
Abstract
Introduction
The Institute of Medicine (IOM, 2000, 2001) and The Joint Commission (2009) have identified threats to quality healthcare within health delivery systems stemming from both processes and the environment. Medical error and hospital-acquired infection threaten patients' health outcomes, creating burdens beyond what originally brought them into the health system. Lighting, noise, aesthetics, ergonomics, design layout, and services within the built environment can affect patients', families', visitors', and healthcare professionals' health and experiences (Codinhoto, Tzortzopoulos, Kagioglou, & Aouad, 2009; Ulrich et al., 2008).
The Joint Commission (2009) sets forth five goals for effective facility design and management. These goals include:
Reduce and control environmental hazards and risks. Prevent accidents and injuries. Maintain safe conditions. Maintain a patient-centered environment. Reduce environmental stress.
The IOM (2000; 2001) identified variability in healthcare practices as a key contributor to poor outcomes. The basis of decision making also varies from past educational training and opinion to the best research available (Estabrooks, 1998; Estabrooks et al., 2005; IOM, 2000, 2001, 2004; Joint Commission, 2009; Pravikoff, Tanner, & Pierce, 2005; Sackett, Straus, Richardson, Rosenberg, & Haynes, 1996; 2000). Evidence based decision making is widely accepted as an essential foundation for reducing variability and promoting safe and satisfying healthcare (Sackett et al., 1996; 2000; IOM, 2000, 2001). Many disciplines within the healthcare profession have embraced the notion of evidence-based practice (EBP) (Satterfield et al., 2009). The purpose of this paper is to propose a systematic approach to incorporating evidence into the healthcare design decision-making processes.
Evidence-Based Decision Making
EBP has been defined in medicine and nursing as the incorporation of the best available research evidence with patient preferences, clinical context, and healthcare resources (Ciliska, 2005; Cullum, Ciliska, Haynes, & Marks, 2008; Sackett et al., 2000; Shaneyfelt et al., 2006). Evidence-based decision making becomes the process for achieving EBP and it involves asking a focused answerable question, acquiring evidence, critically appraising the evidence, applying the evidence to practice, and evaluating the process (Greenhalgh & Macfarlane, 1997; Sackett et al., 2000; Shaneyfelt et al., 2006).
EBP models provide a vehicle for implementing EBP. Many models for systematically moving evidence into practice have been described. Proponents define a transdisciplinary approach to evidence-based decision making (Baumbush et al., 2008). The structures and processes espoused by the various models vary based on theoretical perspectives of originators but all have the main steps of evidence-based decision making incorporated within them (Greenhalgh & Macfarlane, 1997; Baumbush et al., 2008).
Evidence-Based Design
The specialty of built environment design is embracing evidence-based decision making (Cesario, 2009; Hickey, 2010; Hignett & Lu, 2010; Joseph, 2006; van de Glind, de Roode, & Goossensen, 2007). Evidence-based design is informed by multiple perspectives, including those of architects, engineers, interior designers, healthcare professionals, patients, regulatory guidelines, and research evidence. The health, safety, and satisfaction of both patients and caregivers comprise the broad focal areas of space design (Cesario, 2009; Hignett & Lu, 2010; Joseph, 2006; van de Glind et al., 2007).
The research literature demonstrates the connections between the physical and social environment and the promotion of health, safety, and effectiveness outcomes for patients and caregivers. Aspects of environmental design include lighting, noise, aesthestics, ergonomics, and room and unit layout (Codinhoto et al., 2009; Ulrich et al., 2008). Among the patient outcomes affected by environmental design are falls (Hignett & Lu, 2010); sleep disruption caused by unnatural lighting and noise (Ulrich et al., 2008); air, contact, and water transmission of infection (Ulrich et al., 2008); and stress/anxiety (Ulrich et al., 2008). Environmental causes of stress, anxiety, and work-related injury in healthcare professionals have been studied (Hignett & Lu, 2010; Joseph, 2006; Ulrich et al., 2008).
Evidence-based design has been demonstrated to improve health and safety for both caregivers and their patients.
A Systematic Approach to Evidence-Based Design
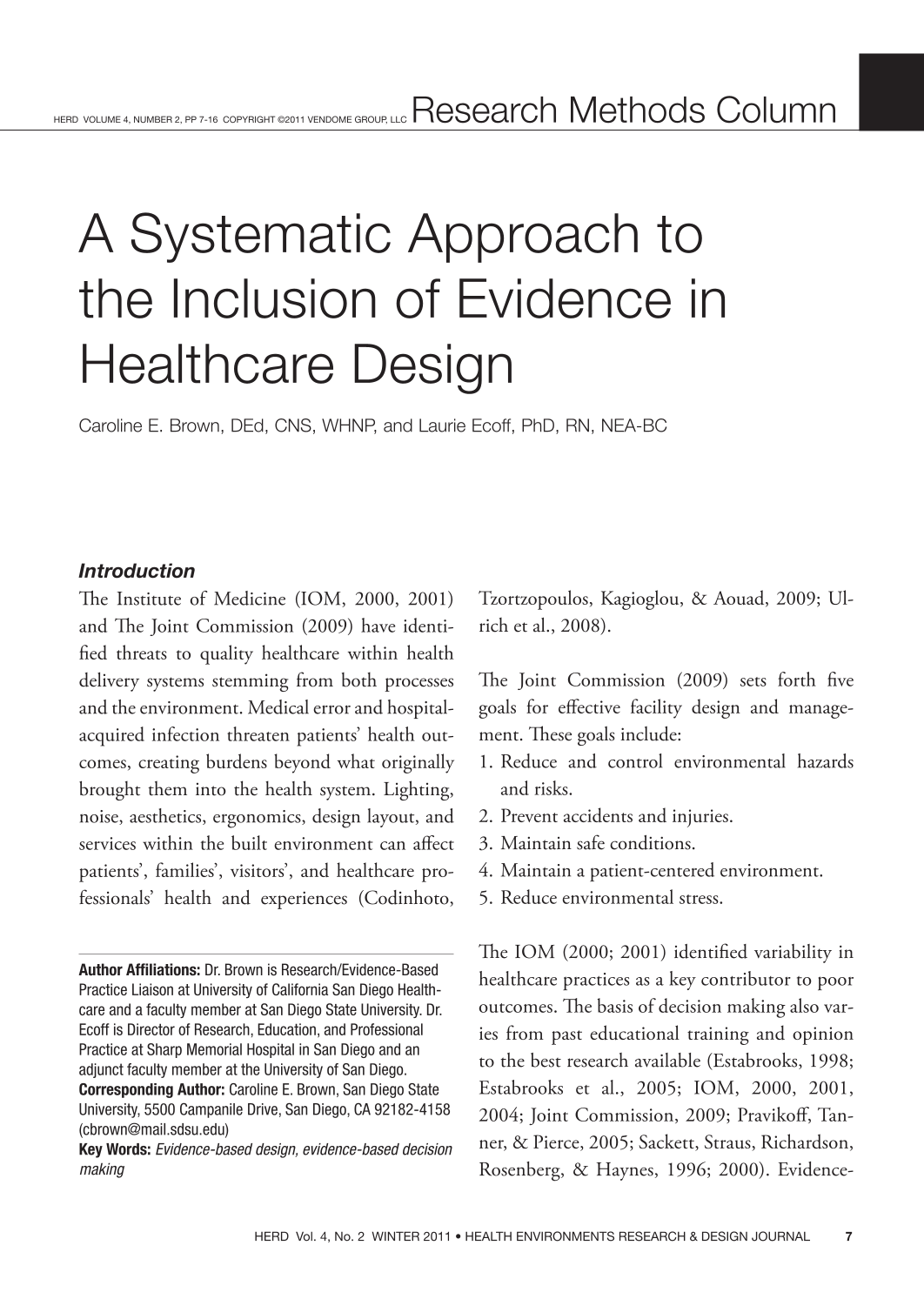
Drawing from EBP models in medicine and nursing, one may apply a systematic approach to the context of the built environment (see Figure 1). Several existing models in organizational theory, nursing, and medicine inform the proposed systematic approach to evidence-based design. Diffusion of innovations (Rogers, 2003), Rosswurm and Larrabee's model for change to EBP (1999), and the evidence-based information cycle (Hayward 2007) are the primary models that influence the proposed approach.
A systematic approach to evidence-based decision making.
The diffusion of innovation theory (Rogers, 2003) is an organizationally derived theory of particular relevance to the evidence-based design Decision-making process. It is a commonly used theoretical framework for the implementation of EBP inquiry (Greenhalgh, Robert, Macfarlane, Bate, & Kyriakidou, 2004). Diffusion is the process by which an innovation is communicated over time through a social system (Rogers, 2003). The main components of the theory include the innovation, the adopter, communication channels and patterns, time, and the organizational social system (Rogers, 2003). The characteristics (relative advantage, compatibility, complexity, trialability, and observability) of the innovation influence how it is disseminated and whether it is finally adopted or rejected (Rogers, 2003). The diffusion of innovation theory informs the implementation phase by providing a framework for how innovations spread throughout an organization. Incorporating these principles into evidence-based design implementation plans may foster successful adoption of an innovation.
The model for change to EBP developed by Rosswurm and Larrabee (1999) was derived from the authors' involvement with engaging nurses in research utilization; it is derived from organizational theory. The model involves a six-step process including assessing the need for change, locating the best evidence, appraising the evidence, designing a practice change, implementing and evaluating a pilot, and broadly implementing and sustaining the change.
The evidence-based information cycle (Hayward, 2007) is a five-step circular model that incorporates the key steps of evidence-based decision making: assessing, asking, acquiring, appraising, and applying. The elements of this model are incorporated into many models of EBP.
The proposed approach to evidence-based decision making in the context of design involved eight steps, delineated in Figure 1. The initial catalyst begins the process.
The Catalyst
The catalyst is a trigger that sets the evidence-based decision-making process in motion. The catalyst for launching an EBP project can be a problem, issue, or concern emerging from a practice or setting. A catalyst can come from a variety of sources. Some examples include newly published research or best practice, new technologies, a change in regulatory agency directives, fragmented and ineffective design settings, or outcomes in the context of the practice setting.
Research published in both the design and practice arenas addresses elements important to health facility design. Regulatory agencies provide specific regulations directing the design of healthcare facilities. The International Building Code has established directives that govern the design and construction of healthcare facilities (International Code Council, 2010). The Joint Commission (2009) has detailed guidelines for planning, designing, and constructing healthcare facilities and for maintaining the environment of care. Outcomes from practice settings relevant to the safety and satisfaction of patients and staff can signal the need to alter something within the built environment. For example, healthcare provider injury related to inadequate patient handling systems provides a catalyst for exploring ways to change the built environment to reduce the risk of healthcare provider injury. Or as another example, new research was published that validates acoustic guidelines for healthcare facilities (Solet, Buxton, Ellenbogen, Wang, & Carballiera, 2010); such research provides an impetus for healthcare facilities to look at existing practices related to sound in their facilities. Both of these examples provide a clear catalyst to initiate the evidence-based decision-making process.
Assessing
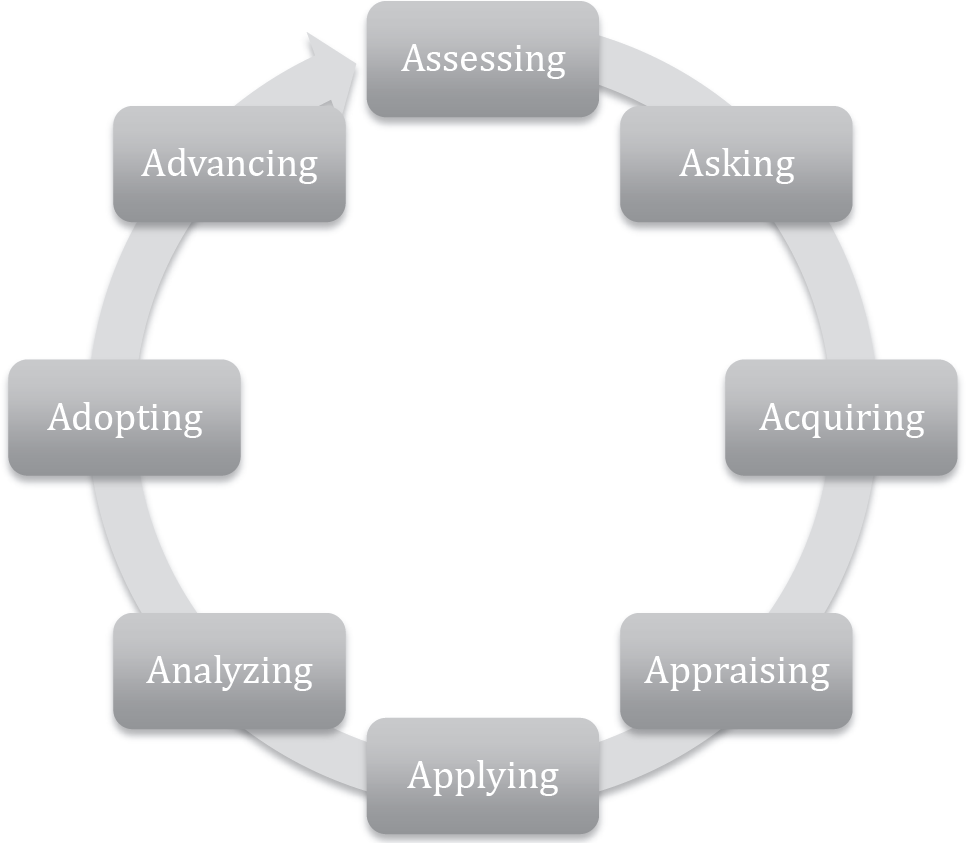
Evidence-based decision making begins with an initial assessment of the problem at hand. Assessing involves exploring the context of a given problem and gathering preliminary information about it. Such assessment uncovers the history of a problem and begins to identify key stakeholders and their understanding of and attitudes toward the problem. This process helps confirm whether a problem exists and is aligned with organizational priorities. It answers the questions “Is this a problem?” and “Why is this problem important?” Figure 2 provides a series of questions to assist in the assessment process. (See Figure 2.)
Questions for guiding assessment.
Asking
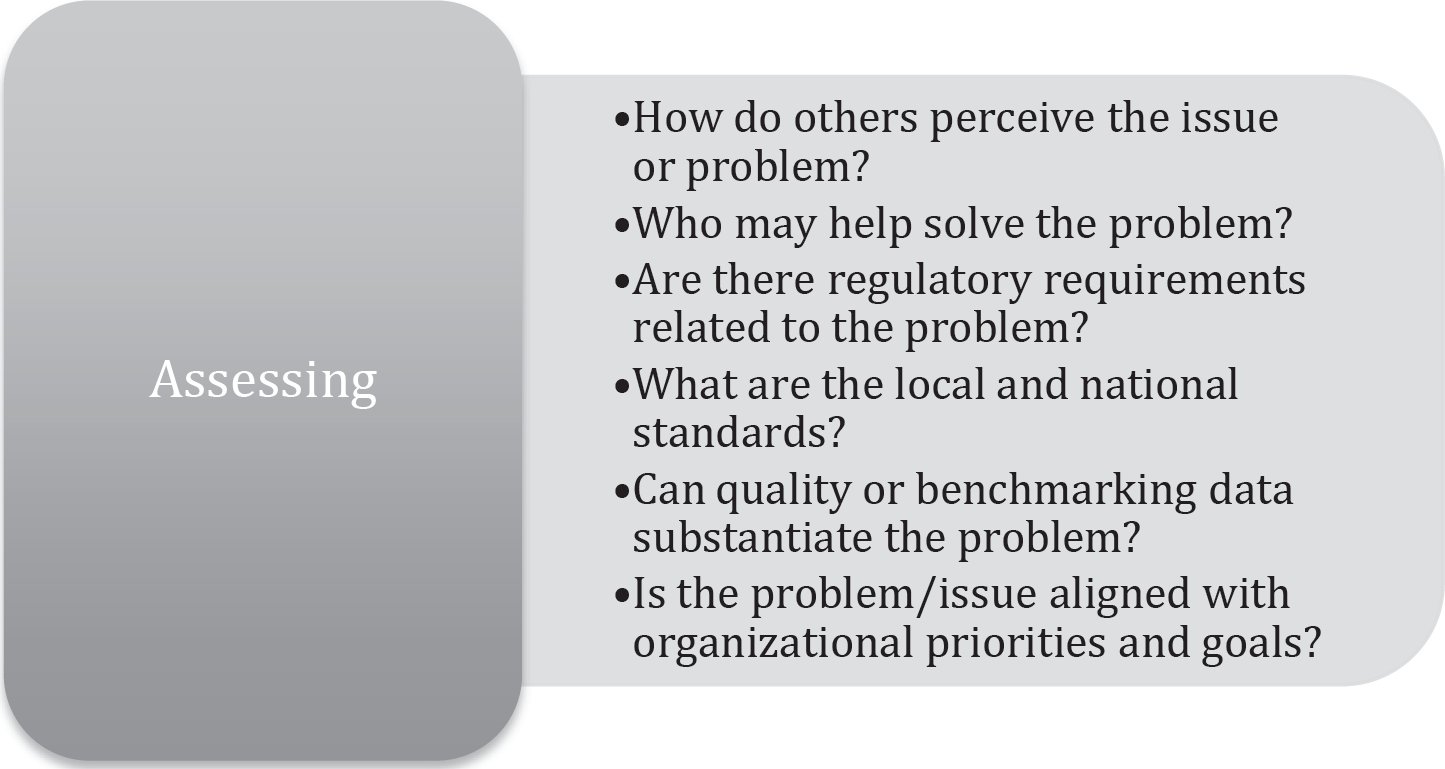
Once a problem or issue is confirmed and deemed relevant and in alignment with organizational priorities, the next step is asking the right question to lead an evidence-based inquiry. The asking process allows the scope of the problem or issue to be narrowed, facilitating a focused review of the literature (Sackett et al., 2000). Asking a good question helps ensure that a topic is searchable and answerable in the literature. In nursing and medicine the PICO(T) model is widely adopted to provide a structure for asking narrow, searchable, answerable questions. In the acronym PICO(T), P represents the population or problem, I is an intervention, C is a comparison, and O is the outcome; T is sometimes added to delineate a specific time frame.
The PICO(T) format is easily adaptable to evidence-based design (see Figure 3). In design, P could address space and occupants. I could embrace interventions within the context of the built environment. C could be an alternative design intervention or the existing elements of the current design; in nursing, C is often usual care. O could be outcomes relevant to the built environment. For example: In inpatient hospital units (P), does the implementation of acoustic guidelines (I) compared to existing units (C) result in lower decibel levels, less patient sleep disruption, and increased patient and staff satisfaction (O)? (See Figure 3.)
Asking a focused question.
Acquiring
The focused question provides a roadmap to the next step in an evidence-based design inquiry: acquiring the best evidence to answer the question. Finding the best evidence starts with your PICO question. Key words in each element of the question provide the starting point for searching databases of interest. In medicine and nursing, PubMed (www.pubmed.gov) is commonly used. Several other databases are also useful for healthcare-related searches. Among these are CINAHL, the Cumulative Index to Nursing and Allied Health Literature (http://www.ebscohost.com/cinahl/) and ERIC, the Educational Information Resource Center (http://www.eric.ed.gov/).
Meta-search engines can be used to search a number of databases at once. Several are particularly appropriate for the health professions; these include SUMsearch 2 (http://sumsearch.org/), Trip Database (http://www.tripdatabase.com:80/index.html), and SCIrus (www.scirus.com). SUMsearch 2 and Trip Database organize evidence based on evidence levels. Trip is color coded and organized by evidence level, for example, evidence-based synopsis, systematic reviews, guidelines, core primary research, extended primary research, and so forth. SUMsearch 2 organizes evidence levels into three categories: original studies, systematic reviews, and guidelines. Meta-search engines can facilitate the search process for busy professionals.
For the design field, InformeDesign (http://www.informedesign.org) serves as a searchable source of peered-reviewed journals from a broad range of disciplines that touch the design world. The InformeDesign database is organized into three topical areas: space, occupants, and issues. The Ripple database beta is another searchable source of design-oriented evidence created to support evidence-based design (http://ripple.healthdesign.org/). The Ripple database is searchable using key words. Figure 4 contains a summary of databases relevant to design.
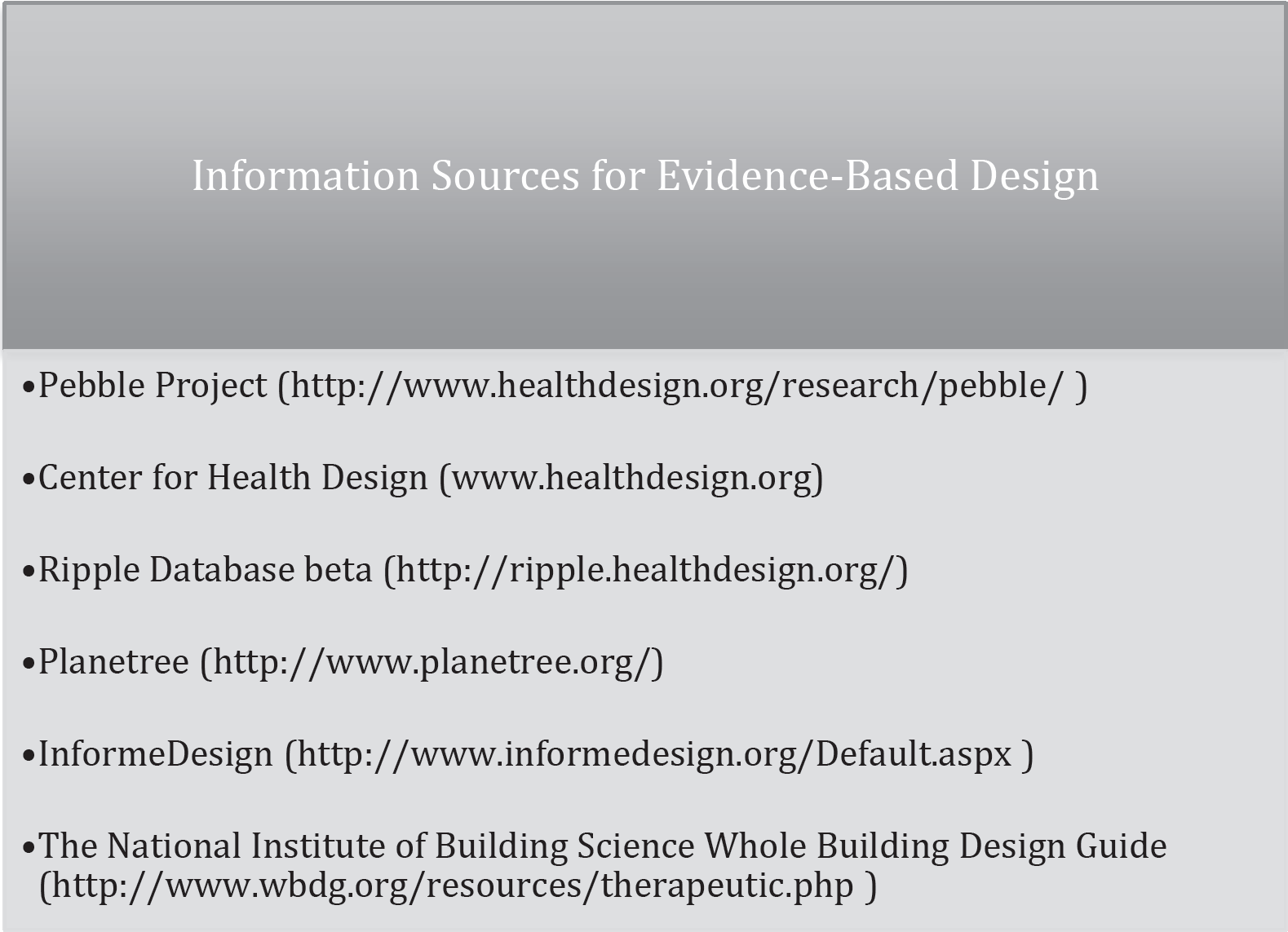
Information sources for evidence-based design.
A key issue for searching databases is looking for the highest level of evidence based on the nature of the PICO question. For example, for the PICO question “In inpatient hospitals units, does the implementation of acoustic guidelines as compared to existing practice reduce unit decibel levels, reduce patient sleep disruption, and increase patient and staff satisfaction?” Systematic reviews, meta-analysis, and randomized controlled trials represent a low potential for bias; therefore they provide the best evidence to answer the question. Conversely, qualitative research would provide the best evidence for the following question:
“What is the effect of soft music during evening hours on hospitalized elderly patients?” The nature of the design question determines the best evidence to search for. When do you stop looking for evidence? The answer to that question depends on the quality of the evidence identified to answer your PICO question.
Appraising
The next step in a systematic approach to evidence-based design is to appraise the quality of the evidence collected and determine whether to move forward with the inquiry process. The process of critical appraisal seeks to determine the value of the evidence for your problem and setting. Critically appraising the research literature centers on three questions: Are the results and conclusion of this evidence valid? Are the results reliable? and Is the evidence relevant and transferable to my setting?
Appraising the validity of quantitative evidence involves evaluating the potential for bias. The research design and sampling methodology provide insight into the potential for bias in a study. Appraising the reliability of quantitative research involves evaluating the adequacy of the sample size and the actual results of the study. Qualitative research is also appraised by evaluating the trustworthiness of the study. Appraising applicability centers on evaluating the potential fit between the sample characteristics described in the body of evidence and your population.
The appraisal process should end with a summary synthesis of the evidence, which clearly articulates the search strategies used. Key “take-away” points should also be delineated and clearly referenced. The summary synthesis and take-away messages provide the inquiry team with a starting point when they share their conclusions with others.
A decision to proceed to the application of the evidence is made when an exhaustive search for evidence yields nothing new. The levels and the quality of the evidence found lead the team to draw a preliminary conclusion. Typically one of three conclusions can be drawn from the evidence: (1) A reliable and valid body of evidence exists that is applicable to my population and/or setting; (2) Inconclusive evidence exists; or (3) Little or no evidence exists. When high-quality research does not exist, the emergent gap in evidence provides justification to design a research study. If inconclusive evidence exists, the team can continue to acquire evidence and broaden its search strategy or develop research. If an adequate body of evidence exists, the team can proceed with applying it.
Applying
Applying evidence to practice varies depending on the availability of valid reliable research to answer your question. When high-quality research exists, it should be balanced with stakeholder values and designers' expertise to create an implementation plan. Albert Einstein once said, “Information is not knowledge,” and this rings true in evidence-based decision making. Clinician expertise, patient preferences, and healthcare resources have an important place in evidence-based medicine (Cullum et al., 2009; Sackett et al., 2000).
Moving forward with the evidence-based decision-making process, the team develops recommendations, specifies measurable outcomes, and creates an implementation plan. Practice recommendations are based on the synthesis of the evidence and take-away messages. Measurable outcomes that specify data sources and collection tools are delineated. Key stakeholders are engaged in the process of creating an implementation plan. Stakeholders possess a unique perspective and may foresee challenges the team might otherwise overlook. The implementation plan should be incremental, allowing for short-term as well as long-term successes.
Analyzing
Analyzing involves answering the questions “Did you accomplish what you set out to, and were there any unintended consequences from what you did?”. Typically baseline data are collected before implementing a change and again at intervals following the change; the difference between baseline and outcome data provides a means to analyze the effectiveness of your evidence-based initiative. The process is enhanced when reliable and valid instruments are used in the analysis process.
Adopting
Adopting moves your project ideas to a broader scale. For example, if you implemented a hardwired patient handling system within one unit of a hospital as a pilot that resulted in positive outcomes, that unit design may be considered as a model throughout the hospital or health system.
Advancing
Advancing involves sharing your findings and lessons learned with others. Dissemination of your findings occurs in local, national, and international contexts. The process of sharing may involve presenting or publishing your findings. Advancing facilitates growth in the knowledge base related to your area of inquiry.
Conclusion
The healthcare environment and facilities exert an influence over physical and psychosocial outcomes for patients, families, visitors, and healthcare professionals (Codinhoto et al., 2009; Ulrich et al., 2008). A systematic approach to evidence-based decision making offers both structure and process for evidence-based design. Evidence-based decision making fosters integration of the best available evidence, design expertise, and stakeholder preferences within available healthcare resources. Outcomes are articulated early in the process and used to evaluate the effectiveness of a given design project. Dissemination of project outcomes through mechanisms such as the Pebble Project® foster sharing and contributes to the overall availability of evidence related to evidence-based design.