
Abstract
Objective:
The purpose of this investigation was to identify safety and efficiency-related design features for inclusion in operating room (OR) construction documents.
Background:
Organizations are confronted with an array of challenges when planning an OR, including inefficiencies in operations, adverse events, and a variety of innovations to choose from. Currently, techniques that can be used in design practice and to inform design decision making for implementable OR solutions are limited.
Methods:
The project team used a structured focus group format with mixed methods to solicit 19 varying surgical team members' reactions to a three-dimensional video mock-up of a proposed OR. Data from the 19 participants were analyzed using stepwise multiple regression and content analysis of open-ended responses.
Results and Discussion:
Results demonstrate that several features of the proposed OR design predict meaningful outcomes, including flexibility and satisfaction with the OR setup, adverse event prevention, team performance, and distractions and interruptions. Participants' suggested solutions include universal booms to support anesthetic and perfusion capabilities, a fixed circulating nursing workstation that faces the patient and is at the foot of the operating room table, a wall-mounted monitor across from the surgeon, and wiring to support a touch-screen control arm in OR surgical fields.
Conclusions:
Findings from structured focus groups with mixed methods lead to implementable design solutions for construction documentation. The expeditious qualities and objectivity of the format are value-adds to the design decision-making process. Future research should use various techniques such as virtual technologies and building information modeling.
Introduction
Because they are the most profitable services, surgical and interventional procedures are the engines of a hospital (Cima et al., 2011). Outpatient procedures increasingly constitute the bulk of profit (The Advisory Board Company, 2006). However, the profitability of surgical and interventional procedures can quickly be offset by exorbitant costs associated with construction, operational inefficiencies, and safety risks. Consequently, a properly planned and designed operating room (OR) setting should contribute to efficient operations, prevent unnecessary costs, and mitigate injury to patients and staff. What follows are efficiency- and safety-related concerns impacted by the planning and design of OR settings. These concerns informed an exploratory pilot project to facilitate design decision making during the construction documentation of a proposed OR set-up.
Cost and Efficiency
ORs come with several challenges, one being their cost. Park and Dickerson (2009) estimated the cost of running an OR at their institution to be upwards of $1,300 an hour. The cost of running an OR pales in comparison to the opportunity cost and lost revenue for an OR that is not utilized. Given the financial implications related to ORs, healthcare organizations considering their construction or renovation assign a high priority to identifying the ideal mix of OR types, efficiency in OR operations, and the number of ORs.
Material and supply costs account for approximately 47% of an OR budget (Souhrada, 1999). An OR with 20% of its budget in inventory has millions of dollars stored away that are not generating revenue, that are taking up space, and that may expire prior to use. There are three systems for supply distribution. First, supplies can be kept at the point-of-service. Second, an organization can use a case-cart system operated by a central sterile department. Carts of instruments and supplies are prepared prior to surgery. A case-cart system is more efficient than a point-of-service system (e.g., it decreases supply costs because inventories are not duplicated) and can be easily tracked. Third, a hybrid of point-of-service and case-cart systems can be used. With a hybrid system, some rarely accessed items are kept in the core of the OR for nurses to retrieve or in bins attached to case carts.
Safety
ORs can be unsafe. Researchers have argued that approximately one-half of hospitals' adverse events are associated with surgical procedures conducted in ORs (Gawande, Thomas, Zinner, & Brennan, 1999; Gawande, Zinner, Studdert, & Brennan, 2003; Leape et al., 1991). The majority of errors in healthcare settings result from latent conditions in the environment (Reiling, 2007). These latent variables set the physical, contextual, and organizational stage for every surgical procedure. They include environmental factors, management decisions, procedures, policies, teamwork, and communication (Wiegmann, El Bardissi, Dearani, Daly, & Sundt, 2007). Errors are also affected by distractions and interruptions, the complexity of a case, long surgery durations, personnel shortages, inefficient scheduling and supply management, fragmented communication among teammates, poor team situational awareness, the complexity of technology, and a surgical team's lack of experience (Barach et al., 2008; Catchpole, Mishra, Handa, & McCulloch, 2008; Cleary, Chung, & Mun, 2004; Girotto, Koltz, & Drugas, 2010; Sudan, 2009). In addition, a higher rate of minor errors during a procedure depletes team members' abilities to compensate for additional errors (Wiegmann et al., 2007).
Catchpole et al. (2007) found that, on average, 9.9 minor errors occur per surgery. Barach et al. (2008), in an observational study of 102 pediatric cardiac surgeries, discovered that on average 1.2 major adverse events and 15.3 minor adverse events occurred during a surgical procedure. An additional finding of the study was that case complexity and surgery duration were statistically significant predictors of major adverse events. Surprisingly, the occurrence of minor adverse events was independent of case complexity, case duration, or team experience.
The Joint Commission has argued that one of the predominant common factors in the occurrence of adverse events is communication failure (The Joint Commission, 2011). Common communication failures in ORs include poor timing of communication, missing or inaccurate crucial information, lapses in equipment coordination (e.g., equipment at incorrect setting or not turned on), failure to keep team members updated on progress, exclusion of key individuals from a communication, and failure to resolve an issue during a communication (Halverson et al., 2011; Lingard et al., 2004). These communication failures can interrupt information and work flow within the OR and, in turn, errors may occur (El Bardissi, Wiegmann, Henrickson, Wadhera, & Sundt, 2008; Wiegmann, El Bardissi, Dearani, Daly, & Sundt, 2007). For example, Barach and colleagues (2008) found that minor adverse events were predicted by coordination and communication failures. In addition, Mazzoco et al.'s (2009) observational research in an OR setting revealed that less information sharing by team members increased the odds of case morbidity and mortality.
Halverson et al. (2011) performed an observational study of OR cases and concluded that communication failures contributed to inefficiencies and delays. Furthermore, communication failures increased tension among members of the OR team. Hull, Arora, Kassab, Kneebane, and Sevdalis (2011) demonstrated that increased tension among team members narrows team members' focus from the team to the self. As such, communication failures may induce stress that threatens teamwork. The disintegration of teamwork could create a risk for errors.
Surgical-site infections (SSIs) are the third leading cause of hospital-acquired infections (Smyth & Emmerson, 2000). One study found that the cost of a single, preventable SSI can result in 11 additional days of hospitalization at a cost of $27,000 for each patient (Sohn & Steele, 2009). Risks for contamination in the OR include personnel behavior and decontamination practices, the number of personnel in the OR, the duration of a surgical procedure, personnel's clothing, surgical instruments, hand hygiene, ambient air, environmental surfaces (e.g., horizontal versus vertical; porous versus smooth), equipment, patient temperature (e.g., risk of hypothermia), the integrity of personnel's gloves (e.g., punctures in gloves), and the skin flora of patients and staff (Ayliffe, 1991; Demir, 2009).
Innovations for Improved Efficiency and Safety
Several innovations in OR design address the challenges of OR efficiency and safety. These include ongoing advances in OR equipment, ambient conditions, and information flow. Ceiling-mounted versus floor-mounted equipment within the OR is only one contentious issue. Over time, ceiling-mounted systems collect dust that could fall and cause infections (Nollert & Wich, 2009). However, ceiling-mounted systems cover the whole patient without having to adjust a table. Table adjustment can be a dangerous undertaking given that many tubes and lines have to be shifted. From a workflow standpoint, a hybrid of ceiling-mounted and floor-mounted equipment is logical. For example, a floor-mounted C-arm would be less likely to interfere with other equipment because it can be brought in from the patient's side (Nollert & Wich, 2009).
Evidence for unique lighting solutions within the OR that prevent team members' fatigue have been available since the 1930s. Sheehan (1950) found in nature blue, green, and yellow light and wall colors that would prevent surgeons from experiencing eyestrain in response to direct and reflected glare in the OR. Anecdotal evidence from recent applications of Sheehan's concepts to the OR indicates that green lighting during surgical procedures reduces eye fatigue and improves image quality on video screens (Gordon, 2007).
Integrated ORs that incorporate the latest in information and telepresence technologies contribute to improved information flow, communication, teamwork, and situational awareness in the OR. Telepresence technologies allow participants to engage in live, face-to-face communications over a computer network. In recent years, OR dashboards or “Walls of Knowledge” have been incorporated into ORs to accommodate a variety of functions, including telecollaboration with colleagues in remote locations, preoperative checklists, equipment monitoring, physiological monitoring (e.g., urine output, blood loss), elements of the patient record (e.g., allergies, blood pressure, medications), process log with timeline and time stamps, handoff and time-out verifications, identification of who is in the OR, and postoperative needs (Bland, 2010; Buzink, van Lier, de Hingh, & Jakimowicz, 2010; Cleary et al., 2004; Greene, 2006; Levine et al., 2005).
Hybrid ORs are analogous to acuity-adaptable inpatient rooms in that they can be used for a multiplicity of procedures without having to transfer a patient. Typically, hybrid ORs combine interventional and open-surgery capabilities in one room by accommodating a variety of imaging technologies including C-arms and magnetic resonance imaging (Nollert & Wich, 2009). Consequently, hybrid ORs can accommodate complex cardiovascular procedures including transcatheter valve replacement and repair, hybrid coronary revascularization, and stent/graft placement. Future research of hybrid ORs will dictate whether they become best practice for the healthcare industry.
Structured Focus Group Format
Focus groups involve a small group of individuals who are interviewed together to identify their opinions or feelings on a particular issue or product (Aubel, 1994). Traditional focus groups are routinely conducted by designers with facility users to receive feedback about the design of an existing facility or future design interventions. Moreover, traditional focus groups have been used in research involving operating room staff. For example, Gillespie, Chaboyer, Wallis, Hsiao-yun, and Werder (2009) conducted three focus groups with 27 OR nurses to examine OR nurse competencies. The focus groups were audio recorded, transcribed, and subjected to a thematic analysis. However, traditional focus groups implemented during the design process have been criticized because participants may provide unconstructive complaints, instinctively convey negative reactions, and ignore operations and challenges outside of their department (Chambers, 2009).
To resolve the limitations of traditional focus groups, Watkins, Lorenz, and Naos (2010) emphasize the value of objective research findings to empower focus groups and design decision making. Structured focus group formats more than fulfill this requirement. The format is democratic in that every participant in the focus group has an equal opportunity to air concerns and ideas. Case in point: a study by Bromley and Fischer (2000) showed that a structured focus group format elicited more information from the quieter group members when compared to a traditional focus group format. Moreover, a structured focus group format may lead to less time spent on off-topic discussions (Bromley & Fischer, 2000). Participants may be more focused compared to participants in traditional focus groups.
A structured focus group format involves mixed-methods research, in which qualitative research involving methods such as interviews can complement quantitative research involving measures such as questionnaires (Tashakorri & Teddlie, 2003). One method compensates for the limitations of the other. For example, quantifiable data from a questionnaire may allow investigators to detect statistical relationships among participants' responses. These can be relationships participants may not have been aware of, but they are crucial to operations and design. Yet another example, the participants' open-ended responses and responses during a traditional focus group format, can offer targeted solutions and support, clarify, or expand upon quantitative findings.
Study Framework and Objectives
This exploratory pilot project developed and used a structured focus group format with mixed methods to facilitate design decision making during construction documentation of a proposed OR set-up. OR team members evaluated a three-dimensional (3-D) video mock-up of a proposed OR set-up. The primary purpose of the project was to explore the impact of OR features on participants' perceived safety and efficiency. In turn, an understanding of OR features that positively or negatively affect OR safety and efficiency would help inform design decision making, design solutions, and design innovations. A secondary purpose was to address gaps between research findings and their application to project delivery by piloting a novel focus group technique. Structured focus group formats may be a particularly useful technique to help translate research findings into project implementation given the limitations of traditional focus group formats.
Methods
Setting and Video Mock-Up
For the current project, a structured focus group format allowed for convenient viewing of a 3-D video mock-up of the proposed OR room. Objective research findings were compiled into a report that project leadership used to inform implementable design recommendations. The structured focus group sessions took place in a large auditorium near the participating military medical center. The large auditorium was outfitted with advanced projection capabilities. Side-tables throughout the auditorium contained items for the participants' reference. These items included floor plans of the future OR suite, and materials and finishes for the future ORs. The front of the room was dominated by a large screen on which animated fly-through scenes and stills of a colored version of a 3-D video mock-up of the proposed OR room were projected. Figure 1 is a still taken from the 3-D video mock-up of the proposed OR room. Figure 2 is the plan of the OR room as shared with the participants.
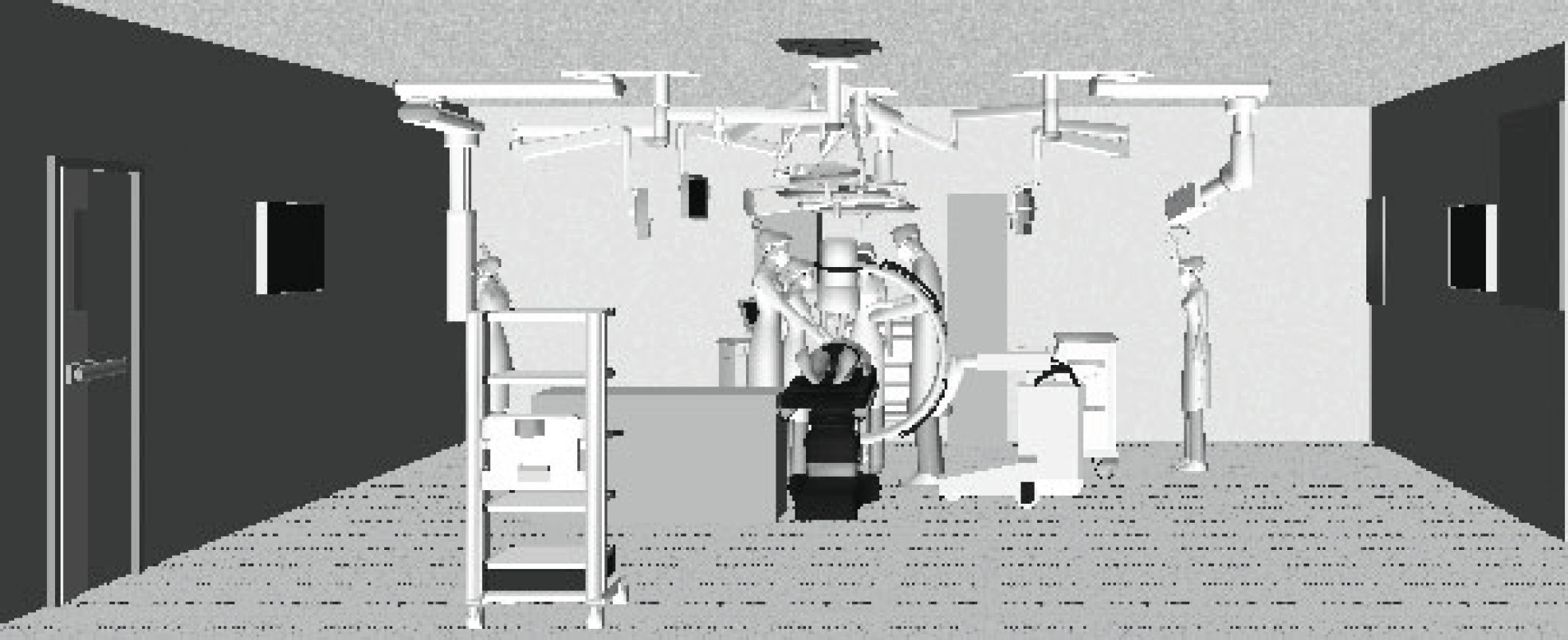
Still from the three-dimensional video mock-up of the proposed OR room. Source: Image courtesy of Naval Facilities Engineering Command and Maquet.
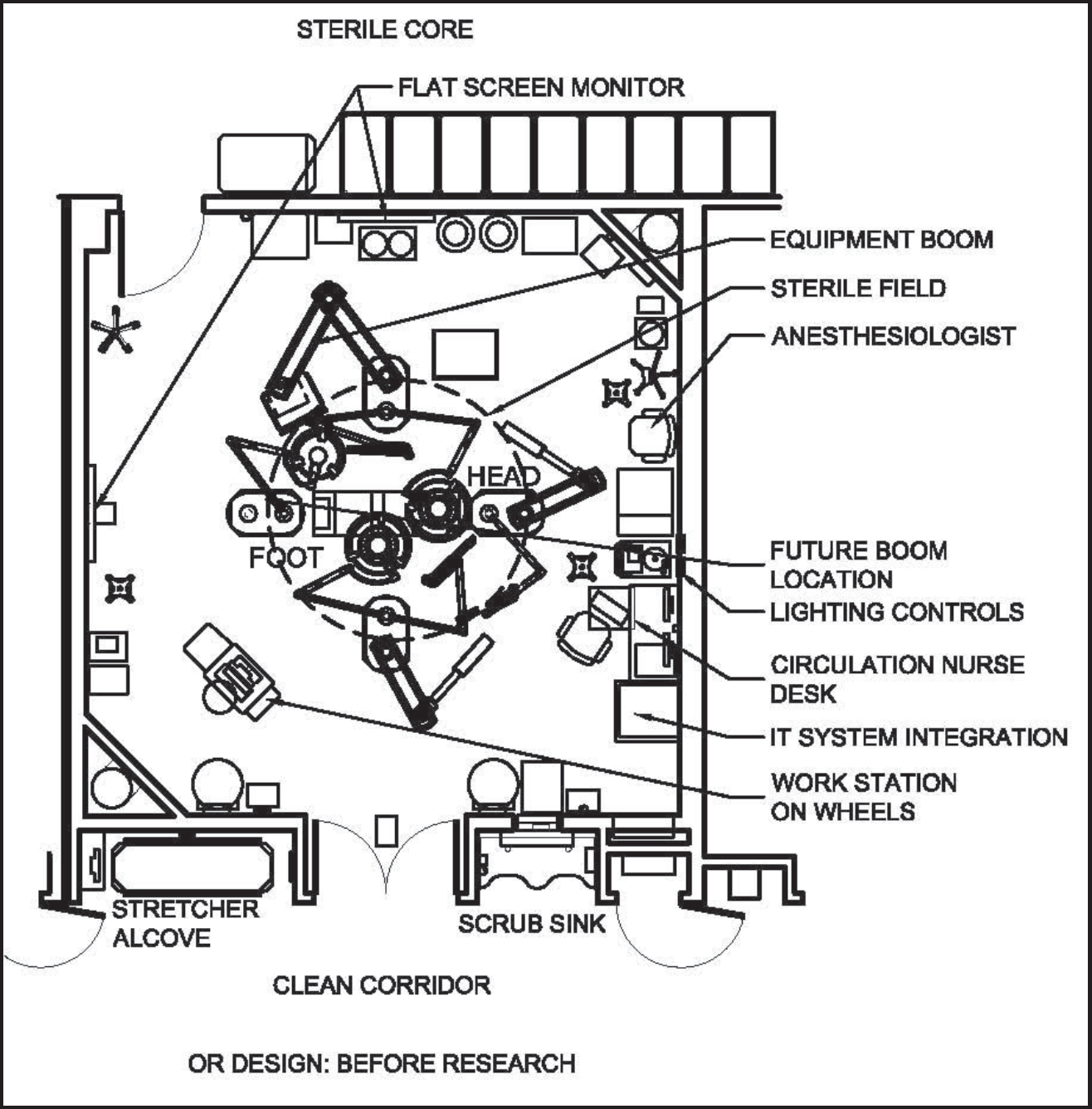
Plan of the OR room as shared with study participants. Source: Image courtesy of Naval Facilities Engineering Command and HKS.
Existing ORs in the organization have ceiling-mounted surgical lights and utility columns for gases and outlets. They do not have boom-mounted equipment. Compared to the existing ORs, the OR illustrated in Figures 1 and 2 was larger at 600 square feet, had improved lighting and lighting controls, and had integrated capabilities.
Participants
A total of 19 people participated in the structured focus groups. Participants consisted of surgeons (N = 5), surgical technicians (N = 3), perioperative nurses (N = 7), perfusionists (N = 2), and two individuals who did not designate their roles on an OR team. Participants were recruited with an e-mail blast to members of the institution's surgical staff. Five of the participants were female and 14 were male. The average height of a participant was 5′ 7″. The average duration of employment at the medical center was 6 years and 7 months.
Procedure
Four 1-hour structured focus group format sessions were held with surgical staff over the course of 1 day. Each session consisted of an introduction, a fly-through of the 3-D video mock-up of the proposed OR, participants' completion of a questionnaire, and a group discussion. Sessions were introduced and led by an environmental psychologist. Participants were not permitted to communicate with each other before the group discussion so that their answers would not be influenced by others' comments. Any questions about the proposed OR room design or questionnaire were directed to a panel consisting of an environmental psychologist, healthcare facility planners, architects, equipment consultants, and construction managers.
Likert-scale responses were analyzed using principal components analysis (PCA) with Varimax rotation and step-down regression analyses. Participants' open-ended responses to questionnaire items were content analyzed using principles from grounded theory (Strauss & Corbin, 1998). Concepts representing discrete parts of the focus group sessions emerged through a process of open coding. Then, concepts were synthesized into larger categories. Once the data were analyzed, findings were presented to key project decision makers to formulate targeted design recommendations implementable on the project. Human subjects review was not required to conduct focus groups.
Research Instruments
A questionnaire was developed specifically for this study. A literature review of published blind peer-reviewed studies and thought pieces identified key topics and questions to address in the questionnaire. The narrowing of topics for and piloting of the questionnaire were conducted with two rounds of focus groups consisting of the medical center's surgical staff, architects, engineers, healthcare facility planners, project managers, and an environmental psychologist.
The questionnaire consisted of closed and open-ended response formats. Closed question formats consisted of Likert-scale questions and questions requiring a “yes” or “no” answer, which were followed by open-ended questions that allowed participants to qualify an answer.
The questions were divided into seven subsections. The first subsection solicited background information from participants. Questions addressed participants' age, gender, height, duration of employment at the medical center, occupation within the OR, and surgical specialty (e.g., general, cardiac, orthopedic). The second subsection dealt with outcomes in the proposed OR. Participants evaluated the proposed OR for its adaptability to a variety of surgical procedures, the prevention of errors, the prevention of surgical-site infections, the prevention of distractions, clarity of visual field, trip hazards, and the accessibility of equipment and supplies. The third subsection dealt with ceiling-mounted booms and set-up. Participants evaluated the booms on the likelihood of boom collision, number of boom-mounted monitors, and boom accessibility. The fourth subsection pertained to participants' impressions of the proposed OR's equipment, supplies, and layout. Participants evaluated the distance to equipment and supplies, the accessibility of light switches, the number and height of wall-mounted screens, the number of outlets or plugs, the orientation of the OR table, and the ease of use of a Da Vinci robot and C-arm within the OR setting. The fifth subsection dealt with obstructions to workflow in the proposed OR. Participants estimated how often circulating nurses would have to leave the OR to retrieve equipment and supplies, and the amount of unnecessary movement by staff. In addition, participants evaluated the ease of documentation, ease of room turnaround, transition of the patient to the post-operative acute care unit (PACU), and team performance. The sixth subsection addressed what the participants would change about the OR and to what extent. Participants were asked what they would change about the nursing work station location, the anesthesia set-up, the telephones, the entry to the OR from the sterile core, the durability of surfaces, and infectious waste disposal. The final subsection addressed the efficacy of the 3-D video mock-up of the proposed OR room for visualizing the proposed OR design. Participants rated how good the video would be for educational purposes and how helpful it was for completing the questionnaire.
Results and Discussion
Data Preparation: Developing Measures of Operating Room Safety and Efficiency
A PCA with Varimax rotation was performed on the questionnaire to develop components that could be used as potential criteria and outcome variables within regression models. Table 1 shares the results of the PCA; it yielded three components. Certain questions were excluded during the development of the components because they served as predictor variables or criterion variables for regression analyses.
Component Structure of the Questionnaire
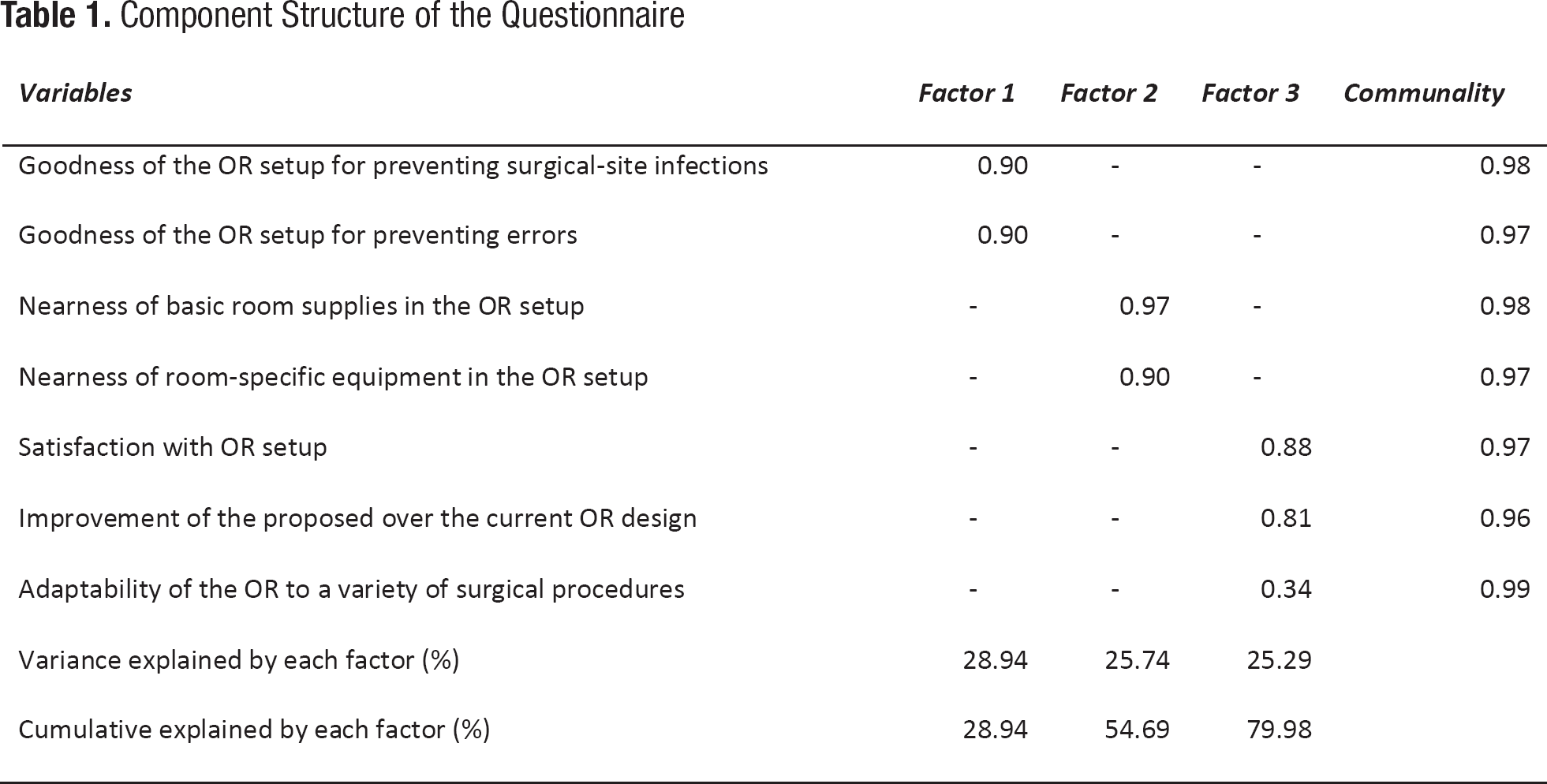
The first component was labeled “Flexibility of and Satisfaction with the Operating Room Setup” (α = .87). Items in this component included “satisfaction with OR set-up,” “degree of improvement of the proposed OR design over the current OR design,” and “adaptability of the OR to a variety of surgical procedures.” The second component was labeled “Prevention of Adverse Events” (α = .93). Items in this component included “goodness of the OR set-up for preventing surgical-site infections” and “goodness of the OR set-up for preventing errors.” The third component was labeled “Proximity of Equipment and Supplies” (α = .87). Items in this component included “nearness of room-specific equipment in the OR set-up” and “nearness of basic room supplies in the OR set-up.”
Predictors of Flexibility and Satisfaction With the OR Set-Up
A step-down regression was performed to reveal a parsimonious model that predicted flexibility and satisfaction with the proposed OR set-up. The step-down regression analyses revealed the following equation:

An examination of the participants' open-ended responses qualified the results from the stepwise regression. The participants conveyed three potential contributors to unnecessary movement in the proposed OR set-up. First, some participants communicated that the anesthesia set-up could conflict with a zone set aside for the nursing work station. Specifically, there was concern that the anesthesia set-up would block the circulation nurse's accessibility to the nursing work station, computer, telephone, and an OR light switch. Second, participants expressed concern that for ear, nose, and throat (Otolaryngology) cases, wherein the OR table is rotated 180 degrees, the required scope and towers located at the head of the bed would be between the entry and exit of the OR. Third, some participants conveyed that the C-arm in the proposed OR set-up would be difficult to maneuver.
The participants offered several suggestions to alleviate some of the challenges of unnecessary movement within the OR set-up. Suggestions included relocation of the nursing work station to the foot of the table, wireless communication devices for surgical team members, light switches inside and outside each door, and training sessions with the C-arm prior to the opening of new ORs designed after the proposed OR set-up.
The participants' open-ended responses conveyed three potential contributors to boom accessibility. There was concern that the perfusion boom, OR boom lights, and monitors could collide with other booms soon after the proposed ORs were built and in use by surgical teams. The proposed perfusion boom location was problematic for a participant because the perfusionist would have to reorient the position of the heart-lung machine, the pump obstructed the approach to the patient, and the heart-lung machine would have to be moved to transition the patient to the PACU.
Solutions to the challenge of boom accessibility were proposed. One participant expressed concern that lights and monitors should be reset to their original positions following each surgery because it would be difficult and time consuming for the surgical staff to arrange them. However, participants suggested that these difficulties would end after the surgical staff became more familiar with the booms' range of motion. Also, a participant recommended switching the location of the perfusion boom to the other side of the OR. As with the C-arm and the prevention of unnecessary movement, participants felt that actual experience with the proposed OR setup would be helpful.
Concerns specific to the “clarity” of equipment location dealt with whether objects were either absent from or obstructing a team member's visual field. First, a participant noted that the wall-mounted OR dashboard was not mounted within a cardiac surgeon's line of sight. Second, some participants were concerned that the current set-up might encourage circulating nurses to chart with their backs to the patient.
Participants suggested several possible solutions to visual field-related challenges. These included an additional wall-mounted screen across from the surgeon and in her or his line of sight, a clear indicator of room temperature when inside the room, floor demarcation cueing where equipment or people should go, movement of the heart lung machine to avoid obstructing patient transfers, a reconsideration of nursing work station orientation and location, a dedicated monitor for perfusion, and moving the perfusion boom to the other side of the OR.
Predictors of Adverse Event Prevention
A step-down regression was performed to reveal a parsimonious model that predicted adverse event prevention in the proposed OR. The step-down regression analyses revealed the following equation:

Predictors of Team Performance
A step-down regression was performed to reveal a parsimonious model that predicted the quality of team performance in the proposed OR. This revealed the following equation:

An examination of participants' open-ended responses qualified the results from the stepwise regression. Earlier, there was a discussion of participants' criticisms of clarity regarding where equipment should be during a procedure within the proposed OR set-up. Participants conveyed two potential difficulties with documentation in the proposed OR set-up. As with comments expressed about quality of the visual field, some participants were concerned that the current set-up might encourage circulating nurses to chart with their backs to the patient. As with comments expressed about contributors to unnecessary movement, some participants were concerned that there could be conflicts between anesthesia and the circulating nurse depending on utilization of the nursing work station. Earlier concerns with boom accessibility as related to flexibility and satisfaction with the OR set-up also applied to ease of documentation. Though the height of the wall-mounted screens in the proposed OR set-up predicted the quality of team performance, participants did not offer a specific reason as to why height would be a problem. However, logic dictates that the height of a wall-mounted screen would affect the visibility of the screen to surgical team members.
Participants' suggested solutions for improving clarity about where equipment should be during a procedure and boom accessibility within the OR set-up were consistent with the suggestions related earlier. Recommendations to resolve the issue of wall-mounted screen height included placing the wall-mounted screen on an adjustable track and setting any wall-mounted screens at eye level.
Predictors of Distraction and Interruptions
A step-down regression was performed to reveal a parsimonious model that predicted how often the participants perceived they would be interrupted or distracted while conducting a procedure in the proposed OR. This analysis revealed the following equation:

An examination of participants' open-ended responses qualified the results from the stepwise regression. Potential direct causes of distractions and interruptions identified by participants included the need to call out of the OR for patients, movement of monitors away from the surgical field, and requests to route images. Consistent with prior concerns shared by participants already related in this article, some participants believed their colleagues would need to familiarize themselves with the proposed OR once it was built, and the location of the nursing workstation was problematic. Participants' concerns with the proximity of equipment and supplies included inconvenient light switch locations for nurse and technician access. Once again, the same concerns with boom accessibility were expressed.
The participants suggested a variety of solutions to address elements that contribute to distractions and interruptions in the proposed OR. Ideas to have light switches inside and outside the doors and to move the perfusion boom to the other side of the OR were consistent with other suggestions to prevent unnecessary movement and improve the quality of the visual field in the proposed OR set-up. Other solutions included the implementation of a computerized patient tracking system and a touch-sensitive monitor panel within the surgical field to prevent requests to route images.
Design Recommendations Based on the Findings
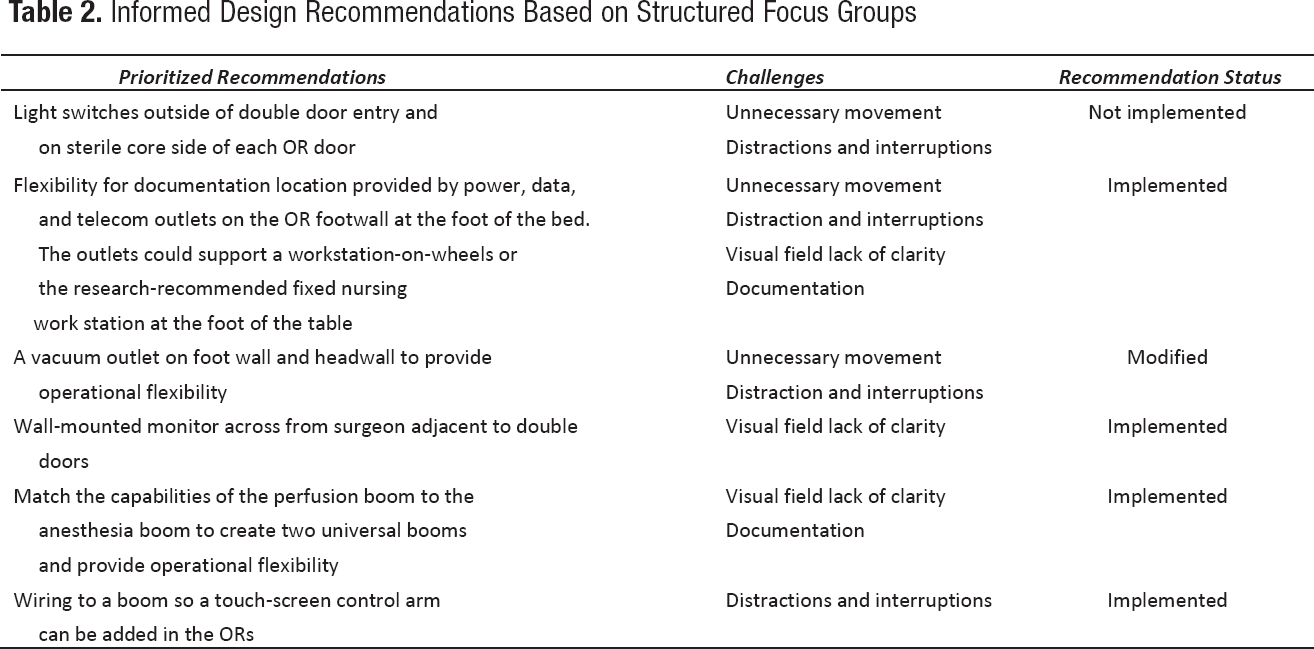
Table 2 shows prioritized design recommendations for construction documentation of the proposed ORs. These recommendations were based on participants' suggested solutions and project leadership's review of a report that consolidated the findings. If, because of time or budgetary constraints, a recommended solution could not be fully adopted in the forthcoming phase of the OR build-out, accommodations were specified so the solution could be fully adopted at a later date. For example, the final build-out included a nursing work station that faces the patient and is at the foot of the OR table. The challenges are paired with each solution suggested and their adoption or modification is indicated.
Informed Design Recommendations Based on Structured Focus Groups
Limitations
Consistent with prior work utilizing mock-ups of healthcare settings, the 3-D video mock-up with structured focus group format helped participants visualize design challenges and recommend design solutions (Watkins et al., 2010). Additionally, the structured focus group format allowed participants to share concerns with less bias and influence from other participants.
The 3-D video mock-up with structured focus group format was expeditious. Its quick turnaround time of approximately 2.5 weeks provided designers, planners, and the client with objective and just-in-time findings to inform design decision making that otherwise could have been based on anecdotes. The structured focus group formats and just-in-time findings translated participants' feedback into implementable design solutions. Moreover, the translation effectively bridged a gap between users and design prevalent in architectural practice. Therefore, structured focus groups with mixed methods can offer a value-added and expeditious service to a building project that already intends to utilize traditional focus groups.
Consistent with the goals of the project, findings from the structured focus groups were limited to a specific building project and not intended for generalizability to other projects. Also, the structured focus groups were piloted as a novel and efficient technique to use when feedback from full and detailed physical mock-ups was not feasible.
The implementation of full and detailed physical mock-ups would not have provided just-in-time and objective findings within the parameters of the building project's aggressive schedule.
A larger sample would have been preferable, but the aggressive schedule of the building project dictated only a few potential dates to host the sessions. Unfortunately, the sessions had to be held on a government holiday when many employees were away. The smaller sample size prohibited statistical comparisons among the OR staff roles (e.g., physician, circulation nurse). Though the smaller sample size could appear discouraging, participants' responses to each question expressed a trend toward normal distribution. Loadings for the components revealed through the PCA were clean and high. Participants provided written responses to clarify their answers to closed questions. These latter considerations suggest that the small sample size may have been mitigated by the integrity and richness of the participants' responses.
Overall, participants thought the 3-D video mock-up was helpful for viewing equipment and details displayed in the mock-up. However, if a finer detail was not displayed in the mock-up (e.g., phones, waste disposal, light switches) the participants expressed difficulty visualizing the detail, the detail's location, and the interactions with the detail. Typically, a participant's question to the panel of experts cleared up confusion about the location of finer details not explicitly conveyed in the model.
Conclusion and Directions for Future Research
This pilot project utilized a structured focus group format with mixed methods to gather participants' impressions of a proposed OR set-up. During the structured focus groups, participants evaluated a 3-D video mock-up of the proposed OR set-up. The purpose was to use results from analyses of the participants' responses to identify safety and efficiency-related design features for inclusion in the proposed OR construction documents. Based on the findings, implementable design solutions were successfully identified and justified. They included universal booms to support anesthetic and perfusion capabilities, a wall-mounted monitor across from the surgeon, and wiring to support a touch-screen control arm in the OR surgical fields.
The efficacy of the structured focus group format piloted here indicates that similar efforts could be a value-add for any building project that already intends to use traditional focus groups. Future structured focus groups of proposed healthcare settings like OR set-ups could involve technologies that may be more likely to immerse participants in a sensory-rich experience of the proposed design. To this end, project teams may consider 3-D glasses commonly used in movie theaters, virtual technologies, and building information modeling.
Project teams may consider an iterative process wherein findings from structured focus groups inform the designs of full and detailed physical mock-ups. Participants could then assess the physical mock-up and offer additional suggestions and refinements based on the kinesthetic, auditory, haptic, olfactory, teamwork experiences afforded by physical mock-ups. For example, research has demonstrated that unacceptable noise levels in ORs can impair team communication and thereby lead to additional procedural time and errors (Goodell, Cao, & Schwaitzberg, 2006; Moorthy, Munz, Undre, & Darzi, 2004; Thrall, 2009). Additionally, research on OR staff training with high-fidelity OR mock-ups involving mannequins indicates that such training contributes to self-efficacy for effective teamwork performance in everyday practice (Paige et al., 2009). Finally, a post-occupancy evaluation performed 6 to 12 months after occupancy of the ORs built following the feedback from the mock-up would demonstrate whether implemented design recommendations impacted key outcomes such as patient safety and efficiencies.
Footnotes
Acknowledgments:
The authors thank the participating clinicians, nurses, and staff. In addition, they thank NAVFAC for facilitating the focus groups and Sallyanne Jarvis, Denver Terrance, Kathleen Smith, Deborah Waitzman, Rebecca Almira, Jason Zoss, Nibu Samuel, Bob Salas, and Patsy Trine for graciously giving their time.