
Abstract
Objective:
To confirm a new method for the research question, “How do different hospital unit layouts affect nurses' walking behavior and distance?”
Background:
Concern is renewed regarding nurses' long walking distances because of the trend toward larger patient rooms with family areas inside, resulting in a larger overall unit size. Studies have found unit design characteristics that support nurses' efficient walking, but few have done it in units designed for patient- and family-centered care. To examine the effect of unit design on nurses' walking behavior, the authors propose a new method of observing a specific task.
Methods:
The authors observed nurses during the task of medication administration.
Results:
Contrary to their hypotheses, results showed: (1) Experienced nurses had more unnecessary stops and longer walking distances than new nurses because of interactions; and (2) nurses in the smaller wing of the unit walked more than those in the larger wing of the same unit. The authors posit that the closeness between the nurses' path to the medication supply room and the central nurses' station affected the frequency of interactions and prompted a deviation from the shortest and most efficient path during medication administration.
Conclusion:
Observing a specific task to identify the effect of unit layout was effective, determining that overall unit shape or unit layout type might not be a good predictor of nurses' walking behavior; instead the characteristics of the path that connects functional spaces such as patient room and medication area might better predict nurses' walking behavior.
Introduction
Nurses spend a large proportion of their time walking during their shifts in nursing units (Burgio, Engel, Hawkins, McCormick, & Scheve, 1990; Cardona, Tappen, Terrill, Acosta, & Eusebe, 1997; Gadbois, Bourgeois, Goehakuegad, Guillaume, & Urbain, 1992). Concern regarding the long distances nurses must walk during a shift has been revisited because of the recent trend of expanding patient room size, with a family area included to realize the patient-centered care concept. Studies have identified some characteristics regarding unit design that support efficient nurse walking patterns (Shepley & Davies, 2003; Sturdavant, 1960). However, few studies have examined units designed for patient- and family-centered care.
Overall, studies have rarely reported on detailed walking behaviors determined by tracking or shadowing observation; studies of this nature could explain the mechanism that links unit layout and walking behavior. Therefore, this pilot study proposes the novel scheme of observing a specific task as a way to examine the effects of the architectural environment on healthcare. The aim of this study was to confirm the ability of this new method to answer this research question: How do different hospital unit layouts affect a nurse's walking behavior and distance?
The significant amount of time that nurses spend walking has raised concerns that this might negatively impact the time spent on patient care. The literature has suggested that more than a quarter of a nurse's time in a nursing home was spent walking (Burgio et al., 1990; Cardona et al., 1997; Gadbois et al., 1992). This was second only to patient care activities, which accounted for 59% of total time. Some researchers believe that less walking time would contribute to more patient care activities and better patient outcomes (Burgio et al., 1990; Hendrich, Fay, & Sorrells, 2004).
Fortunately, some studies have suggested that the layout of nursing units could help in the management of nurse walking distances (Shepley, 2002; Sturdavant, 1960; Trites, Galbraith, Sturdavant, & Leckwart, 1970). These studies often compared the “radial” unit layout design with other types, such as the “corridor” or “racetrack” layouts. The radial layout design is a unit with the nurses' station in the center surrounded by patient rooms with a single circular hallway between them. This type of unit allows direct access to and good visibility of all patient rooms from the nurses' station, which is not the case for all of the patient rooms in the corridor or racetrack/ double-corridor layout design (Lu, 2010; Seo, Choi, & Zimring, 2011) (see Table 1).
Different Unit Layouts
Concern regarding the long distances nurses must walk during a shift has been revisited because of the recent trend of expanding patient room size, with a family area included to realize the patient-centered care concept.
In 1960, Sturdavant compared two intensive care units (ICUs), one with a radial design and the other with a single-corridor design. She found that nurses had to walk less frequently to patient rooms in the radial design because of the increased visual supervision of patients available at the nurses' station. Trites and colleagues in 1969 followed Sturdavant's work by comparing three unit layouts built to study nurse walking efficiency: the radial; double-corridor (racetrack); and single-corridor layouts. Radial designs were more successful from the perspective of functionality because the nurses required significantly less travel to complete tasks. The decrease in the percentage of time spent walking correlated to an increase in the percentage of time spent in patient care activities. Later, Shepley's study confirmed this finding in that the nursing staff in the radial unit required significantly less walking time than staff in a rectangular unit (4.7 steps per minute vs 7.9 steps per minute) (Shepley & Davies, 2003). More recently, Hendrich and colleagues (2004) posited that a design enabling the decentralization of supplies helped significantly reduce walking distance.
Although many studies have shown the effect of unit layout on nurse walking behaviors, the layouts were described only by their overall shapes, i.e., radial, rectangular, or L-shaped. The mechanisms that explain how unit layout affects walking behavior remain unclear. One study attempted to explain the mechanisms by means of the Yale Traffic Index (Thompson & Goldin, 1975). This study found that most of the walking behaviors in nursing units consisted of trips between seven of the 16 areas identified on the wards, in 14 different combinations. The index, based on known trip frequencies and distance measures, was used to make comparative evaluations of wards using different layouts. However, these studies did not address the consequences of the nurses' interactions or interruptions that might have caused the nurses to deviate from the ideal routes, thereby increasing total walking distances. More recently, studies have attempted to understand the mechanism of visibility (Lu, 2010). Increased visibility of patients from the nurses' station allowed for direct observation of patients and thereby reduced nurses' required walking distance (Lu, 2010; Sturdavant, 1960).
In this study, the investigation focused on the mechanisms linking unit layout to nurses' walking distance by tracking the nurses' task-specific activities. Close observation of the nurses helped answer the research question. Participants were followed in two wings of a 20-bed ICU during the medication administration task. Their paths were recorded on the ICU floor plan. The number of stops and interactions were also recorded. Interactions included direct, face-to-face verbal communications. Because previous research showed significant variations among individuals and for different layouts, it was expected that both spatial and individual variations existed during the medication administration task in this setting as well. Two simple hypotheses were developed based on the previous studies:
Nurses will walk less in the smaller 6-bed east wing, which has a radial layout, than in the 14-bed west wing, which has a racetrack layout. Radial units tend to be much smaller than other unit types and have direct visibility of most patient rooms from a central nurses' station. Previous studies have suggested that nurses walked less in radial units compared to other unit types. Experienced nurses will walk less than new nurses, who may seek help during the task. Nurses in the unit have suggested that new nurses can work on their own after 1 year of experience. Many studies found that nurses having less than 1 one year of experience can perform short of expectations (Fero, Witsberger, Wesmiller, Zullo, & Hoffman, 2009). Therefore, it is expected that nurses with less than 1 year of experience will ask for help from other nurses, which results in extra stops and greater distances travelled.
Methods
Setting
The setting for this study was an ICU at a university hospital in Atlanta, GA. The new ICU had 20 single-patient rooms with a floor area of approximately 24,600 square feet (ft2), or 2,280 square meters (m2), as shown in Figure 1. The unit consisted of two parts: a west wing and an east wing divided by a wide corridor running north and south, as shown in Figure 1. There were similarities between the two wings because they were designed at the same time:
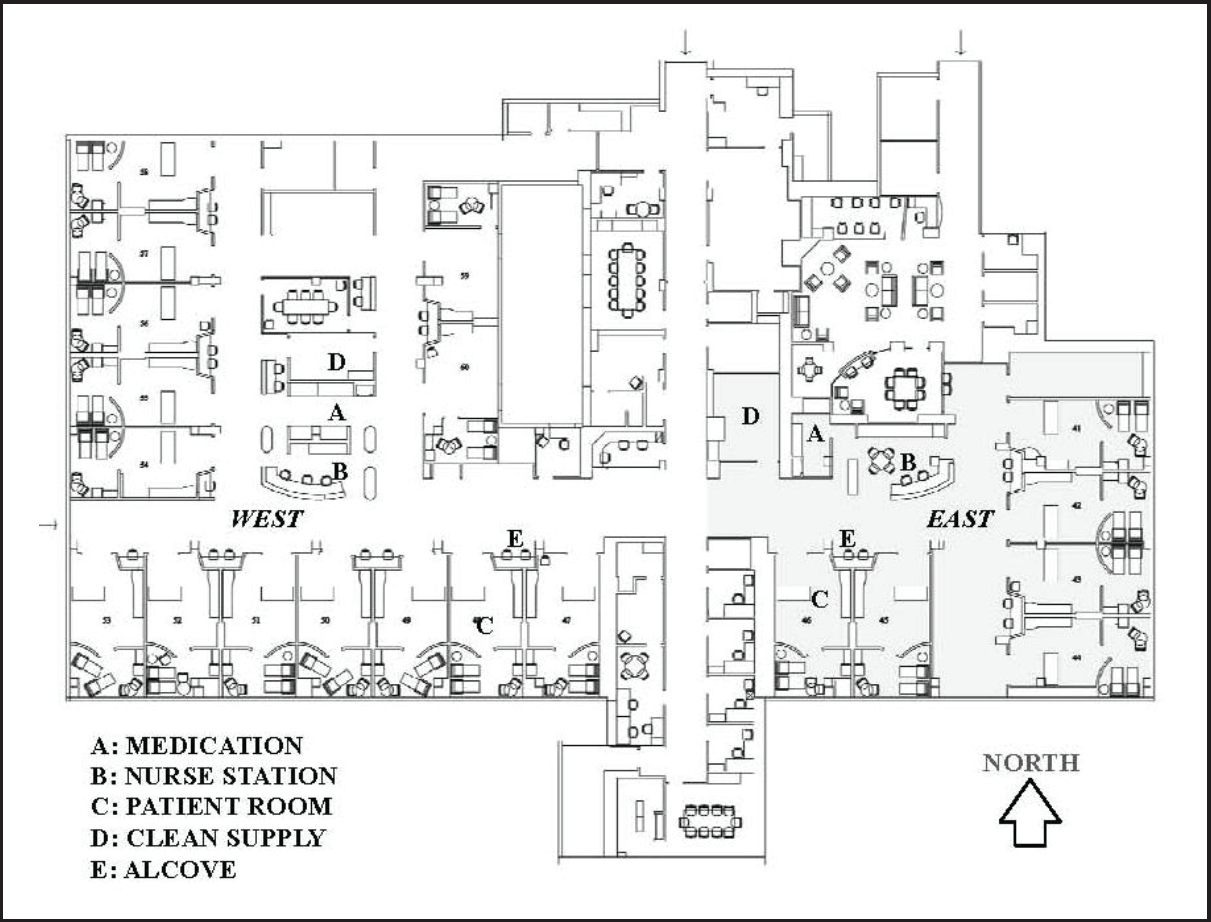
The ICU has 20 single-patient rooms with a floor area of approximately 24,600 ft2 (2,280 m2). The whole floor consists of two parts: the west wing (on the left side) and the east wing (on the right side) divided by a wide corridor running north/south.
Both wings had the same or very similar patient rooms and nursing alcoves in terms of design and size.
Both wings had a single centralized nurses' station of similar design.
Both wings had the same types of patients in terms of diseases and the severity of illness; less ill patients would be transferred to other units.
However, there were also differences:
The west wing had a racetrack or double-loaded hallway; the east wing had an L-shaped hallway. The west wing had 14 patient rooms with a total area of 10,840 The two wing configurations provided a great opportunity to test the effects of the physical environment, because the researchers could rule out many compounding factors such as differences in patient type, unit culture, and policy while comparing the different unit layouts. In addition, the patient rooms were typically full, which meant that the patients were assigned randomly to the available rooms at the time of admission.
Study Participants
Participants were the nurses working in the ICU of the hospital who agreed to be observed for this study. After approval from the internal review board, participants were selected on the basis of convenience when the researchers were visiting the unit. Nurses' experience ranged from 2 months to 7 years. Overall, 12 female ICU nurses participated in the study; several nurses were observed more than once.
The Medication Administration Task
In this study, researchers posited that observing nurses' task-specific activities would provide a better opportunity to examine spatially related differences and individual differences for the following reasons: First, the nurses' activities and underlying motives were better understood in the context of their ongoing tasks. Second, the single task provided a baseline to identify any deviation in activities. Third, focusing on one specific task could control the variance stemming from different tasks. Given these reasons, the basic problem that the researchers faced was choosing an appropriate task to fit the study goals. The nurses' procedures regarding the chosen task could not be too rigid; it would be difficult to find any deviation if everyone performed identically. On the other hand, the task could not be too liberal; otherwise it would be difficult to find a discernible pattern among the differences.
After informal interviews with the nurses, the medication administration task was chosen for this study because this task was believed to be both spatially and individually relevant. At the same time, it was relatively easy for nonclinician observers to understand and capture the procedure because the beginning and end of the task were visually discernible.
Procedure
After being informed about the purpose of this study at the beginning of the observations, participants were followed by a researcher at a distance of 2–5 meters (6.5–16 feet) during the medication administration task. The participants' movements and activities were recorded on unit floor plans. An observation began when a nurse left the substation to distribute medication after looking up the medication particulars. Sometimes it was unclear whether the nurse was leaving the substation for the medication task; some observations were disregarded because the nurses did not go to the medication station. A valid observation followed a nurse who went to the medication station and then came back to the patient room to administer the medication. The observation ended when the nurse went into a patient room. When recording the walking path of the nurse, the researcher also recorded stops and interactions.
Before the observations described in this study, researchers observed the same nurses together in the same unit to make sure that inter-rater reliability was more than 90%. Multiple researchers followed a nurse simultaneously and compared the observations recorded on the floor plans. Extra stops and interactions were compared among researchers to see whether everyone recorded consistently. However, it was deemed impractical to differentiate the exact location or path within a corridor (i.e., one closer to the patient room side versus the nurses' station side). Researchers distinguished location differences only on a larger scale, such as a location within the nurses' station versus the corridor.
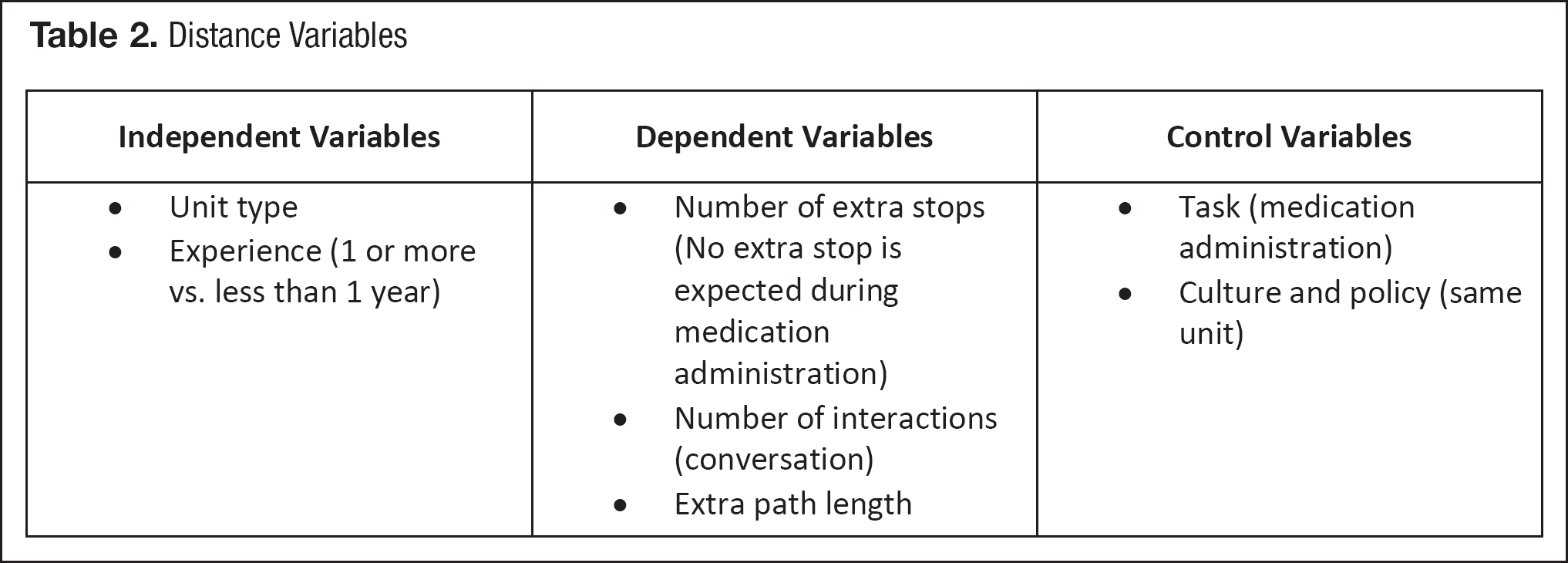
Researchers measured the shortest distance possible for walking the length of a given path. The measured variables are listed in Table 2.
Distance Variables
Data Analysis and Results
The number of extra stops and extra path lengths was calculated to measure the deviation from the most efficient route during the medication administration task. Stops were defined as the time that a participant stayed immobile and performed additional activities, such as talking, checking patient rooms, or using a computer. Researchers defined extra stops as redundant stops that deviated from the most efficient route needed to complete the medication administration task as shown on the right of Figure 2. An efficient route meant the route used when a nurse chose the shortest path possible with no stops other than the medication station. In the same vein, extra length meant the distance from the ideal and most efficient path. Movements inside patient rooms were excluded from this analysis to avoid the influence of other activities or tasks such as tasks other than medication administration and involvement with family members. The researchers used descriptive statistics and the analysis of variance method to analyze the data.
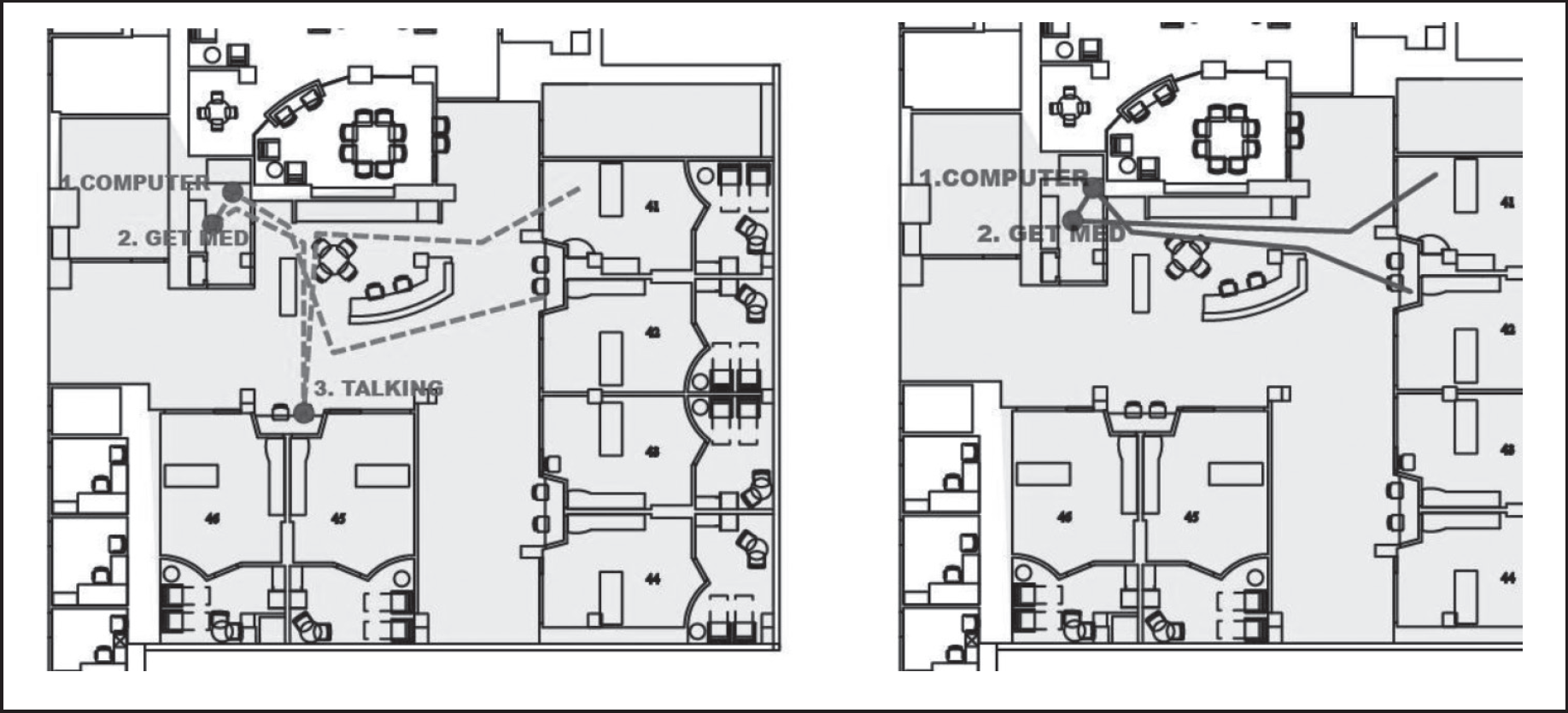
The observed route (on the left-hand picture) vs. the efficient route (on the right-hand picture). One extra stop had an additional length of 47 ft.
Overall Observation Results
Several observations were dropped because the participants were still training or the nurse switched the task with another major task, such as a patient transfer. At the end, researchers obtained a total of 20 observations, 10 in each wing.
The participant's path during the medication administration task was coded into one of the three patterns:
Efficient: taking the most direct route going to the medication distribution room and back Retracing: going to the medication distribution room/supply room twice or more during one medication administration task Deviated: taking a route that deviated from the most direct route to talk to someone or finish other tasks during the medication administration task.
A total of 8 efficient, 4 retracing, and 7 deviated path patterns were observed.
The number of extra stops and extra lengths was used as a measure for the route patterns. The efficient, retracing, and deviated patterns had mean numbers of extra stops of 0.0, 0.5, and 3.0, respectively. The deviated pattern had more stops than the other two groups.
The three route patterns also differed significantly from one another in terms of the value of the extra path lengths (p < .01). The efficient, retracing, and deviated patterns had mean extra distances of 0.6, 73.3, and 109.0 feet (ft), respectively as shown in Figure 3. The retracing and deviated patterns had longer extra paths than the efficient pattern. However, the retracing and deviated patterns did not differ from each other statistically.
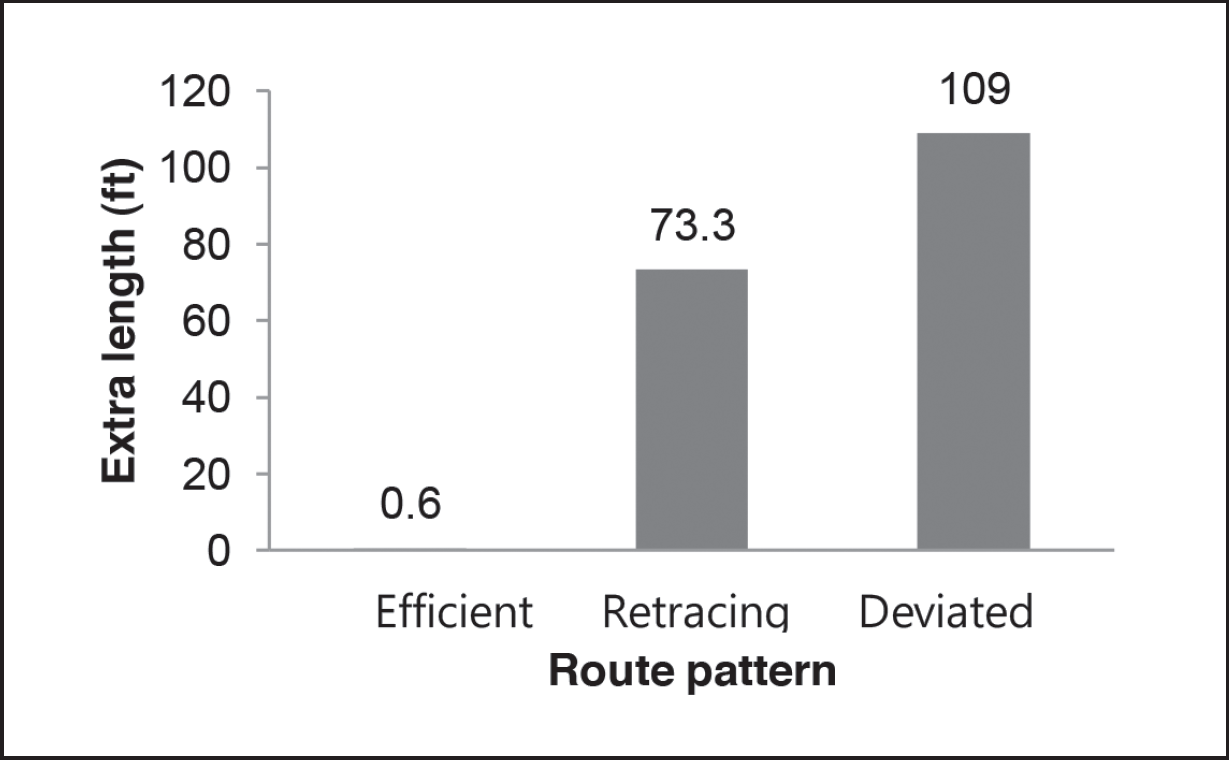
Comparison of extra path lengths among the route patterns. The three route patterns differed significantly from each other in terms of extra path length (p <. 01). The efficient, retracing, and deviated patterns had mean extra lengths of 0.6, 73.3, and 109.0 feet, respectively.
New Nurses vs. Experienced Nurses
The researchers divided the nurses into two groups based on level of experience: new nurses with less than 1 year and experienced nurses with more than 1 year of work experience. Unit nurses suggested that 1 year was an appropriate cutoff point for experience levels. In spite of the small sample size, there was a clear difference between the new and experienced nurses. The mean number of interactions was .5 for the new and 2.2 for the experienced nurses. The mean number of extra stops was .5 and 1.4, and the mean extra path length was 29 ft and 63 ft, respectively, as shown in Figure 4. The results indicate that, in general, new nurses performed more efficiently than the experienced nurses.
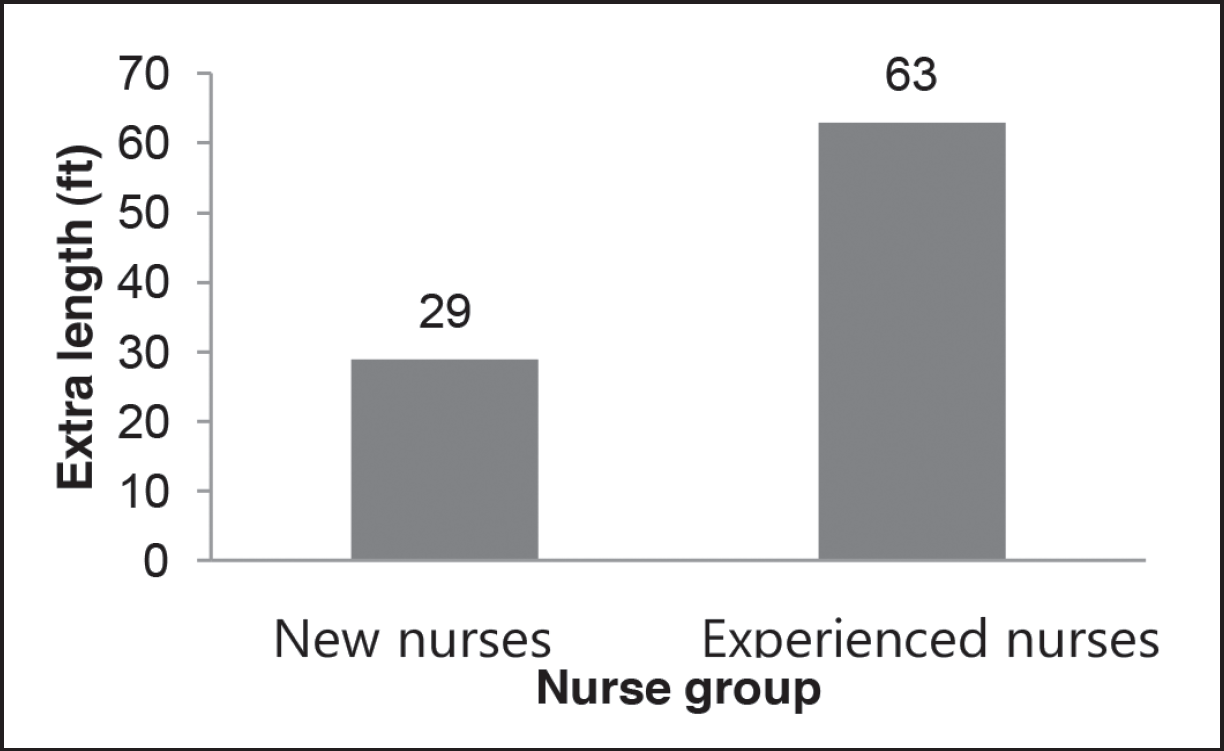
The comparison of extra path lengths in relation to new and experienced nurses. Experienced nurses walk more (63 ft) than the new nurses (29 ft) in terms of extra path length.
A close examination of route patterns also showed interesting differences between new and experienced nurses. The data showed that six experienced nurses and two new nurses fell into the efficient pattern, two experienced and two new nurses fell into the retracing pattern, and seven experienced and no new nurses were part of the deviated pattern group. In other words, the new nurses divided equally into two patterns: efficient and retracing. Similarly, the experienced nurses were nearly equally divided into two patterns: efficient and deviated. The results suggested that the new nurses were less likely to deviate from their paths, whereas experienced nurses were less likely to retrace their paths.
East Wing vs. West Wing
The researchers compared the nurses' observed walking behavior in relation to the east and west wings. When the number of extra stops and extra lengths were compared, the differences between the two wings were surprisingly high, as shown in Figure 5. Average walking distance was 203 ft in the east wing and 117 ft in the west wing. The east wing had a mean of 2.3 extra stops, which is statistically higher than the mean of the west wing at 0.2 extra stops. The east wing had an extra path length mean of 93 ft—statistically higher than the mean of the west wing at 22 ft.
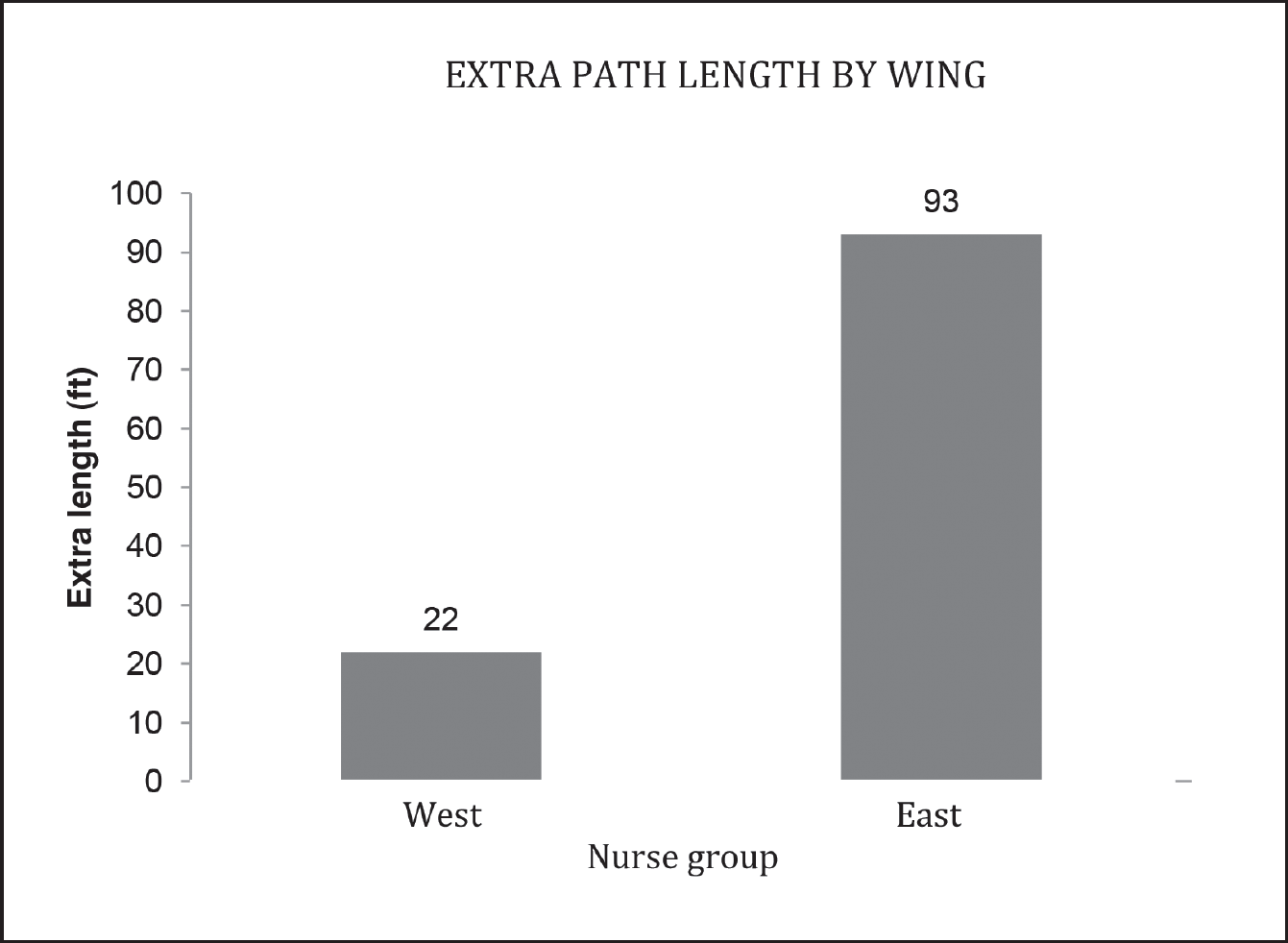
Comparison of extra path length between the east and west wings in the same setting. The east wing had a mean extra path length of 93 ft, which is statistically higher than 22 ft for the west wing.
The researchers also compared route patterns in regard to the east and west wings, as shown in Figure 6. Almost 70% of the west wing routes showed an efficient pattern, compared to only 10% in the east wing. No routes in the west wing showed a deviated pattern, whereas 70% in the east wing did. The east wing has many more deviated paths than the west wing.
Discussion
These results demonstrate that the observation method focused on a specific task was useful for showing the effects of unit layout and for testing-related hypotheses. As mentioned earlier, the observation of a specific task allowed researchers to identify deviations from the baseline and efficient behavior for a specific task; the deviation explained how unit layout affected nurses' behavior.
Based on these observations, neither of the hypotheses was supported. The findings that nurses in a smaller layout did not walk less and experienced nurses deviated more than new nurses were not intuitive. However, it is possible that these findings have been confirmed by other studies (Seo et al., 2011), and with close examination of the observation results these findings might challenge the simple assumption that nurses would walk less if they worked in a smaller unit when different levels of nurse experience and unit design are taken into account. The patient-centered care concept mainly affected the design of patient rooms and did not seem to affect nurses' walking behavior. This behavior might be more affected by the layout of functional spaces, such as the patient room, nurses' station, supply room, and medication area.
Nurses' Experience Level
The results showed noticeable individual differences in walking behaviors during medication administration in an ICU in regard to new nurses and experienced nurses. One hypothesis was that experienced nurses walk less than new nurses, who may seek additional help during the medication task. However, this hypothesis was not supported by these results in that they indicated that experienced nurses had more interactions, more unnecessary stops, and longer walking distances than new nurses.
As shown in Figure 4, new nurses were equally divided between the efficient and the retracing patterns. Experienced nurses were equally divided between the efficient and deviated patterns. Almost half of the new nurses went to the medication/supply room twice or more to perform a medication administration task; a very small proportion of experienced nurses did so. The experience level of the nurses might have influenced their movements and activities for this specific task.
The data also showed that five of seven instances of the deviated walking path pattern occurred because of interactions, i.e., talking with other nurses; all of these interactions involved experienced nurses. It is possible that the experienced nurses were more social than the new nurses. Another explanation is that the experienced nurses were likely to be more capable of interacting during the medication administration task than new nurses, who might have been more focused on the task itself. Experienced nurses might also have helped others more; however, data were not collected to verify these suppositions.
Effects of Spatial Layout: East Wing vs. West Wing
Nurses in the east wing were expected to walk less than the west wing because of its smaller size. However, this was not necessarily the case for nurses in the east wing; they had more extra stops and extra walking distance, which resulted from deviations from the most efficient routes. The results of our field observations contradicted the findings of previous studies (Modern Hospital, 1965a, 1965b; Shepley & Davies, 2003; Sturdavant, 1960; Trites et al., 1970). The design of the east wing had more of the radial layout characteristics, such as direct visibility and accessibility to patient rooms from the nurses' station (see Figure 1), so these findings might be confirmed by another study using the same methods. The study investigated nurses' walking behavior using the same method for two differently designed units: one smaller radial unit layout and one larger racetrack layout (Seo et al., 2011). The study also found that nurses did not walk less in the smaller radial unit; in fact, they walked significantly longer distances, deviating from the most efficient walking path.
The general shapes and average length of the paths among unit components alone seem insufficient to explain the walking behaviors during the medication task observed in this study.
In the current study, behavioral differences between the two wings were also surprisingly high in terms of extra stops, extra walking distances, and the composition of the three route patterns, as shown in Figure 7. The mean value for extra path length was 93 ft in the east wing group—almost four times that of the west wing. As shown in Figure 6, most of the routes—7 out 10, in fact—in the west wing showed efficient patterns, whereas most of the routes—7 out of 9—in the east group showed deviated patterns.
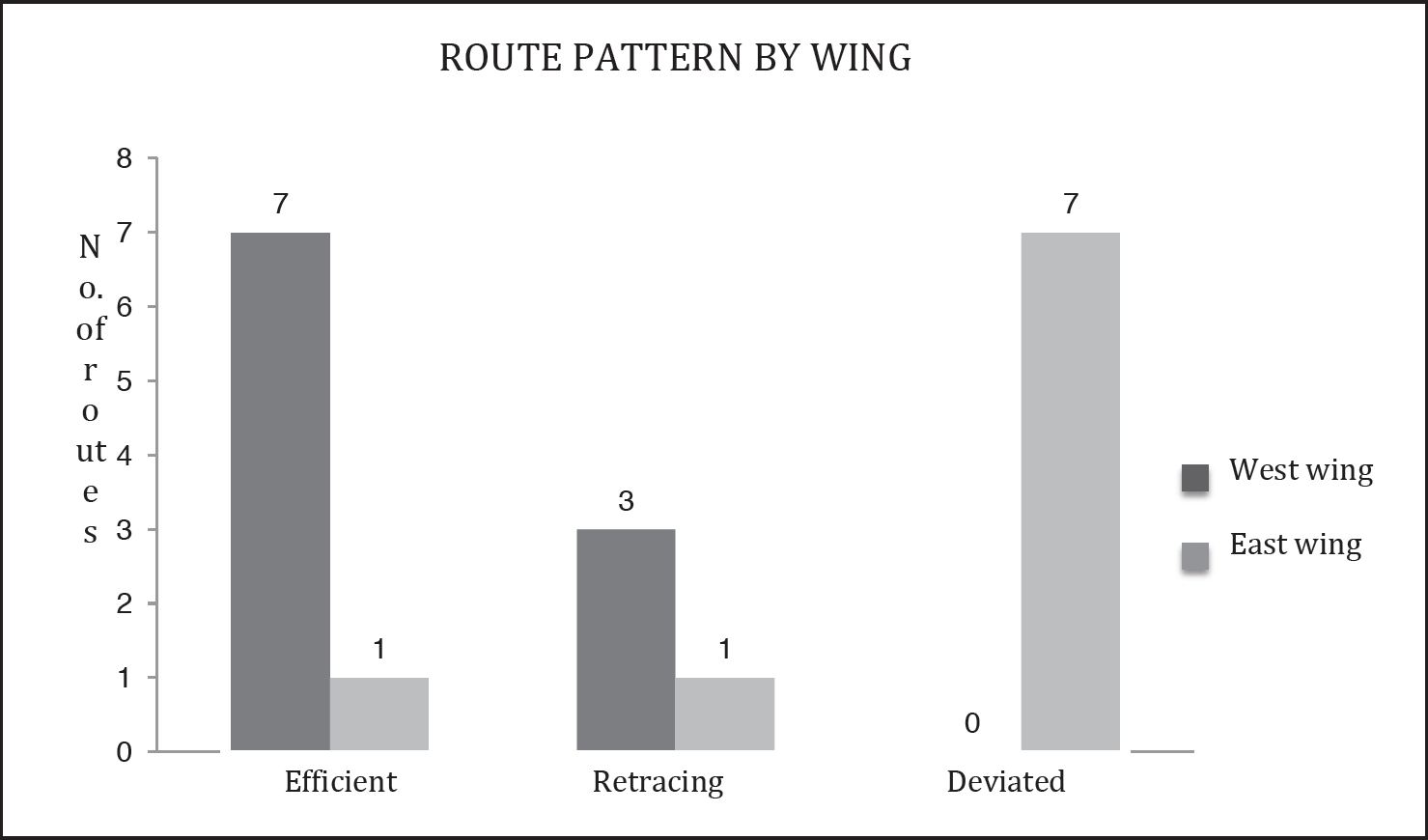
Differences in route patterns between the east and west wings. Seven of 10 routes in the west wing showed an efficient pattern, whereas only 1 of 9 in the east wing did. No routes in the west wing showed a deviated pattern, whereas 7 of 9 in the east wing did.
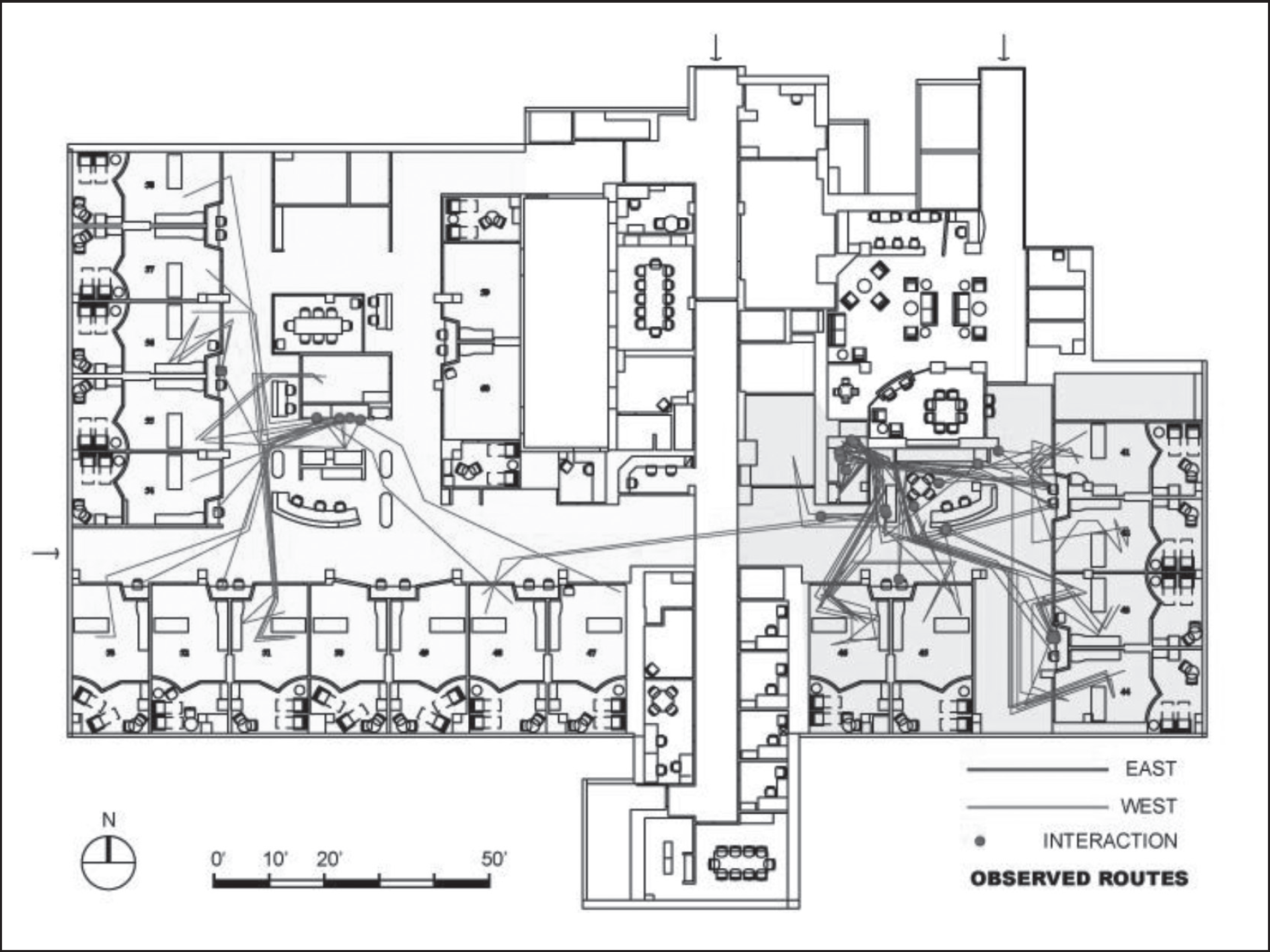
All observed routes in the unit. Routes in the east wing had statistically more extra stops and also were longer than those in the west.
Search for the Mechanism
The most important goal for this research was trying to find the underlying spatial properties that contributed to the behavioral differences identified in this study. Neither general unit shape nor the Yale Traffic Index explains the results of this study. The west wing had a racetrack hallway and the east wing had an L-shaped hallway. The layout of the east wing was more like a radial design than the west wing. In addition, the east wing was much smaller than the west wing. According to the findings of previous studies (Shepley & Davies, 2003; Sturdavant, 1960; Trites et al., 1969; Trites et al., 1970), nursing staff in the east wing should have walked less than staff in the west wing. The Yale Traffic Index study indicated that the east wing should have been more efficient, because it was smaller and had shorter average paths among its components, such as the supply room and nurses' station. However, data in the present study suggested exactly the opposite.
It is possible that nurses in the east wing walk more only during the medication administration task but less during the entire shift compared to those in the west wing: only future studies can verify this. Nevertheless, the general shapes and average length of the paths among unit components alone seem insufficient to explain the walking behaviors during the medication task observed in this study. When all of the efficient routes for the medication administration task were placed on the floor plan, an interesting pattern emerged, as shown in Figure 8. All the efficient routes in the east wing pass through the central nurses' station, where many of the staff work. However, the efficient routes in the west wing only passed close to the central nurses' station. It is possible that, rather than the general shape of the units as a whole, the spatial relationship between the efficient route and the central nurses' station strongly influences the frequency of interactions among nurses.
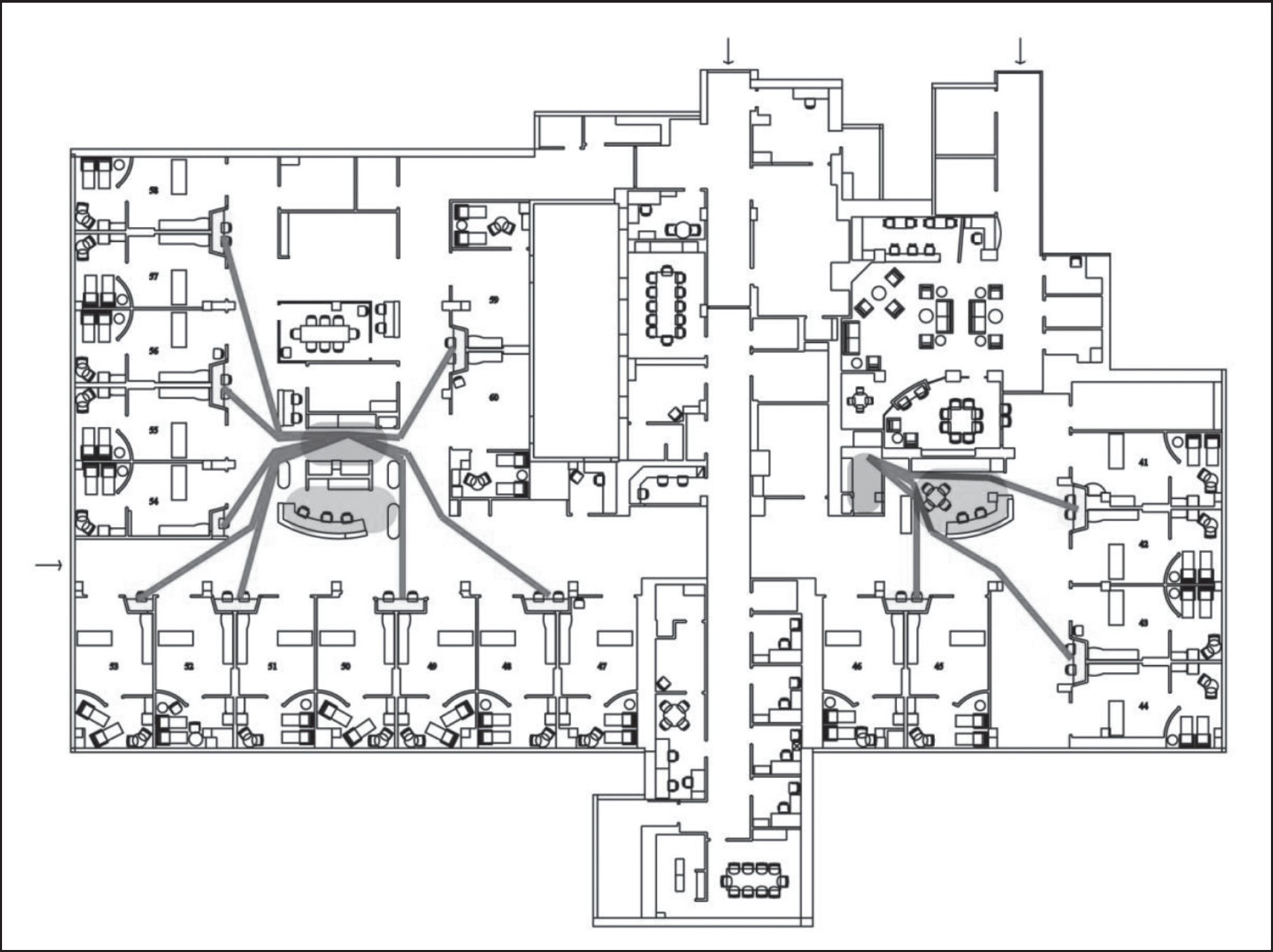
Efficient routes (red lines) to the medication distribution room (gray) from each alcove (yellow). Routes in the east wing passed through the central nurses' station (blue), whereas routes in the west wing did not.
Based on these results, the specific microspatial relationships between the different unit components, rather than their overall spatial properties such as size, shape, average path length, etc., weigh more heavily in influencing nurses' interactions and walking behavior. In the present case, it seemed that the proximity of the efficient paths to the central nurses' station in the east wing increased the number of interactions and the deviation from the efficient routes.
The results of this study seem to relate to the finding of one recent study, which focused on nurse interaction and physical locations in the same setting (Lu & Zimring, 2011). That study showed that more nurses can be expected in the areas with higher visibility regarding patient beds, especially during interactions. Because efficient paths to the medication distribution room overlap with high-visibility zones of both patients and other nurses in the east wing, the layout might provide more opportunity for interaction.
Interactions and Extra Stops as Interruptions
Nurses in the east wing had significantly more interactions and extra stops than those in the west wing. As mentioned earlier, face-to-face verbal communications were considered interactions. Although it was outside the scope of this study to examine the nature of the interactions and extra stops, these behaviors were likely to be interruptions of the medication administration process since the nurses were not supposed to be distracted from the task because of the potential for medication errors. The radial-like unit configuration, which allowed visibility of each other and the paths going through the nurses' station, might have resulted in the nurses being interrupted more frequently in the east wing than the west.
It is well known that nurses routinely experience interruptions, which can cause medical errors (Pape, 2003; United States Pharmacopoeia, 2003). Managing interruptions can have a salubrious effect on performance; studies have shown empirically that interruptions can increase medical errors (Flynn et al., 1999; Westbrook, Woods, Rob, Dunsmuir, & Day, 2010). In fact, given that the majority of interruptions were from other people and not from phone calls and equipment alarms (Biron, Loiselle, & Lavoie-Tremblay, 2009; Drews, 2007; McGillis Hall, Pedersen, & Fairley, 2010; Scott-Cawiezell et al., 2007; Trbovich, Prakash, Stewart, Trip, & Savage, 2010), the physical environment can play an important role because it determines people's visibility and accessibility (Bafna, 2003).
Conclusions and Design Practice Suggestions
It is interesting to see that previous studies favored the radial unit layout in terms of work efficiency and patient safety. However, in this study and at least during the medication task, the radial unit layout seemed to have the opposite effect in regard to walking distance and interruptions. The difference between the previous studies and this study might be the different scope of the research: previous studies focused on overall walking distance for all activities; this study focused specifically on walking during the medication administration task. However, the overall unit layout—i.e., radial, single-corridor, or double-corridor—could not explain the results.
A close examination of paths to the medication supply room revealed that the proximity of the paths to the central nurses' station could influence the frequency of interactions during medication administration, as mentioned earlier. Combined with other studies (Seo, 2011; Seo et al., 2011), this study provides potentially significant new findings in that a unit design such as a radial layout can affect interruptions; if verified by additional studies, this finding could change current design practice. The researchers believe that paths to the medication area or room should be carefully designed to avoid high visibility of other staff members to reduce walking distance and interruptions during the medication administration task. Future studies should further examine this claim considering other tasks.
Future Study Directions
Observing task-specific activities has allowed researchers to document detailed information about recorded walking behavior for a task. Thanks to this detailed information, researchers can suggest additional methodological developments. One of the next steps could be the quantification of route properties that can be correlated to the behavior associated with these routes (i.e., extra stops or extra distance). In other words, would it be possible to find some quantitative measures regarding the routes to predict nurse behavior?
In this study, researchers hypothesized several measurements of route properties that might inspire further research. The first variable, called the closeness value, was to assess whether these routes pass through the central nurses' station. A value of 1 was assigned to a route passing through the central nurses' station, and a value of 0 was assigned to a route that did not. The closeness value can better predict route behavior, as shown in these results.
The second variable, called the path visibility index, measured the nurses' work areas, including both the central nurses' station and alcove that could be seen from the route. The quantified visibility from the path to the nurses' work areas could thereby be calculated. This could be done using new techniques developed by one of the authors (Lu, 2010). Lu developed innovative techniques that can quantitatively measure the visibility of meaningful targets, such as patients. The easier it was to see the nurses' station and alcove from the routes, the more nurses saw and interacted with other staff members, and as a result, the nurses were more likely to deviate from the efficient routes.
Overall, these findings need further investigation because of the small sample size. However, this investigation introduced a useful method and suggested a different perspective from previous studies. Observing task-specific activities was more efficient for the current research topic than traditional tracking or mapping methods, which covered the entire nursing shift. In future studies, researchers can verify the findings of this study with a larger sample size and also explore the differences in the effects regarding different nurses' work areas, such as nurses' stations and alcoves. Observing tasks other than medication administration can be explored as well. Observation of medication administration can also be further developed to examine the relationship between the physical environment, interruptions, and medication errors.