
Abstract

D. Kirk Hamilton, FAIA, FACHA, EDAC

Some design practitioners apparently worry that adopting an evidence-based practice model might reduce their opportunities for creative design solutions. Reactance theory (Brehm & Brehm, 1981) tells us that when persons are threatened with a loss of control, they will resist the imposition. Because on the surface it seems difficult to object to the idea of basing design decisions on the best available information to improve their quality (Stichler & Hamilton, 2008), I ask whether the negative reaction to evidence-based design on the part of some is a reactance behavior. If a designer expects to lose control or creative freedom over design decisions, it is understandable that there might be a strong expression of concern. I must ask whether such concern is justified.
What Is Creativity in Healthcare Design?
Architects and designers are taught to be arbiters of the public taste for aesthetics, at least where the built environment is concerned. For an architect, creativity is bound up in the decisions made in the process of imagining a building that does not yet exist and working to make this intellectual creation a reality. This creativity can be expressed in aesthetic judgment; the introduction of new and novel concepts; innovations in planning or the execution of construction; new or fresh ideas; and new combinations of materials, concepts, and building elements. Design professionals make countless decisions during the process, which affect beauty, comfort, human interaction, and human performance.
Managing change, creativity and innovation is central to the repositioning of organizations in the uptake of new technologies and new techniques, to business developments in the provision of new products and services, and to the formulation and implementation of strategies to secure competitive advantage (Andriopoulos & Dawson, 2009, p. 4).
Architects are change agents in service to their clients. Many would define their role as fostering innovation, and it could be argued that creativity is required to produce innovation. Architecture has always been both an art and a science, and every architect cherishes the part of his or her work that represents an artist's creativity. This is why any apparent reduction in creativity or design freedom will be resented or attacked. It is my contention, however, that an evidence-based process does not diminish the creative opportunities in projects.
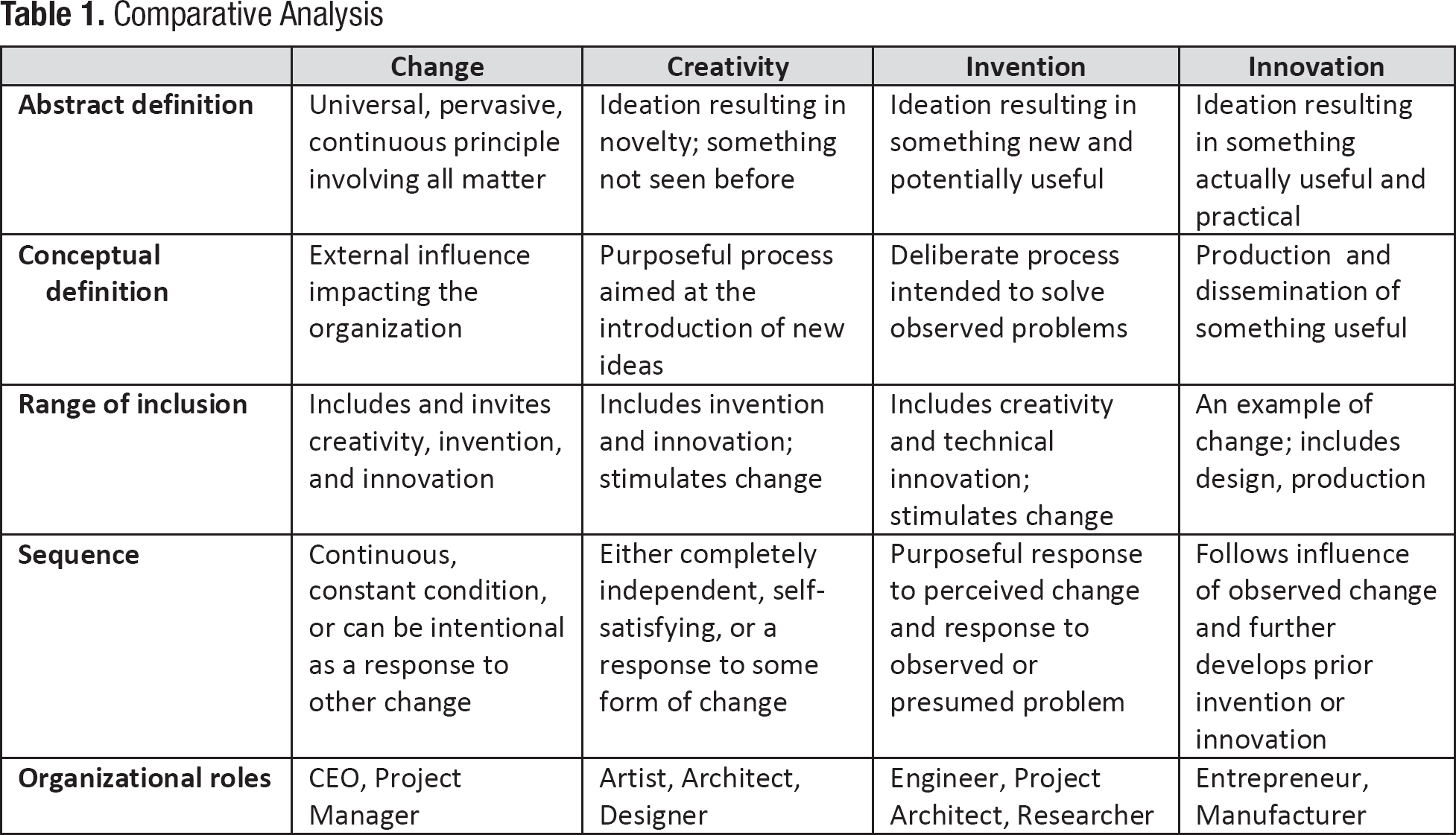
Change, creativity, invention, and innovation. Design professionals often use these terms with a tendency to interchange their meanings. I think distinctions can be made. There are few—if any—common definitions of these terms that might rise to the level of broad consensus. The interactions among these concepts are many and complex. According to Andriopoulos and Dawson, “these processes of change, creativity, and innovation overlap and interlock” (2009, p. 7). In the interest of developing common definitions that may be useful in developing scholarly precision, Table 1 offers a simple and personal analysis of the differences among these terms.
Comparative Analysis
What Types of Decisions Do Designers Make?
If architecture is an art and a science, then both types of decisions must be expected. Aesthetic decisions may be contrasted with functional decisions. One could describe decisions as objective or subjective, rational or arbitrary. These characterizations seem to describe opposites or extremes on the continuum of decision making. Must it always be one or the other? Can we have decisions that address both poles?
Barry Johnson (1996) has written about polarity management, in which the “either/or” can be replaced by a “both/and” model. One of his examples is breathing: if one decided that breathing in oxygen is wonderful and resolved to do it exclusively, one would soon be overcome by carbon monoxide poisoning. The only solution is to breathe out, and if that were now the only action undertaken, one would die of oxygen depletion. The answer, of course, is to balance breathing in with breathing out, maximizing the benefits and minimizing the drawbacks of each.
Healthcare features numerous potential decision polarities. For example, the opportunity for both observation and privacy is desirable in patient settings: should it be one or the other, or can the designer effectively address both? Evidence suggests that there are benefits to centralized and decentralized applications in patient unit design: should it be one or the other, or can the thoughtful designer creatively address both?
Although it is more obvious to characterize subjective aesthetic decisions as creative, I suggest that all design decisions require creative thinking. All designers use empirical evidence or information from practical experience, of course, so perhaps clarity about the types of decisions being made would be useful.
A Decision Evaluation Model
It is possible to think of design decisions for any facility project as occurring in the context of two variables. Figure 1 provides a simplified matrix in which all design decisions can be categorized based on the amount of information available about a topic or issue and also on the importance of the impact of a decision.
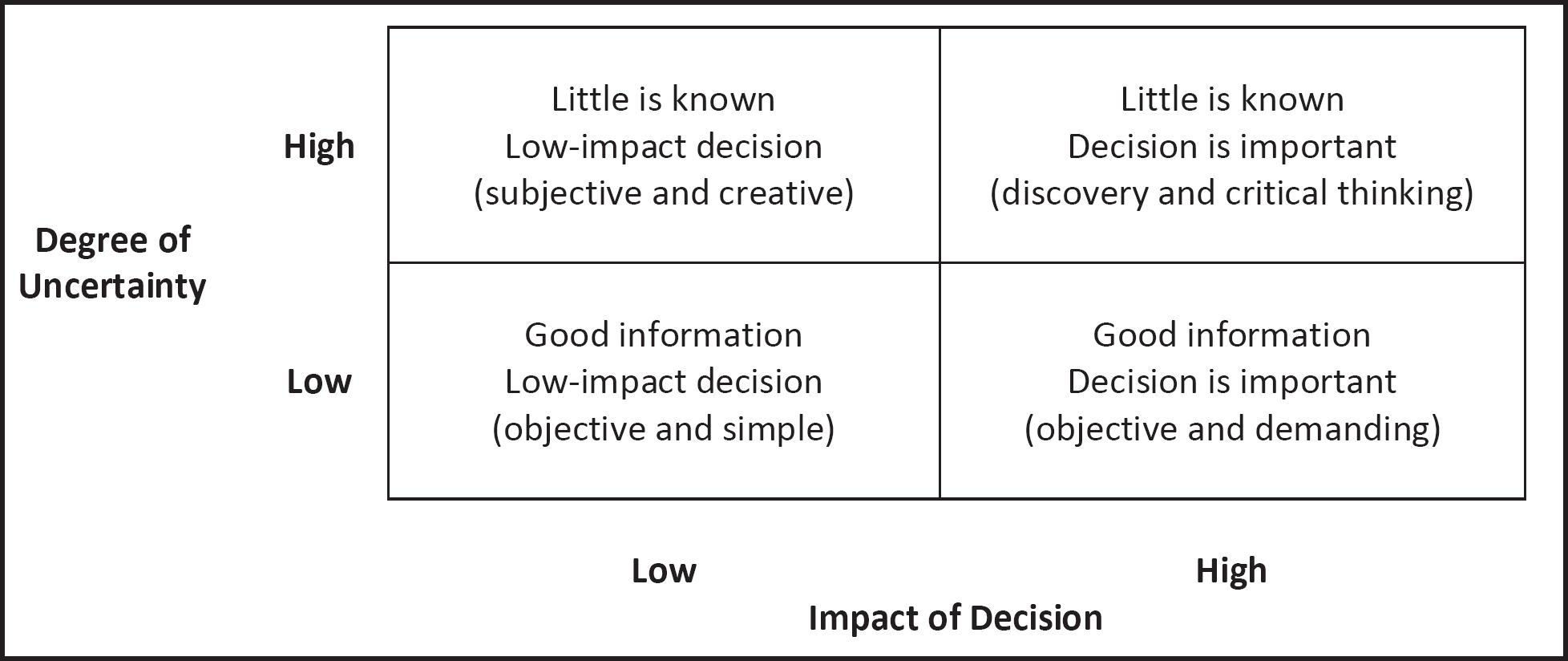
Matrix of decision options.
When little or no information is available to address a topic or design issue, the matrix categorizes it as high uncertainty. On the other hand, if much is known and strong evidence addresses the topic, a designer may approach the decision with some degree of certainty. Decisions that are vitally important because they influence significant outcomes can be described in the matrix as having a high impact. Other decisions about which there are few concerns, or decisions that do not put the organization or outcomes at risk, can be regarded as low-impact decisions.
Figure 1 shows the degree of uncertainty or lack of information available to a designer, with high levels of uncertainty in the two upper boxes. These are the decisions for which there is little reliable information from research or practical experience. Conversely, the lower two boxes represent decisions for which good information is available.
The other variable is the impact of a decision; the two right-hand boxes represent decisions that are important or crucial in some way. Importance can be gauged on the basis of several measures that could be based on clinical, safety, economic, social, architectural, construction, or contextual issues. The left-hand boxes represent less important decisions that, nevertheless, must be made to complete a project.
Creative Interpretation of Evidence
The availability of strong evidence from research does not mean that a design decision will be obvious. The decisions in the lower-right quadrant of the matrix, in which the impact of the decision is important and for which good information is available, need to be made in an objective fashion. These decisions are highly demanding because of their potential impact. These are the decisions the client will expect to be made on the basis of rational and functional criteria.
These are the kinds of decisions some practitioners apparently resist because they seem to limit their design freedom or creativity. Nonetheless, it is my contention that the interpretation of research findings in the context of a designer's unique project requirements is a highly creative activity.
Zone of Maximum Design Freedom
The two left-hand boxes of the matrix offer designers great freedom. These are the decisions for which designers can exercise the most control.
Figure 2 shows how decisions for which good information is available and the impact of the decision is low (lower-left quadrant) should be simple and objective. Such decisions can be made with much freedom on the part of the designer because the consequences of the decision do not demand a particular solution.
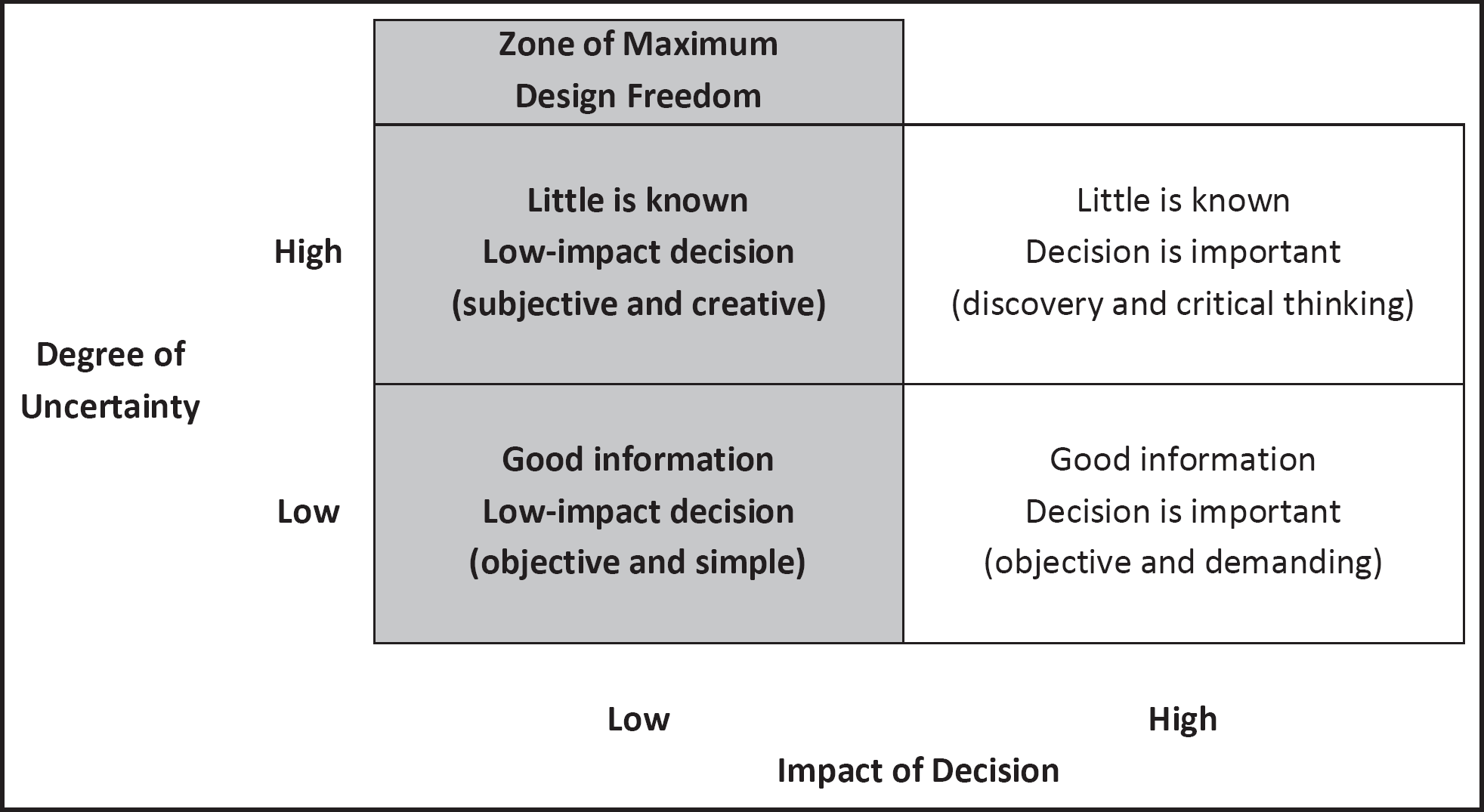
Zone of maximum design freedom.
It also shows how decisions for which little information or few research findings are available and whose impact is low (upper-left quadrant) can be subjective and should be creative. This is the arena in which a designer may exercise high levels of innovative personal aesthetic or rational judgment.
Domain of Highest Creativity
Decisions for projects that have the highest levels of uncertainty or the least available topical information and credible research evidence require great creativity on the designer's part. When little is known about the most promising path, a designer's creativity is always in play. Figure 3 emphasizes the decisions requiring the highest levels of creativity, seen in the top two boxes.
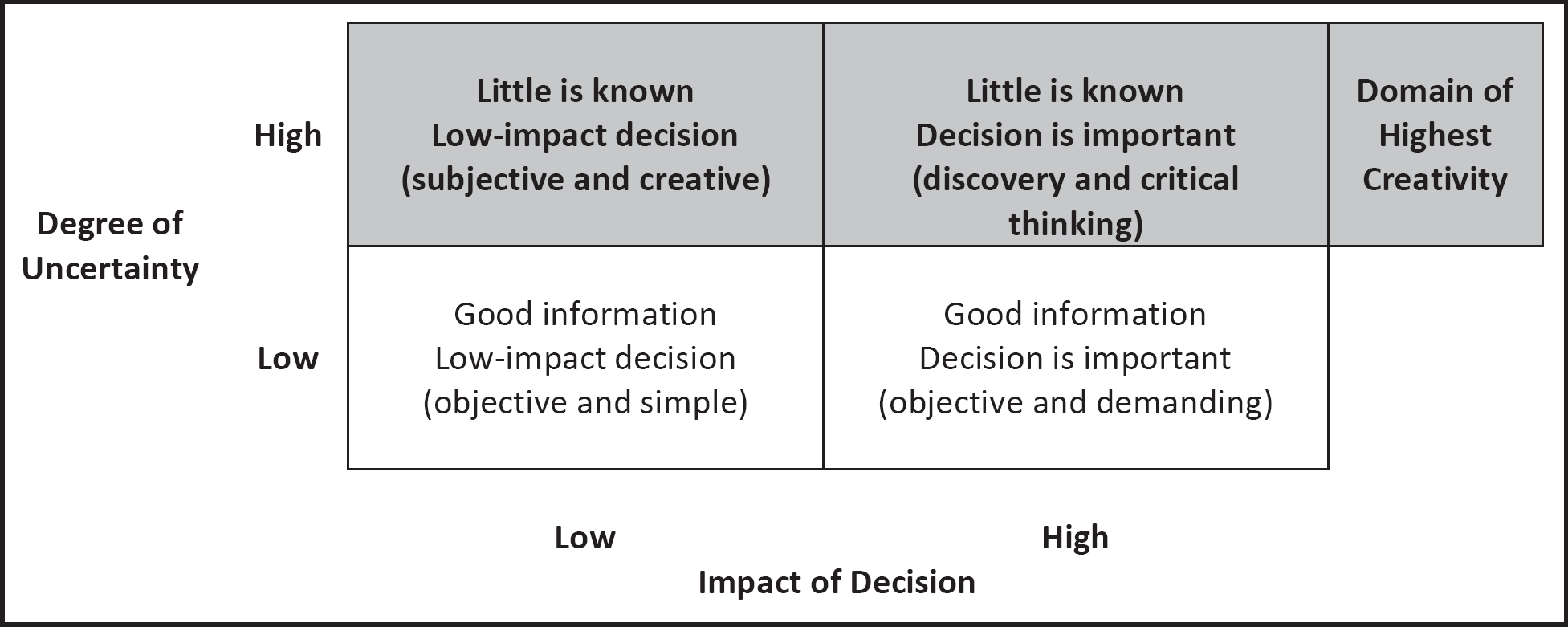
Domain of highest creativity.
The upper-left quadrant of the matrix is seen as both the domain of highest creativity and the zone of maximum design freedom. This, then, represents the set of decisions that will be most interesting to aesthetic, subjective designers who wish to express themselves in exciting artistic and architectural forms. These decisions occur on every healthcare project, and they should provide many opportunities for subjective, creative expression.
The upper-right quadrant, where little information is available to address issues of significant potential impact, represents the most demanding decisions for design professionals. It is important to find a good solution for a difficult problem; surely this is creative work.
Choosing Research Topics
This matrix is also useful for deciding whether potential research topics are worth pursuing. The upper-right quadrant of the matrix, indicating that there is little reliable information or few research findings available and suggesting that the decision will have a significant impact, identifies the type of topic that could offer the highest return from research. These are the types of questions for which researchers and practitioners would most like to find answers.
Conclusion
Designers may find it helpful to consider the kind of decision that is before them. If they begin to discriminate among the types of decisions to be made on sophisticated healthcare projects, they should find ample room for creativity, novelty, and innovation.
This matrix provides a view of a pair of polar opposite decision profiles on the diagonals. The maximum freedom for designers to express themselves with subjective, aesthetic solutions occurs with decisions for which there is little information and that are not crucial from a safety standpoint (upper left). Diagonally opposite, one finds the most restrictive quadrant, suited to objective and rational decisions in the context of good information relating to high-impact issues (lower right). The other diagonal ranges from what is perhaps the least challenging quadrant, where objective decisions using good information must be made for issues with low impact (lower left), to the most challenging quadrant, where vitally important decisions have to be made on the basis of little or no relevant information (upper right).
Perhaps this model for better understanding decisions that must be made will offer design professionals an opportunity to focus their imaginative efforts on the numerous project decisions that are best suited to the exercise of design freedom and creativity in the delivery of invention and innovation. The use of an evidence-based model does not alter the types of decisions that must be made; it simply helps make some of them more effective.