
Abstract
Objectives:
This case study intends to examine how staff characteristics, training methods, and duration of training impact overall staff preparedness and comfortability when transitioning to a new Labor and Delivery.
Background:
A new medical facility offers an opportunity for greater capacity and expanding services, but it also poses new challenges for staff. Success in this transition depends on how quickly the staff can adapt to their new environment and how prepared they are to deliver high-quality care to patients.
Methods:
An optional survey was conducted to determine the staff’s confidence in their training using a 5-point Likert-type scale.
Results:
After responses were collected, a paired samples two-sided t test revealed that there was no statistically significant change in the confidence and preparedness for staff.
Conclusions:
With this overall outcome, medical facilities will have more discernment on ways to improve their employees’ trust and confidence in performing their tasks and providing care while in a new environment. This will then be reflected in the care given toward patients in the future.
Keywords
Background
Within the past 18 years, the value of hospital expansions in the United States has nearly doubled to a monthly rate of 46 billion USD in 2019 (U.S. Census Bureau, 2021). These expansions require staff to successfully transition to a new location, navigate a new workspace, learn how to operate new technology, and continue to function as a team. Staff must overcome these challenges while maintaining confidence and performance in providing patient care. For this reason, it is beneficial to understand how to best prepare and provide support during this transition. Even though these new and expanded medical facilities allow opportunity for improvement, they are just empty spaces. It is up to the staff to bring high-level patient care and experiences to life.
Summa Health System has invested in patient expectations through a master facility plan with up to $350 million worth of facility improvements. The first phase includes the addition of a new seven-story tower to Summa Akron City Hospital, which opened in the summer of 2019. This addition was designed with women’s health in mind by bringing all maternity, newborn, and breast health services on Akron’s campus to one location. There is one floor dedicated to Labor and Delivery (L&D), containing 17 L&D rooms (includes four tub rooms), three operating rooms (ORs), 10 triage rooms, 20 Neonatal Intensive Care Unit (NICU) rooms, and nine perinatal rooms. A second floor is dedicated to postpartum care and contains 36 private patient rooms, a newborn observation area, and procedure rooms. This study focuses on preparedness of Summa Health L&D personnel before and after transitioning to a new facility. The objective is to provide insight regarding factors contributing to overall preparedness in addition to staff characteristics, training methods, and duration of training most beneficial for a unit move.
Introduction
Efforts to improve patient care and satisfaction with new medical facilities create the potential for disruption in patient care performance during the staff’s adjustment period to a new environment. Current literature regarding patient care transitions has focused primarily on critical care units (Intensive Care Units, Emergency Department, and NICUs) and has found that clear communication throughout the process of moving, encouragement for staff to be a part of the design process, timing of preparation, and simulation-based training to be effective in improving employee readiness for change (Knippa & Senecal, 2017; Lin et al., 2016; Magdzinski et al., 2018, Slosberg et al., 2018).
L&D units are unique in that care provided for patients is dynamic and can range from facilitating a healthy patient’s vaginal birth taking several to many hours or an acutely ill patient needing immediate delivery with surgical intervention (Ariadne Labs & MASS Design Group, 2017). Cesarean rates have been one parameter used to assess patient safety. Current literature has found that cesarean delivery (CD) rates vary widely across hospitals in the United States and that this variation is not explained by differences in maternal risk factors, suggesting the need for a better understanding of hospital factors, policies, and other potential reasons for variation (Kozhimannil et al., 2014). Other studies have focused on organizational silence regarding potential harms or near misses and lack of communication for improving patient safety (Sabol & Caughey, n.d.; Maxfield et al., 2013), with both topics consistently being addressed in provisions of care regarding maternal safety by the Joint Commission (2019).
Prior research has established an association between hospital design, environment, and patient outcomes (Laursen et al., 2014). In L&D units, several approaches have been taken to investigate patient safety, such as patient experience and discrimmination at the room level (Vedam et al., 2019), the impact of hospital/birth center design on clinical processes of care (Ariadne Labs & MASS Design Group, 2017; Austin et al., 2018), and communication/teamwork within units, but none have investigated how the staff’s comfortability in their workspace can be impacted when moving to a new building. This case study takes a different approach by investigating human factors as an opportunity for improvement, specifically staff preparedness and confidence in a new environment.
Methods
An online survey was distributed via work email addresses to all L&D staff before and after the move. The survey was administered 2 weeks prior to the move and 4 weeks following using an online platform called Survey Monkey. It included questions about demographics, level of participation in planning of the move, and other questions about the level of confidence they feel about the move and was constructed by Natalie Brzoza, MD (resident), and Derek Ballas, DO (Director of Virtual Care Simulation Lab). The survey was offered to all attendings, residents, nurses, certified nurse anesthetists, and support staff. All personnel were qualified to participate in the study. The areas that were assessed were demographics, level of confidence in providing patient care, level of confidence in patient care scenarios, methods of preparation, and time spent in preparation (Supplemental Material [Questionnaire pre- and postmove L&D].docx). Confidence was scored for patient care tasks, layout navigation, and emergency management on a 5-point Likert-type scale in which a score of 1 was denoted as not very confident and 5 was defined as very confident. A score of 2 was defined as somewhat not confident, 3 was neutral, and 4 was somewhat confident. Those who participated in the survey were entered into a raffle to win a gift card for their participation in both the pre- and postsurveys. The hospital required the physicians to participate in a guided tour of the entire new facility for 2–4 hours. Residents and nurses were obligated to participate in an in-person simulation training in the new unit. The 8 simulations lasted 3–4 hours and depicted patient scenarios including spontaneous vaginal delivery with quantitative blood loss, cord prolapse in perinatal, tub delivery, operative vaginal delivery with postpartum hemorrhage and cardiac arrest, fire in the OR, urgent broadcast code C (emergent cesarean), schedule CD with quantitative blood loss, and breech delivery of twins from triage (Supplemental Material [OB Sim Cases CSection Del].pdf). There was also a scavenger in the new facility, some staff were offered a role in the design team in the new facility, and there were also modules regarding equipment training and checklists expected to take 1–3 hours to complete. During the simulations, staff were expected to manage these conditions and treat them appropriately and efficiently by finding their way around the unit to find the supplies needed.
Results
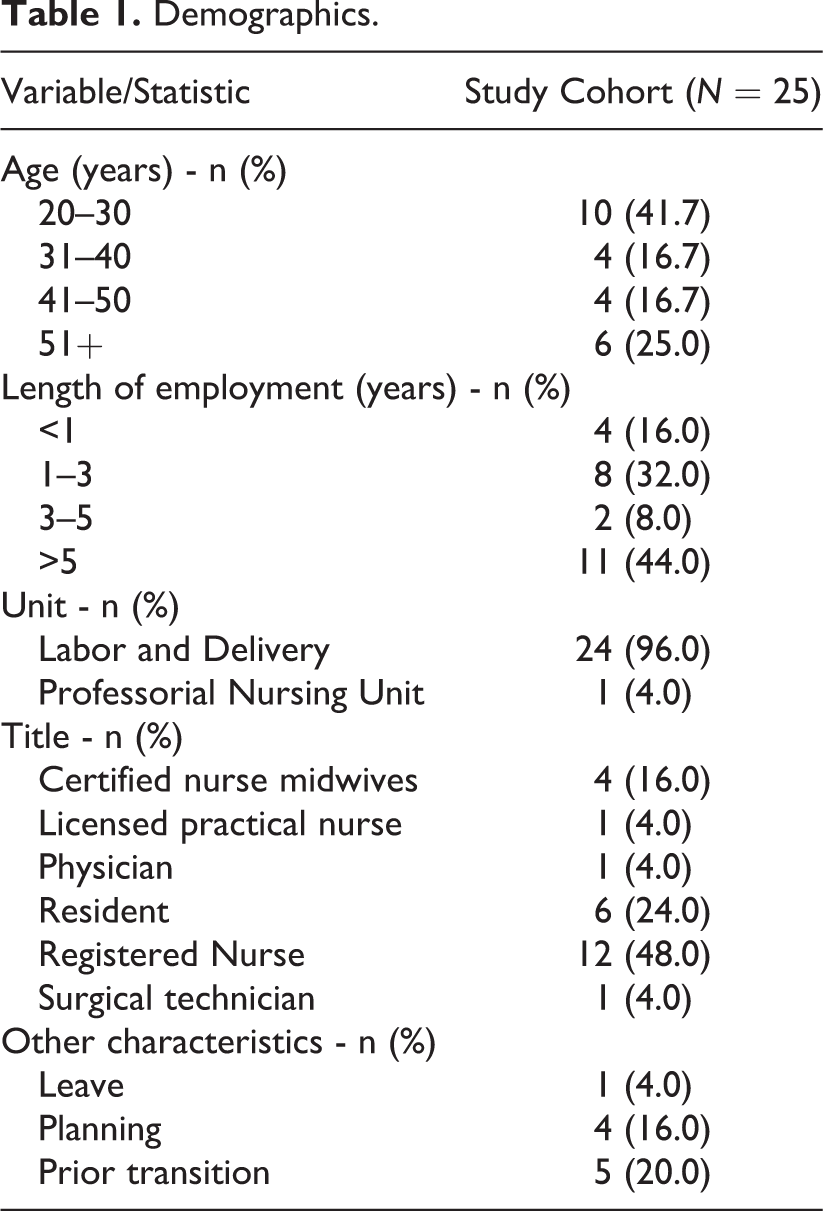
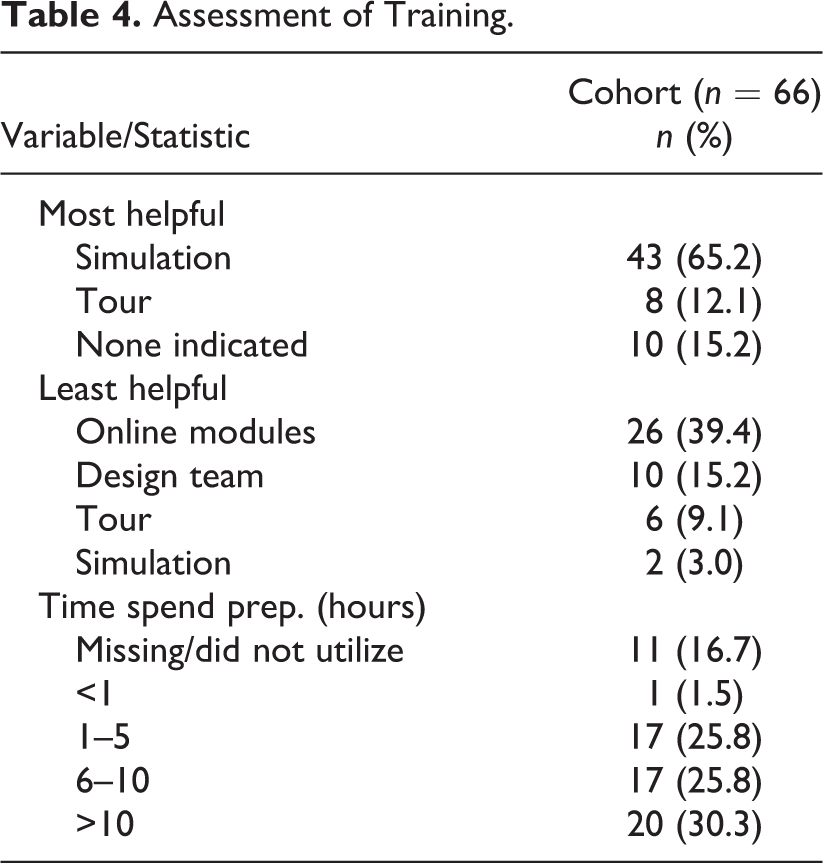
A total of 104 employees took part in the surveys. Forty-eight individuals completed the survey prior to the move, 31 completed the survey after the transition, and a total of 25 L&D staff completed both. Data from the participants who completed both pre- and postsurveys were imported into SPSSv25.0 software (IBM Corp., Armonk, NY). Demographics and assessment of training were summarized and compiled into tables based on age, length of employment, the unit they worked in, title, and other characteristics (Table 1). The overall mean confidence and the change in confidence were calculated for each participant. The overall mean confidence score decreased from before to after the transfer to the new unit (Table 2). The confidence summary by question revealed that the staff were not confident about their ability to find materials in the unit, navigating the unit, or performing emergent procedures (Table 3 and Figure 1). A survey of training methods was done to determine what methods were most and least successful in preparation training (Table 4). The change in confidence was tested for mean equality to zero via paired samples two-sided t test with a p < .05 considered statistically significant and is noted by bolded texts in the tables.
Demographics.
Overall Paired Confidence Summary.
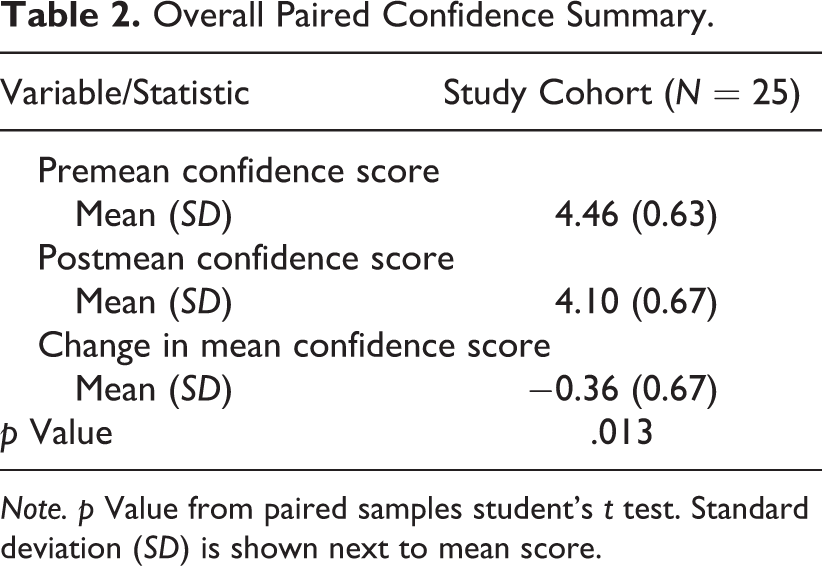
Note. p Value from paired samples student’s t test. Standard deviation (SD) is shown next to mean score.
Mean (SD) Confidence Summary by Question and Survey Response.
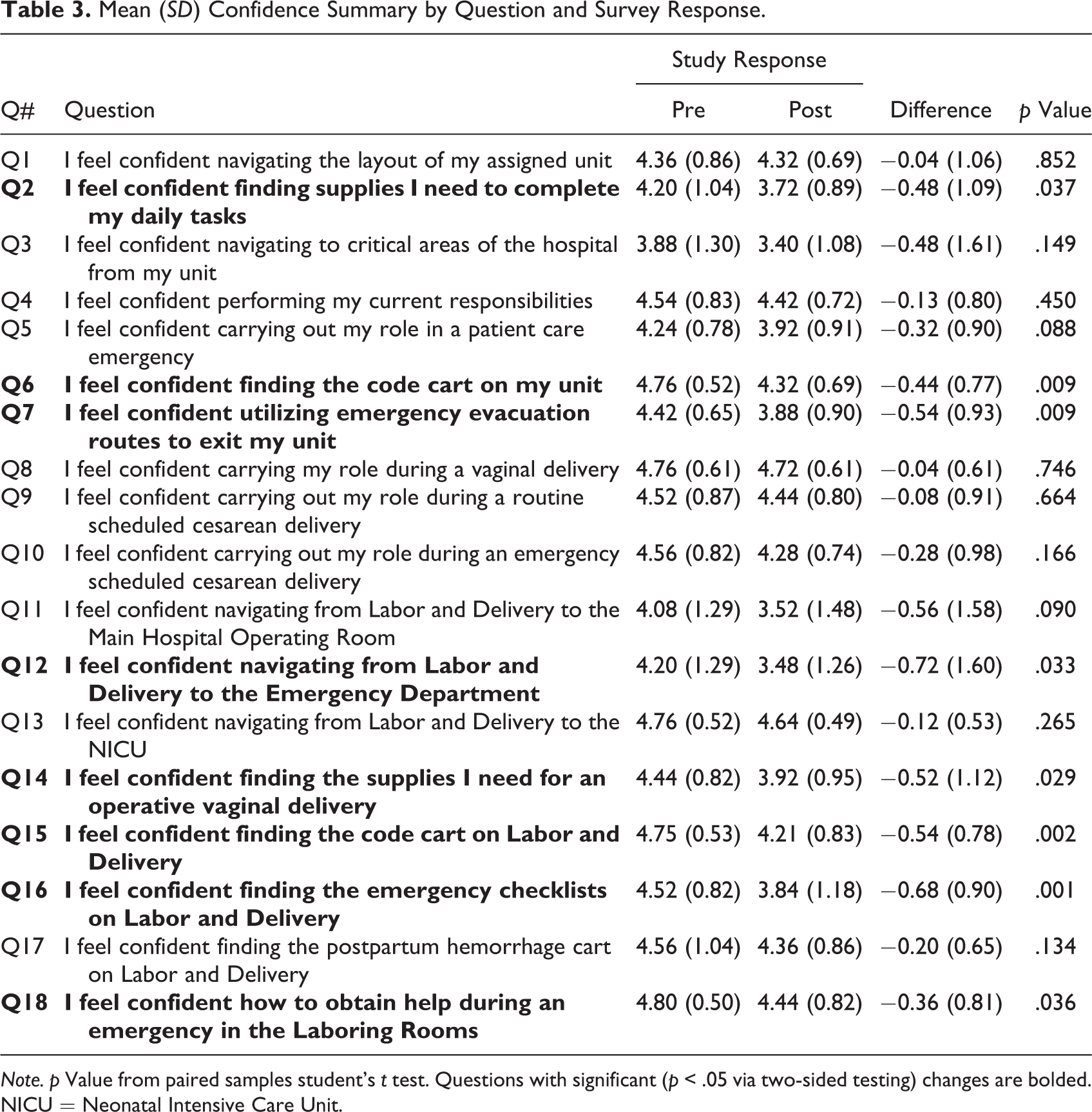
Note. p Value from paired samples student’s t test. Questions with significant (p < .05 via two-sided testing) changes are bolded. NICU = Neonatal Intensive Care Unit.
Assessment of Training.
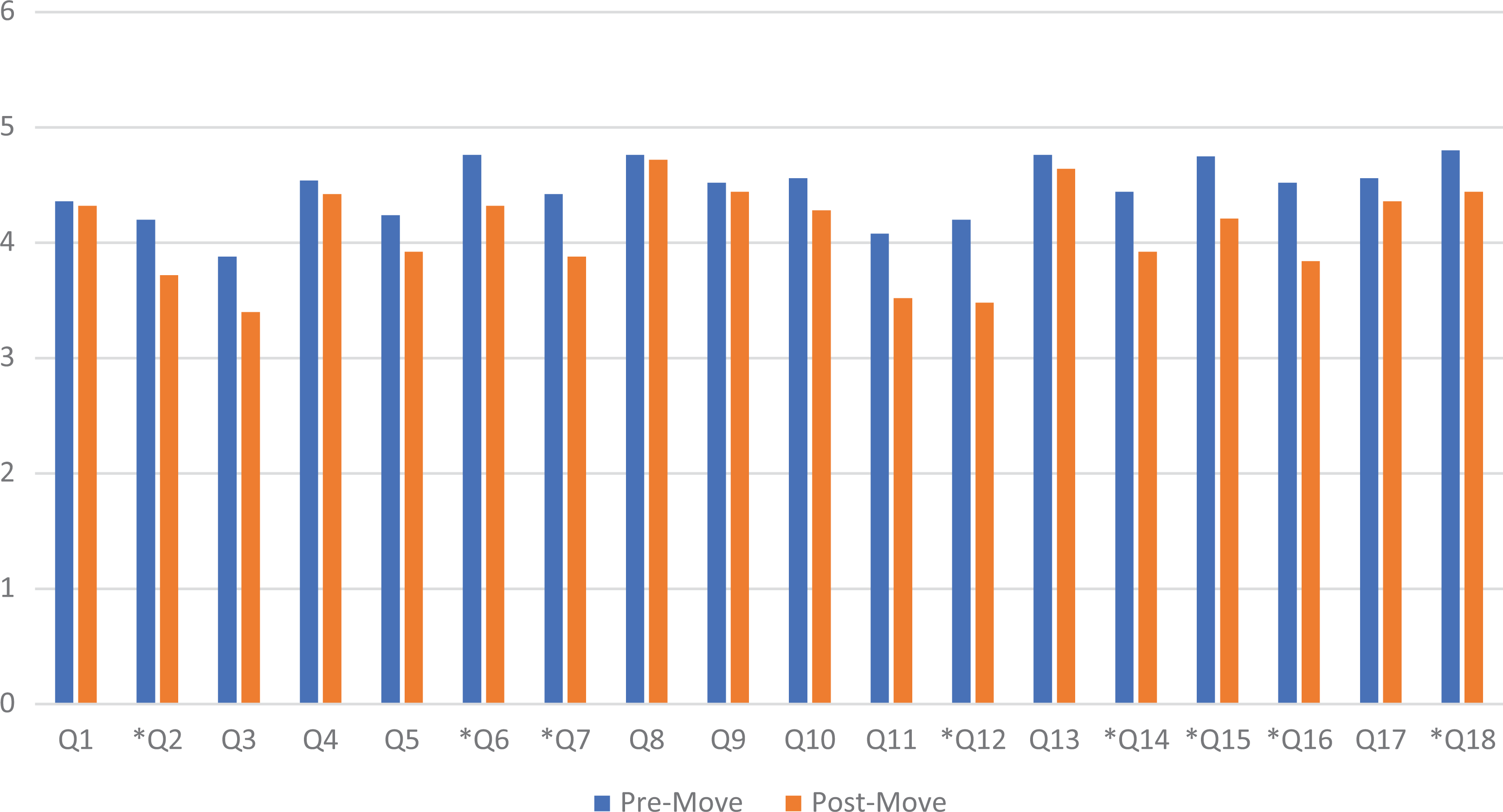
Mean (SD) confidence by question. Note. *Q# = This question was statistically different from pre-move to post-move.
Discussion
This case study demonstrated that employees did not feel as confident in their efficiency in the new L&D unit compared to their premove unit. This result could be due to the lack of time between the premove and postmove surveys given to the employees in the unit; however, this also represents their lack of confidence upon initial transition to the unit shown in Table 3 of the Results section. Twenty-five L&D personnel completed both the pre- and postconfidence questionnaires. Employees reported simulations as the most helpful tool for preparing them for the high-acuity scenarios in the new unit. The simulations given were a series of predetermined high-frequency and intense vaginal and cesarean scenarios: vaginal delivery with quantitative blood loss, cord prolapse in perinatal, tub delivery, operative vaginal delivery with postpartum hemorrhage and cardiac arrest, fire in the OR, emergency room urgent broad case code C, schedule CD with quantitative blood loss, and breech delivery twins from triage. Staff found the online modules to be the least helpful because many individuals reported that hands-on training would be more beneficial. Most participants spent more than 10 hours preparing for the transition to the new building.
One limitation of this study is the small sample size, with only 25 of 104 employees completing both the pre- and postmove surveys. Only 48 employees took the premove survey and 31 took the postmove survey. A potential explanation for low response rates could be that the surveys were given during the summer holiday season when many employees were absent on vacation. Other factors including employee background, age, and time spent within the unit as shown in Table 1 had no significant impact on overall confidence for employees. Additionally, not all staff were given the opportunity to provide feedback during the designing phase of the new facility, as stated in the methods, only a select few were chosen. One study shows that receiving feedback from employees is beneficial, as it builds trust and provides a conduit for communication between supervisors and employees (Auh et al., 2018). When employees can have that relationship with their supervisors, confidence by leadership has been shown to enhance team member confidence and performance (Owens & Keller, 2018). When employees are confident in performing their tasks, it will be reflected in the patient’s experience. One study affirms that confidence can affect performance when the efficacy expectation is strong and our abilities are well developed (Owens & Keller, 2018). In our experiment, the participants suggested that if they all were given early access to the building and more input from the nurses regarding the design and layout of the unit, they might have been more comfortable when transferring.
In the future, it may benefit employees to have a second postmove measurement survey about 8 weeks out from the move as well as give employees the platform to share feedback in the design of a new facility, thus securing a trusted relationship between employees and management, and their overall confidence. Giving patients the opportunity to provide feedback about their medical care and perceived employee confidence may provide valuable insights for future moves. For analytical purposes, it may be valuable to compare employee performance pre- and postsimulation. This could be done by running timed tests during simulations to show employees’ growth in efficiency, communication, and patient care during training. One study found that using timed tests, huddles, and whiteboards over a 6-month time line for employees in their L&D unit showed an overall positive response from patients and employees (O’Rourke et al., 2018).
Conclusion
In conclusion, the overall results show that employees were less confident or less prepared with their transition to their new unit. However, the data demonstrated that the L&D simulation in the new unit was the most helpful tool for preparation in transitioning to a new unit. With the overall data shown, this gives the leaders of L&D units more insight into ways to improve their employees’ trust and confidence in performing their tasks and providing care while in a new environment, so that it will be reflected in the care given toward patients in the future.
Implications for Practice
Identifies factors that aid L&D staff confidence in new environment.
Informs healthcare management decisions in regard to relocation to new unit.
Promote the use of L&D simulations to help staff become more comfortable with the equipment.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867211056075 - Assessing Preparedness of Labor and Delivery Personnel in Transferring to a New Unit
Supplemental Material, sj-pdf-1-her-10.1177_19375867211056075 for Assessing Preparedness of Labor and Delivery Personnel in Transferring to a New Unit by Cassandra Simmons, Claire Allison, Jayde Kee and Derek Ballas in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.