
Abstract
Aim:
The purpose of this scoping review is to map the knowledge about the multisensory birthing room regarding the birth experience and birth outcomes.
Background:
The concept of multisensory birthing rooms is relatively novel, making it relevant to explore its impact.
Methods:
Five databases were searched. The search was limited to articles in English, Danish, Norwegian, and Swedish. There were no time limitations. Fourteen relevant articles were identified providing knowledge about multisensory birthing rooms.
Results:
Eight articles focused on birth experience, six articles focused on birth outcome, and one on the organization of the maternity care. Seven of the studies identified that sensory birthing rooms have a positive impact on the birth experience and one qualitative study could not demonstrate a better overall birth experience. Five articles described an improvement for selected birth outcomes. On the other hand, a randomized controlled trial study could not demonstrate an effect on either the use of oxytocin or birth outcomes such as pain and cesarean section. The definition and description of the concept weaken the existing studies scientifically.
Conclusions:
This scoping review revealed that multisensory birthing rooms have many definitions and variations in the content of the sensory exposure; therefore, it is difficult to standardize and evaluate the effect of its use. There is limited knowledge concerning the multisensory birthing room and its impact on the birth experience and the birth outcome. Multisensory birthing rooms may have a positive impact on the birth experience. Whereas there are conflicting results regarding birth outcomes.
Keywords
Introduction
In recent years, major attention has been paid to the importance of the physical space and its importance for the well-being of patients. The term “healing architecture” was introduced in the 1980s (Simonsen et al., 2022; Ulrich, 1984). There is no clear definition of healing architecture; nevertheless, the term is widely used in the literature and conceptually covers architecture, interior design, and physical settings that affect the healing ability (Aripin, 2006; Simonsen et al., 2022; Thaddeus & Napoleon, 2021). Other terms are used for similar rooms, for example, the “Snoezelen room,” a Dutch term for a controlled multisensory environment that means a room designed to stimulate the senses of people. Multisensory birthing rooms aim to promote comfort and relaxation, thereby causing endorphin release and thus enabling a person’s pain-coping capacities (Schofield et al., 1998). Throughout this article, we will use the term multisensory birthing room to describe birthing rooms using individual or combined visual or auditory effects.
Multisensory birthing rooms are intended to create an immersive environment that can support women giving birth and visitors by reducing stress and increasing well-being in the process (Thaddeus & Napoleon, 2021; Ulrich et al., 2008). Studies have shown that images of nature reduce stress, fear, and pain perception (Spiegel et al., 2019; Ulrich, 1991). Daylight and scenic vistas of nature are some of the elements that previously have shown positive effects on the healing process (Aripin, 2006; Grahn et al., 2021; Thaddeus & Napoleon, 2021). Ulrich et al. describe how to use the “positive distraction” strategically to remove the patient’s attention from pain or anxiety and thus reduce the experience of the pain (Ulrich, 1991).
Giving birth is a life-changing event that generates major psychological impact and physiological changes in the mother (Aune et al., 2015; Nielsen & Overgaard, 2020; Olza et al., 2018). Natural birth is defined as vaginal delivery without complications and with only limited use of medication (Prosser et al., 2018). An essential factor during birth is that the birth-giving mother feels safe and relaxed. The hormone oxytocin promotes natural birth and works optimally when the mother feels safe and relaxed, while the hormone adrenaline inhibits or completely stops the progress of the birth (Uvnäs-Moberg et al., 2019). The surrounding environment significantly affects the amount of oxytocin measured in the blood during childbirth and is very important for feelings of well-being, calmness, and empowerment (Uvnäs-Moberg et al., 2019). Additionally, maternity wards that are designed to be functional and still reduce the feeling of being in a hospital affect the well-being of midwives and, thereby, improve patient care (Hammond et al., 2017).
A scoping review from the World Health Organization that explored the evidence of the importance of art for health describes how music during childbirth is associated with a better birth experience and, indirectly, fewer birth complications (Fancourt & Finn, 2019). A systematic review focusing on how the design of a birthing room influences the maternal and neonate physics, and emotions document the importance of a design with distraction, comfort, welcoming design, an appropriate temperature, familiarity, and a diminished technocratic environment (Nilsson et al., 2020). Another review investigated whether the architecture and design of a birthing room impact intrapartum interventions and concluded that not only the design of the birthing room but also behavior, experience, and practice of the health providers influence the intrapartum interventions (Setola et al., 2019). Multisensory birthing rooms are different in these regard in that birthing room does not need to look like conventional hospital rooms (Hodnett et al., 2012) and cover interior, light, sound, pictures, film, and art. The existing evidence in this area is not clear. A randomized controlled trial (RCT) comparing childbirths in a standard birthing room to childbirths in a specially designed birthing room did not find any difference in clinical obstetric outcomes (Lorentzen et al., 2021). In contrast, an observational retrospective cohort study found that births in sensory birthing rooms, which are characterized by the installation of different visual and auditory effects, can be associated with a lower risk of cesarean section (Wrønding et al., 2019).
The increased attention toward multisensory birthing room and its potential role makes it relevant to uncover its effects in a maternity ward. The purpose of this scoping review is to map the knowledge about multisensory birthing room regarding the birth experience and birth complications.
Materials and Methods
A scoping review provides an overview of existing literature and is distinguished from a traditional systematic review by its research question being slightly broader and can thus examine the scope of literature within a given topic (Levac et al., 2010). Additionally, scoping reviews are characterized by typically not assessing the evidence of included studies (Levac et al., 2010). The motivation for this scoping review is based on the fact that the existing reviews focus more formally on design and architecture in birthing rooms. However, clinicians need a review that intertwines knowledge about multisensory birthing rooms with complication rates and birth experience. This scoping review is based on the methodological framework by Levac et al. (2010). The framework consists of six stages: (1) identifying the research question; (2) identifying relevant studies; (3) study selection; (4) charting the data; (5) collating, summarizing, and reporting results; and (6) consultation. At Stage 1, the research question was identified as follows: To explore existing literature on how healing architecture in a hospital birthing room affects birth experience and birth outcomes. At Stage 2, we performed a literature search linked to the research question.
This search was conducted with the help of an experienced librarian (C.S.) in collaboration with clinicians in the field of obstetrics. At Stage 3, two independent persons (A.E. and D.M.) reviewed the articles, initially at the title and abstract level and then at the full-text level. If necessary, a third person, an obstetrician (L.B.), resolved disagreements. Further, at Stage 4 in Levac’s framework, the authors collaborated to complete an analysis of emerging data. We then, at Stage 5, provided an overview of the literature and data using an analytical framework. Finally, Stage 6 covered the involvement of stakeholders.
Literature Search
Search strategy
The following databases were searched: Ovid MEDLINE® (1946-August 2023), OVID Embase (1974-August 2023), Ebsco CINAHL with full text (1937-August 2023), Clarivate Web of Science Core Collection (1900-August 2023), and Wiley Cochrane Library (1993-September 2022). All databases were searched in August 2021 and updated in August 2023.
The search strategy was developed by a librarian (C.S.) along with the first author (A.E.) and last author (D.M.) and peer-reviewed by another librarian.
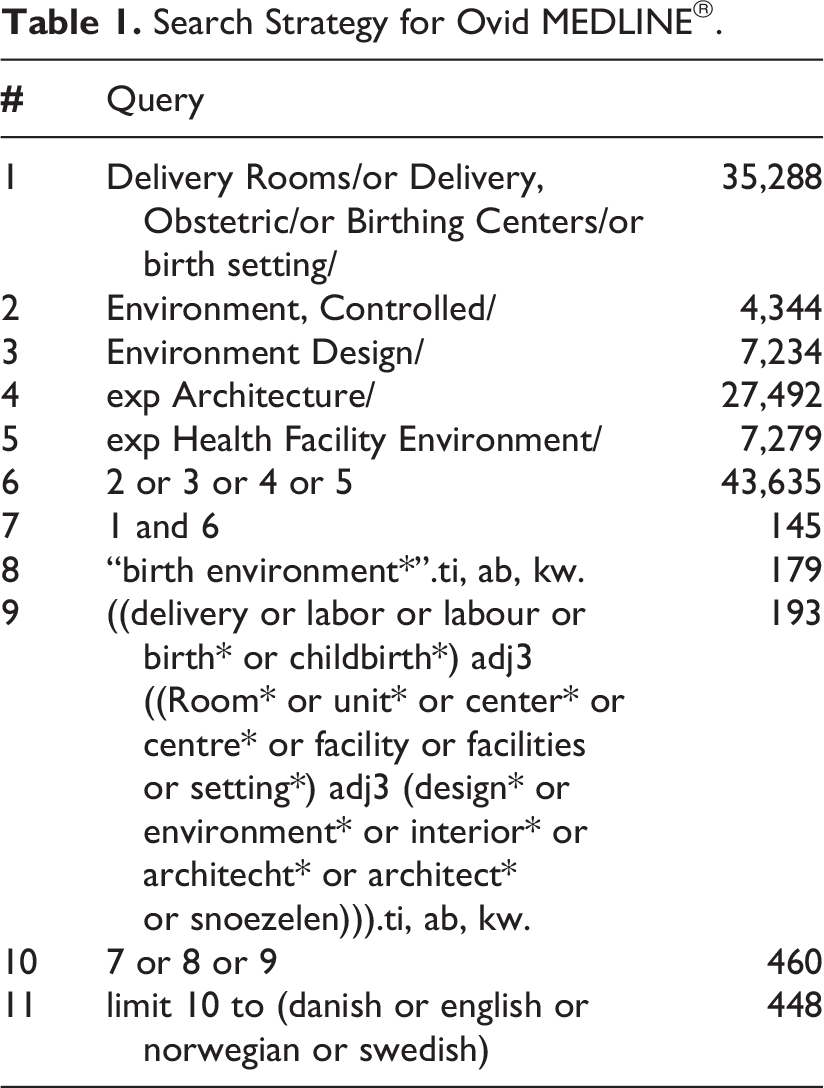
We searched for Birth settings and Architecture using both controlled vocabulary terms, that is, Mesh terms and natural language terms for their synonyms. The search was limited to articles in English, Danish, Norwegian, and Swedish. There were no time limitations. A total of 1,861 unique citations were retrieved from the five databases. Duplicates (1,014) were removed by the librarian (C.S.) using Endnote and Covidence’s duplicate identification strategies. See the strategy for Ovid MEDLINE® in Table 1.
Search Strategy for Ovid MEDLINE®.
Study selection
To be included in this review, articles needed to focus on the effect of birthing room on aspects of birth experience and birth outcomes. Articles were included if they were written in English, Danish, Norwegian or Swedish. Literature reviews, protocols, conference abstracts, editorial comments, and articles not available in the full text were also excluded. We excluded studies with wrong outcomes and interventions e.g. studies that examine the effect of multisensory birthing rooms and the staff experience.
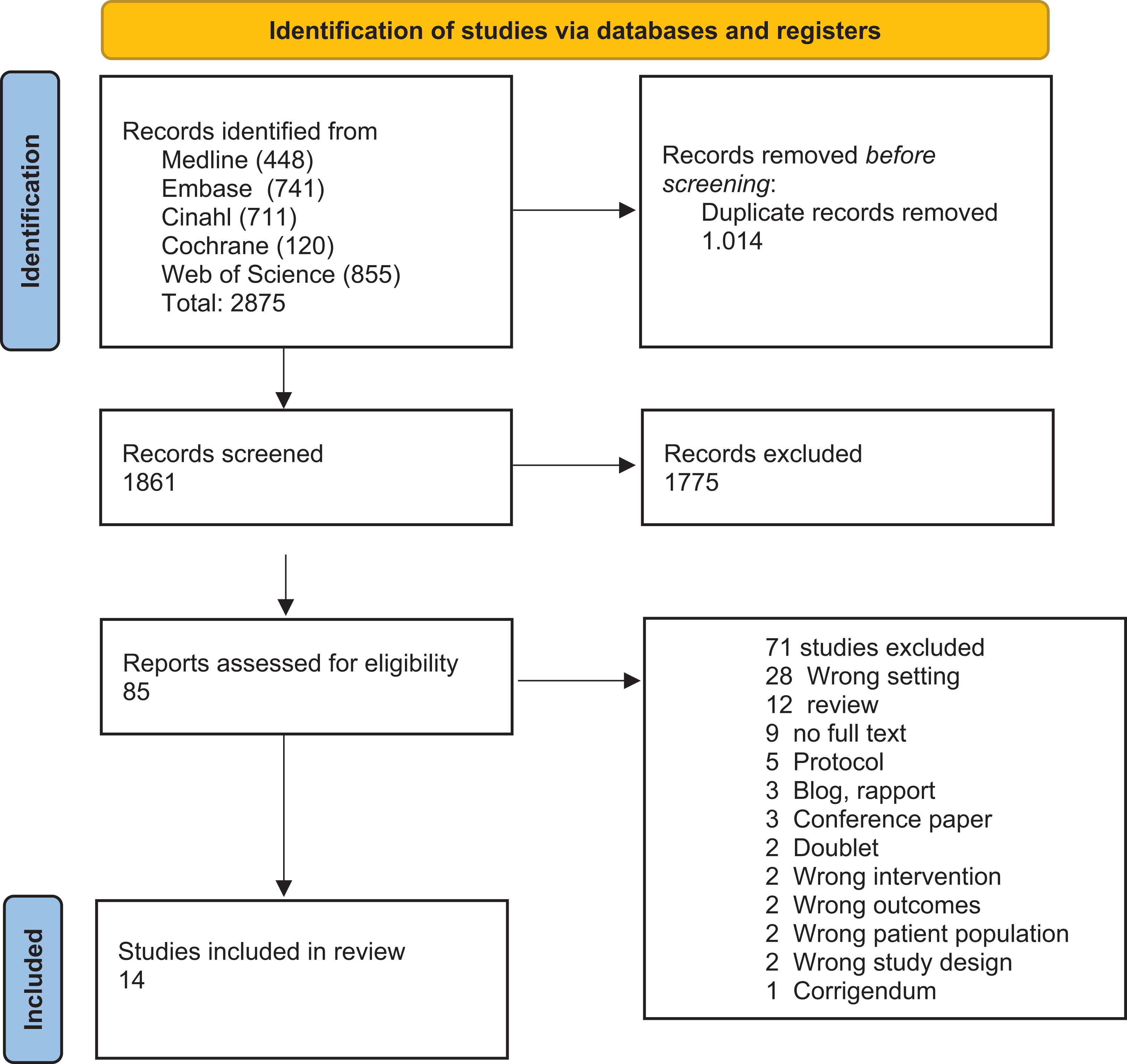
PRISMA flow diagram with search results, study selection, and reasons for exclusion of studies.
Results
This scoping review identified 14 articles eligible for this study (Table 2). Thirteen of the articles were published within the last ten years. Eight of the articles were Scandinavian studies (four from Denmark and four from Sweden), two were from Iran, one from Saudi Arabia, Germany, Canada and Australia respectively. Nine studies were quantitatively designed (eight RCT and one cohort study), three were qualitative, and two were mixed-method studies.
Summary of Included Articles.
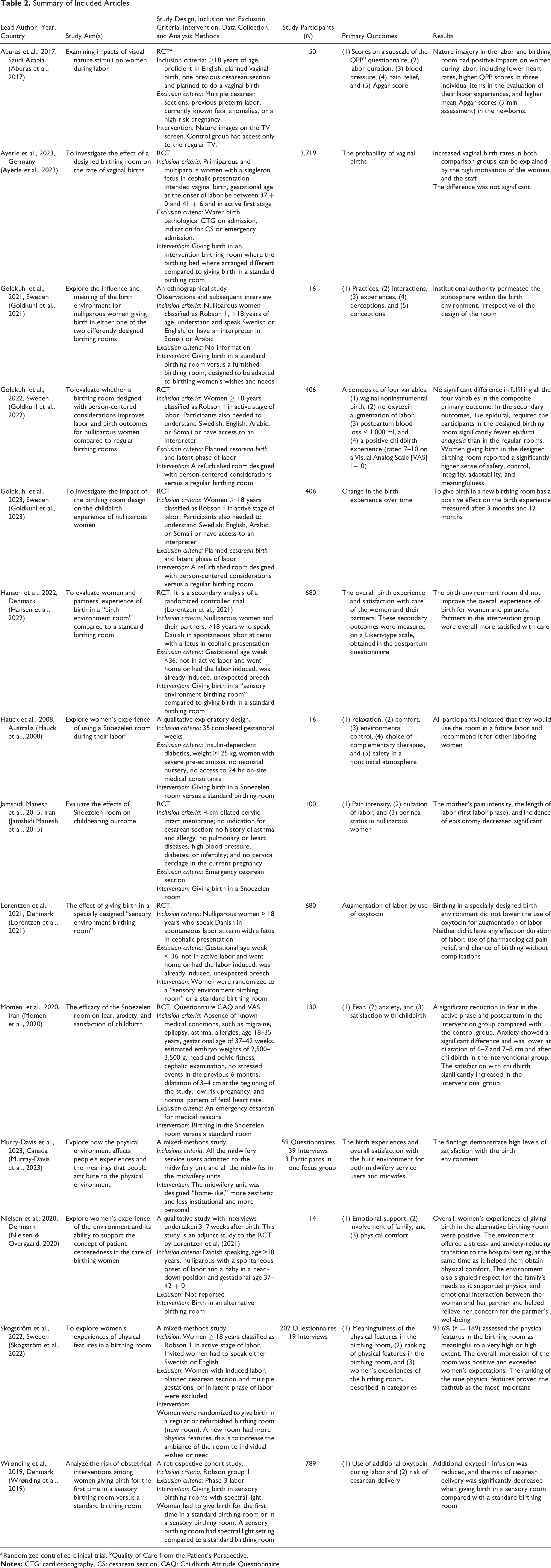
a Randomized controlled clinical trial. bQuality of Care from the Patient’s Perspective.
Eight studies focus on the birth experience, and six describe the birthing room’s impact on obstetric outcomes. One study focused on the organization of maternity care. The article from Aburas et al. examines both obstetric outcomes and birth experience, and therefore this article is categorized under both. The total number thus becomes 15 when summing up the articles under each of the three categories.
Birth Experience
An RCT found that introducing nature imagery to the labor and birthing room resulted in higher Quality of Care From the Patient’s Perspective (QPP) scores in the mothers’ evaluation of their labor experiences (Aburas et al., 2017). A qualitative exploratory study found that women recommended a multisensory birthing room to other laboring women (Hauck et al., 2008). An RCT (Momeni et al., 2020) and a qualitative study (Nielsen & Overgaard, 2020) showed that a multisensory birthing room could reduce anxiety and improve childbirth satisfaction. A mixed-methods study concluded that there is a high level of satisfaction with the birth environment for both midwifery service users and midwives when the birthing rooms are made “home-like” (Murray-Davis et al., 2023). Another RCT demonstrated that the positive birth experience after birth in a multisensory birthing room persists over time. In this study, the birth experience was evaluated after 3 and 12 months (Goldkuhl et al., 2023). A mixed-methods study explored women’s experiences of physical features in a birthing room and found that 93.6% of the women assessed the physical features in the birthing room as meaningful to a high extent. The study found that the overall impression of the room was positive (Skogström et al., 2022). One qualitative study comparing childbirths in standard birthing rooms (control) with new birthing rooms (intervention group) could not demonstrate a better overall birth experience in the intervention group but found that the partners in the intervention group were more satisfied with care. In this study, the new birthing room was furnished with materials and furniture that created a homely atmosphere and video projections on the walls featuring nature scenes to bring nature into the room (Hansen et al., 2022).
Birth Outcomes
An RCT showed that giving birth in a multisensory birthing room decreased the length of labor and incidence of episiotomies compared to giving birth in a standard birthing room (Jamshidi Manesh et al., 2015). A retrospective cohort study (n = 789) found that the risk of cesarean delivery was significantly decreased (OR = 0.57; 95% CI [0.33, 0.97]), and the use of oxytocin infusion was reduced with giving birth in a sensory room versus a standard birthing room (OR, multiple adjusted: 0.71; 95% CI [0.50, 1.03]); (Wrønding et al., 2019). Aburas et al. reported a higher Apgar score in children birthed in a room with visual nature stimuli, and Goldkuhl et al. found significantly lower use of epidural analgesia in births in newly refurnished birthing rooms, where there was a more home-like atmosphere with a sofa, bedspread, cabinet for personal belongings, and the option of dimmed lighting, compared to the regular birthing rooms (Aburas et al., 2017; Goldkuhl et al., 2022). An RCT compared the rate of vaginal birth between a birthing room designed to encourage mobility, self-determination, and uptake of upright maternal positions in labor to a standard birthing room and found no significant difference between the groups (Ayerle et al., 2023).
In one RCT, giving birth in a multisensory birthing room had no effect on either the use of oxytocin or birth outcomes compared to births in a standard birthing room (Lorentzen et al., 2021).
Organization of the Maternity Care
An ethnographical study in Sweden with observations and a subsequent interview found that the organization of maternity care has a more significant impact on the birth experience than the birthing room. A birthing room can be designed to create calmness, safety, and familiarity, but if the personal needs of its users are disregarded in favor of the local instructions and professional recommendations, the importance of the spatial framework will become less significant. The study from Sweden showed that the local instructions and guidelines had a greater influence on the birthing women regardless of whether they gave birth in a regular birthing room or a refurbished birthing room (Goldkuhl et al., 2021).
Discussion
This scoping review aimed to uncover existing knowledge about multisensory birthing rooms and how the environment affects the birth experience and birth complications. The literature search suggested that there were few studies to cover each of these aspects.
Birth Experience
In recent years, there has been an augmented focus on the impact of multisensory birthing rooms on the birth experience. Seven of the eight studies document a positive effect of nature images or multisensory birthing rooms to give better physical comfort and reduce anxiety (Aburas et al., 2017; Goldkuhl et al., 2023; Hauck et al., 2008; Momeni et al., 2020; Murray-Davis et al., 2023; Nielsen & Overgaard, 2020; Skogström et al., 2022). One study could not demonstrate that the birthing room affected the overall experience (Hansen et al., 2022). The overall positive impact of multisensory birthing rooms on birth is supported by studies that investigate the effect of multisensory birthing rooms in other health contexts, for example, in dental clinics or for psychiatric patients (Haig & Hallett, 2022; Ismail et al., 2021).
Obstetric Outcomes
There was an overall trend toward birthing rooms that were furnished based on principles of multisensory rooms with sensory stimuli that were able to reduce the number of complications. Four of the six studies documented an individual positive effect on the pain intensity, length of labor, episiotomy, risk of cesarean delivery, the use of oxytocin infusion, and the Apgar score in newborns compared with a standard-birthing room (Aburas et al., 2017; Goldkuhl et al., 2022; Jamshidi Manesh et al., 2015; Wrønding et al., 2019). From the literature, it is well known that nature images can reduce the level of stress hormones (Ulrich, 1991), and other studies find a positive effect of nature images on pain levels (Diette et al., 2003; Tse et al., 2002). There are divergent results recording births outcomes as a Danish study showed no effect in reducing complications such as cesarean delivery, oxytocin for augmentation and blood loss (Lorentzen et al., 2021), while another Danish study showed that giving birth in a multisensory birthing room could be associated with a lower risk of cesarean delivery (Wrønding et al., 2019). The largest RCT in this field with more than 3,700 participants demonstrated similar vaginal birth rates in specially designed and standard birthing rooms in both comparison groups (Ayerle et al., 2023). Different inclusion and exclusion criteria cannot explain the diverging results, as most of the studies have similar criteria (Goldkuhl et al., 2022; Lorentzen et al., 2021; Wrønding et al., 2019) and include women from Robson Group 1. The Robson’s Ten-Group Classification System divides the women into 10 groups based on obstetric characteristics, which makes it easier for healthcare professionals to compare obstetric outcomes. Robson Group 1 is defined by nulliparous, single, cephalic position, ≥37 weeks, and spontaneous labor (Zeitlin et al., 2021). One study has not divided the women into Robson classification and excludes women in active labor without any systematic medical diseases (Jamshidi Manesh et al., 2015).
Organization of the Maternity Care
An ethnographical study concludes that the institution’s culture permeates the birthing room, independent of the room’s design (Goldkuhl et al., 2021). The reason for this could be credited to the variety of healthcare providers involved in childbirth, their specific role, how they adapt and interact within the room design and facilities, how they integrate themselves into the birth experience, or the timing of entry into the birthing room. Furthermore, the culture of the institution may have an impact on the midwife´s way of providing care. In the study by Goldkuhl et al., the culture was more important than the design of the room (Goldkuhl et al., 2021).
Strengths and Limitations
This scoping review gives the ability to identify the use of healing architecture in birthing rooms. The review is strengthened by rigorous methods based on prespecified criteria defined by Levac et al. (2010). Due to the heterogeneity in methodology, terminology, and assessment procedures used in the included articles, the generalization of study results is limited.
This scoping review is based on searches in the most common health and architecture research literature databases and with no time limit, which can strengthen its validity. Our review was limited by only screening articles available in English or Scandinavian languages. Secondly, we did not appraise the publications’ quality including validity as this is not part of the scoping review method. Another limitation is the heterogeneity of the studies in terms of defining multisensory birthing rooms. Some of the rooms in the included studies had an aquarium, a projector making optical shapes, light music, or aromatherapy (Aburas et al., 2017; Hauck et al., 2008; Momeni et al., 2020). In the studies from Nielsen et al. and Hansen et al., the birthing room was refurnished, with visual, auditory stimuli on three walls and a focus on the interior (Hansen et al., 2022; Nielsen & Overgaard, 2020). The fact that the rooms are arranged very differently means that comparing the effect of these very heterogenic exposures is extremely difficult.
Conclusion
The included studies in this review focused on three main categories: birth experience, obstetric outcomes, and organization of maternity care. Based on the identified evidence, this scoping review demonstrates that a multisensory-adapted birthing environment may improve the birth experience and that there is also a trend toward a reduction in obstetric complications.
The results of this review highlight the importance of investigating which method is most suitable for uncovering the effect of a multisensory birthing room versus a standard birthing room. The existing studies show that the current approaches are not always comprehensive.
The fact that the rooms are arranged very differently means comparing the effect on its users is extremely difficult. A clear definition of multisensory birthing room and detailed descriptions of how the birthing rooms were designed and furnished is needed in future studies.
Implications for Practice
When designing future delivery rooms, nature should be taken into consideration, as it has a documented positive effect on the birth experience. In the same way, there is a tendency to reduce birth complications in birth rooms that incorporate nature.
Further research is required in order to achieve a higher level of insight in the field
There was not an agreed definition of a multisensory birth room. It would be preferable to have a consensus on the definition of a multisensory birth room, with the aim of gathering knowledge that can direct the future design of birth room.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none was declared.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Marie Pedersen and Jensine Heibergs foundation and the North Regional Health Science Research Foundation.