
Abstract
Objective:
The purpose of this study was to translate the Environmental Assessment Tool–Higher Care (EAT-HC) into Japanese and validate its use in small-scale group living facilities in Japan.
Background:
Environment of a facility is shown to improve its residents’ quality of life (QOL). Japan’s “welfare-based nursing homes for the elderly” are gradually shifting to a small-scale group living concept called group care units (GCUs). However, there is no appropriate environmental tool available for evaluating GCUs. The application of valid environmental assessment tools brings about a better understanding of the nature of good environments and the relationship between environments and outcomes for residents living with dementia.
Methods:
The study had a mixed method design conducted in several steps, covering translation and adaptation. The translation phase involved (1) forward translation and (2) backward translation. The adaptation phase involved (3) content validity and homogeneity reliability and (4) concurrent validity and interrater reliability.
Results:
71 Items (92%) met the acceptable level of content validity (item-content validity index [CVI] > .79) and had good scale-CVI of .88. Concurrent validity was confirmed between .65 and .78 (p < .001). For reliability test, the internal consistency of six subscales was between .88 and .98. Overall interobserver agreement was 90.3%. Intraclass correlation coefficients were .80–.98 (p < .001), and homogeneity reliability coefficient for all items was >.76 (p < .01).
Conclusions:
Validation of the EAT-HC-Japanese Version (EAT-HC-JV) was confirmed as an appropriate tool for environmental assessment to enhance the QOL in Japan’s GCUs. For future study, we plan to modify the EAT-HC-JV to adapt to Japanese cultural aspects in order to increase its usability in Japan.
Keywords
Background
Alzheimer’s disease is the sixth leading cause of death worldwide and fifth among adults aged 65–85 (Kochanek et al., 2019). Japan is among the “oldest” countries in the world with one of the highest life expectancies of 81.3 for men and 87.3 years for women (Ministry of Health Labour and Welfare, 2019). Currently, 28.4% of Japan’s population is comprised of people aged 65 and older (Ministry of Internal Affairs and Communications Bureau of Statistics, 2019; Statistics Bureau of Japan, 2019). It is expected that by 2025, one in five people aged 65 or older will suffer from some degree of dementia (Cabinet Office, Government of Japan, 2017). As life expectancy increases in addition to the growing number of older adults with physical and cognitive impairments, residential care homes will be in demand to accommodate the aging population in Japan (Annear et al., 2016).
Japan is one of the three countries (other than Germany and South Korea) in the world with an established universal long-term care (LTC) insurance that provides coverage for older adults aged ≥65 (Rhee et al., 2015). LTC facilities in Japan can be roughly classified into two categories: LTC insurance facilities and private nursing homes. When nursing homes for the elderly began operating in the early 1960s, quality of life (QOL) and physical environment were subjects for improvement. In 2000, the Social Welfare Act (Shakai Fukushi Ho) was revised. This revision created a turning point in the awareness of quality of care and QOL in LTC insurance facilities, including more assistance with activities of daily livings (ADLs) and privacy for the residents and less room sharing (Mori et al., 2012). Although the exact number of residents per small-sized unit for optimal effectiveness has not been determined, placing older adults living with dementia into smaller groups and providing private rooms can reduce overstimulation and support feelings of familiarity (Canham et al., 2017; Fleming & Purandare, 2010; Lee et al., 2016; Morgan et al., 2004).
In 2002, there was a shift to implement a small-scale group living concept, yunitto-gata tokubetsu yogo rojin home, translated as “group care unit” (GCU) approach to one of the LTC insurance facilities called “welfare-based nursing homes for the elderly,” whereas each facility contains several GCUs. The aim of GCUs is to provide a noninstitutionalized feeling with home size space and a homelike atmosphere to enhance privacy, dignity, and QOL of the residents (Ministry of Health Labour and Welfare, 2017b; Mori et al., 2012). A GCU typically houses 9–12 residents. Every GCU resident has a private room, which is mandated to be at minimum 10.65 m2 (114.6 ft2) in size, connected to a communal living/dining area. Each GCU is equipped with a kitchen and a separate entrance (Ministry of Health Labour and Welfare, 2017b). About 40% of the GCU residents are >90 years old, 80% female, >95% have some degree of dementia, and three of the four need assistants with ADLs (Ministry of Health Labour and Welfare, 2017a). Figure 1, drawn by the researcher for this study, shows the examples of floor plan of GCU’s with Tatami area. The aim of GCUs is to provide a noninstitutionalized feeling with home size space and a homelike atmosphere to enhance privacy, dignity, and QOL of the residents (Ministry of Health Labour and Welfare, 2017b; Mori et al., 2012).

Examples of Japanese group care unit’s floor plan with Tatami area.
Powell Lawton (1974), in one of the tenets of ecological change model, posited that “the individual responds to a change applied in the environment,” especially those individuals “at a threshold level of competence” as in the case of older adults living with dementia. By increasing awareness of the impact of physical environment, researchers and LTC administrators can support enhancing QOL of those older adults (Day et al., 2000). Thus, considering the deterioration in functional status associated with advanced stages of dementia, understanding the relationship between physical environment and residents’ behavior is one of the noteworthy aids in LTC (Anderiesen et al., 2014; Chaudhury et al., 2018; Day et al., 2000; Marquardt et al., 2014). Older adults with dementia become sensitive to environment (Chaudhury et al., 2018). As dementia progresses, they tend to find their QOL rooted in their environment (Abrahamson et al., 2012). Creating a homelike atmosphere can help promoting intellectual and emotional well-being, social interaction, as well as reduces agitation, and improves functionality of residents living with dementia. Compared to older adults with dementia residing in traditional LTC facilities, their counterparts in facilities with a homelike atmosphere are reported to be less aggressive, less anxious, and less in need of medication, and have better functioning (Cioffi et al., 2007; Cohen-Mansfield et al., 2010).
While it is shown that the unit environment is important for GCU residents progressing toward advanced dementia (Brennan et al., 2019), there are no appropriate environmental instruments available to evaluate small-scale living facilities. The development and application of valid environmental assessment tools (EATs) brings about a better understanding of the nature of good environments and the relationship between them and good outcomes for residents living with dementia. The availability of easy-to-use EATs facilitates the systematic comparison of one environment with another, contributing to an informed discussion of the strengths and weaknesses of environments and, in appropriate circumstances, laying the foundation for planning the remodeling of poorly performing environments.
Selection of Environmental Instrument for Japan’s GCU
We searched the literature for environmental scales published within the last 20 years. The timing concurs with the expansion of using person-centered concepts in the care of older adults living with dementia. We select environmental instruments that meet the following inclusion criteria: (1) validated scale, (2) used in residential care settings, and (3) focused on residents with dementia. Of the 19 environmental scales found in publications since 2000 (Elf et al., 2017), we selected five that met our inclusion criteria: EAT, Environmental Assessment Tool–High Care (EAT-HC), Environment-Behavior Model for Alzheimer Special Care Units (E-B Model), the Professional Environmental Assessment Protocol (PEAP), and the Therapeutic Environment Screening Survey for Nursing Homes and Residential Care (TESS-NH/RC; see Table 1). Of these five scales, we further eliminated E-B Model that was developed specifically for Alzheimer’s special care unit and EAT for persons living with less mental and physical impairments (Fleming & Bennett, 2015). TESS scales were also eliminated because they were used as supplementals for other scales as TESS do not cover all of the environmental dimensions that left PEAP and EAT-HC. After each question of both PEAP and EAT-HC was considered, we determined that EAT-HC was more appropriate because not only it is user-friendly, but it was also developed specifically for small-scale group living facilities for residents with higher levels of cognitive and/or physical impairments. EAT-HC is easier for the care staff to use in their own facility, while PEAP requires assessment from experts in environment and aging care (Fleming, 2011; Lawton et al., 2000; Norris-Baker et al., 1999). Therefore, EAT-HC was considered the most appropriate instrument for environmental assessment of Japan’s GCUs.
List of Environmental Instruments.
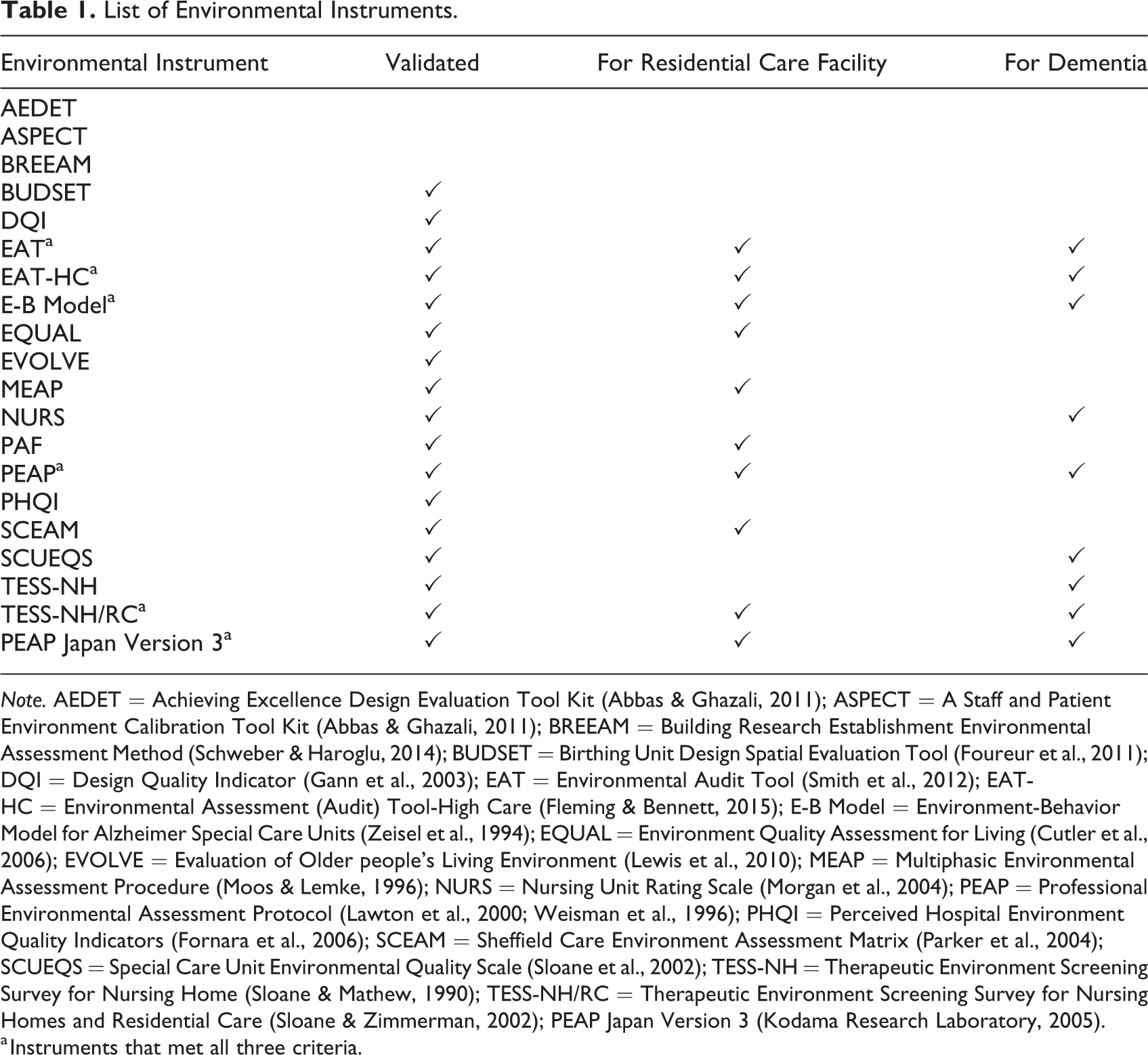
Note. AEDET = Achieving Excellence Design Evaluation Tool Kit (Abbas & Ghazali, 2011); ASPECT = A Staff and Patient Environment Calibration Tool Kit (Abbas & Ghazali, 2011); BREEAM = Building Research Establishment Environmental Assessment Method (Schweber & Haroglu, 2014); BUDSET = Birthing Unit Design Spatial Evaluation Tool (Foureur et al., 2011); DQI = Design Quality Indicator (Gann et al., 2003); EAT = Environmental Audit Tool (Smith et al., 2012); EAT-HC = Environmental Assessment (Audit) Tool-High Care (Fleming & Bennett, 2015); E-B Model = Environment-Behavior Model for Alzheimer Special Care Units (Zeisel et al., 1994); EQUAL = Environment Quality Assessment for Living (Cutler et al., 2006); EVOLVE = Evaluation of Older people’s Living Environment (Lewis et al., 2010); MEAP = Multiphasic Environmental Assessment Procedure (Moos & Lemke, 1996); NURS = Nursing Unit Rating Scale (Morgan et al., 2004); PEAP = Professional Environmental Assessment Protocol (Lawton et al., 2000; Weisman et al., 1996); PHQI = Perceived Hospital Environment Quality Indicators (Fornara et al., 2006); SCEAM = Sheffield Care Environment Assessment Matrix (Parker et al., 2004); SCUEQS = Special Care Unit Environmental Quality Scale (Sloane et al., 2002); TESS-NH = Therapeutic Environment Screening Survey for Nursing Home (Sloane & Mathew, 1990); TESS-NH/RC = Therapeutic Environment Screening Survey for Nursing Homes and Residential Care (Sloane & Zimmerman, 2002); PEAP Japan Version 3 (Kodama Research Laboratory, 2005).
a Instruments that met all three criteria.
EAT-HC
The EAT-HC is a development of the EAT (Fleming, 2011; Fleming et al., 2003) which, in turn, was primarily based on the description of a set of principles used in the design of a number of specialized units for the care of confused and disturbed older adults in Australia (Fleming & Bowless, 1987). Like the TESS-NH (Sloane & Mathew, 1990), which was used as the standard by which the EAT was validated (Fleming, 2011), the development of the EAT and EAT-HC was heavily influenced by the concept of “environmental press” formulated by Lawton and Nahemow (Lawton, 1975; Lawton & Nahemow, 1973). This model postulates that people have individual levels of competence that can be negatively affected by environments that exert more press than the individual can cope with, and the negative consequences increase as the level of competence of the individual decreases as in the case of people living with dementia.
The EAT-HC is a questionnaire containing 77 items with dichotomous scale. EAT-HC handbook that includes the questionnaire and user’s instruction is available for download (Fleming & Bennett, 2017). EAT-HC has 10 key design principles: (1) unobtrusively reduce risks, (2) provide a human scale, (3) allow people to see and be seen, (4) manage levels of stimulation—reduce unhelpful stimulation, (5) manage levels of stimulation—optimize helpful stimulation, (6) support movement and engagement, (7) create a familiar place, (8) provide a variety of places to be alone or with others—in the unit, (9) provide a variety of places to be alone or with others—in the community, and (10) design in response to vision for way of life (Fleming & Bennett, 2017). The total score is the average score of the 10 key design principles.
Therefore, the aims of this study were to (1) translate the EAT-HC into Japanese and (2) test the reliability and validity of this newly translated tool for use in Japan’s GCUs. The following sections describe our process of translation and validation of EAT-HC Japanese version (EAT-HC-JV), results and discussion about the challenges encountered in the process.
Method
The study had a mixed method design, conducted in several steps, covering translation and adaptation. The translation phase involved (1) forward translation and (2) backward translation. The adaptation phase involved (3) content validity and homogeneity reliability and (4) concurrent validity and interrater reliability.
Translation: EAT-HC-JV
EAT-HC was translated into Japanese following an adapted process by the World Health Organization (1998). The process included forward translation, back translation, expert consultation, and adaptation. Forward and back translations were conducted by two authors (S.B. & Y.H.). Because some wordings in EAT-HC are not readily translatable to Japanese, we consulted with three Japanese aging care experts to verify and agree on the choice of words and phrasing in EAT-HC-JV (see Table 2). The modification process between two authors and aging care experts was repeated a few times until we reached a consensus on the wording. After the second back translation, another leading gerontology professor was consulted on the culture and language contexts. Final minor modifications and proofreading were done by the two authors. Finally, the new instrument was ready for psychometric testing.
Wording Modification in EAT-HC-JV.
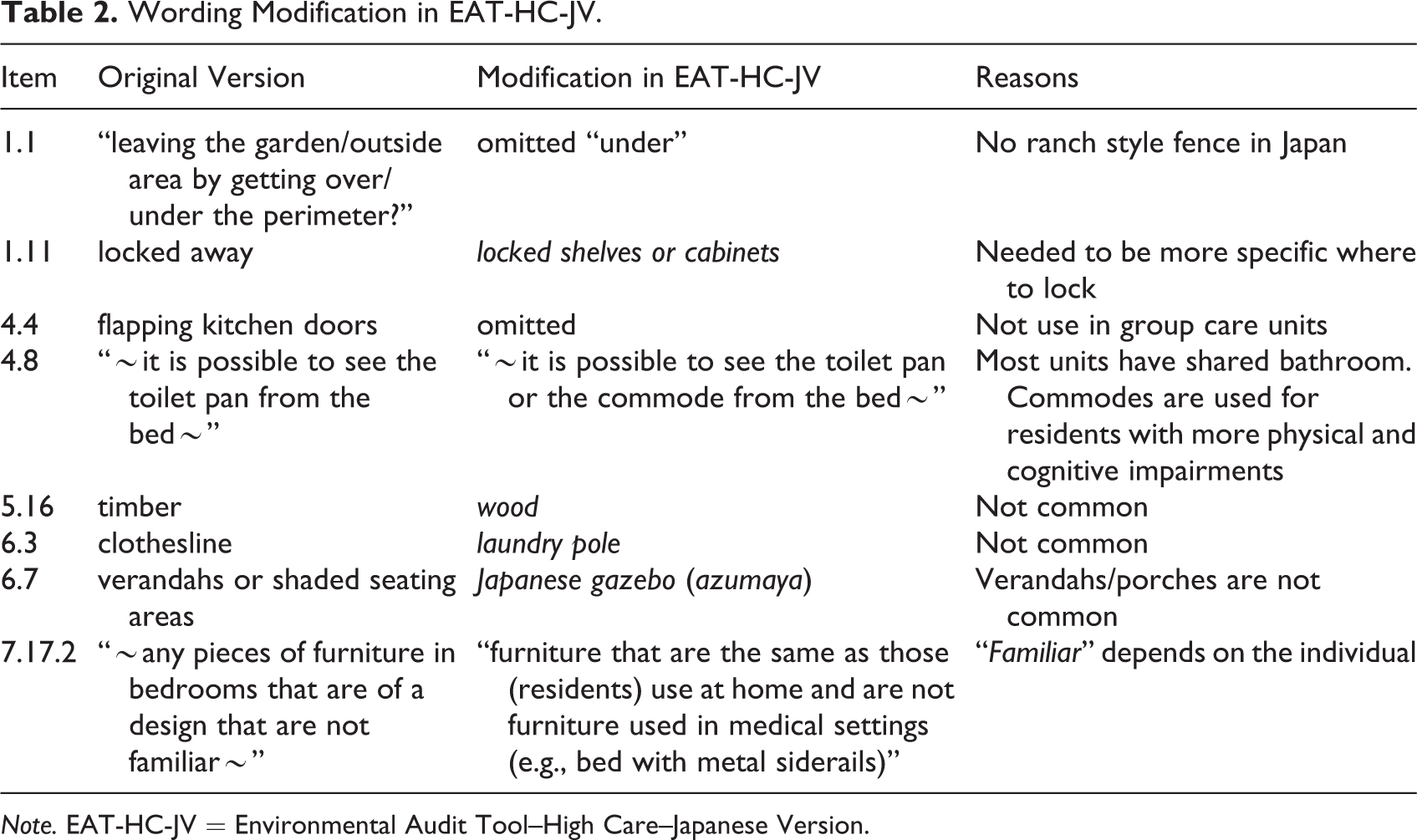
Note. EAT-HC-JV = Environmental Audit Tool–High Care–Japanese Version.
Data Collection
Content validity and homogeneity reliability coefficient
Using purposive sampling, we invited experts with professional and up-to-date knowledge on aging care and LTC facility management from Hokkaido (northernmost island) to Kanto region (eastern part of the main island including Tokyo) to participate. Data collection occurred between May and August 2019. The final sample (n = 12) included four gerontologists and/or senior facility architect and eight chief or facility directors who specialized in dementia care from “welfare-based nursing homes for the elderly.” For the content validity assessment of EAT-HC-JV, participants (n = 12) were asked to determine on a scale of 1–4, where 1 = not at all important and 4 = extremely important, whether each of the 77 items of EAT-HC-JV was appropriate to evaluate GCUs. Participants received the EAT-HC-JV as a word document via email, typed their answers directly into the survey, and emailed the completed survey back to the first author (S.B.). We requested additional comments from participants for any items rated 1 and 2.
Concurrent validity and interrater reliability
The study utilized a convenience sample of 30 GCUs from 11 welfare-based nursing homes for the elderly in the areas around the Kanto region. To be in the study, the GCUs (n = 30) must meet the inclusion criteria of having implemented an assigned unit care staff to residents, and each unit is operating independently. The LTC facilities were two- to four-story buildings, and all GCUs (n = 30) were on the ground to fourth floor. Of the 30 GCUs, three had direct access to outside area, nine had outside area inside the facility, and the rest had no outside area.
Assessment of concurrent validity of EAT-HC-JV occurred between February 2018 and August 2019. Two authors with expertise in gerontology and/or interior design (S.B. & Y.H.) evaluated concurrently and independently each item of the following scales: PEAP, TESS-NH/RC in addition to PEAP Japan Version 3 (PEAP-JV3). PEAP and TESS are the most frequently used instruments in LTC environment assessment although they are not specific to small-scale living units (Elf et al., 2017). PEAP-JV3, culturally specific to Japan, is the only available environmental scale for aged LTC facilities (Kodama Research Laboratory, 2005). Although different assessment tools have different questions and structures, they address similar factors of the environment. The EAT-HC items and the overall total score of unit environment are compared with items of PEAP, TESS-NH/RC, and PEAP-JV3. To account for the residents’ schedule and to ensure maximum daytime lighting, all assessments were conducted between 10 a.m. and 2 p.m.
Data Analyses
Content validity
To test the validity of EAT-HC-JV, we used item-content validity index (I-CVI) and scale-content validity index (S-CVI). I-CVI is calculated using the number of ratings of agreement on an item whether it is important or extremely important (three or four) divided by the total number of experts. An item is considered as acceptable if I-CVI ≥ .80; I-CVI scores between .70 and .79 suggested need to be modified before adaptation (Lynn, 1986). S-CVI is the validation of the total instrument. The scale is considered acceptable if S-CVI ≥ .80 (Polit & Beck, 2006).
Another CVI, Aiken’s V value was also calculated. The formula for Aiken’s V value is: V = S/[n(c − 1)] (Aiken, 1985, p. 136). In this formula, S represents (r − lo), whereas, lo is the lowest validity score while r is the value given by expert, c is the highest validity score, and n is number of experts who gave the score. The V coefficient ranges from 0 to 1. The closer the item index is to 1, the higher the validation of the item (Aiken, 1985). For 12 raters, V ≥ .69 is considered significant, equivalent to p = .05 level, and V ≥ .76 equivalent to p = .01.
Homogeneity reliability coefficient
To test the experts’ consistency of EAT-HC-JV, we used Aiken’s H value to examine homogeneity reliability coefficient for all 77 items. Items are considered significant when H ≥ .44 (p = .05) or H ≥ .55 (p = .01). Formula for Aiken’s H value is: H = 1 − 4S/[(c − 1) (n 2 − j)] (Aiken, 1985, p. 140), where j = 0 if n is an even number and 1 if n is an odd number.
Interrater reliability
The exact count-per-interval of interobserver agreement (IOA) was computed for interrater reliability. Exact count-per-interval is the most precise method of IOA that calculated the percentage of intervals by two researchers recorded the same values (Reed & Azulay, 2011). Internal consistency (Cronbach’s α) and intraclass correlation coefficient (ICC) of EAT-HC-JV subscales were also analyzed.
For analyses, we used SPSS Version 26 and Microsoft Office 365 Excel. This study obtained Institutional Review Board (IRB) approval from J. F. Oberlin University, Tokyo, Japan, to conduct reliability and concurrent validity testing (File #:18005); IRB exemption was obtained from San Francisco State University, CA, USA, to assess content validity (File #: 2019-012).
Results
Validity Assessment of EAT-HC-JV
Content validity
All items obtained rating from each of the 12 experts. However, due to regional customs and/or facility policies, numbers of raters from facility care experts were modified on four items. Specifically, Q4.1, Q5.5, and Q5.16 were rated by 10 experts, and Q7.2 by 11 experts. Depending on the numbers of raters, the cutoff points for Aiken’s V values were set the significance levels of p = .01 and p = .05, respectively, as follow: for n = 12, V ≥ .69 and ≥ .76; for n = 11, V ≥ .73 and ≥ .79; and for n = 10, V ≥ .73 and ≥ .80. See Table 3 for reasons for modification of raters’ numbers on I-CVI and Aiken’s V values.
Reasons for Modification of Raters’ Numbers on I-CVI and Aiken’s V Value.
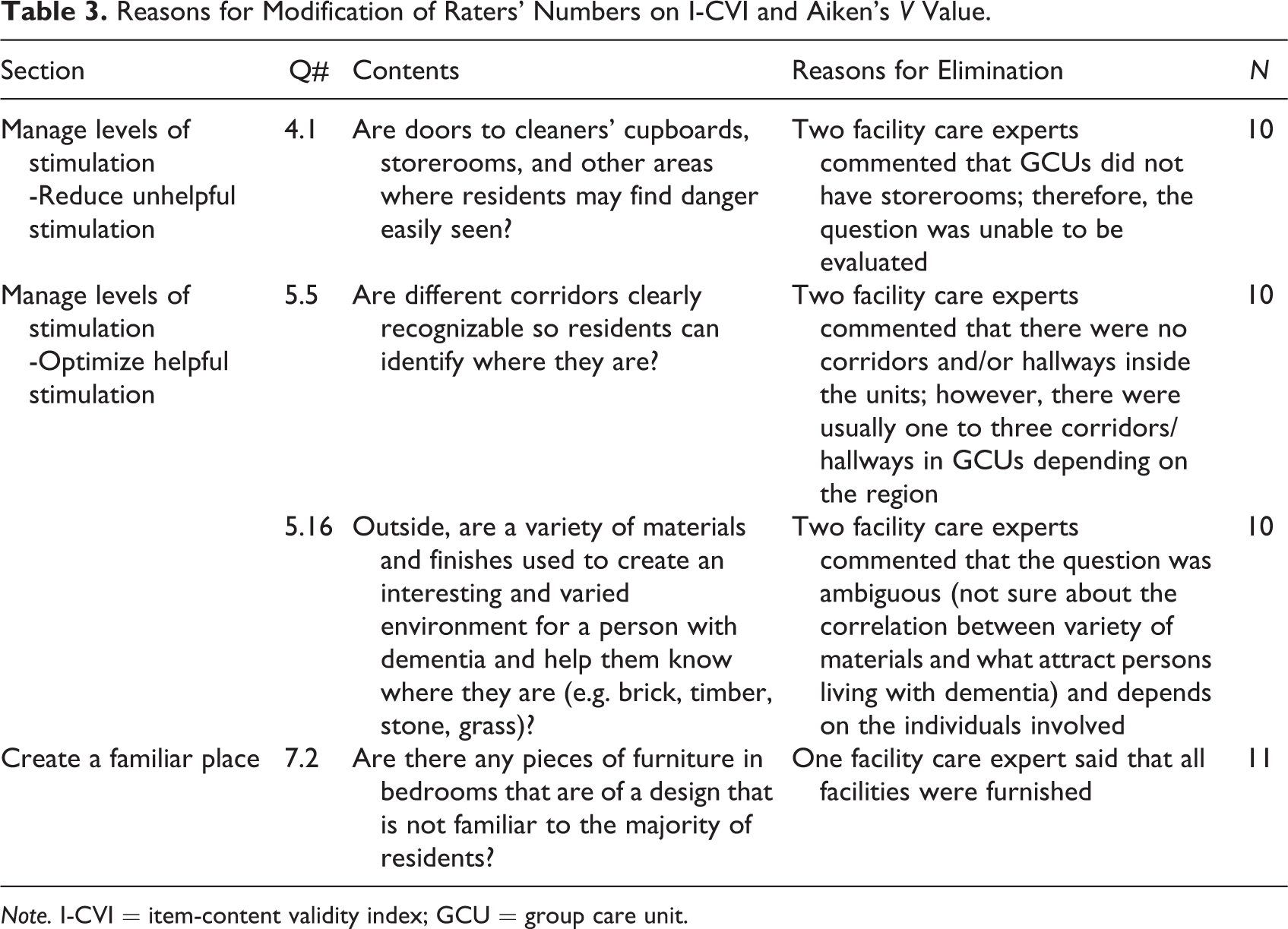
Note. I-CVI = item-content validity index; GCU = group care unit.
Of the 77 items, 71 (92.2%) met the relevant content validity (I-CVI ranged 0.42–1.00) with S-CVI of .88. The same 71 items also met significance on Aiken’s V (p = .05), and of those, 47 met the p = .01 significant level.
Items on EAT-HC-JV That Suggested Modifications by Experts
A total of six items (Q1.1, 1.2, 1.10, 1.11, 2.1, and 5.8) of EAT-HC-JV did not reach significance for both I-CVIs (.42–.75) and Aiken’s V values (.44–.61). For example, Q2.1 had I-CVI score of .75, indicating need for modification of the item rather than elimination. Comments from some of the participating experts pertained to those six questions marked inappropriate are as follows:
Q 1.1: “Can people who live in the unit be prevented from leaving the garden/outside area by getting over or under the perimeter?” and Q1.2 “Can people who live in the unit be prevented from leaving the garden/outside area through the gate?”—the experts did not agree with the wording “preventing from” which, to them, sounded like suggesting restraining the residents.
Q 1.10: “Is there a way to keep residents out of the kitchen if required?”—the experts did not agree with the wording “keep residents out of the kitchen” which, to them, sounded like preventing residents from an opportunity to be engaged and independent.
Q 1.11: “Can appliances be locked away in the kitchen the residents use?”—it was not clear to the facility care experts why the appliances have to be locked away. It sounds like taking away residents’ access to the use of those appliances unobtrusively.
Q 2.1: “Does the scale (height and width) of the common areas allow a person to feel comfortable (and not uneasy because they are too big or too small)?—aging care specialists stated that because an appropriate number of residents per unit has not yet been defined scientifically and the capacity of the GCUs in Japan is usually between nine and 12 persons, the question was deemed unnecessary.
Q 5.8: “Is, or can, the bed be placed so that it is possible to see the toilet pan from the bed when lying down?—experts thought that it is not appropriate to see the toilet or toilet pan from the bed.
Concurrent validity
See Table 4 for concurrent validity of EAT-HC-JV against PEAP, PEAP-JV3, and TESS-NH/RC. All six subscales were significantly correlated (r = .39–.85, p < .05) except for subscale 1 unobtrusively reduce risks with PEAP-JV3 (r = .27). There was a significant correlation (p < .001) between the total score of EAT-HC with PEAP (r = .78), PEAP-JV3 (r = .78), and TESS-NH/RC (r = .65).
Concurrent validity was rerun after omitting items (Q1.1, 1.2, 1.10, 1.11, and 5.8) that did not meet all the experts’ agreements. The results of subscales 1 unobtrusively reduce risks and 4 and 5 manage levels of stimulation did not retain its relevance to other scales. The total scores were slightly lowered than the results of the 77 global questions.
Concurrent Validity of EAT-HC-JV Against PEAP, PEAP-JV3, and TESS-NH/RC.
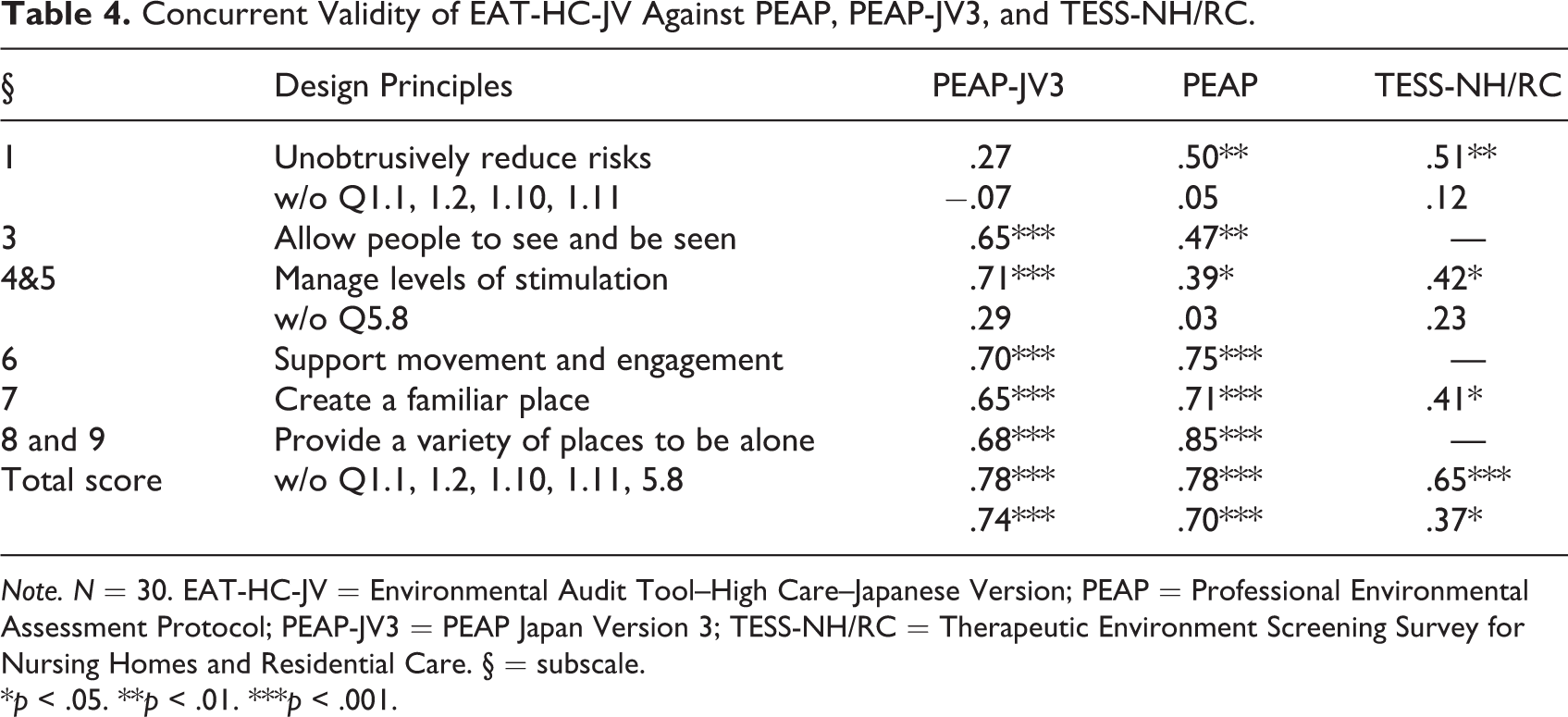
Note. N = 30. EAT-HC-JV = Environmental Audit Tool–High Care–Japanese Version; PEAP = Professional Environmental Assessment Protocol; PEAP-JV3 = PEAP Japan Version 3; TESS-NH/RC = Therapeutic Environment Screening Survey for Nursing Homes and Residential Care. § = subscale.
*p < .05. **p < .01. ***p < .001.
Reliability Assessments of EAT-HC-JV
See Table 5 for the EAT-HC subscale’s internal consistency (Cronbach’s α) and ICC assessment of 30 GCUs. Both Cronbach’s α and ICC demonstrated excellent scores ranging from .88 to .98 and.80 to .98 (p < .001), respectively. Two raters’ absolute agreements, the percentage of exact count-per-interval ranged from 81.6% to 94.3%, and the overall scale of exact agreement was 90.3%. The internal consistency assessed by 12 experts demonstrated that all items were >.55 (p = .01, range = 0.76–1.00). The overall scale was considered a reliable instrument. Table 6 shows the summary of all statistical results of EAT-HC-JV.
Internal Consistency and Interrater Reliability.
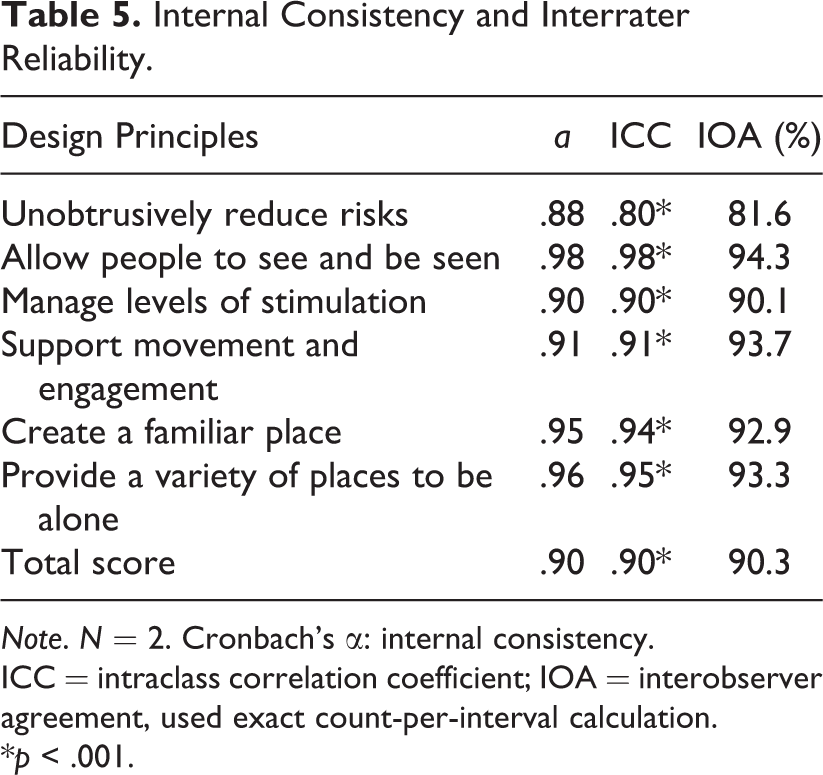
Note. N = 2. Cronbach’s α: internal consistency. ICC = intraclass correlation coefficient; IOA = interobserver agreement, used exact count-per-interval calculation.
*p < .001.
Summary of Statistical Results of EAT-HC-JV.
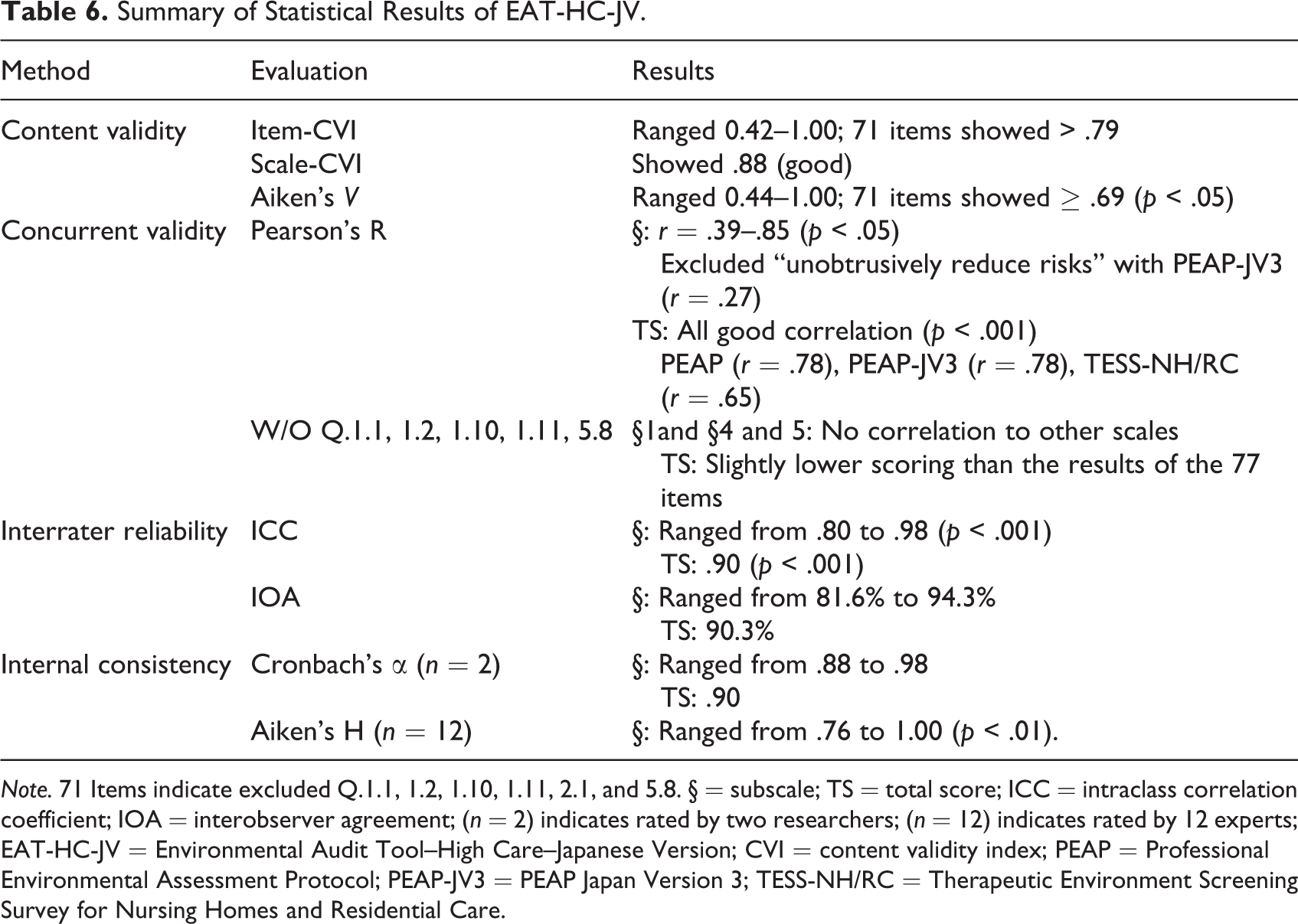
Note. 71 Items indicate excluded Q.1.1, 1.2, 1.10, 1.11, 2.1, and 5.8. § = subscale; TS = total score; ICC = intraclass correlation coefficient; IOA = interobserver agreement; (n = 2) indicates rated by two researchers; (n = 12) indicates rated by 12 experts; EAT-HC-JV = Environmental Audit Tool–High Care–Japanese Version; CVI = content validity index; PEAP = Professional Environmental Assessment Protocol; PEAP-JV3 = PEAP Japan Version 3; TESS-NH/RC = Therapeutic Environment Screening Survey for Nursing Homes and Residential Care.
Discussion
The EAT-HC was developed from EAT for environmental assessment of LTC facilities in Australia. In this study, we succeeded to translate the EAT-HC from English into Japanese and validate EAT-HC-JV with good interrater reliability and good content validity and concurrent validity. In order to stay true to the standardized EAT-HC, we kept the six questions that did not reach the significant standards for I-CVI and Aiken’s V validity testing. We believe that these six questions could prove to be of value for some GCUs.
At the onset, we discussed with the instrument’s authors about the outside space questions that may not be applicable due to the geographical and social conditions of Japan’s facilities (Fleming & Bennett, personal communication, December 21, 2018). Compared to Japan, Australia is approximately 20 times larger geographically but has only about one fifth of Japan’s population (Central Intelligence Agency, 2020). The vast landscape of Australia affords nursing homes with an abundance of outside space for residents to engage in natural surroundings. Buildings are usually one-story, giving the residents easy access to the outside space without needing the accompaniment of an attendant. Conversely, Japan’s facilities are multistory buildings near big cities where space is a luxury, and residents are required to use an elevator with assistance to access outside space or a shop/vending machines on the ground floor. Despite those differences in geographical and social conditions between the two countries, the instrument is focused on small-scale group living facilities, privacy of the residents, creating homelike atmosphere, and support ADLs for residents living with dementia in order to enhance residents’ QOL. That meets the aims of Japan’s GCU facilities. Therefore, we deemed EAT-HC to be applicable for environmental assessment of Japan’s GCUs.
Differences in Cultural Concepts
In addition to geographical and social conditions, there exist differences in cultural concepts. For example, there are distinguished criteria of contrast based on Japanese architectural design, and the study clarified the understanding of contrast from the viewpoint of the Japanese aging care experts. Although these experts believed that three questions about contrast were appropriate to include when assessing GCUs, they require clarification of the evaluation criteria for contrast. A facility care expert said, “Is it supposed to be considered as contrast if a toilet pan was different color from the rest such as floor, wall, and ceiling?” Others said, “it was impossible to imagine there was no contrast inside the units.” From these comments, the majority of facility care experts thought any different color or material was enough to create contrast regardless of complimentary colors. Questions about contrast are as follows: 5.9: Do the toilet seats contrast with the background? 5.11: Inside, Are contrasting materials used so that edges of surfaces and objects can be easily seen (e.g., colored borders, different floor, wall, and ceiling color)? 5.15: Outside, Are contrasting materials used so that edges of surfaces and objects can be easily seen (e.g., colored borders on paths, different colors and materials for seats and ground surfaces)?
From the Japanese architectural perspectives, the use of wood is important to convey the feeling of warmth and serenity; however, this leads to very little contrast (see Figure 2). Unlike in Australia, contrast by using timber that comes in various shades from light to dark does not compromise design, Japan favors a more neutral or natural wood tone design in the GCUs where everything blends in like it does at home. Facility directors and architects wish to continue incorporating warmth and serenity into the GCU design to provide the residents with a homelike atmosphere. Although it has been determined elsewhere in the world that contrast helps residents with low vision or dementia to recognize objects in the environment more easily (Fleming & Bennett, 2017), Japan aging experts and/or architects are hesitant to use clear contrasts that may defeat the unity and harmony of the design (e.g., applying different hue on toilet seat or handrails to distinguish from the background). As Calkins (2018) suggested to take into account both views of “designed by architects” and “people in the setting” in order to provide better functional support, relationships, and higher QOL for residents, Japanese gerontologists need to work more closely with facility directors and architects to find a balance in the cultural aspects of design while promoting a dementia-friendly environment. We also received suggestions from aging care experts on adapting examples in accordance with Japanese culture, such as floor materials and types of doors (sliding doors are more common), and types of indoor/outdoor activities.

Examples of a hallway and a communal area.
Item 5.8 “toilet pan was seen from the bed” was the most controversial question of EAT-HC. The majority of the facility care experts stated that it was not appropriate to see the toilet pan when residents were supine in bed and thus questioned the importance of the item. They would rather provide a view of outside space or of other residents in a communal area from the individual’s bed. In contrast to these experts’ comment, visibility of a toilet pan is intended to reduce confusion, minimize discomfort, and help maintain independence (Fleming & Bennett, 2017; Zeisel, 2017). Other items that received added comments were Q5.12–5.14, 5.17, and 5.18: “inside/outside, olfactory/tactile/auditory cues used to provide a variety of experiences for a person with dementia and help them know where they are.” Some facility care experts wanted clarification on how olfactory, tactile, and/or auditory cues correlate to the variety of experiences for persons living with dementia. These comments might be owing to the limited study of small-scale group living environment for dementia care in Japanese scholarly articles. Therefore, translating EAT Handbook to appropriately use the EAT-HC-JV is our next step (Wild et al., 2005).
Four items from Section 1 unobtrusively reduce risks did not obtain agreement from the experts and thus Section 1 did not demonstrate the correlation with PEAP-JV3. Those four items received additional scores if concepts were implemented unobtrusively. Some facility care experts asked for explanations for items such as why it is acceptable to restrain residents’ behavior if you can control them unobtrusively. The aim of implementing unobtrusively is to provide a “secure perimeter” keeping residents safe from a potential danger (Fleming & Purandare, 2010) which may imply “restraint” in some cultures. For example, in the German context, three items of EAT-HC related to unobtrusively did not fit due to the perspective about deprivation of freedom (Bleckmann, Fleming, et al., 2019).
From the results of content validity and experts’ comments, two key principles (1 unobtrusively reduce risks and 5 manage levels of stimulation—optimize helpful stimulation) emerge as cultural concept of the design gaps. This may be explained by a general lack of awareness on environmental design in East and Southeast Asia compared to Australia and the United Kingdom (Sun & Fleming, 2018). Based on the findings of our study, we hope to engage in conversations with colleagues from around the world about their perspective on secured perimeter among other seemingly controversial items.
Challenges in Translation
Although the sensitivity and concept of original instrument was strictly maintained (Wei et al., 2012), some wording and examples in the original EAT-HC were difficult to explain in Japanese. Along with contrast, some items became unclear during and after the translation. For example, “Does each room have a distinctive character and feel (i.e., is it easy to identify a room as a dining room or a lounge room?)” Facility care experts thought that all rooms have some degrees of characters. In Japanese culture, any small change would constitute “distinctive” while it may not be noticeable in other cultures, especially those using a dementia-friendly design with distinctive contrast. While dementia-friendly design requires things to be bolder to be distinctive, subtlety is the fundamental of beauty as it depicts the personality of the Japanese design. Some items thus become unclear when translated into Japanese. For example, in response to “what proportion of residents can see the inside of a lounge room as soon as they leave their bedroom?” the participant experts claimed that the proportion would differ depending on where the residents stand such as at the door, on the doorframe, or in front of the door. This is specific in Japanese language when a person leaving the room, the exact location where this person is situated in relation to the exit door matters. Another example, “Is the wardrobe (or cupboard) that the resident uses full of a confusing number of clothes and/or irrelevant objects?” also required clarification. Some of the facility care experts requested us to specify the numbers of clothing items that might trigger residents living with dementia to be confused. They strongly suggested a chart with exact numbers of clothing/objects (e.g., <5, 6–10, >10) to facilitate evaluating the question. Others said confusing numbers of clothing/objects depend on the residents. Four facility care experts suggested to explain the definition of “an attractive view.” They considered this notion an insult as they believed there were no LTC facility in Japan built with an unattractive view or unpleasant environment. A facility care expert commented that evaluating “an attractive view” depends on the individual evaluator’s background and that it is difficult to figure out how the residents really feel about the view from their bedroom.
Some examples of activities of EAT-HC may not be done in Japan such as sorting tools and watching birds as well as community socialization such as knitting groups and church groups. However, we decided to leave these examples because they might be done in some rural areas or will be done in the future. A facility care expert from Hokkaido pointed out that wind chimes are hung inside only. In Tokyo, wind chimes are hung outside. Even within Japan, it may be inconsistent to use wind chimes as an example of outdoor stimulation. This suggests needs to further develop a subculture adaptation of EAT-HC-JV for different regions of Japan.
Contributions of EAT-HC-JV
To our knowledge, this is the first study to translate and validate an appropriate instrument for environmental assessment to enhance QOL of older adults living with dementia in Japan’s GCUs. The new instrument can potentially promote designing dementia-friendly environment that encourages intellectual and emotional well-being, social interaction, reduces agitation, and improves functionality of residents living with dementia in Japan’s GCUs. Although Lawton’s environmental press-competence model explains the relationship between physical environment and human behavior, the relationship between the environment and older adults living with dementia need to be discussed further (Nordin et al., 2015). Not only improving small-scale living facility environment, EAT-HC-JV is expected to be used as a comprehensive EAT along with a standardized behavioral tool (e.g., Philadelphia Geriatric Center Affect Rating Scale, assessment tool for occupation, and social engagement, dementia care mapping) to explore the relationship between unit environment and behavior of residents living with dementia. Making EAT-HC-JV available and user-friendly will facilitate future studies of LTC environment and residents’ behaviors (Nordin et al., 2017). Validation of EAT-HC-JV and the experts’ comments provides a solid start for developing a culturally specific version to adapt to Japan’s cultural contexts.
Limitation and Implications
This study used a convenience sample of 30 GCUs from 11 welfare-based nursing homes for the elderly in the regions around Tokyo. All welfare-based nursing homes for the elderly operate under the strict law of Ministry of Health Labour and Welfare. Due to the climate differences, findings of this study may be generalizable to similar regional settings in Japan or other East and Southeast Asian countries.
Studies about the cultural adaptation of the EAT-HC instruments have been conducted outside of Australia (Bleckmann, Palm, et al., 2019; Sun, 2020). Based on this study results, we plan to modify EAT-HC by adapting to cultural aspects of Japan. Developing an environmental assessment instrument with cultural adaptation would set higher expectations for the residents’ QOL (Sun, 2020). Our next step is to translate the EAT-HC handbook to clarify the meaning of each question before applying it to small-scale dementia-care facility design. Having written examples in Japanese would be helpful for designers and facility directors to learn about how physical environment can support residents with physical and cognitive impairments. Hopefully, EAT-HC-JV can help educating facility manager/directors to understand how the environment could meet residents’ need. Using EAT-HC-JV would be the first step in identifying areas for improvement in Japan’s GCUs. For future studies, we endeavor to compare and contrast the use and acceptance of EAT-HC in countries outside of Japan.
Conclusions
This study demonstrated that EAT-HC-JV is an appropriate environmental instrument for Japan’s small-scale living unit facilities. The new instrument, as a comprehensive environmental scale, is the first tool to design especially for GCUs. The availability of easy-to-use EAT-HC-JV facilitates the systematic comparison of one environment with another, contributing to an informed discussion of the strengths and weaknesses of environments and, in appropriate circumstances, laying the foundation for planning the remodeling of poorly performing environments. We are planning to release EAT-HC-JV to the public and translate EAT-HC manual into Japanese. This study is the first step to develop a cultural adaptation of Japan version of EAT-HC.
Implications for Practice
▪ The principles of design of the EAT-HC are appropriate and acceptable for use to assess the environment of Japan’s small-scale group living facilities.
▪ EAT-HC-JV assists in identifying the areas for improvement in small-scale group living facilities and the support of residents’ QOL.
▪ Validation of EAT-HC-JV will lead to the development of a culturally specific version to adapt to Japan’s cultural contexts.
▪ Culturally sensitive aspects to Japan should be included to reflect Japanese architectural design in preserving a homelike atmosphere in small-scale group living facilities.
▪ The findings indicated the need for Japanese gerontologists to work more closely with facility directors and architects to find a balance in the cultural aspects of design while promoting a dementia-friendly environment.
Footnotes
Acknowledgment
The authors would like to thank Dr. Kei Adachi, Dr. Hisao Osada, facility directors, and aging experts for their contributions to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.