
Abstract
Objective:
The focus of this research was to analyze the impact of decentralized and centralized hospital design layouts on the delivery of efficient care and the resultant level of caregiver satisfaction.
Background:
An interdisciplinary team conducted a multiphased pre- and postoccupancy evaluation of a cardiovascular service line in an academic hospital that moved from a centralized to decentralized model. This study examined the impact of walkability, room usage, allocation of time, and visibility to better understand efficiency in the care environment.
Method:
A mixed-methods data collection approach was utilized, which included pedometer measurements of staff walking distances, room usage data, time studies in patient rooms and nurses’ stations, visibility counts, and staff questionnaires yielding qualitative and quantitative results.
Results:
Overall, the data comparing the centralized and decentralized models yielded mixed results. This study’s centralized design was rated significantly higher in its ability to support teamwork and efficient patient care with decreased staff walking distances. The decentralized unit design was found to positively influence proximity to patients in a larger design footprint and contribute to increased visits to and time spent in patient rooms.
Conclusion:
Among the factors contributing to caregiver efficiency and satisfaction are nursing station design, an integrated team approach, and the overall physical layout of the space on walkability, allocation of caregiver time, and visibility. However, unit design alone does not solely impact efficiency, suggesting that designers must consider the broader implications of a culture of care and processes.
As a result of evidence-based design, healthcare facilities are growing in size due to an increased emphasis on patient- and family-centered care, the inclusion of single-patient rooms, and improvements in technology, patient care standards, and operational models (Latimer, Gutknecht, & Hardesty, 2008). Between the years of 1980 and 2008, adult acute inpatient units grew by 118% and patient room size increased by 77%, an outcome described as “supersizing” (Latimer et al., 2008). An additional factor contributing to this growth includes the adoption of an interdisciplinary team approach with greater involvement of ancillary staff (i.e., social workers, dietitians, pharmacists, and therapists) in the delivery of care. These new care models require additional floor space, increased circulation, and more meeting spaces. At the same time, family involvement in patient care and the “rooming-in” concept, along with greater patient demand, have led to a larger patient room footprint including private toilets and showers, increased storage space, and sleeping accommodations for guests. Changes in the unit design have had a significant impact on staff and patient perceptions of the environment as well as efficiency of quality care (Hendrich et al., 2009; Hendrich, Chow, Skierczynski, & Lu, 2008; Zadeh, Shepley, & Waggener, 2012). The challenge now remains to weigh the implications of these changes on efficiency in the patient care process relative to satisfaction and design.
In addition to the physical growth of the healthcare environment, both medical technology and patient acuity levels have increased the amount of multitasking required of nurses as well as their cognitive workload. According to Zadeh, Shepley, and Waggener (2012), Nurses must move frequently among spaces and services and spend less time than desirable at patient bedsides to provide care, and the existing design infrastructure should keep up with this change and move toward efficiency objectives targeted by healthcare organizations. (p. 62)
Factors Impacting Efficiency and Satisfaction Levels
Efficiency and quality of patient care are influenced by two interrelated elements—nurse work processes and the physical hospital environment (Hendrich et al., 2008). The authors suggest that “a holistic approach is needed whereby people, process, and technology come together harmoniously in a physical space to produce the maximum…unit efficiency” (p. 33). Among the factors contributing to caregiver efficiency and satisfaction are nursing station design and location and the impact of the overall physical layout of the space on walkability, allocation of caregiver time, and visibility.
Nursing station design
To address efficiency and improved patient care, one response to the increased physical size of the care environment has been a move from centralized to decentralized nursing stations or some variation thereof. Zborowsky, Bunker-Hellmich, Morelli, and O’Neill (2010) refer to the nursing station as “the heart and soul of nursing care activities in a hospital” (p. 21). Among the factors to consider in the selection of various nursing station design models are ease of patient supervision, walking distances, access to supplies, and collaboration among caregivers. For many years, the centralized nursing station was the primary model utilized in healthcare facilities. Trzpuc and Martin (2010) define a centralized design as having “one main nursing station that is central to the patient rooms in that area” (p. 38). Research suggests that the positive aspects of centralized nursing stations include the provision for collaboration, social interactions, enhanced teaching and learning activities, and a clear demarcation between public and private spaces (Zborowsky, Bunker-Hellmich, Morelli, & O’Neill, 2010). According to Pati, Harvey, and Thurston (2012), “The centralized model provides relatively greater value in the areas of nursing peer support, socialization, mentoring, and consultation with other providers, among others” (p. 518). Conversely, research has found that centralized nursing stations can lead to increased walking distances, unproductive use of nursing time, and increased stress levels (Pati, Harvey, Redden, & Summers, 2015).
At the beginning of the 21st century, the concept of decentralized nursing stations was adopted, placing “smaller nursing workstations throughout a unit, closer to patient rooms” (Trzpuc & Martin, 2010, p. 38). The goal of this model was to improve workflow and caregiver efficiency by placing caregivers in closer proximity to patients, decreasing nurse walking distance, increasing time spent with patients, and enhancing patient safety through the reduction of patient falls. Gurascio-Howard and Malloch (2007) found that RNs assigned to decentralized nursing stations had increased visits to patient and medication rooms, quicker responses to patient calls, and improved patient visibility. On the other hand, several researchers have found that decentralized nursing stations reduce communication and collaboration among staff, result in less patient and peer-to-peer visibility, and provide fewer opportunities for mentoring and networking, all of which can lead to reduced efficiency in the care process (Hua, Becker, Wurmser, Bliss-Holtz, & Hedges, 2012; Pati & Redden, 2015; Zborowsky et al., 2010). Thus, the literature revealed conflicting findings regarding the positives and negatives of these two models and more research is needed.
As a by-product of the disparate findings, a third alternative, which has been labeled the hybrid model, has been recommended. This model includes “a larger, nursing unit with several touchdown areas located throughout the unit and closer to patient rooms” (Trzpuc & Martin, 2010, p. 38). Additionally, Hua, Becker, Wurmser, Bliss-Holtz, and Hedges (2012) have suggested a fourth model that they identify as a multihub design, “in which several essentially identical larger nursing stations are distributed across a nursing unit” (p. 11).
Whatever model is utilized, the overall nursing unit must be seen as “a group of interrelated spaces—a system of parts with permeability between the parts” (Hillier & Hanson, 1984, as cited in Zadeh et al., 2012, p. 56). Pati, Harvey, and Thurston (2012) state that “physical design alone may not contribute entirely to system efficiency optimization, and there need to be parallel interventions in operations as well as culture change” (p. 514). The culture of care can be defined by systemic factors, values, and expectations and can result in “lower levels of achievement in operational flexibility” if not taken into consideration (Pati, Evans, Harvey, & Bazuin, 2012, p. 94). Thus, the design of the unit can either support or hinder a culture of care.
Walkability
The increase in unit size, proximity of support areas, and the adoption of new nursing station models, such as decentralized, have led to a growing interest in how these factors impact the amount of walking done by staff and the resultant level of care. According to Hendrich et al. (2009), “A supportive nurse work environment should enhance the efficiency of nurses while limiting the stress and physical burdens of nursing practice, thereby fostering nurse satisfaction and retention” (p. 7). Research has explored the relationship between walking and nurse fatigue, stress, and efficiency, all of which impact the quality of patient care. Walking is a time consumer for nurses and can lead to waste from a systems efficiency perspective. Less time spent walking translates into greater time spent on patient care activities. On average, nurses spend more than a quarter of their time walking during each shift (Gurascio-Howard & Malloch, 2007; Zadeh et al., 2012). Several significant factors influence the amount of travel in healthcare facilities including time and length of shift, access to supplies, and unit designs.
The amount of walking done by caregivers can vary greatly based on time and length of shift. A 36-hospital time and motion study revealed that the median distance walked during a 10-hr daytime shift was 3.0 miles, whereas night shift nurses walked a median distance of 2.2 miles (Hendrich et al., 2008). It is also suggested that distance walked could increase up to 5.0 miles per 10-hr daytime shift based on unit topography and nurse assignments (Hendrich et al., 2009). Pati and Lee (2011) estimate that for a 12-hr shift, nurses could walk as much as 4.0 miles.
The move to a decentralized design can be attributed to a desire to decrease travel distances by staff (Pati and Redden, 2015). One of the hypothesized benefits of decentralized nursing stations was a decrease in walking, thus leading to more productive use of nursing time. However, in a study comparing three centralized and decentralized units pre- and postmove, Pati, Harvey, Redden, and Summers (2015) found that while there were quality of work improvements in documentation, medication, and supplies with the decentralized models, there were unexpected results in that the amount of walking increased in all units. In the poststudy, distances increased by 0.39, 0.66, and 1.74 miles in the three decentralized units examined. In addition, nurses’ perceptions of walking distances increased as revealed through a staff survey.
Another unit design factor integral to the discussion of walkability is access to supplies, medication, and support spaces by staff. Seo, Choi, and Zimring (2010) hypothesized that distributed substations with supplies might reduce nurses’ walking times when comparing a large and small intensive care unit (ICU). They found that nurses did not walk longer or spend more time getting medications in the larger decentralized unit. Pati, Harvey, and Thurston (2012) suggest that “if support areas are brought closer, the distances walked and time spent in walking by nurses can be substantially reduced” (p. 513). Ultimately, the overall unit shape or layout type might not be a good predictor of nurses’ walking behavior. Instead, the characteristics of the path that connects functional spaces such as patient rooms, medication, and supplies might better predict nurses’ walking behavior (Yi & Seo, 2012).
Allocation of time and room usage
One of the concerns expressed in the literature is that the time nurses spend walking decreases the amount of individual time dedicated to patient care. As noted in a publication by the Ohio Nurses Association, “Nurses spend less than one-third of their time on direct patient care, largely because of inefficient work processes and environments” (as cited in Zadeh et al., 2012, p. 41). The largest consumers of time among caregivers are documentation, medication administration, and coordination of care. These activities can take place in a variety of locations including the nurses’ station, patient rooms, medication and supply areas, and even off the unit, thus further effecting the flow of patient care. A number of studies support the fact that more time is spent at the nurses’ station than any other location (Duffield, Gardner, & Catling-Paull, 2008; Hendrich et al., 2008, 2009). Hendrich et al. (2008) found that nurses spent 39% of their time or 214 min at the nurses’ station while 31% of their time or 171 min was spent in the patient room over a 10-hr shift. The authors also found that 6.6% or 36 min of nurses’ activities could be characterized as waste. Overall, these findings have significant implications for patients’ perceptions of the quality of care as well as nursing unit design.
When comparing the impact of centralized and decentralized unit design on time spent in patient care, Guarscio-Howard and Malloch (2007) found that more time was spent in patient care activities and in patient rooms in decentralized units than centralized. The decentralized nursing model was found to increase visits to patient rooms by 40% and led to 138% more visits to the medication room. Additionally, over a 12-hr shift, the decentralized nurses spent less time in the alcoves than centralized nurses spent at the central nurses’ station. One factor potentially contributing to this is proximity, which encourages more patient room visits. As previously noted, the comparison of decentralized and centralized units is impacted by more than just design. Hendrich et al. (2009) state, “Each nurse’s approach to the work process exerts a greater effect on…patient care time than the physical layout of the nursing unit” (p. 11).
Visibility
Another reason for moving to the decentralized model was to bring caregivers closer to the patients in the increasingly larger building footprint. This was done not only to reduce walking but to provide greater visibility, thus increasing patient safety. Harvey, Pati, Evans, Waggener, and Cason (2006) define patient visibility as “maintaining visual and/or auditory contact with patients” (p. 4). More specifically, visibility into patient rooms is present when the “upper third of the bed [can] be seen when either the door or room blinds are open” (Catrambone, Johnson, Mion, & Minnick, 2009, p. 80). Equally important is the ability to see other staff members within the unit when assistance is needed, which Harvey et al. (2006) label peer line of sight. Lu (2010) suggests that improved visibility has at least three important outcomes. It can enhance patient safety by enabling better observation and faster response to falls and other injuries. Secondly, increased visibility enables nurses to spend more time in direct care at the patient bedside. Lastly, it contributes to enhanced communication between staff and patients and improves patient satisfaction. Several factors can contribute to ideal visibility in healthcare facilities. Not only does the shape of the unit structure impact visibility but also the location of doors and windows along corridors, position of patient bathrooms, and the location of the nurses’ station. Zborowsky et al. (2010) maintain that neither centralized nor decentralized nursing station designs contribute to superior visibility; however, they contend that the number of patient beds that can be viewed from the nursing station is a critical factor.
Study Purpose
As the complexity of the work environment evolves to better address issues such as teamwork, walkability, allocation of time, and visibility, more research will be required to examine the influence of the physical layout of the space on clinical processes and their impact on efficient patient care. Thus, it is the purpose of this research to examine efficiency through the lens of a centralized and decentralized unit design. Three specific research objectives were identified for the study: To analyze the impact of decentralized and centralized hospital design layouts on the delivery of efficient care. To determine the impact of decentralized and centralized hospital design layouts on caregivers and the resultant level of satisfaction. To gain a richer understanding of design decisions to help impact future investigations through a pre- and postoccupancy study.
Since 2010, a growing body of research has included both pre- and postoccupancy evaluations to determine the sources of design problems, how the new design responds to these issues, and the effectiveness of the design responses (see, e.g., Kotzer, Zacharakis, Raynolds, & Buenning, 2011; Schreuder et al., 2015; Shepley, Rybkowski, Aliber, & Lange, 2012). An even smaller number of studies have specifically examined the pre- and postoccupancy impacts of moving from a centralized to a decentralized care delivery model (see Pati and Redden, 2015).
Study Setting
In this single-case study, an interdisciplinary team with members from healthcare, communication, statistics, and design conducted a multiphased pre- and postoccupancy evaluation of a cardiovascular service line in an academic hospital that moved from a centralized to decentralized model. Prior to the move, the service line was housed in four separate locations, each containing a centralized nursing station. Three of these locations focused on progressive and acute care (36 beds; see Figure 1), while the fourth was an ICU (16 beds; see Figure 2). Rooms in the progressive and acute care settings were both single and/or double occupancy depending upon patient census. The decentralized model unified the entire service line on one floor with two-person recessed alcoves outside each pair of rooms. Each decentralized station faces the patient rooms and provides a direct view to the patient headwall. The floor was divided into two towers, one for progressive (32 beds) and one for ICU (32 beds). All rooms in the new model were single occupancy with provision for family and visitors. The new cardiovascular unit includes a double-corridor racetrack design with a resident workroom anchoring one end and an interdisciplinary care team station at the opposite end. In the core, medication, clean and soiled utility, nourishment, equipment rooms, as well as breakrooms, and multidisciplinary office cubicles are provided. These are mirrored on each hallway within the towers (see Figure 3).
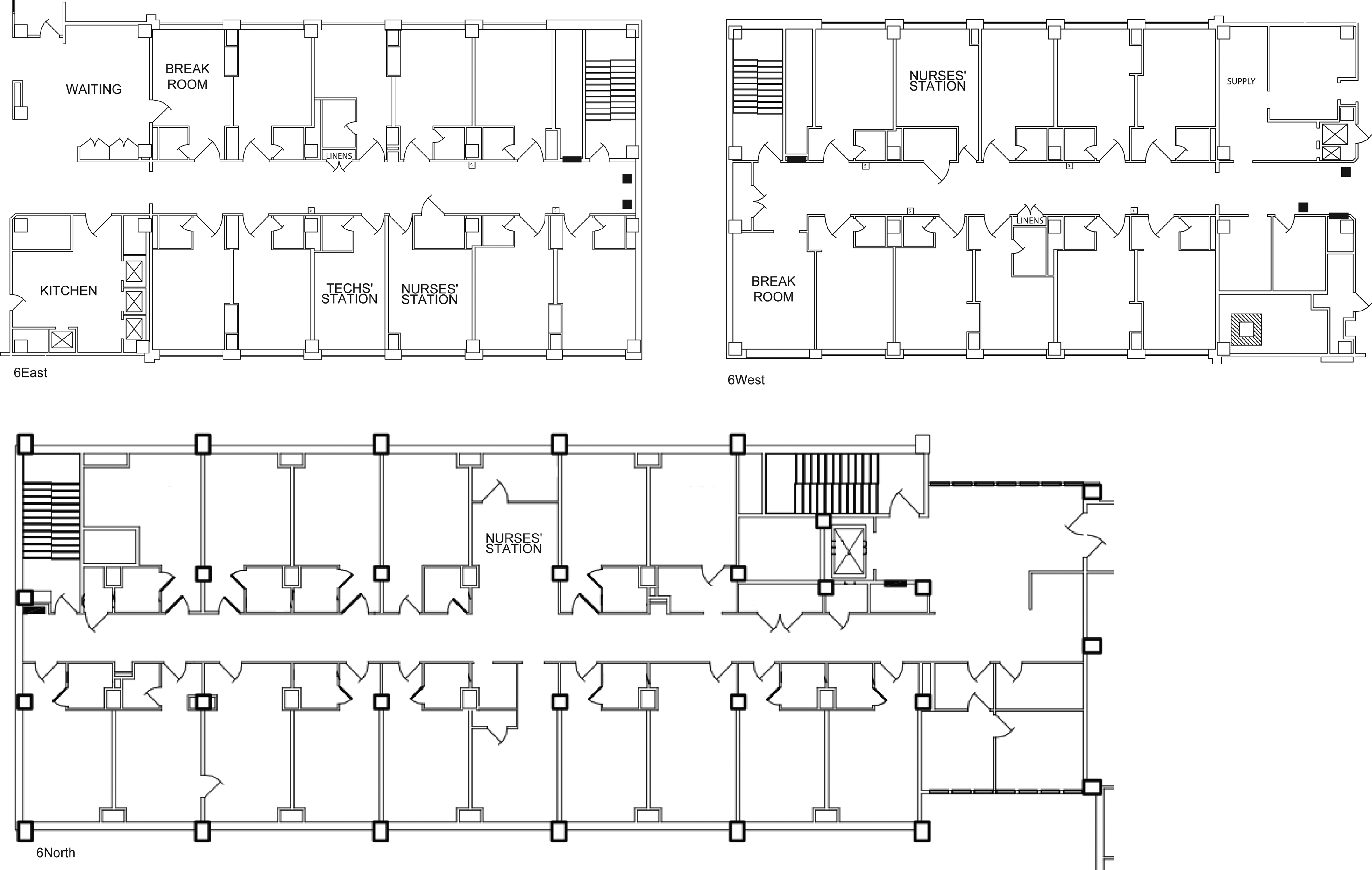
Centralized design models of progressive and acute care units.
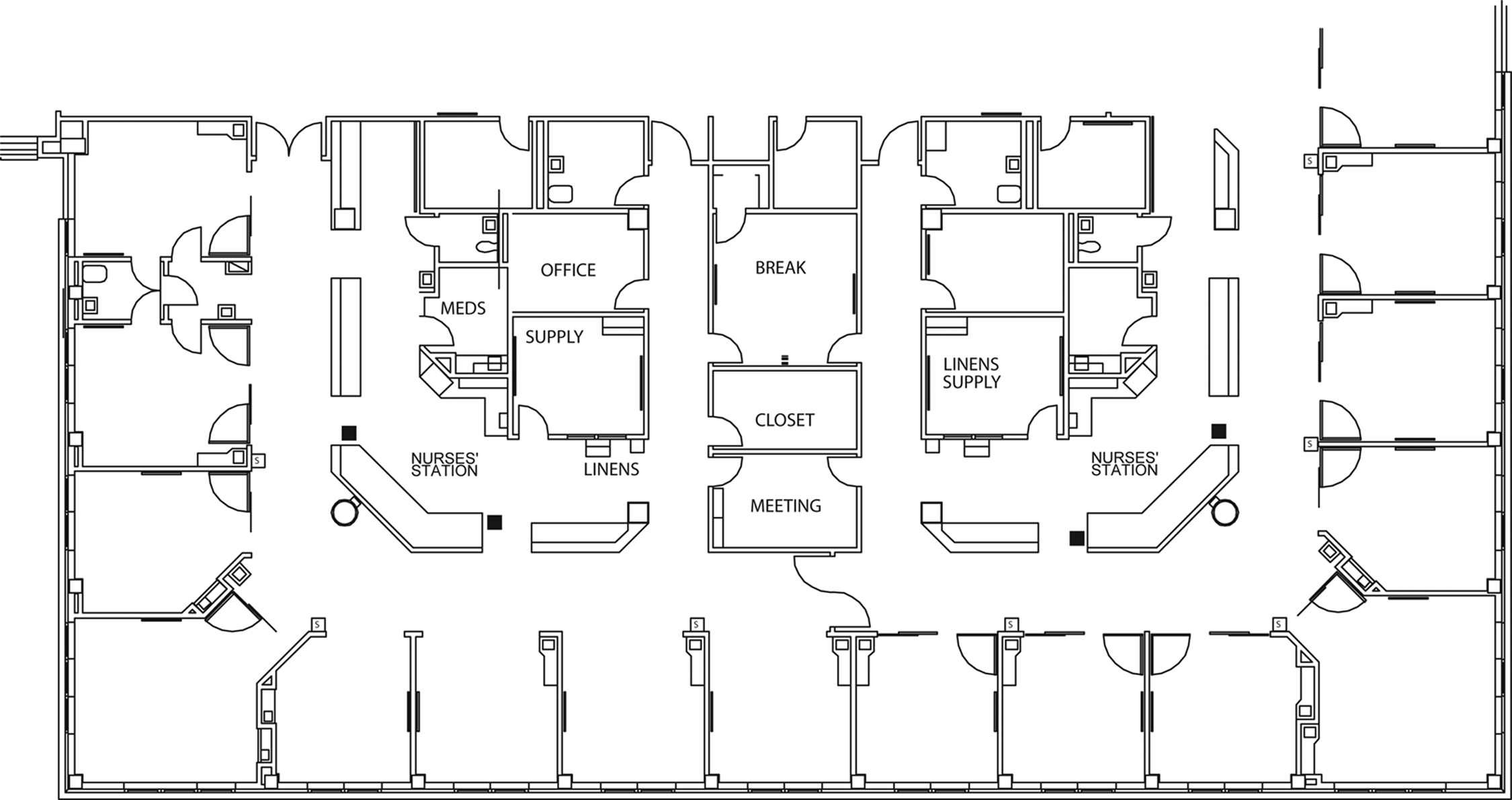
Centralized design model of intensive care unit.
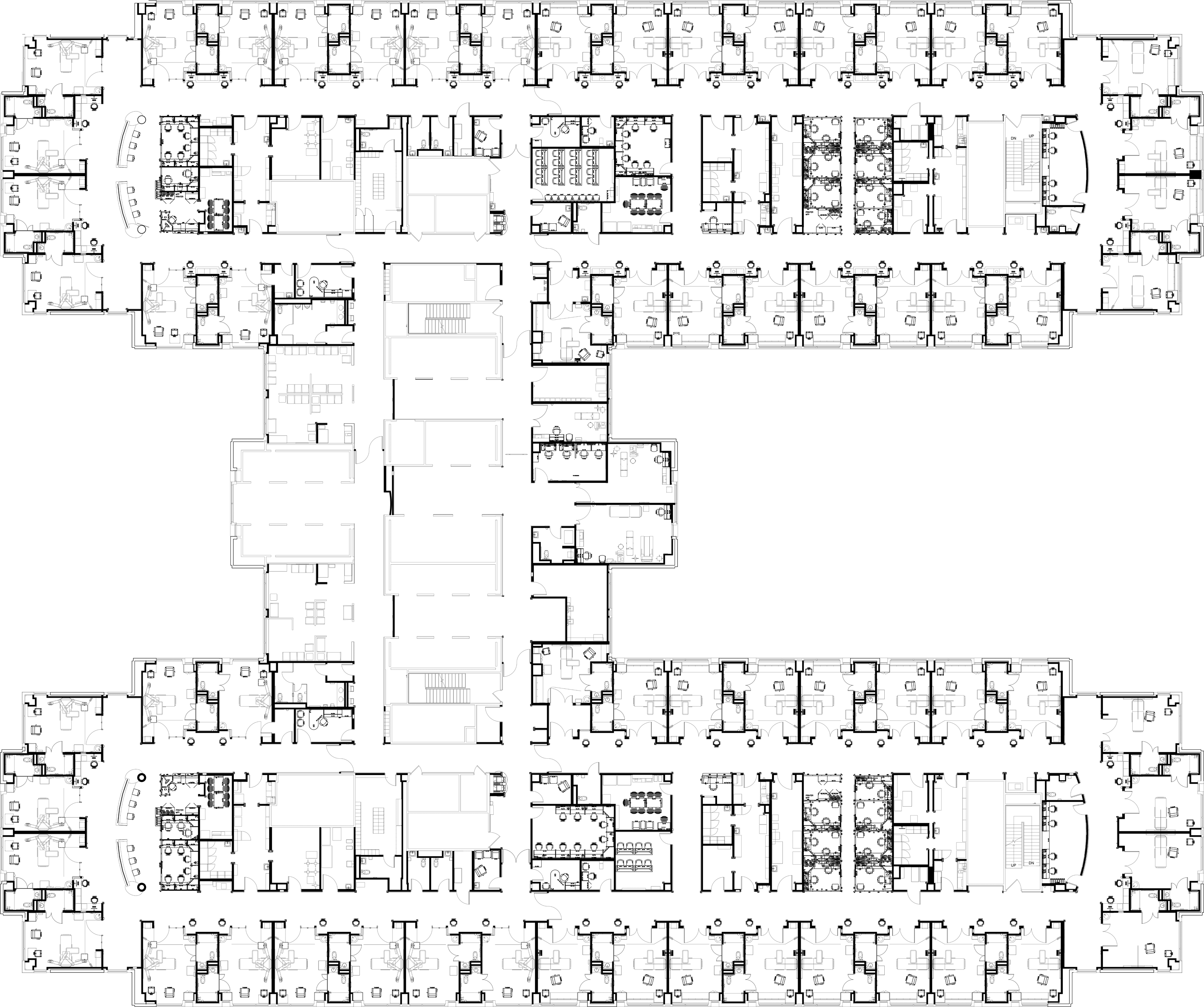
Decentralized design model of intensive and progressive care unit.
Method
This study examined the impact of walkability, room usage, allocation of time, and visibility in relation to efficiency and caregiver satisfaction in a pre- and postoccupancy evaluation. Data collection methods included pedometer measurements of staff walking distances, room usage data, time studies in patient rooms and nurses’ stations, visibility counts, and staff questionnaires yielding qualitative and quantitative results. Participant groups for this study included managers, nurses, physicians, technicians, and therapists. Institutional review board approval was obtained for the use of all instruments. Prior to obtaining data, human subject certification was also obtained and training in the use of the instruments occurred to ensure validity and reliability of findings. The prestudy was conducted in the fall of 2014 and the poststudy was initiated in the summer of 2015, 6 months after the opening of the new unit.
Walking distance of nurses and technicians was collected using electronic, battery-operated pedometers. The data collection took place over all hours of the day. Prior to data collection, staff members completed a survey to gather demographic information including their height, which they selected from one of the six disjoint categories. For each height category, the midpoint was used to determine the average steps per mile for someone of that height. This was then used to transform the steps taken into miles walked per participant. During the data collection period, staff members were further asked to complete a short electronic survey after each shift to record the number of steps taken and length of shift; nurse and technician shifts ranged from 2 to 15 hr. To account for this difference, measures were standardized per person to miles walked per hour per shift. Overall, 24 staff members participated in the prestudy yielding a total of 205 entries. The postoccupancy evaluation had 21 participants for a total of 179 entries. An attempt was made to collect data from the same participants in both the pre- and poststudies; in total, 11 participants contributed to the matched pairs data. The 11 matched pair participants contributed 119 entries in the prestudy and 114 in the poststudy.
Observations were conducted to determine frequency of staff presence in patient rooms and nurse stations. Room usage was tallied each time a staff member entered a room or station over the course of 4-hr observational shifts. To analyze the patient room data, observations were averaged per room per observational shift. For the nurses’ stations, the centralized model included only one station per unit compared to one nurses’ station for every two-patient rooms in the decentralized model. To account for this difference, data were analyzed by averaging visits to the nursing station over an observational shift. A total of 48 hr of observation (12 shifts) occurred during the prestudy while postobservations encompassed a total of 68 hr (17 shifts). A single 4-hr shift had between 1 and 10 observational pairs collecting data.
Observational studies were also conducted to measure the amount of time nurses were spending at their stations and in the patient rooms. Using a stopwatch, nurses were timed from the moment they arrived at either their desk or the patient room to the moment they left. The summary analysis was conducted using the same methodology as for the room usage.
Visibility counts were completed to identify two types of visibility: patient visibility and peer line of sight. Patient visibility was measured by identifying the number of patient beds in direct view from the nurses’ seat at a station. Peer line of sight was determined by identifying the number of additional nurses’ seats that could be seen from the nurse’s seat at a station. The range of values was given for both patient visibility and peer line of sight counts.
Staff questionnaires were electronically administered to a variety of healthcare professionals. All staff members from the cardiovascular service line had the opportunity to participate; however, self-selection bias could be present because involvement was not mandatory. The questionnaire was piloted in another unit 6 months prior to this study. A total of 66 questions divided among seven categories were asked in the survey. However, only 16 of these questions focusing on efficiency, staff satisfaction, and centralized and decentralized unit design were relevant to the focus of this article. Space was allocated for open-ended comments. Staff outcomes from the premove yielded 45 usable surveys while the postmove yielded 98 surveys. Responses were recorded on a 5-point Likert-type scale, with 1 indicating strongly disagree, 5 indicating strongly agree, and 3 being a neutral value. Thus, when averaging across the sample, a mean greater than 3 implies overall agreement with the statement. Statistically significant differences were valued at p < .05.
Results
Walkability
Overall outcomes of walkability from the pedometer measures prior to the move indicated that the mean walking distance per hour among participants was 0.347 miles or 4.16 miles per 12-hr shift; in the decentralized unit, the mean walking distance per hour was 0.339 miles or an average of 4.07 miles per 12-hr shift. For the matched pairs, the average difference in miles walked per individual (post minus pre) was 0.020 miles per hour or 0.245 miles based on a 12-hr shift. When comparing walking distances of nurses and technicians, nurses walked an average of 3.75 miles in the prestudy and 4.00 miles in the poststudy, while technicians walked an average of 7.19 miles in the prestudy and only 3.88 miles in the poststudy over the course of a 12-hr shift. While the findings for decreased walking in the poststudy for technicians confirm previous literature, this significant decrease might be attributed in part to the fact that the unit design prior to the move was in four different areas on two different floors, while in the poststudy, all units were now contained on one floor. Comparisons were also made in walkability between the progressive care and intensive care cardiovascular units. In the progressive unit, all participants in the prestudy averaged a total of 3.71 miles per 12-hr shift as compared to 4.21 miles in the poststudy. Interestingly, in the ICU, walking decreased from 4.55 miles to 3.64 miles over 12 hr.
Allocation of Time and Room Usage
During the 4-hr observational shifts, data were collected in each unit for the amount of time nurses spent at their stations and in patient rooms. Overall, nurses averaged 1:04:01 at their centralized stations in the prestudy and 0:51:44 at the decentralized stations in the poststudy. The overall average time nurses spent in patient rooms during a 4-hr observational shift was 0:18:40 in the prestudy; this increased to 0:23:53 in the postevaluation. These data were further examined by unit type. For progressive care, nursing time in patient rooms in the prestudy averaged 0:14:14 as compared to 0:18:27 in the poststudy. However, nursing time in patient rooms decreased for the ICU from pre to post; the average time for the prestudy was 0:33:02 and the average time for the poststudy was 0:28:48.
Overall outcomes from the room usage data revealed that the number of visits by staff per patient room increased from 9.36 visits per 4-hr observational shift to 15.64 visits per observational shift in the poststudy. This reflects a 67% increase in visits to patient rooms in the decentralized model. In examining the data by level of care, progressive care reflected a change from 9.43 patient room visits per 4-hr observational shift to 13.58 in the poststudy, representing a 44% increase. For the ICU, patient room visits per shift increased from 9.11 in the prestudy to 17.41 in the poststudy, a 91% increase. Regarding nursing station usage, the number of visits increased from 61.15 to 66.55 per observational shift. However, this value contains some bias due to the design of the unit, as three observational zones were utilized in the prestudy as compared to five in the poststudy due to sightlines. This bias contributes to a decrease in the average number of poststudy visits, which means that the increase is more substantial than the data indicate.
Visibility
Due to the nature of the design of the old unit’s progressive care, no patient beds were directly visible from the centralized nursing stations. On average, three nurses were assigned to the unit per shift and all could be seen when seated in the station. The use of glass doors and positioning of the nurses’ stations in the prestudy’s ICU allowed for visibility ranging from two to four patients and four to nine peers. In the new unit, the majority of nurses seated at their decentralized station could only see one patient through the window into the room regardless of whether the room had wood or glass doors. However, the nurses seated at the four stations anchoring the end of each tower (ICU and progressive) could see two patients each. For peer line of sight, the number of seated colleagues that could be seen from a specific nursing station ranged from 3 to 11 for both progressive and ICU units. This does not account for the number of nurses working during different shifts. Observations over time suggest the number of peers that could be seen at any 1 time would be at the smaller end of the range.
Staff Satisfaction
Ten questions were presented to the staff regarding overall efficiency. There was a significant difference in responses to five of the questions, all of which rated the centralized unit more positively than the decentralized unit. More specifically, there was a significant difference in the mean responses (M pre = 4.21, M post = 2.94, p = .00) to the layout of the units in supporting the staff’s ability to work as a team. When asked about the unit layouts’ ability to support individual work, a mean of 3.97 was reported for the prestudy and 3.83 for the poststudy, a nonsignificant difference. Further, the staff rated the old unit significantly higher than the new unit in its ability to support reasonable walking distances (p = .00) and efficient patient care (p = .00). Regarding patient rooms, the respondents perceived that the location of the supplies within the rooms of the decentralized unit contributed to greater efficiency (p = .05). There was not a significant difference in the means regarding the impact of the layout of the patient room in supporting efficient care when moving from the centralized to the decentralized model. Surprisingly, staff perceptions of their ability to monitor patient rooms were significantly higher (p = .04) in the centralized model (see Table 1).
Pre-/Postquestionnaire Outcomes.
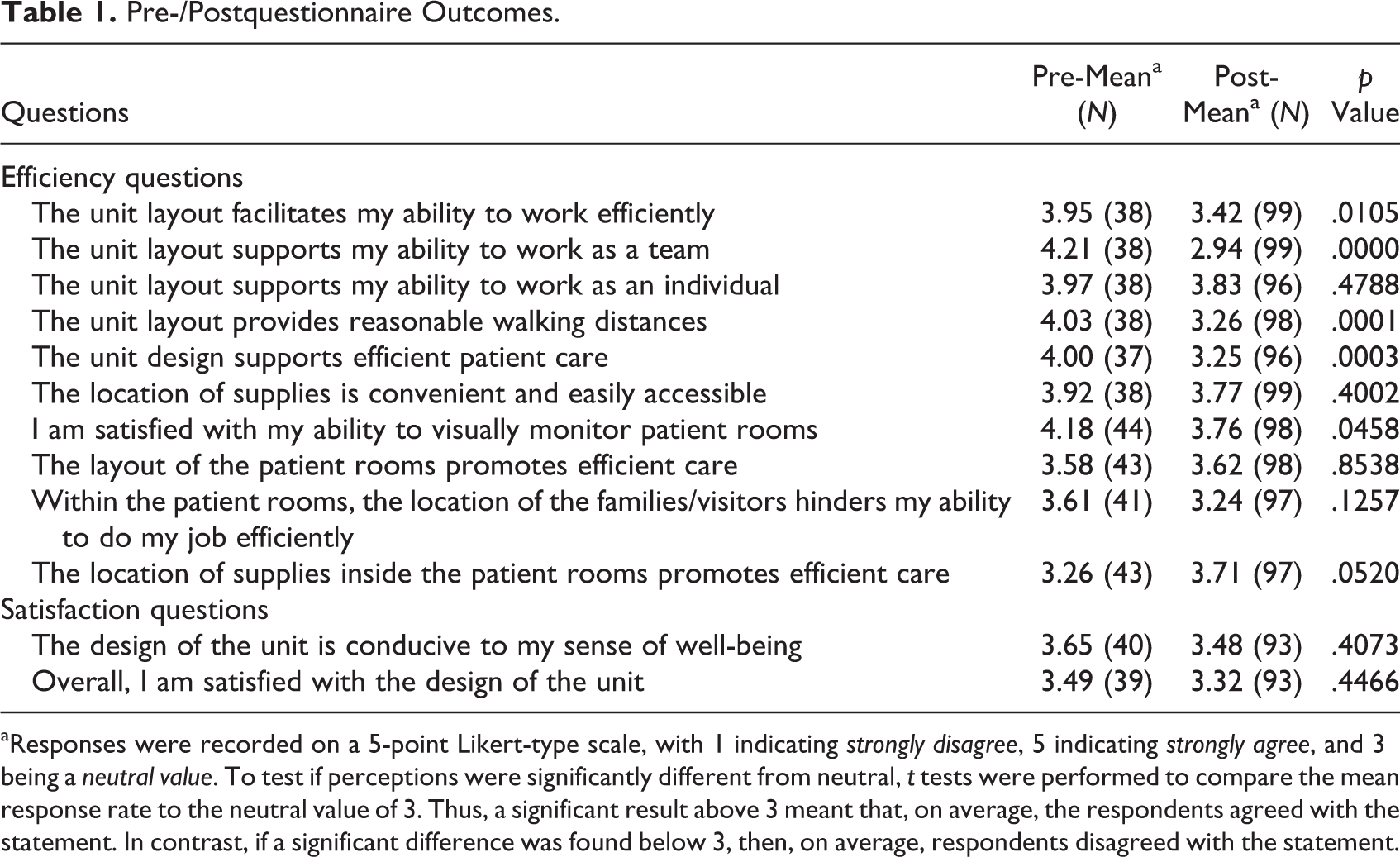
aResponses were recorded on a 5-point Likert-type scale, with 1 indicating strongly disagree, 5 indicating strongly agree, and 3 being a neutral value. To test if perceptions were significantly different from neutral, t tests were performed to compare the mean response rate to the neutral value of 3. Thus, a significant result above 3 meant that, on average, the respondents agreed with the statement. In contrast, if a significant difference was found below 3, then, on average, respondents disagreed with the statement.
When addressing satisfaction with the design of the units, there was a nonsignificant difference between the centralized and decentralized units (M pre = 3.49, M post = 3.32, p = .45). There was also a nonsignificant difference perceived between the staff’s sense of well-being (see Table 1). On the postquestionnaire, specific questions comparing satisfaction levels with the two models were added. Contrary to the data on the pre-/postquestions, these direct comparison questions were all overwhelmingly positive toward the decentralized model (see Table 2). When asked specifically if they preferred the design of the new unit layout over the old, the difference was significant in favor of the new model (M = 3.64, p = .00). Further, responses regarding storage in the new unit, the size of the unit, and patient room design all significantly favored the new model.
Direct Comparison Questionnaire Outcomes.
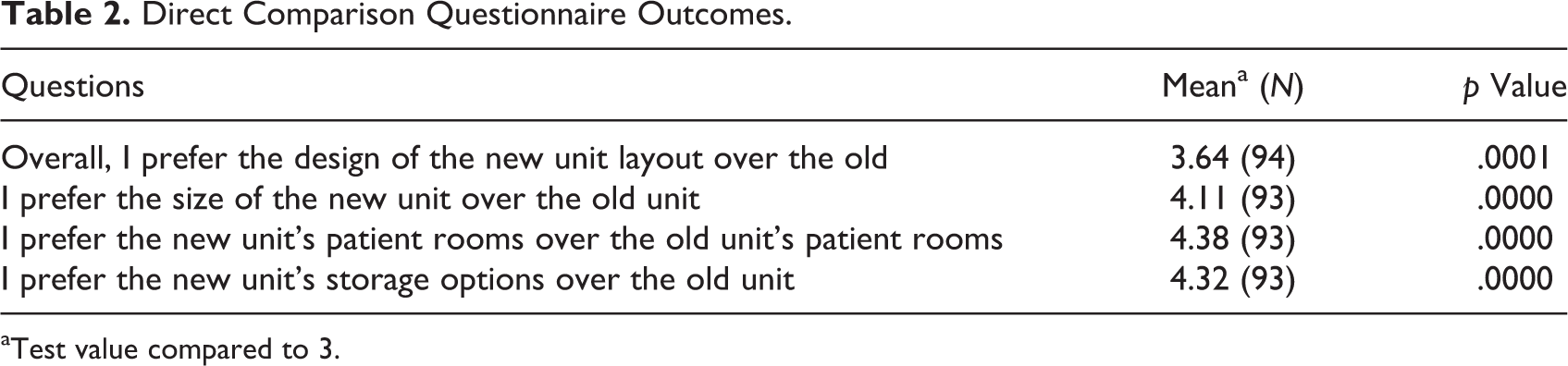
aTest value compared to 3.
As part of the questionnaire, staff were asked to respond with open-ended comments on two questions: (1) what is working well in the new unit and (2) what needs to be improved or changed? Outcomes revealed mixed responses relative to walkability, visibility, teamwork, room usage, and staff satisfaction. Thus, these open-ended comments further exposed the complexity of comparing centralized and decentralized design models.
Discussion
Caregiver efficiency and satisfaction are influenced by nursing station design, an integrated interdisciplinary team approach, and outcomes such as walkability, allocation of caregiver time, and visibility. Overall, data indicate that this study’s decentralized unit design positively influences proximity to patients in a larger design footprint. However, outcomes suggest that staff walking distances increased because staff are not always assigned to every station nor are their room assignments always in close proximity to their patients. This emphasizes the important role of care delivery processes in streamlining patient care. It was also found that the location of supply and medication rooms further contributes to increased walking if these spaces remain in the central core rather than being disbursed throughout. An important consideration as suggested by Yi and Seo (2012) is that the characteristics of the path that connects functional spaces are more important in predicting walking behavior than unit shape or nursing station model. This suggests that support spaces should be distributed in close proximity to decentralized nurse stations within the design footprint.
The findings of this research confirm the literature suggesting more time is spent at the nursing station than any other location and that the decentralized model results in increased visits to and time spent in patient rooms (Duffield et al., 2008; Hendrich et al., 2008, 2009). This is certainly one of the strengths of the decentralized model in that increased time at the patient bedside leads to improved patient care and safety measures. While it was found that a significant amount of nurses’ time was spent at the nursing station in both pre- and poststudies, the decentralized model did contribute to less time being spent at the nursing station than in the centralized model, which supports Guarscio-Howard and Malloch’s (2007) findings. One of the limitations of this study was that the research did not critically examine how other time was spent and what amount of time was contributing to waste. This would offer a stronger comparison of efficiencies within these models and suggest how the design could lead to improved processes and care.
The positives and negatives outlined in the literature regarding visibility and its impact on efficiency were confirmed in the research findings (Zborowsky et al., 2010). Within the design of this particular decentralized model, the majority of nurses and technicians could only see into one room from their seated position. While potential sightlines to peers existed, the findings support that the decentralized model contributes to feelings of isolation. Further, this was once again impacted by nursing shift assignments, meaning that the decentralized model could function differently at any given time. Although the decentralized model positions staff closer to the patient, views to more than one patient and peer line of sight can both be limited. While the literature notes that safety and efficiency are achieved when patient visibility is enhanced, decreased interaction between staff in the decentralized model could potentially be a barrier to patient safety and teamwork. Therefore, future designs should consider offering increased sightlines to multiple patients while enhancing opportunities for peer-to-peer interaction and support.
Lastly, an important outcome revealed by the data was the conflicting responses in the pre- and postquestionnaires and in the direct comparisons of the old and new units. The centralized design of the old unit was rated significantly higher in its ability to support teamwork, reasonable walking distances, and efficient patient care. The centralized unit was also perceived to be more conducive to the staff’s sense of well-being. One reason for the high favorability toward the centralized model may be due to the fact that the questionnaire was administered prior to the move, and responses may have been based on familiarity with this model. Building upon this, perceptions of the decentralized model, as revealed through the questionnaire, may have been lower as the staff more critically analyzed the changes in the new space, to which some may have been resistant. One suggestion for addressing this would be to ensure greater inclusion and transparency with the staff during the design process and in training to prepare them for a cultural change. However, as previously stated, when staff were asked to directly compare the old and the new models, their responses were significantly positive toward the decentralized model. This could be due to the inclusion of positive design attributes or the influence of the “newness” factor. Future research studies might more specifically ask a question comparing satisfaction with the efficiency of the old versus the new models to elicit a more critical comparison.
Conclusion
While the study exposed both positives and negatives of the centralized and decentralized models, implications of each for efficiency, teamwork, and staff satisfaction were revealed. The decentralized model was adopted in part as a response to the increased size in the unit footprint needed to accommodate larger patient rooms. Staff responded positively to the improved patient room designs yet felt that the decentralized design disconnected them as a team. Additional factors impacting efficiency, as revealed by the research, included disjointed supply sources, geography of assignment, and visibility issues. These inefficiencies support the recommendation to place greater emphasis on the convenient placement of support spaces such as medication and supply rooms, offer increased sightlines to multiple patients, and enhance opportunities for peer-to-peer interaction and support. Yet at the same time, nursing stations should be positioned to maintain increased time in room. This suggests consideration of a hybrid model, which combines a centralized collaborative unit with touchdown spaces dispersed periodically outside of patient rooms. This hybrid design model would maintain the positive aspects revealed by the research but address staff concerns.
This study revealed that unit design alone does not solely impact efficiency. Future studies examining efficiency should further assess healthcare processes and a culture of care as interrelated, contributing factors to a care environment. For example, it was determined that aspects such as nursing assignments significantly influence how a unit operates. This suggests that when designers are proposing new design models, they must also be sensitive to the broader implications of that change on the culture and processes. These factors must be addressed upfront and in tandem with the design process to ensure optimal workflow efficiencies. This research further confirms the need for more pre- and poststudies to test the impact of these models on both efficiency and processes for patient care.
Implications for Practice
Cultural shifts need to be addressed upfront and in tandem with the design process to ensure optimal workflow efficiencies.
A hybrid model should be further tested to determine whether it addresses the positive and negative aspects of the centralized and decentralized models.
The location of supply and medication rooms contributes to increased walking if these spaces remain in the central core rather than being disbursed throughout.
Future designs should consider offering increased sightlines to multiple patients while enhancing opportunities for peer-to-peer interaction and support.
Footnotes
Acknowledgment
The authors would like to thank UK HealthCare for funding this interdisciplinary study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This interdisciplinary study is funded by UK HealthCare.