
Abstract
The purpose of this study was to collect the perceptions of design professionals and clinicians regarding design process success strategies and elements of interprofessional engagement and communication during healthcare design and construction projects. Additional objectives were to gather best practices to maximize clinician engagement and provide tools and techniques to improve interdisciplinary collaboration for future projects. Strategies are needed to enhance the design and construction process and create interactions that benefit not only the project but the individuals working to see its completion. Meaningful interprofessional collaboration is essential to any healthcare design project and making sure the various players communicate is a critical element. This was a qualitative study conducted via an online survey. Respondents included architects, construction managers, interior designers, and healthcare personnel who had recently been involved in a building renovation or new construction project for a healthcare facility. Responses to open-ended questions were analyzed for themes, and descriptive statistics were used to provide insight into participant demographics. Information on the impressions, perceptions, and opportunities related to clinician involvement in design projects was collected from nurses, architects, interior designers, and construction managers. Qualitative analysis revealed themes of clinician input, organizational dynamics, and a variety of communication strategies to be the most frequently mentioned elements of successful interprofessional collaboration. This study validates the need to include clinician input in the design process, to consider the importance of organizational dynamics on design team functioning, and to incorporate effective communication strategies during design and construction projects.
Keywords
The dynamics of the healthcare environment are impacted by technology, service line, financial, and regulatory changes, which often lead to expansion, renovation, or design of new facilities. These design and construction projects require the collaboration of representatives from significantly different backgrounds to produce optimal results (Suter et al., 2009). While interprofessional collaboration during the design process produces optimal results, nurses often leave design meetings frustrated from misunderstandings, architects and interior designers leave wondering why there are so many design changes, and the construction team must make adjustments during completion of the project. Interprofessional collaboration strategies are needed to mitigate frustrations, decrease potential delays due to change orders, keep project costs down, and create interactions that benefit not only the project but also individuals. Such strategies will support the meaningful interprofessional communication and collaboration essential to the success of any healthcare design project (Clark, 2014; Reno et al., 2014).
Significance/Aim/Purpose
Interprofessional teamwork can improve the quality of a healthcare design project when time and effort is dedicated to ensure all team members can easily understand and collaborate with one another (Quan et al., 2014). The purpose of this study was 2-fold. The first was to collect the perceptions of design and construction professionals and clinicians regarding successful elements of engagement and communication during design and construction projects in the healthcare environment. The second was to gather insight into strategies recent design project participants perceived as contributing to effective interprofessional collaboration and communication. Additional objectives were to gather best practices to maximize clinician engagement and provide tools and techniques to improve and promote interdisciplinary collaboration in future projects.
Review of the Literature
The physical space of a healthcare facility can have an impact on healthcare providers, patients, and their significant others. When the clinical perspective is not effectively integrated into a design project, clinicians may create work-arounds. A work-around is a method of accomplishing an activity when the usual system/process is not working well (Rouse, 2005). For example, supply rooms or cabinets may be designed in a size that is unsuitable for supply storage. As a result, clinicians will place the supplies in an alternate space or location but may increase the likelihood of ergonomic injury due to unnecessary bending or reaching or possibly increase walking distances. Including clinicians in healthcare design projects can significantly mitigate potentially dangerous work-arounds (Rodriguez, Ford, & Adams, 2011).
One of the main barriers to successfully engaging and drawing upon the expertise of clinicians in the design process is the lack of mutual language or shared context (Suter et al., 2009). While some authors have suggested interprofessional competencies to promote interdisciplinary collaboration, this may not be feasible when real-time decisions need to be made to keep a project on track (Lamb, Zimring, Chuzi, & Dutcher, 2010; Stichler, 2014). This study seeks to identify strategies to promote interdisciplinary collaboration and communication while still adhering to the design schedule.
Method
Design
Data for this study were collected using Qualtrics©, a web-based survey platform. After receiving an invitation e-mail, participants read the online consent form and voluntarily chose whether or not to participate. The e-mail contained a brief introduction and a link to the online survey. This was a one-time survey, and no identifying information was required for participation. If a participant was willing to be contacted to provide additional information, they had the option of providing their e-mail address. Responses from open-ended survey questions were used to elicit an understanding of the perceptions of various professionals involved in healthcare design projects. Descriptive demographic information was also collected. The study protocol was approved by the institutional review board of the principle investigator’s (PI) academic institution.
Sample
E-mails were sent to colleagues of the PIs who work in the healthcare design industry. Potential participants included architects, construction managers, interior designers, and healthcare personnel who have recently been involved in a building renovation or new construction project for a healthcare facility. Snowball sampling was used in that initial study participants were asked to share the survey e-mail to colleagues within their professional network. Respondents included clinicians (8%), facility administrators (18%), architects (45%), construction managers (9%), and a mix of other industry professionals (20%). The largest group of respondents were architects, and the majority were between the ages of 45 and 65 and had significant experience with 20% having between 5 and 9 years of tenure in the industry and 75% having over 10 years. Eighty percent of participants reported an inpatient facility project as their most recent.
Data Analysis
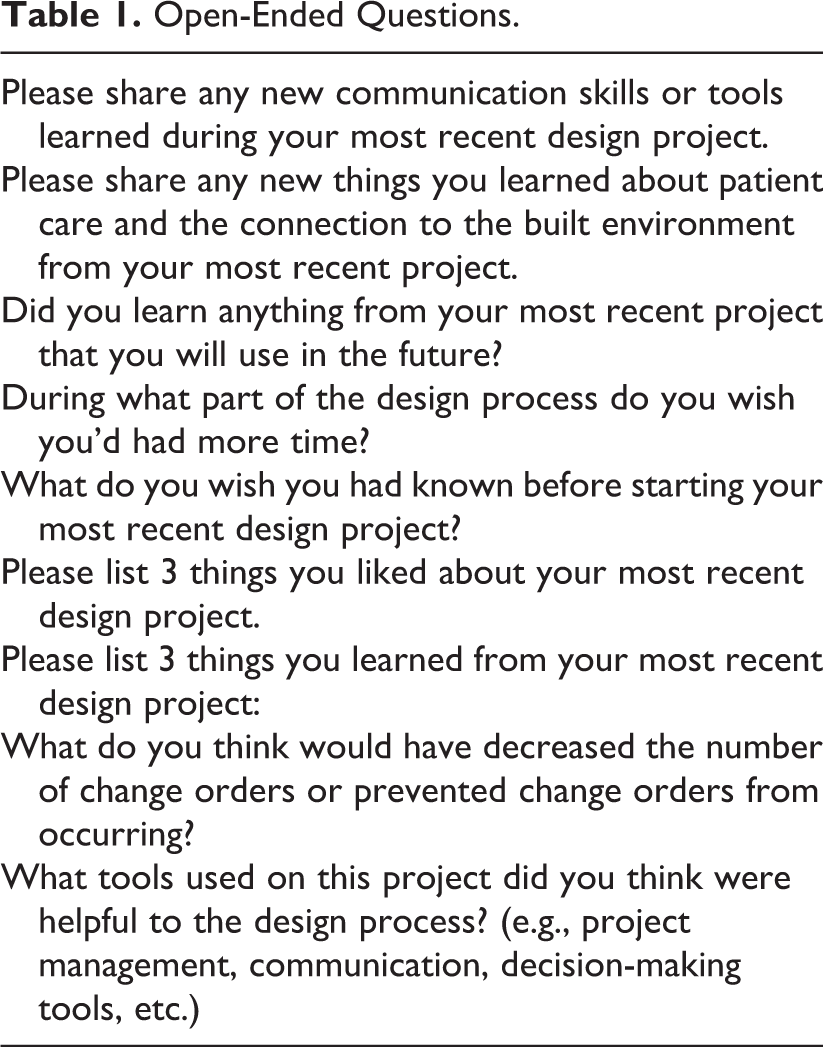
Descriptive statistics were used to analyze the demographic information, but because of the high percentage of architects, limited information was obtained. The bulk of the data was culled from content analysis of the open-ended questions (Table 1). All participant descriptions were horizontalized, so no hierarchy whereby one reality may be more valued than another (Ihde, 1977). NVivo Qualitative software (Version 8) was used to first code the open-ended text responses and then to examine essential features, structures, relationships, or invariants among the accounts. Resultant themes from the coding process were vetted by two professionals in the healthcare industry. Finally, the results of the analysis were presented at a national conference for discussion of issues and refinement of tools and techniques to promote effective interdisciplinary collaboration (Table 2).
Open-Ended Questions.
Common Roadblocks Experienced by Participants and Suggested Solutions From Industry Professionals.
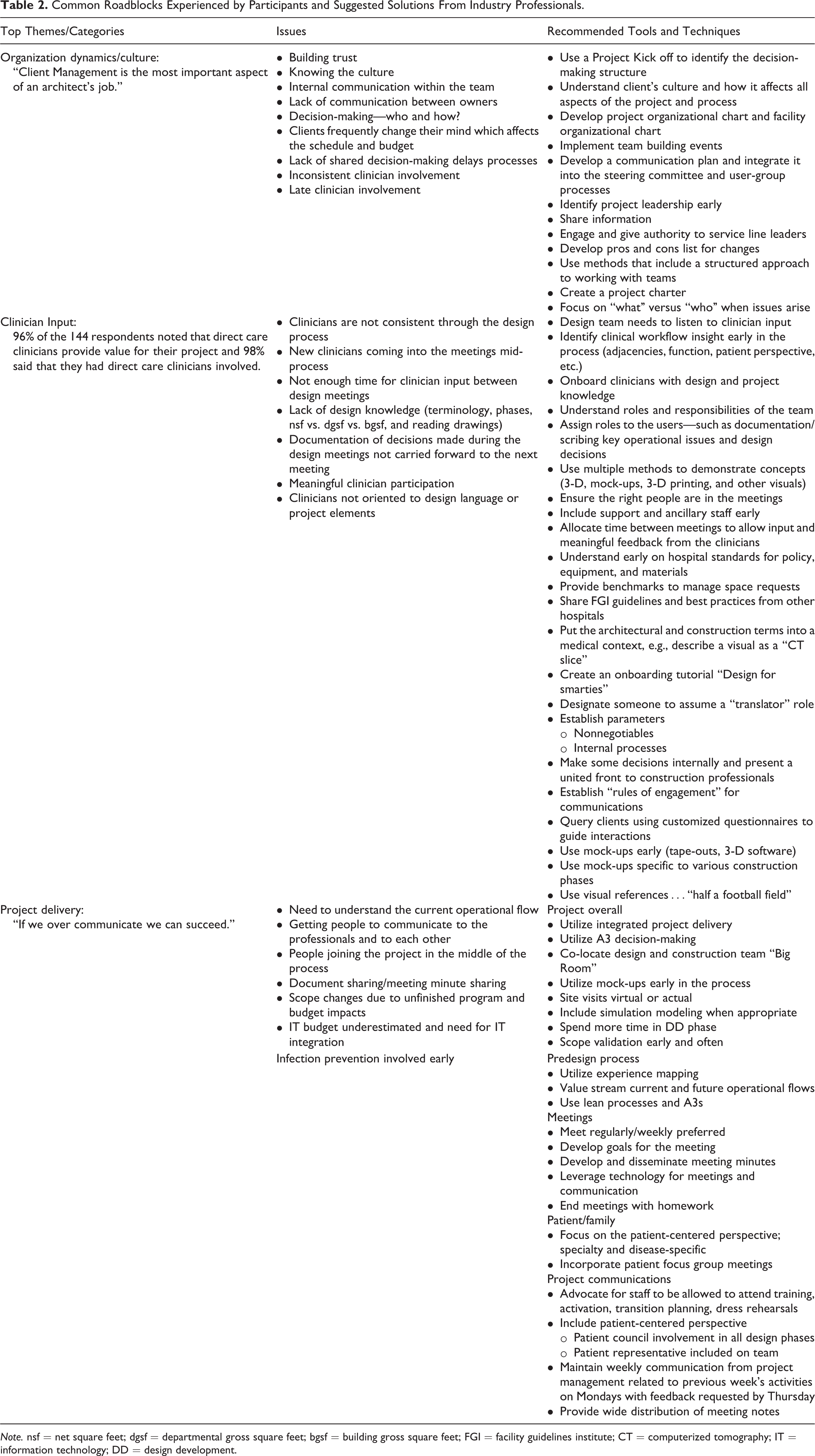
Note. nsf = net square feet; dgsf = departmental gross square feet; bgsf = building gross square feet; FGI = facility guidelines institute; CT = computerized tomography; IT = information technology; DD = design development.
Findings
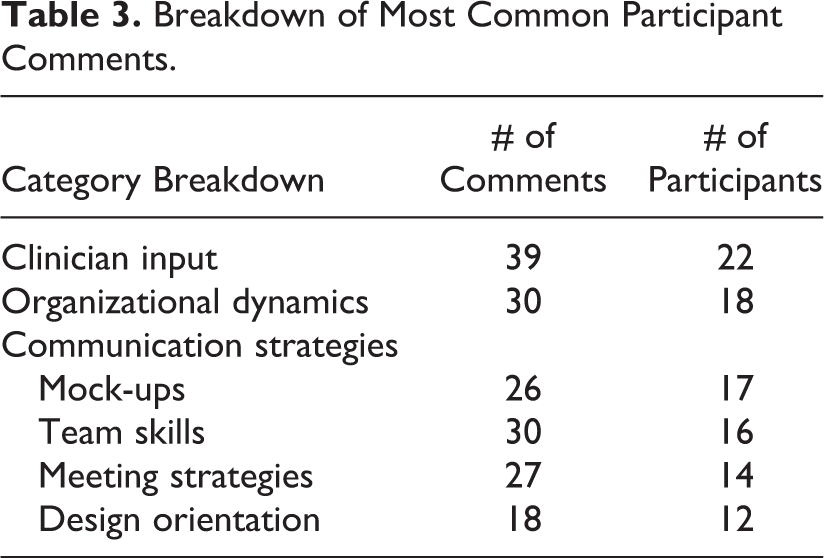
Qualitative analysis revealed themes of clinician input, organizational dynamics, and a variety of communication strategies to be the most frequently mentioned elements of successful interprofessional collaboration (Table 3).
Breakdown of Most Common Participant Comments.
Clinician Input
Clinician input was by far the most commented on element of successful design collaboration. Of all design industry professionals participating, 98% valued the input of direct care clinicians and had direct care clinicians involved in their projects.
The majority of architects responding emphasized the importance of clinician input and several noted they would have liked more time for this type of exchange. Several also noted they would have liked to have had clinician input earlier in the design process.
The hospital/nursing administrators responding to this survey were supportive of including the clinician’s perspective in healthcare design projects in order to maximize the benefits to the project and the clinicians. One hospital administrator noted clinicians need to be more assertive when they are asking for something and focus on the reason for the request regardless of the cost. Another noted the importance of clinical input by stating “architects do not understand what it takes to keep patients and staff safe.”
Throughout the design process, there are cost estimates done on the building project. If it is determined the design and project costs are over budget, it is necessary to determine which elements of the design need to be modified or deleted to decrease the cost. These changes are referred to as value engineering. One hospital/nursing administrator noted that while clinical input was incorporated at the beginning of their project, more engagement of clinicians should have occurred in value engineering decisions.
Finally, design and construction professionals indicated they wish they had understood the importance of the clinician experience, as it related to the end product and had learned to take the thoughts of stakeholders and use them in their respective design processes earlier in the project. One construction/project manager noted participation from stakeholders will always save money by reducing change orders.
Organizational Dynamics
The second major theme identified had to do with the organizational dynamics influencing collaboration during healthcare design projects. Architects mentioned it was important for them to understand the client organizational culture, hierarchy, and relationships between departments. One participant described the need to manage implications the design would have on staffing logistics when working with two related departments. Another architect described a situation where “the leadership appears to work in a group and closely with each other, but actually do not inform each other about decisions and often overrule other’s decisions.” In contrast to these examples, architects liked projects where there was good interdisciplinary participation and the team worked well together to achieve the goals and ideals of the hospital.
Clinicians felt it was important the administrators of the organization be supportive of clinician involvement and input. Without this support, clinicians may be included too late to have a meaningful impact. One specific comment by a clinician emphasized the importance of including a “communication link” early in the process. This would be a designated individual who would work with both the project professionals and the clinicians to translate the specific language used by the various disciplines. This role was described as critical to keep all parties oriented to project progress and to assist in making informed decisions.
Hospital/nurse administrators expressed frustrations when decisions were not communicated with transparency or when decisions that had been made at a corporate level were not up for negotiation or input from the team. Other administrators noted the importance of role clarification especially related to decision-making. Hospital/nurse administrators also noted meetings did not have the desired benefit if the right people were not at the table.
Interior design professionals mentioned the importance of organizational dynamics when they described the impact of team member changes during the project. They noted that when members of the client team changed during the project, the design might also need to be changed to reflect new opinions or agendas. Projects seemed to run more smoothly when administrators created an organizational dynamic in which clinicians were supported to (a) be part of the team, (b) be consistent throughout the project, and (c) be allowed scheduling flexibility to attend design meetings.
Communication Strategies
Communication strategies are related to organizational dynamics but specifically address the exchange between design professionals and clinicians. Four areas frequently mentioned include mock-ups, team skills, meeting strategies, and design orientation.
Mock-ups
Mock-ups are used by design professionals to create visuals for stakeholders to use in considering the impact of the proposed design. Architects considered mock-ups to be a critical communication tool. Some mentioned full-sized mock-ups that allowed users (clinicians) to better understand the space, while others used software that enabled scenario testing. Several architects noted better mock-ups, earlier in the process, would have been beneficial to their projects. One architect noted, “actually standing in the space offers much more value than looking at a drawing or a simulation.” An architect and clinician both noted the benefits of repeated refinement and testing of a full-sized mock-up. Another clinician who had worked on a pediatric project mentioned the benefits of including parents during mock-up walk-throughs.
Construction and project managers noted the benefits of creating even simple mock-ups, including columns or placing tape on the floor to help clinicians understand how equipment would fit into the space. Several found this process not only beneficial but enjoyable when clinicians were included and collaborated with the team.
Hospital and nurse administrators noted value was achieved from investment in full-sized mock-ups. One hospital administrator noted, “Mocking up one room and having staff actually see the real design before they did all of the rooms was critical as the vision of the designers and the vision of what staff asked for were not always the same.”
Team skills
One architect noted, “client management is the most important aspect of an architect’s job” and it was evident in the team skills that were emphasized by various participants. Collaboration was a key word in architect comments. When members of the design team worked well together and were committed to success of the projects, the projects ran more smoothly. One architect emphasized the need to get to know team members and understand underlying issues related to strong opinions that team members may express.
Construction and project management professionals’ comments were consistent with those of architects. They also described the benefits of building trust and collaboration among team members and one noted the need to “push people to communicate with one another.”
Hospital/nursing management also described working in a collaborative manner with team members to be one of the things they enjoyed most about their most recent healthcare design project. While they also emphasized the importance of communication and role definition within the team, they felt strong interdisciplinary collaboration enhanced the end product. One hospital/nursing administrator felt prepared for the collaborative approach because of previous experiences working with shared governance groups.
An interior designer also emphasized the importance of celebration to team cohesiveness. This participant wrote, “remember to celebrate the process and help the users realize the excitement of the outcome.”
Meeting strategies
Design meetings are a part of every project and participants described several strategies that contributed to productive exchanges with team members. Architects and design professionals noted the importance of keeping accurate meeting notes to not only remind participants of decisions that had been made but also share progress with other stakeholders not intimately involved with the project. Another strategy shared by respondents was to have clear goals and an agenda for the meeting to promote focused discussion. Interior designers shared two strategies they found helpful to promote productive meetings: (1) recognize when clinicians should work out an operational issue during a design meeting or whether it should be tabled for the hospital to solve off-line. It is hard to accomplish everything required during design meetings because important but time-consuming policy conversations tend to arise. (2) Give meeting participants a deliverable/homework to accomplish for the next meeting. Several architects as well as hospital administrators noted while not novel, weekly work sessions and disseminating resulting updates were important to keep stakeholders engaged and informed.
Design orientation
The fourth communication element was design orientation and the importance for all stakeholders to have a shared understanding. There were many clinicians and hospital/nursing administrator comments related to the learning curve they experienced when working on their most recent design project. Several emphasized the importance of understanding the language used and the impact of their decisions. One clinician in particular would have liked to have had a better understanding of what they agreed to and the complexity of the change request process. Hospital/nursing administrators noted they had limited or no experience with the phases of design, design principles, or how to read a floor plan. From the design industry professional’s perspective, the benefits of investing the time to provide stakeholders with a good design orientation are reliant on consistent design team membership and regular participation.
Discussion
This study reinforced the notion of interprofessional collaboration and emphasized the importance of not only a competent collaborator but one who has worked in the clinical environment and has a keen understanding of how work is accomplished in the healthcare space (Clark, 2014; Rodriguez, Ford, & Adams, 2011). The importance of choosing the right members for a design project cannot be overemphasized (Stichler, 2011, 2014).
Our study noted the importance of organizational dynamics to interprofessional collaboration. Teamwork is jeopardized when there is frequent turnover on the design team or when the organizational culture does not foster clinician participation. The best laid design plans can go awry if organizational structures are not in place to support those plans. To mitigate negative outcomes, when issues arise, it is important for members of the design team to take good meeting notes and put decisions in writing in case a new set of players require orientation to the project (Reno et al., 2014).
Communication strategies recommended from participants were consistent with others in that using mocked up spaces can be beneficial to get clinicians and industry professionals to have a shared understanding (Clark, 2014; Reno et al., 2014; Stichler & Okland, 2015). Because clinicians are accustomed to working with other disciplines on behalf of their patients, they have the potential to work well on design teams; however, they may be unfamiliar with meeting strategies, the design process, terminology, reading, and understanding drawings and techniques that are second nature to industry professionals. Creating a nurse champion to orient new clinicians to the design team is just one of the several strategies that can be used to bring clinicians up to speed and provide them with a shared, design orientation (Clark, 2014; Reno et al., 2014; Stichler & Okland, 2015).
Limitations
When considering the number of people who may be involved in healthcare design projects within the United States, garnering 144 responses is not a large number, but it is enough to provide some interesting insights. While the snowball sampling method is not likely to provide a representative sample, the method was used, as there are innumerable disciplines and specialties who contribute to healthcare design projects and there is not a master repository for such contributors (Trochim, 2001). Given that two of the PIs worked in architecture firms, it is not surprising that architects were the most represented specialty. This is also supported by the assumption that the architects invited to participate might have forwarded the survey link to other architect colleagues. Information from this study should be used with consideration of the sampling method since colleagues from similar projects or like design firms could be sharing similar experiences. Because data on the number and diversity of firms were not collected, it is impossible to mitigate the possibility of homogenous responses.
Conclusions
Information from this online survey will be useful to individuals involved in healthcare design projects. This study validates the need to have clinicians educated in the design process at the design table and the importance of interprofessional collaboration between design and construction professionals and healthcare personnel. It is hoped those who use the resulting information will enjoy more productive relationships when working on healthcare design projects.
Recommendations for Future Study
The study of clinician impact on healthcare design projects is in its early stages. There are many opportunities for future study including the difference in perceptions of various disciplines involved on a design project, different methods of preparing design team members to work together, and exploring to what degree financial metrics are impacted when clinicians are consistently included on design teams and when design teams work together well. Another important area relates to patient and staff safety. It would be interesting to determine whether patient and staff safety metrics are improved when (a) clinicians are included on design teams and (b) design teams work together well. Finally, a future inquiry into the impact of patient and visitor feedback during the design process is also recommended. The combinations are innumerable, and it is important to continue to build the science of healthcare design to promote best practices for future initiatives.
Implications for Practice
Provides validation to the Chief Nursing Officer (CNO) and healthcare administrators the importance of including clinicians on design projects.
Encourages designers to enhance their meeting strategy to ensure clear communication and understanding in design meetings.
Defines the importance and value of mock-ups during the design process.
Identifies organizational project structures to enhance the design process and the design end result.
Supplemental Material
Supplemental Material, Identification_of_Tools_and_Techniques_to_Enhance_Interdisciplinary_Collaboration_During_Design_and_Construction_Projects - Identification of Tools and Techniques to Enhance Interdisciplinary Collaboration During Design and Construction Projects
Supplemental Material, Identification_of_Tools_and_Techniques_to_Enhance_Interdisciplinary_Collaboration_During_Design_and_Construction_Projects for Identification of Tools and Techniques to Enhance Interdisciplinary Collaboration During Design and Construction Projects by Yolanda Keys, Susan R. Silverman, Jennie Evans in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
Special thanks to the Texas A&M University-Corpus Christi CONHS Graduate Research Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Texas A&M University-Corpus Christi CONHS Graduate Research Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.