
Abstract
Introduction
Predicting and preventing Hospital Acquired Infections (HAI) is an evolving challenge in the U.S. and worldwide. The U.S. Centers for Disease Control and Prevention reports that nearly 1.7 million hospitalized patients annually contract HAI while receiving treatment for other health issues and that more than 98,000 patients, equating to one patient in seventeen, die because of these infections (Haque et al., 2018). Hospital settings that support curative efforts can often be a significant source of infectivity risk (Suleyman et al., 2018; Tajeddin et al., 2016). This issue is due to the inherent complexity of the socio-technical systems they comprise and the fact that several aspects of their engineered components can serve as vectors in the transfer of infection-causing microbes to human occupants (Boyce, 2016; Dancer, 2014; Deshpande et al., 2017; Donskey, 2013).
In complex healthcare settings, variability in human performance, even among well-trained clinical and environmental support staff, can compromise achieving infection risk prevention objectives (McGuckin & Govednik, 2015; Rutala & Weber, 2013). This challenge is compounded by the unpredictable nature of individual behavior, particularly in high-risk socio-technical care delivery contexts such as Intensive Care Units (ICU) (Carayon, Wetterneck et al., 2014). Ample opportunity exists to use computational technologies to assist healthcare designers, facility operations experts, and clinical staff in strategically planning safe patient care in complex care settings.
Agent-based Modeling (ABM) has precedent use and shows great potential as a collaborative design tool (Anumba et al., 2002; Stieler et al., 2022; Wang et al., 2009). Collaborative systems design approaches enhance team member confidence and empowerment (Zamenopoulos et al., 2019) while increasing commitment to goal achievement processes (Latham & Locke, 2007). Healthcare design and facility teams can leverage the scenario planning capabilities of ABM to enhance the performance of design supporting operational activities, improving care environment safety and efficiency while concurrently building team cohesion and effectiveness.
This article presents a scenario simulation that illustrates how ABM outcomes may be interpreted through the Human Factors construct of the Theory of Planned Behavior to understand better how human action may reinforce or moderate HAI risk in a high-risk healthcare setting. The term socio-technical in this article on healthcare infection risk prevention through design refers to the seminal description of social, technical, and environmental components that compose a human activity system (Pasmore, 1988; Trist, 1981). This frame of reference for socio-technical systems has also been used in formative Human Factors research (Carayon, 2006). To improve clarity in the following narrative, the term “framework” will describe social or psychological constructs. The terms “model” or “structure” describe computational analysis elements or methods.
Considering Human Factors in Healthcare Resilience
Literature based discovery research suggests that Human Factors/Ergonomics (HFE) body of knowledge offers viable frameworks to aid in infection risk prevention (Drews et al., 2019). Further HFE influences human-dependent infection control measures and speaks to the necessity of having a physical environment of care designed to be resilient to the variability of human behavior (Hung et al., 2020). The proactive safety of care delivery operations significantly relies on the design of healthcare environments and how individuals and teams respond to these settings (Carayon, Xie et al., 2014; Henriksen et al., 2021). In complex environments aimed at addressing acute or chronic safety issues and prioritizing performance objectives, limited resources are allocated to promote responsive resilience processes instead of relying solely on reactive barriers and defenses (Hollnagel, 2014).
Understanding how humans respond to complex healthcare environments can benefit significantly from the theoretical foundation provided by the Theory of Planned Behavior (TPB). TPB is a frequently employed expectancy-value model for understanding the connections between human attitudes and behavior (Ajzen, 1991; Conner & Armitage, 1998). Research supports those attitudes, which are characterized by individual perceptions and beliefs, can be reliable predictors of behaviors, which are characterized by action (Armitage & Conner, 2001; Yuan et al., 2023). This psychological premise offers valuable insights into human decision-making processes and behaviors within intricate socio-technical systems (Gao & Tang, 2023) like care delivery environments. TPB places individuals’ attitudes on their capabilities encompassing self-efficacy (Bandura, 1977) and perceived situational control within a comprehensive framework encompassing the interplay between beliefs, intentions, and behavior outcomes (Ajzen, 1991). In healthcare infection control, which relies on human intention to engage in safe infection control practices (Shekelle et al., 2013), the belief in benefits of a specific behavior, which defines the individual's conviction in the positive outcomes of these practices (Gould et al., 2018), and perceptions about the availability of essential resources to enact these behaviors (Dyson et al., 2013; Sadule-Rios & Aguilera, 2017) can meaningfully influence the effectiveness of infection risk prevention efforts within care environment design objectives. Additionally, research suggests that peer influence within clinical teams significantly affects hand hygiene adherence, particularly when senior clinicians model proper behavior(Asudani, 2017; Monsalve et al., 2014; Sands & Aunger, 2020).
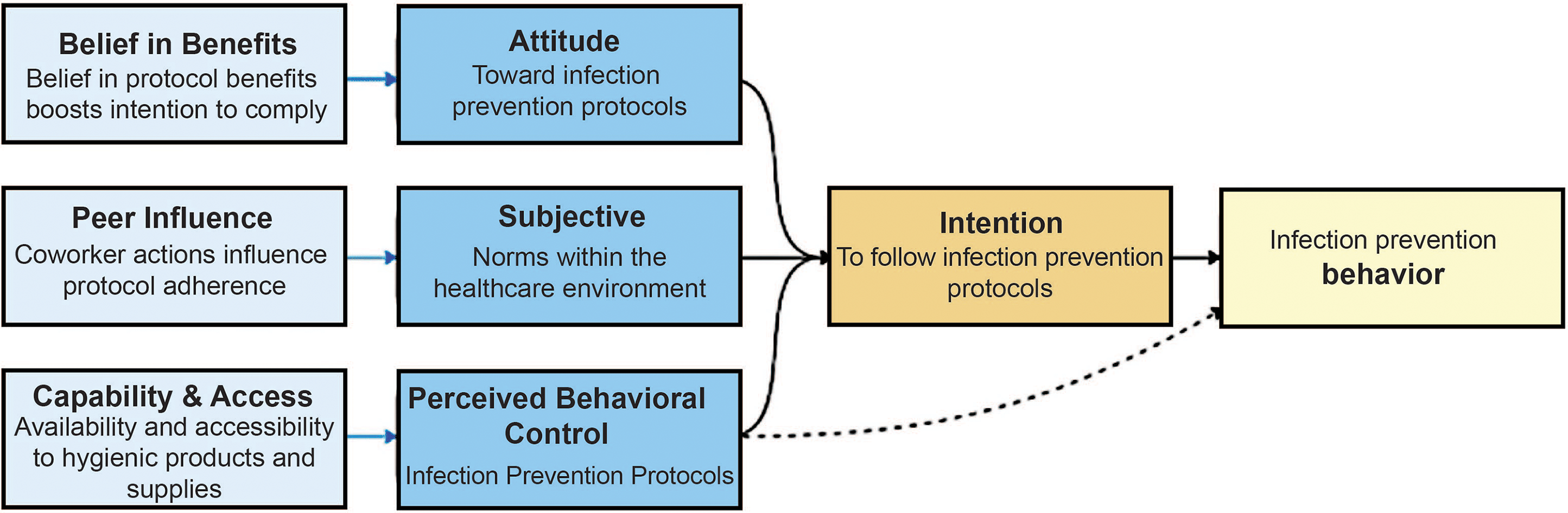
Figure 1 illustrates a framework the study team developed based on research-derived attitudinal and belief-based antecedents to clinical infection prevention behaviors. This map delineates factors influencing healthcare workers’ compliance with infection prevention protocols. This model depicts the pathways from individual attitudes and there potential influence on planned behavior, highlighting “Belief in Benefits, (Gould et al., 2018)” “Peer Influence (Asudani, 2017; Monsalve et al., 2014; Sands & Aunger, 2020), “and “Capability” (Bandura, 1977) and “Access” (Dyson et al., 2013; Sadule-Rios & Aguilera, 2017) as antecedents to “Attitude,” “Subjective Norm,” and “Perceived Behavioral Control” (Ajzen, 1991). These components collectively shape the ‘Intention’ to follow protocols, which in turn Predicts actual “Infection Risk Prevention Behavior.”
Relational diagram of behavioral coding syntax and TPB semantics.
Seminal research in TPB suggests that individuals enact implementation intentions when stimulated by environmental cues congruent with their intended goal of engaging in specific behaviors (Conner & Armitage, 1998; Gollwitzer & Brandstätter, 1997; Orbell et al., 1997). The existence or absence of environmental factors that can facilitate safe behaviors, like clinician observance of hand-hygiene moments to mitigate pathogen transmission within healthcare settings, is essential for successfully implementing intended infection risk prevention practices. For example, the salience and accessible proximity of Hand Sanitization Devices (HSD), such as hand wash sinks and hand-sanitizer dispensers, encourage higher rates of hand hygiene compliance in nursing staff, and the design of these features within the healthcare unit seems to moderate this outcome (Cai et al., 2020).
The perceived difficulty of acting, combined with tangible external factors within a given environment, contributes to an improved understanding of individuals’ or groups’ capabilities of translating intentions into actions. For instance, scenario simulation research indicates that the integrative impact of environmental factors in a healthcare setting, such as HSD's visual prominence and proximity, significantly affects nurses’ perceived control over adhering to critical moments of hand hygiene compliance (Platt et al., 2022). Perceived Behavioral Control (PBC), a component of TPB, plays a pivotal role in comprehending human behavioral outcomes within intricate socio-technical contexts. As outlined by Ajzen (1991), PBC refers to an individual's perception of the ease in performing an intended behavior. PBC is a fundamental aspect of shaping the behavior of individuals and their intention to act (Hagger et al., 2022). Further, PBC highlights the significance of actual behavioral control, emphasizing that the availability of resources and response opportunities can substantially influence the likelihood of successfully executing intended behavior (Ajzen, 1991).
The analysis of TPB, regardless of the context, should always consider the composition of the setting in which human intention and subsequent action occur (Conner & Armitage, 1998). This evidence implies that integrating TPB and integrative computational modeling of socio-technical systems within a healthcare context offers the potential for a better understanding of the environmental factors that influence individual and collective human behavior and decision-making regarding the practice of infection control safety. Prior research has set a precedent for using ABM to assess the TPB in the context of pathogen transmission (Abdulkareem et al., 2018; Palomo-Briones et al., 2022). The following scenario simulation study aligns with enhancing the infection control potential of healthcare facilities’ design and operational planning. It explores the possibility of using ABM as a digital design decision support tool, in tandem with the TPB, to foster socio-technical resilience. The next sections of this article examine how Hand Hygiene Compliance (HHC) rates influence the spread of specific pathogens and thus heighten or moderate the risk for infection in an inpatient healthcare environment.
Agent-Based Modeling in Healthcare Resilience Planning
ABM is highly effective in simulating individual human-like entities’ varied behaviors, which are called agents, within complex socio-technical systems (Khodabandelu & Park, 2021). ABM can be particularly effective in addressing the integrative effects of dynamic human actions, complex pathogen transmission trajectories, and the care environment design's responsiveness against infection risks. This claim is supported by the precedent use of ABM in assessing the migration of infection-causing pathogens in healthcare environments (Gingras et al., 2016; Marshall & Galea, 2015). ABM has also been used to evaluate the effectiveness of targeted clinical and human-driven operational interventions in care settings to reduce the transmission risk of HAI-causing pathogens (Barker et al., 2018; Codella et al., 2015).
ABM complex systems modeling consists of agents engaging in dynamic interactions with each other within a virtual environment and aims to predict the possible emergent outcomes of these exchanges (Khodabandelu & Park, 2021; Klügl & Bazzan, 2012). Regardless of the modeling platform used, all ABMs have commonalities in their structural elements, which are as follows (Khodabandelu & Park, 2021):
Agents are goal-oriented entities that are assigned defined behavioral responses to their virtual environment within the model code. Agents can act independently of one another and behave proactively during a model's temporal simulation to initiate autonomously governed actions. Agents are adaptive and have the capacity for learning and developing responsive behaviors through their interactions with each other and their environment. This characteristic can shape their behaviors and decision-making abilities.
A key emphasis of using ABM to predict outcomes of elements in complex dynamic systems is founded on understanding the evolution of heterogeneous and interacting agents. The two types of agents used in the model described in this paper are human agents (e.g., clinical staff and patients) and environmental patch agents (e.g., care environment building material). A distinct benefit that ABM offers in complex environment analysis is that it can deduce the specific behavior of discrete system parameters because the interactive structure that leads to individual and collective agent behavior is made transparent through the modeling process (Schieritz & Größler, 2003). The dynamic modeling outcomes of this digital technology demonstrate how specific interventions can influence individual agents’ characteristics, preferences, and behaviors (Liu et al., 2018). Using ABM to evaluate systems behavior in safety-critical scenarios and quantifying system outcomes related to critical interdependencies assists experts in evaluating better performance and recovery tradeoffs (Nan & Sansavini, 2017). This combined approach has also proven helpful in distilling knowledge from frontline experts to inform model development and simulate emergent interaction outcomes in socio-technical environments (Okada et al., 2018). Adjusting ABM parameters based on real-world scenarios offers the ability to forecast the impact of specific environmental antecedents by analyzing single- and multi-factor measures. It enables real-time prediction of interventions that may moderate human or environmentally induced hazards (Ye et al., 2020).
Principles of HFE, like visual cue salience and the proximity compatibility of task-related resources in work environments, have been acknowledged for providing a viable theoretical foundation for designing error-resistant healthcare processes and systems (Carayon, Wetterneck et al., 2014). For example, the HFE-derived premise of salience in the context of design safety describes the visual distinctiveness of essential objects within their surroundings (Fracker, 1988). The Proximity-Compatibility Principle (PCP) utilized in Human Factors design delineates the immediate visual closeness of safe behavior-support mechanisms and information to the user's tasks (Wickens & Carswell, 2016). Cue salience and PCP within environments contribute to the concept of “task ecology,” ensuring that resources with performance safety-related purposes are easily discoverable and interpretable in the environmental domain (Baber et al., 2019). Previous research in healthcare operations and design has illustrated environmental design factors, including visual salience and proximal accessibility of infection control resources like hand sanitization dispensers, can impact safe hand hygiene behaviors (Cai et al., 2020; Platt et al., 2022).
Research on the use of computational modeling to better understand the integrative effects of safe exchanges between humans and their environment suggests that combining principles of HFE in ABM helps forecast the probability of operational goals aligning with the expected outcomes of a system's design (Calero Valdez & Ziefle, 2018). Using ABM for proactive risk detection has also proven effective in helping professionals make improved decisions, reducing operational hazards, and identifying latent dangers in complex safety-critical circumstances (Samaad et al., 2018; Thapa et al., 2005).
Methods
The scenario presented in this article serves as an example of how to employ ABM to assess environmental antecedents conducive to promoting PBC within an ICU setting. ICU patients are especially susceptible to contracting HAI due to longer than average length of stays within the care delivery environment and health vulnerabilities (Dasgupta et al., 2015; Yue et al., 2017). Thus, the study team focused the model on an ICU environment to analyze the transmission patterns between humans and contact surfaces in this unit type. The hypothetical ICU ABM simulation comprised eight (8) typical ICU patient rooms and four (4) isolation rooms. Although this computerized ICU environment approximates typical ICU plans, the underlying complexity model was crafted through close collaboration with healthcare facility professionals and clinical infection control experts from a southeastern US-based academic health system, who were integral investigative team members (Platt et al., 2023).
The ABM was developed using NetLogo software (version 6.2.2) to assess the effectiveness of interventions in controlling the infection spread rate within an ICU. NetLogo serves as both a modeling language and an integrated environment, specifically designed to simplify the creation of ABM (Wilensky & Rand, 2015). The NetLogo visual interface was consistently utilized throughout the development phase for model calibration and verification. This action ensured that each modification adhered to the logical procedures, and expected results were observed in real time within the software's visual interface. Figure 2 illustrates the model's interface and architecture and how the level of exposed patients and contaminated patches within the environment are simulated via tunable human, pathogen type, and environmental variables.
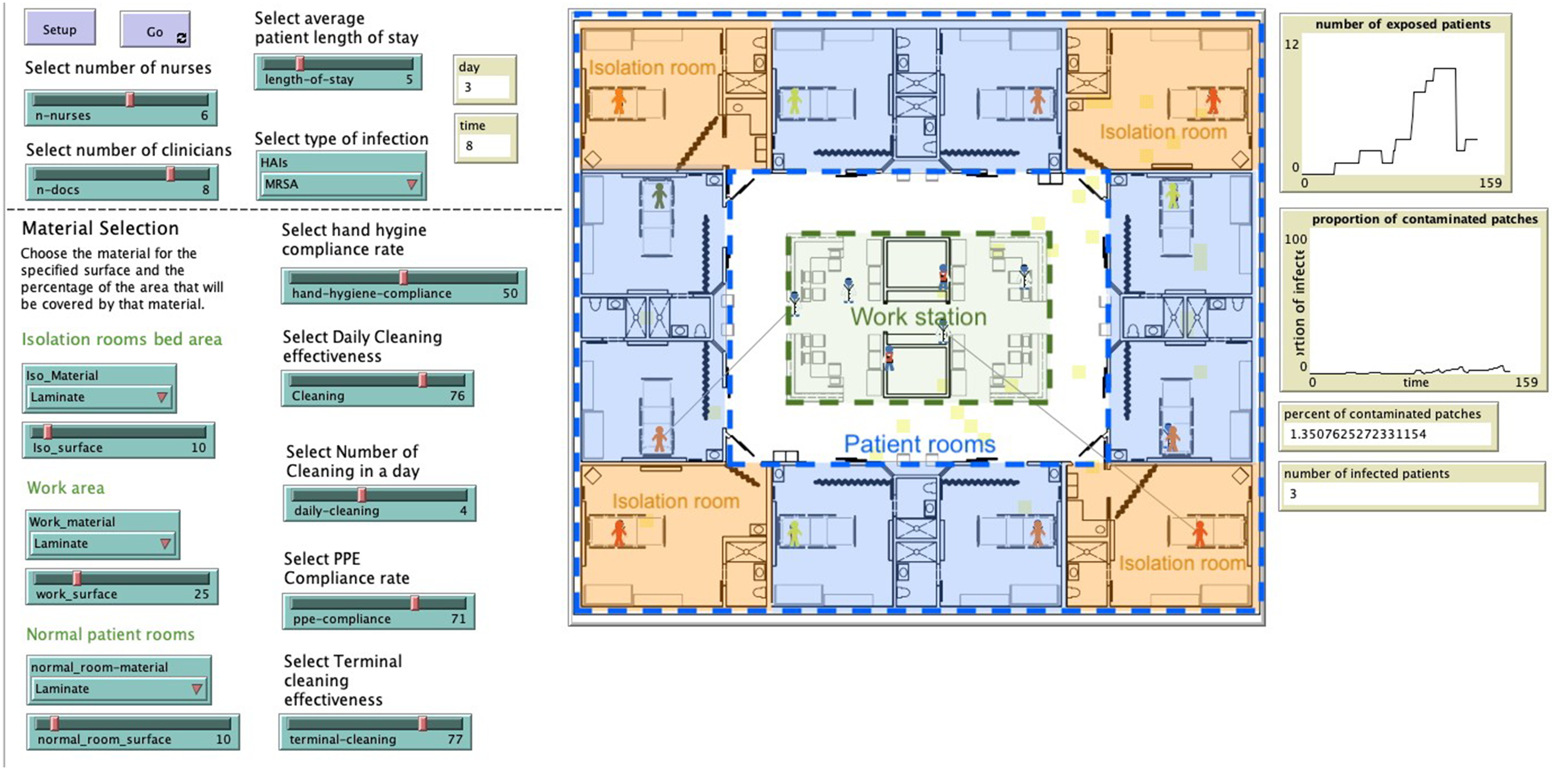
Infection prevention through the design ICU agent-based model.
The model's architecture is designed to replicate pathogen transmission dynamics by simulating interactions among various human agent types, including mobile physician and nurse caregiver agents, stationary patient agents, and environmental patches. Following typical ICU staffing ratios, the team opted for a staffing configuration of one nurse for every two patients and one doctor for every three patients. The data used to inform the model parameters and agent types was drawn from both precedent literature on ABM to evaluate pathogen spread in healthcare facilities (Abuosi et al., 2020; Barker et al., 2018; Codella et al., 2015; Dancer, 2008; Landelle et al., 2014; Lopez et al., 2014; Otter et al., 2013; Sands & Aunger, 2020; Tenorio et al., 2001) and the hospital-based subject matter expertise of the clinical, operations and infection control personnel that collaborated with the investigative team in this study. Although consideration was given to adding “visitor agents” to the model parameters as well, the study team decided to constrain human agent types to patients and clinicians due to the limited predictability of visitor actions and the incongruity of data related to observed and reported infection control behaviors in this group of individuals (Gaube et al., 2021). The decision to constrain model agent typology was founded on research on the spread of HAI, suggesting that the primary risk factor for patient infection in acute care settings stems from contact with clinical care providers (McLaws, 2015; Toney-Butler et al., 2023; Zimlichman et al., 2013). National action plans for HAI control developed by US-based federal agencies such as the Centers for Disease Control and Prevention (CDC) and the U.S. Department of Health and Human Services (HHS) prioritize stemming infection spread through specifically raising clinical staff awareness of safe infection control behaviors (Policy (OIDP), 2021; Weiner, 2016). The decision to not include visitor agents also enhanced model parsimony. Optimizing the trait of model parsimony is crucial in complex health risk computational models as this approach augments heightened accuracy in prediction and improved generalization of model findings (Sun et al., 2016). For these multiple and evidence-based reasons, the parameters of this model were set only to include human agents that represented clinical care providers and patients.
Precedent research also supports that clinical staff may underestimate the role of environment of care surfaces in spreading infection causing pathogens to vulnerable patients (McLaughlin et al., 2013). Unlike precedent infection control ABM studies (Barker et al., 2018; Codella et al., 2015), the scenario simulation model presented in this research contained more nuanced and tunable interior material type response information embedded within the code for model environmental patches. The environmental surface infectivity data was informed by ISO 22196 controlled bench tests of a plastic laminate assay that measures the antibacterial activity on plastics and other non-porous surfaces. Material coupons were inoculated (treated and untreated) with approximately 600,000 Clostridioides difficile (C. diff), Carbapenem-resistant Enterobacterales (CRE), and Methicillin-resistant Staphylococcus aureus (MRSA) bacterial cells and then tested after 24 h test for recovery of Colonizing Forming Units (CFU) proportions for each strain. Plastic laminate was selected for the scenario simulation due to its widespread use on horizontal and vertical high-touch surfaces in healthcare. Results of the ISO testing of contact surface material assay antibacterial properties were applied to the model.
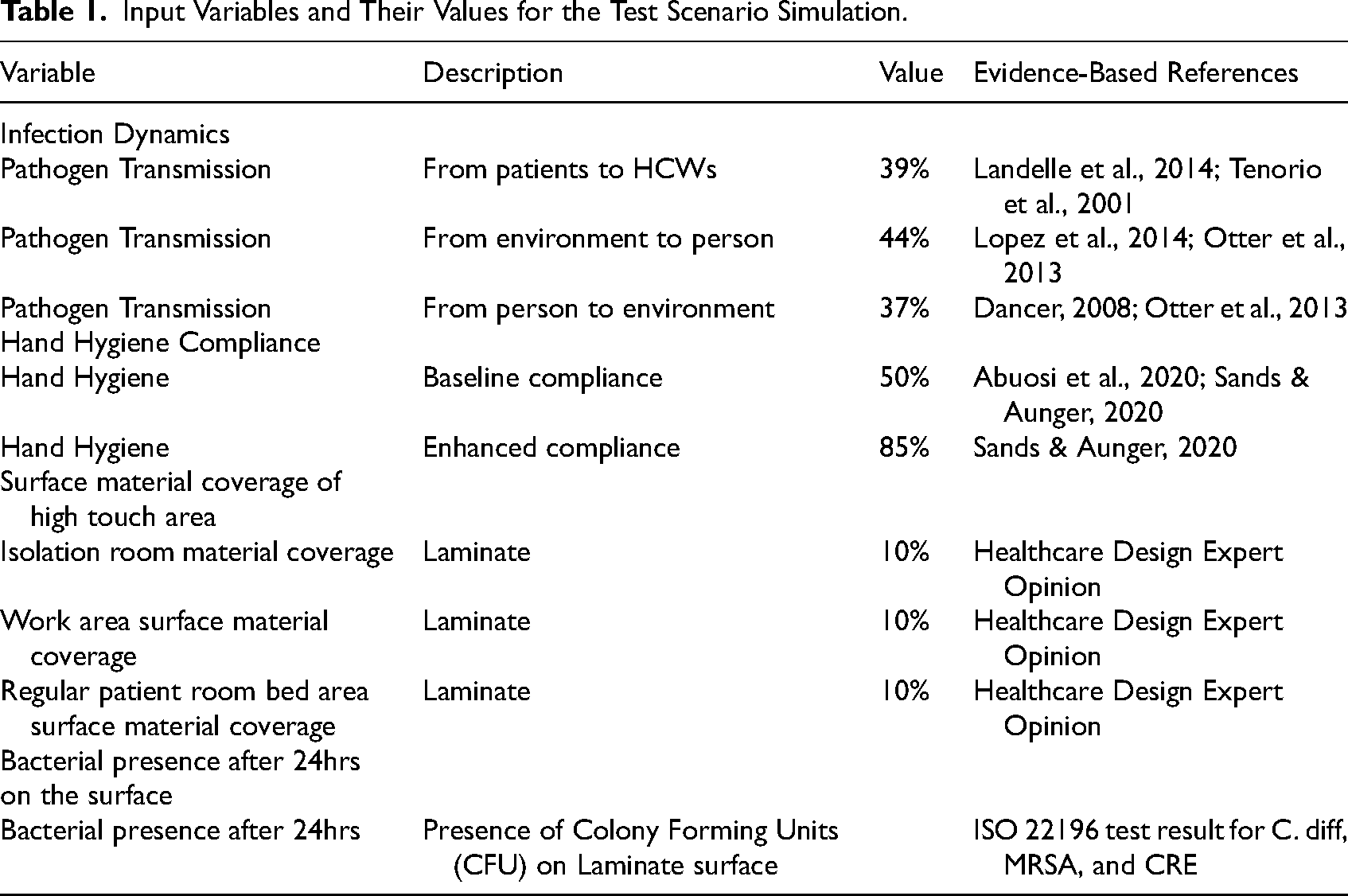
The list of input variables and values relevant to the hand hygiene aspect of the overall environmental infectivity of the model are delineated in Table 1.
Input Variables and Their Values for the Test Scenario Simulation.
Transmission simulation initialization is through the patient agents distributed across 12 rooms, each potentially in one of four infection stages: ‘clear,’ ‘exposed,’ ‘colonized,’ or ‘infected.’ Notably, only the latter two stages, ‘colonized’ and ‘infected,’ are triggers for transmitting infection to other agents. The human agents in the model are further categorized based on their infection levels and interaction frequencies. Infectivity transmission is determined by contact with carriers or contaminated areas. The transmission points encompass networked interactions, such as human-to-human transmission, and patch interactions, such as transmission between humans and the environment, and vice versa.
The model initiates with a foundational assumption, wherein 25% of the patients are initially infectious, as all ICU patients are considered susceptible owing to their vulnerable health status. The agents’ statuses are reset after each model temporal shift. Programmed rules embedded within the model's code govern agent movement, and the model operates on a 12-h shift, divided into two 6-h units. Nurses make hourly visits to patients, while doctors make two visits within each 6-h unit. These simulated interactions can potentially result in exposure and transmission of pathogens.
To demonstrate the ABM concept and its application to the impact of HHC behavior and infectivity level in the environment, two levels of hand hygiene compliance rates (Baseline-50% HHC observance and Enhanced-85% HHC observance) were chosen as the metric for model scenario testing. This process facilitated an assessment of the ABM's capability to accurately represent and predict the impact of varying levels of hand hygiene compliance on infection transmission within the ICU environment. Figure 3 illustrates the programmed model feedback loops between the agents (patients and healthcare workers), their behaviors (hand hygiene), and the environment (patient rooms, workstations) that contribute to infection control outcomes.
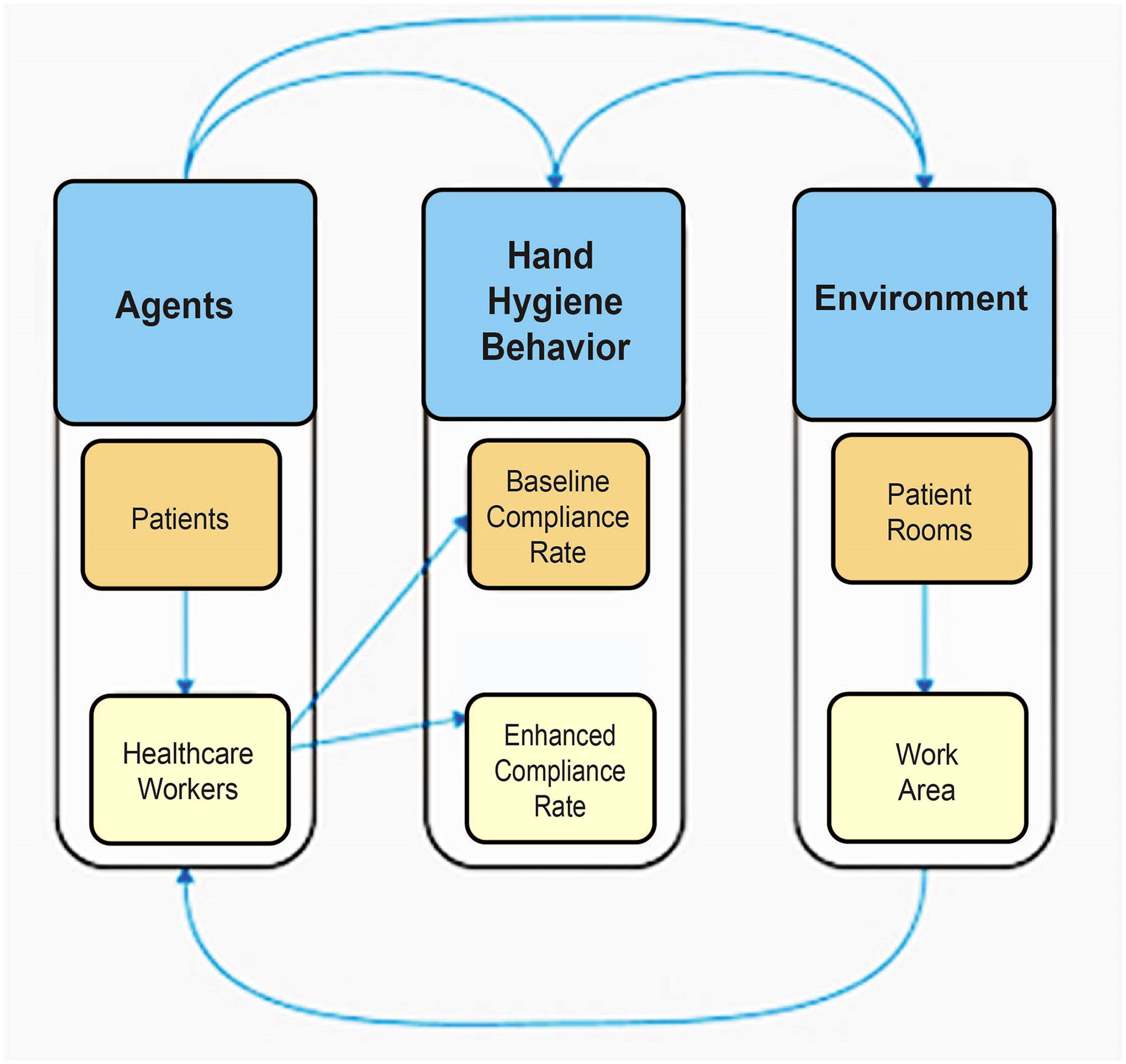
Schematic of the ABM for infection control in a healthcare setting.
Caregiver agents, i.e., nurses and physicians, interact with patients, and the environment, such as floors and walls, each of which can expose them to pathogens. These agents then exhibit behaviors that influence infection spread, such as the level of HHC. This feature of the model is an important aspect that supports the assertion of the utility of this approach used to evaluate the planned behavior within caregiver agents in a hypothetical healthcare setting. Therefore, all the other variables were kept constant except for HHC rates to determine how this caregiver agent behavior impacts patient and environmental infectivity.
Results
The simulation of this ABM was run on a 30-day temporal frame. Each HHC scenario test was repeated 20 times to ensure the reliability of model outcomes. Data collected included the level of infectivity among ICU patients and environmental contamination. The simulation results depicted in Figure 4 (patient infectivity based on HHC) and Figure 5 (environmental infectivity based on HHC) suggest that patient infection rates and environmental contamination displayed a reduction in amount or variability based on improved HHC behavioral adherence.
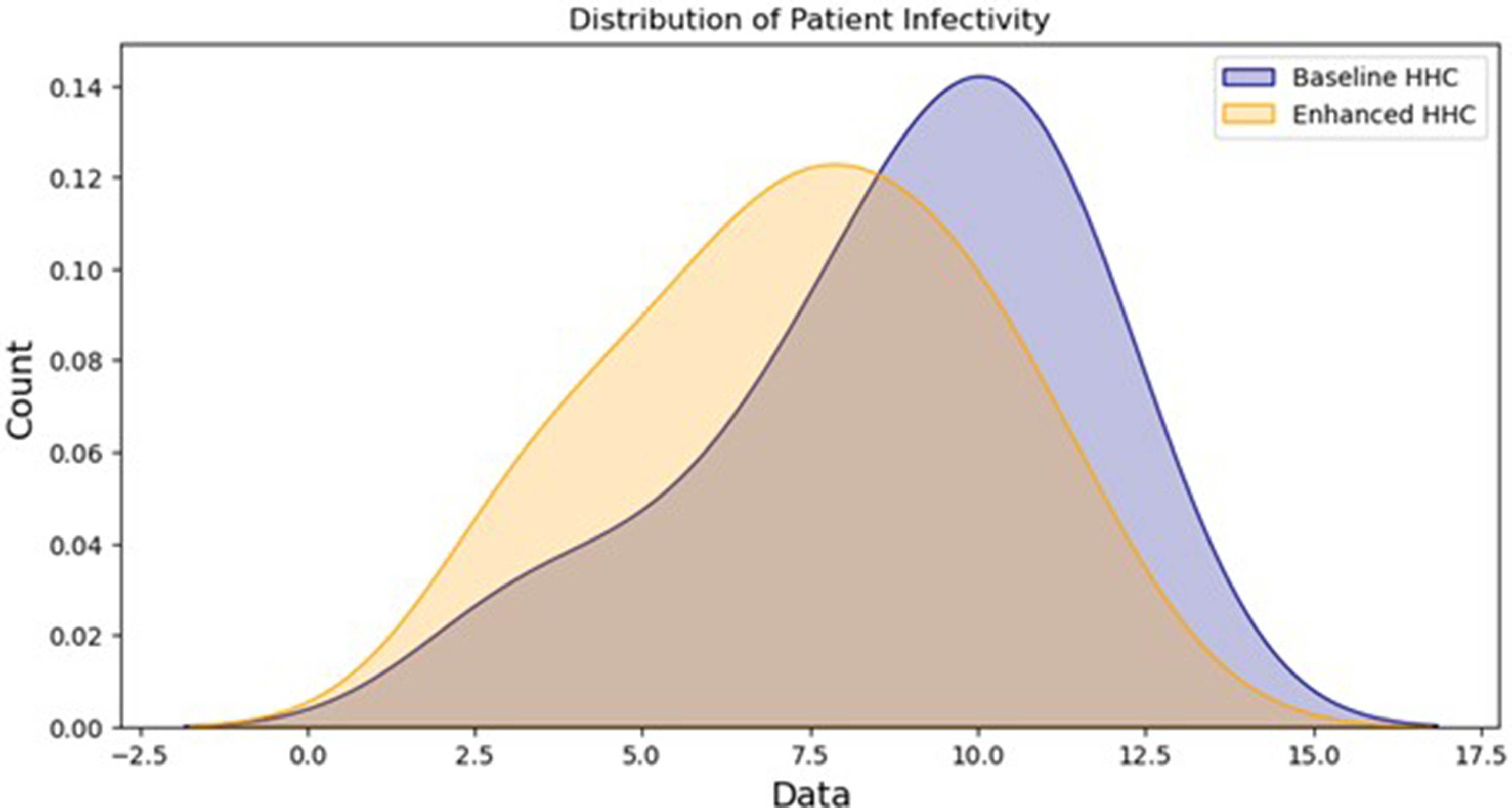
Comparison of the number of infected patients at the levels of hand hygiene.
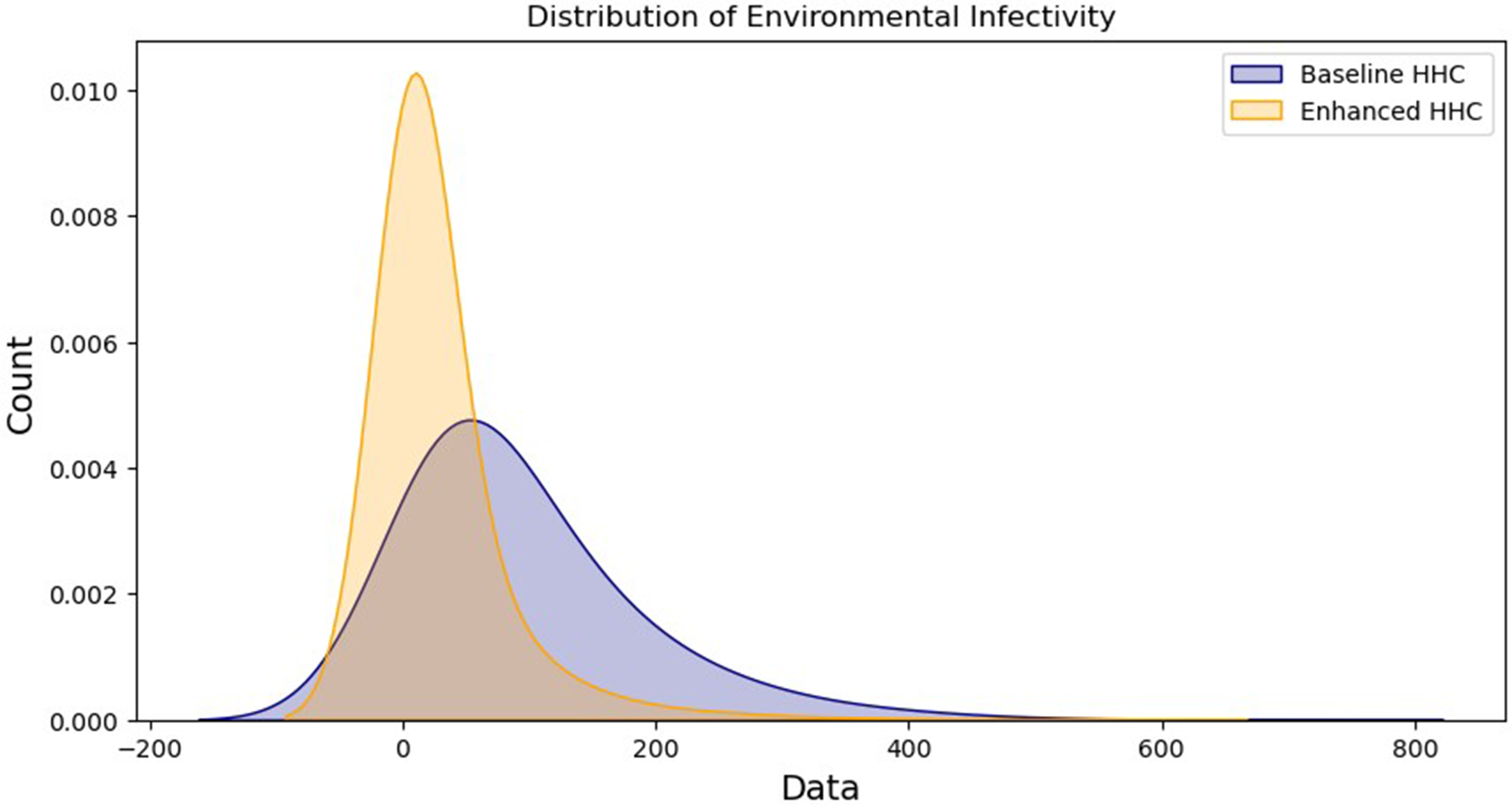
Level of environmental contamination at the two hand hygiene compliance rates.
Statistical analysis of non-parametric distributions for patients and environmental infectivity indicates significant differences attributed to variations in hand hygiene adherence behavior. A Mann-Whitney U test on simulation outcomes indicates significantly lower numbers of infected patient agents at the enhanced caregiver agent hand hygiene compliance rate (M = 7.36, n = 20) compared to the baseline (M = 8.79, n = 20) (U = 229.0, p < .01). Another Mann-Whitney test on median infectivity levels in the environment shows a significant difference between patch contamination at the enhanced hand hygiene compliance rate by caregiver agents (M = 27.28, n = 20) compared to the baseline (M = 92.16, n = 20) (U = 210.0, p < .01) with a visible difference in observation variances between both scenarios.
Interpreting Scenario Simulation Results Through a Human Factors Framework
In the context of this ABM, the scenario with enhanced HHC reflects an environment where TPB factors would be reliably positively influenced, leading to improved hand hygiene and, assumably, better infection control outcomes. This circumstance includes critical aspects such as environmental affordances supporting the rigorous observance of optimal HHC. For instance, placing hand sanitizers at every doorway might increase an agent's PBC over hand hygiene (Gould et al., 2018). Simulating scenarios in ABM, such as the one presented, also sheds light on how barriers to safe care delivery behaviors may undermine effective infection control. For example, should the design impede the salient and proximal availability of environmental resources meant to support optimal HHC, it could lead to a decline in agents’ PBC, thereby diminishing the probability of their adherence to the practice (Ahmadipour et al., 2022). By integrating TPB principles, interventions within the care environment can be designed to predict and actively shape and enhance PBC related to hand hygiene, thereby improving infection control outcomes.
These outcomes of ABM simulations afford healthcare designers and facility operations specialists more holistic and actionable insights on priorities for controlling pathogen spread through environmental and operational interventions. Employing TPB to ground truth assumptions regarding infection risk prevention by simulating scenarios within an ABM offers valuable insights into comprehending the elements of the healthcare environment that may either promote or hinder adherence to practices conducive to infection control. The result of this study suggests a broader potential for ABM simulations in healthcare design.
Extending ABM Scenario Decision Support Utility Through HFE
Research on incorporating HFE in the development of risk analysis in complex healthcare settings indicates that a more efficient pathway to solution development is achieved by focusing on creating floor plan representations that are easily understood by a diverse group of experts (Wooldridge et al., 2022). ABM enables the design and healthcare operations team to create design paradigm hierarchies that facilitated the most efficient operations in safety-critical scenarios (Delcea et al., 2020), a consideration that would be of vital importance in ICU planning. The scenario simulation suggests that decomposing the fundamental components of the TPB can effectively guide empirical investigations into the design drivers of caregiver behaviors. Additionally, this approach can expand the use of ABM to highlight the factors that influence or inhibit care provider intentions.
The scenario simulation ABM presented in this article as an example modeled hand hygiene adherence as only a probabilistic variable. However, the model code of this scenario simulation could be extended to include a variable related to PBC within the perception attributes of caregiver agents’ adherence to infection control, as demonstrated in prior research utilizing ABM to investigate the TPB within complex circumstances (Scalco et al., 2017). Extending agent traits within the model, such as levels of skepticism and social pressure, can also be achieved by incorporating Fuzzy Logic coding. Computational design coding that uses Fuzzy Logic integrates variable trait membership functions based on a degree or level of outcome (Zadeh, 1976). A Fuzzy trait refers to a conditional attribute that can have varying degrees of membership or truth values, rather than just binary true/false values (Dubois, 1980).This approach has been used in prior ABM social simulation research for modeling agent behavior that is best understood through threshold values rather than discrete numerical variables or probabilistic values (Izquierdo et al., 2015; Liu et al., 2018).
PCB could also be represented as a fuzzy trait among caregiver agents, denoting the level of belief in their ability to control their behavior through environmental resource allocation and availability. This approach to evaluating the boundaries of perception of control in healthcare settings has been used in previous healthcare research (McLaughlin et al., 2013; Zheng et al., 2017) and research investigating health-related TPB in complex socio-technical settings (Gagnon et al., 2015; Trifiletti et al., 2022). For instance, the TPB component of “attitudes,” encompassing individual beliefs concerning the outcomes of infection risk prevention behaviors like hand hygiene compliance, could be employed to program agent-type behavior. Within this context, it is essential to recognize that some caregiver agents may be coded to emulate their human counterparts in holding strong convictions regarding the effectiveness of such behaviors. In contrast, others may harbor higher levels of skepticism regarding the role of hand sanitation in stemming infection-causing pathogen spread (Gould et al., 2018). Considering the TPB aspect of “subjective norms,” a variable of social pressure may be embedded in agent behavior coding that directs their behaviors to perform or not perform safe infection control behaviors. These characteristics mimic observational research in healthcare settings, suggesting that the unit's culture can meaningfully influence the level of adoption of hand hygiene (Schwappach, 2018). Finally, research supports that Fuzzy Logic and associated decision rule algorithms can be developed that successfully predict the infection resilience levels of interior materials often used within healthcare spaces (Platt & Chen, 2023). Fuzzy Decision Rule Algorithms can then be embedded in ABM code (Bressane et al., 2024) dictating materiality response to pathogen presence.
Implications of Scenario Modeling Findings
This computational research of the dynamics of healthcare design and operations is intended as a theoretical foundation, laying the groundwork for future empirical research. A notable and unique benefit of using ABM, such as the version presented in this article, to evaluate the TPB of caregiver agents is the ability to run multiple sequential experimental scenarios through model simulations. This process enables investigators to run numerous virtual experiments that share study protocol parallels with physical experiments. This data-driven evidence-based approach ensures that interventions and changes are not based on assumptions but informed by empirical observation of these phenomena through computational models that reflect real-world circumstances. Moreover, this approach enables a crucial advancement in applying data-driven, model-based technology to practice by utilizing empirical HFE research to examine the effectiveness and safety of using models to support care delivery decisions (Denton, 2023). Precedent research conducted with healthcare design researchers and infection control experts suggests that the integration of the TPB with HFE concepts like Salience and PCP may prove valuable in creating scenarios for predicting HHC due to a measurable relationship of the centrality of these environmental design factors with concepts related to observing “Moments for Hand Hygiene (Platt et al., 2022).”
Developing infection risk prevention strategies that encompass the physical care environment and account for human behavior in transmitting or mitigating hospital-acquired infections in dynamic healthcare environments is a multifaceted endeavor. Addressing this challenge calls for adopting a system of systems methodology that acknowledges the interconnectedness and interdependence of various components. Such an approach recognizes that changes in one part of a socio-technical system can cascade through others, emphasizing the need for a holistic view when implementing design changes or interventions. This method aligns well with the capabilities of ABM, which inherently models the multifaceted interactions between agents and their environments. Leveraging the novel abilities for experimentation and forecasting ABM offers could provide the most resilient and comprehensive route to consistently achieving Infection Risk Prevention goals.
Limitations
The model developed for this study, although informed by experts in clinical care, infection control, and research of the built environment, uses a closed-system hypothetical care environment for simulation. Such a controlled environmental context could influence the significance level of the HHC behavior-based results obtained in the simulation outcomes. ABM's inherent complexities can also sometimes result in contradictory results. For example, in Figure 5, the simulation results suggest that although enhanced observance of HHC decreased the variability of environmental contamination, the overall count of infected environmental “patches” was higher for enhanced HHC. Such an anomaly may suggest that the parsimony of model variables could be constrained further or may indicate that another type of behavior-based intervention, like cleaning and disinfection consistency and thoroughness, may elicit more impactful results.
Conclusion
This article presented a healthcare environment ABM Scenario simulation as a premise for incorporating a Human Factors framework for understanding the emergent behavior of heterogeneous caregiver agents. Using ABM to inform infection prevention through design strategies would enable design and healthcare operations teams to develop prioritized design frameworks that optimize efficiency in safety-critical scenarios, which is particularly crucial for ICU planning. The utility of incorporating TPB to guide agent infection risk prevention behaviors provides valuable insights into human response due to emergent circumstances in healthcare settings. More consistent infection control goals may be achieved in dynamic settings such as healthcare ICUs by better understanding how the care environment shapes healthcare professionals’ attitudes, subjective norms, and perceived behavioral controls. More importantly, by anticipating potential behavioral lapses, TPB can inform strategies that explain endemic system risk factors and actively work to prevent them from becoming actual hazards. Used within the context of ABM, TPB offers unparalleled insights through iterative simulations that make it easier to design healthcare environments that prioritize patient and staff safety while optimizing resource utilization.
Implications for Practice
Dynamic systems modeling may offer valuable insight for promoting patient safety in healthcare planning, particularly regarding infection risk during clinician-patient interactions. Agent-Based Modeling (ABM) and the Theory of Planned Behavior (TPB) can be used to analyze how healthcare space design and care delivery scenarios influence clinician behaviors related to infection prevention. Computational scenario analysis of simulated healthcare environments enables the ability to evaluate the extent to which human behaviors may impact infection risk prevention outcomes in healthcare settings. Integrating behavioral theories and computational modeling to improve infection control practices in healthcare environments offers a viable method for improving understanding of how complex socio-technical systems in care delivery settings may impact patient safety. ABM as a collaborative design tool offers healthcare planning and facility teams the ability to leverage its scenario modeling capabilities to enhance the performance of care environment design safety and efficiency while concurrently building team cohesion and effectiveness.
Supplemental Material
sj-pdf-1-her-10.1177_19375867251317234 - Supplemental material
Supplemental material, sj-pdf-1-her-10.1177_19375867251317234
Footnotes
Acknowledgments
The authors acknowledge the generous support from the University of Florida Office of Research for the development of research described in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The University of Florida IRB (IRB202001819) determined that the research protocol was considered exempt approved as non-human because it posed minimal risk and did not involve human subjects on July 2, 2020.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by the University of Florida Office of Research under Grant (grant number AWD08485).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.