
Abstract
Objective:
The purpose of this study was to compare perceptions and behaviors of end users participating in simulations in a high-fidelity physical mock-up of an operating room (OR) prototype with the perceptions and behaviors of end users in the built out ORs postoccupancy.
Background:
Simulation-based evaluations of high-fidelity physical mock-ups of proposed layouts are increasingly being conducted during the facility design process to understand impacts on workflow and potential adverse patient safety outcomes. Nevertheless, it is unclear to what extent user experiences in these simulated healthcare spaces are similar to those in built and occupied healthcare environments.
Methods:
Using interviews, surveys, and observations, this study compared user evaluations in a high-fidelity physical mock-up of an OR with user evaluations of the built and occupied OR postoccupancy. Workflow disruptions were also analyzed using video recordings for a simulated pediatric surgery and five pediatric surgeries in the actual OR.
Results:
This study found that user perceptions and behavior in the two types of environments were mostly similar with regard to perceived support for the location of surgeon workstation, perceived space and task performance, perceived access to storage locations, boom setup, and OR cleanability. Participant’s ratings differed for supportiveness of the mobile Circulating Nurse (CN) workstation, maneuvering booms, and environmental disruptions.
Conclusion:
Simulation-based evaluations are extremely beneficial during the design process and can provide valuable input to design teams as well as clinical teams about workflow and safety issues that allow design issues to be addressed before construction.
Keywords
The physical environment of healthcare settings is one component of a multidimensional, dynamic work system that involves users with distinct roles, tasks, technologies, tools, and organizational protocols associated with their work (Carayon et al., 2006). Until recently, the physical environment was merely considered a backdrop for the work that needed to occur in healthcare settings. However, a growing body of evidence-based design (EBD) research has shown that the built environment can play a critical role in improving patient safety and quality (Joseph et al., 2018; Ulrich et al., 2008). Simulation-based evaluations of physical mock-ups are increasingly being conducted to help teams proactively evaluate proposed layouts for their impacts on workflow and potential adverse outcomes (Bayramzadeh et al., 2018; Colman et al., 2019). This is especially true for patient care spaces such as intensive care patient units, trauma bays, and operating rooms (ORs), where complex procedures may be performed on highly vulnerable patients (Colman et al., 2019). Nevertheless, it is still unclear to what extent these evaluations can predict workflow issues and outcomes in actual healthcare environments postoccupancy.
ORs are particularly challenging environments, and Wahr et al. (2013) suggest that poor room and equipment ergonomics are a major factor impacting interruptions and workflow disruptions that can lead to errors and surgical site infections in the OR (Wahr et al., 2013). A recent study showed that anesthesia work areas are particularly prone to disruptions due to inadequate space and environmental hazards that cause slips, trips, and falls (Joseph et al., 2018). The location of doors, size, and layout of the OR have also been identified as key factors impacting workflows and flow disruptions (FDs) in the OR (Bayramzadeh et al., 2018). Using physical mock-ups to study the interactions between the built environment and other system components (people, equipment, tasks) is particularly important while designing ORs, in part due to end-users’ difficulty in visualizing these interactions using other types of design communication media such as building plans or perspective drawings (Wingler et al. 2019.
Simulation techniques, where users reenact tasks or scenarios from clinical practice, have been used for the analysis of adverse events in healthcare and have been found useful in the detection of system-based errors (Slakey et al., 2014). A recent study, conducted during the schematic design phase of a new freestanding children’s hospital, used two rounds of simulation-based mock-up evaluation to test 11 clinical areas and was successful in identifying a range of built environment features that potentially impacted patient safety (Colman et al., 2019). However, no studies were found in healthcare settings that compared outcomes and experiences of end users in physical mock-ups with those in the actual built space using postoccupancy evaluation (POE) techniques. POE is defined as the process of evaluating buildings in a systematic and rigorous manner after they have been built and occupied for some time (Preiser et al., 1988). Given the need to understand how planned clinical spaces may impact workflows and patient outcomes in the future, the purpose of this study is to compare perceptions and behaviors of end users participating in simulations in a high-fidelity physical mock-up of an OR prototype with the perceptions and behaviors of end users in the built out ORs postoccupancy.
Method
Context and OR Characteristics
This study was conducted as part of a larger 5-year project focused on designing a safer and more ergonomic OR. The project involved in-depth study of ORs through literature review, video observation of 35 surgeries, case studies at three facilities, and interviews and focus groups with surgical team members. The surgery videos were coded and analyzed, yielding rich information about the dynamic interactions between surgical team members, their tasks, locations in the OR, door openings, and disruptions in the OR. This was followed by the development of EBD objectives that provided a framework for the design and evaluation phase. These objectives included (1) improve movement and flow, (2) improve visual and information awareness, (3) improve ergonomics, (4) reduce disruptions, and (5) reduce contamination to support cleaning practice. The high-fidelity physical mock-up was developed following three rounds of an iterative design process, utilizing simulation-based evaluation with surgical teams including a tape-on-the-floor mock-up and a cardboard mock-up (Bayramzadeh et al., 2018). A highly realistic OR prototype was then constructed and included flooring and wall surface materials found in ORs, a complete array of fully functional fixed and movable equipment (e.g., surgical table and booms), integrated data and video systems, and surgical instrument capabilities. The design concepts developed as part of the project were then implemented at a new pediatric ambulatory surgery center (PASC; Figure 1).

Mock-up prototype versus the built operating room.
The overall size, proportions, and layout of the prototype OR and the final built ORs are similar with an angled surgical table orientation and clearly defined work zones for surgical team members. The position of the OR table is also intended to provide a more efficient, effective, and protected workspace for anesthesia staff by eliminating the need for other staff to move behind them. Both rooms minimize clutter and related trip hazards and reduce the potential for surface contamination through flush wall surfaces, which can enhance cleaning, recessed storage, and the use of overhead booms that support cable and tube management. Figure 2 compares the features of the OR prototype and the built OR in the PASC.
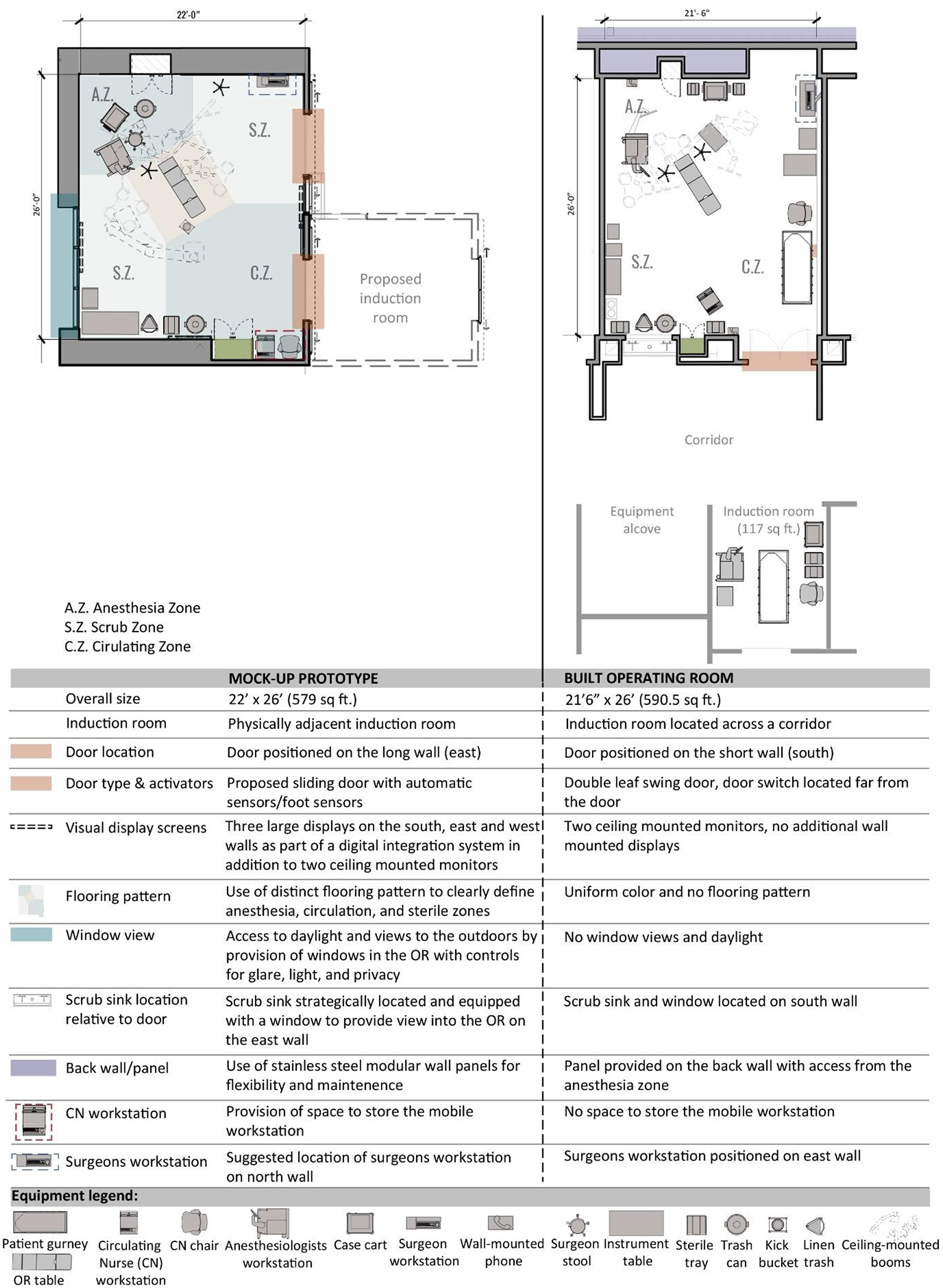
Features of operating room (OR) prototype versus built OR.
Data Collection
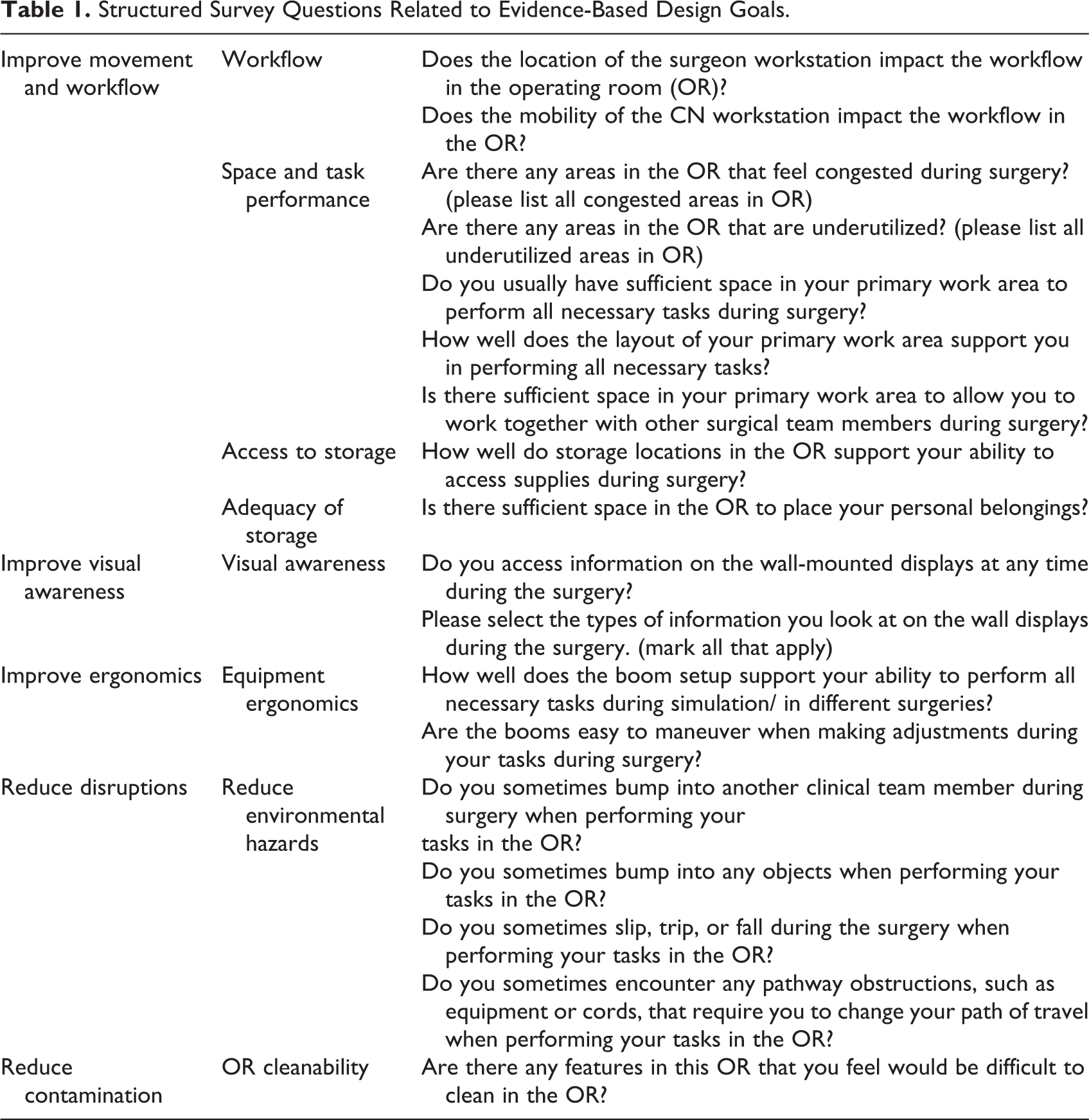
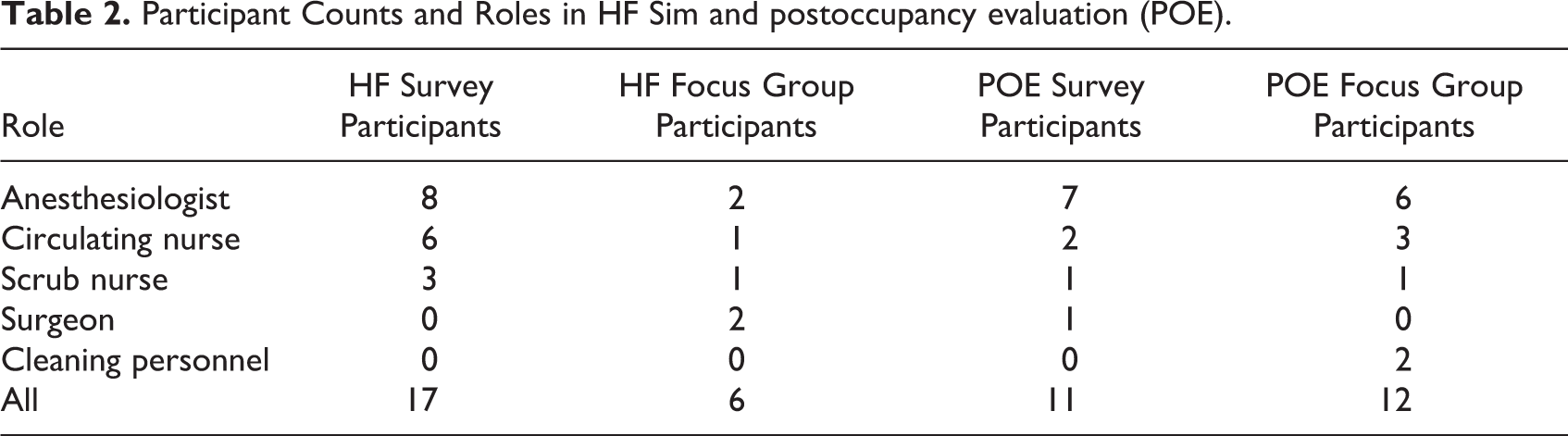
A multilayered data collection approach was implemented for evaluating the high-fidelity mock-up referred to as HF Sim (December 2018) and for the POE of the built OR referred to as POE (December 2019–January 2020)—data collection included survey, focus groups, and analysis of video recording of simulations/surgeries. Simulation scenarios were created based on actual surgery scenarios for pediatric surgeries. The three simulations for the pediatric surgery were led by a clinician leader and were enacted by frontline surgical team members. A structured survey was created based on literature review and key findings from the project and was sent to clinical team members to revise and validate before data collection in the HF Sim phase. The revised version of the survey was employed using the Qualtrics platform to collect data on an identical set of questions for both phases (Table 1 for survey questions); the response categories for 13 questions were yes, no, and not applicable. Three questions inquired about the quality of support provided by different environmental design features and had three choice response categories: extremely well, moderately well, and not well at all. There were two questions that asked participants to select items from a predesigned list of items including different spaces in the OR. During POE, participants responded to the questions based on their overall experience in the built OR. Table 2 shows the participant distribution between HF Sim and POE. Focus groups were conducted after the simulation sessions in HF Sim and between surgeries in POE. A range of topics were discussed in both phases, including OR size, design, equipment layout, OR cleanability, overall flow, work processes, and integration of induction rooms.
Structured Survey Questions Related to Evidence-Based Design Goals.
Participant Counts and Roles in HF Sim and postoccupancy evaluation (POE).
A pediatric hernia surgery, which is usually relatively short in duration (30–45 min), was simulated by the surgeon, circulating nurse, scrub nurse, and the anesthesiologists during HF Sim and was recorded and coded to identify the location and type of FDs based on an existing taxonomy (Palmer et al., 2013). Five pediatric hernia surgeries during the POE phase were also video recorded and coded for FDs. FDs were defined as deviations from the natural progression of a procedure that potentially compromise safety or efficiency (Palmer et al., 2013). An OR location map was prepared prior to data collection, which organized the OR into the functional zones (Figure 3). Prior to data collection, training was conducted with all observers to ensure the reliability of data capture. Video recordings of the HF Sim session and POE surgeries were coded using a template in Excel and Noldus Observer XT 10, respectively. Approval for this study was received from the health system’s institutional review board.
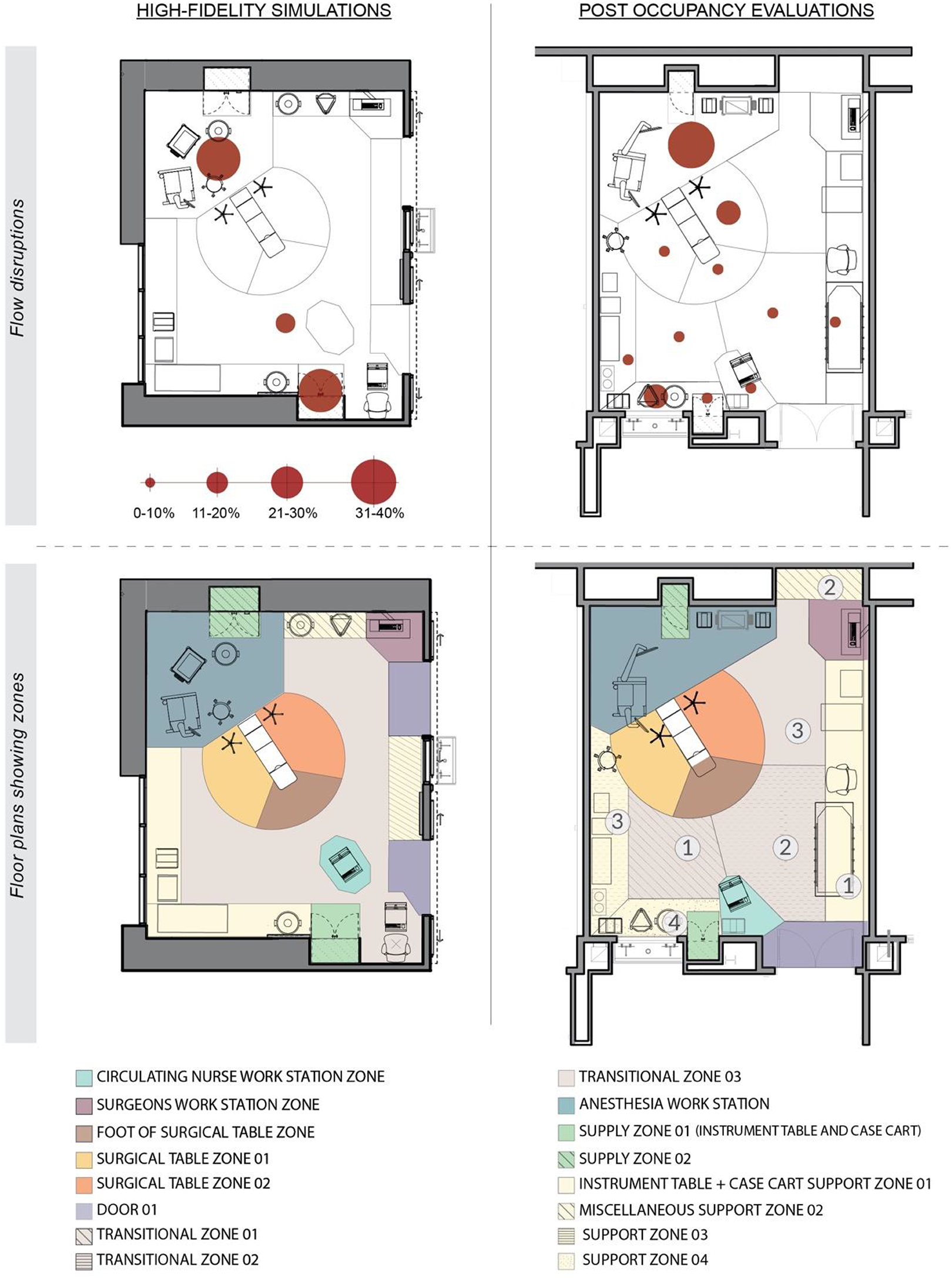
Distribution of flow disruptions.
Analysis
Data from the structured survey questionnaires were analyzed using Pearson’s χ2 test in SPSS statistics to compare responses between HF Sim and POE. Data from the focus groups (HF Sim and POE) were transcribed for further qualitative analysis. First, focus group responses were grouped based on participant role. Next, participant responses were thematically organized under relevant built environment categories-OR space, storage, and supplies, workstation, and so on; the content under each category was also organized according to whether it reported a barrier, facilitator, or had no impact. Comparative analysis was then conducted by grouping comments from the focus groups, into their associated EBD goal to understand the similarities and differences between the two phases. The location and frequency of FDs in the HF Sim and POE were compared using descriptive statistics.
Results:
The findings from the observations, survey, and the focus group for HF Sim and the POE are summarized as they relate to the five EBD goals—(1) improve movement and flow, (2) improve visual and information awareness, (3) reduce disruptions in the OR, (4) reduce contamination in the OR, and (5) improve ergonomics. Figure 4 shows the participant responses to questions on the survey.
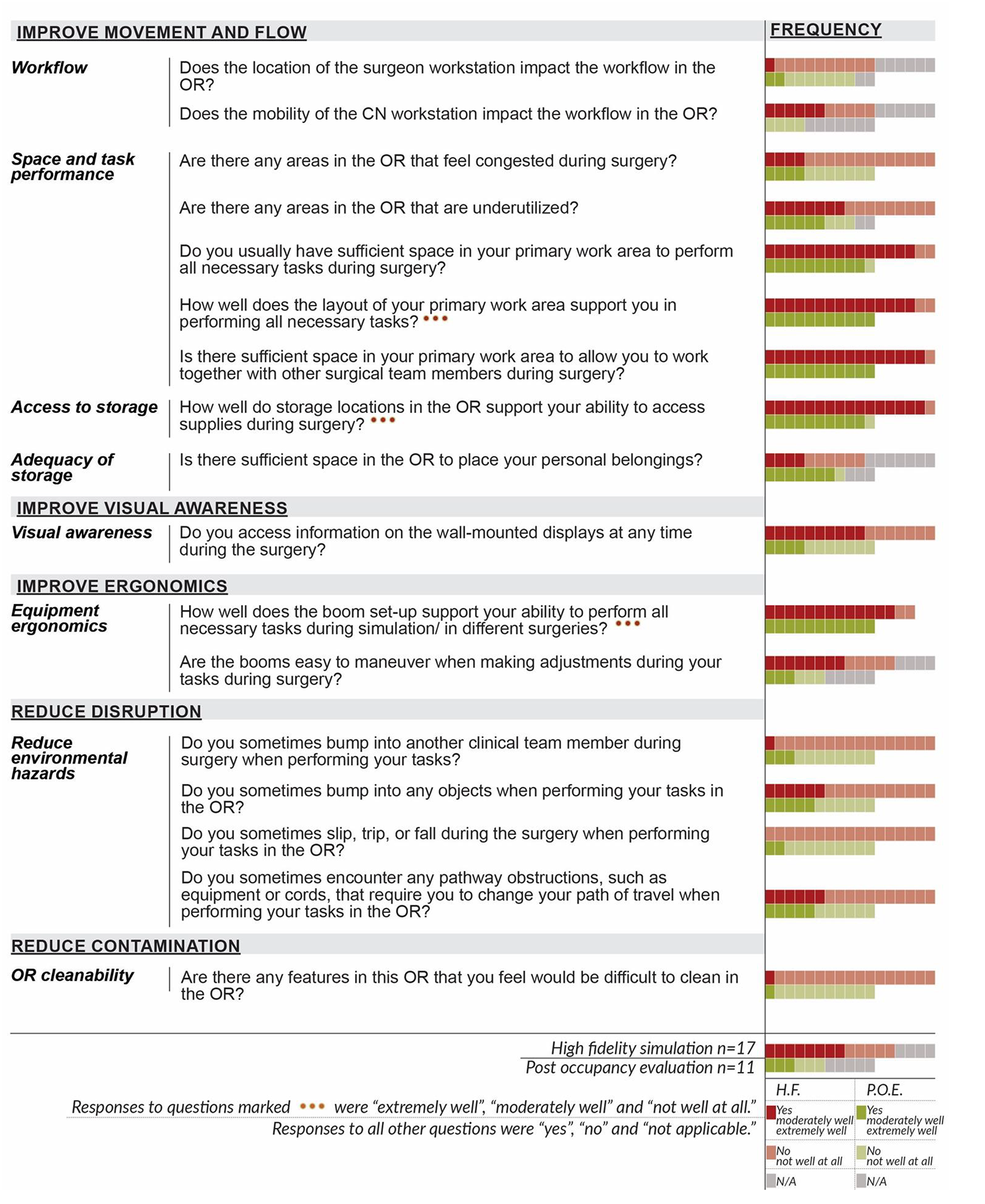
Participant responses to survey questions in HF Sim and POE.
Improving Movement and Flow
Improved workflow
Ease of access to surgeon’s workstation
The majority of the participants in HF sim (n = 10) and POE (n = 7) indicated that the location of the surgeon’s workstation in the corner of the OR did not impact the OR workflow. In the HF Sim focus group, the surgeons mentioned their preference for a mobile surgeon workstation and also a designated workstation with counter space, a place to sit, and document.
Mobility/placement of workstations
The perception regarding the mobility of the CN workstation did not differ between the two phases. During HF Sim, one third (n = 6) of the participants noted that the mobility of CN workstation impacted the workflow in the OR while approximately one third (n = 5) indicated that there was no impact; the other participants did not find this question applicable to them. A third of the POE participants (n = 4) indicated that the mobility of CN workstation did not impact the OR workflow, while the remaining (n = 7) participants indicated that the question was not applicable to them. During focus groups, CNs in the HF Sim stated that they preferred a mobile workstation to a fixed workstation. However, no specific concerns related to workstation type (fixed or mobile) were brought up during in the POE focus groups. In the POE focus group, circulating nurses mentioned that they preferred being close to the OR door while also facing the surgical table. The one challenge mentioned by nurses in the POE group was that due to the location of outlets, when the mobile workstation was being charged and used at the same time, nurses were unable to face the surgical field.
Workflow and access associated with the induction room
The integration of the induction rooms (which would result in induction taking place in a separate room adjacent to the OR) was a controversial issue in the HF Sim focus group. The nurses and anesthesia team members discussed potential challenges with the induction rooms, including the need to modify flows, need to staff team members in the OR as well as in the induction rooms, and managing overlaps between team members.
The focus group findings from the POE indicate that there were mixed perceptions about the separation of the induction room from the OR with a hallway in between. Some anesthesia team members and circulating nurses thought that the separate induction room imposed additional workload as compared to the patient being induced in the OR and slowed down the workflow. On the other hand, the scrub nurse, cleaning personnel, and some of the anesthesia team preferred the physical separation of the induction room from the OR.
The design of the induction room in the ASC also created several challenges for workflow and patient safety. While one anesthesia technician found the space in the induction room adequate, anesthesiologists and CRNAs preferred a bigger and wider induction room. As depicted in Figure 5, the sliding doors of the induction room open only half the width of the door opening, resulting in a tight opening for transferring the patient gurney from the induction room to the OR. While staff liked the sliding doors in general, one CRNA explained the problem with door one opening only halfway, “The door sliding concept is good; however, it does not slide all the way, it slides halfway, and it leaves a small window. And the CRNA is cramped next to the machine.” Further, the door opening for Door 1 is on the same side of the room as the anesthesia work area, resulting in conflicts while the patient bed is moved out. The door opening button for Door 1, on the other hand, is located on the opposite side of the room from the door opening, creates additional workflow disruptions and potential device disconnections from the patient during transitions. Figure 5 demonstrates the movement and access challenges in the induction room.
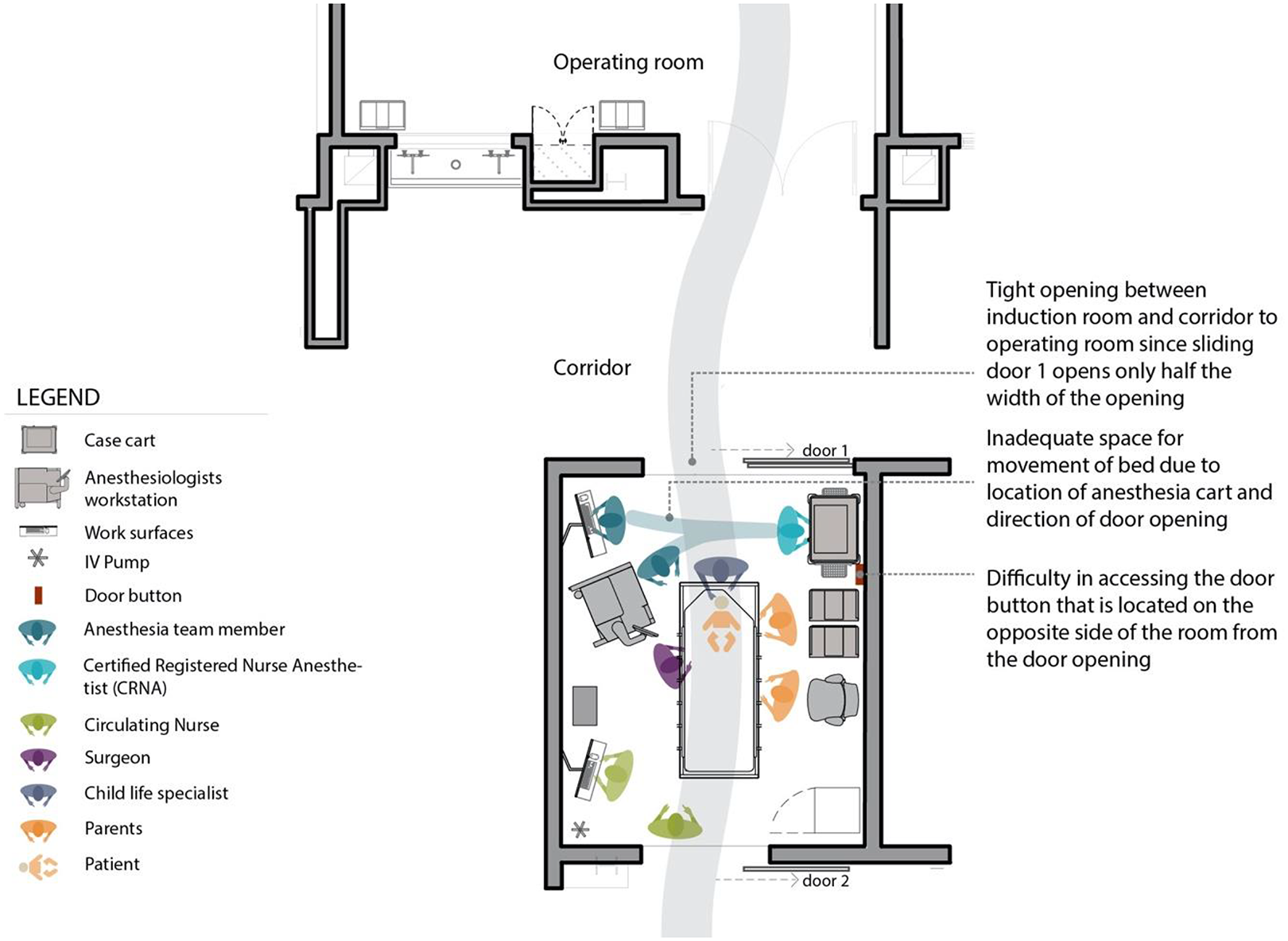
Induction room challenges.
The separation of the induction room from the OR resulted in a visual disconnect that made tracking the vacancy/occupancy of the induction room difficult for anesthesia technicians and circulating nurses. According to an anesthesia technician,
‘The problem with the induction room is that there is no way to know when the induction room is occupied or vacant and ready to be cleaned for the next case. There is no visibility to that area. The technician keeps guessing, waiting until they can go in the induction room for clean-up.’
‘It is a more natural environment to put the kids to sleep. Lights in OR are frightening for children, and it is good that children go to the induction room. The induction room is a much warmer environment from the perspective of family and children.’
Space and task performance
OR congestion
The perception of congestion in the OR did not differ between the two phases. Majority of the participants in the HF Sim (n = 12) and the POE (n = 7) indicated that there were no areas in the OR where they felt congested during surgery.
OR underutilization
The perception regarding OR underutilization did not differ between the two phases. In both phases, the participants were divided in how they perceived the utilization of the space in the OR—with nearly half the participants feeling there were some underutilized areas in the OR and the other half feeling that there were no underutilized areas or that they found the question not applicable to them (n = 2 in POE). Although the perception of OR space underutilization was rated similarly in both phases, different areas were identified as being underutilized in the two phases: Anesthesia zone, instrument setup area, surgeon workspace, and corners of the room were perceived as being underutilized in HF sim, while only corners of the OR were listed as underutilized space in the POE.
Space in primary work area
The majority of the participants in HF Sim (n = 15) and the POE (n = 10) indicated having sufficient space in their primary work area to perform all necessary tasks during surgery. According to POE participants, the new ORs were bigger in size and therefore easily accommodated all the necessary equipment (e.g., x-ray, c-arm) along with the stretcher in the room.
Layout in primary work area
The majority of the participants in HF Sim (n = 15) and all survey participants in the POE (n = 11) indicated that the layout of their primary work area supported them (moderately to extremely well) while performing surgery related tasks.
While the angled surgical table was perceived positively by clinicians during the HF Sim, there were mixed comments about this feature during the POE focus groups. According to some anesthesia team members and circulating nurses, angling the surgical table in the room did not influence workflow during the surgical procedure, while others indicated that this feature enhanced the workflow. One circulating nurse found that the angled surgical table enabled better utilization of space: “The tilted bed works well. It gives us enough room on both sides, plenty of space to bring the patient to the room, flipping the gurney, transfer the patient on to the table, we don’t have to move the bed.” Nurses mentioned that not all surgeons utilized the angled surgical table orientation; some preferred to orient the table parallel to the long wall of the OR.
Space for teamwork in primary work area
The majority of study participants in HF Sim (n = 16) and all participants in POE (n = 11) mentioned having sufficient space in their primary work area to work together with other surgical team members during surgery.
Access to storage
The majority of survey participants in both HF Sim (n = 16) and POE (n = 10) indicated that the storage locations supported easy access to supplies in the OR moderately to extremely well. Participant in the HF Sim focus group mentioned the need for both in-room and central storage space. Similarly, participants in the POE focus group felt the need for more storage space. Some anesthesia team members mentioned that the provided storage space was proportioned for a small surgery room and felt more storage space was needed for anesthesia supplies. All circulating nurses indicated the need for larger storage space, and one nurse suggested having an entire wall of storage in the OR. In both phases of data collection, circulating nurses found the structure of the cabinet “with hinged doors” appropriate and helpful in maintaining the cleanliness of supplies.
Adequacy of storage
A smaller number of HF Sim participants (n = 4) thought there was enough space in the OR to keep personal belongings such as personal phones compared to more than half of the participants (n = 7) in the POE; however, the perception regarding the adequacy of storage did not significantly differ between the two phases. The circulating nurses in the HF Sim focus group mentioned the lack of space for personal belongings in the prototype OR. However, this was not brought up as an issue in the POE focus group findings.
Ease of access to wall-mounted outlets, switches, and fixtures
The door opening button location in the built OR was mentioned as being challenging by most of the participants (refer to Figure 2). A cleaning staff member mentioned, “The only issue is the door key; I wish it was closer to the door.” This resulted in someone having to keep the button pressed to prevent accidental closures while people or equipment were moving through the door. The POE focus group participants indicated that the button should have been located closer to the door. Another door related problem was identified by a scrub nurse,
‘Automatic doors are great, but they don’t stay open long enough. You need to hit [the door opening button] two times, so that it does not close when moving the patient out. Air handlers and air pressure affect the doors, sometimes you get trapped in the room.’
Anesthesiologists in the POE focus group noted the location of the phone (mounted on the wall behind the anesthesia machine) to be inappropriate since visual access to patient monitors was blocked when they were talking on the phone.
Improve Visual Awareness
The majority of study participants in both HF Sim (n = 16) and POE (n = 10) agreed on being able to see all the necessary information to perform surgery related tasks. Participants in the HF Sim focus groups indicated that the wall-mounted monitors in the OR prototype were too high and indicated that wall-mounted and boom-mounted displays should be at or below eye level, as well as out of the way so that they would not bump their heads on the displays. There were mixed opinions between surgeons regarding the preferred location for the wall-mounted screens; one surgeon preferred the screens to be at the back of the anesthesia work area or at the foot of the surgical table, whereas the other surgeon preferred the wall-mounted screens to be located over the nurse work area or on the wall by the door. Patient vitals, OR schedule, real-time imaging, time and date, surgical checklist, and surgical site video were the types of information participants looked for on the wall-mounted displays.
The anesthesia team members in the POE focus group indicated having access to all necessary visual information with no obstructed views. Other surgical team members did not comment on the location or functionality of display screens in the new PASC OR.
Improved Ergonomics
The majority of HF Sim participants (n = 15) and all POE participants (n = 11) thought that boom setup supported their ability to perform necessary tasks during surgery moderately or extremely well. Although participants thought booms supported their tasks during surgery in both phases, adjusting the booms was clearly an issue in the POE; therefore, the perception regarding boom adjustments differed between the two phases. While more than half of the HF Sim participants (n = 8) rated the booms as easy to maneuver and adjust for surgery-related tasks, only a few participants (n = 3) thought the booms in the new ORs were easy to adjust.
The surgeon in the HF Sim focus group indicated a higher preferred height for the booms to minimize light and monitor conflicts. Locating the surgical booms on the left side of the surgical table (when standing at the foot) was suggested to optimize space use on the back wall and to enhance circulation. The circulating nurse mentioned that there was a lot of crossing occurring between the boom monitors and suggested that placing the booms (each containing a light and a monitor) slightly further apart from the center line of the table. The surgeon in the HF Sim focus groups indicated that the light boom should be right over the surgical field to mitigate equipment lights and monitor conflicts and also to keep the unnecessary equipment out of the operative field.
Challenges related to booms were again brought up as a concern in the POE focus group. According to the anesthesia technician and some circulating nurses, the height of the monitors on the boom was low and often got in the way. However, some other CNs found the height of the mounted screens appropriate. Participants also indicated technical difficulties with moving the boom arms, which sometimes hit each other and were hard to handle. According to some POE participants, the placement of the boom, along with the technical difficulties in moving it, led to the space between the boom and the back wall being utilized inadequately.
Reduce Disruptions
Bumps
The number of perceived bumps to other team members was different and lower in the HF Sim in comparison to the POE; only one of the participants in HF Sim noted bumping into other team members compared to nearly one third of POE participants (n = 3). One third of the participants in the HF Sim (n = 6) and nearly half of the POE participants (n = 5) mentioned bumping into objects in the OR.
Slip, trips, or falls
All participants in the HF Sim (n = 17) and the majority of participants in the POE (n = 9) reported to not have slipped, tripped, or fallen during surgery related tasks.
Pathway obstructions
Pathway obstructions by equipment or cords that sometimes resulted in participants changing their path of travel were reported by half the participants in the POE (n = 5) in comparison to the one third in HF Sim (n = 6).
FDs
Figure 3 demonstrates the distribution of the FDs in different locations of the mock-up OR (HF Sim) and the built OR (POE). The proportion of FDs in the anesthesia work area remained similar between the two ORs (30%–40%). There were fewer FDs in the supply zone in the POE (0%–10%) when compared to the HF Sim. The supply zone accounted for a large portion (30%–40%) of the FDs in the HF Sim. There were no FDs recorded in surgical table Zone 2 (left of the patient head on the surgical table) during HF Sim. However, the surgical table Zone 2 accounted for around 29% of all observed FDs in the POE. A small proportion of FDs were also observed in other zones of the room during POE (nurse workstation, Support Zone 1, instrument table-case cart support zone).
Reduce Contamination
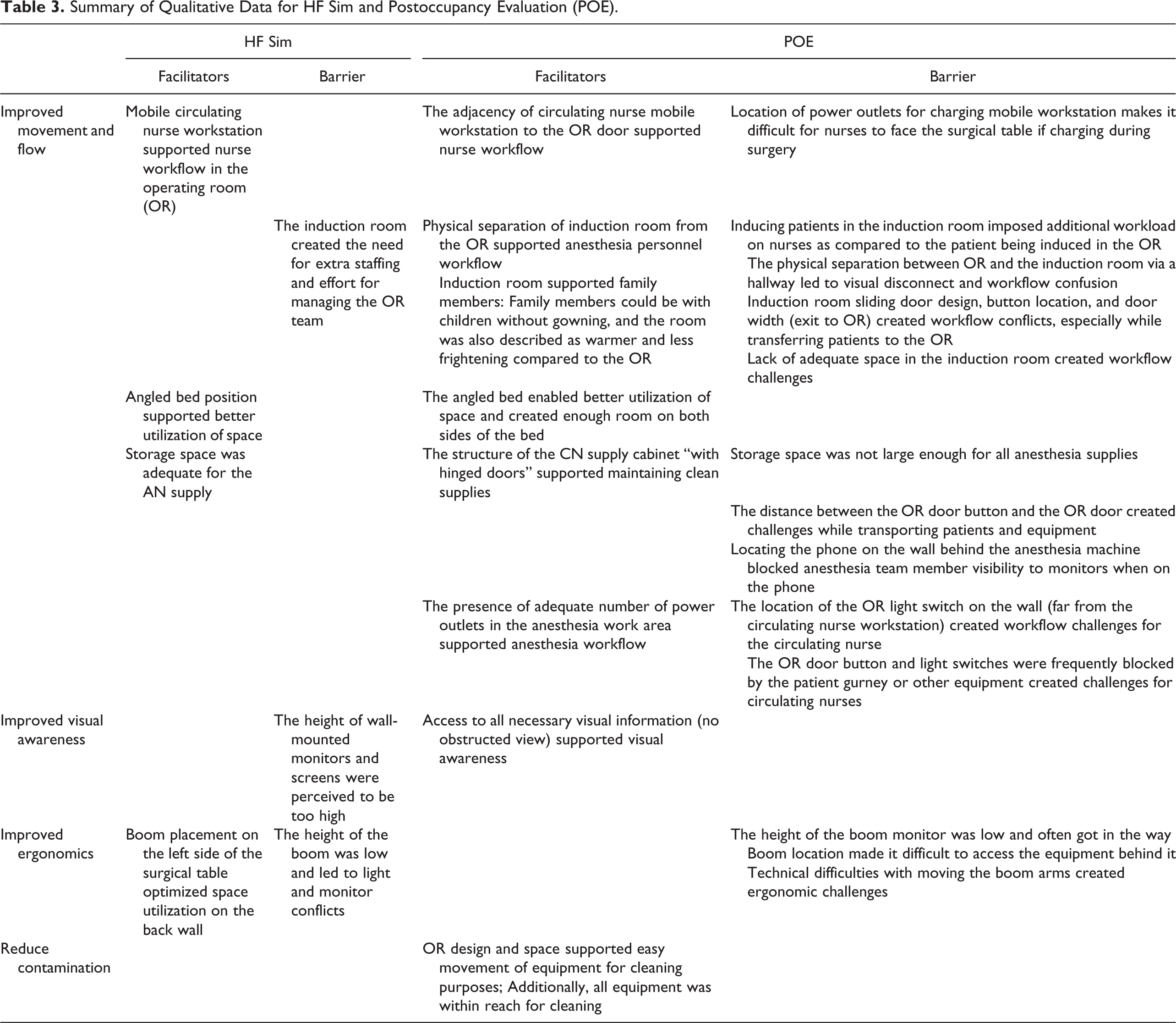
There was a high agreement between study participants regarding the cleanability of the OR; the majority of the study participants in both HF Sim (n = 16) and POE (n = 10) found the OR easy to clean. Additionally, according to the POE focus group, the design of the new OR provided adequate space for the housekeeping team to easily move around the equipment for cleaning. Table 3 demonstrates the summary of qualitative findings for the HF sim and POE.
Summary of Qualitative Data for HF Sim and Postoccupancy Evaluation (POE).
Discussion
Simulation-based evaluation of physical mock-ups are extremely valuable in obtaining key input from clinicians and support staff within the context of their workflows regarding overall layout, room size as well as placement of different design features. This study found that participants in the two phases (physical mock-ups and actual built and occupied ORs) had a similar perception regarding the majority of the EBD objectives. Specifically, end-user’s perceptions regarding the availability of space in the OR and their primary workspace as well as ease of access to supplies and storage were similar and positive. However, differences were observed in responses to specific ergonomics and functionality issues such as the utilization of booms and experiences with bumps and slips, trips, and falls. These issues cannot be fully explored during a simulation and are better understood after experiencing the occupied space for a period of time. Additionally, other issues related to the placement of switches, phones, and door buttons emerged during the POE and not in the HF Sim since the simulations did not include specific scenarios that required interaction with these elements. Future simulations should consider a range of tasks within specific scenarios that require interactions with all types of built environment features, such that their location and placement can be effectively tested prior to implementation.
The circulating nurse workstation was mobile in both phases. However, the location of the charging station/docking area for the workstation differed between the ORs. One of the potential benefits of a mobile workstation is being able to face the surgical table and getting closer to the surgical table as needed to observe the surgery while also reducing travel within the OR. However, the circulating nurses were tethered to the wall in the new ORs due to the need to charge their workstation. Increased battery life for workstations would potentially provide greater confidence to nurses to untether themselves from the charging station.
While the high-fidelity mock-up did not include a fully built-out induction room (only tape on the floor to designate an adjacent induction room), the new surgery center included induction rooms that were located across the corridor from the OR. As a result, this study was able to explore the functionality of the induction room in greater detail during the postoccupancy phase than was possible during the simulation. Specific issues with the layout of the induction room, design of doors, and switches were identified during observations. Users identified congestion and conflicts while moving the patient gurney out of the induction room to the OR due to the small size and location of the door opening and due to the sliding door opening on the same side as the anesthesia machine. These issues could potentially have been identified and addressed if the induction room had also been mocked up. There were also some mixed perceptions about the separate and parallel induction rooms in both HF Sim and the POE. Although some anesthesia team members and circulating nurses found the separate induction room to be imposing additional workflow, the scrub nurse, cleaning personnel, and some of the anesthesia team preferred the separation of the induction room from the OR in the POE. Anesthesia team members were comfortable with the induction room concept and felt it was more family-friendly, allowing parents to accompany their child through induction in a less threatening environment. The POE identified that other than the ergonomic challenges of the room itself, the induction room concept worked well for parents, surgeons, and anesthesiologists.
Similar findings were observed between HF Sim and POE related to space and task performance, access to storage, the utilization of the OR space for primary tasks during surgery, working with team members, and accessing supplies. These similarities suggest that simulation-based evaluations are a feasible method to test OR design concepts prior to building the actual space, especially concepts related to overall layout and organization. Ratings for perceptions of OR congestion and underutilization during HF Sim provided a good indicator for the performance of the actual built environment, as the negative and positive responses in the two phases remained similar. Additionally, the responses for whether the OR space and layout were supportive to perform tasks during surgery, work with other team members, and access supplies from storage locations remained highly positive for both HF Sim and the POE. There was only one instance regarding improved movement and flow which was rated differently between the two phases, where availability of space for personal belongings was rated considerably higher in POE in comparison to the HF Sim. This may be explained by the fact that in the simulation, no specific storage area was designated for personal belongings and some clinicians identified this as a concern.
This study showed that responses regarding the overall supportiveness of booms during surgical tasks remained similar (highly positive) between the two phases. Thus, participants were satisfied that booms were included. However, ease of maneuvering the boom, placement of the boom, and moving boom arms were brought up during the simulations and remained an issue in the POE phase.
The perception of bumps, slips, falls, as well as the observed location and number of disruptions in OR zones varied between the two phases. This may be attributed to the differences between a short surgical simulation (even a very realistic one) and the everyday experience of working in the OR in live clinical situations. No bumps, slips, and trips were observed during the simulation or surgery observations. However, it is reasonable to expect that the clinicians may have experienced some bumps, slips, and trips during the months of working at the surgery center and their responses reflect this experience. Similarly, disruptions were more scattered among the OR zones in the POE video observations in comparison to the HF Sim, in which disruptions only occurred in three locations. Despite the differences in the distribution of disruptions by location, it is worthwhile mentioning that the proportion of anesthesia-related disruptions to overall disruptions remained the same between the two phases.
Limitations
This study garnered feedback from clinicians in similar ORs using similar methods. However, there are unavoidable differences in functionality between a fully built out and occupied OR and a high-fidelity physical mock-up that impact how realistically a surgery can be performed in these two settings. Further, the layouts were different in regard to some features (e.g., door placement, workstation placement, and induction room adjacency), all of which could contribute to differences in overall flow patterns and disruptions within the OR. Only one simulation conducted for hernia surgery with induction room was available for comparing FDs in the observed surgeries, though other types of surgery simulations were conducted. A larger set of simulations may have helped in uncovering additional issues with the OR prototype. This study recruited a convenience sample of participants working in the built ORs for the POE; while the participants involved in the HF Sim were recruited from the staff working in the existing facility. There was no attempt to specifically recruit the same group during the two phases of this study. However, the participants were recruited from the same health system, so it is possible that some participants may have participated in both phases. Not all key staff members (e.g., cleaning personnel) were involved during HF Sim and POE. For a more holistic perspective, further engagement with other key stakeholders is recommended. These differences may potentially impact the comparisons and study findings.
Conclusion
Simulation-based evaluations are extremely beneficial during the design process and can provide valuable input to design teams as well as clinical teams about workflow and safety issues that allow any design issues to be addressed before construction. Design challenges identified postconstruction are often expensive to remediate. This study shows that clinicians responded in a similar fashion to many aspects of the OR design related to overall room size, available space, and access to supplies and storage. However, in order to fully understand ergonomics and usability issues, it is important that the mock-up include as many details as possible and that scenarios are designed to facilitate interactions with these elements such that they can be effectively evaluated.
Implications for Practice
This study provides a framework for conducting a comparative evaluation between features in a mock-up OR and the actual built OR based on EBD goals.
The study highlights the critical role of simulation-based mock-up evaluation in predicting design challenges in the postoccupancy phase
This study provides both a qualitative and visual demonstration of built environment features, barriers, and facilitators in the OR and in the induction room
This study provides a visual demonstration for how FDs were observed in the mock up simulation and in the postoccupancy phase
Footnotes
Acknowledgments
The authors would like to thank the RIPCHD.OR Study Group for their contribution to the work supporting this study. They would also like to acknowledge Rutali Joshi and Uniza Rahman for their support with graphics development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Agency for Healthcare Research and Quality (grant number P30HS0024380).