
Abstract
Objective:
This study investigated issues related to noise, lighting, and temperature in trauma rooms that impact patient care and staff performance.
Background:
Uncontrolled sensory stimuli can hinder healthcare delivery quality in trauma rooms. High noise and temperature levels can increase staff stress and discomfort as well as patient discomfort. Conversely, proper lighting can decrease staff stress levels and reduce burnout. Sensory overload in trauma rooms is a crucial concern, but no studies have been conducted on this issue.
Method:
Using a convenience sampling method, 65 trauma team members (e.g., surgeons, physicians, nurses) from six Level I trauma centers in the United States were recruited to participate in 20 focus groups. Focus groups were semi-structured and 1 hr long.
Results:
Staff covered issues related to communications and disruption from noise sources (e.g., equipment, conversations). Having control over lighting allows staff to change light intensity and facilitate their work during the resuscitation. A well-maintained temperature can provide patient comfort or reduce risk of hypothermia, given that patients can lose body heat rapidly due to loss of blood.
Conclusion:
Excessive sensory stimuli can result in disrupted communication, fatigue, and stress, making staff susceptible to errors. Staffs’ control over environmental conditions may lead to a more efficient, comfortable, and safer environment. Technology should be reliable and flexible to facilitate this.
Keywords
Introduction
Trauma rooms, where rapid assessment of injuries and effective trauma resuscitations are crucial to prevent deaths, often cause staff to experience sensory overload. As environmental sensory stimuli in acute care environments, noise, lighting, and temperature have garnered much attention for their positive and negative impacts on patient care. In complex environments such as trauma rooms, intensive care units (ICUs), and operating rooms (ORs), noise, light and temperature affect not only patients but also providers and the care they deliver (Bayramzadeh, Ahmadpour, Aghaei, 2021).
Studies show that high noise levels from equipment in ORs can increase staff stress levels (Ward et al., 2020) and hinder staff communication, concentration, and coordination during surgery (Bayramzadeh & Aghaei, 2021; Keller et al., 2016; Padmakumar et al., 2017; Pennathur et al., 2013). Similar issues such as high ambient noise and noise-based interruptions are observed in hospital sonography environments which result in a high cognitive load for staff (Stigall-weikle et al., 2022). Communication is a key component of patient safety during surgery (Katz, 2014), and communication failures can lead to procedural delays and inefficiency (Halverson et al., 2011).
Similarly, constant environmental noise in emergency departments (EDs) results in staff physical and emotional exhaustion and increased interruption and distractions (Welch et al., 2013; Zamani, 2019). High noise levels impair communication, lead to fatigue, reduce patient safety, decrease staff satisfaction, and hinder healthcare delivery quality as a source of distraction in similar environments, including trauma rooms (Basner et al., 2014; Bayramzadeh, Anthony, et al., 2021; Hasfeldt et al., 2010; Terzi et al., 2019).
Additionally, lighting has significant implications for complex healthcare environments. For example, dimmed light, as an intervention in quiet time protocols, can decrease nurses’ stress levels (Riemer et al., 2015). Daylight in ICUs can reduce staff stress and burnout, resulting in fewer medical errors (Gharaveis et al., 2020). Further, proper adjustments to lighting offer behavioral advantages. For example, dimmed lights can promote quietness (Bayramzadeh, Ahmadpour, Aghaei, 2021; Davis et al., 2020). Balancing illumination that supports both staff and patient needs can be an environmental design challenge that requires consideration (Zores-Koenig et al., 2020). Providing patients with lighting control in patient rooms reduces cognitive demands on nursing staff, reduces disruptions, and increases patient satisfaction (Lavender et al., 2020). Proper lighting provides an improved and invigorating atmosphere to minimize work exhaustion and improve productivity (Idkhan & Baharuddin, 2019).
Temperature is another sensory stimulus in complex healthcare environments that impacts patients and staff. Elevated temperature levels in ORs can negatively impact both staff self-rated subjective performance (Hakim et al., 2018) and executive functioning (Ward et al., 2020). Further, staff can perceive workload as higher than usual when working in a warm OR (Ward et al., 2020). Temperature plays a significant role in environments such as trauma rooms and ORs where patients are susceptible to hypothermia (Alam et al., 2018; Engorn et al., 2017). In trauma rooms, patients are usually unclothed for examination when their injuries include active and profuse bleeding. Environmental temperature factors into maintenance of core body temperature to avoid hypothermia which occurs when core body temperature drops below 95 °F. Common among trauma patients, hypothermia contributes to increased mortality rate (Lapostolle et al., 2021). In ORs, the frequency of hypothermia in infants during cesarean procedures increases at a colder temperature, and the average body temperature of infants is lower in colder settings (Duryea et al., 2016). Based on the impacts of temperature variability on staff and patients, balancing temperature in trauma rooms is challenging (Uścinowicz et al., 2015).
Excessive sensory challenges can create an unsafe environment by causing distraction and interruptions for healthcare staff (Hogan & Harvey, 2015). Despite its significant impact on both staff and patients from safety, efficiency, and overall perceived experience perspectives, the role of sensory stimuli in trauma rooms is understudied. This study aimed to investigate issues related to noise, lighting, and temperature in trauma rooms that impact patient care and staff performance.
Method
This qualitative study used focus groups to collect data about sensory stimuli in Level I trauma rooms from the staff’s perspective. Since sensory stimuli in trauma rooms are understudied, focus groups are deemed helpful by allowing participants to share and discuss their opinions to develop an in-depth, shared understanding of the issues being discussed (Stewart & Shamdasani, 2014). This research complied with the tenets of the Declaration of Helsinki and was approved by the institutional review board. Informed consent was obtained from each participant.
Sample Selection
A convenience sampling method was used to recruit trauma staff with different roles. A sample of hospitals with a Level I trauma center located in various geographic locations was contacted to represent a larger population. Among those hospitals, six agreed to participate in the study. The participating hospitals were from five states in the United States. All facilities were large urban teaching hospitals with at least six trauma rooms. They were between 3 and 20 years old. Four facilities included enclosed rooms, and two included open bays. Each participating hospital’s administration distributed email invitations from the research team to staff members working in the trauma bay and ED. Among the invitees, 65 staff—including all target roles including but not limited to Emergency Medicine (EM) physicians, surgeons, nurses, and technicians—participated in the focus groups. Each focus group in each institution included participants representing different specialties. Based on the number of participants, 20 online focus groups were conducted. Although 115 volunteers agreed to participate in focus groups, due to unexpected schedule conflicts with patient events at the time of sessions, only 65 staff were present, resulting in low attendance for some sessions.
Data Collection
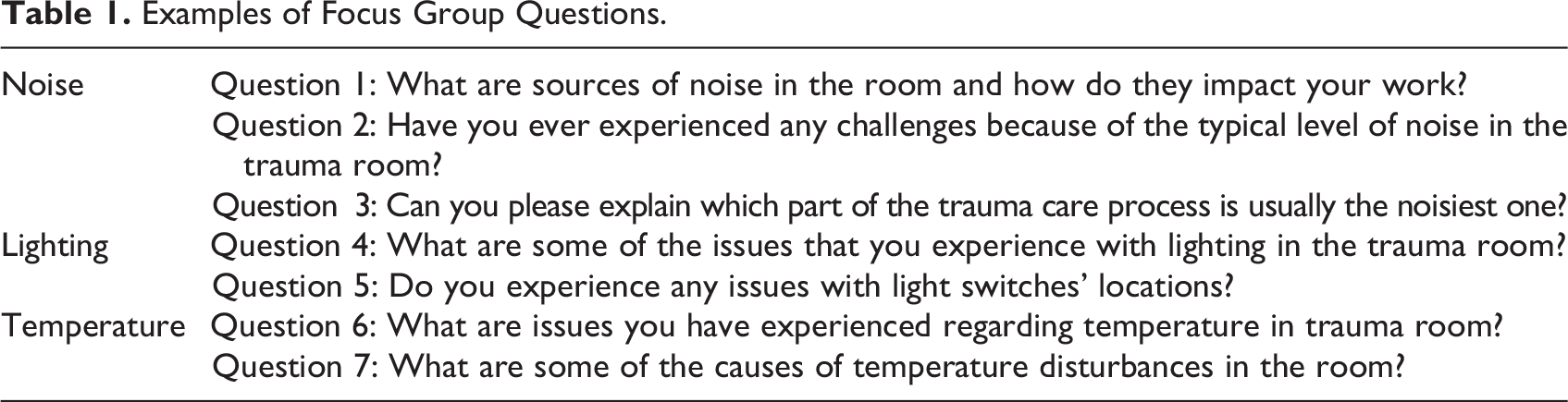
After conducting a literature review on noise, lighting, and temperature in trauma rooms revealing a significant gap in the literature, the focus group questionnaire was developed using a semi-structured format with open-ended questions for each of the three categories. The semi-structured format allowed for discussion of any unanticipated query, adding various numbers of additional questions. Six questions were formulated such that participants could describe their experience with issues related to each category and explain their importance to trauma rooms. For example, questions covered issues such as lighting control, disruptions caused by noise, and the impact of temperature on staff and patients (Table 1).
Examples of Focus Group Questions.
The research team conducting the focus groups included three individuals with architectural design or nursing backgrounds. A discussion guide was used to inform participants about the research procedure and background. Online sessions not lasting more than 60 min were conducted using Microsoft Teams and were video recorded. During focus groups, the research team screen shared visual slides to show questions and help participants remember the questions and stay focused during discussions. All participants were asked to provide written informed consent prior to the focus group session.
Data Analysis
The video recordings of focus groups were transcribed verbatim by research team members for analysis purposes. Transcripts were de-identified by naming each participant by their role and then numbering them accordingly. Using NVivo Version 12, a qualitative data analysis platform, thematic analysis guided by Braun and Clarke (2006) was used to generate themes and a codebook based on focus group questions. Two phases for analysis included a combination of deductive and inductive coding. Given the focus on noise, lighting, and temperature in the first phase, the team used a deductive approach to analyze the transcripts and organize the data under these three categories. In the second phase, themes were extracted from each of the categories using an inductive approach and sorted into a thematic structure to describe data related to each category. Two researchers conducted the thematic analysis of transcripts. Researchers identified criteria for themes and subthemes; themes were mutually exclusive and included subthemes related to their respective theme. After the first researcher extracted themes and subthemes from the transcripts, which were then reviewed by the second researcher. Then, both researchers conducted an independent thematic analysis for 80% of the transcripts simultaneously. Researchers then reviewed initial themes and subthemes to discuss and resolve all discrepancies until they yielded consensus between the coders. A final codebook was generated, and its themes and subthemes are presented in the Results section.
Results
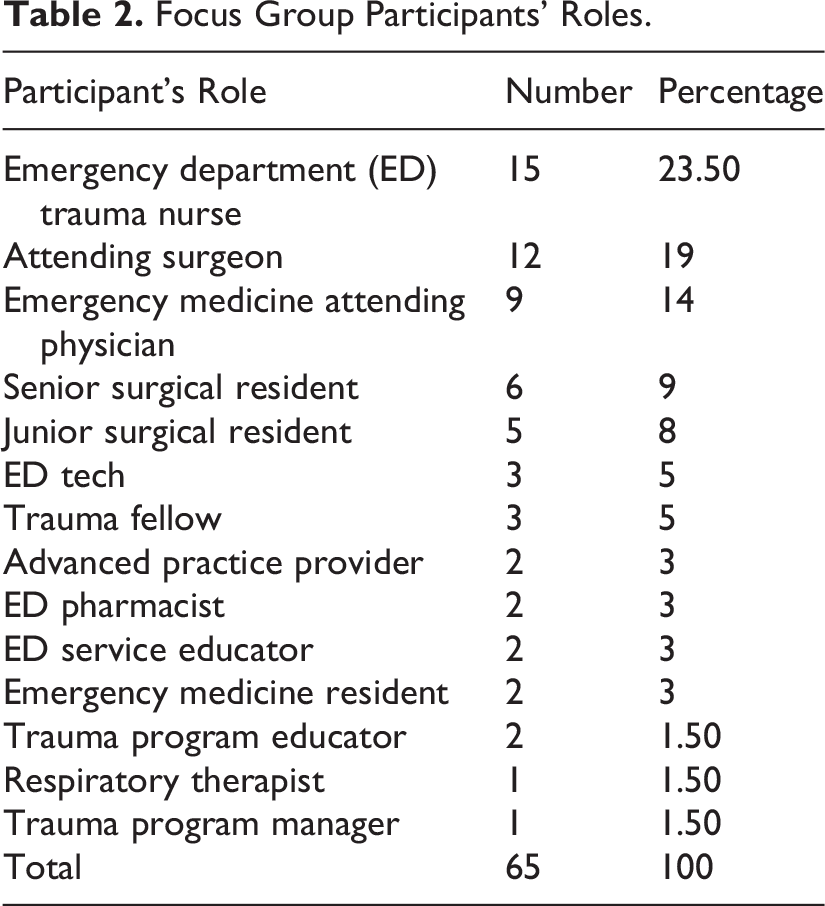
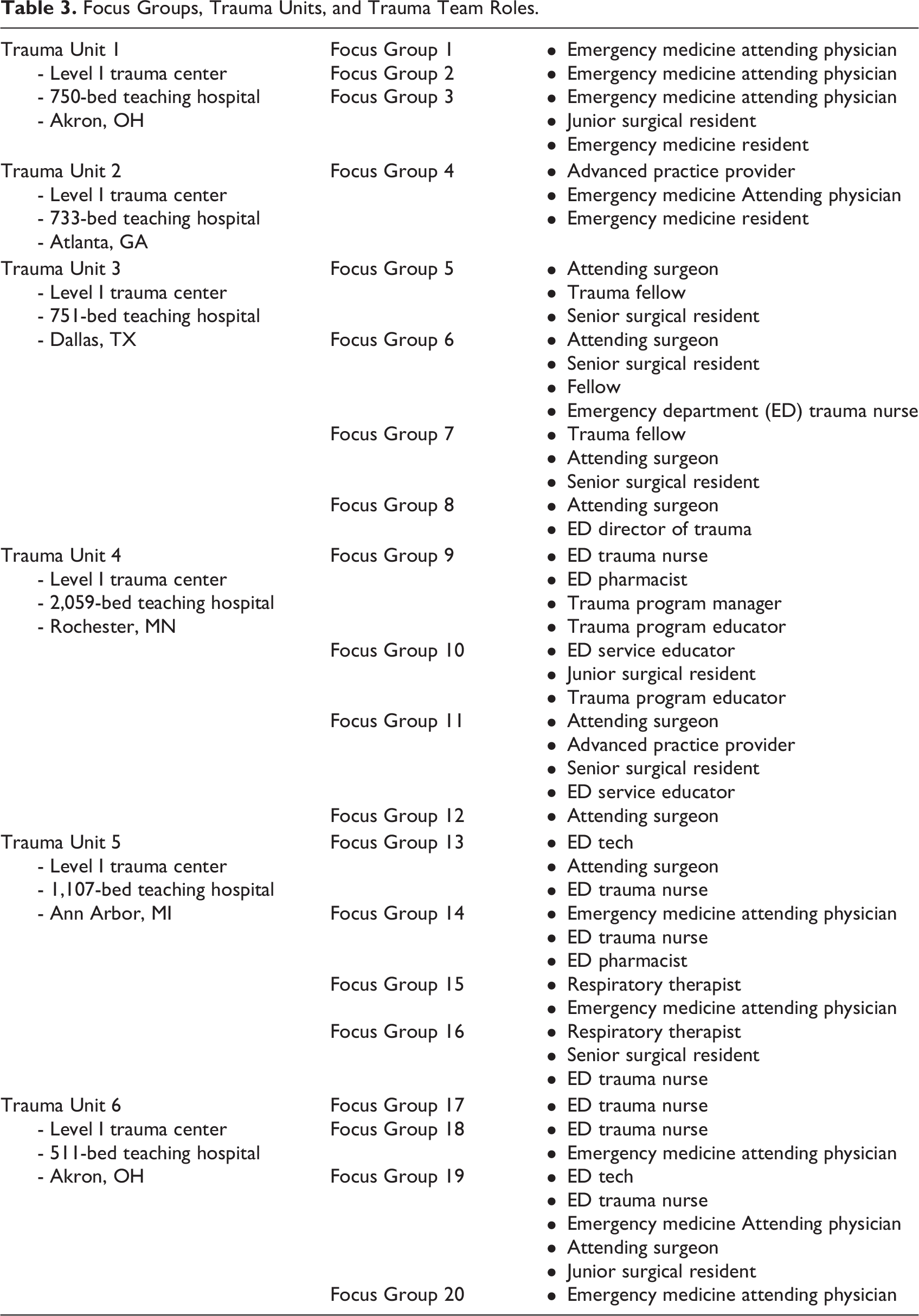
Sixty-five staff members participated in focus groups, including those with direct care trauma roles (e.g., ED nurse, EM physicians, attending surgeons) and trauma support roles (e.g., Trauma Program Educator). The number of staff members from each hospital was four, four, 20, 13, 10, and 14, respectively (Tables 2 and 3).
Focus Group Participants’ Roles.
Focus Groups, Trauma Units, and Trauma Team Roles.
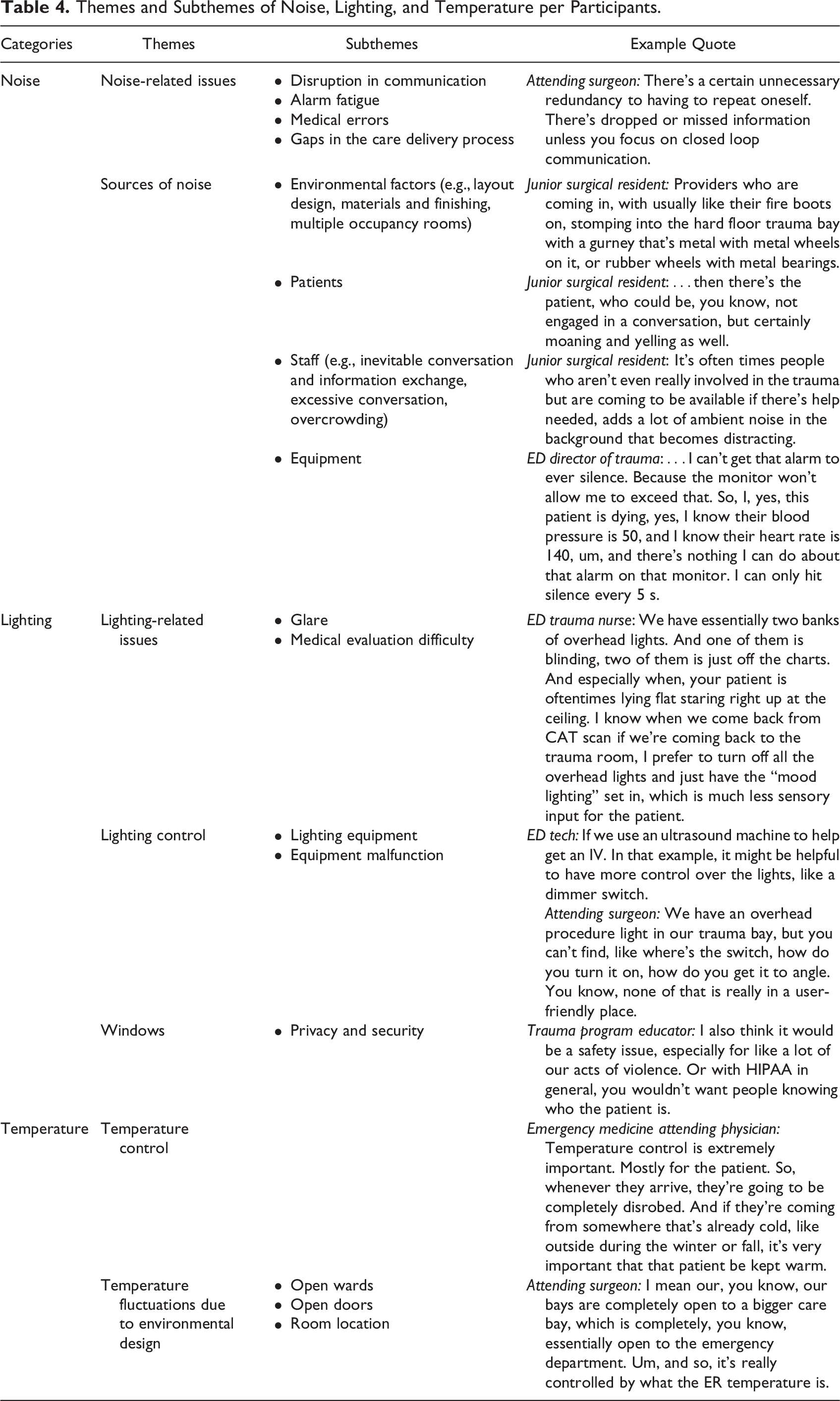
Findings were divided into three main categories: noise, lighting, and temperature. Major themes and subthemes were identified for each category (Table 4).
Themes and Subthemes of Noise, Lighting, and Temperature per Participants.
Noise Category
Theme 1: Noise-related issues
High noise levels in trauma rooms were highlighted in almost all focus groups as a distracting factor that impacts communication. Staff explained during simultaneous communication it is difficult to hear what is being communicated resulting in raised voices or shouting. Constant equipment beeping, without the capability of being silenced for an extended period, was reported to lead to alarm fatigue, increasing staff stress and distraction.
Further, one participant expressed concern that noise could lead to medical errors and provided an example in which failure to hear patient lung sounds may delay an intervention such as placing a chest tube. Another issue raised was how noise influenced the care process and created frustration among staff. For example, repeating the same question to ensure information was not lost sometimes resulted in multiple reevaluations of the patient and led to delayed care.
Theme 2: Sources of noise
Environmental factors, patients, staff, and equipment were four subthemes identified as sources of noise. Examples of environmental factors included doors, layout design, materials and finishes, and multiple occupancy rooms. Staff expressed differing opinions about whether trauma room doors should be open or closed and discussed the advantages and disadvantages of each option. Staff tended to leave the doors open due to the time-consuming act of repeated openings and closings. Open doors allowed noise to travel inside the room, which notably increased noise levels. On the other hand, doors were often slammed when closing, which became another source of noise in the room. Staff who worked in trauma centers with a combination of open bays and enclosed rooms shared that noise from other patients or units could drift inside the room. Further, interior finishes contributed to increased noise levels in some trauma rooms. For example, walking and pushing gurneys with metal wheels on the hard floor was reported as an unpleasant noise. Several statements were made about the positive and negative aspects of open wards with multiple beds compared to single-patient trauma rooms. According to staff, although an open bay allows for faster access to each patient, multiple beds in open trauma bays cause higher noise levels and interrupt the flow of communication. If more than one patient in a critical situation occupied the bay, increased noise levels increased trauma teams’ stress levels and caused distractions and chaos.
Another source of excessive noise identified by staff correlated with the severity of the patient’s situation. Patients could be a source of noise by moaning and/or screaming in pain, which increases noise levels in the trauma room. Similarly, the increased number of staff to care for more severe cases increased the noise in the room. However, there was no mention of perceived correlation between case severity and equipment noise.
Trauma team members were viewed as an important source of noise in trauma rooms. Examples included inevitable conversation and information exchange, excessive conversations, and overcrowding. The noisiest part of trauma care occurred shortly after a patient’s arrival when Emergency Medical Services personnel reports relevant patient information while other staff talk to the patient or others to collect supplemental information, leading to excessive conversation. Further, staff indicated overcrowding in the trauma room correlates with excessive noise levels and compromised patient privacy. As the care process moves forward, students and observers may enter the room for educational purposes or curiosity and consequently add to the background noise. EM attending physician: As you can hear people in the background, “look at that” or “what happened?” The cops, nurses, and students talk to each other. It becomes exceedingly hard to hear what is going on because there’s so much background static. When a patient that is ticking away at 140, I can’t get that alarm to ever silence. This patient is dying, and I know their blood pressure is 50, and I know their heart rate is 140, and there is nothing I can do about that alarm on that monitor. I can only hit silence every 5 s.
Lighting Category
Theme 1: Lighting-related issues
Glare and lighting for medical evaluation issues were two subthemes that emerged from lighting. Staff indicated that both glare and angled antiglare screens hinder the ability to view ultrasound and X-ray results. Light color combined with white walls and LED lights were reported to cause disturbances to sensory-sensitive staff members. An overly bright trauma room impeded clinicians’ ability to evaluate patients’ pupil size and light responsiveness needed for guiding resuscitation decisions and interventions.
Theme 2: Lighting control
Lighting equipment and equipment malfunction were two subthemes for lighting control. Staff wanted easy-to-adjust lighting systems to facilitate their work. Discussions revealed a critical challenge in trauma care is adjusting light intensities based on individual task requirements when simultaneous tasks by staff require different illumination needs. Adjustable lighting equipment enables staff to dim the lights during ultrasound and radiology evaluations to see images more easily. An attending surgeon mentioned: It may be helpful to dim the lights when you are trying to do a more nuanced ultrasound assessment. Then, with light booms, that is just focused on procedures. I do not think we use the light booms enough to optimize our procedures. It has an up and down arrow to turn it on and it is supposed to dim the lights. We will have X-ray come in and they are like, “can I dim the light?” and then they hit a button and the whole room goes dark.
Theme 3: Windows
When staff were asked about having windows in trauma rooms, privacy and security were their main concerns. Staff explained that trauma rooms do not need natural light, and windows might distract staff. Windows may also compromise patient privacy and security, which are critical concerns in trauma bays as patients can be victims of abuse, attacks, and attempted battery, or can be the perpetrator of a crime.
Temperature Category
Theme 1: Temperature control
Compared to other healthcare environments, trauma rooms have a higher temperature ranging from 75 °F to 85 °F, depending on the facility. Staff explained that warmer temperatures are required to accommodate patients who are losing blood or have sustained burns because they tend to rapidly lose body heat. Also, staff typically remove patients’ clothing to facilitate comprehensive examinations, requiring a warmer room for patient comfort and to prevent hypothermia. Although staff members complained about difficulties with temperature control and maintenance, they also mentioned that because patients benefit from the heat, staff gladly work through the discomfort despite the heat being reinforced by wearing gowns, masks, and face shields. A junior surgical resident said: Providers do not like the heat. We are already sweating, when you put a gown on in the room and you are standing there waiting for the patient to come and it’s 90°, you’re not enjoying it, but we know the importance for the patient itself.
Theme 2: Temperature fluctuations due to environmental design
Focus group discussions revealed that environmental design factors such as open wards, open doors, and room location can lead to temperature fluctuations. Open trauma bays divided by curtains or those without doors experience more issues with temperature control. Trauma room doors are commonly left open, which disrupts temperature maintenance. To explain the frequent door openings, one junior surgical resident said: Most times when you run the trauma the door is open. Probably because people don’t have time to close the door. People are coming in and out to get blood, or supply, so it’s hard to keep it closed at all times.
Potential Solutions
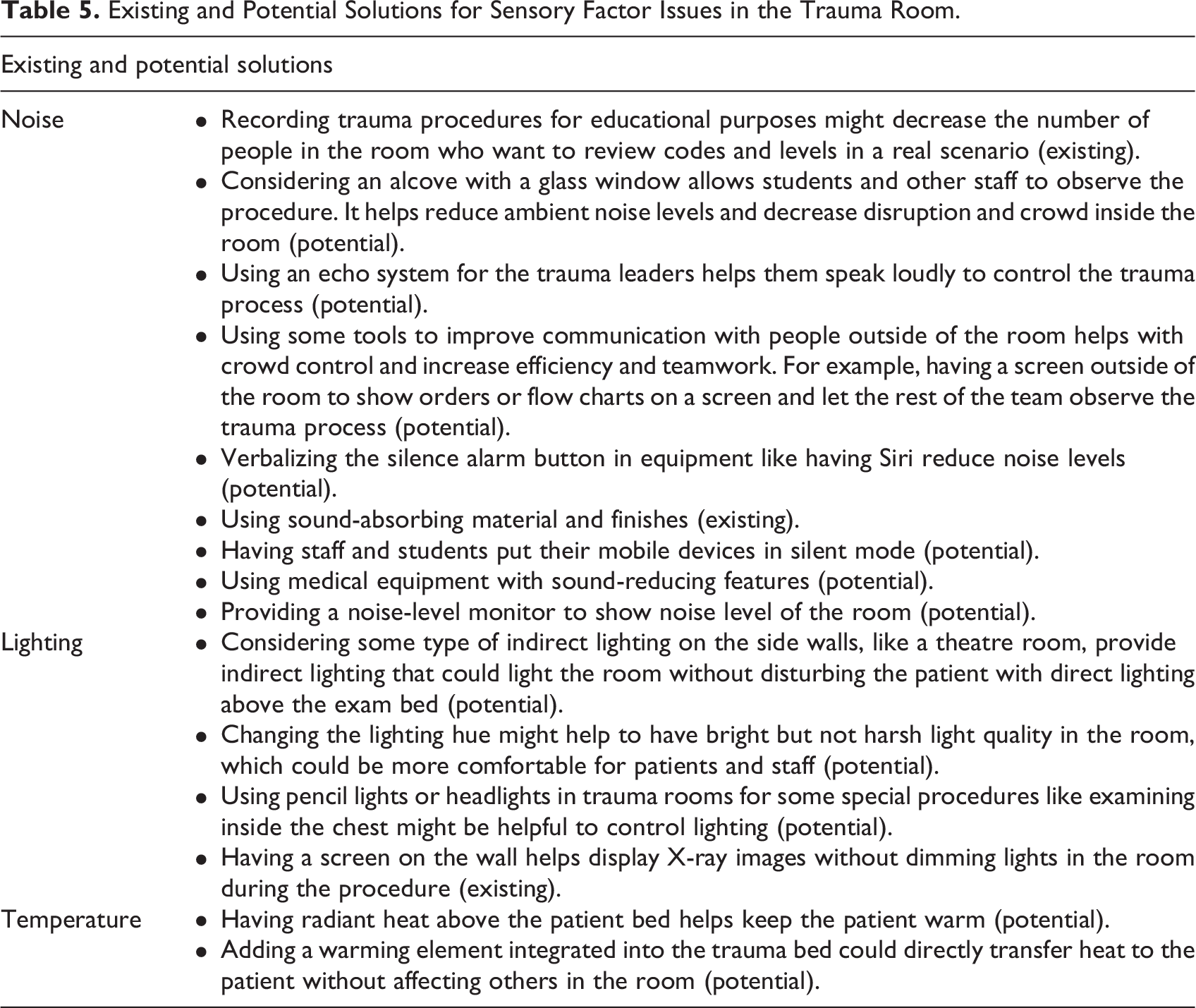
During focus group discussions, staff provided feedback about potential and existing solutions for issues related to each category (Table 5). Some of these solutions require in-depth research to evaluate their impact on all aspects of trauma care. Regarding noise, one potential solution proposed by staff was considering an alcove with a glass window to allow students and other staff to observe the procedure from outside the room to help reduce ambient noise levels and decrease disruption and crowding inside the room. Regarding lighting, having a digital screen on the wall helps display X-ray images without dimming lights during the procedure. Further, integrating a warming element into the trauma bed could directly transfer heat to the patient without affecting others in the room.
Existing and Potential Solutions for Sensory Factor Issues in the Trauma Room.
Discussion
Trauma rooms are complex environments where patients’ lives are at stake. Staff face multifaceted challenges and as such must be supported in their work to achieve desired outcomes in stabilizing patients. Among factors affecting staff performance, the role of sensory stimuli is understudied. This study uniquely focused on staff perceptions of issues associated with sensory stimuli that originate from the environment during task performance in trauma rooms. The study comprehensively analyzed sensory stimuli in the three categories of noise, lighting, and temperature, which are presented by the current literature as the predominant categories of sensory stimuli in trauma rooms.
Challenges with sensory stimuli seem similar across various staff roles in trauma rooms. Loud, unnecessary, or interruptive noise primarily present negative ramifications, including hindered communication, alarm fatigue, medical errors, and disruptions in the care delivery process as found in other studies (Bayramzadeh, Anthony, et al., 2021). Also, patient care can directly be impacted by noise-related implications such as delayed care due to compromised communication. Since implementing measures to mitigate noise is essential (Taylor et al., 2017), the main sources of noise were first identified—patients, staff, and equipment. Examples of sources of noise included patient moaning, loud and simultaneous staff conversations, and beeping/alarming equipment. Identifying the attributes of each source was vital for developing targeted interventions to reduce noise levels effectively. The findings underscored how environmental design plays a key role in controlling noise levels. Enclosed bays, sound absorbent materials and finishes, and single-bed rooms are some of the design considerations that can decrease noise levels.
Further, lighting is an essential part of any patient care process including patient evaluation and medical procedures. To optimize lighting, regular maintenance is required to ensure the equipment works properly. Proper lighting avoids creating glare and allows adjustment of light during highly demanding care processes that require multiple light levels simultaneously for different purposes, including X-ray viewing, IV administration, and examination of patients’ pupil size. The competitive needs of staff for various lighting levels could be a source of potential conflict within the team.
Lack of control was identified as the major issue when it comes to environmental systems and conditions such as lighting. Control over lighting can be reinforced and facilitated by adding additional control panels in various locations for quick and easy access. This access is critical, because lighting is a critical factor that requires immediate adjustment for visualizing the injury site or reading imaging results. In addition to lighting switch access, usability by staff from a user experience perspective must be considered, which means being intuitive to operate without instructions. Usability may also be reinforced by providing training on how to use the technology. Additionally, staff unanimously agreed that the presence of windows does not add value and causes distractions in the highly intense environment of a trauma room.
The influence of temperature on staff physical and mental work performance varies based on the nature of the work environment and tasks (Idkhan & Baharuddin, 2019). In the trauma room, proper temperature should be prioritized for patient comfort and then staff comfort, both of which can have implications for patient safety in the form of hypothermia or staff task disruption. In addition to providing control over temperature, preventing or minimizing the chances of temperature fluctuation is important. Enclosed spaces help contain the air and maintain the temperature. Adjacency of trauma rooms to building entries and exits must be avoided due to a high likelihood of cold air penetrating the room.
To improve staff and patient experience, it is beneficial to allow staff to adjust the temperature based on each trauma resuscitation. Issues with temperature control can be related to the availability of technology, permission to adjust (vs. a preset, controlled temperature by the organization), and knowledge of how to use such control panels or adjustment features. Empowering staff to have control over the necessary temperature adjustments can improve their comfort and experience in the trauma room.
Temperature did not seem to be an issue for trauma staff, who are prepared for any type of crisis and are devoted to patient care despite imposed environmental difficulties. Although elevated temperatures make their job difficult, it is rarely stated as a disruptor to their work. The existing literature shows an attempt to understand the impact of temperature on patient hypothermia (Duryea et al., 2016; Engorn et al., 2017); however, studies in this area are limited and show contradictory results in relating environmental temperature to patient outcomes. Although outcomes resulting from temperature fluctuations need more investigation, this study shows they influence both patients and staff.
Understanding staff perception of excessive sensory stimuli that can add stress to work procedures in trauma rooms is important because of their firsthand experience. Types of influential sensory stimuli include auditory, visual, and haptic as manifested through noise, lighting, and temperature. Given that potential added stress by excessive sensory stimuli can lead to adverse events, uncovering the causes, implications, and solutions is paramount to alleviate such stressors. Eliminating sources of noise, glare, inflexible light levels, and unbalanced temperatures is critical in achieving a supportive and efficient work environment. Further, control over environmental conditions such as noise, light, and temperature can improve the efficiency of procedures and the comfort of users.
This study comes with limitations. The sampling method used a convenience sampling approach. Although including six hospitals in the focus groups produced information saturation, design variability of other trauma centers may add to the knowledge gained through this research. The context in which staff work impacts their experience and responses. Each organization has a different culture and technologies available that impact work procedures. As such, variability of responses might be substantial and an unknown consensus among themes might persist. Further, each focus group, being comprised of staff with diverse backgrounds, lent itself to challenges associated with interprofessional discussions. For these reasons, generalizability of the data may not be possible. Given that this study is one of very few on sensory stimuli in trauma rooms, future studies should expand to other research methods to build consensus on the results. Future studies may develop potential solutions for issues related to sensory stimuli and evaluate their effectiveness in the form of a comparative, quasi experiment, or experiment methods. Additionally, quantitative approaches on noise levels, lighting distribution, and temperature measures can complement this qualitative study by triangulating and contextualizing the data. Examples include use of noise simulation software to compare various design prototypes in their effectiveness of noise reduction as well as comparison studies of existing trauma bays that might include a buffer space between trauma rooms and the hallways. Lighting distribution can be measured using light measuring devices in existing facilities. Additionally, a survey study could measure providers’ perspective on attitude toward a dim space and resulting reduced conversations. A larger sample size for a quantitative approach will help with generalization of issues found in this study and future potential solutions. Future research may also go beyond the design of the physical environment and consider behavioral interventions to reduce noise given the importance of behaviors and teamwork in healthcare.
Conclusion
Sensory stimuli such as noise, lighting, or temperature can create positive or negative outcomes ranging from comfort and efficient care to disrupted communication and teamwork, fatigue, medical errors, stress, and a delayed care process. To improve patient healthcare outcomes in trauma rooms, it is essential to understand how sensory stimuli impact staff. Effective design and implementing environmental control measures can address issues related to noise, lighting, and temperature, which provides staff with improved workflow efficiencies and comfort. It is critical to empower staff with control over environmental conditions and enable them to tailor the environment to their immediate needs during resuscitation and patient care procedures. Despite their importance, sensory stimuli have not been studied in the context of trauma rooms. This study highlighted the necessity of optimizing the sensory environment in trauma rooms to enhance staff performance and patient care. Recognizing and addressing the nuances of noise, lighting, and temperature are fundamental for designing trauma rooms that support staff and contribute to better healthcare outcomes.
Implications for Practice
Excessive sensory stimuli can impede patient care in trauma rooms, and the physical environment can facilitate effective control of sensory stimuli
High noise levels from equipment can cause distraction and alarm fatigue among trauma teams.
Proximity of trauma rooms to the building entrance can impact temperature fluctuation due to cold and warm fresh air penetrating the rooms.
The ability to control environmental conditions such as light and temperature can add to efficiency of procedures and comfort of providers in trauma rooms.
To maximize the utilization or proper lighting, both adjustability of technology and training of providers on using such technology are needed.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231215080 - The Impact of Sensory Stimuli on Healthcare Workers and Outcomes in Trauma Rooms: A Focus Group Study
Supplemental Material, sj-pdf-1-her-10.1177_19375867231215080 for The Impact of Sensory Stimuli on Healthcare Workers and Outcomes in Trauma Rooms: A Focus Group Study by Sara Bayramzadeh and Sahar Ahmadpour in HERD: Health Environments Research & Design Journal
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grant number R18HS027261 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.