demonstrates the benefits of single rooms. For example, single rooms significantly reduced the rates of respiratory, urinary tract, and catheter-related infections in a pediatric intensive care unit (Ben-Abraham et al., 2002). Single rooms with solid doors and walls in an emergency department provided superior speech privacy compared to open spaces separated by curtains (Karro, Dent, & Farish, 2005; Mlinek & Pierce, 1997). Patients slept better in single rooms because of lower noise levels (Gabor et al., 2003). And single rooms were associated with higher patient satisfaction with healthcare services (Janssen, Klein, Harris, Soolsma, & Seymour, 2000).
Single-bed rooms also should benefit caregivers for some of the same reasons they benefit patients (e.g., less noise, more privacy). In one study, nurses working in single-room neonatal intensive care units reported lower stress and higher job satisfaction than nurses in open units (Shepley, Harris, & White, 2008). However, considerably less research has been done on the effects of single-bed rooms on staff.
Aside from single rooms, offering patients choice and a sense of control is an important design consideration for patient rooms. To a degree, a patient's loss of control is inherent in the experience of hospitalization and can result in negative consequences such as high stress levels (Ulrich, 1991). Personal control over the environment can improve patients' physical and emotional comfort and contribute to healing by facilitating coping with stress effectively. Specific design features believed to foster a sense of control include enabling patients and families to individually control lighting and temperature, television programming, and Internet access; to personalize their rooms by selecting artwork (Sadler & Ridenour, 2009; Suter & Baylin, 2007); and to gain access to the outside (e.g., window views, gardens).
Family Support Spaces
Families are an important source of social support for patients and can provide information and other assistance in patient care (Williams, 2005). Studies of both pediatric and adult patients in different healthcare settings (e.g., acute and long-term care facilities) have found that family presence contributes to reducing patient stress, alleviating pain, improving clinical outcomes, reducing length of stay, and increasing patient satisfaction (Bay, Kupferschmidt, Opperwall, & Speer, 1988; Chatham, 1978; Happ et al., 2007; Hendrickson, 1987; Mason, 2003). Likewise, family members' freedom to visit and stay with patients during hospitalization meets families' emotional needs and increases their satisfaction (Powers & Rubenstein, 1999).
A healthcare building that supports family presence typically incorporates certain features specifically designed for the comfort of family and other visitors. Such features include quiet waiting rooms with flexible, comfortable group seating; an overnight bed in patient rooms; Internet access; work spaces; personal storage; and private bathrooms. Much remains to be learned about specific design features that contribute the most to encourage family social support.
Staff Support Spaces
The health and performance of patient care staff directly influence the quality of care. A small but growing body of evidence suggests that effective facility design can reduce staff stress, enhance staff safety, boost productivity, and improve quality of care and job satisfaction (Berry & Parish, 2008; Malkin, 2008; Ulrich et al., 2008). Limited existing evidence suggests that certain environmental approaches that benefit patients (e.g., daylight, nature views, sound-absorbing ceiling tiles) also benefit nurses and other staff by reducing job stress, burnout, dissatisfaction, and turnover (Alimoglu & Donmez, 2005; Blomkvist et al., 2005; Pati, Harvey, & Barach, 2008).
One study found that brief bright light exposure can alleviate stress related to nightshift work (Leppamaki, Partonen, Piiroinen, Haukka, & Lonnqvist, 2003). Nursing unit layouts that fit work patterns (e.g., decentralized work stations and supplies adjacent to patient care areas, acuity-adaptable rooms that minimize nursing time when transferring patients) can improve nursing efficiency by increasing direct patient care time and reducing walking distances (Gurascio-Howard & Malloch, 2007; Hendrich et al., 2004; Shepley, 2002). Moreover, environmental features (e.g., hand-rub dispensers and ceiling lifts) can enhance staff safety.
Physician Support Spaces
Obviously physicians are important users of healthcare spaces. Some literature suggests that environmental elements, including quality of physician spaces, noise, temperature, humidity, anesthetic vapors, lighting, and facility and parking convenience can affect the work performance, health, job-related stress, and job satisfaction of physicians (Ramsay, 2000; Weinger & Englund, 1990). However, very limited research has directly measured the impact of the built environment on physicians.
One area that has attracted research attention is the acoustic environment of operating rooms. Studies have shown that background and peak noises in operating rooms may interfere with communication and auditory monitoring and distract physicians from their core tasks (Hodge & Thompson, 1990; Murthy, Malhotra, Bala, & Raghunathan, 1995). Auditory distractions may cause physicians to take a significantly longer time to complete surgical tasks, even though experienced physicians may be able to avoid the negative influences of distractions on the quality of work (Goodell, Cao, & Schwaitzberg, 2006). Furthermore, loud noise caused by certain surgical procedures has the potential to cause hearing loss (Love, 2003). Conversely, appropriate ambient music selected by physicians has been found to improve physicians' work performance in operating rooms (Sanderson et al., 2005). Environmental design that supports physicians' unique needs in specific situations may facilitate their work and improve healthcare efficiency and quality.
The Strength of Evidence Linking Environmental Variables and Outcomes
Taking stock of EBD in healthcare involves more than a pictorial and narrative profile of the domain of the discipline as it has evolved to the present. It is also important to consider the state of research in the field—where it is strong and where it is not—and point to the future in hope of encouraging the research needed to fill many gaps in current knowledge. In the remainder of this article, the state of EBD research is considered in a series of matrices that reveal knowledge gaps visually. This is followed by an illustrative listing of research priorities organized around the middle and right side of the conceptual framework shown in Figure 1, the outcomes sections of the framework.
The matrices showing the relationships between environmental variable categories and outcomes are presented in Tables 1 through 5. The first four tables depict direct linkages between environmental variable categories and outcomes for patients (Table 1), family (Table 2),
State of EBD Research for Patient Outcomes
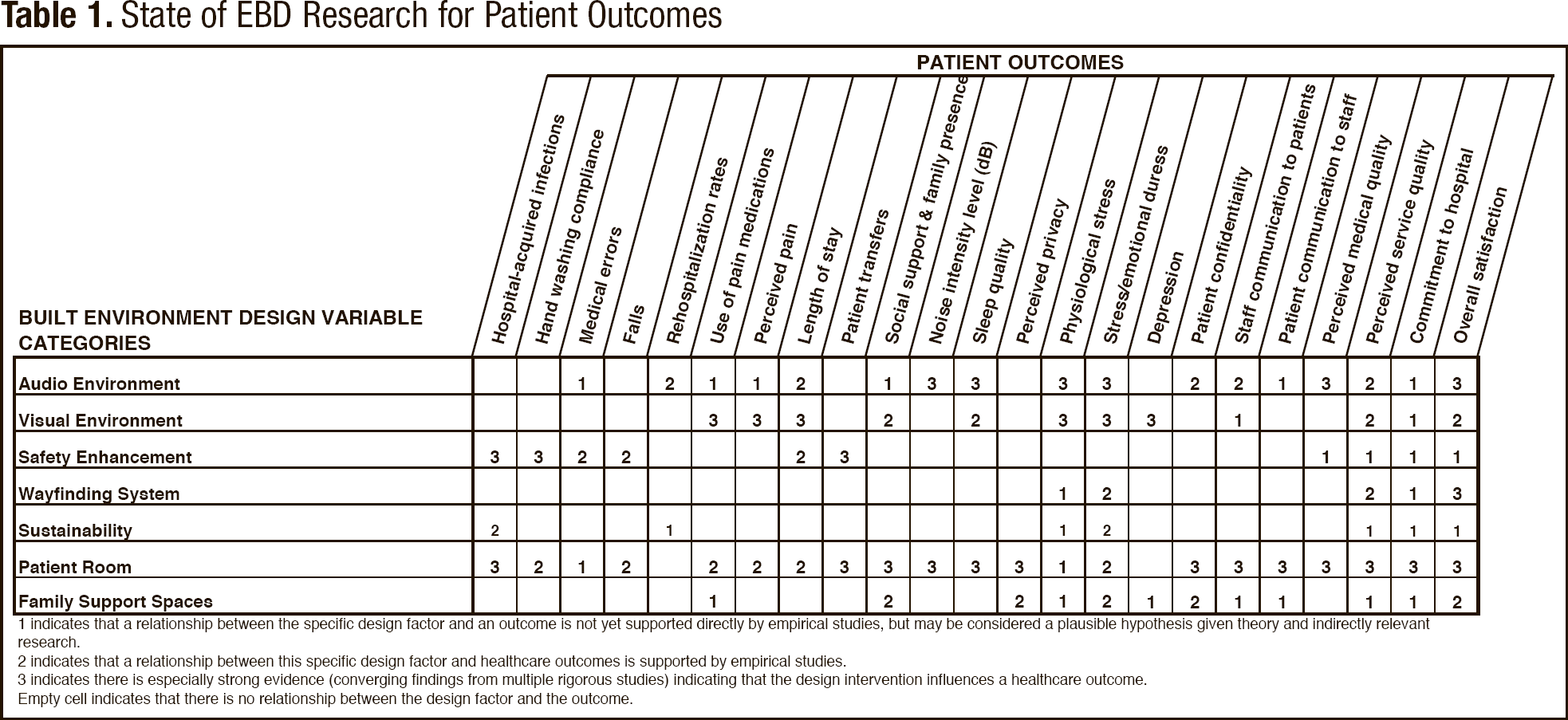
indicates that a relationship between the specific design factor and an outcome is not yet supported directly by empirical studies, but may be considered a plausible hypothesis given theory and indirectly relevant research.
indicates that a relationship between this specific design factor and healthcare outcomes is supported by empirical studies.
indicates there is especially strong evidence (converging findings from multiple rigorous studies) indicating that the design intervention influences a healthcare outcome. Empty cell indicates that there is no relationship between the design factor and the outcome.
State of EBD Research for Family Outcomes
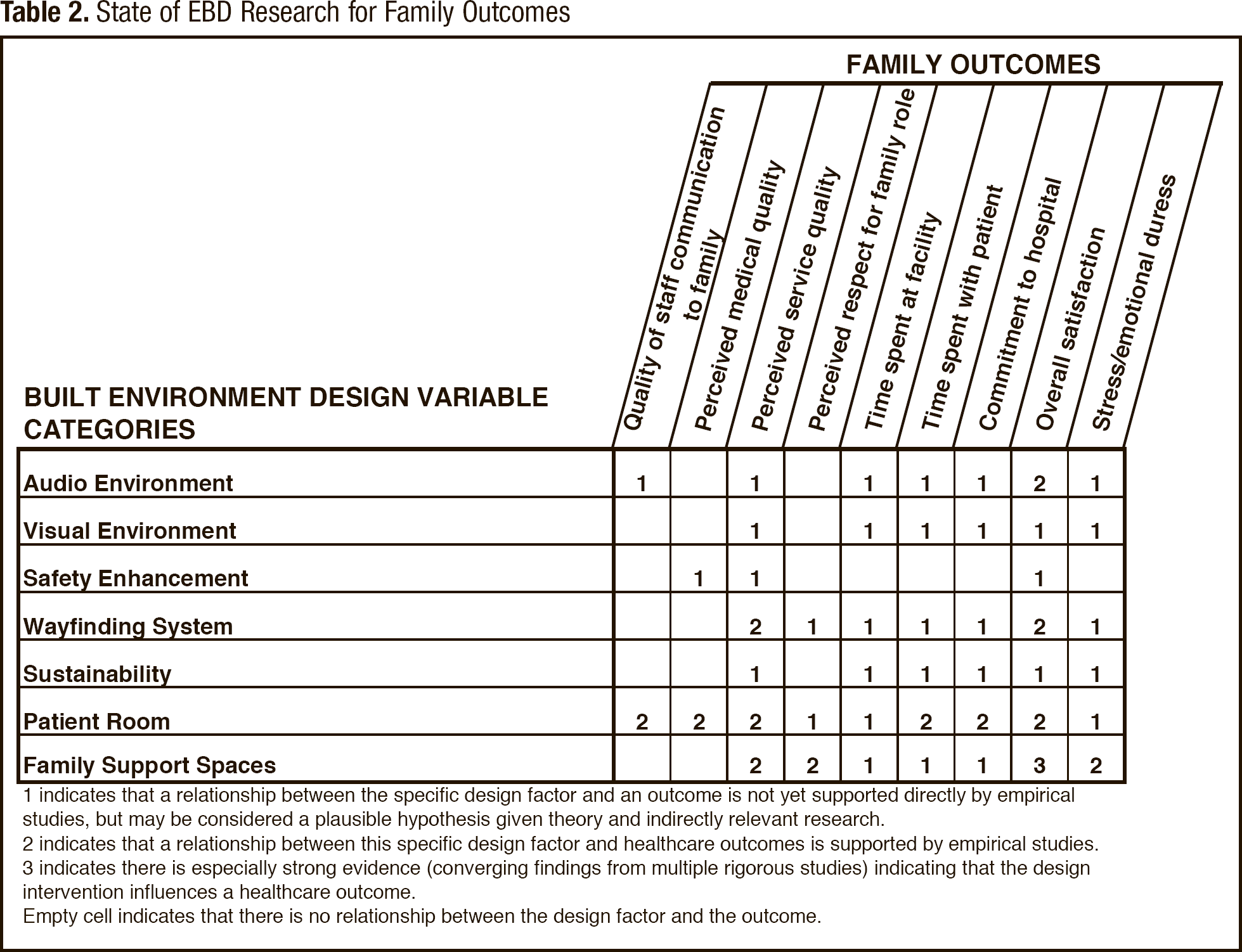
indicates that a relationship between the specific design factor and an outcome is not yet supported directly by empirical studies, but may be considered a plausible hypothesis given theory and indirectly relevant research.
indicates that a relationship between this specific design factor and healthcare outcomes is supported by empirical studies.
indicates there is especially strong evidence (converging findings from multiple rigorous studies) indicating that the design intervention influences a healthcare outcome.
Empty cell indicates that there is no relationship between the design factor and the outcome.
State of EBD Research for Nurses and Other Staff Outcomes
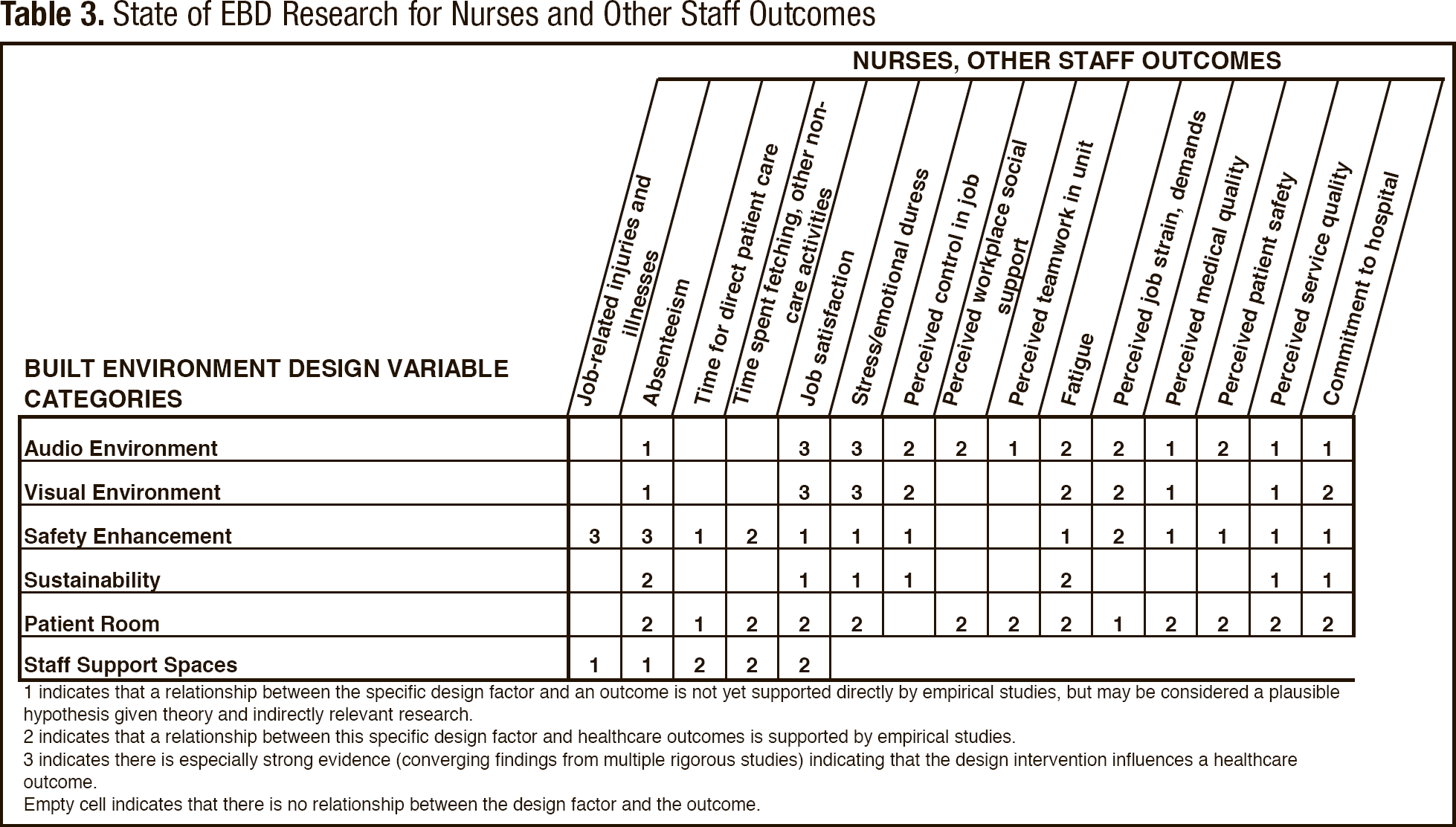
indicates that a relationship between the specific design factor and an outcome is not yet supported directly by empirical studies, but may be considered a plausible hypothesis given theory and indirectly relevant research.
indicates that a relationship between this specific design factor and healthcare outcomes is supported by empirical studies.
indicates there is especially strong evidence (converging findings from multiple rigorous studies) indicating that the design intervention influences a healthcare outcome.
Empty cell indicates that there is no relationship between the design factor and the outcome.
State of EBD Research for Physician Outcomes
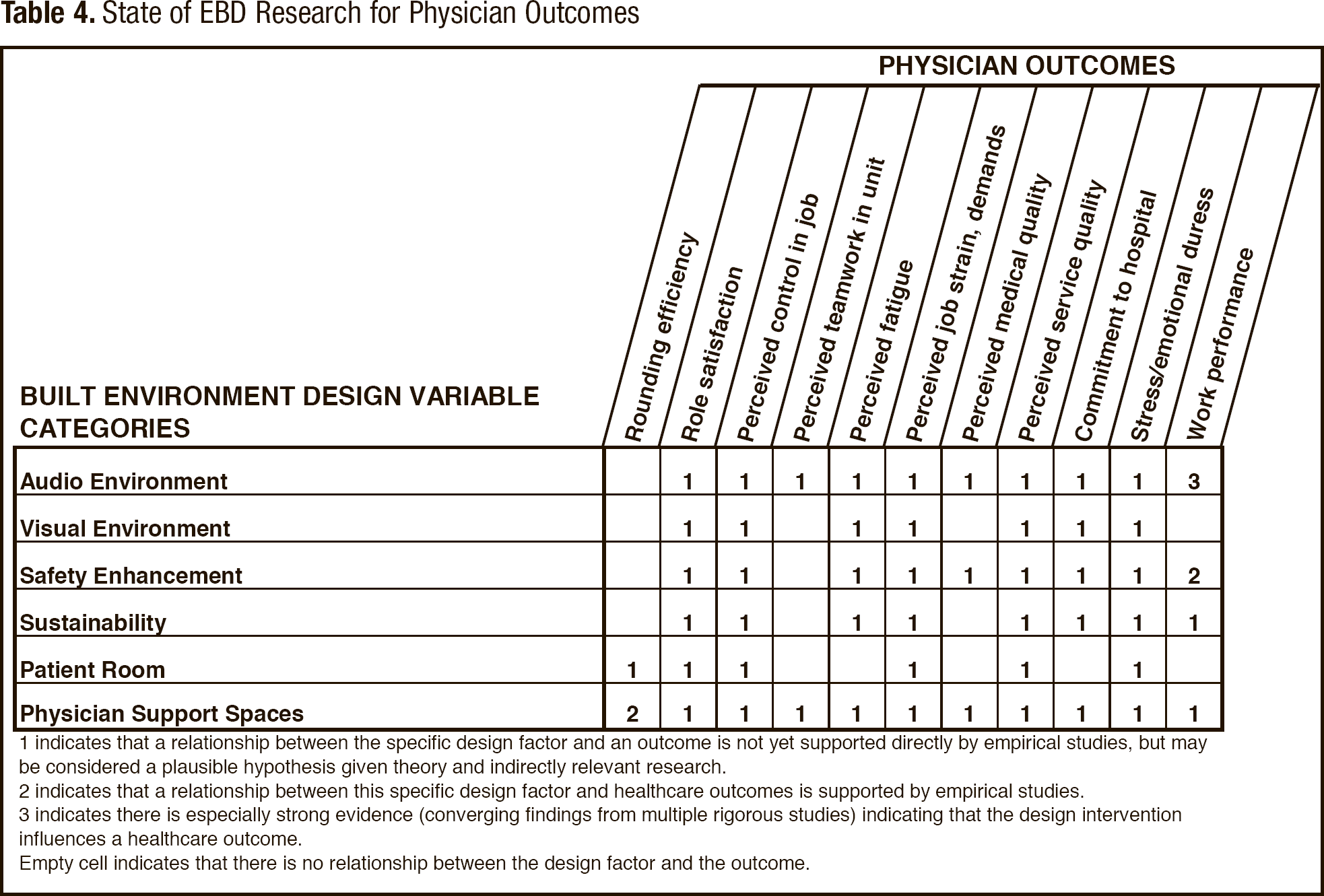
indicates that a relationship between the specific design factor and an outcome is not yet supported directly by empirical studies, but may be considered a plausible hypothesis given theory and indirectly relevant research.
indicates that a relationship between this specific design factor and healthcare outcomes is supported by empirical studies.
indicates there is especially strong evidence (converging findings from multiple rigorous studies) indicating that the design intervention influences a healthcare outcome.
Empty cell indicates that there is no relationship between the design factor and the outcome.
State of EBD Research for Organizational Outcomes
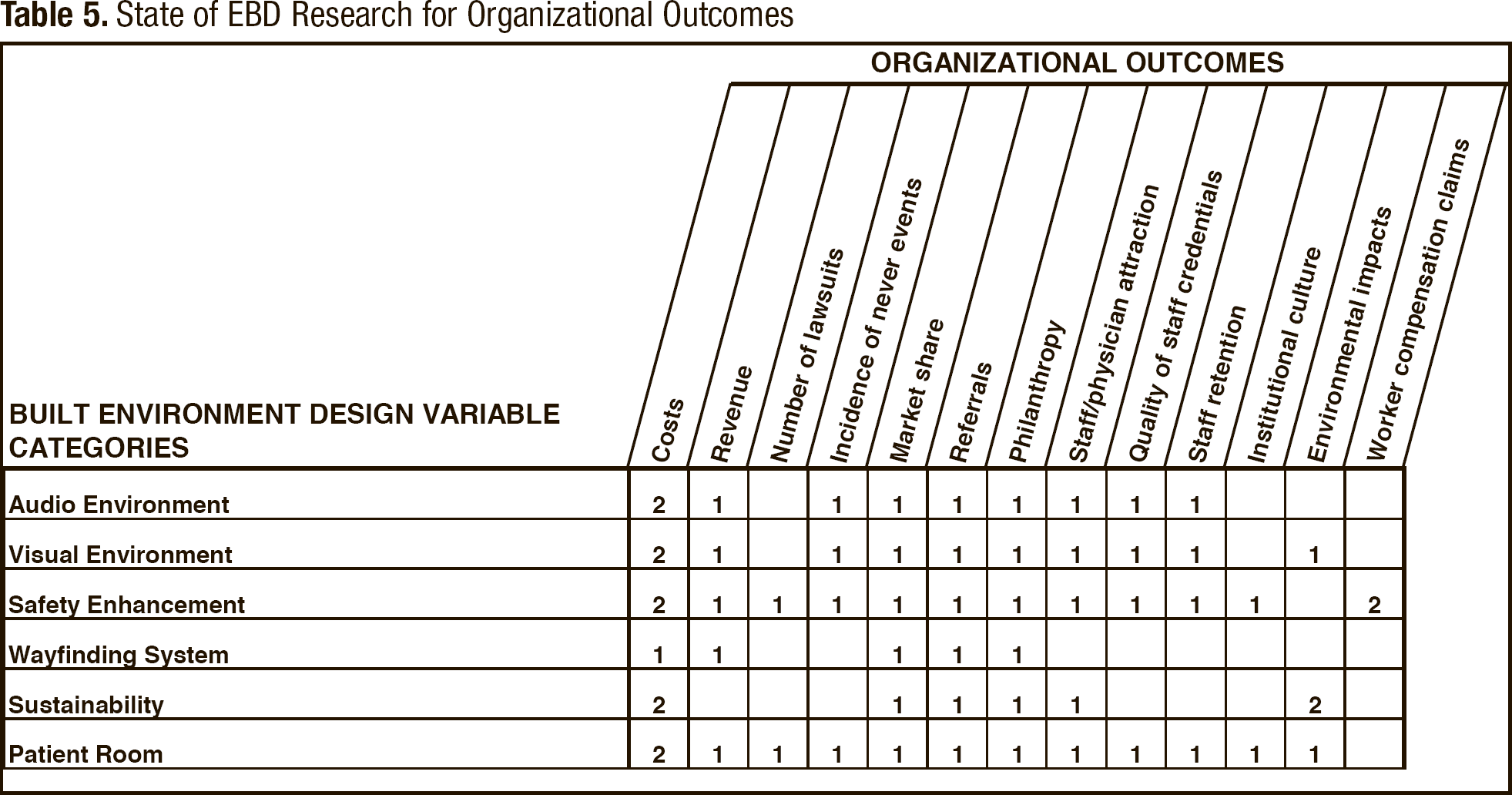
The abridged matrices contain cells representing an intersection or potential relationship between environmental variable categories (listed in rows) and a particular participant or organizational outcome (listed in columns). Each cell reflects the authors' assessment of the strength of current evidence supporting a specific relationship. Some cells are blank, indicating no plausible theoretical or empirical basis for proposing a relationship at this time. The other cells contain a 1, 2, or 3, denoting the assessment of a plausible or demonstrated relationship:
A 1 indicates that a relationship between an environmental variable category and an outcome is not yet supported empirically but can be considered a plausible hypothesis given theory and indirectly relevant research from related fields (such as health psychology, environmental psychology, healthcare safety, and service quality). A 2 denotes that a relationship between a variable category and an outcome is directly supported by empirical research. A 3 indicates especially strong evidence (converging findings from multiple studies) that the variable category influences an outcome.
Only environmental variable categories that have some relevance to an outcome (i.e., one or more cells containing a number) are included in a particular matrix.
The process for evaluating the strength of evidence for relationships drew on a detailed review of the research literature on evidence-based healthcare design (Ulrich et al., 2008) and from empirical studies published since the review. Criteria for identifying studies as relevant and scientifically sound for the evaluation included the following: the study should be empirically based and examine the influences of one or more environmental variables on outcomes; and the study should be published in a peer-reviewed research journal. For each study, the evaluation process also considered the quality of the research design and methods, and greater weight was accorded to evidence obtained from studies having control groups or comparison conditions. Qualitative studies without controls were excluded.
The strength of evidence indicating environment/outcome relationships has developed rapidly and substantially in recent years (Ulrich et al., 2008). The total number of pertinent empirical studies may now exceed 2,000 articles. The quality of evidence also has been enhanced by advances in understanding the mechanisms or pathways by which environmental variables affect outcomes, ranging from infection, pain, and depression to patient satisfaction and staff lifting injuries (Ulrich et al., 2008).
The appearance of a growing number of randomized controlled trials (RCTs), considered the strongest research design (Jadad & Enkin, 2007), suggests a trend of increasing scientific rigor. For example, Table 1 reflects findings from several RCTs that examined the effects of randomly assigning a nature distraction on patient intake of pain drugs and/or reported pain (e.g., Diette, Lechtzin, Haponik, Devrotes, & Rubin, 2003; Lee et al., 2004). The strength of the authors' evidence judgments also is informed by numerous quasi-experimental studies, several hundred observational studies with controls, and a few well-conducted epidemiological investigations.
The majority of environment/outcomes studies, however, are not well controlled, because most design changes in healthcare facilities involve multiple environmental variables simultaneously (Ulrich et al., 2008). This creates confounding variables that blur the independent effect of the specific environmental factor of primary interest. The approach employed here was conservative and revised the evidence strength ratings downward for studies that were difficult to evaluate clearly.
Finally, it was deemed that the quality of evidence supporting some environment/outcome relationships is strengthened by consistent patterns of findings derived from multiple studies carried out in different sites (Ulrich et al., 2008). For example, research has consistently found that high noise levels worsen patient outcomes, and several investigators working in different countries have reported a significant association between single-bed patient rooms and lower infection rates. Validity and quality are strengthened when findings are consistent, in accord with hypotheses based on established theory (for example, stress and pain theories), and compatible with the growing knowledge base concerning mechanisms by which environmental factors affect outcomes (for example, infection transmission mechanisms).
Priorities for the Future
The information contained in the matrices (Tables 1 through 5) offers a detailed overview of the current status of environment/outcome research, revealing many issues for which sound findings are available and numerous areas that lack empirical studies. Examination of the research strength ratings across the five matrices supports the following broad conclusions:
The majority of strong healthcare facility design studies have focused on patient outcomes (Table 1). Few reliable studies have examined the influence of design factors on family outcomes (Table 2). Compared to patient-outcome research, a limited amount of environmental research has addressed nonphysician staff outcomes (Table 3). Little rigorous research is available concerning the possible relationships between environmental variables and physician outcomes (Table 4). Empirical research is lacking for most types of organizational outcomes with the exception of some studies on costs (Table 5).
Despite a substantial increase in the quality and quantity of EBD research in recent years (Ulrich et al., 2008), the matrices reveal major knowledge gaps. The ratings suggest numerous promising topics for future research. In this regard, the cells containing “1” merit attention because they denote environment/outcome relationships that have not yet been studied empirically but represent plausible hypotheses in light of theory and indirectly relevant research. Also, EBD research needs to encompass to a much greater degree ambulatory care, long-term care, and other nonacute healthcare facilities.
Table 6 presents priority research questions for each of the five key stakeholder groups represented in Tables 1 through 5: patients, family, nonphysician staff, physicians, and healthcare administrators. These research priorities are not intended to be a comprehensive listing. The abridged matrices in Tables 1 through 5 contain approximately 200 cells with “1” ratings, suggesting that many additional issues that merit research attention could potentially be included in Table 6.
Research Priorities for Key Stakeholder Groups
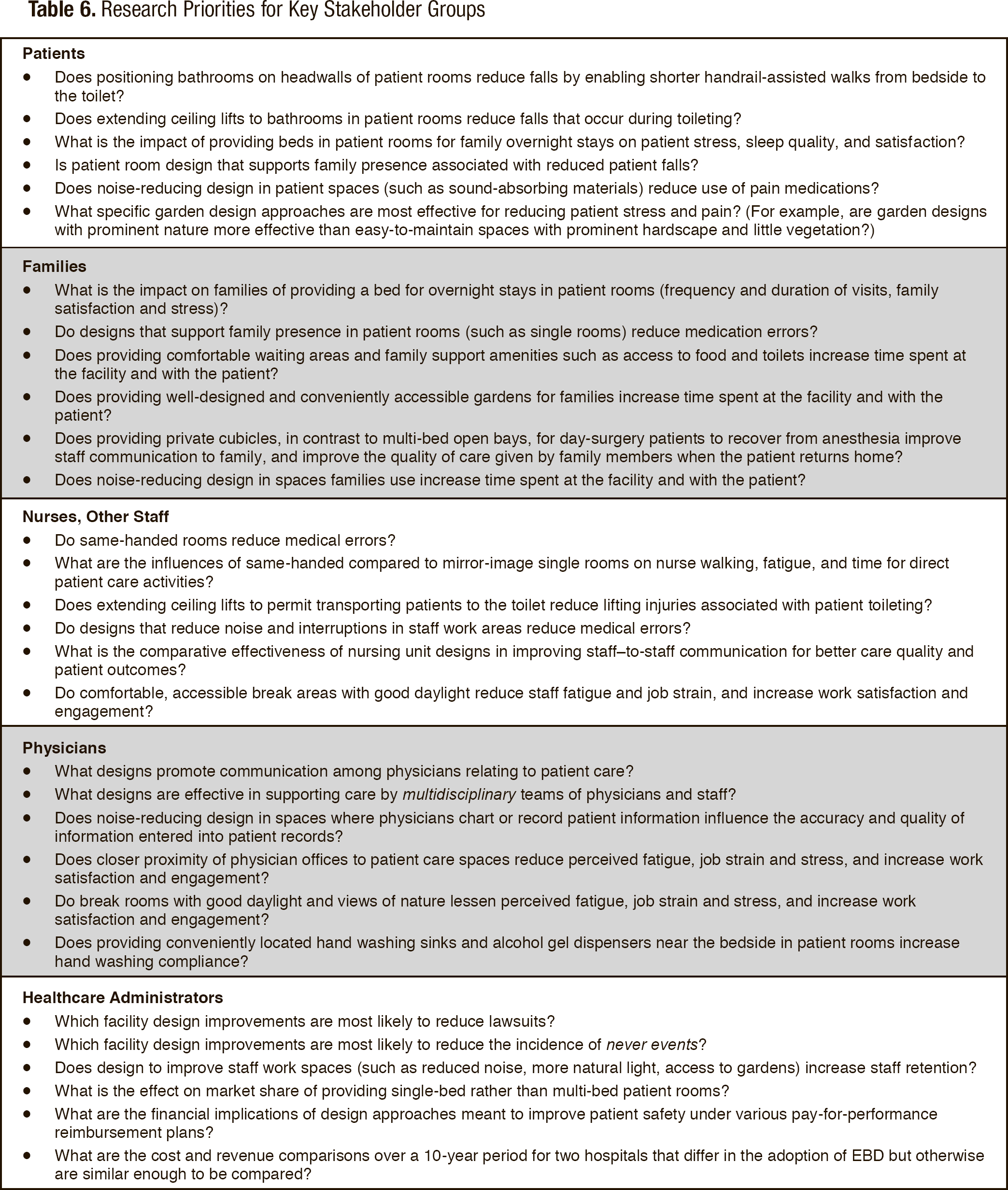
The criteria for identifying the research priority examples in Table 6 accorded particular importance to design features judged to have the potential to improve patient safety (such as increasing hand washing compliance) and reducing never events, especially falls. Apart from causing serious harm to patients, falls, errors, and infections are major concerns for healthcare administrators, because they may lead to lawsuits, increase costs, and lower revenues under performance-based reimbursement plans. An example of a priority research question related to falls is whether extending ceiling lifts to bathrooms in patient rooms reduces falls during toileting. Investigators have reported that approximately 10% to 30% of all falls occur in the toilet area (Kerzman, Chetrit, Brin, & Toren, 2004; Krauss et al. 2007; Schwendimann, 2006). Although it appears that no published research has examined the effects of extending ceiling hoists into bathrooms, it seems reasonable to hypothesize that the provision of such extended hoists might lessen the frequency of falls during toileting, and possibly also reduce staff injuries caused by manually assisting patients within bathrooms.
The authors also prioritized research that addresses the need for more rigorous study of design features—such as overnight beds or more pleasing waiting areas—intended to increase family presence and social support for patients. Additionally, weight was given to design features that could lessen staff and physician fatigue and job strain, enhance work satisfaction, and possibly increase employee retention—all important concerns for administrators.
Finally, a high priority was accorded to research that would shed light on the effectiveness of design features in improving communication among clinicians serving the same patient. The need for such research is pressing, given the mounting evidence that better communication among clinicians is associated with improved quality of care and safety (Baggs, Ryan, Phelps, Richeson, & Johnson, 1992; Gittell et al., 2000; Puntillo & McAdam, 2006; Zwarenstein, Goldman, & Reeves, 2009).
The conceptual framework proposed in this paper (Figure 1) is intended as a step toward improved understanding of the myriad relationships among the healthcare built environment and participant and organization outcomes. Although parts of the framework are supported by considerable empirical evidence (for example, certain patient outcomes), the large number of important issues that remain unresearched or under-researched is sobering. Improving healthcare requires improving the built environment in which healthcare is delivered; yet what is known about EBD pales in comparison to what is unknown. To the extent that researchers address these knowledge gaps, theory in EBD will continue to develop and mature, and the field will increasingly be underpinned more broadly yet deeply by reliable knowledge flowing from an expanding body of empirical research.
Footnotes
Acknowledgment
The authors are grateful for the contribution of James W. Varni, Professor and Vice Chair for Research, Department of Pediatrics, College of Medicine, and Professor, Department of Landscape Architecture and Urban Planning, College of Architecture, Texas A&M University, who collaborated with Roger Ulrich, Leonard Berry, and Janet Parish on the development of the initial versions of the conceptual framework featured in this article.