
Abstract
OBJECTIVE:
This comparative study in two ICUs examines the impact of the patient-centered unit design on family involvement, operationalized as percentages of family presence and family–patient/family–staff interaction in patient rooms.
BACKGROUND:
As hospitals have become more patient-centered, there has been a trend toward including a family area inside the patient area to promote family presence, support, and involvement in patient care. There is growing evidence that family members play an important role in supporting patient care, and that the physical environment affects family involvement. However, few empirical studies have attempted to show the effectiveness of the patient-centered design on family members' presence and their behavior.
METHODS:
This study compared the degree of family presence and family–patient and family–staff interactions in two intensive care units (ICUs) with different physical environmental conditions, but housing patients of similar acuity and disease type.
RESULTS:
The analysis identified a significant difference in family presence in patient rooms (t = −2.176; df = 79.0; p = 0.03) between the traditional and the patient-centered units. Patients in the family-centered care unit (M = 37.77; SD = 34.02) spent significantly more time with their family members in patient rooms than did patients in the traditional unit (M = 23.89; SD = 21.90). Patient-related variables other than unit design had no significant impact on family presence and interactions.
CONCLUSIONS:
Findings demonstrated that the patient-centered unit (5K) was associated with increased family presence in the patient rooms and increased family interaction with patients, when compared with the traditionally designed unit.
Keywords
Introduction
The patient-centered care concept has persisted for more than three decades since Planetree identified a need for patient-centered care that assures that “care should be organized first and foremost around the needs of patients” (Planetree, 2012). Numerous hospitals have been built upon the inherent principles underlying this concept (France et al., 2005). One of the most frequently utilized facility features has been the inclusion of a family area inside the patient room that promotes family presence, support, and involvement in patient care. However, few empirical studies have attempted to show the effectiveness of the design feature on family members' presence and their behavior. Therefore, to verify this effect, we observed family members in the units of two hospitals with different design concepts, one of which was traditional and the other patient- and family-centered intensive care units. We believe that the theory of affordances by James J. Gibson (1979) provides a useful framework for a more thorough understanding of these effects. According to Gibson (1979), “The affordances of the environment are what it offers the animal,” including the human, “what it provides or furnishes, either for good or ill” (p. 127) and it “implies the complementarity of the animal and the environment” (p. 127). Gibson also stated that the composition and the layout of surfaces constitute what they afford and different layouts afford distinct behaviors for a variety of animal species and humans, and different mechanical encounters. In fact, this investigation is a comparative study that demonstrates how the affordances of an environment can affect human behavior. The design of the patient rooms in one of the two units afforded more activities for family members (e.g., staying over night).
The patient-centered care concept has persisted for more than three decades since Planetree identified a need for patient-centered care that assures that “care should be organized first and foremost around the needs of patients.”
Patient-Centered Care and the Role of the Family Members
Patient-centered care, one of the six goals of the Institute of Medicine (IOM) for improving the quality of care in hospitals (Institute of Medicine, 2001), is defined as “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” (IOM, 2001, p. 6). In recent years, patients have increasingly sought more involvement in their own health care, particularly with the support of their family members (IOM, 2001). Patients rely on family members to ask questions about procedures, to help them understand medical information, and to make sure that complete care is given (Meyers et al., 2000). The assertive and supportive roles of family members are particularly important when patients are critically ill because, in many instances, the patients are unable to make decisions or speak for themselves and have limited sources of support. In critical care environments, family members become the spokespersons for and the protectors of their loved ones, who may be compromised physically and/or psychologically (Hupcey, 1998). Therefore, patient-centered care also needs to be family-centered.
Providing appropriate care and consideration to family members and encouraging them to take an active role in patient care may help them effectively address patients' various needs and preferences. In fact, the Institute for Patient- and Family-Centered Care advocates care that recognizes the vital role that families play in ensuring the health and well-being of individuals and families in all settings where they receive care and support, and it emphasizes “an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care providers, patients, and families” (The Institute for Patient- and Family-Centered Care, 2013).
The theory of affordances by James J. Gibson provides a useful framework for a more thorough understanding of these effects.
The Positive Impact of Family Members and Their Presence on Patients' Clinical Outcomes
Family members play a critical and positive role in patient care. Some studies have actually demonstrated that the presence and interaction of family members improve patients' clinical and psychological outcomes (Chatham, 1978; Happ et al., 2007; Hendrickson, 1987). An experimental study involving 20 male patients who underwent open-heart surgery investigated the impact of patient–family interaction on patients' postoperative behaviors in an acute care setting (Chatham, 1978). For decades, postcardiotomy psychosis, a condition in which patients exhibit certain disturbing post-operative behaviors (e.g., impairment of orientation, memory, intellectual function, and judgment), has been a major concern. The study found that patients with certain types of support and interactions with family members (e.g., eye contact, frequent touch, and verbal orientation to time, person, and place) exhibited fewer manifestations of postcardiotomy psychosis (Chatham, 1978).
In a time-series quasi-experimental study involving 24 patients at risk of complications due to an increase in intracranial pressure (ICP), researchers observed a decrease in patients' intracranial pressure when family members were present (Hendrickson, 1987). In a qualitative study of 30 patients being weaned from long-term mechanical ventilation (LTMV), Happ et al. (2007) found that family presence, support, and interaction (e.g., touching, talking, and bedside surveillance) helped patients better cope with their treatment process and facilitated their clinical progress. The study showed that patients were able to manage significantly longer daily weaning trials when family members were present (p < 0.0001).
The Physical Environment and Family Presence and Involvement: Single Patient Rooms, Private Areas, and Flooring
Emerging evidence has demonstrated the positive impact of the physical environment on family members' behaviors and responses, including their presence and interaction with hospitalized loved ones or staff members. Studies identified that certain environmental and physical design factors such as single-patient rooms, private discussion areas, or carpeted flooring are associated with greater family presence and interaction, plausibly because by providing suitable spaces for families, family members spend more time with and provide care for hospitalized loved ones (Chaudhury, Mahmood, & Valente, 2005; Ittelson, Proshansky, & Rivlin, 1970; Kirk, 2002; Quan, 2006; Sallstrom, Sandman, & Norberg, 1987; Ulrich, Zimring, Quan, & Joseph, 2004; Ulrich et al., 2008).
Several studies have identified the positive impact of single-patient rooms on family presence and their interactions (Chaudhury et al., 2005; Ittelson et al., 1970; Kirk, 2002; Quan, 2006; Sallstrom et al., 1987). A review paper by Chaudhury et al. (2005) identified several studies that found that patients preferred single-patient rooms. In the United Kingdom, Kirk (2002) found that the majority of patients preferred a single room because it afforded greater privacy and a more accommodating environment for family members, it reduced noise and embarrassment, and improved quality of sleep. Similarly, in the United States, a survey conducted in assisted-living facilities demonstrated that 82% of respondents preferred a private room (Ittelson, Proshansky, & Rivlin, 1970). The authors also noted that private rooms proffered greater freedom with regard to patient behaviors and activities in their rooms. A comparative evaluation of family visitation between single- and multi-bed patient rooms found that patients' family members and other visitors stayed significantly longer (about 35% longer) in single rooms than in multi-bed rooms (Quan, 2006). In addition, the same study showed that patients and family members in units with single rooms reported higher satisfaction than those in units with multi-bed rooms (Quan, 2006). Another survey study conducted in neonatal intensive care environments found that single-patient rooms were perceived to be less stressful for both family and staff than open-bay multi-bed rooms, likely the result of the greater privacy and control over the environment with respect to noise, lighting, temperature, and traffic (Harris, Shepley, White, Kolberg, & Harrell, 2006).
Other studies demonstrated that providing single patient rooms and additional private discussion areas within a unit could facilitate communication among patients, family members, and staff (Astedt-Kurki, Paavilainen, Tammentie, & Paunonen-Ilmonen, 2001; Kaldenburg, 1999). A study by Astedt-Kurki et al. (2001) identified several factors that facilitated or complicated interactions among adult patients' family members and nursing staff. Using a questionnaire, data were collected from 155 nursing staff working on wards and in outpatient departments at a university hospital in Sweden. Interestingly enough, one of the factors complicating interactions was the absence of a peaceful place for discussion and the staff's haste, shift-work, and family members' shyness in approaching the staff. Semi-private patient rooms are perceived as busy places where roommates and their families can overhear discussions. This study implies that private and peaceful places contribute to improved communication. Kaldenberg (1999) found that staff members in multi-bed rooms, out of respect for patient privacy, are reluctant to discuss patient issues or to provide information when they are within hearing distance of a roommate. National survey data also show that patients in single rooms consistently report significantly higher satisfaction with communication with nurses and physicians than patients in shared rooms (Kaldenberg, 1999).
In addition, Harris (2000) identified that the use of carpeted flooring instead of vinyl flooring in telemetry unit patient rooms was associated with an increase in family presence. Findings of this study demonstrated that family members and friends in patient rooms with carpeted flooring stayed substantially longer during visits than those in patient rooms with vinyl flooring. In addition, Ulrich et al. (2008) identified several other advantages of carpeting: noise reduction (Philbin & Gray, 2002), greater ease of walking and perceived safety of the elderly (Wilmott, 1986), and a reduction in fall-related injuries (Healey, 1994); at the same time, they recognized concerns regarding infection control (Anderson, Mackel, Stoler, & Mallison, 1982; Beyer & Belsito, 2000; Boyce, Potter-Bynoe, Chenevert, & King, 1997).
Affordances of the Environment
The affordances of the environment are what it offers individuals, and it is perceived properties of the environment that support the individual's actions (Gibson, 1979). We believe the effects of the physical environment in hospitals, such as single versus multi-patient rooms or designated versus no designated family zones in patient rooms, can be explained by the affordance theory. Studies on affordances of the environment often examine outdoor areas such as playgrounds, towns, or neighborhoods, for their environmental resources supporting certain activities, often for children (Clark & Uzzell, 2002; Cosco, Moore, & Islam, 2010; Kyttä, 2002, 2004). We propose that studies in healthcare will demonstrate increased family presence when the physical environment offers better affordance for family activities. In addition, because they are private and suitable in size to provide comfortable personal space for two to three family members, single-patient rooms with a designated family zone provide greater affordance for seating and sleeping and opportunities for private conversation with patients and caregivers. In our study, patient rooms in one of the units offer greater affordance for seating more than two family members near the patient, storing belongings, and lying down or staying overnight. We believe that the extent to which patient rooms provide affordances contributes to the behaviors of family members.
Recent Trends in Practice
Recognizing the crucial role of family presence in patient care and associated improvements in clinical and psychological outcomes, an increasing number of critical care units are cultivating a more patient- and family-centered culture. Strategies employed often include policies that do not restrict family visitation and the provision of comfortable family zones in patient rooms and family areas in public areas that encourage family presence and involvement (Douglas & Douglas, 2004; Douglas & Douglas, 2005; France et al., 2005; Rashid, 2006; Seo, Choi, & Zimring, 2011). Furthermore, the 2010 Guidelines for the Design and Construction of Healthcare Facilities now provide specific design provisions for patient- and family-centered rooms. For example, the Guidelines recommend that all single-bed rooms have a clear floor area of 250 square feet, an additional minimum of 30 square feet per family member, and a home-like atmosphere (The Facility Guidelines Institute, 2010).
Interestingly enough, even though an increasing number of hospitals have adopted patient-and family-centered design, scarce empirical research has been devoted to understanding the impact of the physical environment on family presence and involvement in acute care settings. Therefore, this exploratory study aims to understand whether or not patient- and family-centered ICU design (i.e., spacious patient rooms with delineated family zones and accommodations and comfortable and accessible public family areas elsewhere on the unit) affects family presence and their interactions with patients and staff members. Through a series of observations, this study compares a patient- and family-centered ICU with a traditionally designed ICU that has smaller patient rooms lacking a delineated family zone.
Research Questions
This study addresses the following topics and research questions:
Methods
This study compared the degree of family presence and family–patient and family–staff interactions in two intensive care units (ICUs) with different physical environmental conditions, but housing patients of similar acuity and disease type.
Study Settings and Research Design
The study was conducted in two ICUs, the 5K neurological ICU (Figure 1) and the 2D trauma ICU (Figure 2), both at Tampa General Hospital (TGH) in Tampa, Florida. These units were selected for comparison because they are similar in terms of operation but considerably different in terms of their physical design. A nursing leader recommended these units for comparison because the patients are similar in acuity and the unit policies regarding visitation are the same (visitors are permitted 24 hours a day, 7 days a week). Doctors administer care to patients in both units, and one nursing director manages and nurses rotate between the units, depending on the workload. However, one unit (5K) was built with patient-centered care in mind, while the other unit (2D) was built before that concept was adopted by the hospital. As a result, the physical designs of the two units differ considerably (see Figures 3, 4, and 5, below).
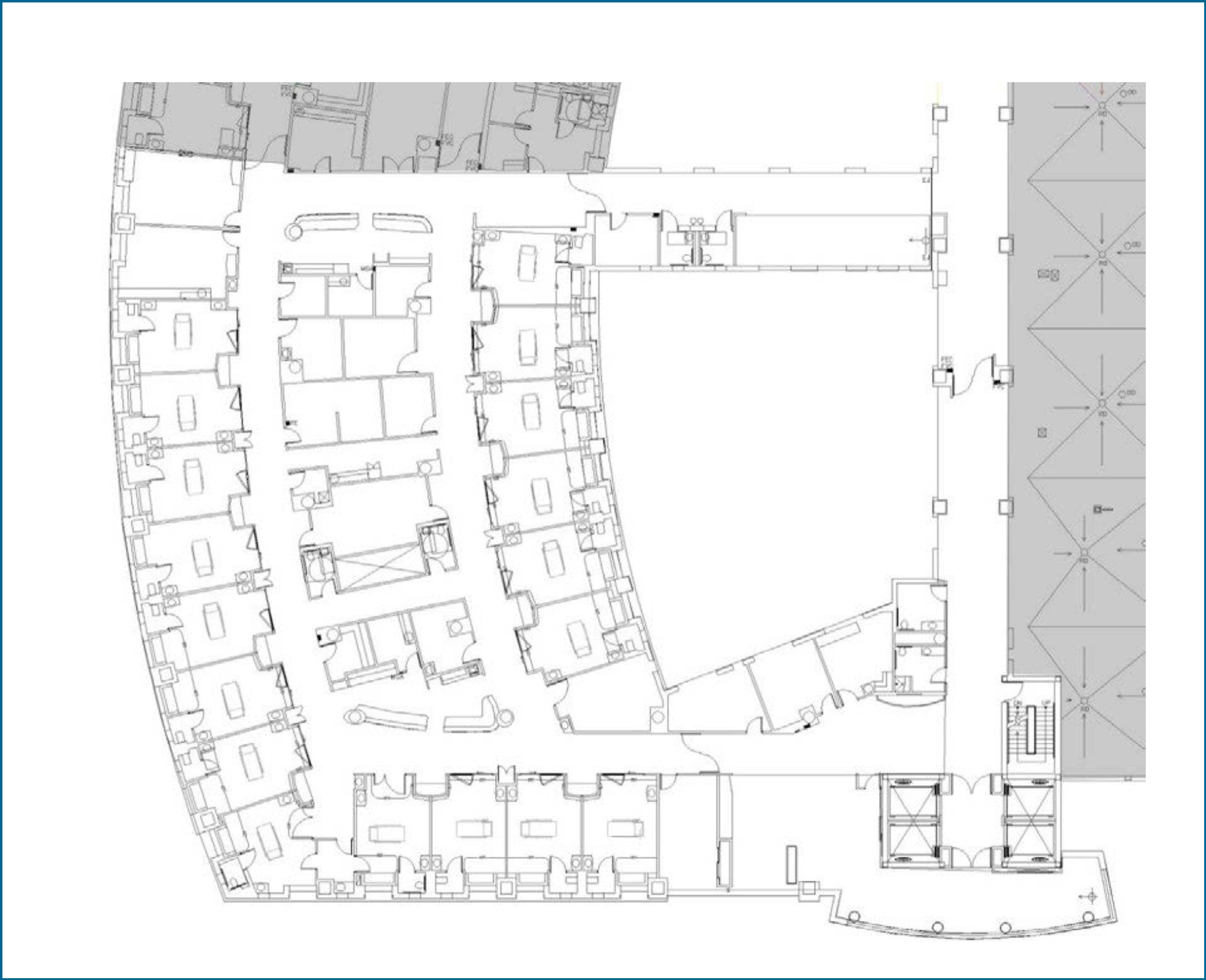
Patient-centered unit: 5K neurological ICU floor plan (1/32″ = 1′–0″).
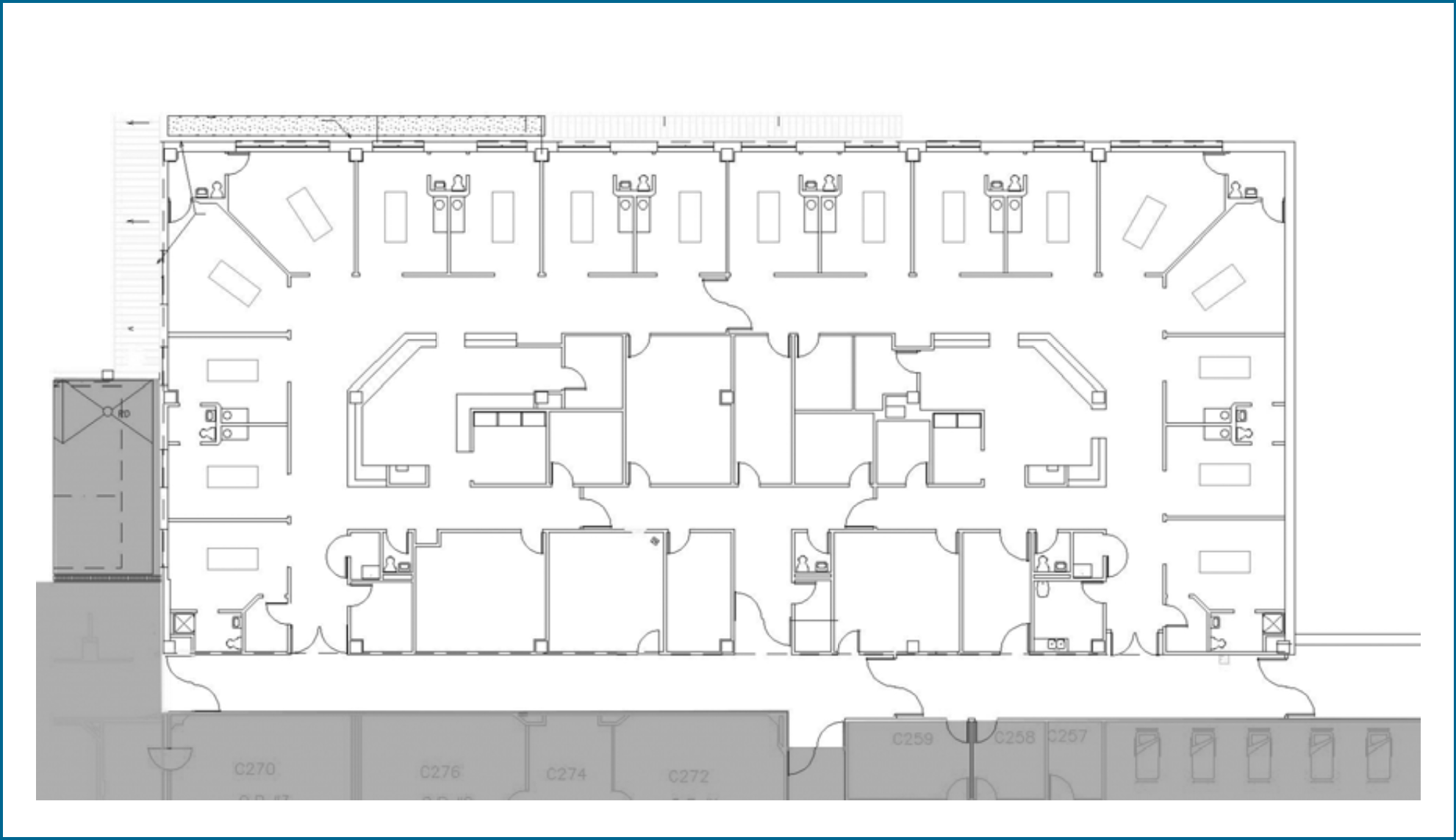
Traditional unit: 2D trauma ICU floor plan (1/32″ = 1′–0″).

A patient room in each unit.
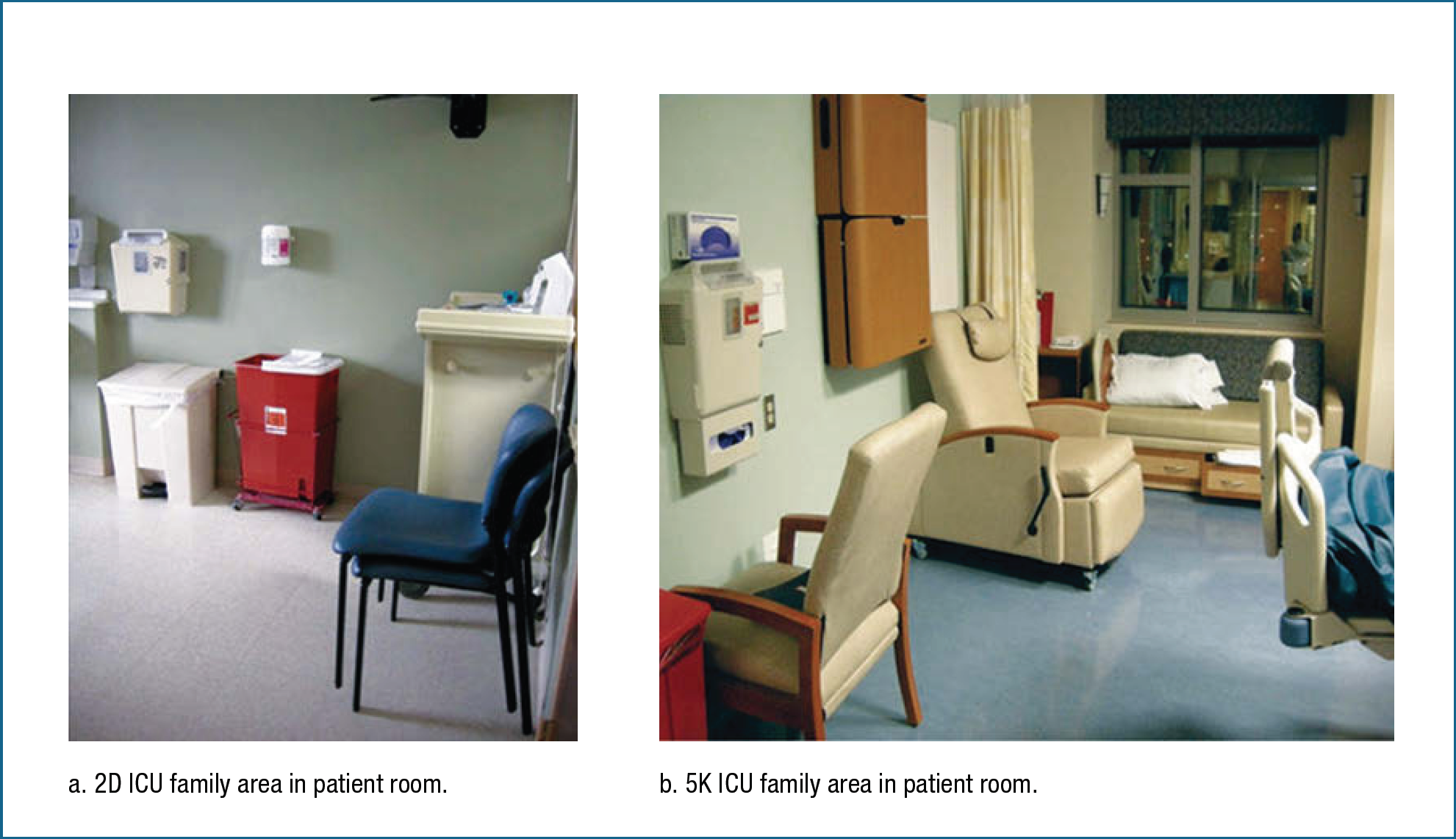
A family area in a patient room.
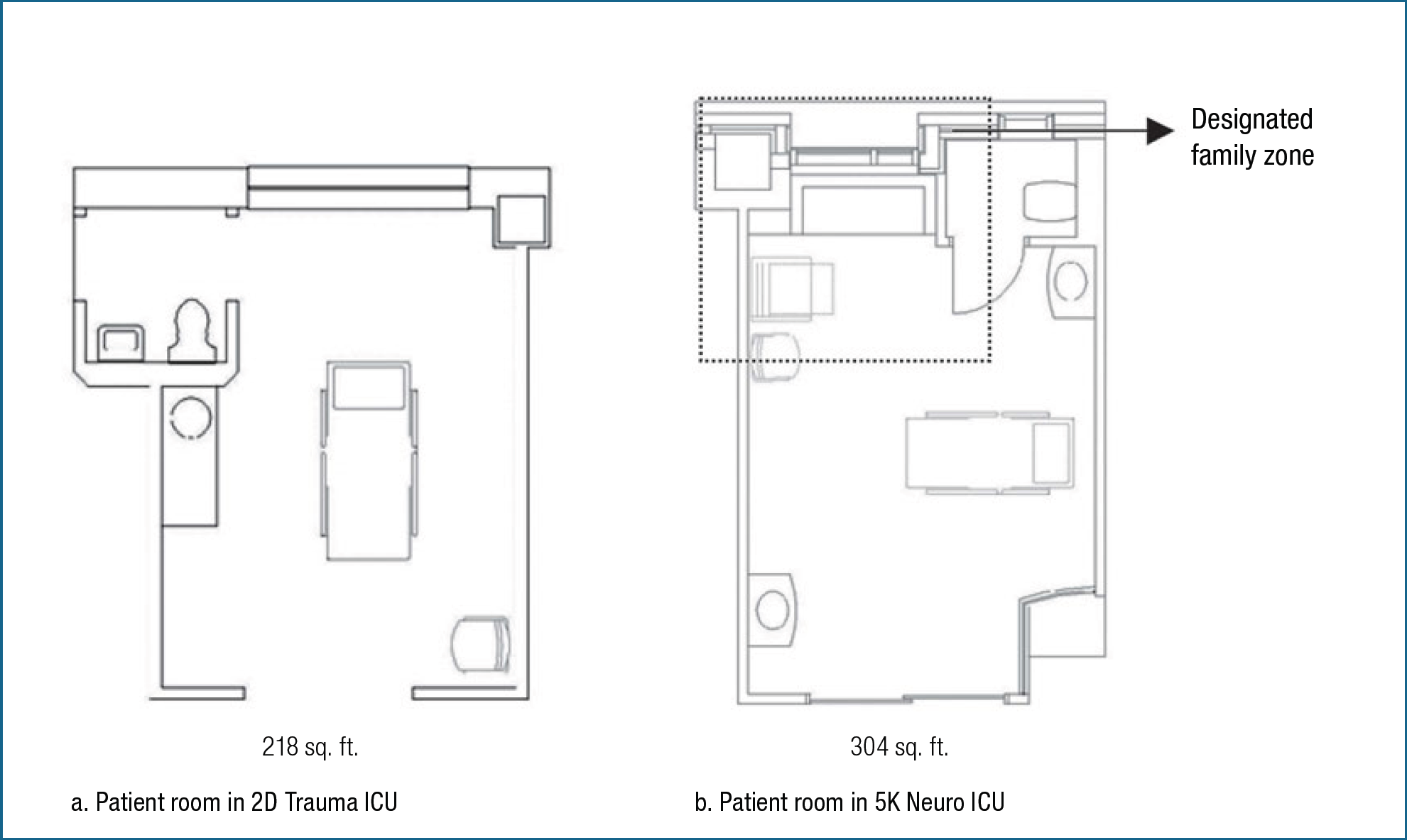
The design typology and size of the patient rooms (1/8″ =1′–0″).
The 5K neurological ICU, designed as a patient- and family-centered unit, includes larger spaces and more comfortable accommodations for visitors than the 2D trauma ICU. Patient rooms in the 5K ICU are 40% larger (304 square feet) than those in the 2D ICU (218 square feet) (see Figures 3, 4, and 5). The patient rooms in the 5K ICU have a clearly designated family area (approximately 60 square feet) in each room that includes the following accommodations: a sleeper sofa, a recliner, a non-reclining chair, and a privacy curtain. In contrast, patient rooms in the 2D ICU, regarded as a traditionally designed unit, do not provide a designated family area and offer a small, non-reclining chair for one or two visitors. We compared family presence and interaction between the two units and used behavior mapping to collect observational data for quantifying family presence in patient rooms and on the units as well as family interactions with patients and staff. Informal interviews with nurses were used to collect patient data (e.g., level of consciousness), variables that may plausibly affect family presence and interaction.
Behavior Mapping
Behavior mapping, a research method involving the direct observation and systematic recording of peoples' locations and activities (Cosco et al., 2010), is a non-intrusive, direct observation method for understanding the behavioral dynamics of a built environment. Useful for linking behavior with environmental attributes (Cosco et al., 2010), behavior mapping can be useful for both the identification of environmental affordances and particularly design practice because it records the precise location of people on floor plans instead of categorized locations such as indoors, outdoors, patient rooms, or family areas. Researchers have used this method for recording children's outdoor activities and other patients' activities (Bell & Smith, 1997; Cosco et al., 2010).
Cosco and his colleagues (2010), using behavior mapping methods, observed entire areas by systematically scanning behaviors of children in two childcare settings. They recorded the locations of subjects on a paper floor plan and used handheld computers with pull-down menus to record gender and physical activity level based on the Child Activity Rating Scale (CARS), a five-point scale ranging from “sedentary” to “vigorous” activity. Bell and his colleagues (1977) utilized behavior mapping to quantify changes in the behavior of Alzheimer's (dementia) patients. They first identified 36 behaviors that they wanted to record. On each observation day, an observer walked a predetermined path in the unit and checked each patient for 36 different behaviors. Observed behaviors were recorded on a check sheet, and the total frequency of the behaviors was tabulated at the end of the day. This sweep of the 24-bed unit occurred every 30 minutes and took about 10 to 20 minutes to complete. The method does not require the same daily census, but a change in census might affect the outcomes of the observations, so it requires an extended observation period of several weeks.
In our study, we were interested in the presence of family members and their interactions with patients and caregivers. We recorded the locations of people and their activities at the same time on the floor plans of both units studied. We documented whether or not family members were interacting with a patient or a staff member, and if so, whether the interaction was physical or verbal. This approach allowed us to quickly sweep the entire unit every 15 minutes instead of every 30 minutes. We believe the relatively small number of behaviors observed improved the accuracy of the observations. To train and test inter-rater reliability, two researchers conducted the same observations simultaneously in an ICU of another hospital (not the test site), and inter-rater reliability for behavior mapping reached 95% before the researchers started the observations at the study sites.
Procedure
During an observation sweep or round, the observer, the first author of this study who had had experience in behavior mapping, walked around one of the units on a pre-determined path that allowed her to visually inspect every space in the unit (excluding bathrooms or behind closed doors). The observer recorded the locations of people, their roles (i.e., family member, visitor, or staff member), and interactions on the floor plan during each round. Each round was completed every 15 minutes over a 12-hour period (10 a.m. to 10 p.m.) on each observation day. The observer recorded physical and verbal interactions between family members and staff as well as family members and patients. The physical interactions included activities such as holding hands, providing water, rubbing hands or feet, cleansing the face, combing hair, and changing the position of a patient. After each round, the researcher followed up with the nurses to differentiate family members from other visitors or staff when a new person showed up in the patient rooms.
The observer conducted 12 hours of observations per day for 10 weekdays (5 weekdays per unit) over a 5-week period (2 consecutive weekdays per week—1 day in one unit and the next day in the other unit). Researchers limited observations to weekdays (Monday through Thursday) to avoid introducing noise in family presence data on weekend days.
Subjects
Researchers observed a total of 105 patients during the study with some being observed more than once. A total of 24 patients were excluded for one of two reasons: They had been admitted to the unit less than 24 hours (11 patients), or they were out of their rooms for more than 1 hour for diagnostic or treatment activities (13 patients). The explanation for the first is that newly admitted patients who are in the unit less than 24 hours may not have as much family presence because family members may not have yet been contacted or because they may be en route to the hospital from out-of-town locations; and the reason for the second is that family presence in patient rooms is typically low because family members often accompany the patients to diagnostics and treatments that take place outside of the patient room. Therefore, such situations may preclude an accurate assessment of family presence in the patient room.
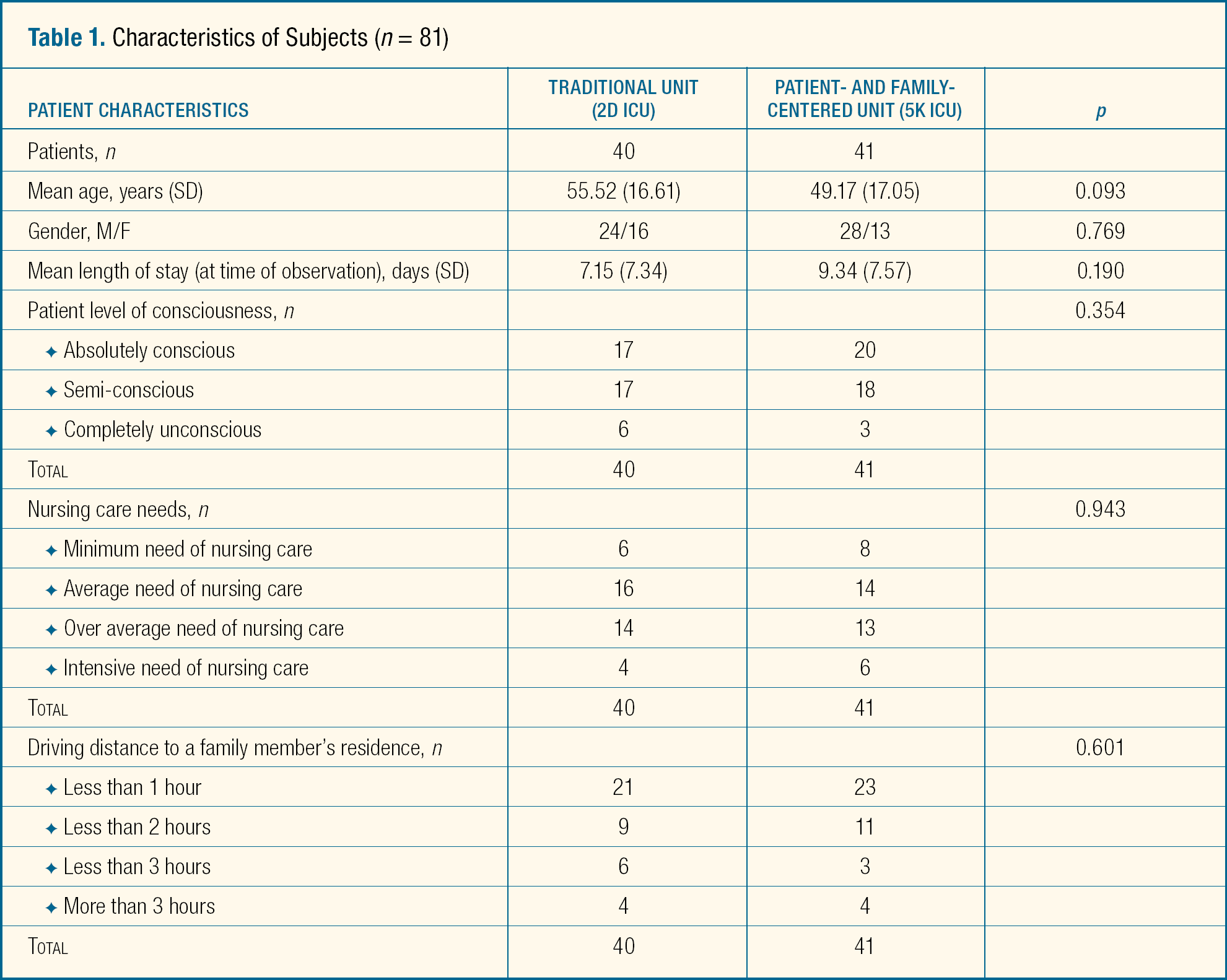
Among the 81 patients included in the analysis (see Table 1), some were observed more than once. Since the unit of analysis for this study was a patient, we included only one 12-hour observation period per patient, randomly selected, in this study. Each patient had 49 data points of observation, so a total of 3,969 total data points were included in the analysis.
Characteristics of Subjects (n = 81)
Dependent Measures
To evaluate dependent variables, we collected behavior mapping data. First, we measured family presence in patient rooms as the percentage of presence (out of a total of 49 observations during the 12-hour period) of at least one family member. For example, if a family member was present in a patient room during 27 of the 49 observations, family presence in the patient room was 55%. Then we measured the interactions between family members and the patient (physical or verbal) as the percentage of observations out of a total of 49 observations in which family members were interacting with the patient. Finally, we measured interactions between family members and staff (physical or verbal) as the percentage of observations out of a total of 49 during which any family member present interacted with a staff member. To examine potentially confounding variables, we also evaluated patient characteristics (both demographic and clinical), entered the data for the dependent measures into Microsoft Excel, and then analyzed the dependent measures and patient characteristics using the statistical analysis program Statistical Packages for the Social Sciences (SPSS) 20 for Windows.
Informal Interviews
During the observations, the researcher asked nurses specific questions about the observed patients in order to identify patient-related variables that may affect family presence and interaction (refer to Table 1, above). These variables included
Patient length of stay at the time of observation.
The level of consciousness (i.e., absolutely conscious, semi-conscious, and completely unconscious).
The amount of nursing care the patient required (i.e., minimum, average, above average, or considerably above average, according to Levenstam and Bergbom, [2002]).
Driving time to the family member's residence (0 ≤ hour < 1; 1 ≤ hours < 2; 2 ≤ hours < 3; or hours ≥ 3).
In most cases, nurses referred to patients' medical records and asked family members to provide data on driving time to their residence. Anecdotal evidence suggests that these variables are plausibly related to family presence and interaction, potentially serving as confounding variables. Therefore, researchers collected and analyzed these patient-related variables to determine their associations with the dependent variables (i.e., family presence and interaction). If we had found an association with the dependent variables, we would have had to control the impact of these variables to isolate the impact of unit design on the dependent variables.
Statistical Analyses
For the statistical analyses, we used a two-step process. First, we conducted a Pearson correlation analysis that identified patient-related variables significantly associated with the dependent variables. Because the main interest of this study lies in the impact of unit design on family presence and interaction, we had to determine whether or not unit design and the dependent variables (i.e., family presence and family–patient/family–staff interaction) were significantly associated. However, it was also important that we identify patient-related variables other than unit design that were significantly associated with the dependent variables and then control the impact of the patient-related variables other than unit design by introducing appropriate statistical techniques in order to isolate the impact of unit design on the dependent variables. If the Pearson correlation analysis had identified a significant association between any patient-related variables other than “unit design” and the dependent variables, we would have had to employ multivariate regression analyses to control the impact of the patient-related variables other than unit design. If not, we would have had to conduct independent sample t-tests to identify statistically significant differences in the dependent variables between the two different unit designs. However, the results of the Pearson correlation analysis revealed no significant association between the patient-related variables other than unit design and the dependent variables. (The results will be further discussed in the Results section, below; also see Table 2.) This finding indicates that unit design is the only patient-related factor associated with the dependent variables. Therefore, as a second step, we employed an independent samples t-test to identify any statistically significant differences in the dependent variables between the two different unit designs (traditional versus patient- and family-centered units).
Correlation Matrix for Independent and Dependent Variables (n = 81)
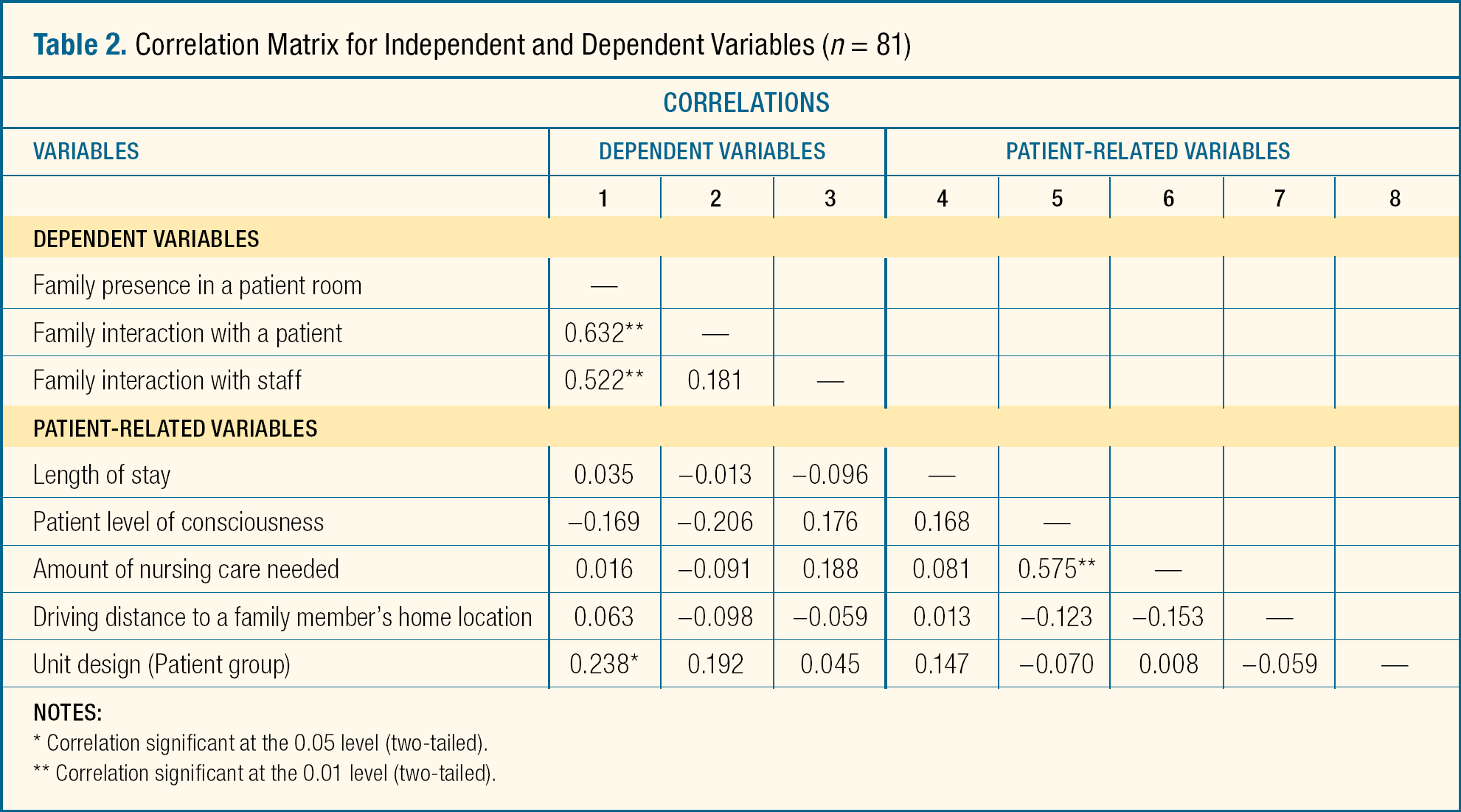
Correlation significant at the 0.05 level (two-tailed).
Correlation significant at the 0.01 level (two-tailed).
Results
Unit Design
The Pearson correlation analysis demonstrated that only one patient-related variable (i.e., unit design) was significantly associated with the dependent variables, and none of other patient-related variables were significantly associated with the dependent variables (Table 2). In other words, only the unit design affected the dependent variables (i.e., the degree of family presence in patient rooms and family–patient or family–staff interactions) and other patient-related variables (i.e., patient length of stay, the level of patient consciousness, the amount of nursing care needed, or driving distance to a family members' home location) did not affect the dependent variables (i.e., the degree of family presence in patient rooms and family–patient or family–staff interactions).
Family Presence and Family–Patient/Family–Staff Interaction
The Pearson correlation analysis also revealed significant positive correlations between family presence and family–patient and family–staff interaction at the level of p < 0.01 (see Table 1, above), indicating that family–patient and family–staff interactions increase as family presence in patient rooms increases and providing a possible answer to the question of whether longer family visits are actually necessarily associated with greater family interaction and involvement in patient care. Such associations indicate that family presence near the patient potentially affects the level of family interaction with patients and/or staff, which in turn affects family involvement in patient care.
The Patient Level of Consciousness and the Amount of Nursing Care Needed
The analysis also revealed a significant positive correlation between a patient's level of consciousness and the amount of nursing care required, indicating that the amount of required nursing care increases as the patient level of consciousness weakens. (Higher scores of the patient level of consciousness indicated that the patient's level of consciousness was weak.) However, because many factors could affect a patient's nursing care needs, we question the significance of this finding. Studies have provided evidence that patient acuity determines patient nursing care needs (Hughes, Iezzoni, Daley, & Greenberg, 1996; Iezzoni, Ash, Schwartz, Daley, Hughes, & Mackiernan, 1995), and as predicted, a patient's level of consciousness is only one of many factors that determine patient acuity (Bastos, Sun, Wagner, Wu, & Knaus, 1993; Knaus, Draper, Wagner, & Zimmerman, 1985). However, according to the results of the current study, as the nursing care needs of neurological or neurological-related trauma patients increased, their level of consciousness decreased.
Because the Pearson correlation analysis identified no significant associations among the patient-related variables (other than unit design) and the dependent variables, we employed an independent samples t-test to identify any statistically significant mean differences between the dependent variables of the two units (or between patient groups determined by differences in unit design). Findings from the independent samples t-test addressed the two research questions of the current study.
Unit Design and Family Presence in Patient Rooms (Research Question 1)
The analysis identified a statistically significant difference between family presence in patient rooms (t = −2.176; df = 79; p = 0.03) in the traditional and that in family-centered units (Table 3). The findings demonstrated that patients in the patient- and the family-centered care unit (M = 37.77; SD = 34.02) spent significantly more time with their family members in their rooms than those in the traditional unit (M = 23.89; SD = 21.90).
Unit Design and Family Presence and Interaction
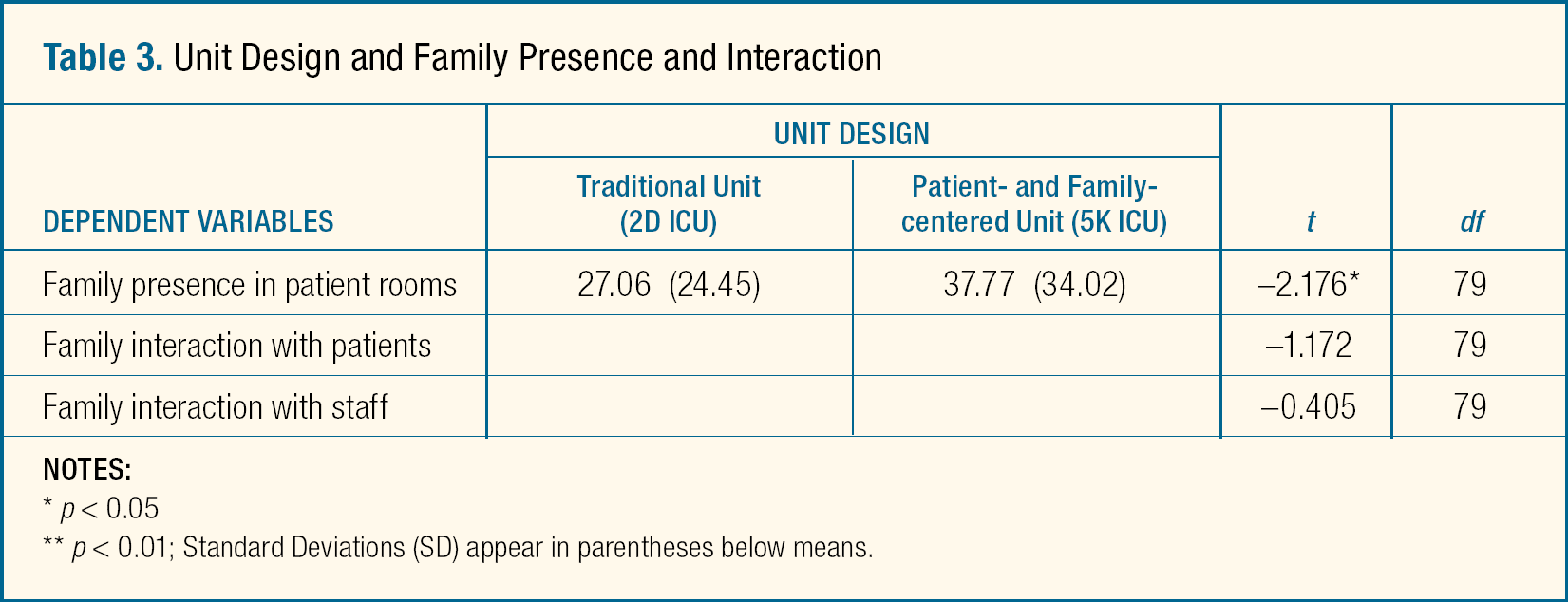
p < 0.05
p < 0.01; Standard Deviations (SD) appear in parentheses below means.
To validate the results, researchers ran an additional independent samples t-test to determine any statistically significant differences among the other patient-related variables (e.g., patient age, length of stay, or patient level of consciousness) that might have affected the dependent variables in the units (see Table 1, above). The results of the test identified no significant differences, suggesting that the patients in the two units were similar enough that these characteristics did not explain the observed variability among the dependent measures. Therefore, we assume that the degree of family presence is influenced by the design (i.e., traditional or patient- and family-centered) of the unit.
Unit Design and Family–Patient or Family–Staff Interaction (Research Question 2)
The findings identified a marginally significant difference in family–patient interaction (t = −1.712; df = 79; p = 0.09) and an insignificant difference between family–staff interaction (t = −0.405, df = 79, p = 0.68) in the units (see also Table 3). Findings demonstrated that family members in the patient- and the family-centered care unit (M = 10.66; SD = 12.16) interacted more (i.e., it was marginally significant) with their hospitalized loved ones than those in the traditional unit (M = 6.67; SD = 8.05), but the findings did not show significant or marginally significant differences between family–staff interactions in the units. These findings suggest that if unit design allowed for more family presence, the degree to which families and patients interacted would increase, but not the degree to which families and staff members interacted.
Discussion
Anecdotal evidence has suggested that having a designated family zone in patient rooms will increase family presence and support in patient care (France et al., 2005). As this study demonstrated that family members in the patient- and family-centered unit spent more time in patient rooms with their hospitalized loved ones than family members in the traditionally designed unit (p = 0.03), it not only confirmed that a designated family zone in patient rooms promotes patient–family interaction but also provided evidence that justifies the patient- and family-centered design approach. We believe this finding can be explained by the theory of affordances (Gibson, 1979).
Family members in the patient- and family-centered unit spent more time in patient rooms with their hospitalized loved ones than family members in the traditionally designed unit.
Although the study identified only a marginally significant effect on family–patient interactions (and a non-significant effect on family–staff interactions) in the units, it found significant correlations between family presence and family interaction with patients and staff, suggesting that a physical environment that encourages family presence can also afford family members increased opportunities for verbal and physical interactions with patients and staff, which in turn may lead to increased family involvement in patient care and physical and emotional support for patients. In addition, as mentioned before, some studies have suggested that family presence improves a patient's progress (Chatham, 1978; Happ et al., 2007; Hendrickson, 1987). Therefore, we can posit that family presence is emotionally, physically, and clinically beneficial to patients, but the mechanism that promotes such benefits has not yet been clarified.
A physical environment that encourages family presence can also afford family members increased opportunities for verbal and physical interactions with patients and staff, which in turn may lead to increased family involvement in patient care.
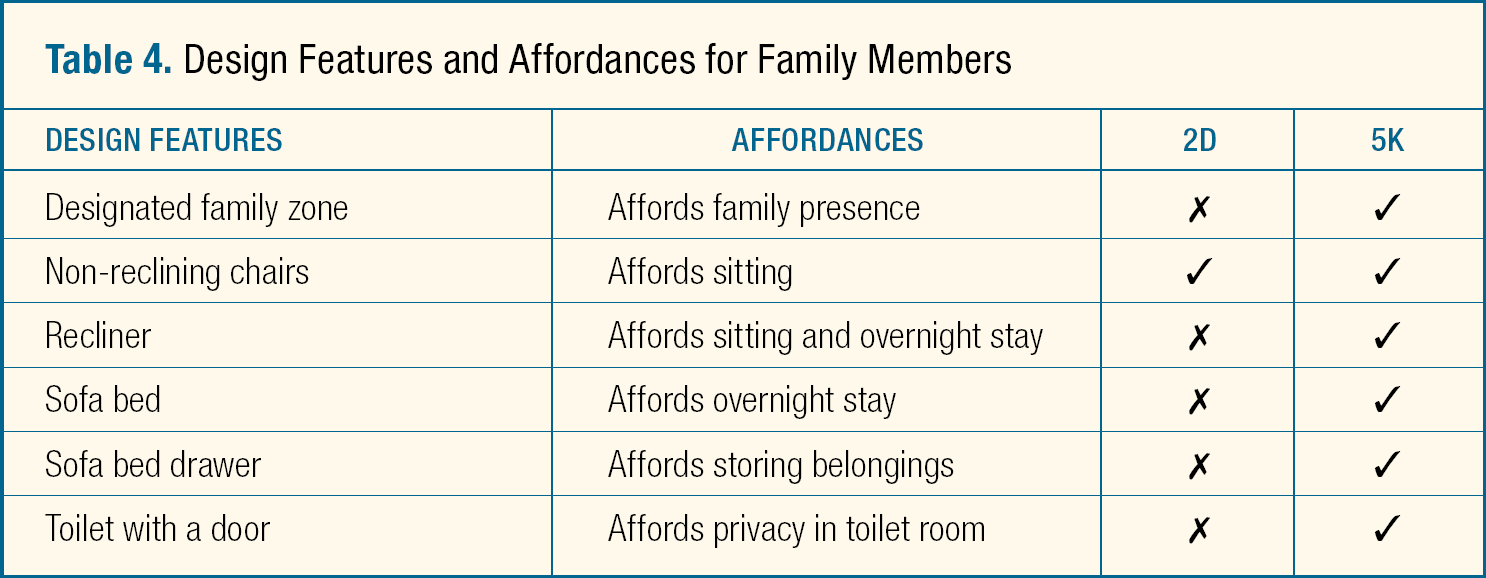
We believe that design features affording family members the ability to remain comfortably at the patient's bedside in 5K accounts for the increased presence of family members in the unit. Such design features are (a) a designated family zone or area with suitable square footage, which provides two to three family members with comfortable personal space at an appropriate distance from perceived-to-be staff areas; and (b) increased design features such as recliners, sofa beds, and sofa bed drawers that are larger and more ergonomically comfortable. Table 4 illustrates the design features and related affordance for the activities of family members. The ergonomically comfortable recliners and sofa beds in 5K may increase affordance perceived by visitors for prolonged sitting. In addition, a designated family area with such recliners and sofa beds may increase the perception that family members are welcome and encouraged to remain close to their loved one and to stay longer. By contrast, the hard-surfaced, non-reclining chairs in 2D were universally used but not specifically designed for family members.
Design Features and Affordances for Family Members
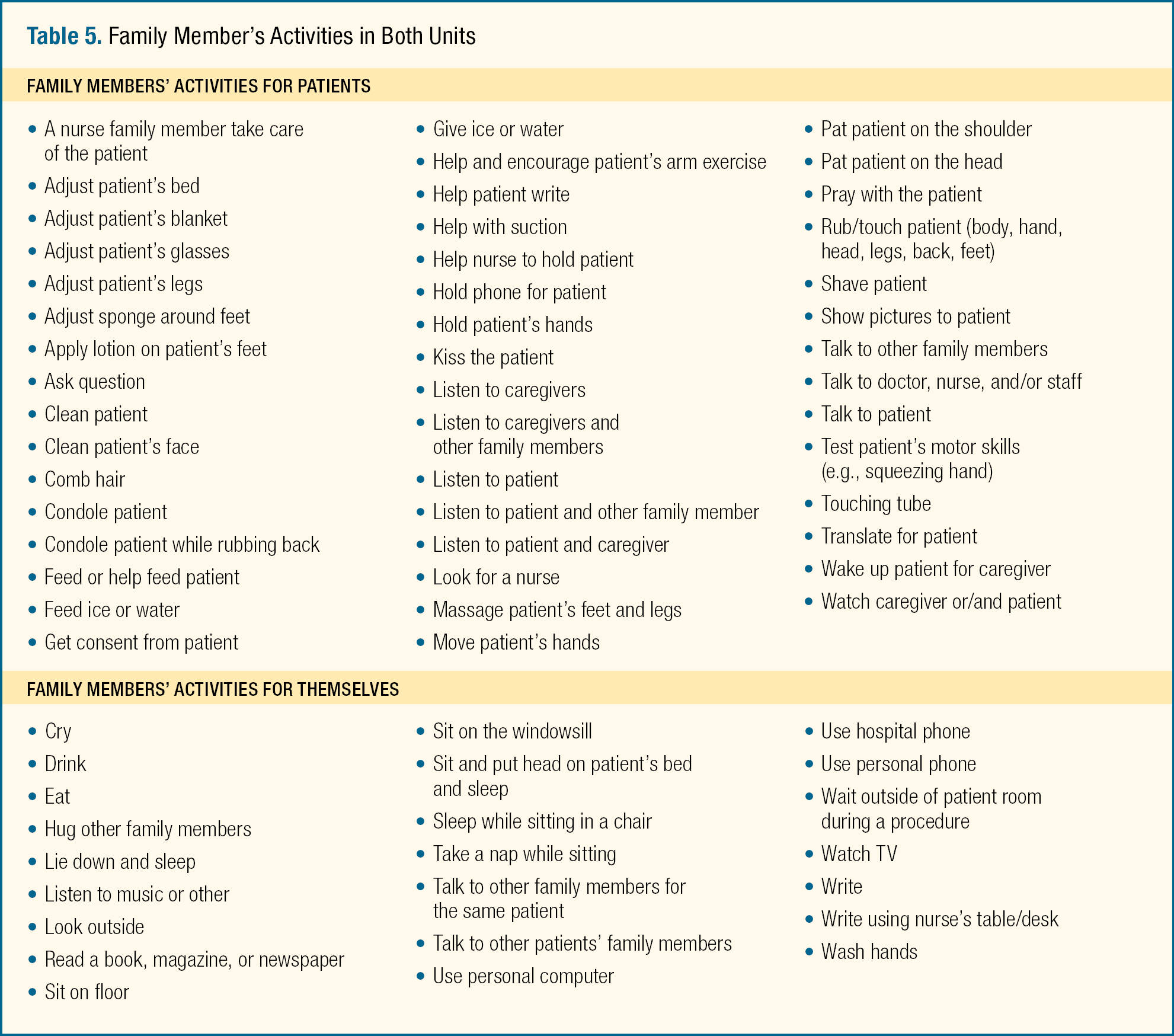
We recorded the activities of family members on the basis of convenience (Table 5). We did not have a pre-defined list of family behaviors to observe but were rather inclusive in recording various activities of family members that we could observe. Later, we categorized the activities into similar ones as we nearly approached a point that no more new activities of family members can be observed. Family members engaged in various activities to support patients, which was true in both units. Patients would miss out on this support if their family members were not nearby. Our documentation of family member activities demonstrates emotional and physical support, and it is not difficult to imagine that having family members next to patients is beneficial to the patients. While most of the family members' behaviors while in the units were similar, several behaviors such as sitting on the floor and on the windowsill in 2D were different, probably because of the limited space for family members in the unit. In addition, some family members in 5K brought their laptop computers and used them in the patient rooms, which was not observed in 2D.
Family Member's Activities in Both Units
Methodological Challenges
Other researchers faced unique challenges when identifying operational measures that accurately represented the degree of family presence and interaction with patients in the critical care settings. Studies pertaining to primary care settings have investigated the degree of family presence by simply measuring the duration of family presence in minutes through constant observations or audio or video tape recordings (Clayman, Roter, Wissow, & Bandeen-Roche, 2005; Ishikawa, Roter, Yamazaki, & Takayama, 2005; Jansen et al., 2010; Schmidt, Lingler, & Schulz, 2009; Street & Gordon, 2008) because the average length of patient visits for routine medical check-ups was only between 20.2 to 25.1 minutes (Wolff & Roter, 2011). However, unlike routine medical visits to primary care, the lengths of patient visits or stays in critical care settings vary significantly from one day to months, as does associated family presence. Therefore, measuring the duration of family presence in hours or minutes cannot be practically applied to patients in critical care settings. In fact, when researchers observed family members of patients in a neurological critical care unit in another hospital for 5 consecutive weekdays to further develop the methods and operational measures of this study, they identified the following trends:
The degree of family presence varied among patients: some family members visited their loved ones for 1 or 2 hours in the morning; some visited during the evening after work; and some stayed with their loved ones all day long.
The degree of family presence, however, remained similar throughout the weekdays per patient: family members hardly ever visited some patients; some only visited during the evening; and some almost always visited during weekdays.
Based on these preliminary observations, researchers concluded that to ensure that data are representative of the degree of family presence per patient, each patient needs to be observed at least 12 hours, mainly from 10 a.m. to 10 p.m., during which time most family members appear on the unit.
After determining the appropriate hours for observing each patient, researchers also faced another challenge in identifying appropriate methods that would allow researchers to observe a considerable number of patients during this 12-hour period in a manner appropriate for advanced statistical analyses. Considering the long hours of the observation period suggested for patients in critical care settings, it was not practical to measure the duration of the family presence in hours or minutes through constant observations (e.g., shadowing or tracking procedures) per patient. Through such continuous observation methods, researchers could observe only one or two patients during the 12-hour period. Therefore, the observer used behavior mapping procedures to quantify the degree of family presence through periodic observations (instead of constant observations) and to collect the data from a large number of patients (instead of one or two patients) during the 12-hour period. We designed the behavior mapping procedures used in this study to collect quantitative measures of family presence and interactions that did not include the actual duration of family presence and interactions but instead the proportion (percentages) of total observations made during the 12-hour per patient period. During the 12 hours (10 a.m. to 10 p.m.), each patient was observed a total of 49 times at 15-minute intervals. For example, if a family member was observed in a certain patient room only once in the 49 observations, the family member was most likely in the patient room less than 15 minutes. In this case, the operational measure of the family presence was 2% (1 out of 49 observations) instead of the actual duration of the presence (15 minutes).
The ultimate benefit of this method was an increase in the practicality of the study. With periodic observations, researchers were able to observe a large number of patients over 12 hours. We understand that such periodic observations provide only approximate estimations of the duration of family visits, but deviations (± 15 minutes from actual durations) are acceptable, especially in light of the practicality that the method adds.
Strengths
The strengths of this study include that the study investigated plausible patient-related factors that may affect the dependent variables but found no significant differences. Therefore, the significant differences between the dependent variables of the units can be solely attributable to the design of the unit. Another strength is that this study contributed to the body of knowledge in both substantive and methodological areas in the field of architecture. First, the study is one of the first attempts to explore the effects of unit design on family presence and involvement in intensive care settings. Second, the study developed both operational measures that represented the degree to which families were present and interacted with patients in critical care settings (see the “Dependent Measures” section, above) and unique behavior mapping procedures that facilitated data collection for the suggested operational measures.
Limitations and Future Directions
One limitation of the study is that although demonstrating that the patient- and family-centered unit design was associated with a higher degree of family presence in patient rooms, the study did not directly investigate family members' perspectives about and responses to designs, which might explain this association in more explicit terms. Further investigation could identify critical aspects of the design that encourage family members to stay longer with their loved ones and become actively involved in their care. Secondly, the patient data in this study (i.e., length of stay, level of consciousness, amount of required patient care, and distance to a family member's residence) were obtained through informal interviews with nurses rather than through direct review of facts or relevant clinical information on patient medical records or other clinical documents. Even though most nurses obtained this information by referring to patients' medical records or directly questioning family members, such data collection through interviews adds subjectivity to the data that could weaken their reliability. Therefore, for future studies, we recommend employing a more appropriate methodology (e.g., medical chart reviews) when collecting such patient-related data. That is, future study requires further refinement and validation of the potentially confounding variables. In addition, future research could account for other confounding variables affecting family presence and involvement in patient care. As recent studies suggest that window views and daylight may be associated with less pain and improved patient sleep and depression (BaHammam, 2006; Wakamura & Tokura, 2001 Martiny, 2004 Walch, Rabin, Day, Williams, Choi, & Kang, 2005; Ulrich, 1984; Ulrich et al., 2008), these variables may also influence family behaviors and presence. However, since window views and daylight were beyond the scope of this study, we did not record differences between window views and daylight of the units either qualitatively or quantitatively during the study in 2008. Now that the hospital has undergone a series of renovations of and additions to its buildings since 2008, and one of the study units (2D ICU) has been completely renovated, we are unable to identify the characteristics of these variables. Therefore, we recommend further research that account for the effect of window views and daylight on family behaviors and presence.
As hospitals struggle to remain competitive during this climate of healthcare reform, it is even more critical that they justify every square foot of space designed. Although a cost-benefit analysis was beyond the scope of this study, the investigation does signify an association between patient- and family centered units and increased family presence. Thus, hospitals need to recognize the important role of the physical environment, especially the patient- and family-centered unit design features, in encouraging family presence and involvement in patient care and incorporate such design features into the design of their current and future units. A logical next step in future research would be to determine whether family-centered design is directly associated with improved clinical outcomes for patients.
The investigation does signify an association between patient- and family-centered units and increased family presence.
Implications for Practice
Behavior mapping is a useful data collection tool for understanding relationships between the physical environment and occupant behavior.
A designated family zone with comfortable accomodations (e.g., sleeper sofa, recliner) for two or three family members should be included in intensive care patient rooms. It is plausible that the affordances of a family-centered design may also have benefits in the medical–surgical as well as other inpatient environments.
Providing a designated family zone in inpatient rooms will likely increase family member presence and support (emotional, physical) of patients.
Footnotes
ACKNOWLEDGMENTS
This research received a research grant from the American Institute of Architects (AIA) the Academy of Architecture for Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.