
Abstract
Objective:
To investigate whether a patient’s proximity to the nurse’s station or ward entrance at time of admission was associated with increased risk of adverse outcomes.
Method:
We conducted a retrospective cohort study of consecutive adult inpatients to 13 medical–surgical wards at an academic hospital from 2009 to 2013. Proximity of admission room to the nurse’s station and to the ward entrance was measured using Euclidean distances. Outcomes of interest include development of critical illness (defined as cardiac arrests or transfer to an intensive care unit), inhospital mortality, and increase in length of stay (LOS).
Results:
Of the 83,635 admissions, 4,129 developed critical illness and 1,316 died. The median LOS was 3 days. After adjusting for admission severity of illness, ward, shift, and year, we found no relationship between proximity at admission to nurse’s station our outcomes. However, patients admitted to end of the ward had higher risk of developing critical illness (odds ratio [OR] = 1.15, 95% confidence interval [CI] = [1.08, 1.23]), mortality (OR = 1.16, 95% CI [1.03, 1.33]), and a higher LOS (13-hr increase, 95% CI [10, 15] hours) compared to patients admitted closer to the ward entrance. Similar results were observed in sensitivity analyses adjusting for isolation room patients and considering patients without room transfers in the first 48 hr.
Conclusions:
Our study suggests that being away from the nurse’s station did not increase the risk of these adverse events in ward patients, but being farther from the ward entrance was associated with increase in risk of adverse outcomes. Patient safety can be improved by recognizing this additional risk factor.
Conventional wisdom suggests that sicker patients should be admitted closer to nurse’s stations on the wards as this may improve patient outcomes due to enhanced care and improved monitoring. Conversely, patients who are admitted farther away from the nurse’s station or other high-traffic areas (e.g., entrance of the ward) may suffer from delays in care, which could increase their risk of adverse outcomes. However, studies involving patient location within a ward been limited, with most work focusing on patient-level physiological risk factors for the development of critical illness (Churpek et al., 2014a; Knaus et al., 1992; Smith, Prytherch, Schmidt, Featherstone, & Higgins, 2008). Care-level factors have also been extensively studied where decreased staffing, off-hours shift periods, and increased workload have all been associated with poor patient outcomes (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002; Laupland, Shahpori, Kirkpatrick, & Stelfox, 2008; Weissman et al., 2007). One study investigating the association between room location and risk of patients in the intensive care unit (ICU) found that patients in rooms with low visibility from the nurse’s station were associated with higher mortality compared to those admitted to high-visibility rooms (Leaf, Homel, & Factor, 2010). Other studies report that ward patients in isolation rooms are at increased risk of adverse events and outcomes (Abad, Fearday, & Safdar, 2010; Stelfox, Bates, & Redelmeier, 2003). No study has investigated the relationship between admission room location and outcomes in a large-scale general ward population. Therefore, we aimed to estimate the association between proximity to the nurse’s station and to the ward entrance at the time of patient admission and the risk of adverse outcomes. Our hypothesis is that patients admitted to locations farther away from the nurse’s station or away from the entrance of the ward would suffer adverse outcomes in terms of clinical deterioration, mortality, or LOS.
Method
Setting and Study Population
We conducted a retrospective cohort study, performing a secondary analysis of data collected from consecutive adult admissions adult patient admissions from January 2009 until December 2013 at an academic medical hospital with approximately 500 inpatient beds. All patients admitted to 13 medical–surgical wards were included, while patients from the ICU and postpartum wards were excluded from the analysis. The study was approved by the hospital Institutional Review Board (H IRB).
Data Sources
Time and location-stamped vital signs and laboratory results were collected from the electronic health record (EHR, Epic, Verona, WI) data. Demographics and discharge disposition (e.g., mortality status) were collected from administrative data. The Clinical Research Data Warehouse at the hospital provided all data elements.
Outcomes
The primary outcomes of interest were the occurrence of critical illness events (defined as a composite of ward cardiac arrest or transfer to ICU), inhospital mortality, and hospital LOS. Cardiac arrests, defined as lack of palpable pulse without resuscitation, were identified using a prospectively validated database maintained by the hospital (Churpek, Yuen, Park, Gibbons, & Edelson, 2014a; Volchenboum et al., 2016). ICU transfer information was derived from the hospital’s admission–discharge–transfer database. Only data pertaining to the first critical illness event were included in the analysis, since subsequent critical illness events may be associated with additional confounding factors.
Proximity Calculation
Detailed hospital floor places were obtained from the hospital facility service. Room and nurse’s station coordinates were extracted from these files using the dxfgrabber Python 3.6 package (https://pypi.python.org/pypi/dxfgrabber). Online Supplemental Figure 1 depicts the architectural layout of a typical ward in hospital. Each ward has approximately 20 beds and operates with 4:1 patient–nurse ratios on average and one charge nurse. Each ward has one nurse’s station centrally located midway through the ward. There is no direct visibility to rooms that are not opposite the nurse station. Ward entrance was defined as the coordinates of the hallway entrance of each ward and is located at the end of each unit. All hospital wards considered in this study had the same architectural design. Patient admission room was determined from the location-stamped first ward vital sign, obtained from EHR data. Proximity between nurse’s station and patient admit room and between ward entrance and patient admit room was calculated using Euclidean distance metrics, defined as the straight-line distance between two points in two-dimensional Euclidean space. Proximity was categorized into at or below versus above the median distance.
Potential Confounders
We adjusted for a number of potential confounders (all calculated using data at the time of admission), including patient severity of illness using the electronic Cardiac Arrest Risk Triage (eCART score), a previously published early warning score calculated from vital sign and laboratory result data (Churpek et al., 2014a, 2014b), time of day (day: 7 a.m. to 5 p.m., evening: 5 p.m. to 10 p.m., and night: 10 p.m. to 7 a.m.), weekday versus weekend, year, and the specific ward to which the patient was admitted.
Statistical Analysis
First, we compared patient clinical characteristics between patients across all the primary outcomes using χ2 tests for categorical variables and t tests for numeric variables. We also compared the distribution of patients with and without primary outcomes against proximity to the nurse’s station and the ward entrance. Next, we utilized logistic regression to measure the association between proximity to nurse’s station or ward entrance at admit and each primary outcome, after adjusting for confounders. Sensitivity analysis was also performed by including only patients who remained in the same room for at least 48 hr since admit to avoid transient effects from patients with shorter stay. Analyses were performed using R, version 3.3 (R Project for Statistical Computing), with two-sided p value < .05 denoting statistical significance.
Results
Study Population
Among 83,635 ward admissions that were included in this study, a total of 4,129 experienced a critical illness event, 1,136 died, and 41,182 patients had a longer LOS than the median LOS of 3 days. Patient clinical characteristics are shown in Table 1. Patients who experienced critical illness events were older (60 years vs. 57 years, p < .001), less likely to be female (50% vs. 56%, p < .001), and had higher severity of illness at admit (median eCART: 7 vs. 5, p < .001). Compared to patients who were discharged alive, patients who died were older (64 years vs. 57 years, p < .001), less likely to be female (48% vs. 53%, p < .001), and had a higher severity of illness at admission (median eCART: 11 vs. 5, p < .001). Patients who had a greater-than-median hospital LOS were slightly older (57 years vs. 56 years, p < .001) and less likely to be female (50% vs. 55%, p < .001) than patients with a shorter (i.e., lesser or equal to median) LOS.
Comparison of Patient Clinical Characteristics at Admission With Respect to Development of Critical Illness, Mortality, and Longer LOS.
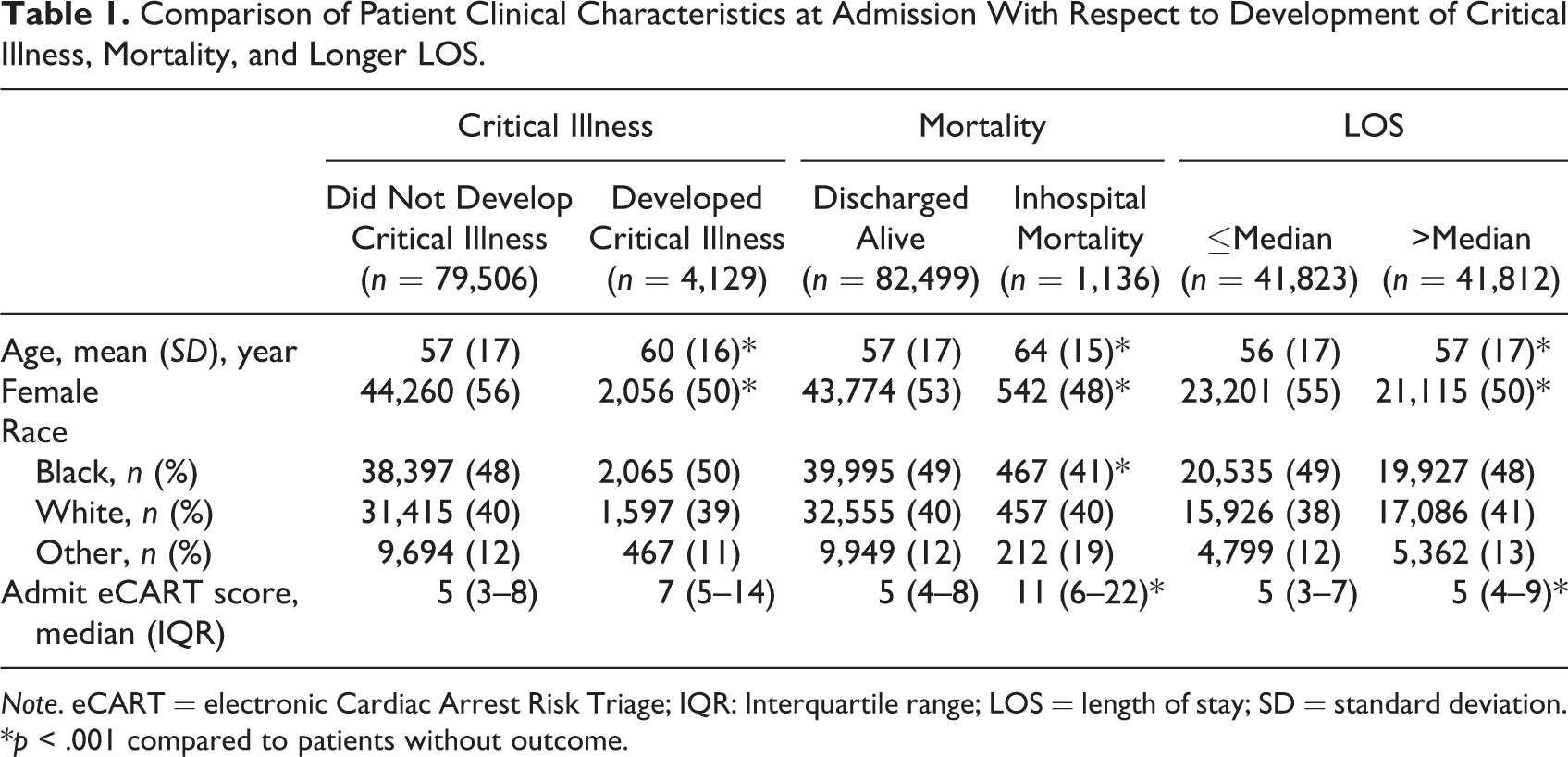
Note. eCART = electronic Cardiac Arrest Risk Triage; IQR: Interquartile range; LOS = length of stay; SD = standard deviation.
*p < .001 compared to patients without outcome.
Unadjusted Analysis of Patient Location at Admit and Outcome
There was no relationship between patients who experienced critical illness or mortality and proximity to nurse’s station at admission (Table 2). Patients who were admitted farther from the nurse’s station had lower risk of having a longer LOS than those admitted closer to the nurse’s station (49% vs. 51%, p < .001). Patients who were admitted farther from the ward entrance had a higher chance of developing critical illness (54% vs. 50%, p < .001), death (59% vs. 50%, p < .001), and a longer LOS (55% vs. 45%, p < .001) compared to patients admitted closer to the ward entrance.
Comparison of Patient Location at Admission Within the Ward With Respect to Development of Critical Illness, Mortality, and LOS.
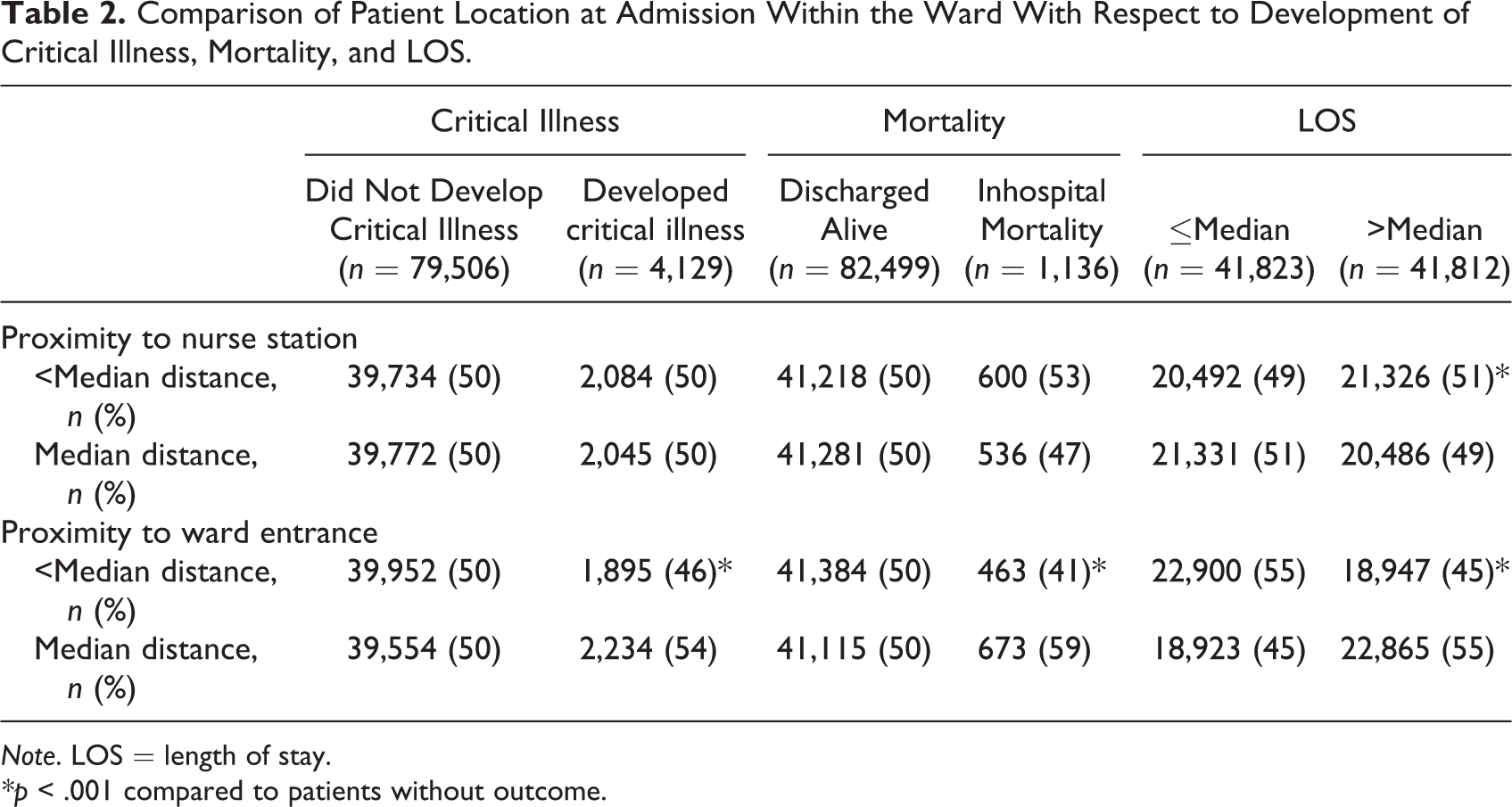
Note. LOS = length of stay.
*p < .001 compared to patients without outcome.
Figure 1a depicts no discernable association between likelihood of a critical illness event or mortality and patient admission location distance (represented as quartiles) from the nurse’s station. While the likelihood of critical illness did not show any observable trend with distance from ward entrance (Figure 1b, distance represented as quartiles), an increased risk of mortality per quartile increase in distance from the ward entrance was noted (Q1: 1.1 per 100 patients, Q2: 1.1 per 100 patients, Q3: 1.45 per 100 patients, and Q4: 1.8 per 100 patients).
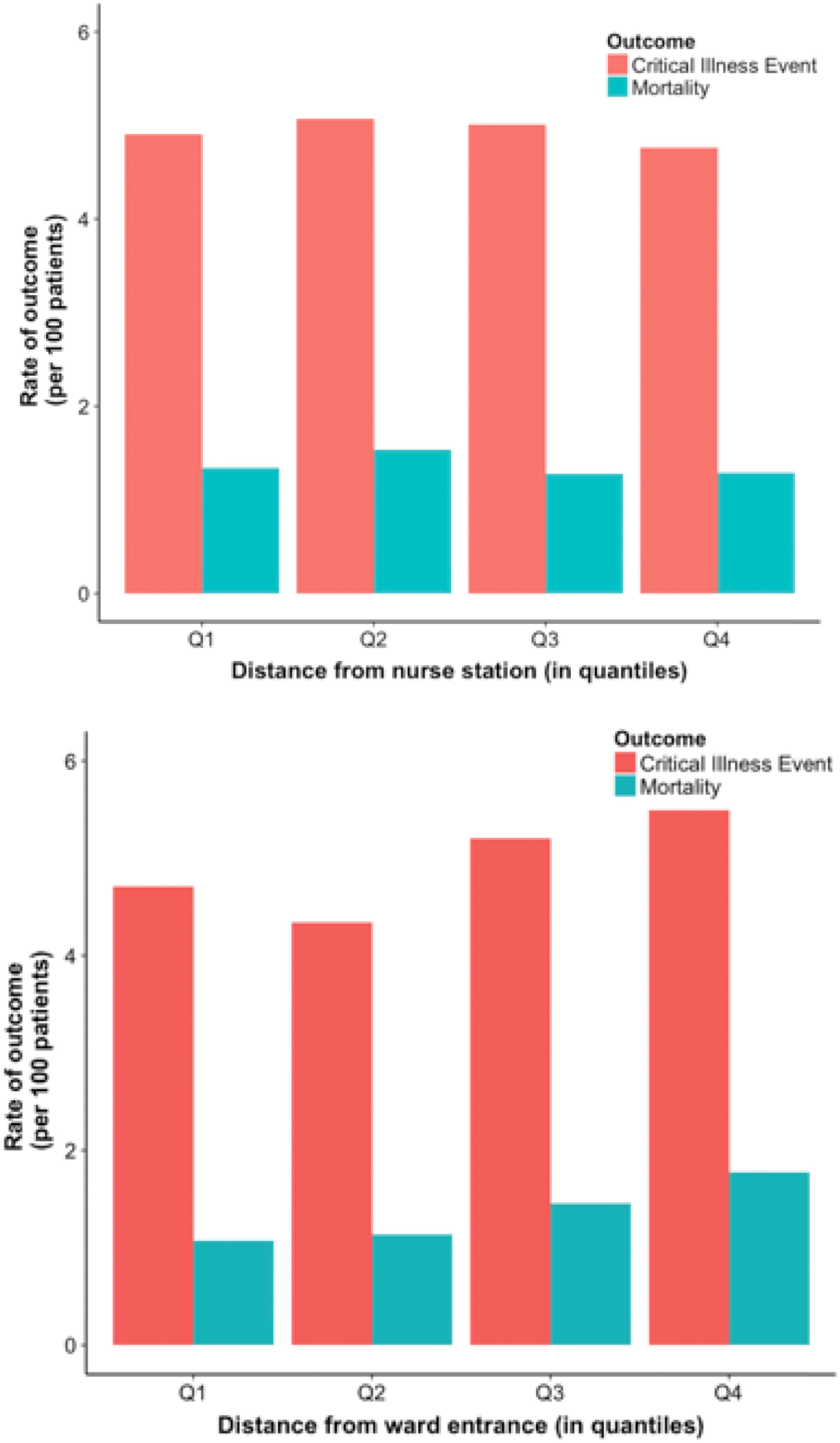
The association between patient outcome and patient admission location within a ward. Figure depicts the proportion of patients with outcome (critical illness event or mortality) per 100 patients in relation to distance from (a) nurse station and (b) ward entrance (distance expressed in increasing quartiles from Q1 to Q4) within a ward.
Adjusted Analysis of Patient Location at Admit and Outcome
The odds ratios (ORs) and 95% confidence intervals (CIs) for the fully adjusted models are shown in Table 3. Patients admitted farther away from the nurse’s station were at similar risks of critical illness events, mortality, and higher-than-median LOS compared to patients admitted closer to the nurse’s station in the fully adjusted model (p > .05 for all analyses). Patients admitted to greater than the median distance from ward entrance had an increased risk of critical illness event (OR = 1.15; 95% CI [1.08, 1.23]) and increased risk of mortality (OR = 1.16; 95% CI [1.02, 1.33]), as compared to patients admitted closer to the ward entrance. Finally, patients admitted to the end of the ward had increased LOS compared to patients admitted closer to the ward entrance (β coefficient for LOS = 13 hr; 95% CI [10, 15]). After removing patients in isolation rooms—which are mostly located at the end of the ward—the association was preserved (OR for critical illness event = 1.15, 95% CI [1.07, 1.23]; OR for mortality = 1.16, 95% CI [1.01, 1.33]; and β coefficient for LOS = 13 hr, 95% CI [10, 14]). No dependence on the exact ward, medical versus surgical wards, or year was observed (data not shown). Additionally, a sensitivity analysis utilizing only patients who stayed at least 48 hr in the same room revealed similar increased LOS for patients admitted farther from the ward entrance as compared to patients admitted closer to the ward entrance (OR for critical illness event = 1.14, 95% CI [1.06, 1.23]; OR for mortality = 1.20, 95% CI [1.03, 1.38]; and β coefficient for LOS = 12 hr, 95% CI [10, 15]).
The Associations Between Proximity to the Nurse’s Station and Ward Entrance at Patient Admission and Outcomes.
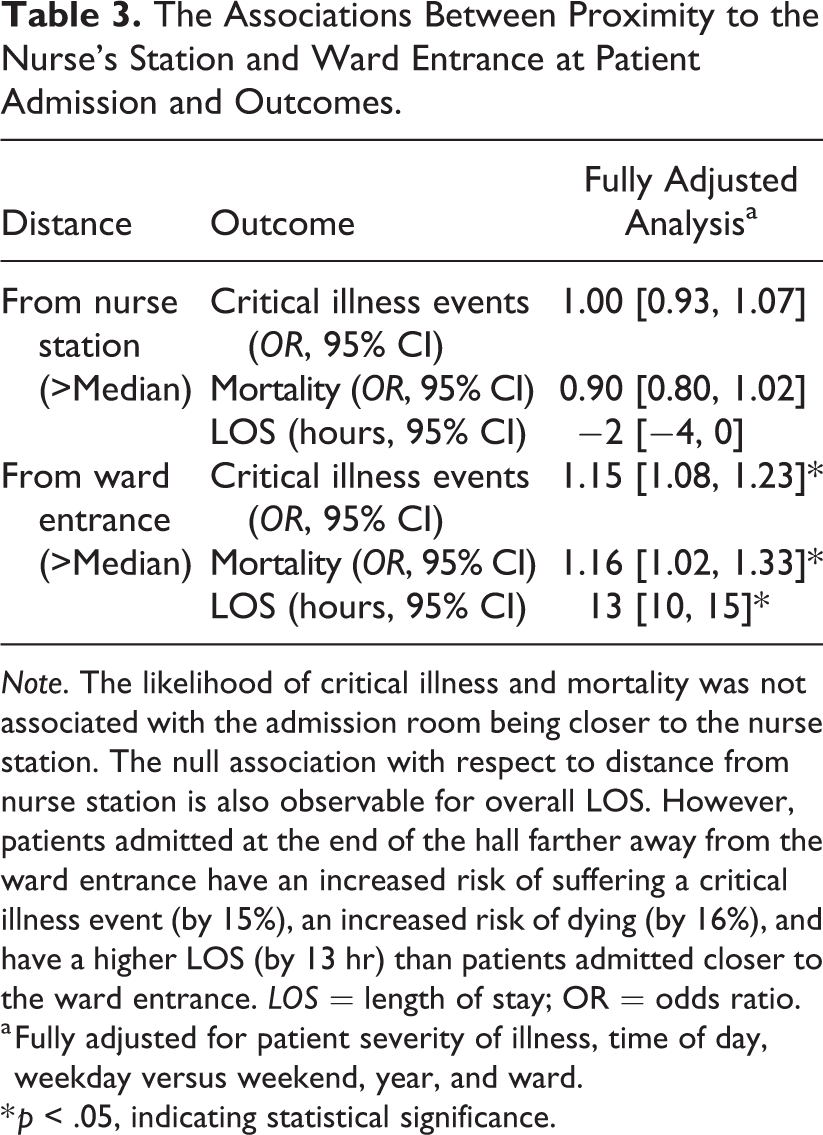
Note. The likelihood of critical illness and mortality was not associated with the admission room being closer to the nurse station. The null association with respect to distance from nurse station is also observable for overall LOS. However, patients admitted at the end of the hall farther away from the ward entrance have an increased risk of suffering a critical illness event (by 15%), an increased risk of dying (by 16%), and have a higher LOS (by 13 hr) than patients admitted closer to the ward entrance. LOS = length of stay; OR = odds ratio.
a Fully adjusted for patient severity of illness, time of day, weekday versus weekend, year, and ward.
* p < .05, indicating statistical significance.
Discussion
In this observational study of more than 80,000 patient admissions, we found that there was no association between proximity to nurse’s station at the time of admission and risk of patient developing critical illness, dying, or experiencing increased LOS. However, we found that patients admitted distal from the ward entrance increases the patient’s risk of developing critical illness by 15%, inhospital mortality by 16%, and overall LOS by 13 hr compared to patients admitted proximal to the ward entrance, after adjusting for potential confounders. These results have important implications for the design of wards and patient monitoring, and they suggest that patients located in rooms farther from the ward entrance are at higher risk of delays in care and hospital discharge.
Previous studies have established that the design and architecture of specific medical care facilities can influence quality of care as well as certain outcomes (Leaf et al., 2010). For example, improving ICU design to better facilitate care access has led to decreased incidence of patient falls (Hendrich, Fay, & Sorrells, 2004) and increased patient satisfaction and care (Lu & Zimring, 2011; O’Connor et al., 2012). On the other hand, in a study by Pettit, Wood, Lieber, and O’Mara, (2014), no relationship was found between low visibility and mortality in a population of trauma patients in the ICU, after adjusting for patient acuity. In recent work on a sample of 24 nursing units from three acute care hospitals, Brewer, Carley, Benham-Hutchins, Effken, and Reminga (2018) reported that nursing unit shape and design can lead to increased falls, possibly from architectural design impeding visual and aural monitoring. Within an emergency-department (ED) setting, it has been noted that patients in rooms with doors had a longer wait time to initial assessment than patient in rooms without doors (Hall, Kyriacou, Handler, & Adams, 2008). Studies have also established that patients in isolation rooms have increased risk of adverse events and outcomes (Abad et al., 2010; Stelfox et al., 2003). Some evidence also exists between improved patient room layouts and better care (Chaudhury, Mahmood, & Valente, 2009). However, these studies are constrained by the specific locations (ICU, ED, etc.) and specialized rooms (such as isolation rooms) and are not generalizable across different patient population characteristics with varying levels of severity of illness. Our study adds to this literature by investigating the association between several patient outcomes and distance between admission location and two major points on the ward, namely, the nurse’s station and the ward entrance, in a large-scale hospital setting with a diverse and complex patient population.
Our finding that the distance from the nurse’s station had no appreciable association with patient outcomes has several potential explanations. First, nurses were utilizing mobile computer carts during the study period. This may have resulted in nurses spending more of their time outside their respective patients’ rooms, thereby mitigating the effect of distance from the nurse’s station on outcomes. Second, the design of the wards at the hospital is such that the nurse’s station (located in the center of the ward) does not have direct visibility to any of the rooms on the wards. It may be that a direct line of sight is needed to yield any beneficial effect from patient proximity to the nurse’s station. Finally, there may be other nursing rounding practices or environmental design aspects that may have mitigated the effect of nurse’s station location on outcomes that were not investigated in this study. These results challenge the conventional wisdom that placing patients closer to the nurse’s station will result in improved outcomes.
While nurse’s station location did not impact patient outcomes, the increase in risk of the development of critical illness along with mortality and the increase in LOS for patients farthest from the ward entrance suggest that these patients may experience decreased attention and delays in care that lead to worse outcomes. Since proximity to ward entrance does not improve access to supplies, or view to the nurse’s station, it is suspected that there might be a workflow issue driving this result that would need to be evaluated with future time in motion studies. For example, decreased traffic to these rooms during rounding by the medical team or consults may result in systematic delays in placing diagnostic or medication orders on a daily basis, thereby contributing to increased overall LOS. To put the half-day increase in LOS experienced by patients admitted away from the ward entrance in context, it is estimated that a half-day reduction in LOS among pneumonia patients is associated with reduction in hospital costs of over US$1,000 per hospitalization (Raut et al., 2009). Extrapolating across the nation would result in an increase in costs of roughly US$500–US$900 million in a single year (Raut et al., 2009). Thus, our findings in the context of LOS are both statistically and clinically significant. If our findings were replicated in other settings, this would suggest that efforts to mitigate the detrimental effects of admitting patients at the far end of the wards would have significant potential cost savings.
Although our results cannot prove causality, they suggest that further investigation of mechanisms and efforts to demonstrate effective mitigation strategies are necessary. These efforts could include maximizing nursing presence on the far end of the wards, special attention to these patients during consults or planning for discharge, and consideration of a lower threshold for review by a rapid response team when these patients show early signs of deterioration. Efforts to reduce systematic delays in care such as rotating the order in which patients are seen during daily rounds should also be considered. Future work is needed to determine what aspects of care are driving the increased LOS and what interventions may improve outcomes for these patients.
There are several limitations to our study. First, this study was performed at a single academic medical center, so our results may not be generalizable to other hospitals with different ward structures and design. Second, while our primary aim was to understand the impact of location at admission, several room transfers may have occurred during a patient’s stay eventually contributing to their outcome. However, our sensitivity analysis that included only patients who stayed in the same room for at least 2 days found similar results to the main analysis. Finally, other environmental factors, such as location of automated medication dispensing systems or supply rooms or the location of other patients assigned to nurses’ care, all of which were not included in this study, may impact nurse movement and patient outcomes.
Conclusions
In conclusion, in this hospital where the nurse’s station does not provide visibility and the ward entrance is at the end of double rows of linear patient rooms, the location of a patient at admission in relation to the nurse’s station did not impact their outcome. However, we discovered a clinically and statistically significant result in that patients admitted to rooms located farther away from the entrance of the ward tend to have increased risk of adverse outcomes as well as increased duration of hospital stay, thereby posing implications for patient outcomes, hospital throughput, and revenue. Recognition of this additional risk factor could improve quality of care, hospital operations, and workflows for reducing cost.
Implications for Practice
Recognizing that patients at the end of the ward are at risk of lapses in care–attention may improve their outcomes. Hospitals looking for areas of quality improvement within patient-centered care metrics such LOS could increase nursing presence for patients located at the end of the ward. Special attention to patients at the end of the ward must also be given during periods of consult, rounding, or discharge. Rapid response teams might consider adjusting the threshold for activation based on patient location.
Supplemental Material
Supplementary_Figure - Association Between Room Location and Adverse Outcomes in Hospitalized Patients
Supplementary_Figure for Association Between Room Location and Adverse Outcomes in Hospitalized Patients by Anoop Mayampurath, Christopher Ward, John Fahrenbach, Cynthia LaFond, Michael Howell and Matthew M. Churpek in HERD: Health Environments Research & Design Journal
Footnotes
Authors' Note
Drs. Mayampurath and Churpek are supported by a career development award from the National Heart, Lung, and Blood Institute, K12 HL 119995-05 and K08 HL121080, respectively. Dr. Churpek has a patent pending (ARCD. P0535US.P2) for risk stratification algorithms for hospitalized patients.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Mayampurath is supported by a career development award from the National Heart, Lung, and Blood Institute (K12 HL 119995-05). Dr. Churpek is supported by a career development award from the National Heart, Lung, and Blood Institute (K08 HL121080). Dr. Churpek have a patent pending (ARCD. P0535US.P2) for risk stratification algorithms for hospitalized patients.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.