
Abstract
OBJECTIVE:
To assess expert knowledge, perceptions, and experience on the role of the built environment in the acquisition and transmission of healthcare-associated infections (HAIs), facility design decision-making considerations, and strategies for intervention through facility design and technologies.
BACKGROUND:
Healthcare-associated infections pose a serious and costly threat to public health in the United States. A growing evidence base suggests that the built environment can play a role in interrupting the chain of infection.
METHODS:
Semi-structured individual interviews and triads were conducted with 26 experts in hospital administration, architecture, interior design, infection control, and air and water quality. A grounded theory approach was used for interview coding and interpretation.
RESULTS:
Participants characterized the shift in thinking about the relationship between the built environment and HAI transmission as a “progression,” as accountability for infection prevention has expanded beyond clinicians. Organizational leaders aim to make informed design decisions, but this can be challenging due to the paucity of efficacy and return on investment data. Emerging interventions include copper impregnated materials, seamless flooring, and chilled beams.
CONCLUSIONS:
No single intervention is entirely effective in mitigating HAI risk; multiple interventions are needed. In addition to the built environment, human behavior must be considered, as noncompliance can render even the best designs ineffective. Increased multidisciplinary collaboration is needed to improve the application of evidence and experience in healthcare facility design. In the absence of conclusive evidence regarding interventions aimed at reducing HAI transmission, a combination of research data and practical experience should be used to inform design decisions.
Keywords
Healthcare-associated infections (HAIs) are a serious and costly threat to public health in the United States, afflicting an estimated one in twenty hospitalized patients and responsible for $28 to $33 billion in preventable healthcare expenditures annually (U.S. Department of Health & Human Services, 2012). Over the past decade, the importance of these infections as causes of preventable harm has gained increasing attention among both healthcare professionals and other groups, including consumer advocates, insurance providers, and legislators. Stimulated in part by legislative mandates and public reporting of HAI rates, expanded efforts have been made to eliminate preventable HAIs.
While the majority of efforts to date to reduce HAIs have focused on standardizing best practices in healthcare processes, there is growing evidence that the overall building design and its components, referred to as the built environment, can also play a significant role in the transmission of pathogens in healthcare settings. A range of design interventions has been asserted as affecting HAIs, including single-patient rooms, airborne-protective isolation rooms, better sink and toilet room design, antibacterial surfaces, cleanable surfaces, improved location of hand cleaning rubs and sinks, electronic hand hygiene reminder systems, and better air filtering (Bartley & Streifel, 2010; Ulrich et al., 2008).
Although the evidence base linking design to HAI is growing, the field largely remains an idiosyncratic patchwork of best practices and inferential steps from laboratory or epidemiological research. This article is the result of a large multidisciplinary project, examining the role of the environment in the acquisition and prevention of HAIs, which included an extensive literature review used to determine relevant topics for the interview guides. The complete results of the literature review can be found as topical reports available within this special supplement to HERD (Denham et al., 2013; Jacob, Kasali, Steinberg, Zimring, & Denham, 2013; Steinberg, Denham, Zimring, Kasali, Hall, & Jacob, 2013; Zimring, Denham, et al., 2013; Zimring, Jacob, et al., 2013).
We also sought to obtain a better understanding of current practice and potential areas for future research and development in this area through discussions with a multidisciplinary group of experts involved in design decision making in healthcare facilities. We sought their perceptions of the evolution of the role of the built environment in HAI transmission, including its impact on healthcare facility design and the application of evidence-based design. Other topics discussed included factors that may enhance or prohibit the adoption of innovative HAI risk-reduction strategies and the challenges of balancing patient- and family-centered care with HAI risk reduction.
Methods
We conducted in-depth interviews and triads with experts. An in-depth interview is a qualitative research technique that uses open-ended questions to explore an individual's detailed perspective on various issues and offers a complete picture of opinions and ideas. Triads (interviews with three participants) strike a balance between individual interviews and focus groups, in that they use fewer participants (3 versus 6–12 participants in focus groups), thereby enabling more in-depth discussion of issues than focus groups.
Participant Recruitment
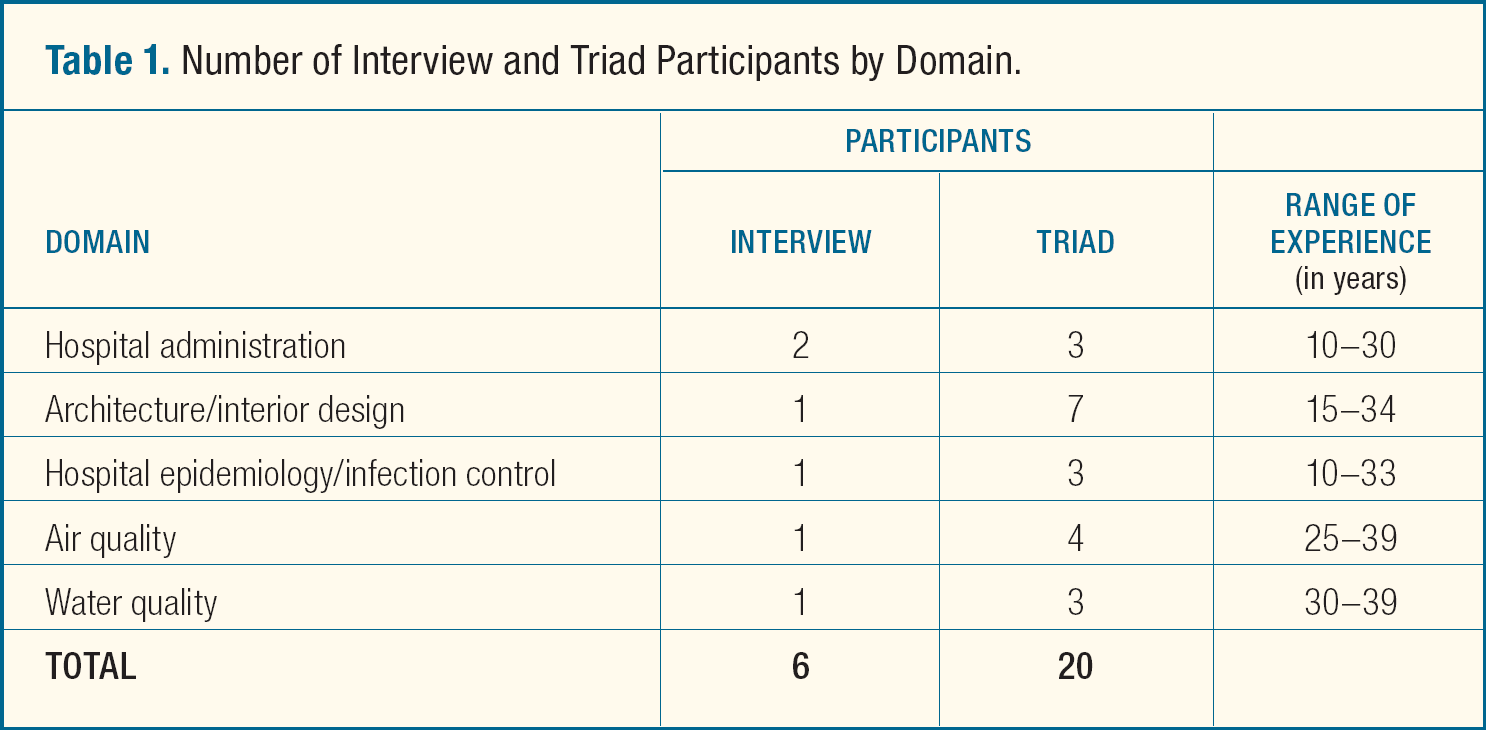
Interview and triad participants were recruited from the project team's extensive network of professional contacts, comprising a convenience sample. The sample included leading experts in the field of healthcare design and infection control, including presidents, CEOs, and CMOs of top healthcare organizations, and principals of major architectural firms. At the close of each interview and initial triad, participants were asked for recommendations of others who might be able to provide valuable insight as triad participants. This blend of convenience and referral sampling produced a diverse pool of experts across multiple domains. Nine experts were individually interviewed, and 17 experts participated in triad interviews. See Table 1 for the distribution and experience levels of experts across domains. This project was reviewed by the Institutional Review Board and received exempt status as research not involving human research subjects.
Number of Interview and Triad Participants by Domain.
Discussion Guides
We drafted an initial list of potential interview discussion topics and converted the topics into interview questions. Separate discussion guides were developed for each of the following domains: hospital administration, architecture, interior design, hospital epidemiology and infection control, air quality, and water quality. The interview and triad guides included questions pertaining to perceptions of the role of the built environment in mitigating infection risk in acute care hospital settings; the types of input that healthcare facilities seek from external sources regarding HAI prevention; currently used design strategies; promising strategies for the future; and issues and strategies that are particularly relevant to each respective domain (e.g., the air quality discussion guide included questions regarding high-efficiency particulate air (HEPA) filters, air flow strategies, and the use of ultraviolet germicidal irradiation (UVGI) to prevent spread of airborne infections). For a sample discussion guide, see Appendix A.
Data Collection and Analysis
Six semi-structured in-depth interviews and seven triads (three mixed triads, including participants from multiple domains, one air quality triad, one water quality triad, and one architecture/interior design triad) were conducted by telephone. See Table 1 for the number of participants broken down by interview type and domain. The interviews lasted approximately 1 hour; the triads lasted 60–75 minutes. All discussions were audio-taped to ensure accuracy of notes. Participants' responses remained anonymous to project team members not involved in data collection.
Interview and triad notes were transcribed in real time or from an audio recording and then manually coded. Code outputs were reviewed for additional analysis, summary, and interpretation using a grounded theory approach. Developed by Glaser and Strauss, grounded theory is a method for developing themes, based on qualitative data, utilizing a bottom-up perspective (Corbin & Strauss, 2008; Glaser, 1967). In this application, we applied grounded theory methods to develop the set of concepts, categories, and their interrelationships, which are summarized below.
Results
Many themes emerged during the interviews and triads. The experts describe a shift in thinking across domains, with growing recognition that the built environment is an important factor in the transmission of HAIs. This is supported by an increased number of facility design and infection control guidelines. There is little evidence, however, linking design strategies and technologies to a reduction in infection rates, causing the experts to question the accuracy of the term “evidence-based design.” Ultimately, participants rely on a combination of available literature and experience to guide decisions for strategies and technologies to mitigate the risk of infection.
Perceived Role of the Built Environment in the Acquisition and Prevention of HAIs
The participants acknowledged that the built environment plays a role in the transmission and acquisition of HAIs, though the extent of its role remains unclear. Of the three mechanisms for transmission of infection (contact, air, and water), there was consensus among the participants that contact is the primary mode of transmission, estimated to cause 80%–90% of HAIs, followed by air (5%–10%) and water (5%–10%). These estimations are based on the experience of the participants and may not be substantiated by research. The current state of evidence on the transmission of HAIs is reported in subsequent reports available in this special supplement to HERD (Denham et al., 2013; Jacob et al., 2013; Steinberg et al., 2013; Zimring, Jacob, et al., 2013).
Participants characterized the shift in thinking about the relationship between the built environment and transmission of HAIs as a “progression.” Over time, as the discussion of this relationship has expanded and involved broader circles of professionals—including healthcare administrators and experts in hospital epidemiology and infection control, air quality, water quality, architecture, and interior design—valuable new research, insights, and strategies have emerged.
Many participants identified the increasing complexity of patient rooms over time as a catalyst for greater attention to the relationship between HAIs and the built environment. The addition of couches and recliners to accommodate family members, stationary computers, and shelving increases the surface cleaning requirements for room turnover and also provides greater opportunities for contact transmission of HAIs. One participant, an infection preventionist, said, “Thinking back to 1975 when all we had was an overhead table, bedside table, and an IV pole, it was easy to turn over a room. Now, we have a hugely complex environment with frequent patient-to-surface contact—adequate cleaning on a daily basis is becoming insurmountable.”
Thinking back to 1975 when all we had was an overhead table, bedside table, and an IV pole, it was easy to turn over a room. Now, we have a hugely complex environment with frequent patient-to-surface contact—adequate cleaning on a daily basis is becoming insurmountable.
Other reported contributors to an increased awareness of the role of the built environment in the acquisition and prevention of HAIs include tuberculosis outbreaks, HIV in the late 1980s and, more recently, the Severe Acute Respiratory Syndrome (SARS) epidemic. Research conducted in the late 1980s, examining the impact of construction on indoor air quality, resulted in the development of a list of precautions that should be taken during hospital construction and renovation in order to control exposure to debris. Regulatory agencies, such as the American Society of Heating, Refrigerating and Air Conditioning Engineers (ASHRAE) and the Centers for Disease Control and Prevention (CDC), established safety and infection control guidelines, which reflected the increased awareness that the environment should be optimized to mitigate infection risk. The experts reported that with this awareness came growing public concern, with increased reports of outbreaks of multidrug-resistant organisms, such as methicillin-resistant Staphylococcus aureus (MRSA), in hospitals. Experts noted that research in recent years has also found that organisms such as MRSA, vancomycin-resistant Enterococcus (VRE), Legionella, pseudomonas, acinetobacter, and norovirus are strongly linked with the environment. See Zimring, Jacob, et al. (2013) for more information on pathogens and their environmental niche.
Guidance for Facility Design
Roughly half the experts indicated that their clients request strategic guidance and data in selecting an approach for HAI prevention. The other half reported having clients who are generally aware of current research findings on HAI prevention and request assistance with fine-tuning their HAI prevention approach, guidance on meeting code requirements, or confirmation that their potential selections are worthwhile investments. Despite the requests for guidance on HAI and design, many experts stated that organizational leaders do not blindly take the advice of the experts and are increasingly requesting data to support expert recommendations, including post-occupancy study data and data demonstrating a reduction in infection rates. Organizational leaders recognize the importance of design decisions and aim to make informed decisions based on available data.
Participants identified a number of resources that inform their design recommendations, including clinical consulting groups, academic institutions with healthcare design/architecture programs, peer-reviewed journals, and industry standards and guidelines. Standards and guidelines are issued by ASHRAE, Leadership in Energy and Environmental Design (LEED); CDC, National Institutes of Health (NIH), U.S. Environmental Protection Agency (EPA), Facility Guidelines Institute (FGI), Association for Professionals in Infection Control and Epidemiology (APIC), and American Society for Plumbing Engineers (ASPE).
Participants indicated that more data supporting specific interventions' abilities to reduce infection would be helpful in informing construction decisions. Very little research linking a particular strategy or design to infection outcomes and cost savings currently exists, however. Consequently, decision makers must rely on a combination of experience, evidence, and potential payoffs of a particular technology (e.g., cost savings from delayed replacement of equipment and cleaning agents). In the absence of cost and efficacy data, the design decision-making process still resembles a trial and error process.
There is a massive gap between people responsible for construction and design of healthcare facilities and people who maintain them. The greatest designs can be immediately undone by poor maintenance.
Perceived disconnects among the design team, construction team, facilities team, and frontline staff are thought to be part of the reason for this trial and error approach. Interventions may have a higher likelihood of success when there is open dialogue and each party understands the needs and restrictions of multiple stakeholders. Careful analysis from multiple perspectives can avoid costly mistakes from both patient safety and financial standpoints. When assessing new equipment or a decorative feature, part of the analysis should include identification of requirements for proper maintenance (e.g., cleaning regimen, filter replacement) and the persons responsible for maintenance. As an architect who participated said, “There is a massive gap between people responsible for construction and design of healthcare facilities and people who maintain them. The greatest designs can be immediately undone by poor maintenance.”
Evidence-Based Design
The lack of data demonstrating a reduction in infection rates as an outcome for a design strategy prompted a discussion of the definition and parameters of evidence-based design (EBD) among the participants. Evidence-based medicine (EBM) has been defined as “the integration of best research evidence with clinical expertise and patient values” (Sackett, Strauss, Richardson, Rosenberg, & Haynes, 2000). For many, EBD represents a similar high standard. As a result, participants expressed concern that some define and use the term rather loosely, especially in recent years when many viewed EBD as a buzzword in healthcare design. As one administrator participant commented, “If we get hung-up on the gold standard of research, we do ourselves a disservice. There are people in the field with a lot of experience and history which may not be the gold standard, but it's pretty good. We need to be open-minded about what we need to do in the interim.”
If we get hung-up on the gold standard of research, we do ourselves a disservice. There are people in the field with a lot of experience and history which may not be the gold standard, but it's pretty good. We need to be open-minded about what we need to do in the interim.
Given the dearth of rigorous outcome based evidence to support EBD, some prefer the terms “evidence-informed” or “evidence-influenced” design and use the limited evidence that is available to inform decisions in areas that have yet to undergo extensive assessment. In some cases, even if data are not available, many participants find that explaining their rationale in practical terms can be an effective approach to adoption of a proposed intervention. Participants reported commonly applying the precautionary principle to implement interventions that appear to have a promising net benefit, in the absence of data proving that an intervention will cause harm. Some facilities use a phased approach and implement interventions in one area to test them on a limited basis, assessing their experience before proceeding with implementation on a larger scale. One participant who was a mechanical engineer remarked that, “We base all of our design on our experience. We've done this 29 times and we know it works and we did it another way and it didn't work, so evidence is showing us this is the way to do it.”
Despite awareness of EBD, not everyone is a proponent. Opponents noted that in the context of the design decision-making process, hospitals must proceed with their timelines and cannot delay decision making in order to wait for evidence to emerge supporting each decision. Moreover, they noted that there is insufficient funding allocated for this type of research. The arguments against EBD cited most often by participants were the lack of evidence and the diminished value placed on first-hand experience in the assessment of the effectiveness of interventions.
Overall, the participants advocated using a mix of guidelines and peer-reviewed literature to inform design decision making, since both provide useful insights. Although many experts acknowledged the value of the rigor of peer-reviewed literature, they also emphasized the importance of expert judgment and experience when identifying practices and strategies that are deemed effective for HAI prevention.
[When we don't have research evidence], we base all of our design on our experience. We've done this 29 times and we know it works and we did it another way and it didn't work, so evidence is showing us this is the way to do it.
Strategies with Greatest Impact on Reducing HAI Risk
Contact was cited as the most common mechanism for the transmission of HAIs. The key strategies noted by experts for minimizing the transmission of HAIs through contact included promoting hand hygiene compliance, establishing and monitoring routine cleaning of high-touch surfaces, and improving terminal room cleaning. Increased use of technologies in the patient room, such as touch-screens and stationary computers, create a greater need for determining methods for routinely disinfecting devices without damaging them. The participants also emphasized the importance of selecting non-porous hard surfaces, which are less likely to promote microbial contamination and are easier to clean, during design or renovation phases, and abandoning the use of pressboard in cabinetry, under-sink storage areas, and plastic laminate around sinks.
Cleaning and disinfecting products are gaining greater attention as hospitals look to consolidate cleaning agents and search for products that can effectively clean and disinfect multiple surfaces. Several experts mentioned a movement towards “green” disinfection products and cited the EPA and LEED as resources for analysis of low-emitting materials and disinfection products. As chemical content analysis research is conducted on various products, experts call for cooperation and partnership among all parties to prioritize an assessment of environmental impact of during the facility design and construction process, as well as during the cleaning process. Manufacturers are urged to become more actively involved in these efforts by sharing data, test results, and descriptions of the chemical content of their products. Such information is needed to identify disinfectants that are effective in reducing HAI risk while also less corrosive and harmful to the environment than some current widely used disinfectants.
Strategies mentioned for mitigating the spread of airborne pathogens included high quality filters, air exchange rates, and room pressurization. Dividing mechanical systems into zones was discussed as a strategy to allow more flexibility for adapting rooms to patients with different levels of illness. It also can reduce the risk of infection by preventing contaminated air from being recirculated into areas with immunocompromised patients. Participants also noted proper filtration and re-circulation as key strategies for ensuring both air and water quality and safety.
More than half of the participants interviewed indicated that single-patient rooms have had the greatest impact on reducing HAI risk in the hospital setting. However, most participants agreed that no single strategy is entirely effective in leading to HAI reduction; instead it has been a combination of strategies that has played a role in reducing HAIs. One participant indicated that raised awareness of HAIs alone has contributed significantly to their reduction, because it has resulted in action at all levels.
Participants agreed that in spite of new technologies and design strategies that may emerge in the future targeting the prevention of HAIs, the most prominent determinants of HAI prevention pertain to human factors and human behavior. They acknowledge that human factors, especially poor hand hygiene compliance, can undermine even the best design.
Infection Control Technologies
The three technologies most frequently mentioned for infection prevention include high-efficiency particulate air (HEPA) filters, ultraviolet germicidal irradiation (UVGI), and hydrogen peroxide vapor (HPV). The efficacy of HEPA filters for the reduction of airborne pathogens is strongly supported through research. The necessity for their widespread use is still debated, however, because they represent a substantial investment due to increased energy consumption, maintenance costs, and expensive filters that need frequent replacement. The discussion of HEPA filters and their energy consumption is clearly an important consideration for hospital executives designing future facilities. These costs must be weighed against the benefit of the HEPA filtration technology versus other air filtration methods.
Participants noted that UVGI has received increased interest in the peer-reviewed literature, but added that it is not 100% effective against all pathogens (e.g., Clostridium difficile) and requires direct surface exposure in the linear path of UV light for a specified period of time. HPV is also under investigation for its ability as a “touchless” supplemental environmental disinfection strategy (emitted by a sprayer) to disinfect air and surfaces, and it is not limited by line of sight as is UVGI. An advantage of HPV over traditional cleaning strategies is that its only residue is water, which is less toxic and damaging to surfaces than other disinfectants. Both technologies require vacating the room while in use, which increases the length of time needed for room turnover, a characteristic that some experts feel hinders operational efficiency. Participants stated that although UVGI and HPV are effective in killing organisms, operational considerations in terms of requirements for consistent and effective use limit the practicality of these technologies.
The lack of research evidence demonstrating the abilities of HEPA filters, UVGI, and HPV to reduce infection rates contributes to the varying opinions on both technologies, often leaving discussion of cost as the primary determining factor for implementation. For further reading on the current state of evidence on these technologies, see Jacob et al. (2013) and Steinberg et al. (2013).
Emerging Strategies and Technologies
Participants mentioned a number of interventions that are currently in limited use that may be promising in the near future. Copper plumbing and copper impregnated materials have been shown to be antimicrobial in comparison to PVC and other materials. Participants noted that copper handrails and door rails were considered by the 2014 Healthcare Guidelines Revisions Committee (the group charged with developing and maintaining the Guidelines for the Design and Construction of Healthcare Facilities) as an emerging topic warranting additional assessment. Data exists supporting the antimicrobial properties of copper surfaces, but evidence demonstrating copper's ability to prevent and reduce infection risks in patients is lacking. For further reading on the applications of copper on surfaces, see Steinberg et al. (2013) and for water decontamination, see Denham et al. (2013) also appearing in this special supplement to HERD.
Participants expressed increased interest in flooring materials. Given the 24/7 hospital operating schedule, flooring is a very difficult area in which to maintain cleanliness. For example, the floors of emergency departments are very challenging to keep clean and are areas where infection risk can be quite high given the traffic flow and nature of the patients entering and exiting. This has encouraged experts to seek out flooring alternatives with lower microbial buildup, such as seamless flooring (i.e., no cracks present at the wall/floor seam).
A greater focus on sustainability issues and reduction of energy use are driving many to look more closely at using alternative air flow strategies such as chilled beams. Chilled beams use chilled water pipes in modular units that are ceiling-mounted and primarily transfer heat through convection rather than radiation (Roth, Dieckmann, Zogg, & Brodrick, 2007). The participants noted greater discussion and debate regarding how to enhance infection reduction while using technologies such as chilled beams to reduce energy consumption, and how such features affect the building codes that are currently in place. ASHRAE Standard 170 currently permits chilled beams, but there is concern about excess condensation and the potential for growth of organisms (i.e., mold) if the systems are not properly maintained.
Resistance to Implementation of Technologies Aimed at Infection Prevention
Healthcare organizations are suffering from decreasing reimbursement rates with increasing operating costs. Changes in reimbursements for preventable events, such as HAIs, have often led decision makers to opt for the safer route, rather than the most innovative; stakeholders are often hesitant to embrace innovative strategies with little evidence demonstrating reductions in HAI rates. Hospital administrators are reported to be gathering more data to make informed decisions in order to promote more judicious use of funds. Participants shared concern from healthcare organizations that often have little cash on hand, making interventions requiring significant up-front investments and ongoing maintenance costs challenging. Many do what is necessary to meet code requirements and guidelines, but they do not go beyond the minimum requirements.
Participants agreed that interventions that have support from the top down, primarily from hospital executives, receive less push-back from clinical and facilities staff and are most easily implemented. On the other hand, high-level executives are also often recognized as deterrents to innovative design approaches. Several experts considered infection control and frontline staff as key proponents of innovative design features with promising potential to reduce HAIs. Participants stated that, given their responsibility for maintaining interventions that may have an impact on HAI prevention, hospital facilities departments largely affect the degree to which interventions are implemented and the likelihood of successful implementation in the long run. Experts agreed that how an intervention is presented and, in particular, the way in which the payback and benefits are described have a lot of influence on staff buy-in of innovative strategies.
Conclusions
As new research emerges over time, more is revealed about the role that the built environment and human factors play in transmitting organisms that result in HAIs. Some participants characterize the prevention of HAI transmission as a moving target because research is still largely inconclusive on how to effectively manage and prevent transmission of pathogens and aggregations of microorganisms. Optimizing the built environment to minimize the risk of infection can become even more challenging when attempting to build healing environments focused on patient- and family-centered care, which calls for a more aesthetically pleasing, homelike environment. Many experts have found that design considerations are often chosen over infection control, emphasizing the need for continued education for patients and families in addition to healthcare workers.
The multidisciplinary team of experts who participated in these interviews and triads rely on a combination of research and experience. Most are reticent to term this approach “evidence-based” when compared with the level of evidence required in the practice of evidence-based medicine, characterized by randomized control trials, scientific rigor, and peer-reviewed publications. In order to develop a common definition and advance the field of “Evidence-Based Design” for mitigating the risk of HAIs, a methodology for evaluating the quality of evidence still needs to be established. This can only be accomplished with multidisciplinary collaboration involving a broad group of health professionals and design experts in the healthcare facility design planning and decision-making process. Collaboration that is based on a foundation of mutual understanding and open dialogue should lead to improved integration of evidence and experience in efforts to reduce design-related healthcare infections.
Forward-thinking teams are eliminating the previously siloed construction, design, and infection prevention considerations. They are beginning to evolve a more integrated and holistic approach. Healthcare decision makers recognize that until conclusive evidence emerges for interventions aimed at reducing and preventing HAI transmission, they must make best use of the resources available to inform their design decisions—a combination of research data and practical experience.
Implications for Practice
Multiple interventions, including those that focus on the built environment and those that focus on human behavior, are necessary to mitigate healthcare-associated infection risk, as no single intervention is entirely effective.
Experts suggest that, given the limited availability of data linking design to patient outcomes, decision makers should utilize a combination of guidelines, peer-reviewed literature, expert judgment, and experience to inform design decisions.
Thorough analysis from multiple perspectives can avoid costly mistakes from both patient safety and financial standpoints. This calls for greater multidisciplinary dialogue and collaboration to improve the application of both evidence and experience in facility design.
Footnotes
ACKNOWLEDGMENTS
We thank Emily Richmond, Altug Kasali, Amy Allison and all experts for their careful and thoughtful participation in the Healthcare-Associated Infection–Design (HAI-Design) project. Financial Support: This HAI-Design project was funded under contract HHSA290201000024I (ACTION II) to RTI International in collaboration with Emory University and the Georgia Institute of Technology from the Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services. The opinions expressed in this article are those of the authors and do not reflect the official position of the Agency for Healthcare Research and Quality or the U.S. Department of Health and Human Services.