
Abstract
Objective
The objective of this was to explore how the physical environment in a hospital contributes to care partner inclusion practices.
Background
Despite their vital efforts in caring for people living with dementia (PLWD), care partners of PLWD often report feeling not included in their loved ones’ hospitalizations. This phenomenon goes against research, policy initiatives, and hospital design frameworks that underscore the importance of including care partners in hospital care. To ensure that care partners are systematically included in hospital care, health systems must create an environment that prioritizes care partners’ presence.
Methods
This descriptive qualitative design employs a multimethod approach to data collection. Our team conducted direct observations in a large academic hospital and interviewed 23 clinicians/administrators and 15 care partners of PLWD to understand the relationship between hospital environments and care partner inclusion. Observational data were analyzed using a framework analysis, and interview data were analyzed through thematic analysis.
Results
Direct observations revealed an underutilization of environmental resources such as family-centered spaces and environmental communication tools. Interview data revealed that adequate space for care partners, the layout of patient rooms, parking accessibility, room personalization, and comfort level of the hospital space all impact care partner inclusion.
Conclusion
Our findings highlight opportunities for health systems to create hospital environments that support PLWD and their care partners. In pursuit of systematic care partner inclusion, health systems can make adequate space for care partners, allocate dementia-friendly parking spaces, increase utilization of environmental communication tools, and increase comfort level of the environment.
Keywords
Introduction
Following hospitalization, our healthcare system is increasingly reliant on the care partners (family or friends) of older adults to help meet basic needs. This is particularly true for care partners of people living with dementia (PLWD), whose caregiving tasks increase with disease progression. In 2022, over 11 million care partners provided 18 billion hours of unpaid care to PLWD, valued at $339.5 billion (Alzheimer's Association, 2023). Despite this incredible reliance on care partners for in-home support, care partners often report feeling left out of PLWD's care during hospitalization, leaving them feeling ill-equipped to manage post-discharge care responsibilities (Schulz et al., 2018). Care partners’ feelings of exclusion contrast research and policy on care partner inclusion in hospital care. Including care partners in PLWD hospital care reduces hospital readmission rates and healthcare costs (Alzheimer's Association, 2023; Mollers et al., 2019; Rodakowski et al., 2017). Policy initiatives, such as the Caregiver Advise, Record, and Enable Act and the National Strategy to Support Family Caregivers, advocate for systematic inclusion of care partners in hospital care (AARP, n.d.; Administration of Community Living, n.d.). Implementation of these initiatives may include mechanisms to enhance care partner and hospital team interactions.
To promote care partner presence in the hospital, health systems should ensure that hospital environments are welcoming, comfortable, and considerate of care partners’ needs. This concept is seen in evidence-based design (EBD) in healthcare (Ulrich et al., 2010). The EBD framework categorizes the physical environment of hospitals into nine distinct categories, one being family support spaces (Ulrich et al., 2010). This framework posits other aspects of the physical environment, such as audio and visual aspects, as variables that can influence the care delivery experience (Ulrich et al., 2010). A focus on integrating the family into hospital design can also be seen in the SSAFeR Place approach for designing palliative care environments (Miller et al., 2022). The SSAFeR framework stands for a safe place, shared place, aesthetics, place for family, and reflective place. Like the EBD framework, the SSaFeR Place approach emphasizes the impact of aesthetics and ambiance on the hospitalization experience for the patient and care partners (Miller et al., 2022). The inclusion of family into hospital design frameworks suggests a trend toward increasing care partners’ presence in the hospital.
Hospital environment national initiatives generally focus on increasing sustainability (e.g., initiatives to reduce carbon footprints) (American Hospital Association, n.d.; U.S. Department of Health and Human Services, 2022a) and reducing the incidence of healthcare-associated infections (Centers for Disease Control and Prevention, 2019; U.S. Department of Health and Human Services, 2022b). Guidance surrounding the physical environment for PLWD is generally geared toward PLWD living at home or in long-term care facilities. However, as PLWD are more likely to experience hospitalization and rehospitalization than their counterparts without a dementia diagnosis, it is important to understand how the physical environment impacts their care delivery during hospitalization (Shepherd et al., 2019). Given the research, policy, and frameworks surrounding care partner inclusion in hospital care, this study aimed to explore how the environmental conditions within a hospital setting can impact the degree of care partner inclusion in hospital care.
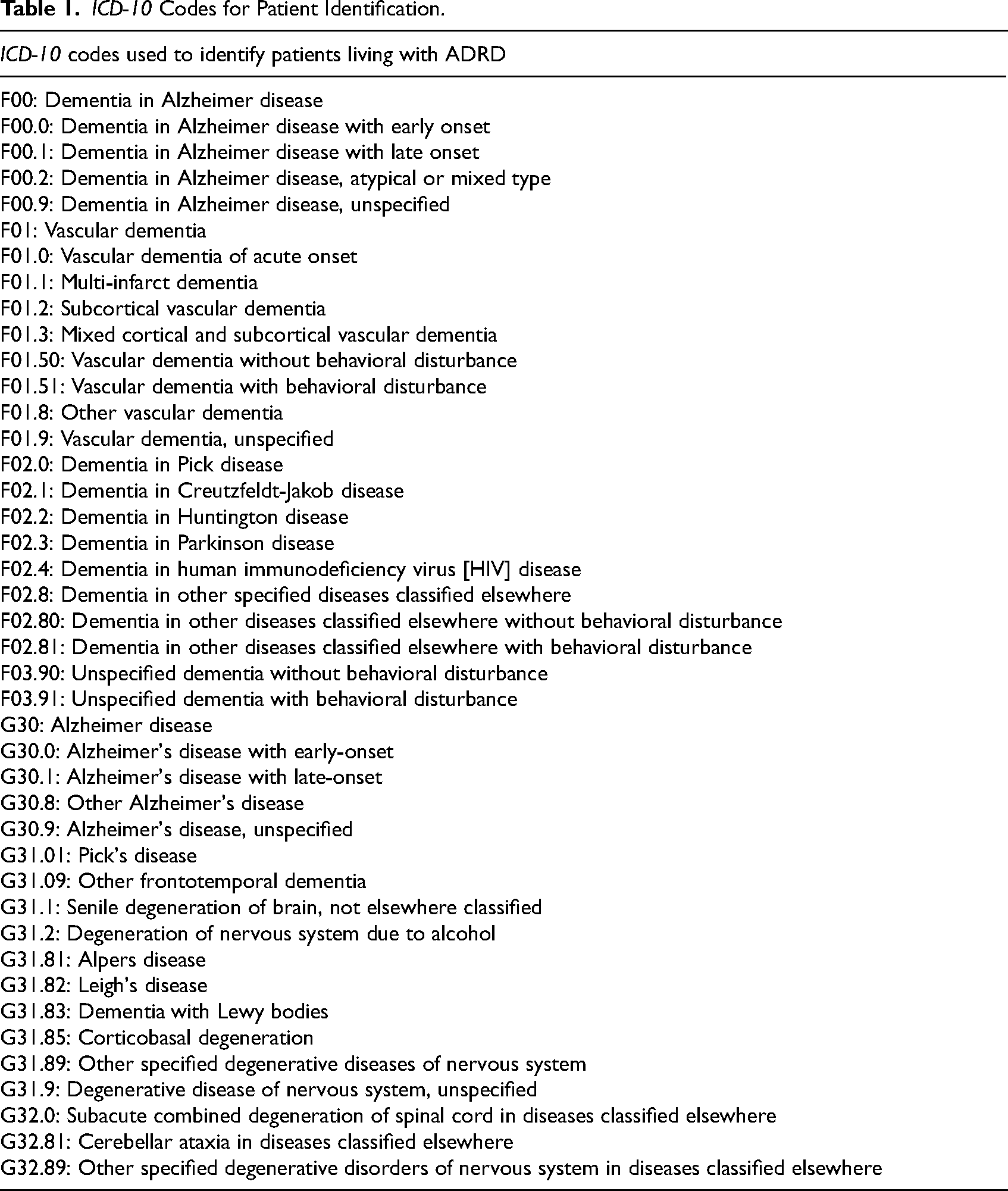
ICD-10 Codes for Patient Identification.
Methods
Design and Setting
This work is part of a larger study on creating the Alzheimer's Disease and Related Dementias (ADRD) Systematic Hospital Inclusion Family Toolkit (A-SHIFT). A-SHIFT aims to guide health systems in systematically identifying, assessing, and educating care partners of hospitalized people living with ADRD. More information on the broader methodology of A-SHIFT can be found in the protocol paper by Fields et al. (2023). The study described in this paper uses descriptive qualitative methods (Sandelowski, 2000) and multiple data sources to investigate the impact of the physical environment on care partner hospital inclusion. This study was approved by the University of Wisconsin-Madison Institutional Review Board.
Observation Data Collection
Our first data source in this study was direct observation of a large academic hospital in the Midwest. This hospital is part of an integrated health system comprising eight hospitals and more than 80 outpatient sites. Our team conducted 27 h of direct observations between September and October 2022. Specifically, we observed how aspects of the physical environment contributed to patterns of care partner inclusion. Since the larger A-SHIFT study was informed by SEIPS-2.0 (Holden et al., 2013), we used this framework's definition of “internal environment” to guide our observations: “lighting, noise, vibration, temperature, physical layout and available space, and air quality” (Holden et al., 2013).
To increase variety in the observed physical environment, our observations spanned four units: trauma/medical-surgical, orthopedic, family practice, and neuroscience/stroke. Observations were completed in 3-h blocks to represent morning, afternoon, and evening shifts. At the beginning of each shift, our team was given a list of patients with a dementia-related ICD-10 code among our targeted units. See Table 1 for a complete list of ICD-10 codes used for patient identification. Team members then floated between these patients’ rooms and, with permission, entered patient rooms when care team members provided care to the patients. Additionally, team members documented inpatient unit layouts and environmental resources. We used Vosaic software to record our observations and took qualitative field notes during each 3-h block shift (Nelnet Business Services, 2016). All data were collected and stored on lab-issued laptops, which were password-protected and kept in a locked lab space.
Interview Data Collection
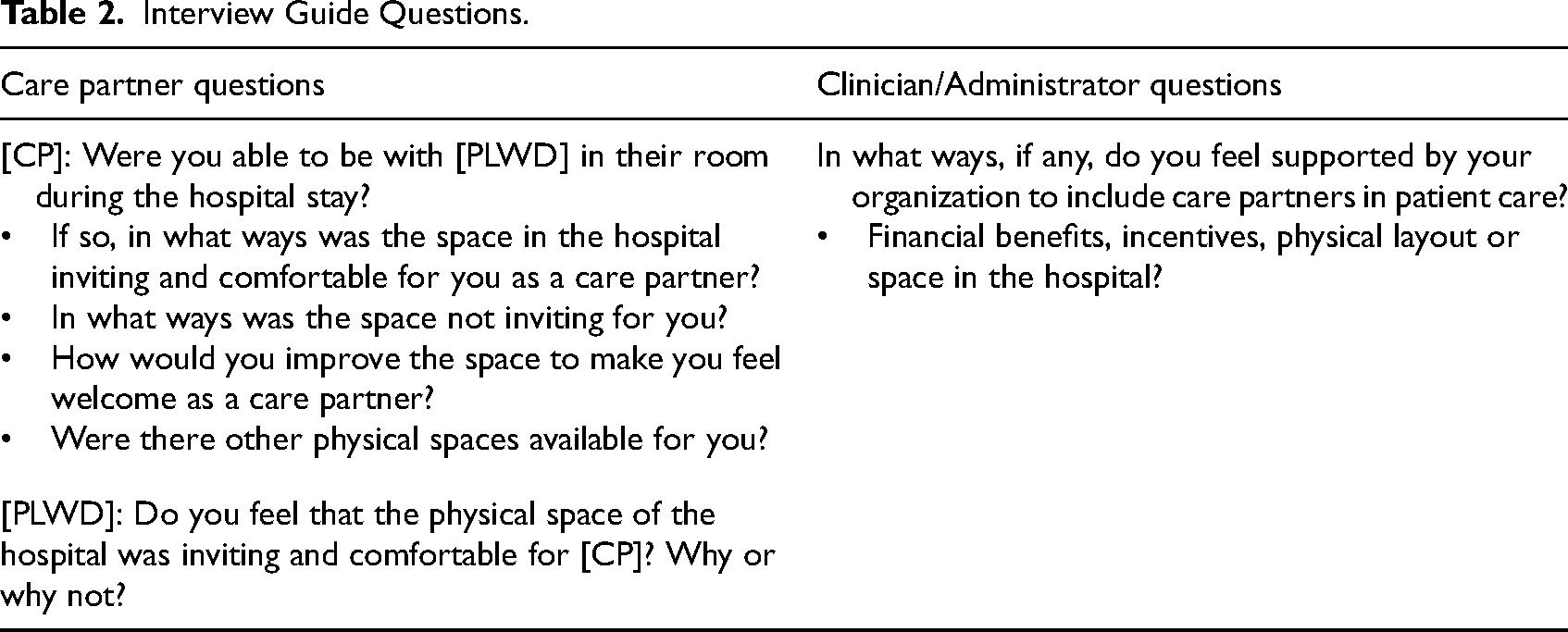
Our team collected data through semistructured interviews with 15 care partners and 27 current or prior hospital clinicians/administrators. Care partners were conveniently recruited through established caregiving listserves and through posting flyers in the community. For a care partner to participate, they had to (a) provide unpaid care to a relative or friend with an ADRD diagnosis who had experienced a hospitalization, (b) be at least 18 years of age, and (c) speak and understand English. The PLWD were invited to participate in these interviews, but their participation was not required. Clinicians and administrators were recruited through purposive and snowball sampling. We leveraged our team's multidisciplinary backgrounds to recruit individuals of various disciplines from a range of health systems across the United States. For a clinician or administrator to participate, they had to (a) have at least 5 years of professional experience in their respective position in a hospital setting and (b) speak and understand English. Both care partners and clinicians/administrators were compensated $50 in the form of an electronic gift card for their participation. Given that these interviews were part of the larger A-SHIFT study, the interview guide included questions that covered a range of factors contributing to care partner inclusion in hospital care. See Table 2 for interview questions that elicited participant's reflections on the physical environment within the hospital. Interviews were conducted over videoconferencing software, lasted up to 60 min, and were audio-recorded and transcribed verbatim for analysis.
Interview Guide Questions.
Data Analysis
Observation Data Analysis
We conducted a deductive framework analysis on qualitative field notes from our direct observations to explore factors of the physical environment that influenced care partner inclusion (Gale et al., 2013). This methodology was selected due to its appropriateness for qualitative health research done by multidisciplinary research teams (Gale et al., 2013). The deductive framework approach for qualitative analysis involves using a preexisting coding scheme based on previous literature to characterize a qualitative dataset (Gale et al., 2013). In line with our observations, three team members (CS, AY, and KI) used the SEIPS-2.0 framework definition of “internal environment” to conduct initial structural coding of any excerpt about the physical environment. Underneath the parent code “internal environment,” our team designated the coded content as either an existing strength or an area of opportunity for inclusion based on team discussions. All coding was completed in NVivo 14 software (QSR International, 2018).
Interview Data Analysis
To continue identifying factors influencing care partner inclusion, we conducted a deductive/inductive content analysis of the interview data. First, two research team members (CS and SH) individually coded transcripts using structural coding for excerpts related to the internal environment, meeting weekly with each other to resolve any discrepancies in coding. After completing this, each team member was given the structurally coded excerpts from a set of interview transcripts to code. We split up our team so that at least two members coded all transcripts. Each team member identified initial categories of physical environment factors that influenced the identification, assessment, and education of ADRD care partners. We then conducted a team-based affinity diagramming process to discuss, combine, and refine our codes using Mural software (Mural, 2011). During a virtual meeting with the entire research team, each team member created sticky notes for each factor identified in the initial coding, which could all be visualized on the screen. We then used team-based consensus discussion to group similar categories and generate and refine labels for the final categories for care partner and clinician/administrator data.
Our team used several strategies to increase the rigor of this qualitative study. Through regular team meetings, we reviewed the data and discussed how our backgrounds, beliefs, and experiences could have influenced the results. For example, one team member is a nurse practitioner who provided insight into traditional hospital room layouts’ purpose, functionality, and limitations. Two team members with backgrounds in occupational therapy helped illuminate how the physical environment can facilitate and hinder desired processes for care partners and clinicians/administrators. Another team member is a human factors engineer whose focus on systems thinking has helped our team recognize the physical environment as one factor contributing to the care partner inclusion practices. Our analysis also benefited from an interdisciplinary team-based approach to integrate these perspectives. We also continued to collect data from participants until data saturation was reached.
Our analysis also benefited from an interdisciplinary team-based approach to integrate these perspectives
Results
Observational Data
We observed a total of 27 h across four units (trauma/medical-surgical, orthopedic, family practice, neuroscience/stroke) and five patient rooms. Across these 27 h, three care partners were present. In addition to care partner interactions, our results reflect field notes focused on the physical environment beyond spaces in which care partners were present. Analysis of observational field notes yielded two themes: spaces dedicated to care partners and environmental resource utilization. Observations related to these two themes provide insight into how the hospital environment can potentially influence care partner inclusion practices in real time. Demographic data on PLWD, care partners, or clinicians were not collected, as our focus was the physical environment.
Spaces Dedicated to Care Partners
A learning center focused on providing health education to patients and care partners was present on one unit. A board of health-related pamphlets, including mindful aging, stress reduction, diabetes education, meditation classes, and parent–child classes, was outside the learning center for public use (Observation: 9/9/2022). A family waiting room with couches, chairs, a telephone, and a television was available (Observation: 10/21/2022). We generally saw care partners standing at the bedside or sitting on cushioned chairs in patient rooms. Care partners typically had the space to remain in patient rooms when 1–2 care team members entered, but we witnessed a care partner have to leave the room during a patient transfer to a transport bed given a tight space (Observation: 9/9/2022). We also noted efforts from the staff to make the physical environment more comfortable by playing music and dimming the unit lights (Coding Meeting 1/25/2023).
Environmental Resource Utilization
Care partner-focused spaces in this hospital included a family waiting room and a learning center. However, these spaces went largely unutilized. On one occasion, the family waiting center was marked closed, and the space was used for a meeting among hospital staff (Observation: 9/8/2022). Across observations, one individual used the family waiting room (Observation: 9/9/2022). We did not witness any care partners utilizing the learning center. Beyond spaces dedicated to care partners, we also saw an underutilization of the environment to communicate information for PLWD and their care partners. For example, we noted that all patient rooms had whiteboards, allowing care team members to communicate updates to care partners and share care partner information with the rest of the care team. However, we did not see updates or care partner information shared on any of these boards. Further, bulletin boards and shelves that could serve as areas to keep resources for PLWD and their care partners were empty (Observation: 10/21/2022).
Interview Data
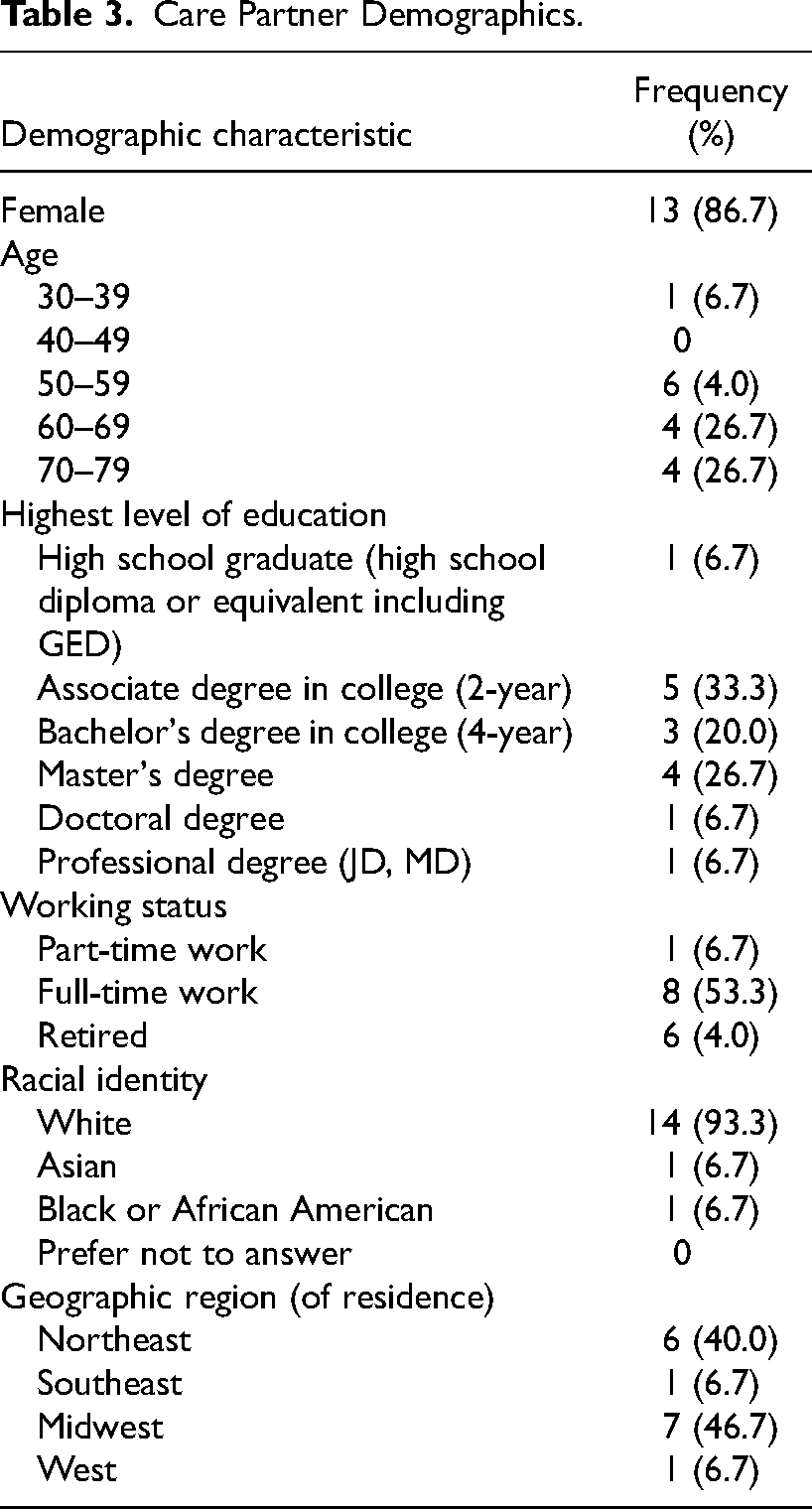
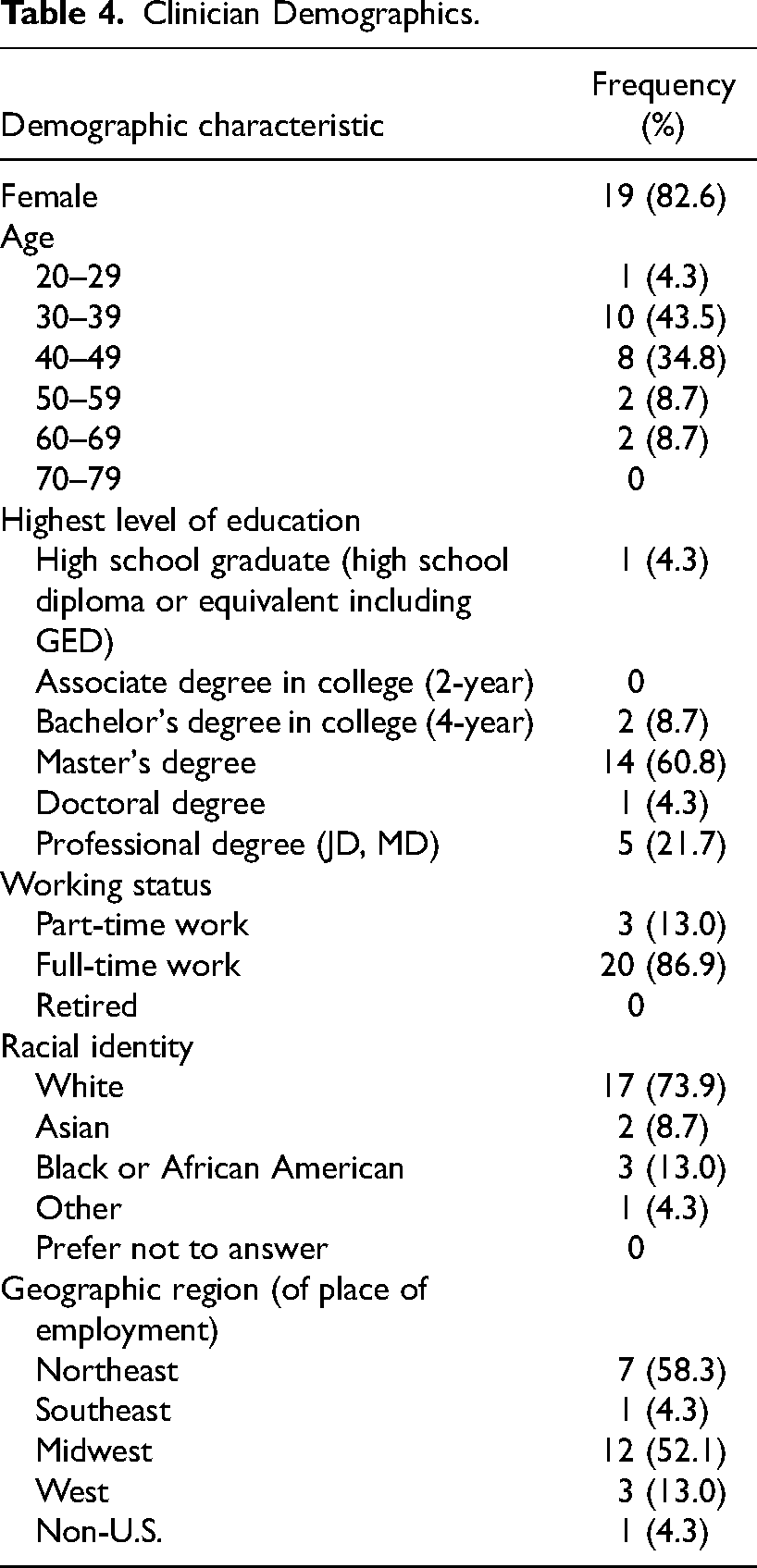
The thematic analysis of interview data resulted in six themes across both participant groups: space for care partner, space for dyad, layout of the space, comfort level of the space, personalization of the space, and parking. Below, our findings are described in detail with exemplar quotes in italics with the interview identification number. Demographic tables for care partners and clinicians can be found in Tables 3 and 4.
Care Partner Demographics.
Clinician Demographics.
Space for Care Partner
Space for care partners refers to areas available for care partners to comfortably remain while visiting their loved ones. This theme encompasses both space within patient rooms and areas in the larger hospital that support care partners’ presence in the hospital. Many care partners commented on the presence or lack of rooms large enough to seat them comfortably. One care partner noted the difference in room size between units: “They had a pullout, in the first room she was in there, the first night, there was no pullout bed or anything. It was just a tiny, little room on the cardiac floor. But then they put her in critical care, and there was a large pullout area where you could sleep if you wanted to sleep and a desk if you needed it. It was a big room” (CP6).
“They had a pullout, in the first room she was in there, the first night, there was no pullout bed or anything. It was just a tiny, little room on the cardiac floor. But then they put her in critical care, and there was a large pullout area where you could sleep if you wanted to sleep and a desk if you needed it. It was a big room” (CP6)
Others expressed an appreciation for newly renovated patient rooms designed with family in mind. One care partner stated, “[The physical environment] was very good, actually. Her particular hospital, just a few years before, built a brand-new hospital, so it was all single rooms. She was, happened to be in a pretty large room with a lot of space to move around. I mean, it was clean and well equipped and lots of seating for visitors in the room, large windows with a good view.” (CP9). Another care partner noted that a lack of space was a barrier in attending their loved one's therapy session: “…where he was, was pretty right quarters, and we just kind of stood in the little, I wouldn’t even call it a hallway, but just a little area between the different, like the nurses’ station and that. And we were definitely in the way” (CP14).
“[The physical environment] was very good, actually. Her particular hospital, just a few years before, built a brand-new hospital, so it was all single rooms. She was, happened to be in a pretty large room with a lot of space to move around. I mean, it was clean and well equipped and lots of seating for visitors in the room, large windows with a good view.” (CP9)
“…where he was, was pretty right quarters, and we just kind of stood in the little, I wouldn’t even call it a hallway, but just a little area between the different, like the nurses’ station and that. And we were definitely in the way” (CP14)
The concept of available space came up frequently when care partners discussed private and shared rooms. Some care partners noted that the PLWD's private room made their experience in the hospital more comfortable, as they had more space to stay in the room (CP4, CP5, CP6, CP9, CP10). One care partner expressed their appreciation for having a private room, adding, “Because, you know, they don’t have a filter, and if there's another patient in the room with them, you know, they could say things. They could say things that aren’t very nice or things, you know, either to them, about them or even not about them, having nothing to do with them, because you just don’t know” (CP4).
“Because, you know, they don’t have a filter, and if there's another patient in the room with them, you know, they could say things. They could say things that aren’t very nice or things, you know, either to them, about them or even not about them, having nothing to do with them, because you just don’t know” (CP4)
Several clinicians echoed the care partners’ preference for a private room. One clinician added, “Our hospital has double occupancy rooms. And so . . . logistics of doing caregiver training, like . . . in that space or caregiving involvement, knowing you’re trying to work with, I’m sorry, I have an email, a patient, and then the roommate is maybe throwing a fit. I mean, the family member might be distracted. The patient is certainly distracted. I’m distracted. So sometimes logistics can be challenging” (C1).
“Our hospital has double occupancy rooms. And so . . . logistics of doing caregiver training, like . . . in that space or caregiving involvement, knowing you’re trying to work with, I’m sorry, I have an email, a patient, and then the roommate is maybe throwing a fit. I mean, the family member might be distracted. The patient is certainly distracted. I’m distracted. So sometimes logistics can be challenging” (C1)
Multiple clinicians in our study (C23, C24) noted that the available space for care partners dramatically diminishes once numerous care team members enter the patient's room. One clinician shared, “I could say in our hospital, some of the rooms are very small, and it's hard to get even, like there's room for one other chair maybe, but it's very tight in there. And so as soon as, you know, you get a couple providers or team members in there, it can, I think, get uncomfortable for the caregiver to be in there” (C23). Some clinicians also discussed spaces outside the hospital rooms dedicated to care partners, such as waiting rooms, family cafeterias, and conference rooms. These clinicians noted that these additional spaces helped enable private conversations with care partners or provided additional space for care partners (C10, C12, C16). One clinician highlighted that a lack of appropriate space could diminish the care partner's presence, stating, “I think that there needs to be physical space for a caregiver. It matters. They don’t want to stay when there's nowhere to sit or go to the bathroom or if they’re very hungry, like an accessible place to eat” (C1).
“I could say in our hospital, some of the rooms are very small, and it's hard to get even, like there's room for one other chair maybe, but it's very tight in there. And so as soon as, you know, you get a couple providers or team members in there, it can, I think, get uncomfortable for the caregiver to be in there” (C23)
“I think that there needs to be physical space for a caregiver. It matters. They don’t want to stay when there's nowhere to sit or go to the bathroom or if they’re very hungry, like an accessible place to eat” (C1)
Layout of the Room
This theme captures reflections on room design and the organization of furniture and equipment. Some care partners and clinicians noted that the layout of the hospital rooms can influence the extent of care partner involvement. One care partner shared that their father's phone was not within his reach, impacting their ability to communicate with him when not physically present. They added, “…And I had been trying to get him touch with him. The phone was not nearby, and so that's why he wasn’t able to answer the phone.” (CP13).
“…And I had been trying to get him touch with him. The phone was not nearby, and so that's why he wasn’t able to answer the phone.” (CP13)
The clinicians’ comments were more focused on how furniture arrangement can impact care partner inclusion. One clinician noted that their hospital's room layout creates a division between the staff and care partners. They shared, “So it tends to be very much like a separation, you know, in terms of, like this is my part of the room. This is your part of the room. And in my part of the room, there's the computer. There's the bathroom. You know, there's the door” (C19). Another clinician (C24) explained that while care partners often have recliners to sit in, they frequently need to move to allow the care team members to tend to the patient. This clinician suggests that some newly renovated rooms in their hospital include a “care partner nook” that gives the care partners a designated space to stay near the patient comfortably. Once a clinician even compared their hospital rooms to a “Jenga game,” adding, “You have to like take one chair out and like to make room for somebody to sit, and like there's never enough chairs. Like in some of the rooms, there's a big column in the middle” (C18).
“So it tends to be very much like a separation, you know, in terms of, like this is my part of the room. This is your part of the room. And in my part of the room, there's the computer. There's the bathroom. You know, there's the door” (C19)
“You have to like take one chair out and like to make room for somebody to sit, and like there's never enough chairs. Like in some of the rooms, there's a big column in the middle” (C18)
Comfort Level of the Space
This theme reflects perspectives on the comfortability of patient rooms, particularly regarding furniture for sleeping and environmental conditions. Many participants noted that their only option for sleeping in the hospital room was a reclining chair (CP4, CP8, CP10, CP13). While some care partners had no complaints about their sleeping arrangements, one care partner (CP3) noted that the size of the furniture was insufficient. Other care partners (CP6, CP8) shared that they had access to pull-out beds for more comfortable sleep. One care partner added, “And then they had sheets and bedding that fit it. I mean it wasn’t like they just threw, it all fit. It was just like a nice bed” (CP8). Knowing that the COVID-19 pandemic altered their experience, one care partner described their ideal setup: “If it was an optimum room, they would have a bed, whether it be a rollaway bed or something for you to have a comfortable night's sleep, not that you do in a hospital. But at least, have someplace where you can rest” (CP15).
And then they had sheets and bedding that fit it. I mean it wasn’t like they just threw, it all fit. It was just like a nice bed” (CP8)
“If it was an optimum room, they would have a bed, whether it be a rollaway bed or something for you to have a comfortable night's sleep, not that you do in a hospital. But at least, have someplace where you can rest” (CP15)
While one clinician shared that their hospital offered cots to care partners who opted to stay overnight (C8), several clinicians shared that they were only able to provide recliners for sleeping (C12, C16, C18, C22-24). One clinician drew attention to the discomfort of sleeping in a recliner, stating, “And I don’t, I would say in a lot of the rooms, there's nowhere for them to spend the night, maybe like a chair that you could lay back a little bit. But who wants to sleep, yeah, right? Who wants to sleep in that?” (C18). Another clinician noted that the older rooms in the hospital were too tight for comfortable sleeping arrangements, but the newly renovated units had sufficient room for a sofa bed (C24).
“And I don’t, I would say in a lot of the rooms, there's nowhere for them to spend the night, maybe like a chair that you could lay back a little bit. But who wants to sleep, yeah, right? Who wants to sleep in that?” (C18)
Some care partners also drew attention to environmental conditions (i.e., light and noise) that made their experience in the hospital less pleasant (CP3, CP4, CP13). One care partner shared, “Like kind of confusion, again, like another new room, very bright, and her, the person across the hall was experiencing some sort of distress, so there was a lot of screaming happening across the hall. I remember a surgeon or a nurse or somebody was facetiming their kid, essentially like speakerphone, you know, in the hallway. So my mom thought, this was like not her surgeon, but my mom thought he was talking to her. You know, so, again, I guess, also, so like environmental stressors around” (CP3). A different care partner shared her gratitude for the placement of technology in the room, as it was positioned to reduce the amount of light in the room at night (CP6). Concepts related to light and noise were less discussed among clinicians.
“Like kind of confusion, again, like another new room, very bright, and her, the person across the hall was experiencing some sort of distress, so there was a lot of screaming happening across the hall. I remember a surgeon or a nurse or somebody was facetiming their kid, essentially like speakerphone, you know, in the hallway. So my mom thought, this was like not her surgeon, but my mom thought he was talking to her. You know, so, again, I guess, also, so like environmental stressors around” (CP3)
Personalization
This theme refers to care partners’ ability—or lack thereof—to tailor their loved ones’ hospital rooms to their preferences. Some care partners wanted to modify the environment to reduce unpleasant environmental stimuli for the PLWD. One participant shared, “…I remember all that stuff was happening in the hallway, and I remember like closing the door, and then the nurse like told me that they couldn’t have it closed, because they need to hear if like, you know, her vitals things were like hooked up to her finger and all that. So I think they needed to know if like, you know, whatever signal was coming. But I was like, oh, my God, like if the thing goes off, I will let you know. But for now, like there's so many environmental triggers happening, like I can’t even count, you know, in the hallway. And no one here seems to be mindful of that, so like let me just keep this closed, and I like vow to let you know, if something is beeping” (CP3). One clinician noted that encouraging care partners to modify the environment by bringing in the PLWD's personal items can help manage the PLWD's behaviors (C3).
“…I remember all that stuff was happening in the hallway, and I remember like closing the door, and then the nurse like told me that they couldn’t have it closed, because they need to hear if like, you know, her vitals things were like hooked up to her finger and all that. So I think they needed to know if like, you know, whatever signal was coming. But I was like, oh, my God, like if the thing goes off, I will let you know. But for now, like there's so many environmental triggers happening, like I can’t even count, you know, in the hallway. And no one here seems to be mindful of that, so like let me just keep this closed, and I like vow to let you know, if something is beeping” (CP3)
Parking
This theme captures perspectives on the ease and accessibility of parking at the hospital campus. Both participant groups mentioned parking as a relevant factor to care partner presence in the hospital. When asked about their mother's hospital admission process, one care partner shared, “We couldn’t find any parking that morning, and so it was like freezing cold, and my mom's like why are we outside? It's not even light outside yet. Like what's going on? You know, so I’m trying to like park, find where we’re going. You know, like it was just little things where it's like, okay, maybe there should be not just like disabled spots but like maybe there should be dementia-friendly parking” (CP3). One clinician expressed that the challenge of obtaining parking vouchers was a primary barrier to care partners’ involvement (C27).
“We couldn’t find any parking that morning, and so it was like freezing cold, and my mom's like why are we outside? It's not even light outside yet. Like what's going on? You know, so I’m trying to like park, find where we’re going. You know, like it was just little things where it's like, okay, maybe there should be not just like disabled spots but like maybe there should be dementia-friendly parking” (CP3)
Data Source Comparison
Both data sources provided information on how available space for the care partner and the comfort level of the space can influence care partner inclusion. Our observations revealed real-time utilization patterns of resources in the physical environment, such as communication boards, bulletin boards, and dedicated family spaces. Interviews helped further understand the link between the physical environment and care partner inclusion practices. Accounts from care partners and clinicians were more focused on the care delivery process and the hospitalization experience. These perspectives illuminated tangible solutions that can be implemented to reduce challenges associated with care partner inclusion.
Discussion
Our study investigated the physical environment within the hospital setting related to care partner inclusion practices. Observational data revealed the type of space available for care partners in the hospital. These data also revealed utilization patterns of environmental supports related to care partner inclusion. Interview data from care partners provide valuable insights into their perceptions of and preferences for the hospital environment, illuminating strategies to make it as welcoming, comfortable, and supportive as possible. Care partners and clinicians/administrators shared that available space, room layouts, comfortability, ability to personalize space, and parking can all impact the experience of care partners of hospitalized PLWD. Our study adds to the existing literature by highlighting clinician perspectives on the relationship between the physical environment and care partner inclusion. Data from clinician interviews highlight that the physical environment within the hospital can directly impact their ability to support care partners of hospitalized PLWD.
The most glaring finding from both data sources was the importance of creating available space for care partners to be present, active members of the care team. Care partners and clinicians/administrators appreciated hospital rooms that allowed care partners to remain comfortably in the room when care teams entered. Some health systems have recognized these preferences and have created space for care partners in the hospital setting. For example, Emory University Hospital previously renovated its neurocritical care units to be more patient- and family-centered, adding family areas to each patient room (Samuels, 2009). The Veterans Health Administration offers accommodations to some care partners through their Fisher Houses, providing a place to stay for care partners and patients receiving care at their hospitals (U.S. Department of Veterans Affairs, 2014). While these renovations and resources may be inaccessible for some hospitals, our findings show that innovative solutions, such as creating “care partner nooks” or adjusting the furniture layout, can allow care partners to remain comfortably in the room. In making space for care partners to stay comfortably in the hospital, health systems can work toward Goal 2 of the National Strategy to Support Family Caregivers, which is focused on integrating care partners into care teams (Administration of Community Living, n.d.). As one of our clinicians highlighted, care partners may not want to stay in the hospital to collaborate with the care team without designated spaces.
Our team was interested to hear how care partners described their preference for modifying the PLWD's environment within the hospital. Multiple care partners described their efforts in advocating for a more soothing atmosphere, and they often expressed that loud and bright environments were particularly distressing for their family members or friends living with dementia. Patient and care partner preferences for a soothing, quiet, and homelike environment align with previous literature on this topic (Digby & Bloomer, 2014; Miller et al., 2022). Further, clinician input about the benefits of room personalization is congruent with research demonstrating care partners’ distaste for a bleak, impersonal environment (Beardon et al., 2018). Care partners can increase personalization by bringing in the PLWD's comfort items, such as blankets or pictures of loved ones. By awarding care partners the freedom to make reasonable adjustments to the PLWD's hospital room, health systems may be able to improve the experiences of care partners throughout their family members or friends’ hospitalization.
Our observations revealed an underutilization of environmental communication tools, specifically whiteboards. Whiteboards are known to be useful communication tools, allowing care team members to share key information regarding patient status and plan of care among the care team (Goyal et al., 2020). In pediatric populations, using plain whiteboards with plain language has been a helpful tool in communicating key information to care partners (Nowacki et al., 2018). Given that whiteboards tend to be prevalent across hospital settings, this is an opportunity for health systems to use the environment to enhance communication with care partners. In addition to sharing care-related updates with care partners, care team members can use the whiteboard to share information regarding the PLWD's family members or friends who may be visiting or providing care upon discharge. Our team noted these whiteboards’ presence but minimal use, pointing to a low-cost environmental modification to increase communication with care partners.
Strengths and Limitations
One strength of our work was the use of multiple data sources to examine how the physical hospital environment can influence care partner inclusion practices. Through observations and semistructured interviews, we were able to witness the physical environment ourselves and hear firsthand accounts of how the physical environment can impact care partners. We purposely staggered our observations in shifts aligned with visiting hours to maximize the chance of observing care partner interactions. Our recruitment strategies allowed us to interview clinicians/administrators and care partners from all over the country, making our interview findings generalizable beyond the hospital we observed. Further, we interviewed clinicians with a range of clinical positions, including some with administrative and leadership responsibilities, which widened the scope of perspectives within our study.
One limitation of our study is the minimal care partner presence witnessed throughout our observations. Due to the unpredictable nature of patient care and the timing of hospital admissions, we were not able to observe an admission process. We compensated for the lack of an observed admission by asking the participating care partners and clinicians questions about hospital admissions that they have experienced. Given this limitation, it is possible that we missed an increased level of care partner presence during the admission process. The same could be said for the discharge process, as some of the patients we observed remained in the hospital after our observations concluded. Further, our observations did not capture the hospital policies that impact the physical environment, such as specific infection control policies that may have affected space utilization. Another limitation of this study is the lack of diversity in our interview sample, as the majority of participants we interviewed identified as White and female.
Conclusion
The physical environment can potentially impact the hospitalization experience for both PLWD and their care partners. Our observation findings reveal aspects of the physical environment that have the potential to foster or hinder care partner inclusion, including environmental communication tools and spaces dedicated to care partners. Interview findings highlighted strategies health systems can use to ensure their units are patient and family-centered. These include ensuring space for the care partner, allowing for environmental personalization, considering care partners in the layout of patient rooms, providing comfortable sleeping arrangements, and allotting dementia-friendly parking spaces. In making these adjustments, health systems have the opportunity to align with research and policy efforts pushing for stronger care partner inclusion.
Implications for Practice
The physical environment within hospitals has the potential to influence care partner inclusion practices, particularly care partners of PLWD.
Clinicians and care partners alike report that available space, personalization of patient rooms, patient room layouts, comfortability, and parking all contribute to care partner inclusion.
In pursuit of systematic care partner inclusion, health systems should maximize environmental resources (i.e., shelves, white boards, and bulletin boards), ensure available space for care partners, allow for customization of patient rooms, and allocate dementia-friendly parking spaces.
Health systems should design hospital units—both common spaces and patient rooms—with care partners in mind to ensure their presence is prioritized.
Clinicians and care partners can use these findings, in conjunction with policy initiatives related to care partner inclusion in hospital care, to advocate for environmental changes in their local hospital system.
Footnotes
Acknowledgments
The authors would like to the thank Katie Istvanek, Andrea Yahr, and Teresa Thuemling for their efforts in data collection and analysis. This project was funded by the National Institute on Aging (1R21AG077439-01).
Declaration of Conflicting Interests
AS receives royalties from Wolters Kluwer, Taylor Francis Publishers, and Thieme Publishers.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging, (grant number 1R21AG077439-01).