
Abstract
Objective:
The study aims to investigate what design practitioners and healthcare facility managers deem as important benchmarking metrics worldwide, investigating country differences in benchmarking usage and which metrics are prioritized.
Background:
Benchmarking is a regular practice in the healthcare sector, both for clinical and managerial aspects to compare, measure, and improve standardized processes. However, limited knowledge is available about benchmarking procedures in hospital planning, design, and construction.
Methods:
A web-based survey was designed, revised, and pilot-tested in five countries; it was adjusted according to local experts’ suggestions and submitted globally via SoSci multilingual platform to persons involved in hospital design, research, construction, and facility management. It was composed of closed questions on 5-point Likert-type scale ranking frequency or importance and open-ended questions divided into six sections. Two hundred and eighty full responses have been collected. Statistical analysis was performed via PowerBI and R-Studio, while qualitative analysis was performed via MAXQDA.
Results:
The findings reported allow for both specific insights per each country or category as well as enabling general considerations of a practice that is becoming always more international with 30%–50% of respondents working in the international context. The evaluation of the survey highlights the most important benchmarks, among others. For example, for respondents from the top five countries (Sweden, Spain, Germany, Italy, and the United States), the most important metric for benchmark comparability is whether the project was new construction, new construction attached to an existing hospital, or interior renovation. Construction date, client type (public vs. private), and country of location were also generally rated as the most important metrics by respondents. Other metrics that were consistently rated as important globally included inpatient unit layout, walking distances, number of floors, and whether all patient rooms are private. Space-related metrics are considered very important elements in the design and planning of healthcare facilities worldwide. Regarding cost-related metrics, all countries consider the ratio construction cost per building gross area as the most important.
Conclusions:
Benchmarking emerges as a relevant tool for hospital design and planning as it can support efficiency, standardization, and confidence; currently, benchmarking is still underutilized due to the challenge of international comparison, access to data outside each specific company, and variation design metrics nationally. Benchmarking strategies should be further investigated to support knowledge exchange and to ensure reliable and comparable information globally.
Keywords
Introduction
Benchmarking is a continuous quality improvement process by which an organization can assess its internal strengths and weaknesses, evaluate comparative advantages of leading competitors, identify best practices of industry functional leaders, and incorporate these findings into a strategic action plan geared to gain a position of superiority. (Min et al., 1997)
Benchmarking is thus one approach to “the search for and implementation of best practices” (Rogers et al., 1995).
In the context of hospital projects, benchmarking supports strategic planning by refining the planning focus and setting targets and goals (González et al., 2005).
Benchmarking extends the design process by offering designers objective performance measures, baseline standards, and specialty-specific targeted outcomes. Industry benchmarking data allow for accurate comparison between projects and against to industry leaders by standardizing measures to deliver uniform data. Metrics provide a comprehensive overview of the planning and design process, highlighting the most effective practices for the development of a client’s new facility. Architects and designers formulate design decisions by considering clients’ requirements, conducting research, referencing case studies, and analyzing historical data. Metrics play a crucial role in offering insights to identify the most effective best practices for the clients’ design. Additionally, metrics leverage historical data to generate cost estimates that can be periodically utilized throughout the various project phases (Badlato, 2017).
Health services research primarily applies benchmarking to identify optimal practices for national health systems and treatments. The World Health Organization’s World Health Report found that while healthcare costs varied significantly, health status among countries was comparable (World Health Report, 2000). This emphasizes the potential for improving healthcare performance through the understanding of international practices. International benchmarking data can thus provide the standardized, harmonized data necessary to compare health systems globally. Furthermore, benchmarking data have been used to explain efficiency variations across hospitals and offer strategies for enhancing their processes (Van Lent et al., 2010).
The built environment of the hospital has been shown to impact healthcare processes and outcomes (Codinhoto et al., 2009; Zhang et al., 2019). Given that benchmarks are commonly used to compare healthcare processes internationally, an international comparison of benchmarks for healthcare architecture is equally relevant. Benchmarking is a collaborative process of sharing specific industry practices and metrics to compare results and outcomes. This approach applied to different industries tends to result in improved performance, reduction of cost variations, and definition of reliable state of the art suggestions for new designs or processes (Choi et al., 2020; Kahn, 2009; Searles et al., 2013). Hence, in the healthcare sector, it is considered a regular practice, both for clinical and managerial aspects (Feibert et al., 2019; Fry et al., 2016; Wind & Van Harten, 2017). Healthcare facilities, a fundamental part of the healthcare service delivery supply chain, are understudied and approached only as local or episodic experiences (Lavy et al., 2019; Mulva & Dai, 2009; Sharma et al., 2021; Viergutz & Apple, 2022). However, healthcare facilities around the world continue to face similar challenges despite their cultural and geographic differences. Rapid developments in medical technology, novel patient therapies, and pandemic-response have not only changed operational procedures and processes. These changes demand flexible space and a redesign of existing hospital structures (Brusamolin et al., 2023). Another challenge is the increasing average age of patients in the course of demographic change accompanied by the associated increase in chronic diseases and multimorbid conditions (Song & Ferris, 2018). These examples of future challenges in the hospital sector demonstrate that this does not only affect individual facilities but whole supply chains at global level. Supporting international exchange could spur strategies and proposals for design and implementation to learn from each other how to deal with such challenges and opportunities in the future. Moreover, COVID-19 stressed the links that supply chains, and particularly the healthcare supply chains, have worldwide (Brambilla et al., 2023; Wang et al., 2022). Like other industries, healthcare organizations and design-related organizations are gradually becoming more internationally minded. Design or construction firms frequently work in multiple countries, and in some cases, the cross-border work is fluid and concurrent, such as for teams in the United States and Canada or in the Scandinavian countries. It is common for a team to compile project information from all countries worked in to inform future work in any one of the countries. Similarly, a hospital organization with locations in multiple countries may manage its hospital area information centrally, for example, to evaluate energy usage or to plan maintenance and repairs (Li et al., 2020). There is an opportunity for continued collaboration across countries to learn best practices in hospital planning, space programming, and operations. For example, principles of evidence-based design as key determinants for single-patient bedrooms that became prominent in the United States in the 1990s and 2000s have gradually been adopted in some other countries also (Anåker et al., 2019). Within this global context, and for internationally focused healthcare and design-related organizations, different tools such as international standards could be supportive. While examples for other building typologies or specific regions are available (AA.VV., 2011; International Property Measurement Standards, 2014), there are few or none for hospital design, nor does the fact that the comparability between different factors such as hospital area supports comparison. It is also a fact that comparison may be unclear due to different international norms in area measurement (Viergutz & Apple, 2022). As a result, limited knowledge is available about benchmarking procedures in hospital planning, design, and construction, and benchmarking strategies should be further explored to achieve comparability (Kahn, 2009; Mulva & Dai, 2009; Searles et al., 2013)
Therefore, the aim of the study is to explore the importance of benchmarking for hospital design and planning according to professionals in the sector. Specifically, this study sought to understand which professions currently leverage benchmarking data for hospital planning, how frequently benchmarking is currently used on projects worldwide, and which benchmarking data sources are most relevant across professions and/or regions.
Method
Research Design and Distribution
This study consisted of an online web-based survey (Callegaro et al., 2015) emailed to persons involved in hospital design, research, construction, and facility management. The English version of the survey was developed through an iterative process, gradually refining the content. The survey was then translated into four additional languages (Swedish, Spanish, German, and Italian) and a glossary of terms was created to clarify concepts within the different geographical contexts. Once the survey was ready and uploaded to a multilingual online survey platform, it was pretested by two local experts per language. The pilot test participants are experts in their respective fields of healthcare design and planning, design, and research. Then, all authors discussed and included comments in the reviewed English survey based on the pretested findings. Finally, the reviewed English survey was translated into the four languages and uploaded again to the online survey platform. The survey was administered from September 2022 to November 2022. Because the survey was aimed at experts in hospital planning, design, research, and construction, survey participants were recruited via email invitations to specific personal contacts and participants to related studies (Cambra-Rufino et al., 2021), social media publications (i.e., LinkedIn), and newsletters on local related centers or national associations. The survey was administered and developed using the professional software SoSci Survey Version 3.3.10 (2022-07-03) whose servers and operators are in Munich, Germany (Online Annex). This software provides data protection in accordance with European General Data Protection Regulation (GDPR). All survey phases are summarized in Figure 1.
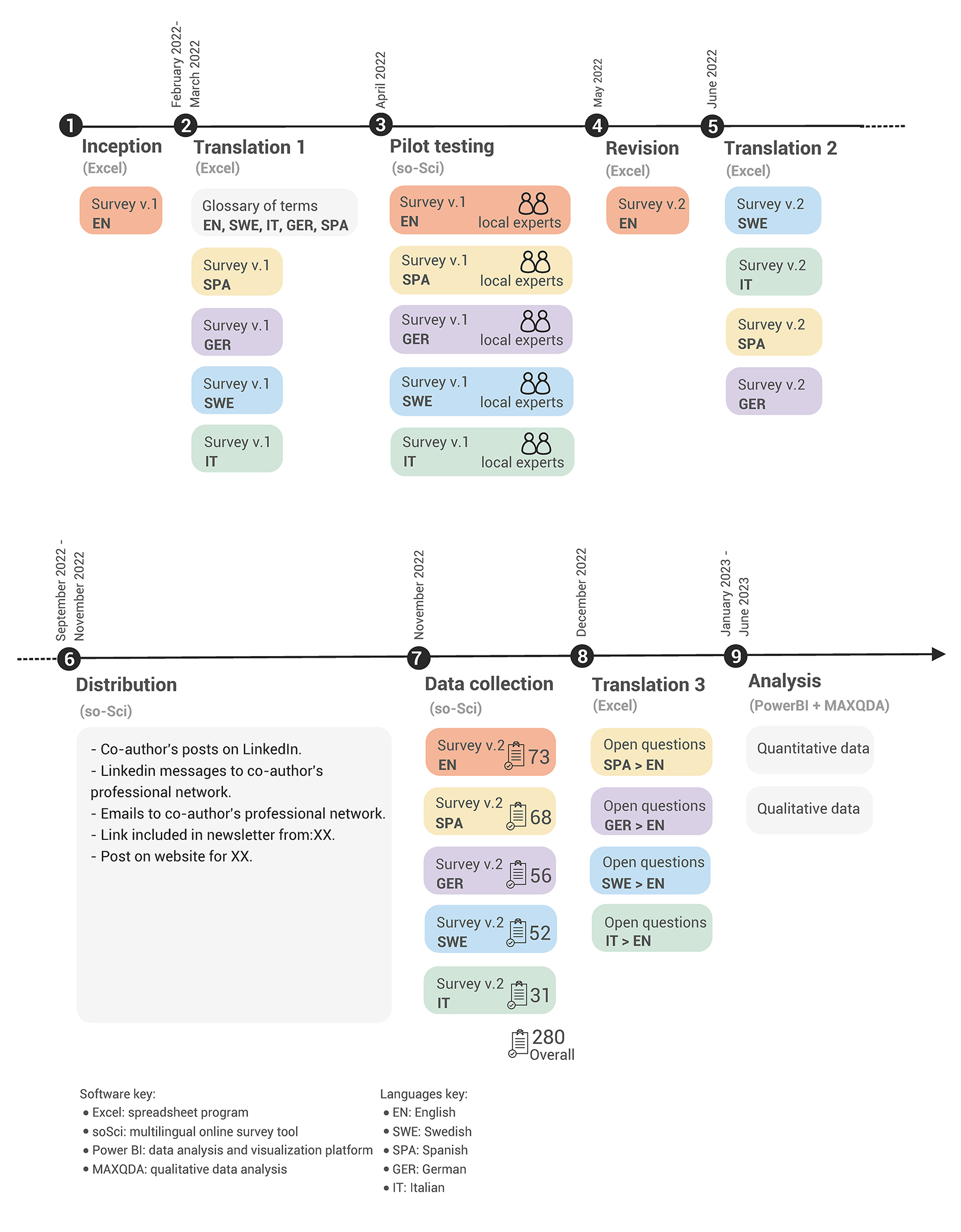
Survey phases diagram.
The survey consisted of six content sections with introductory questions to filter out respondents who had no recent experience in this field or did not report using hospital design benchmarking (Figure 2). The survey platform did not save any personal information from respondents. Only when the survey was finished, respondents interested in learning more about the survey results or further research collaboration were free to contact the authors or enter their email addresses independently from their answers to the survey.
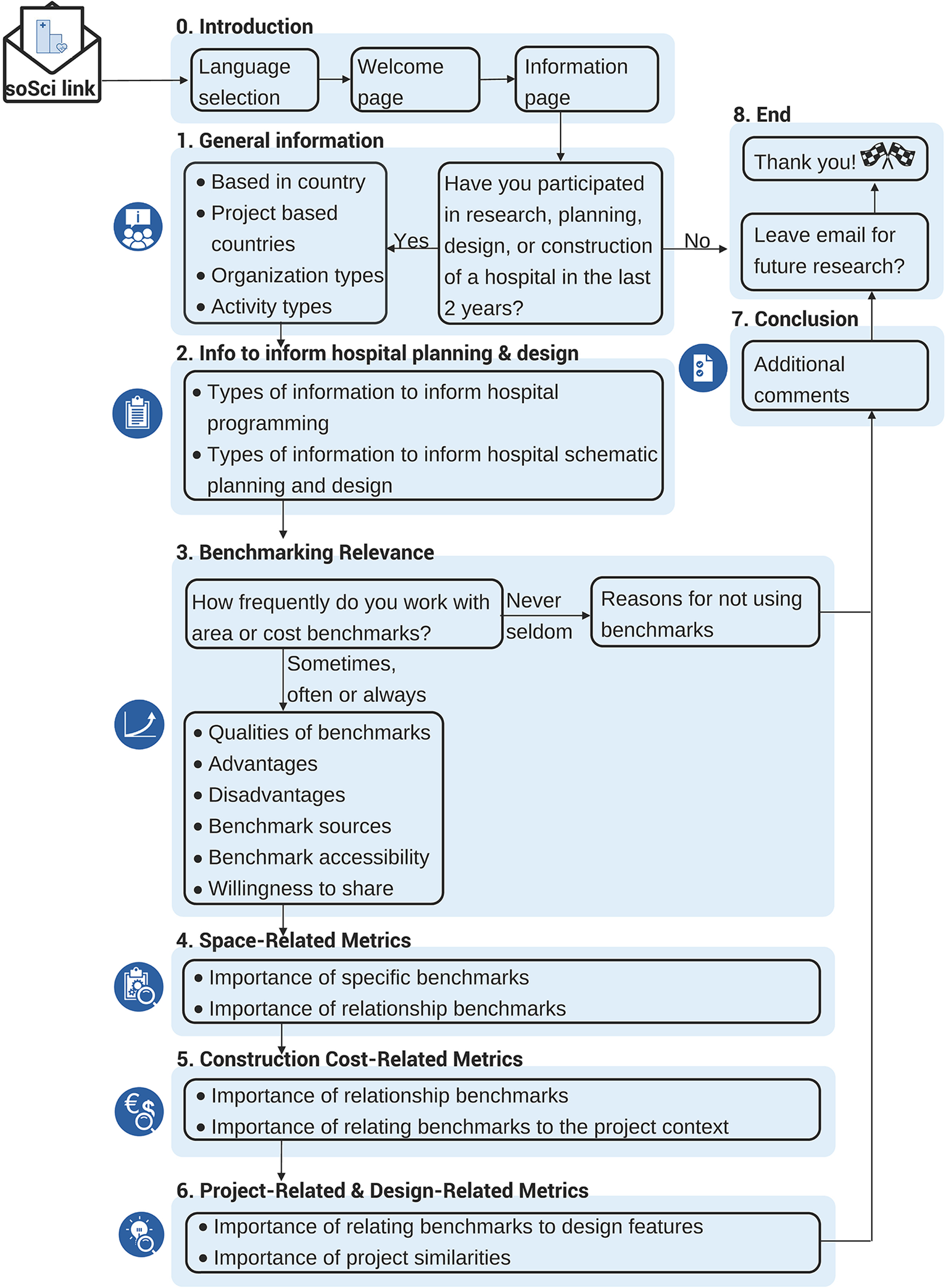
General overview of the survey flow.
Data Analysis
The survey results included quantitative and qualitative data.
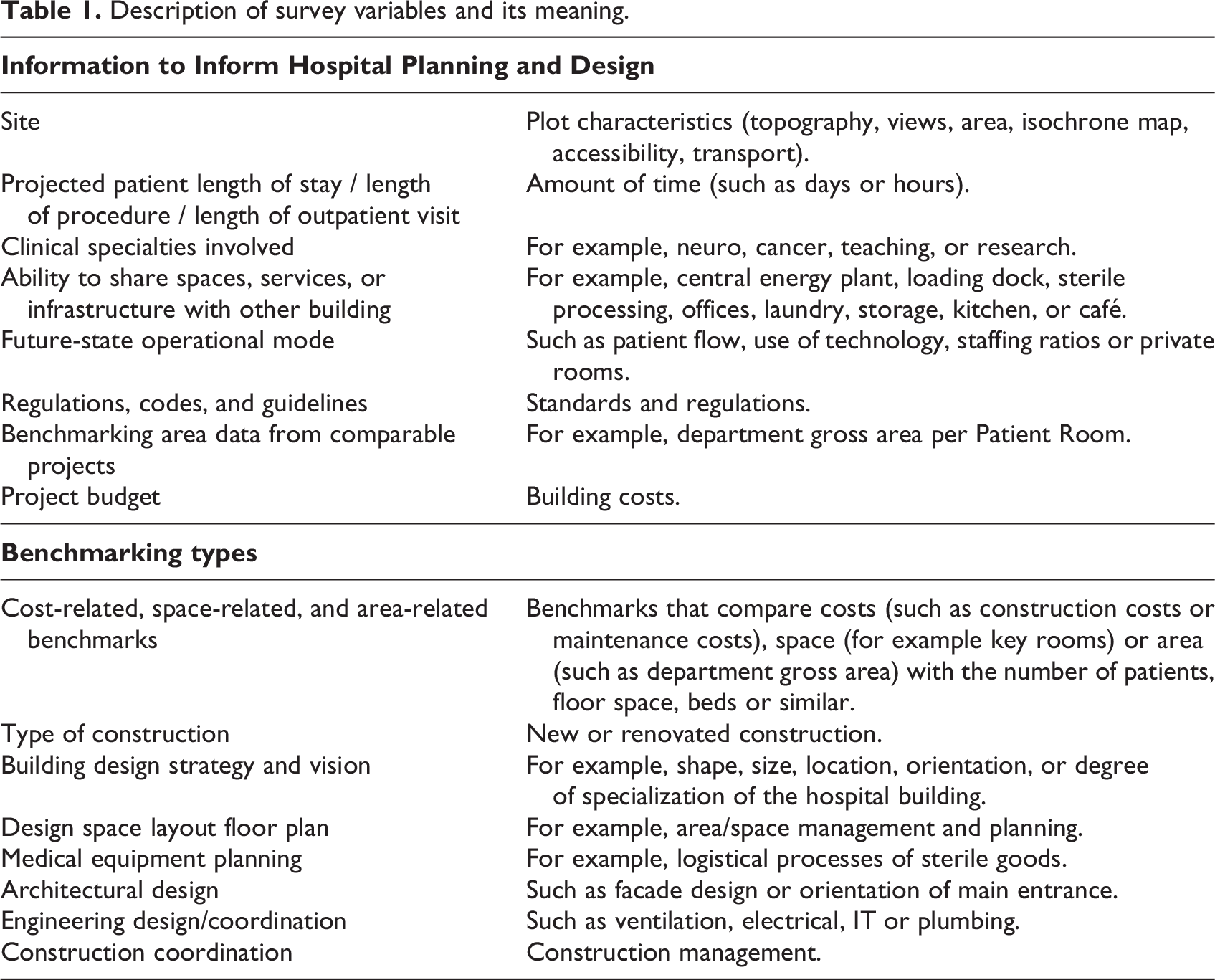
Quantitative data were collected using two 5-point Likert-type scales to rate frequency and relevance. The scale for frequency ranged from never (1) to always (5) while the scale for relevance, ranged from not important (1) to very important (5). The variables listed in the questions are defined in Table 1.
Description of survey variables and its meaning.
The results were analyzed using Microsoft Power BI version 2.1, a software for preliminary analysis and for creating charts. Inferential analysis was conducted in R 4.3.0/R Studio software for statistical computing. Analysis of variance testing was performed to determine the statistical significance of differences across respondents from specific groups.
Qualitative data were collected using open-ended responses. This format provided opportunities to reflect on answers not shown as default response options and generate novel responses (Porst, 2014). Data coding was considered for the analysis of free-text responses (Popping, 2015; Rädiker, 2020) using the software MAXQDA Version 2022.4.1 (2023-01-17). This software helped to subcategorized according to the answers given (inductively), and then super-categorized at a macro level to create meaningful clusters of information.
Results
The survey was started by 530 persons and 280 respondents fully completed the survey (success rate: 53%), respectively, from English (26%, n = 73), Spanish (24%, n = 68), German (20%, n = 56), Swedish (19%, n = 52), and Italian languages (11%, n = 31).
Where Do They Work?
The 530 persons who started the survey came from 38 different countries. The five top countries with the highest participation were Sweden, Spain, Germany, Italy, and the United States. The prevalence of organization types responding varied across countries (Figure 3), Sweden had many responses from healthcare planning/management agencies (governmental) while this sector was not strongly represented in other countries, probably due to cultural differences in healthcare systems. In Italy, many hospital projects are led by engineering firms with subcontractors doing architectural design, which may explain the low number of responses from architecture/design firms in that country. For the United States, nearly all responses were from architecture/design firms. In general, most of the respondents (48%, n = 133) were from architecture/engineering firms.
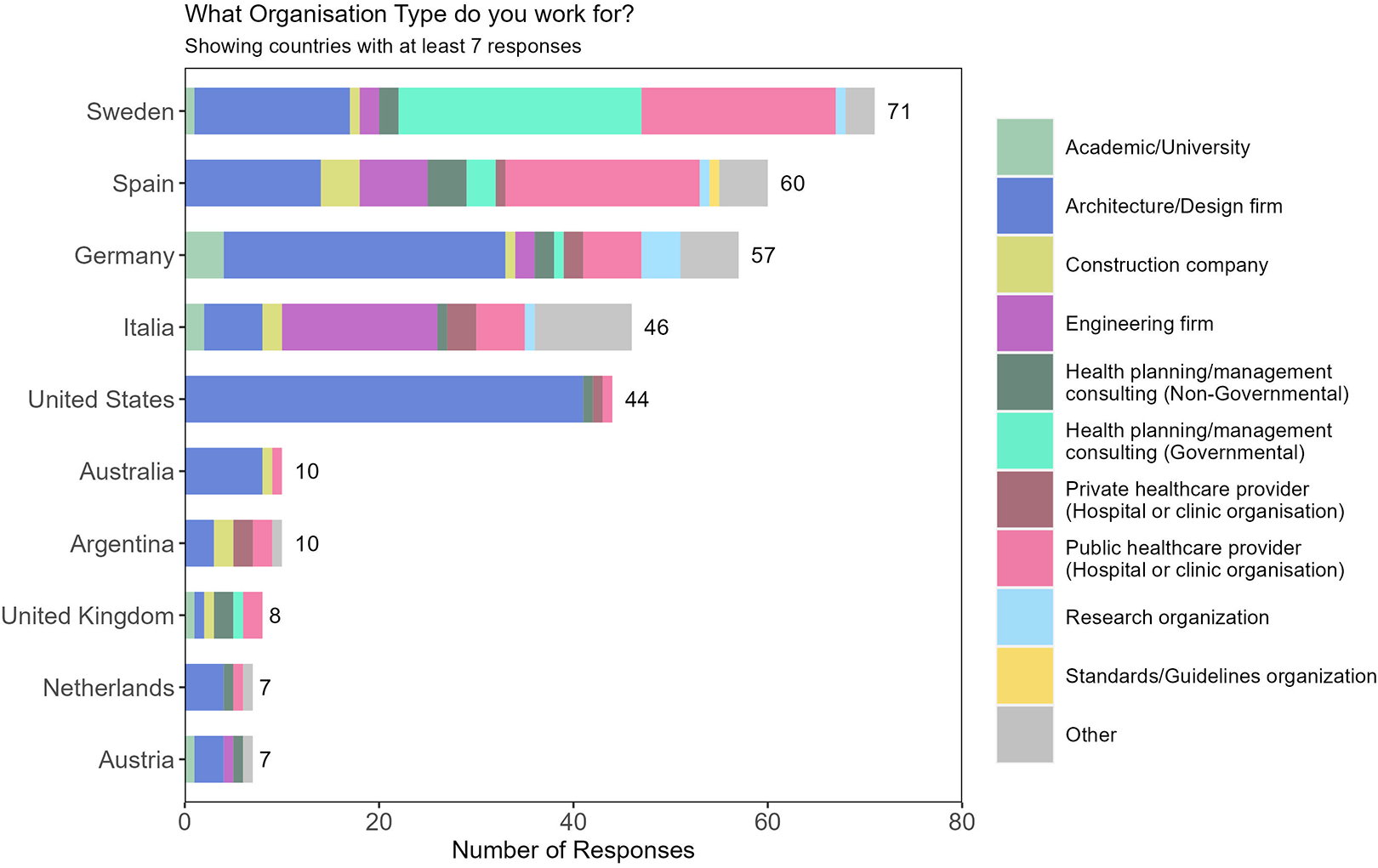
Prevalence of organization types within different countries respondents.
In terms of internationalization, from the top five countries the respondents worked in 62 countries in the past 3 years (44 when considering only respondents in architecture/design firms and engineering firms).
Specifically, from Sweden, 33% of respondents (n = 6) have worked in other countries, notably in Germany and the United Kingdom. From Spain, 50% of respondents (n = 10) have worked in other countries, with the majority being in Central and South America. From Germany, 33% of respondents (n = 10) have worked in other countries, with the distribution quite spread across many countries. From Italy, only 18% of respondents (n = 4) have worked in other countries. Finally, from the United States, 57% of respondents (n = 21) have worked in other countries, primarily Canada and China. Interestingly, although many Spanish and Swedish respondents work in other countries, no one reported working in Sweden or Spain from outside those countries (Figure 4).
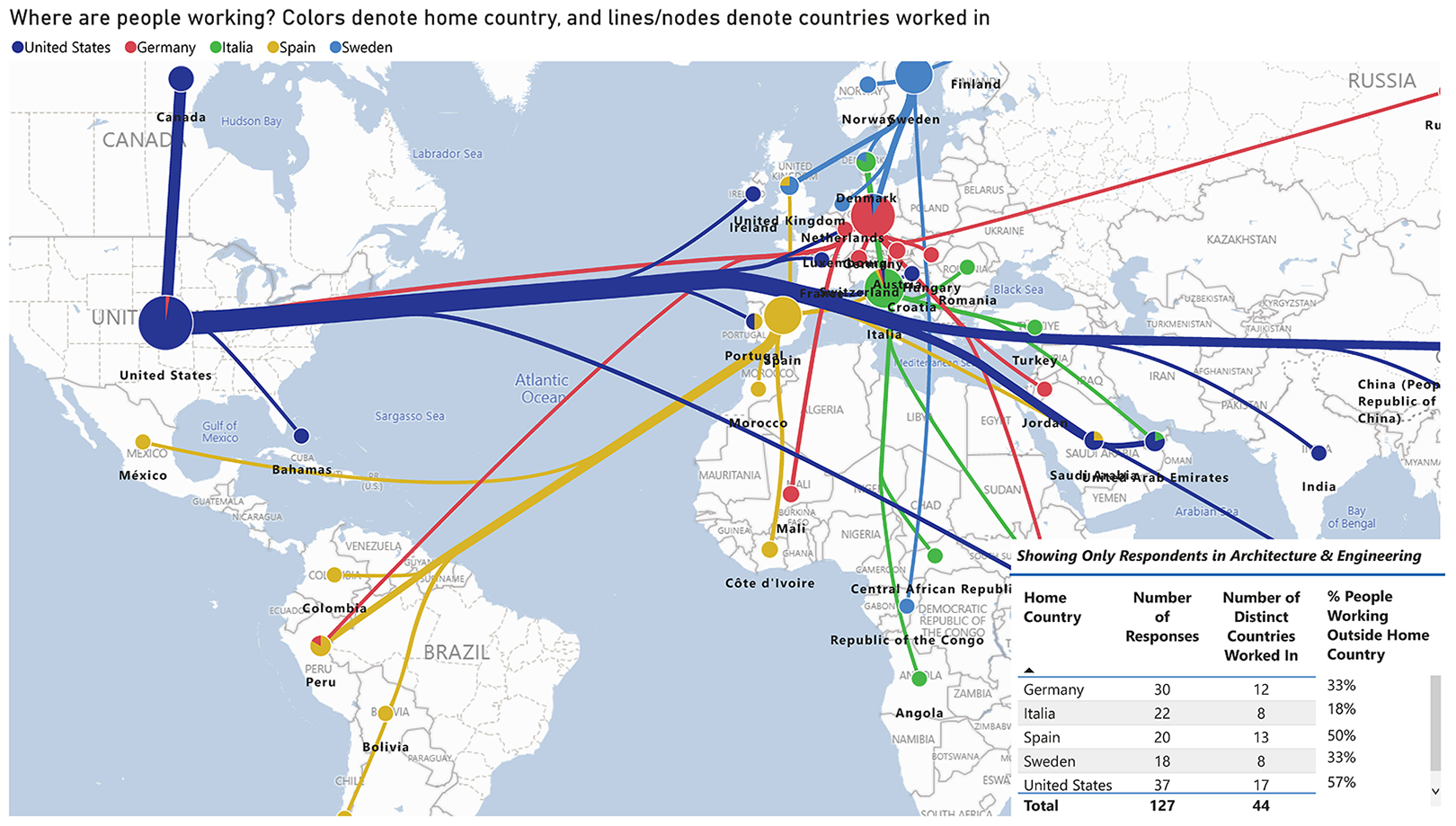
Relationships between home countries of respondents and countries in which they have significant experiences in hospital planning or design.
Who Does What?
Across all countries, public healthcare providers and health planning/management agency (governmental) performed “health planning activities” significantly less frequently than did their private counterparts.
Practice differences emerged between architecture/design and engineering firms in different countries. The difference in practice was analyzed for respondents from (A/E) firms in the top five responding countries. Analysis shows American and Italian respondents report performing planning and research tasks more often than did Swedish architects (Figure 5).
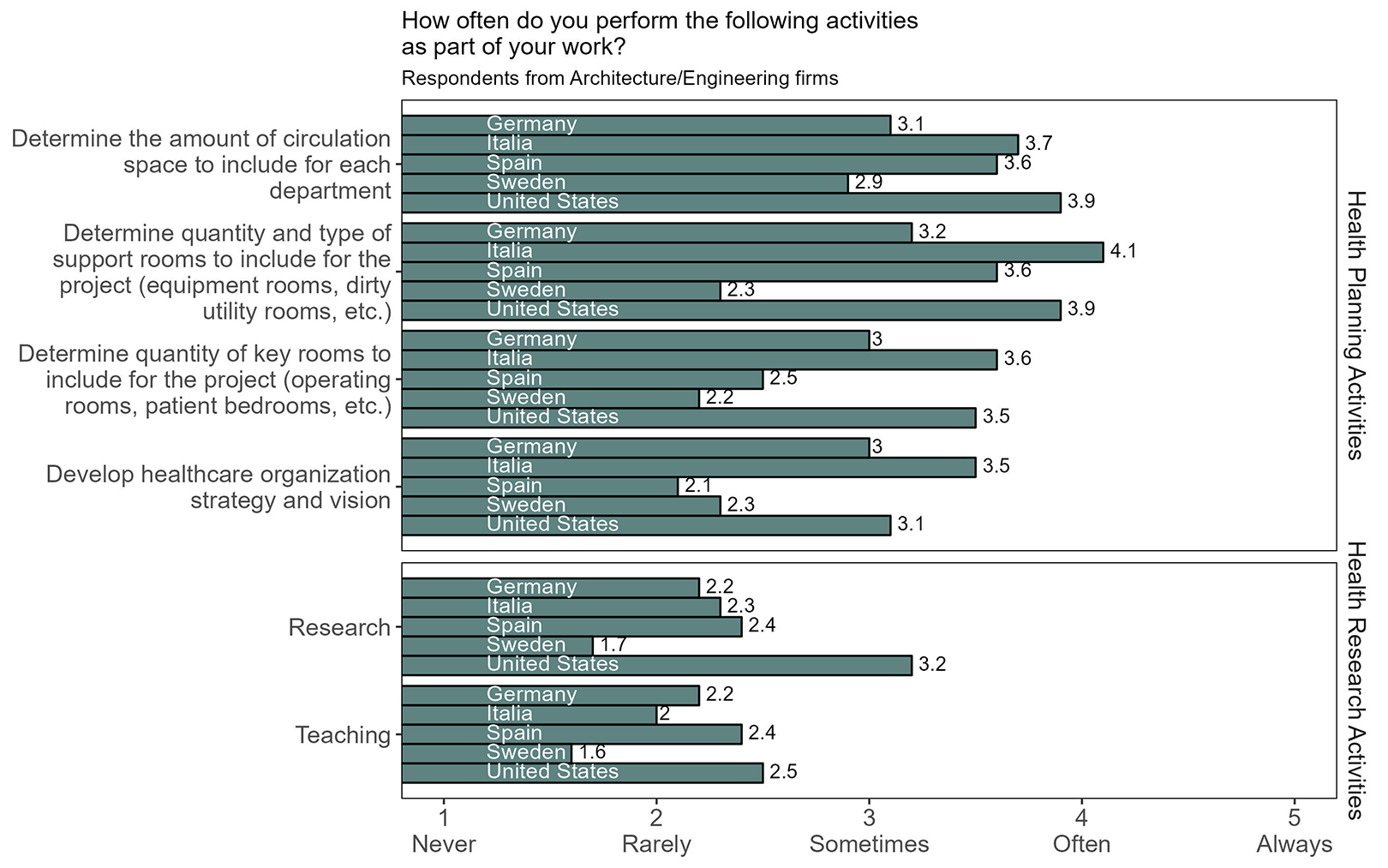
Prevalence of replies about planning activities in different countries.
Other “Health Research,” such as research, teaching, developing standards or guidelines, or doing comparisons of past projects obtained the lowest response scores (1.6 to 3.2 out of 5; Figure 5). Globally, they are mainly done by healthcare planning/management consulting (nongovernmental) firms, while governmental ones are focused on “standards development” activities. Diversities emerge when looking only at architecture/design and engineering firms. In the United States and Australia, “benchmarking and research” emerged as quite frequent (3.2 to 3.6 of 5) as well as “Developing Standards or Guidelines” (3.2 of 5). Italy rated the lowest for these activities (1.8–2.6 of 5; Figure 5).
When asked to report on “design and construction activities,” respondents from architecture/design firms in the top five responding countries reported that they often or always (4.4 of 5) produce design space layout floor plans, while respondents from all other organization types report perform such activities only sometimes (3.3 of 5; Figure 6). Respondents from architecture and engineering firms and private healthcare providers in the top five responding countries were also more likely than their counterparts from other organizations to be involved in developing a building design strategy and vision (4.04 and 3.8 respectively, of a possible 5). Public healthcare providers reported participating in building design strategy and vision activities slightly less than did their public counterparts (3.8 and 3.1, respectively, of a possible 5).
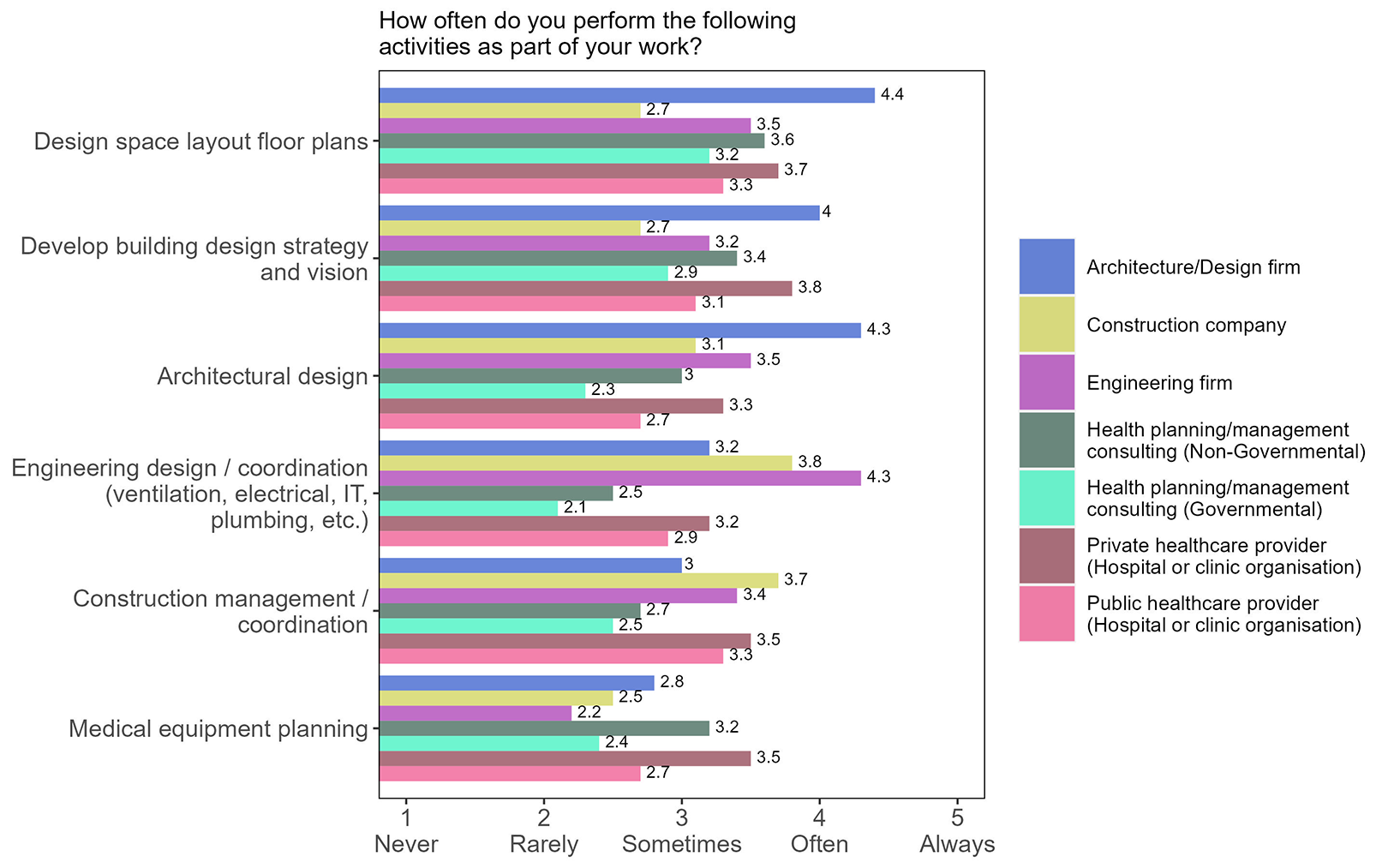
Frequency of hospital planning activities among respondents.
Which Information Do They Use?
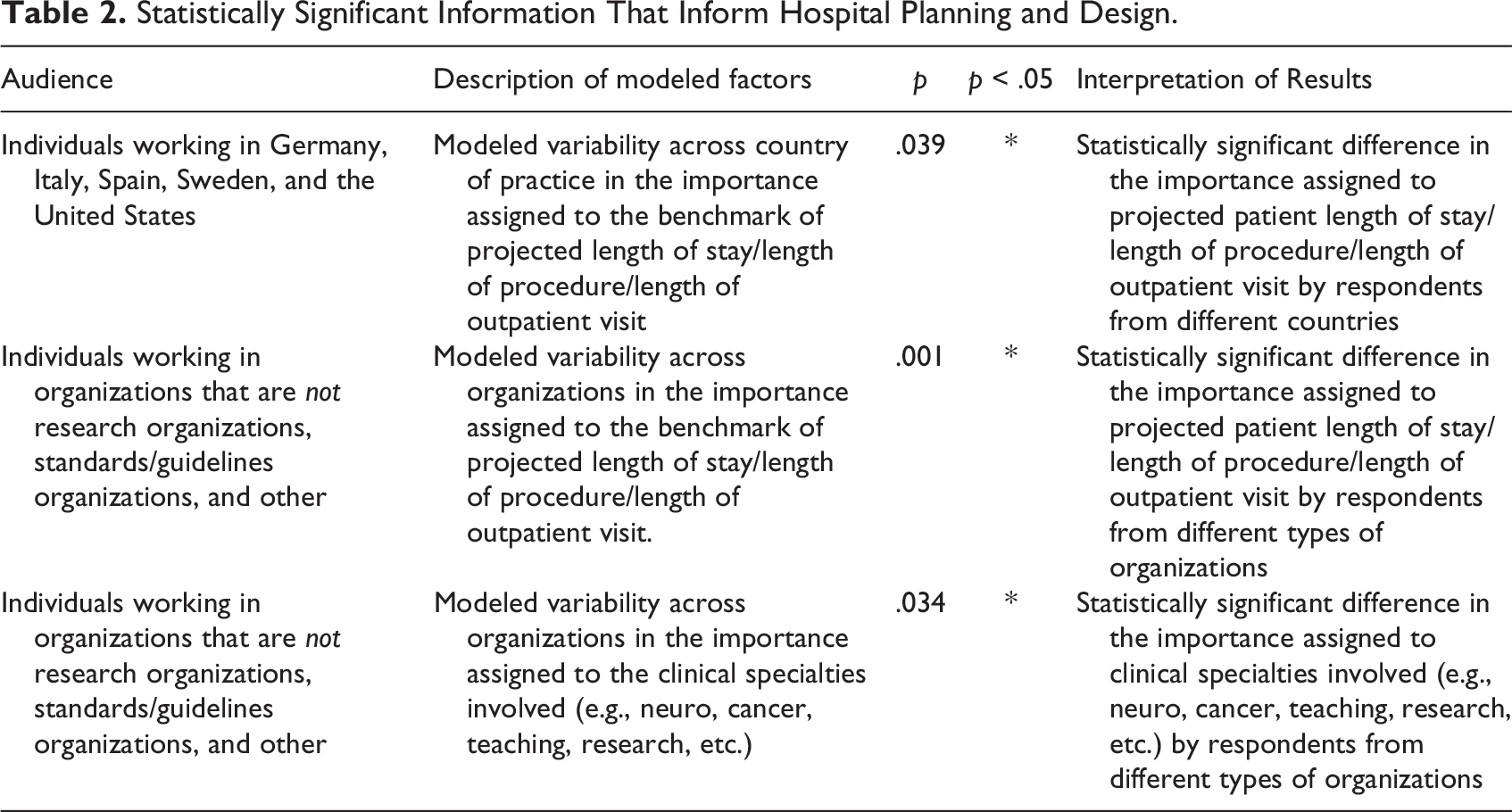
In terms of information to inform hospital planning and design, the analysis showed a statistically significant difference between respondents from the five countries analyzed in the relative importance assigned to specific benchmarks, including patient length of stay/length of procedure/length of outpatient visits (p = .039). Respondents from the United States were more likely than respondents from Germany, Italy, Spain, and Sweden to say that this metric is “important” or “very important” for planning. The analysis also revealed a significant difference in the importance of this metric across different types of organizations (p = .001). Private healthcare providers rated this metric as more important than other groups. This analysis excluded research organizations and standards and guidelines organizations due to low response from these groups. There was a statistically significant difference (p = .034) in the importance that respondents from different types of organizations assigned the metric of clinical specialties involved (e.g., neuro, cancer, teaching, research). There was also a statistically significant difference across organizations in the importance assigned to metrics related to projected growth in patient volume (p = .049). Across countries, respondents differed in the importance they assigned to metrics related to healthcare resources in the project area. Respondents in the United States and Spain rated these factors as more important than did respondents practicing in the other countries.
Respondents were also asked to rate the importance of relevant factors for hospital schematic planning and design. The only metrics where the importance differed between the programming phase and the design phase were site/plot characteristics and the projected length of stay. Site and plot characteristics were indeed considered more important during the design phase, and the projected patient length of stay was considered more relevant during the programming phase (Table 2).
Statistically Significant Information That Inform Hospital Planning and Design.
How Frequently Are Benchmarks Used?
Frequency of benchmarking use differed significantly (p = .002) across organization types. Respondents from academics/universities reported they rarely (2.3 of 5) work with benchmarking, while respondents from private healthcare providers often (4.3 of 5) work with them. There was also a statistically significant difference in the frequency of use reported by respondents from the top five responding countries (p = .004). Cost-related metrics are often taken into account in the planning process, especially in Italy (4.2 of 5), Germany (4.1 of 5), and Spain (4.0 of 5). In Sweden, this is only sometimes the case (3.0).
In terms of advantages and disadvantages of using benchmarking, the inductive analysis clustered the individual responses into supergroups.
Firstly, the advantages were grouped into three categories: efficiency, standardization, and confidence (Figure 7). Efficiency was linked to having a head start, more support or orientation at the beginning of the process, and better communication with clients. Regarding the category standardization, several subcategories were emphasized such as comparability, consistency, area benchmark and reference: “helpful for generally always required functional areas”. In relation to confidence, terms such as reliability, accuracy, error prevention, or budget emerge from the open responses.
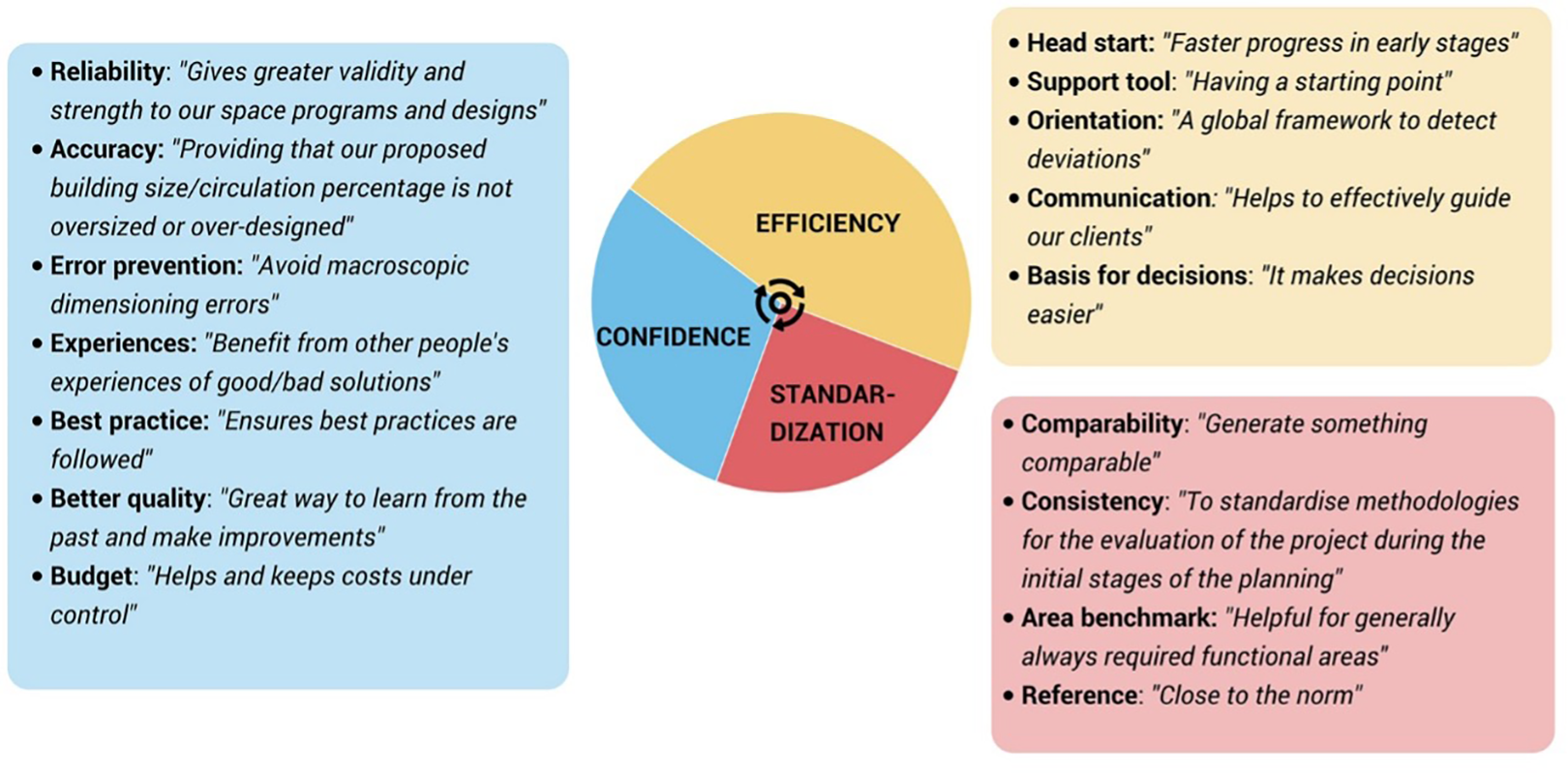
The advantages associated with leveraging benchmarking are organized into categories including efficiency, standardization, and confidence. Factors related to each are listed in the box of the corresponding color.
Secondly, the disadvantages were grouped into the following categories: rigid, incomparable, misleading, and time-consuming (Figure 8). Within the rigid group, several people thought benchmarking could limit creativity, become a restriction, or avoid differentiation: “simply suggest a range of what everyone else is doing.” The incomparability was related to the difficulty of benchmarks transferability. In terms of misleading information, several aspects such as costlier buildings, deviations, or lack of reliability were appointed. Finally, relating to time-consuming, some people thought that they involved a time delay in the project and needed a continuous updating: “reflect older not current projects.”
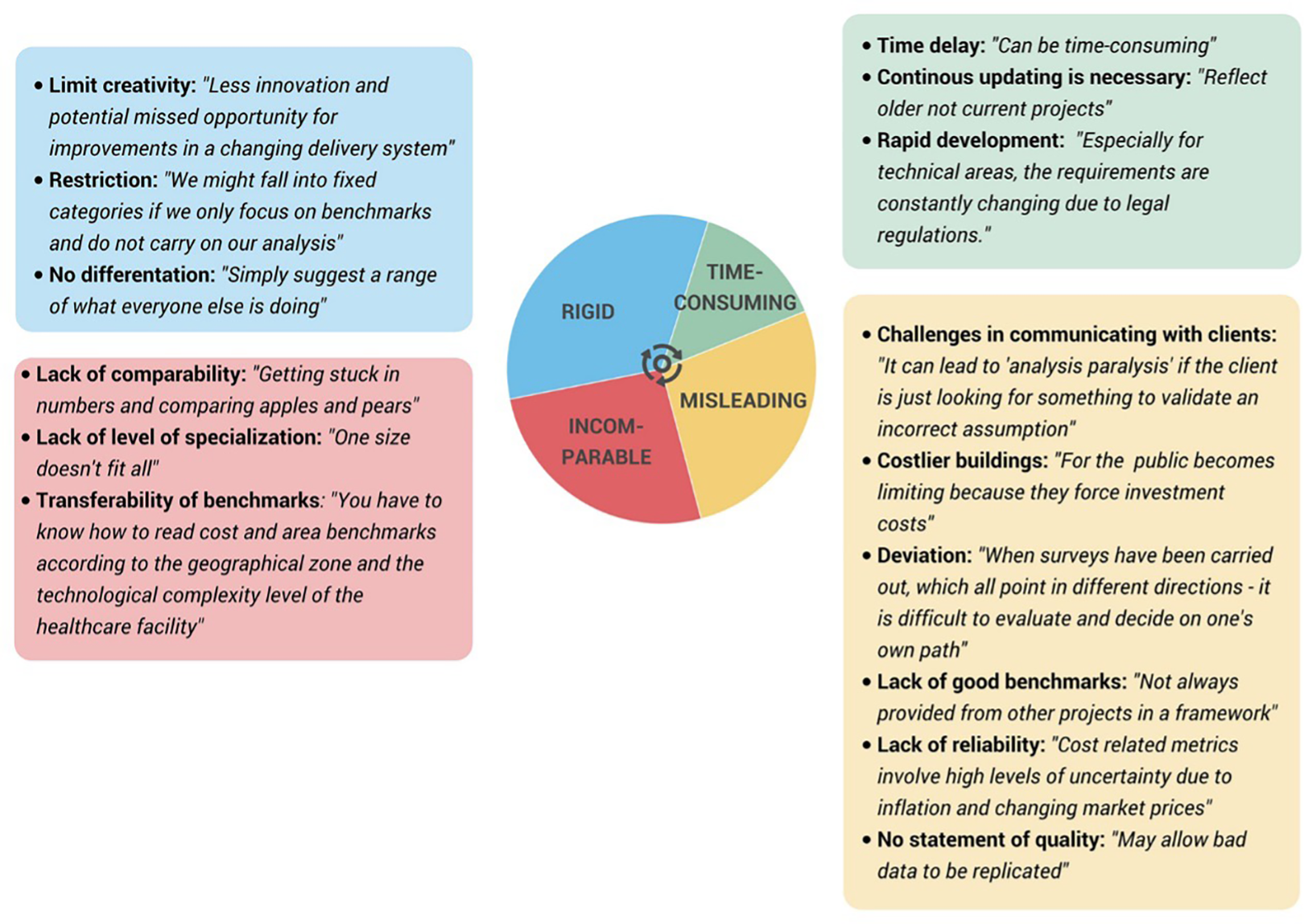
The disadvantages associated with the use of benchmarking are organized into categories according to common factors. These themes are related to the rigid nature of benchmarks, the lack of comparable data, the presence of misleading data and the time associated with the use of benchmarks. Factors related to each theme are listed in the box of the corresponding color.
Apart from the advantages and disadvantages, sources for benchmarking are reported to be mainly firm-wide sources (the own company) with a statistically significant difference between the countries (p = .007).
The qualitative analysis of the individual answers given shows that operating (patient data), cost, and area benchmarks are the most difficult to obtain. Willingness to share benchmarking data was statistically significantly different between countries, primarily due to German respondents indicating reluctance to share. Respondents were most likely to indicate they would be willing to share benchmarks only within their own company (always in all countries) rather than other categories such as the general public.
Top Benchmarks
Space-related metrics are globally considered as very important elements for the design and planning of healthcare facilities scoring in a range between 4.0 and 4.8 of 5. A statistically significant difference (p = 0.004) has been found in the frequency of use of department gross area as a benchmark across respondents from different countries. Practitioners in the United States, Sweden, and Spain viewed department gross area as a statistically significantly more important metric than did those in Germany and Italy (p = .004). Given that department gross area was rated less important in Italy and Germany, the corresponding space-relationship metrics (department grossing factor and department gross area per key room) were also rated less important. In contrast, these were rated as always important in the United States and Sweden. Surprisingly, the net to building grossing factor was rated important in most countries, though rated neutral/indifferent in Germany. Moreover, the metric building gross area per bed was rated important in most countries though neutral/indifferent in Sweden.
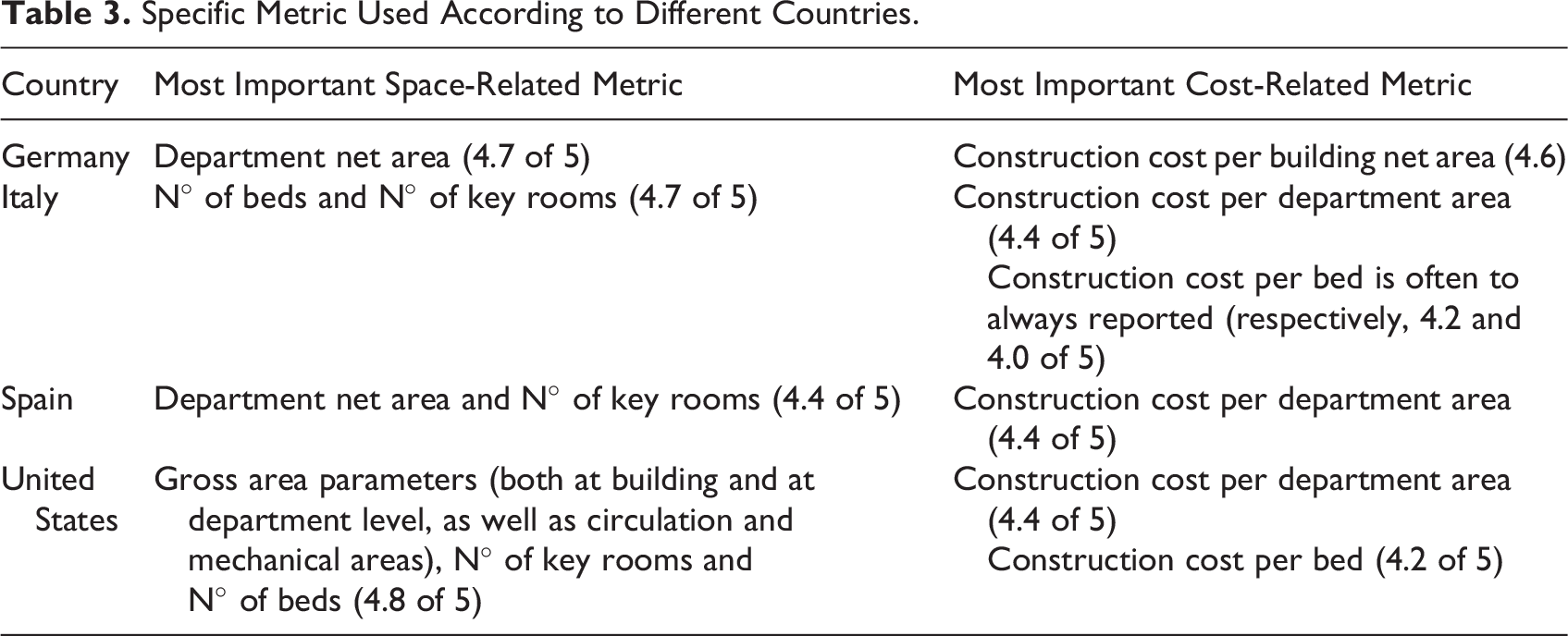
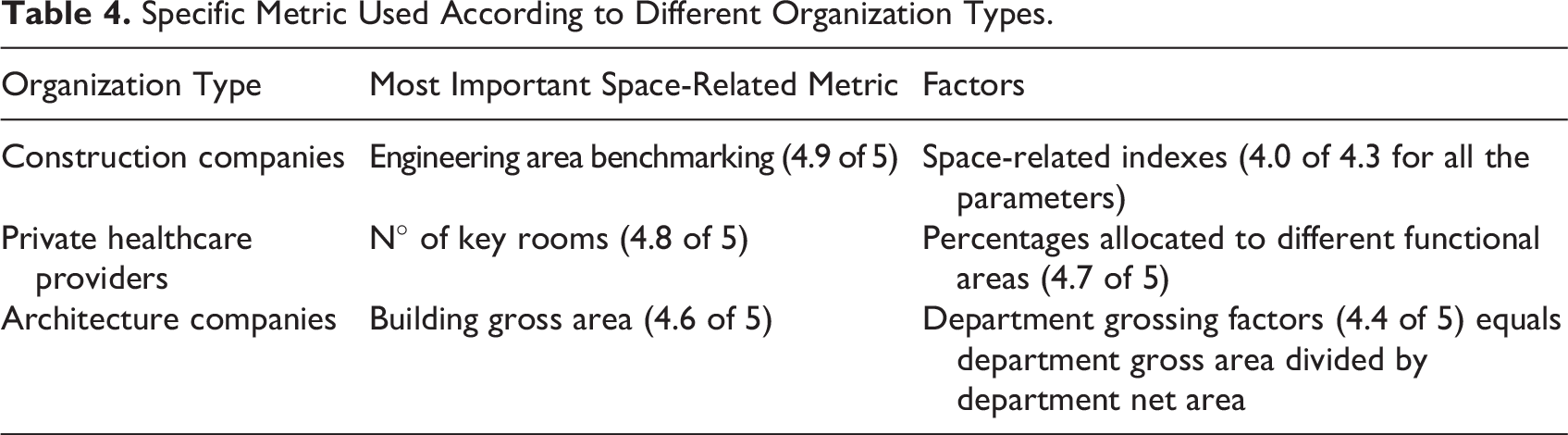
In terms of cost-related metrics, all the countries consider the ratio construction cost per building gross area as the most important (between 4.3 and 4.7 of 5). For both metrics type, minor differences on the specific metric used according to different countries or organization type as reported in Tables 3 and 4.
Specific Metric Used According to Different Countries.
Specific Metric Used According to Different Organization Types.
The most important metric for benchmarking comparability for respondents from the top five countries was whether the project is new construction freestanding, new construction attached to an existing hospital, or interior renovation (4.5 of 5). Respondents also generally rated the metrics of construction date, client type (public vs. private), and country of location as most important. Other metrics that were consistently globally rated as important (4 of 5) included inpatient unit layout, walking travel distances, number of stories, and if all patient bedrooms are private. In contrast, less importance (3.5 of 5) was given to benchmarking the number of months taken for design or construction. Respondents from the United States and Swedish architecture/design and engineering firms were statistically (p < .001) more likely than those from other countries to indicate that patient type metric (outpatient vs. inpatient) is very important (4.7 of 5) to consider. Respondents from the United States and Spain were statistically (p = .012) more likely to assign high importance (4.5 of 5) to the patient treatment type benchmark (cancer, neuro, ortho, etc.) than their counterparts in Sweden, Italy, and Germany (3.8 of 5). Finally, Swedish respondents assigned statistically significantly (p = .015) greater importance (4.8 of 5) to the number of outpatient visits, while German respondents rated this as less important than those from other countries (3.6 of 5). Generally, respondents also think that it is important to compare projects if they have similar hospital type, country, and care model (4 of 5).
Finally, comparing organization types, respondents from healthcare planning/management agencies (governmental) felt it very important (4.2–4.5 of 5) that benchmarked projects have similar health system types and similar models of care, while healthcare planning/management consulting (nongovernmental) felt this less important (3.5–3.6 of 5).
Discussion
This article shed light into the perspectives from professionals in the hospital design and planning sector regarding benchmarking. The results provide an overview of the countries were these people work, the type of organizations involved in the sector, the tasks they perform, the information they base their decisions on, the way they feel about benchmarking, and the top benchmarks used in the industry. The following discussion relates our results with relevant aspects such as the globalization of the hospital design and planning practice, the discordances in benchmarking, and finally, the success of benchmarking in practice.
Globalization in Practice
Our study shows that most hospital planning and design work in a country is performed by persons living in that country, but there is also a significant amount of cross-border work. For all countries, approximately 30%–50% of hospital planning and design practitioners report doing work outside their home country. Thus, it is important for practitioners to have an awareness of varying regulations, cultural norms, and benchmarking practices. Interestingly, the design expertise can be “exported” or “imported” internationally. Those in the United States, Sweden, Germany, Spain, Italy, and Australia were very likely to work in other countries, though often not in the same countries. However, it appears rare that persons from outside the country are working there—thus, these countries currently “export” expertise but do not “import” it. In contrast, design expertise was reported to often be “imported” to South America, Africa, the Middle East, China, and other Asian countries.
There was also some variation in the types of work that practitioners perform in various countries. For determining the healthcare organization strategy and vision or determining the number of key rooms (operating rooms, bedrooms, etc.), our data show that this is sometimes done by architecture/design and engineering firms in Italy and the United States but rarely by those in Spain or Sweden. Space programming activities such as determining quantities and types of support rooms (equipment rooms, soiled utility, etc.) or determining the amount of circulation space are often done by architecture/design and engineering firms in Italy, Spain, and the United States but sometimes or rarely done by those in Sweden and Germany. A practical implication of these results can be that if an organization often determines the amount of circulation space to include in a department, then they will greatly benefit from benchmarking information on department grossing factors. Moreover, if a practitioner often works internationally, they will benefit from benchmarking comparisons of room sizes and room counts varying by country. This is consistent with the idea of continuous improvement through competitive benchmarking, which is already well-established (Sharma et al., 2021).
Discordances in Benchmarking
Benchmarking was deemed relevant by all practitioner types and all countries included in the survey, with some variation. As one may expect, architecture firms use area-related metrics more than cost-related metrics, while engineering and construction firms are the opposite. Germany, the United States, and Spain rated highly for often having firm-wide benchmarks available at one’s own company, while Italy and Sweden rated lower (statistically significant). Italy and Sweden also rated slightly lower for having industry-wide benchmarks available. This may denote an opportunity in these countries—however, in all countries, the highest frequency was benchmarks from one’s own personal experience. Most respondents didn’t report having difficulty in finding the benchmark information they needed. This may mean that their information may be just from one person and may not include a large sample size of projects or may not include many types of metrics. Such self-collected benchmarks are easier to customize and access but may be less accurate and have a less robust dataset so highly targeted comparisons are not possible without industry-specific metrics (Sharma et al., 2021). Some organizations have developed industry benchmark databases but they are not common as they are a challenge to develop consistently and to maintain up-to-date. For example, the Construction Industry Institute at the University of Texas several years ago created an extremely robust hospital design benchmarking database, but information now appears to be sparse (Kahn, 2009; Mulva & Dai, 2009). As another example, the Australasian Health Facility Guidelines (AusHFG) include benchmarking ratios of department grossing factors and percentages of circulation space and engineering space; the specific nature of the information may make updating more feasible. Indeed, a third-party organization such as a university or public planning guidelines agency may serve as a means to increase information sharing (Gola et al., 2020). In the survey, a person’s willingness to share information drops dramatically as the dispersion expands from one’s own company to hospital clients to industry organizations to the general public. Public health planning agencies were the most willing to share benchmarking information, while private health planning agencies were the least willing. Surprisingly, public, and private healthcare providers, as well as architecture firms in Italy, are only often willing to share within their own organizations and Germany rated the least likely to share benchmarking information.
Benchmarking Success
A practitioner working internationally could benchmark projects in other countries if they have similar hospital type, similar models of patient care/staffing models, and similar healthcare system types (private vs. public). Among our results for architecture/design firms, across metrics, there was some variation between countries that may be deeper investigated in future studies. For example, a statistically significant difference was found that types of patient care (outpatient vs. inpatient) were rated very important in the United States and Sweden but rated neutral to important in Italy. A potential reason could be that in the United States and Sweden, inpatient and outpatient care are distinct established operational models with different design characteristics, while this clear separation is under development in Italy with specific and new territorial care centers in Italy. As another example, statistical significance was found in that patient treatment type (cancer, neuro, ortho, etc.) was rated between important and very important in Spain and the United States, while it was rated lower in Germany, Italy, and Sweden. A potential reason could be that in the latter countries, spaces are designed more generally (flexible universal design) to accommodate a variety of clinical specialties (Brambilla et al., 2021). The most important context metric was that hospitals benchmarked be of similar types (cancer, general, academic, etc.). This is in alignment with open-ended responses which often discussed the importance of making comparisons meaningful and accurate and literature on benchmarking within the healthcare industry (Thonon et al., 2015).
Survey results indicate that traditional project drivers (such as future-state operational models, regulations, guidelines or budget) were more relevant than benchmarks to programming and planning. This finding is consistent with the results of previous studies (Cambra-Rufino et al., 2021). Interestingly, respondents across countries and across practitioner role type rated future-state operational model as a slightly more important programming driver than project budget. However, after the programming phase completes, the two factors were rated similarly for the planning phase. As expected, the anticipated growth in patient volumes was rated the most important driver for programming, while the clinical specialties involved was also rated very highly (e.g., neuro, cancer, teaching, research). Respondents denoted different priorities for the planning phase, with the most important drivers being the space program in addition to access to daylight and outdoor views. Interestingly, there was not a lot of variety across countries on these topics despite cultural differences. For example, architects in the United States commonly perform space programming, while this is rare in Canada or Australia. Thus, the driver may be important regardless of who performs the work.
Conclusions
This international survey on the use of benchmarks for hospital design and planning collected quantitative and qualitative data from 280 specialist respondents worldwide.
The findings reported in the study allow both specific insights per each country or category as well as general considerations of a practice that is becoming always more international. Benchmarking emerges as a very important tool for hospital design and planning which is currently underutilized due to difficulties in international comparison, data availability outside each specific company as well as specific design metrics. Further studies are needed to expand the knowledge on this topic.
In more detail, the survey revealed that for the majority of respondents benchmarking in hospital design and planning is important. Four conclusions can be summarized. (1) Across all countries examined in the study, architecture firms use area-related metrics more than cost-related metrics, while the opposite is true for engineering and construction firms. Specifically in relation to area benchmarks, a uniform opinion in most countries showed the importance of the metric “building gross area per bed.” This shows the overall number of beds is still a key planning factor. Practitioners in the United States, Sweden, and Spain consider department gross area as a more important metric than those in Germany and Italy. One reason for this is the fact that this metric (department gross area) is not defined in German standards (DIN 277, 2021). It can also be concluded from this that the net-to-gross building factor was classified as important in most countries, but as neutral/indifferent in Germany. (2) Across all countries surveyed in the study, public health planning agencies were the most willing to share benchmarking information, while private health planning agencies were the least willing, constituting barriers to creating global benchmarking strategies. (3) “Patient type (outpatient vs. inpatient) was rated very important in the United States and Sweden but rated neutral to important in Italy.” (4) Patient treatment type (cancer, neuro, ortho, etc.) was rated between important and very important in Spain and the United States, which is significantly higher than the ratings given by respondents in Germany, Italy and Sweden.
Study Limitations and Future Developments
The study involved several practitioners and healthcare-related experts from several countries; nevertheless, only respondents from the most recurrent countries have been included in the analysis; therefore, further research is needed to expand knowledge in other context, such as developing countries. Moreover, starting from the existing dataset, in-depth studies can be performed in each single subsection exploring deeper implications.
Implications for Practice
Practitioners could review their planning process through benchmarking at an early planning stage with a continuous collection and review of benchmarks for actuality. Different countries use different definition of building/department gross/net area, therefore practitioners should be very careful when comparing projects with different ratio or normalize them.
More data and up-to-date data should be exchanged between the institutions in order to obtain a wider and more diverse database to enable high-quality benchmarking. Practitioners in Germany, for example, could consider adding another metric during the planning process (e.g., department gross to net area). This would enable benchmarking in an international context in order to identify potential.
Practitioners could use benchmarking to classify the current project status (e.g., costs per building gross area) and use it during communication processes with the client to highlight strengths and weaknesses and to identify the best solutions.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867241239324 - Benchmarking Relevance for Hospital Design and Planning: An International Web-Based Survey
Supplemental Material, sj-pdf-1-her-10.1177_19375867241239324 for Benchmarking Relevance for Hospital Design and Planning: An International Web-Based Survey by Hannah-Kathrin Silja Viergutz, Laura Cambra-Rufino, Michael Apple, Abigail Heithoff, Goran Lindahl, Stefano Capolongo and Andrea Brambilla in HERD: Health Environments Research & Design Journal
Supplemental Material
Supplemental Material, sj-pdf-2-her-10.1177_19375867241239324 - Benchmarking Relevance for Hospital Design and Planning: An International Web-Based Survey
Supplemental Material, sj-pdf-2-her-10.1177_19375867241239324 for Benchmarking Relevance for Hospital Design and Planning: An International Web-Based Survey by Hannah-Kathrin Silja Viergutz, Laura Cambra-Rufino, Michael Apple, Abigail Heithoff, Goran Lindahl, Stefano Capolongo and Andrea Brambilla in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgment
The authors would like to acknowledge the respondents from all over the world who took part in the survey and shared their experience for improving the quality of benchmarking in the entire hospital design and planning global community. Thanks also go to Alexandra Bertsch and Torben Flatemersch for their technical support in creating the online survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research did not receive any funding, but the coauthor Laura Cambra-Rufino obtained a “Margarita Salas” contract within the “Programa de recualificación del sistema universitario español” funded by the Next Generation EU.
ORCID iDs
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.