
Abstract
Purpose:
To evaluate the association between elements of the built environment and physician well-being using a scoping review.
Background:
Physicians currently report low work satisfaction, high burnout and depression. The built environment has been shown to affect well-being in the general population, but its relationship to physician well-being is not well understood. Gaining a better understanding of this relationship will allow for better evidence-based design for physician well-being.
Methods:
A scoping review of the literature was conducted of Scopus and PubMed databases using key words for (1) environmental variables such as “environmental design”; (2) physician terms, such as “doctor”; and (3) outcome measures of well-being, such as “burnout.” Studies were included if they had at least one measure of the built environment and one measure of physician well-being. Of 1,723 abstracts screened, 146 full-text articles were reviewed, leaving 16 articles to be included for data extraction.
Results:
Included studies were from all around the world, except for, notably, the United States. Robust interpretation of the data was challenging because of the lack of standardization in the assessment of environmental factors and physician well-being. Excessive noise was the variable most linked to well-being. Suitable surroundings, including lighting, furniture, and art, were also linked with satisfaction, but it was unclear whether there was an association with well-being.
Conclusion:
Understanding how environmental factors affect physician well-being is paramount but considerably understudied. Standardization of research approach should be developed in order to produce more robust research to create evidence-based designs for physician well-being.
Introduction
Physicians work closely with patients and other healthcare professionals in order to prevent, diagnose, and treat injuries and illnesses. There are over 18 million physicians worldwide (Crisp & Chen, 2014), including 1 million in the United States (Young et al., 2021). The immense burden placed on physicians due to the occupational stressors they endure has been well-documented. Long hours, overwhelming workloads, trying to achieve work–life balance, and the emotional weight of patient care are just a few of the stressors that physicians deal with on a daily basis (O’Dowd et al., 2018). Despite the inherent challenges of the profession, physicians are required to meet the demands of the job and provide exemplary care to their patients. As a result, physicians have historically been expected to be “superhuman” and sacrifice personal well-being for the sake of their profession and patients (LaDonna et al., 2021), leading to physician distress (T. D. Shanafelt, Dyrbye, et al., 2021) and meaningful reduction in work satisfaction (Friedberg et al., 2017). Additionally, compared to the general population, physicians report significantly higher levels of burnout (Mirrakhimov et al., 2013), depression (Pereira-Lima et al., 2019), and suicidal ideation (T. D. Shanafelt, Dyrbye, et al., 2021).
In response to these deleterious findings, several efforts have been initiated to improve physician well-being. Initial efforts mostly focused on stress management, wellness, and resiliency (Vasquez et al., 2021). Although some initiatives have proven to be successful in the short-term, the stigma regarding mental health among physicians and state medical licensure concerns have blunted the potential long-term benefits (Dyrbye et al., 2017). More recently, medical institutions have begun to institute system-based preventative interventions to combat the root causes of burnout (T. Shanafelt, Trockel, et al., 2021). It is notable that a recently published comprehensive evidence-based strategy guide for reducing burnout did not include any recommended changes to the physician’s physical work environment (Swensen & Shanafelt, 2020), even though several systematic reviews have shown that elements of the built environment, which includes interior and exterior spaces, are associated with well-being (Gianfredi et al., 2021; Lipson-Smith et al., 2021; Moore et al., 2018). Given that physicians are at high risk for reduced well-being due to environmental stressors (Alvaro et al., 2016), evaluation of previous research regarding the association between the built environment and physician well-being may inform the development of better sustainable solutions to physician burnout. Therefore, the purpose of this scoping review was to evaluate the published literature regarding the association between elements of the built environment and well-being among physicians.
Method
The review methodology was based on the current best practices for conducting scoping reviews (Peters et al., 2021). The goal of this scoping review was to evaluate the current state of the literature regarding the association between built environment and physician well-being.
Protocol
The protocol was developed using the scoping review methodological framework proposed by the Preferred Reporting Items for Systematic and Meta-Analysis (PRISMA) Protocols Extension for Scoping Reviews (Tricco et al., 2018). The PRISMA-ScR checklist can be found in the Supplemental Materials. The process began with identifying the research question and was then followed by a comprehensive search of studies in databases, selecting relevant studies, charting the data, and then summarizing and reporting the results, respectively. Charting the data consisted of recording the following information for all eligible studies: author(s), purpose of study, sample, relevant measures, and key findings.
Eligibility Criteria
Studies were deemed eligible for data extraction if they contained the following data points: (1) at least one measure of the built environment in a healthcare facility, (2) any measure of physician well-being, and (3) physician participants. The authors purposefully employed a broad search strategy in order to find all relevant studies. In an effort to increase consistency, two reviewers screened all 1,920 publications. Abstracts were judged for preliminary evaluation by both reviewers independently. The reviewers discussed the results and modified the screening and data extraction manual before the screening for this scoping review began. Both reviewers independently evaluated the titles, abstracts, and then full text of each publication identified by our searches for relevant publications. In cases of disagreement, the abstract was included in order to ensure inclusivity. For each included abstract, the full text was evaluated by both reviewers to evaluate final inclusion. In cases where it was unclear whether the sample contained physician input, study authors were contacted for clarification.
Search Strategy
A comprehensive search of the PubMed and Scopus databases was conducted in February 2022. The Scopus database was utilized because of its ability to search grey literature. A subsequent follow-up search was conducted in September 2022 to find any newly published articles, but none were found. Search terms included one term for a variable of built environment (“built environment” OR “physical environment” OR “healing environment” OR “evidence-based design” OR “interior design” OR “hospital design” OR “clinic design” OR “green space” or “noise”), a second search term to isolate studies of physicians (“physician” OR “clinician” or “doctor”), and a third to find well-being (“health” OR “well-being” OR “wellness” OR “quality of life” OR “satisfaction” OR “depression”). The references of included studies were also examined for any additional resources that were not found in the database searches. Upon secondary review of the outcomes utilized by the included articles, we became aware that burnout was regularly used to assess physician well-being, but it had not been included in our initial search. Therefore, we conducted subsequent searches of both databases to include only “burnout” as the well-being variable, without the previously included variables. Our search yielded 18 articles, none of which met the inclusion criteria. The search included studies from the last 20 years (February 2002 to February 2022). Articles were included from any country as long as they had a searchable abstract in English, and, if necessary, could be translated using Google translate in order to maintain the maximum breadth of the search. Only the study from Brazil (Marques et al., 2018) had to be translated.
The Covidence citation program was used to organize and evaluate articles for inclusion (Cleo et al., 2019). Following the initial search, 1920 articles were found. Duplicative titles were removed (n = 197), which left 1,723 articles to consider for review. The titles and abstracts of all 1,723 articles were evaluated to determine if they contained the three primary study parameters: (1) built environment component, (2) physician sample, and (3) measure of well-being. The initial review of titles and abstracts was intentionally inclusive in order to ensure full sampling of articles. If either of the reviewers voted for inclusion, then that article was included for full-text screening. Following the review of abstracts, 143 articles remained for full-text review, of which 16 met the inclusion criteria. Full-text articles were accessed via (1) free full text, (2) various university libraries accessed by the authors, (3) internet search, and (4) author request. Full-text versions of all 143 articles were accessed. Upon review of references of included studies, no additional studies were included, such that the total number of studies included for review was 16. Discarded articles were reviewed once more to confirm exclusion before the analysis was complete. A flow diagram of the article selection process is summarized in Figure 1.
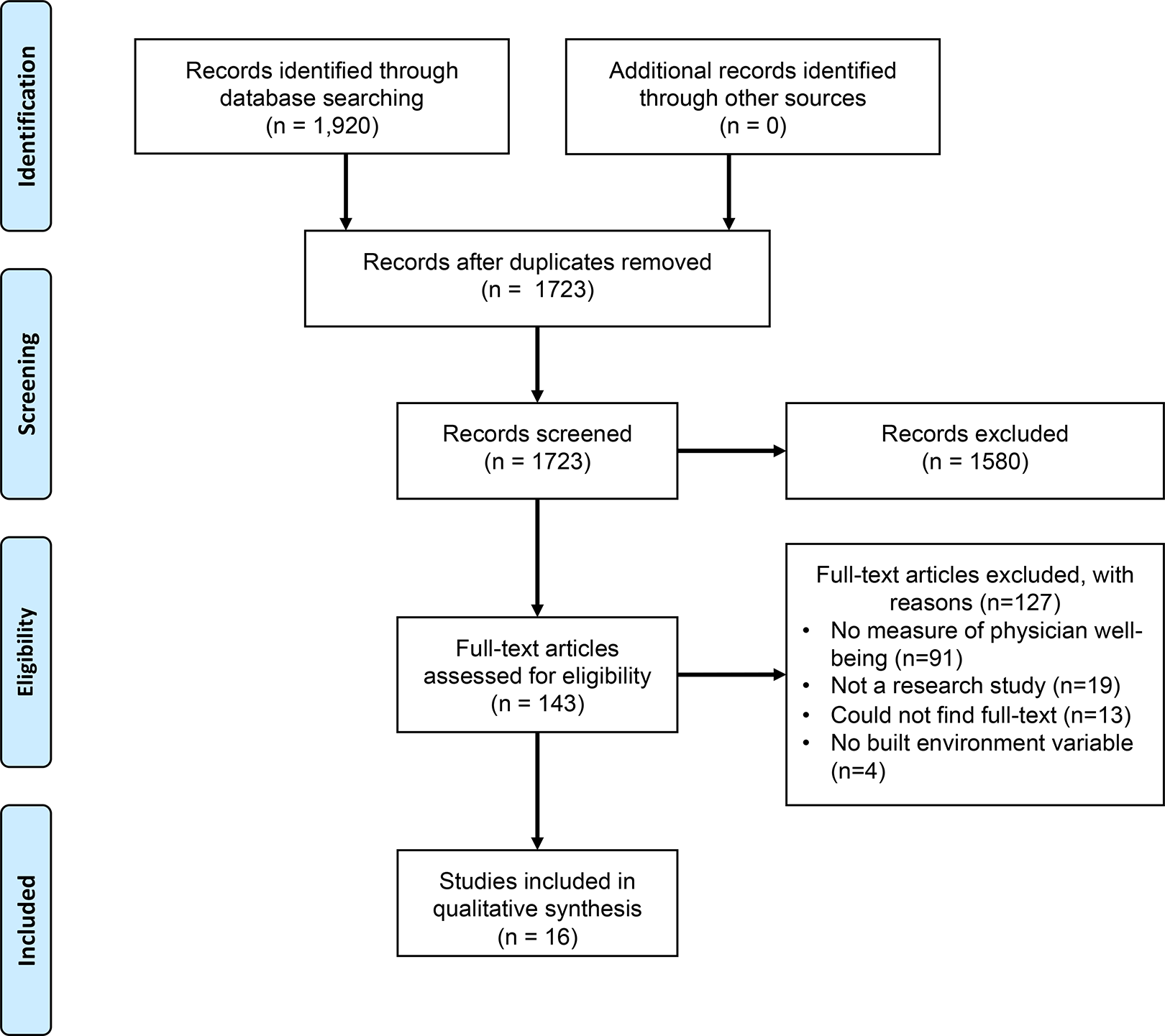
PRISMA flowchart for study selection.
Data Extraction
The goal of this scoping review was to evaluate the association between the elements of built environment and physician well-being. Initial data extraction charts were developed according to the Population/Concept/Context guidelines recommended by the JBI Scoping Review Methodology Group (Tricco et al., 2018). Population elements included physician demographics and type of healthcare facility. The concept examined was that there may an association between built environment and well-being, so any parameters related to the built environment and well-being were extracted, as well as the source of the measurement. The geographic location was also extracted in order to provide context and summarize the breadth of the literature. Because this was an exploratory scoping review, data extraction item lists were refined as data extraction took place, with new variables being created under the headings of “Built Environment Variable” and “Measure of Well-being.” Therefore, in addition to demographic information, all variables related to interior or exterior environment, as well as physician well-being, were extracted independently by both reviewers. The extracted data were then compared to ensure synchronicity.
Data Synthesis
Each article was reviewed by two reviewers, and a data-charting form was developed to organize the data. The two reviewers charted data independently. Data and results were discussed continuously and the data-charting form was updated as necessary. Inconsistencies were discussed and resolved to verify data. The collected data points were study location, sample size, sample demographics, type of healthcare facility, research methodology, built environment variable(s), measure(s) of well-being, and relevant findings. Each article was reviewed to describe any associations between the elements of the built environment and physician well-being.
Study Quality
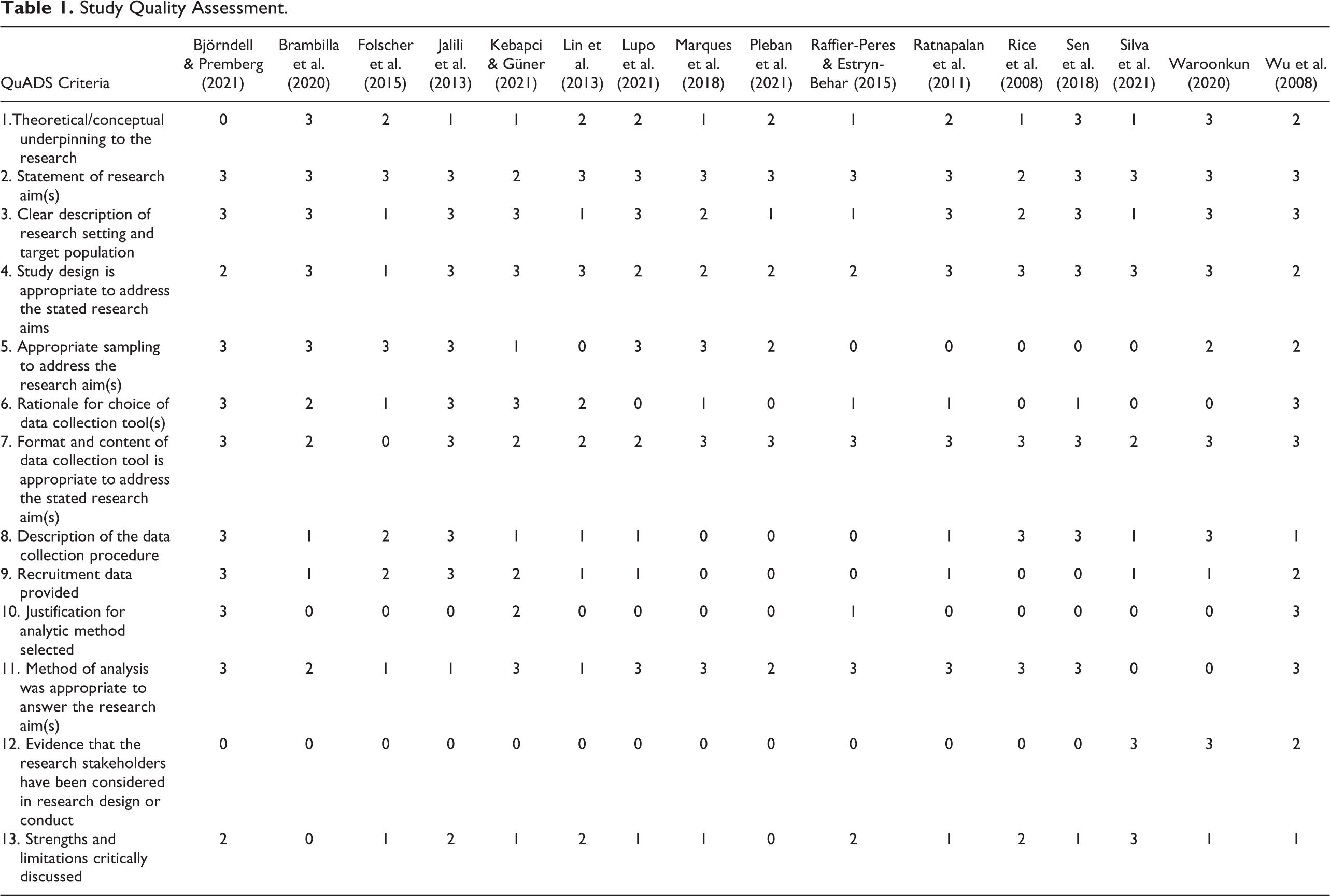
Critical appraisal of the individual sources of evidence was conducted using the Quality Assessment with Diverse Studies (QuADS), which has been shown to be a reliable and valid evaluation tool for heterogeneous studies (Harrison et al., 2021). Evaluations were done in duplicate by both reviewers. Disagreements were discussed until consensus was reached. Study quality overview can be found in Table 1.
Study Quality Assessment.
Data Analysis
Because this is a new field with limited findings, the data were analyzed following a narrative outline. Following initial narrative descriptions, common themes and findings were highlighted, as well as best practices for future variable capture.
Results
Setting and Sample
An overview of the included studies can be found in Table 2. Of the sixteen studies that met the inclusion criteria, all had been found in peer-reviewed journals. Nine were conducted in Europe (Björndell & Premberg, 2021; Brambilla et al., 2020; Rice et al., 2008; Lupo et al., 2021; Pleban et al., 2021; Raffier-Peres & Estryn-Behar, 2015; Ratnapalan et al., 2011; Sen et al., 2018; Silva et al., 2021), three in East Asia (Lin et al., 2013; Waroonkun, 2020; Wu et al., 2008), two in the Middle East (Jalili et al., 2013; Kebapcı & Güner, 2021) and one each in Brazil (Marques et al., 2018) and South Africa (Folscher et al., 2015). Notably, none of the studies that met the inclusion criteria had been conducted in the United States, indicating a significant gap in the literature.
Overview of Included Studies.
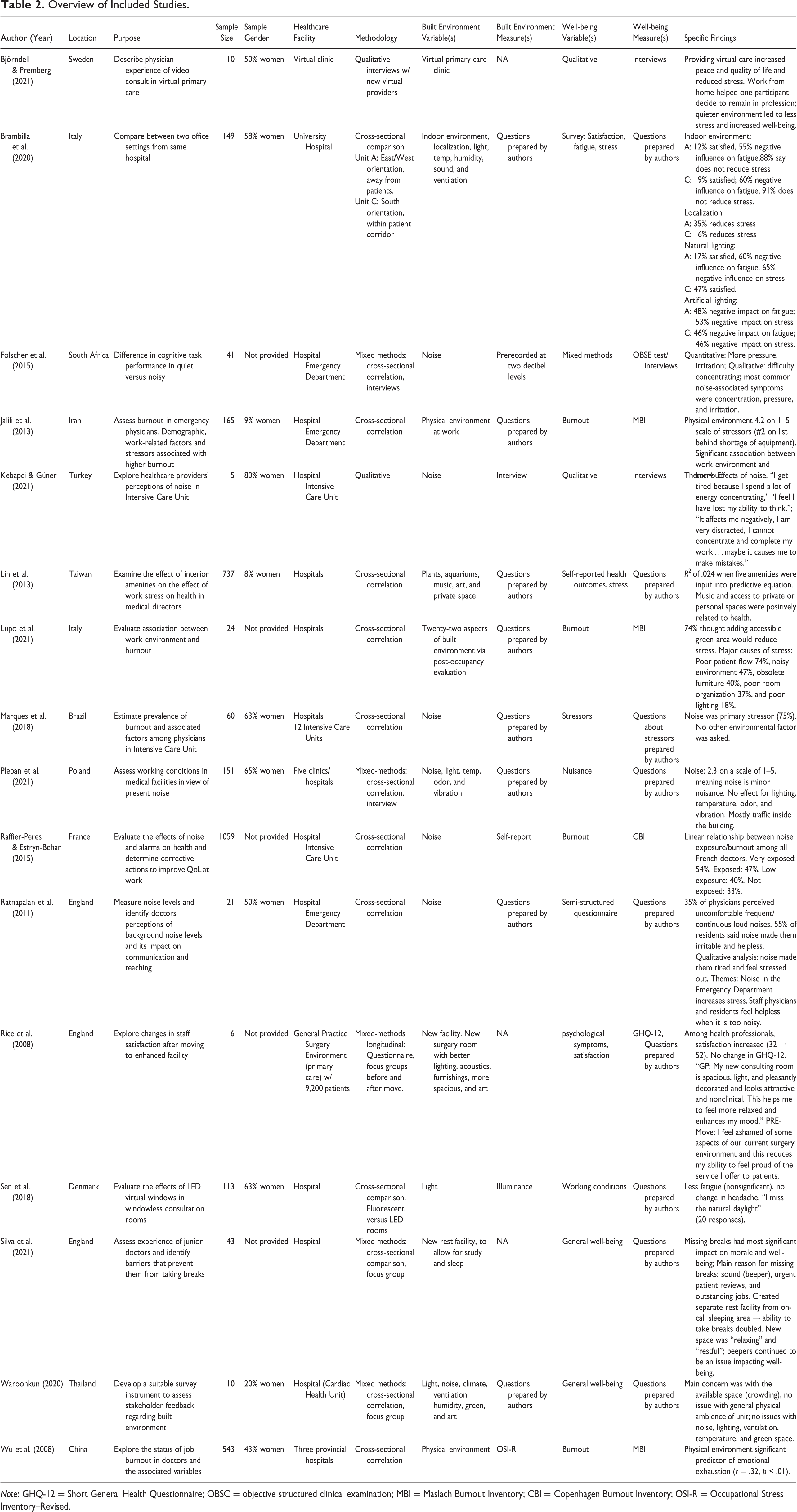
Note: GHQ-12 = Short General Health Questionnaire; OBSC = objective structured clinical examination; MBI = Maslach Burnout Inventory; CBI = Copenhagen Burnout Inventory; OSI-R = Occupational Stress Inventory–Revised.
Thirteen of the studies were conducted in hospital settings, one included combined data from physicians in clinics and hospitals (Pleban et al., 2021), one included data from a general practice with surgical capabilities (Rice et al., 2008), and one reported from a virtual primary care facility (Björndell & Premberg, 2021).
Methodology
The sample sizes of the included studies varied greatly from 6 to 1,059 participants (mean ± SD: 226 ± 337). The sum of included sample sizes was 3,137 physicians. Ten of the studies included physicians only, whereas the remaining six studies included a mix of medical personnel, from which the results were stratified by healthcare profession, such that physician-only data could be extracted.
The methodologies utilized also varied greatly, with all but one of the studies using some type of cross-sectional design. Qualitative-only methodologies were implemented in two studies (Björndell & Premberg, 2021; Kebapcı & Güner, 2021) to evaluate physician perceptions of the association between built environment and well-being. Four studies used mixed-methods designs, utilizing surveys and interviews, to explore how the built environment was linked to physician satisfaction (Folscher et al., 2015; Pleban et al., 2021; Silva et al., 2021; Waroonkun, 2020). Two studies used cross-sectional comparison design to compare well-being across two different built environments (Brambilla et al., 2020; Sen et al., 2018), and seven used cross-sectional correlations to evaluate the relationship between exposure to various built environment elements and well-being (Jalili et al., 2013; Lin et al., 2013; Lupo et al., 2021; Marques et al., 2018; Raffier-Peres & Estryn-Behar, 2015; Ratnapalan et al., 2011; Wu et al., 2008). One study used a longitudinal mixed-methods design with surveys and interviews, in which the evaluations were conducted before and after moving to a newly constructed hospital unit (Rice et al., 2008).
One of the challenges faced in creating a narrative of the included results was the lack of standardization in measures for the built environment. The primary built environment variable evaluated was noise. Five studies assessed noise as the lone built environment variable (Folscher et al., 2015; Kebapcı & Güner, 2021; Marques et al., 2018; Raffier-Peres & Estryn-Behar, 2015; Ratnapalan et al., 2011). However, among those studies, one prospectively applied a standardized dose of noise in a surgical setting (Folscher et al., 2015), whereas the other four each used a different survey of perceived noise that had been created by the authors. Other variables assessed were physical environment, light, temperature, humidity, sound, ventilation, plants, art, private space, and furnishings. Only one of the studies used a validated measure of the physical environment: the Occupational Stress Inventory–Revised (Wu et al., 2008). A comprehensive built environment assessment tool based on postoccupancy evaluation created by Lupo et al. (2021) merits further investigation as a standardized built environment evaluation.
Similarly, the assessments of physician well-being varied greatly. Four studies assessed well-being via the three domains of burnout (emotional exhaustion, depersonalization, and low personal accomplishment) through utilization of the Maslach Burnout Inventory (MBI; Jalili et al., 2013; Lupo et al., 2021; Wu et al., 2008) or Copenhagen Burnout Inventory (Raffier-Peres & Estryn-Behar, 2015). The two qualitative studies used semi-structured interviews to explore feelings of well-being (Björndell & Premberg, 2021; Kebapcı & Güner, 2021). One study used the Short General Health Questionnaire (Rice et al., 2008) and another used the Objective Structured Clinical Examination to evaluate pressure and irritation (Folscher et al., 2015). The others created quantitative surveys specifically for the purpose of their study.
There was substantial variability in the methodologies used, both in the research strategies and the assessment tools utilized to measure the built environment and well-being. Nearly all of the studies were cross-sectional and only one was conducted in a primary clinic setting, limiting the strength of the conclusions and the generalizability of the results.
Results
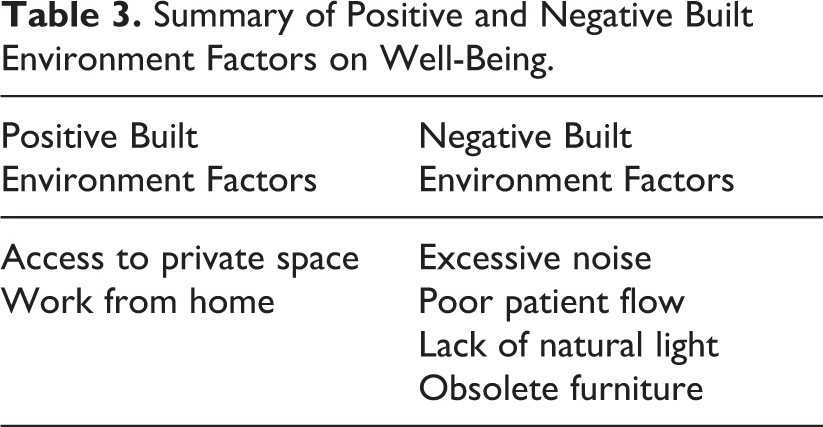
Although it was challenging to compare across studies due to variety of methodologies, the findings clearly indicate that several factors of the healthcare built environment have meaningful impact on physician well-being. A summary of the positive and negative built environment factors can be found in Table 3. The Björndell & Premberg study (2021) a qualitative study that was the only included manuscript that evaluated physician perceptions of providing virtual care from home, found that those physicians reported increased peace and quality of life, and reduced stress. One major finding was that the home environment was quieter, which led to reduced stress and increased well-being. One of the participants stated that changing from hospital-based work to home-based work helped them decide to remain in the profession.
Summary of Positive and Negative Built Environment Factors on Well-Being.
As stated previously, noise was the exclusive built environment variable in five studies, which included both qualitative and quantitative evaluation. Studies that included a qualitative component found that physicians perceived that noise had a negative impact on job performance and quality of life. One representative quote was, “I get tired because I spend a lot of energy concentrating” (Kebapcı & Güner, 2021). Physicians who were interviewed after both quiet and loud shifts found that the most common noise-related complaints were feelings of pressure and irritation (Folscher et al., 2015). Physicians also reported feeling helpless when the emergency department was noisy, and that the noise makes them feel tired and stressed (Ratnapalan et al., 2011). Cross-sectional correlations found similar results, with 75% of physicians indicating that noise caused an increase in stress in one study (Marques et al., 2018), and 55% of physicians reporting that noise made them feel irritable and stressed in another (Ratnapalan et al., 2011). A large study (n = 1,059) in France found a correlation between perceived noise and burnout. Symptoms of burnout were found in 54% of physicians who reported being “very exposed” to noise, compared to only 33% in physicians who did not feel exposed to noise.
Four studies provided results of comparisons. Physician well-being following patient visits in a room with fluorescent lighting was compared to well-being following visits in a room with two high luminescence LED “virtual windows.” The primary responses were that the physicians missed the natural light and that they lacked fresh air, and there was a small, nonsignificant lower fatigue in the LED condition (Sen et al., 2018). Another study compared physician well-being in two different units that had different levels of light and noise (Brambilla et al., 2020). One unit was located away from the patient corridor and had an east/west orientation, where there was a quieter and more private environment with lower light. The other unit was located within the patient corridor and had a south-facing orientation, where there was more natural light but a louder environment. A majority of the physicians (∼90%) reported that neither of the environments reduced stress. However, 35% of the physicians reported that the unit that was located away from the patient corridor reduced stress compared to 16% for the unit located in the patient corridor, indicating that a quieter work environment may reduce stress. Nearly three times as many physicians were satisfied with the amount of light in the south-facing unit; respondents from the unit with less natural light felt that it had a negative impact on fatigue (60%) and stress (65%).
Physician well-being was also evaluated before and after moving to a new facility, where the new facility had better lighting, acoustics, furnishings, and art (Rice et al., 2008). Satisfaction increased, but there was no improvement in the General Health Questionnaire scores. Qualitative analysis found that the physicians felt better in the new facility, with one physician stating “my new consulting room is spacious, light, pleasantly decorated, and looks attractive and non-clinical. This helps me to feel more relaxed and enhances my mood.” However, because this study assessed all clinic staff, the data regarding physician perceptions were highly limited. Residents were asked about their well-being following the establishment of a new relaxation center that was quiet and had low light for resting and/or studying (Silva et al., 2021). They found a large increase in residents’ ability to rest during breaks and that the residents found the new space to be relaxing and restful. Despite creating a new rest space, a major concern that remained unchanged was the noise and disruption caused by the continued use of beepers in the rest facility for on-call residents. These studies suggest that natural sunlight, sound, space, privacy, and furnishings likely have a positive impact on physician well-being, whereas adding LED lights to simulate natural light is likely insufficient.
Two studies of physician well-being that used the variable “physical environment” to assess the built environment found associations between the two variables. Wu et al. (2008) found that self-reported physical environment was a significant predictor of emotional exhaustion. Jalili et al. (2013) found that physical environment was reported as a stressor on most shifts and was ranked second for causes of stress among physicians. They also found correlations between physical environment and each of the three domains of the MBI.
Four studies evaluated multiple individual components of the built environment. Two of the studies, conducted in Poland and Thailand, found virtually no association between measures of the built environment and well-being, except for the minor nuisance of crowding/foot traffic (Pleban et al., 2021; Waroonkun, 2020). It is unclear if physicians in these two studies are satisfied by the built environment because (a) the built environment was conducive to well-being or (b) physicians have become used to working in poor built environments. Another study found that plants, aquariums, music, art, and private space were a significant predictor of physician health, although the explained variance was very low (Lin et al., 2013). One other study found that major stressors for physicians were poor patient flow (74%), noisy environments (47%), obsolete furniture (40%), poor room organization (37%), and poor lighting (18%; Lupo et al., 2021). Additionally, 74% of physicians reported that adding an accessible green area into the building design would reduce stress (Lupo et al., 2021). These contradictory findings illustrate the inherent challenges of assessing built environment and physician well-being in hospitals without standardized, validated assessment tools. Due to the lack of consistency in all of the measures and the fact that they were rarely validated, it is not yet possible to make strong conclusions based on the included data.
Discussion
The primary findings from this scoping review were that (1) built environment parameters such as noise, sunlight, and facility design were associated with physician well-being; (2) the heterogeneity and lack of validation among the measures of both the built environment and physician well-being make it challenging to collectively evaluate the totality of the evidence; and (3) there was a striking lack of research regarding well-being among physicians based in the United States.
The findings regarding the positive association between the built environment and workplace well-being support similar findings among a range of professions. Previous studies have found an impact of noise exposure on well-being among nurses (McCullagh et al., 2022), access to sunlight for office workers (Boubekri et al., 2014) and general work environment (Kropman et al., 2022; Parra-Giordano et al., 2022), among a wealth of other workplace studies. Given the rising impact of burnout among physicians in the United States (Niven & Sessler, 2022), and the clear evidence that workplace environment has an impact on well-being, it is essential that more research is conducted to clarify the elements of the built environment that may have the greatest impact on physician well-being, as well as those elements that may be modifiable. During our evaluation of the literature, it was striking that so many articles were excluded because they did not assess physician well-being. There are a multitude of studies regarding the well-being of patients and other staff, but physicians were largely left out. This scoping review illuminates how well-being of physicians has been understudied, likely because physicians are often expected to be superhuman.
In order to fully evaluate this phenomenon, it is imperative that researchers are able to compare across studies. This scoping review illustrated the extreme heterogeneity in assessment tools that makes the synthesis of research findings difficult. The majority of the included studies utilized nonvalidated assessment tools for built environment and well-being. Future research regarding the built environment of healthcare facilities should utilize validated measures. One promising assessment tool may be the Facility Evaluation Tool for outpatient and community health centers that was created by the Center for Health Design (2015). Similarly, the postoccupancy evaluation questionnaire employed by Lupo et al. (2021) may also be a viable assessment tool that can be modified to fit various healthcare facilities. Likewise, the most used measure of well-being among physicians was the MBI. Although extensively validated, the MBI only assesses the wellness components emotional exhaustion, depersonalization, and personal achievement, which are negative aspects of well-being. A more comprehensive measure of positive well-being such as the Mental Health Continuum may better capture varied aspects of physician well-being (Lamers et al., 2011).
Considering that there are approximately 1 million practicing physicians in the United States (Young et al., 2021), and that burnout has caused tremendous strain on the profession, it is also notable that this scoping review found no studies of the impact of the built environment on physicians in the United States. Furthermore, only two of the included studies evaluated clinic built environment. In the United States, nearly 10% of patients receive their healthcare from Federally Qualified Health Centers. As such, there is a clear need to conduct more research to evaluate built environment factors in the United States, and specifically in clinics and rural health centers. Furthermore, because of the historical underrepresentation and disinvestment of non-White physicians (Yancy & Bauchner, 2021), these studies of health centers in the United States should also include race/ethnicity as a determinant to evaluate the association of race/ethnicity and built environment variables.
One of the primary limitations of this scoping review is that the search may not have captured sources that found negative findings, possibly leading to selection bias. Furthermore, several studies referred to hospital “staff” which may have included physicians. When the results were not differentiated by profession, this review was not able to extract that data. Because this direction of study is relatively new, and the terminology has not yet been standardized, it is possible that our search missed some relevant articles that used terms the authors were not familiar with. Many search terms were included, leading to nearly 2,000 screened abstracts, but it is possible that there are other studies that could have been included.
Physicians are currently experiencing high levels of burnout and depression, leading many to retire, quit, or avoid the field altogether. In order to ameliorate the physician experience, many researchers and practitioners are searching for evidence-based strategies to improve physician quality of life. One such method that would lead to sustained improvements may be through the modification of the built environment. The preliminary findings summarized in this study illuminate the potential for the built environment to improve physician well-being, while also identifying several gaps in the literature that should lay the groundwork for exploratory studies to evaluate best practices to improve physician quality of life. Further research should be done to (1) validate measures of healthcare built environment characteristics, (2) standardize the use of a positive well-being assessment for physicians so that studies can be easily compared, (3) conduct research regarding the association between the built environment and physician well-being in the United States, and (4) conduct controlled interventions to assess the impact of various built environment components on physician well-being.
The search protocol can be accessed in the Supplemental File.
Implications for Practice
Positive built environment components such as access to quiet, natural sunlight, efficient office organization, and access to privacy improve physician well-being.
Given the high rates of physician burnout, physician well-being should be a primary consideration when designing healthcare spaces.
Reducing noise exposure should be a primary consideration when designing healthcare spaces.
More research needs to be done to evaluate the reliability and validity of healthcare built environment variables.
No research on this topic in United States clinics has been published, indicating a significant research need.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231151687 - Exploring the Association Between the Healthcare Design Elements and Physician Well-Being: A Scoping Review
Supplemental Material, sj-pdf-1-her-10.1177_19375867231151687 for Exploring the Association Between the Healthcare Design Elements and Physician Well-Being: A Scoping Review by Amerigo Rossi, Nina Brojan Heyman, Mónica Ortiz Rossi, Sarah Wolf and Takeesha White in HERD: Health Environments Research & Design Journal
Footnotes
Author’s note
The ideas in this article are those of the authors and do not necessarily represent policy of the American Medical Association.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.