
Abstract
Purpose:
The purpose of this article was to investigate and report the implementation of evidence-based design (EBD) principles relating to user controls into hospital renovation projects.
Background:
Progress requires the application of the most recent knowledge and technology. When it comes to the design and construction of healthcare facilities, the latest knowledge comes in the form of EBD research. EBD is the process of basing decisions about the built environment on credible research to achieve the best possible outcomes. The desired outcomes of EBD recommendations include improvements to enhance user control. User control factors include the individual control over bed position, air temperature, lights, sound, and natural light.
Method:
A list of recommendations from existing EBD literature related to user controls was compiled. Construction documents from 30 recent healthcare facility renovation projects across the United States were obtained and analyzed. Implementation levels for the EBD categories of user controls were reported.
Results:
The findings indicate relatively extensive industry use of EBD principles relating to user control of temperature, lights, and natural lighting.
Conclusions:
The findings indicate that EBD recommendations related to user controls are being adopted in practice at consistently high levels. These findings also reveal that there are still areas of potential improvement which could inform those who influence or determine building design, codes, standards, and guidelines. The results are helpful to owners, designers, and contractors by providing a glimpse into how well the industry is recognizing and implementing known best practices. The findings likewise introduce new opportunities for further research which could lead to additional improvement in the healthcare facilities of the future.
Keywords
Progress comes as a result of taking the ever-advancing knowledge and technology available, and putting it to good use (Whitaker, 2018). This is certainly true when it comes to healthcare facilities. Over the years, hospitals and clinics have been able to deliver care with increasingly better outcomes (Radley et al., 2018). In order to continue to achieve improvements in patient care, it is important to constantly evaluate current means and methods. One element that influences the delivery of care is the design and construction of healthcare facilities themselves. Design factors have been shown to both positively and negatively effect healing (DuBose et al., 2018). The practice of researching, evaluating, and incorporating the most effective strategies in healthcare facility design and construction is known as evidence-based design (EBD). EBD uses a scientific approach to connect design elements to healing outcomes. The question is to what extent and to what consistency are EBD principles being put to use in healthcare construction projects today? This report focuses on the EBD principle of enhancing user controls to determine the level of adoption into modern hospital renovation projects. The EBD principles focused on user controls result in improved environmental variables that can reduce stress and improve wellness. These factors include user controls over bed position, air temperature, lights, sound, and natural light (Huisman, 2012).
EBD as defined by The Center for Health Design (CHD, 2016, 2017 and 2018) is the process of basing decisions about the built environment on credible research to achieve the best possible outcomes. Research focusing on how the design of healthcare facilities could influence patient healing and medical staff performance has been ongoing since the 1980s (Alfonsi, 2014). While a review of the literature reveals many studies related to EBD for healthcare facilities, there is a gap in the literature pertaining to the implementation of EBD recommendations in practice.
The question remains whether or not, or to what extent, EBD recommendations for enhancing user controls are being put to use by the design and construction community for healthcare facilities. The intent of this article is to determine whether or not renovated hospitals are implementing the design elements relating to user controls that are known to improve healing and comfort for patients as well as to improve performance and satisfaction for medical staff.
The EBD recommendations studied in this research include design recommendations for enhancing user controls. Users may include hospital administration or staff, patients, or visitors. For the purpose of defining enhancements to user controls for this research, enhancements were analyzed for improved patient control of five control categories identified by EBD literature: control over bed position, control over air temperature, control over lights, control over sound, and control over natural lighting.
Due to the variety of variables which influence hospital design, including local building code jurisdictions, design firms, owners, and the existing facilities themselves, much can stand between EBD research and their inclusion in actual construction documents. An analysis of final construction documents for hospital renovation projects from various locations, design firms, and owners is a straightforward way to discover an answer to this question: To what extent and to what consistency are EBD principles relating to user controls being put to use in healthcare construction projects today? The results of this study will be instructive to owners, designers, and contractors by providing insight into how well the industry is recognizing and implementing these known best practices. The findings likewise open up new opportunities for further research which could lead to additional improvement in healthcare facilities of the future.
Literature Review
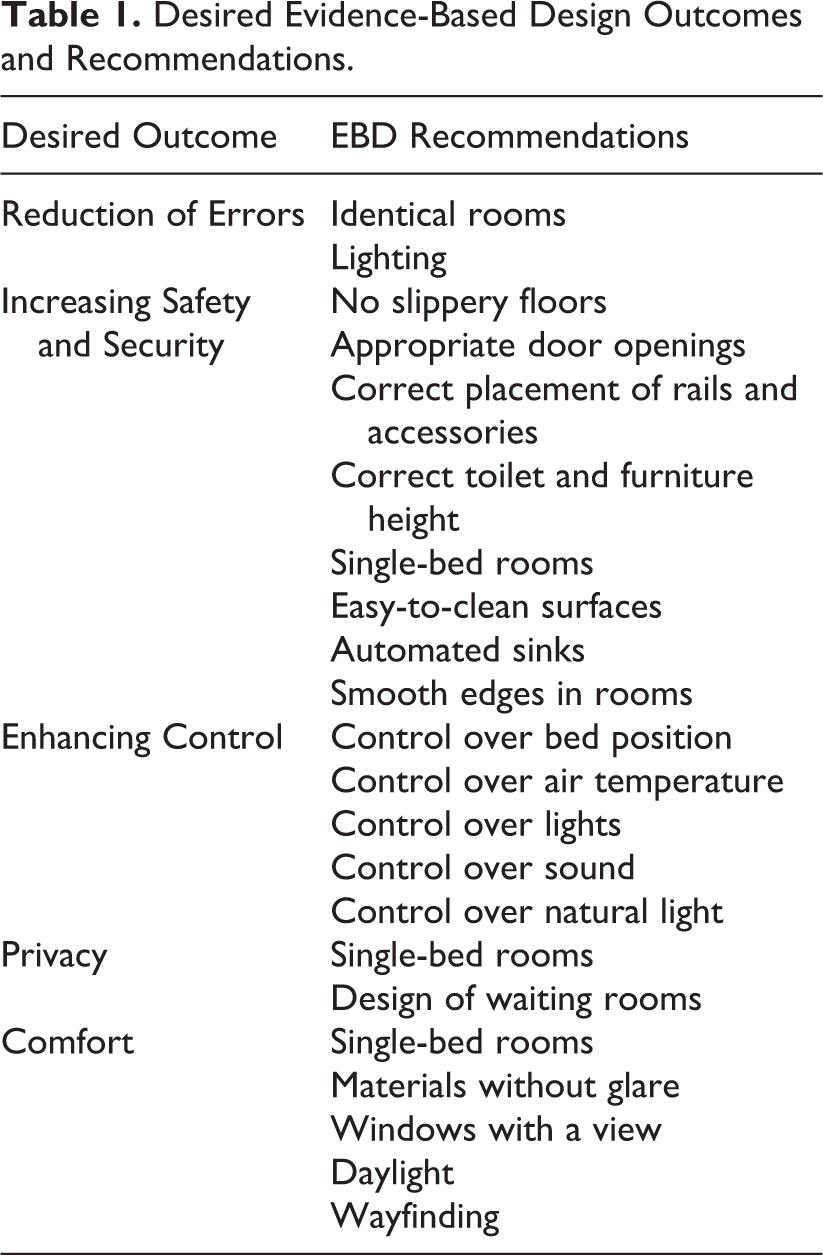
The body of knowledge supporting EBD principles is evidenced by significant, systematic reviews of research. Dijkstra (2006) and Huisman (2012) provide substantial evidence to merit industry adoption and standardization of EBD principles. The Huisman recommendations, which are both more comprehensive and more recent, are the primary background used for this research. The list of EBD recommendations from the Huisman study are shown in Table 1, organized by the desired outcome each recommendation seeks to achieve.
Desired Evidence-Based Design Outcomes and Recommendations.
Enhancing Control
Hospital patients recovering from illness or injury are under significantly more stress than usual (Bieliauskas, 2019). First, the patient is dealing with the stress associated with the illness or injury itself as well as the recovery process. On top of that, there is additional stress related to not being at home and in a normal, familiar environment (Ulrich, 1984). In healthcare contexts, lack of user of control is a pervasive problem that increases stress and adversely affects wellness (Ulrich, 2001). Patients’ sense of control can be markedly reduced by health facilities that are often, for instance, noisy, confusing from the standpoint of wayfinding, invade privacy, and prevent personal control over lighting and temperature (Andrade & Devlin, 2015 ; Ulrich, 1991). Giving patients control over the following environmental variables reduces stress and improves wellness: bed position, air temperature, lights, sound, and natural light (Huisman, 2012). Enhancing control, in other words giving a patient choice, has been shown to reduce stress (Steptoe & Appels, 1989). It gives a user a feeling of control over circumstances and improves the healing environment (Winkel & Holahan, 1985).
There is little to no literature that identifies if the user control elements are being implemented in hospital design. One aim of this study is to fill the gap in the literature by conducting an analysis of EBD use in recently designed healthcare renovation projects with respect to designs related to improving user controls. An understanding of how well the EBD recommendations related to user control are being implemented in hospital renovation projects today will be valuable in the ongoing effort to make progress toward improving healthcare.
Method
Progress requires the application of the most recent knowledge and technology. When it comes to the design and construction of healthcare facilities, one contribution to knowledge comes in the form of EBD research. While extensive EBD research has been published, few studies have been done to verify that these practices are being implemented in hospital remodel projects. An analysis of final construction documents for hospital renovation projects from various locations, design firms, and owners was a straightforward way to discover and answer research questions. Final construction documents represent the project as it was built, other construction documents do exist that provide different levels of design that may or may not have been implemented into the final product. The design and construction documents used for analysis are referred to in the engineering, design, and construction industry as “as-built” drawings. They are drawn after construction of a particular space to show what was actually put in place during construction.
The analysis of construction documents to verify the implementation of EBD user control principles provided a perspective second only to actual site visits to completed projects. With the large sample size of projects, analysis of design documents provided a feasible method to study many recent healthcare renovation projects across the United States, without having to travel to the facilities themselves. The results of this research relied upon the assumption that the EBD recommendations found in the as-built construction documents were unchanged through project completion and were utilized in the completed operational facilities. The analysis of construction documents provided evidence of the degree to which the latest healthcare research has influenced the healthcare design and construction community.
Selecting EBD Recommendations to Study
At the outset, this study aimed to verify the entire list of EBD recommendations in the Huisman study as listed in Table 1. Unfortunately, construction documents do not consistently contain all of the information needed to do a complete analysis. For example, construction documents do not generally contain information related to the patient beds. Consequently, without a physical visit to each facility, it was not possible to find out to what degree patients have control over their bed position. Other limitations relating to not having information on the equipment installed also let to limits on the type of analysis that could be performed.
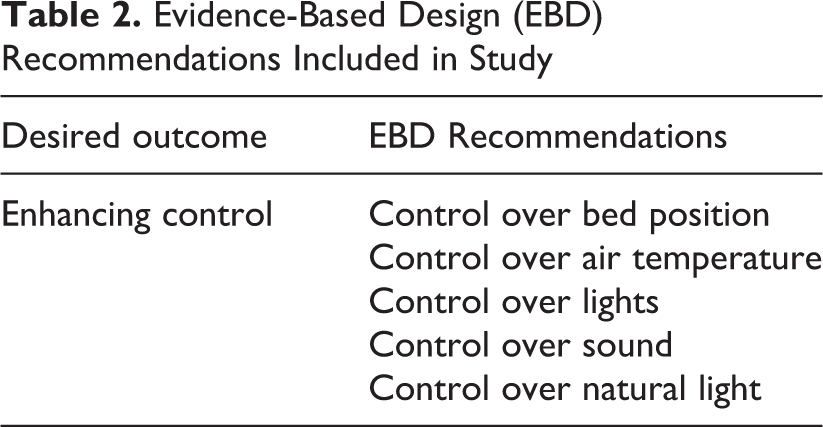
A list of each user control EBD recommendation provided by Huisman is shown in Table 2, with the recommendations in bold representing those which were able to be analyzed by using construction documents. A description of the methodology used to analyze each recommendation follows.
Evidence-Based Design (EBD) Recommendations Included in Study
To perform a proper analysis of whether or not EBD relating to user controls were implemented in practice, a review of construction documents for healthcare facility renovation projects was required. Construction documents for 30 projects were obtained from the archives of a general contracting firm. This firm is among the top 10 largest healthcare contractors in the United States as ranked by Modern Healthcare. It is also ranked in the 2017 Engineering News Record top 100 list of general contractors. This general contracting firm was selected due to the large variety of data contained in the archives, which is due to its large national footprint of operations.
Inasmuch as the articles in the Huisman paper were published between 1984 and 2011, the construction documents obtained for the purpose of this article were limited to those archived by the general contractor from 2012 to 2018 (Huisman, 2012). Care was taken to ensure the data set included diversity among healthcare organization, design team, project location, and project type to ensure that the results are not influenced by any one of those factors in particular. The data includes 30 renovation projects. Of the 30 projects for which construction documents were obtained for analysis, there exists diversity among many factors that were analyzed to determine their influence on the findings. No significant outliers were identified in the data.
Data Analysis Methods
With as-built drawings identified and collected, the next step was to determine how the user control EBD recommendation could be analyzed. The greatest challenge to determining if EBD principles relating to user controls were used is that the literature defining user controls does not specify what is considered an enhancement to user controls. The researchers had to define the enhancement using the broad definition of self-supporting systems, such as control over the position of the bed, control over the temperature (air conditioning and heating), control over the lights (including dimmers), control over the sound (music and television), and control over the natural light (Huisman, 2012). The criteria for deciding if user control was enhanced is given for each category in this section. Most of the EBD user control recommendations selected for analysis were related in some way to the patient rooms of the facilities. The first action taken with each set of construction drawings was a thorough floor plan review to quantify patient rooms or bed locations and to organize by type. Once room counts were established, the user control EBD recommendations were evaluated. After all of the documents were analyzed for the identified EBD recommendations, the results were tabulated and conclusions were drawn.
User control was studied for control of the position of bed, control over the temperature, control over lights, control over sound, and control over natural lighting. Bed specifications were not provided in the as-built construction documents, and therefore, this recommendation could not be verified thoroughly in this study. Control over bed position was seen as the user ability to control or adjust the bed to comfort. In terms of bed location in the room, all the plans showed this as a fixed place with no user control. The authors do note that all patient room headwalls featured electrical outlets which could be used to power a patient bed with the recommended features. Enhanced user control for air temperature was defined as a user’s ability to control room temperature within the room. The mechanical plans and specifications were analyzed to determine whether or not a thermostat was placed within each patient room or not. Patient rooms containing a dedicated thermostat were determined to follow the EBD recommendation of giving patients control over air temperature. An example of plans showing user control of temperature is given in the as-built drawing of four patient rooms shown in Figure 1. Each room in the figure has its’ own thermostat near the entrance (shown in the drawing as a circle with the letter “T” inside), allowing each patient to adjust the temperature to meet their individual preferences without impacting others.
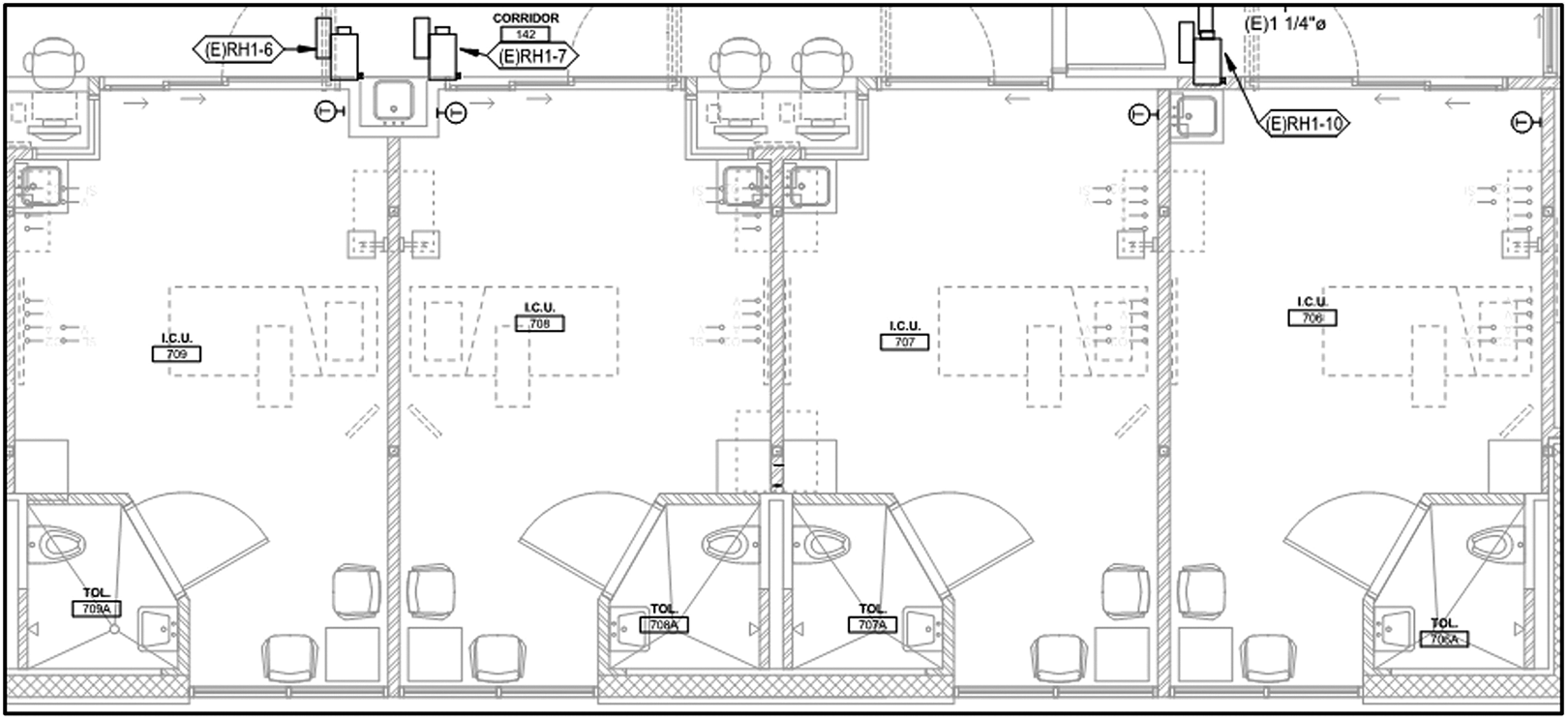
Patient rooms with individual thermostats.
To determine whether patients had control over their room lighting, the electrical plans were checked for light switches within the patient room either near the bed location or at the room entrance. The patient room in Figure 2 features a light switch at the head of the patient bed which controls the light fixture overhead (indicated in the drawing with the letter
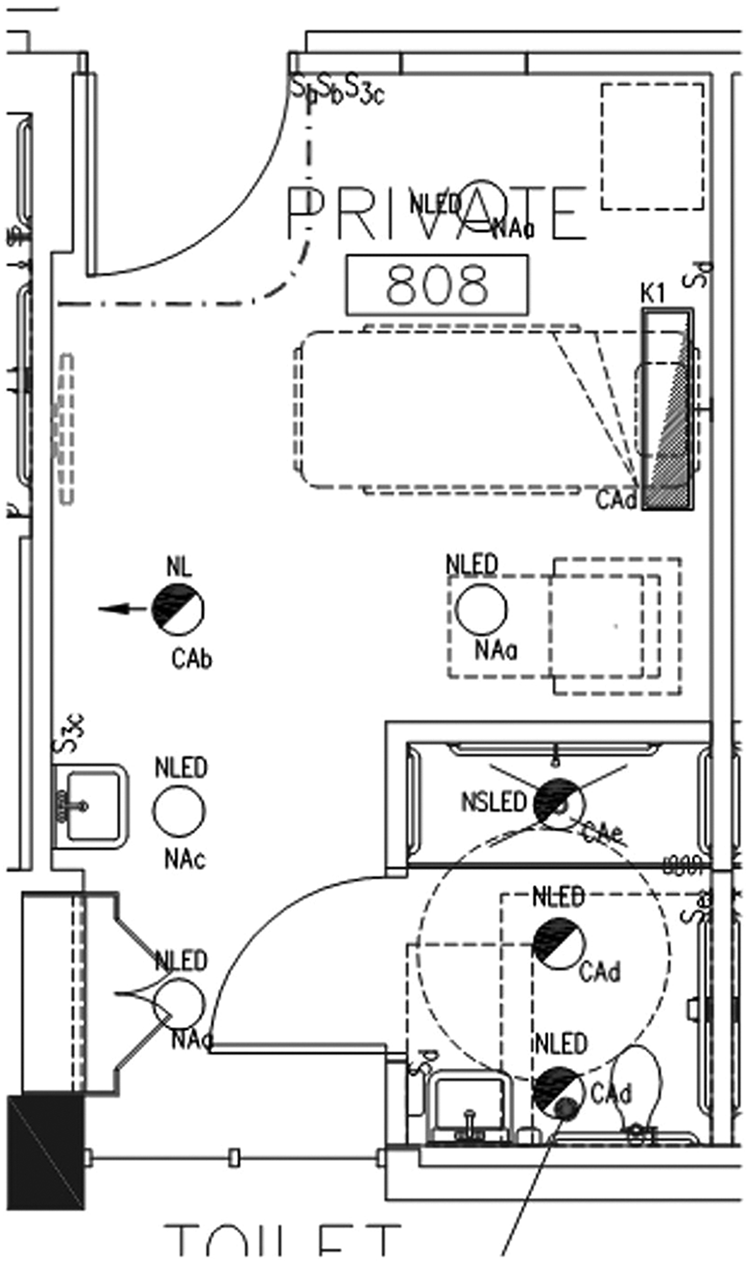
Patient room with light control near the bed.
For the recommendation of control over sound, the Huisman study referenced control over music and television (Huisman, 2012). These features are not typically shown in construction documents, so this element was not included in this analysis. Traditionally, these types of controls are integrated into the bed. All drawings showed this capability. The construction drawings were checked for window coverings to determine compliance to control over natural light. If window coverings that could be controlled by a patient were specified, it was determined that this recommendation was satisfied. For example, Figure 3 shows that Keynote 26 calls for window coverings in the patient rooms.
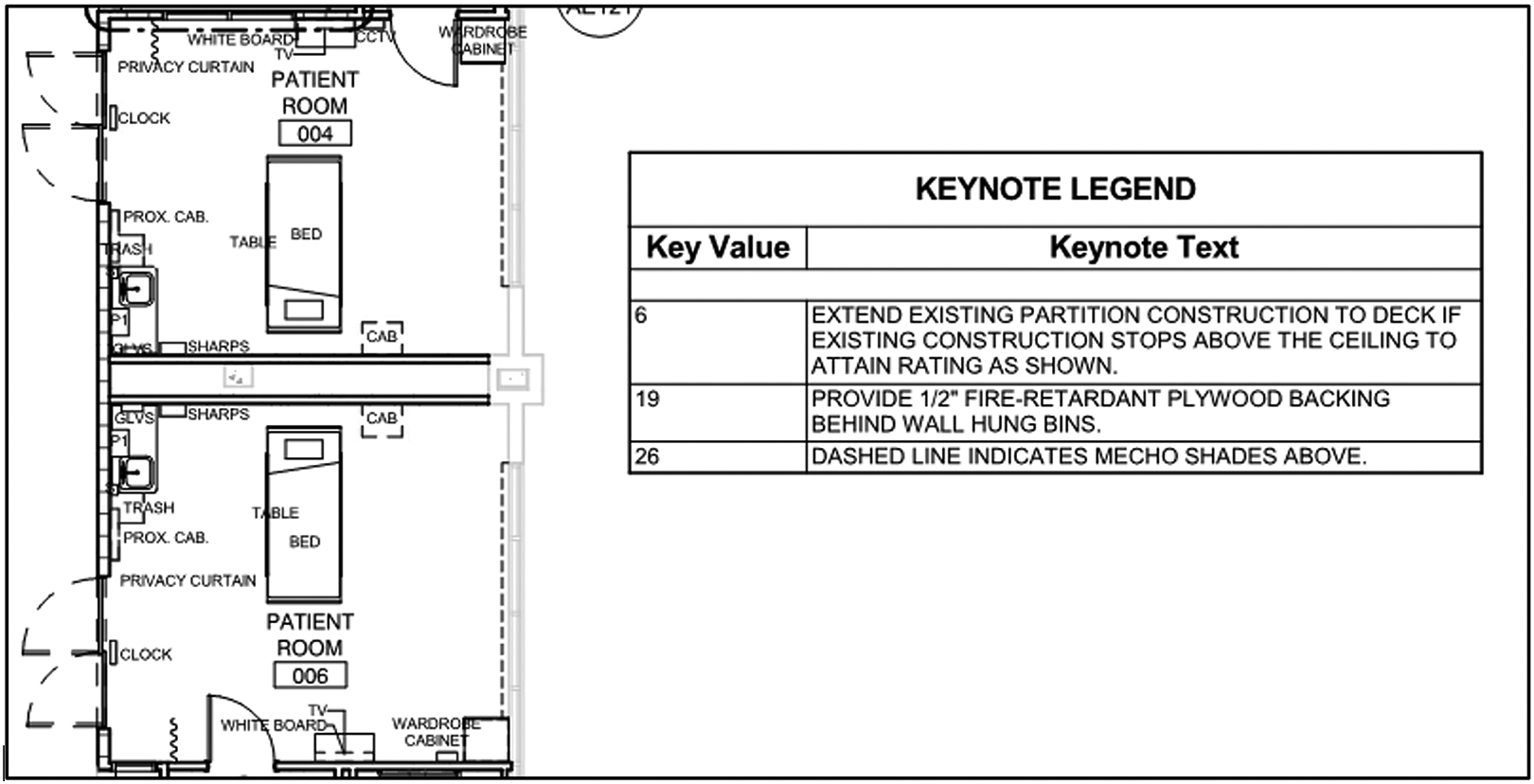
Patient rooms featuring window coverings.
In summary, the construction documents for 30 recent hospital renovation projects were obtained and analyzed. Key project information was compiled for the purpose of sorting the results once the analysis was complete. Each EBD recommendation relating to user controls which could be found within the documents was noted and tabulated. After the analysis was complete and all of the information was organized, it was then possible to sort the data in order to extract the findings, observe patterns and trends, and draw conclusions.
Findings
At the outset, it was stated that the purpose of this research was to determine to what extent and to what consistency proven EBD principles related to user controls are being put to use in healthcare facility renovation projects today. In order to best show this, the findings will first be presented in a manner to show the extent of industry adoption. Next, the same results will be presented in a format which best articulates the consistency of EBD utilization. To best understand extent, the results were tabulated by each of the EBD recommendations used for analysis. The extent of industry adoption was manifest by how many of the projects in the analysis included the recommendation in the design. The higher the adoption rate of any given recommendation among all projects, the greater the extent.
To best understand consistency, the results were compiled by each of the projects analyzed. The consistency of industry adoption was apparent by how many of the EBD user control recommendations chosen for analysis were included in the design of each project. A project exhibited greater consistency when most, if not all, EBD principles were found in the design. Low consistency was evident in projects which featured only a few EBD user control recommendations.
In response to the research question posed, the use of EBD recommendations relating to user controls were found to be fairly extensive. Table 3 contains the data that show the extent to which the design and construction industry has adopted each EBD recommendation from the Huisman paper selected for analysis in this study. The data show that all recommendations have been adopted by the industry at some level and were detected in most of the plans analyzed.
Extent of Evidence-Based Design Implementation.
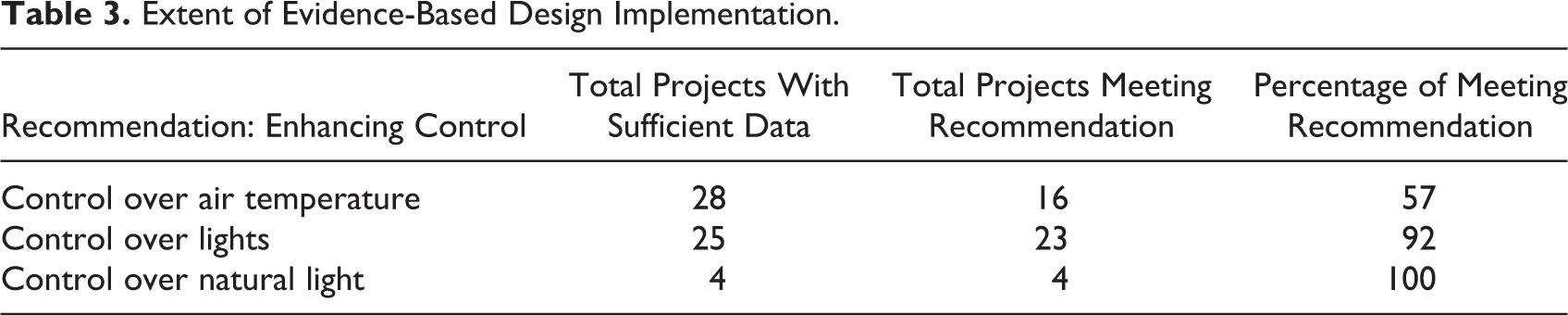
The findings indicate fairly extensive industry use of EBD principles relating to user controls. For the EBD principle of control over lights 23 of 25 renovation designs or 92% adopted the design recommendations. For control over natural light, designs changes were found in all projects. The EBD principle with the least amount of adoption was the control over temperature. This was implemented in the design for only 16 of 28 projects or 57%.
In response to the question this study set forth to answer, the consistency of EBD use is relatively high overall, with moderate adoption of user controls of temperature. The data collected for this study, when sorted, could possibly provide an explanation as to what factors most contribute to the findings. Some notable results were tabulated and are shown in Table 4. Of the states where the projects were located, two states, California and Utah, had enough variety of projects to perform further analysis of the findings. When the eight projects located in California were sorted, the average EBD implementation rate is 83%, which is close to the overall average of 81%. The eight projects located in Utah had an average EBD inclusion rate of 82%, also very close to the overall average. All other states contained either one or two projects, which was not enough information to detect any trends. The project location did not play a significant factor in how consistently EBD principles were utilized.
Project Variables and Evidence-Based Design User Control Implementation.
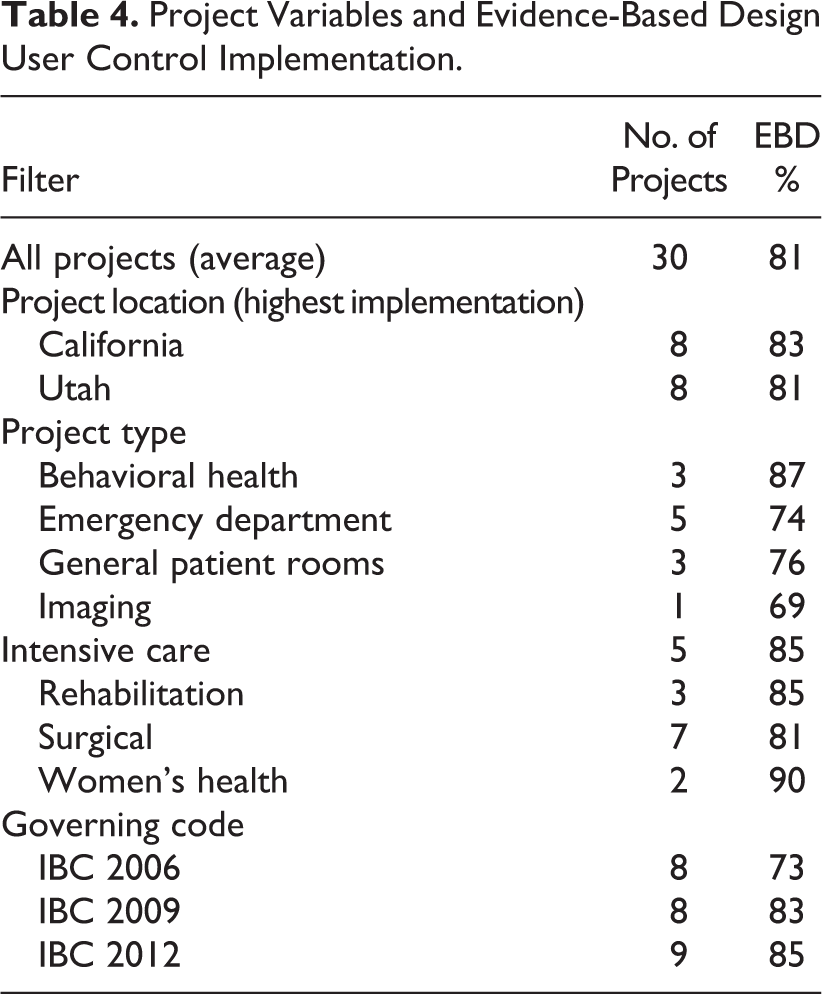
Project type is another potential variable which could influence the findings. When sorted by project type, the EBD implementation rates ranged from a high (90%) to a low (69%), relatively close to the overall average of 81%. Four project types scored above the average: women’s health (two projects averaging 90%), behavioral health (three projects averaging 87%), intensive care (five projects averaging 85%), and rehabilitation (three projects averaging 85%). It is possible that facilities that provide this type of care place a higher emphasis on improved patient outcomes and experience. Further research would be required to determine that for sure.
An analysis of how the owner possibly impacted the EBD user control results did not reveal any noticeable patterns. The same holds true after sorting the data by architect, mechanical engineering firm, and electrical engineering firm. The large variety of owners and designers represented in this set of data incumbers an analysis of how those variables may influence the results. This fact is advantageous to this study because the wide variety of projects offers a glimpse into what the design and construction industry is doing as a whole.
The analysis of the data collected for this study indicated that EBD recommendations are found extensively and consistently in recent healthcare facility renovation project construction documents. Some recommendations are found in all projects, while others appear in most. Projects implement an average of 81% of the known EBD user control recommendations. Sorting the data by different influencing variables provided additional insight into industry trends.
Conclusions and Recommendations
The purpose of this study was to compare the design of recent healthcare renovation construction projects with fundamental EBD principles relating to user controls to determine whether or not the latest research is being utilized by the healthcare design and construction industry in practice. A comprehensive literature review was conducted in order to determine and compile the latest known EBD recommendations for user controls. Construction documents for recent healthcare facility renovation projects were obtained for analysis. The extent and consistency of compliance with EBD recommendations was documented. The data were sorted and analyzed to extract results and observe patterns. Judging from the results contained herein, it was evident that the EBD recommendations relating to user control related to control over temperature, control over lights, and control over natural lighting are being put into use by the healthcare design and construction community.
The extent and consistency of EBD use today may be an indication that known benefits to healthcare facility users are being realized. The findings in this study reveal that there are areas of potential improvement which could inform those who influence or determine building design, codes, standards, and guidelines. The results are instructive to owners, designers, and contractors, and provide a glimpse into how well the industry is currently recognizing and implementing best practices. These results likewise open up new opportunities for further research which could lead to additional improvement in healthcare facilities of the future.
While the above results are encouraging, and definitive conclusion can be drawn due to the size of the sample obtained for this research, further research into this topic is warranted. Many opportunities exist to expand on this effort. Further research into the EBD recommendations made by Huisman but not included within this study is necessary. More recently designed projects can be analyzed to determine whether or not the design industry has taken note. Studies of construction documents produced pre-2011 (prior to the publication of the Huisman recommendations), pre-2005 (prior to the publication of the Dijkstra study), and pre-1984 (prior to any EBD research) may also shed light on when industry adoption of EBD principles took hold.
The construction documents analyzed for this study came from projects with a variety of owners, designers, and locations; however, the projects were all renovation projects. Research from multiple general contractor sources with still more owner, designer, and location variety could be completed to ensure these results can be replicated. Future research should include new hospitals and other types of healthcare facilities. A study of deferent hospital project types including inpatient versus outpatient could be insightful. Research can also be done to determine whether EBD adoption differs between publicly administered healthcare facilities and privately owned and operated facilities.
Additional research can be conducted to understand find how EBD principles are being adopted into building codes. A thorough analysis of the International Building Code in 2006, 2009, and 2012 may reveal what EBD recommendations, if any, have become the national minimum standard and when those standards were adopted, if at all. An investigation of the differing standards, if any, unique to specific hospitals or specialized care units within hospitals may explain the differing rates of EBD adoption observed among different project types. A better understanding of how facility design standards govern the design and construction of healthcare facilities could also prove to be instructive.
While it is evident from this research that EBD principles have been noticed and implemented in practice, there is still room for improvement. Additional inquiry into the previously mentioned subjects may help uncover some of the challenges or roadblocks which are preventing further improvement.
It should further be noted that EBD principles may also be applicable to industries outside of healthcare and wellness. Further research into how the design of the built environment impacts the well-being of users and occupants in several other areas may prove to be valuable. If changes in design elements can improve healing and satisfaction for hospital patients and users, surely similar outcomes can occur in other sectors of the built environment such as office, institutional, retail, education, government and municipality, religious, and residential.
Furthermore, academic institutions may seek to participate in more EBD research as a means of contributing to the design and construction practices associated with improving the end user experience in all sectors of the built environment. Researchers in the medical field can collaborate with design and construction researchers to find new ways in which designs can help improve patient outcomes. Design and construction researchers can work in partnership with medical researchers to determine how the latest design and building technology can be put to use to improve healthcare environments. In addition, design and construction courses with heavy emphasis in EBD research, whether in healthcare or any other industry, will bridge the gap between the researchers making new discoveries and the future professionals tasked with the ultimate implementation of those findings in practice.
Implications for Practice
The analysis of design and construction documents of hospital renovation projects indicate the level of implementation of Evidence Based Design criteria related to user controls.
EBD principles regarding user controls are widely implemented in current hospital renovation projects; areas of focus for improved implementation have been identified.
Project stakeholders should assess alignment with user-controlled EBD principles to maximize the user experience and improve healing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.