
Abstract
Background
The delivery of preventive and primary care has evolved through various physical environments, from early twentieth-century house calls to centralized settings like physician offices and hospitals, and more recently, through rapid adoption of telehealth. This shift occurred amidst an increasing emphasis on patient/person-centered care models.
Aim
This article conceptually examines the role of the physical environment in optimizing patient/person-centered care within telehealth, focusing on preventive and primary care in the pre-acute stages.
Method
A rapid scoping review was conducted to identify key underlying dimensions of patient/person-centered care. Each dimension was further examined to identify theoretical background and measurement instruments used in the field, to obtain a detailed comprehension of the concepts. A series of brainstorming sessions among contributing authors, in association with logical theory-supported arguments, were conducted to articulate conceptual associations and detect the potential role of the physical environment.
Result
An articulation of the relationships between six underlying dimensions of patient/person-centered care is proposed: Shared Decision-Making, Autonomy, Communication, Empathy, Trust, and Privacy. Furthermore, the potential role of the physical environment in the pathway to patient outcomes is posited.
Keywords
What role does the physical environment potentially play in optimizing patient/person-centered care in telehealth? Telehealth refers to real-time, two-way audiovisual communication between a patient and a healthcare provider located at a different site, facilitated by telecommunications equipment (American Medical Association, n.d.). This article conceptually examines the manner in which the physical environment of care delivery matters in telehealth. It specifically focuses on preventive care and primary care in the pre-acute stages. For the remainder of this article, the term “care” denotes preventive and primary care unless stated otherwise. In preventive/primary care, the physical environment of care delivery has undergone numerous manifestations over the past centuries. House calls were common in the early twentieth century (Fortin Ensign et al., 2019), where the environment of care used to be the patient's home. Factors such as increased specialization within the medical discipline, the need for specialized equipment, and the economics of revenue generation, among others, led to care services moving to centralized settings such as physician offices and hospitals (Fuchs, 1988). Meanwhile, the philosophy of care changed over time within these centralized settings, with the latest focusing on patient/person-centric models (Gartner et al., 2022); all delivered within a provider's office or hospital. The COVID-19 pandemic triggered the latest change in the environment of care delivery, resulting in a quick and massive adoption of telehealth.
Telehealth represents a fundamental shift from traditional healthcare delivery models, which are predicated on the centralization of services in medical campuses and brick-and-mortar buildings that necessitate patient travel (Kamidani & Okada, 2025). Unlike conventional in-person healthcare, which requires patients to overcome geographical and logistical barriers to attend face-to-face interactions in a clinical setting, telehealth leverages telecommunications technologies to provide clinical services at a distance (Kruse et al., 2017). This remote delivery model encompasses a broad range of synchronous (real-time) and asynchronous (time-independent) modalities, including live video consultations and the digital transmission of medical imaging (Gajarawala & Pelkowski, 2021). This core difference directly addresses the challenge of “distance decay,” where the likelihood of accessing care decreases as the travel distance increases, a significant barrier in traditional care models (Alvandi, 2017).
While telehealth as a concept has been in operation since the early 1900s (e.g., telegraphs, radio, and ECG transmissions) (Jagarapu & Savani, 2021), broad clinical adoption did not occur until the mid-twentieth century, and it was during the COVID-19 pandemic that telehealth witnessed a sudden widespread expansion (Gajarawala & Pelkowski, 2021). Since then, numerous lines of inquiry have examined the advantages as well as shortcomings of it. Studies suggest that the adoption of telehealth has addressed issues pertaining to healthcare access, including those for underserved communities, the elderly, and other disadvantaged groups (Gajarawala & Pelkowski, 2021; Shah et al., 2024).
The massive expansion of telehealth modalities of care delivery, however, occurred, and continues to occur, during a period when care models of the twentieth century have been challenged in favor of more patient/person-centric ones; models that are expected to deliver better population health. The Institute of Medicine (2001) defines patient-centered care as an approach in which healthcare is delivered with respect for and responsiveness to each person's needs, preferences, and values, ensuring that these guide all clinical decisions. Related and somewhat overlapping concepts such as “patient-centered care,” “person-centered care,” and “person-focused care” had already emerged long before COVID-19 as the desired overarching philosophy of care delivery in the United States (Švab & Cerovečki, 2024). While such philosophical perspectives have differences, they share similar foundational directions away from treating/managing diseases to treating whole persons (Starfield, 2011). These philosophies changed the roles of and expectations from patients and providers, including enabling patients to make decisions about their own treatments in collaboration and consultation with care providers, in conjunction with such relationship-builders as empathy, dignity, and respect from care providers.
Arguably, the older house call model, perhaps, constituted an ideal patient/person-centric one, occurring within the privacy, confidentiality, comfort, and familiarity of patients’ homes, and conducive to treating whole persons. Telehealth offers an opportunity to recreate such a model of practice, albeit in a different form and modality, where providers visit patients in the latter's choice of setting that affords privacy, confidentiality, comfort, and familiarity (Edirippulige & Armfield, 2017).
A related question, as a result, pertains to whether telehealth fits into and satisfies the key performance objectives of the prevailing patient/person-centered care philosophy. Several published studies in the context of telehealth suggest mixed outcomes, with some areas exhibiting greater levels of performance while others needing work; mostly within solitary dimensions of performance. Examples include work on the physician–patient relationship, trust, and the shifting dynamics of patient autonomy in primary care amidst eHealth adoption (Ramachandran et al., 2023); provider–patient communication during telemedicine consultations (Nguyen et al., 2024); empathy (Sperandeo et al., 2021); trust (Liu & Tao, 2022); and privacy concerns in telemedicine and eHealth (Kato-Lin & Thelen, 2022). Notably, a larger volume of published literature is available on these topics focused on in-person, hospital, and physician-office-based care delivery, although publications articulating all underlying dimensions of patient/person-centered care philosophy in the context of telehealth, in a comprehensive essay, are not widely available. Consequently, two questions emerged for exploratory examination: (1) what are the underlying dimensions of patient/person-centered primary/preventive healthcare and (2) in what possible ways are these dimensions of performance associated with the physical environment of care in telehealth?
The telehealth environment refers to the physical space where a virtual healthcare encounter occurs, recognizing that even video calls are shaped by the built environment (Taylor, 2024). In healthcare settings, telehealth often happens in dedicated rooms or kiosks typically designed according to the Facility Guidelines Institute and evidence-based design principles. For example, spatial layout mitigates distractions by situating rooms away from high-traffic zones; incorporating acoustic treatments (e.g., carpeting and sound-absorbing panels), enhancing privacy; and including visual cues such as signage or institutional branding reinforce professionalism during care delivery (Sun et al., 2023).
By contrast, home-based telehealth takes place in nonclinical areas. Telehealth design studies confirm that environmental conditions, whether in purpose-built suites or living rooms, impact the quality of virtual care (Duane et al., 2022; Sun et al., 2023). Additionally, some patients and providers choose alternative locations (like cars, workplaces, or public spaces) for telehealth when home environments are unsuitable or schedules demand flexibility; these improvised settings, however, often lack clinical design and may present communication challenges.
For the purpose of this exploration, patient-centered care (PCC) was operationally defined as healthcare that enables alignment with the patient's values, needs, and desires, and is achieved when providers actively involve patients in discussions and decisions about their care (Gartner et al., 2022). It emphasizes a shift from disease-centered to person-focused interactions, where patients are viewed as whole individuals within their social and emotional contexts (Olsson et al., 2013).
Dimensions of Patient-/Person-Centered Care
Exploration
Toward answering the aforementioned questions, a rapid scoping review was done by the authors to identify the underlying domains constituting patient/person-centered care in patient–provider interaction. Google Scholar was used to source relevant peer-reviewed articles published during 2014–2024 to maintain the focus and manageability of the review and capture only the latest thoughts. Since telehealth arguably involves more than medicine and includes mental healthcare, health education, as well as other psychological and social phenomena, Google Scholar was used to search and extract relevant publications from multiple fields in an economical and time-efficient manner. This approach enhanced sourcing for this manuscript by indexing scholarly materials from diverse and international sources, which led to a more inclusive and global perspective within a reasonable time than relying on more narrowly focused databases (Gehanno et al., 2013). Titles and abstracts were screened to select the most pertinent studies. Additionally, hand searching and reviewing the references of the identified articles were undertaken, when necessary, particularly in cases where relevant theoretical explanations or deeper conceptual foundations were not adequately addressed within the past 10 years. The necessity for hand search was determined based on the absence of detailed or high-quality discussions on specific concepts within recent literature, prompting the inclusion of earlier foundational works that were frequently cited and widely recognized in the field.
The literature search-analyses involved two broad phases. The first phase involved a quick initial exploration of literature on patient–provider interactions in patient-centered care, published during 2014–2024. The intent was to identify any and all possible phenomena associated with the latter as identified by other authors in various fields of study. Twenty-one frequently cited articles on the topic were manually selected for general review to identify dimensions of patient/person-centered care (Table 1).
Reviewed Articles Used to Identify Dimensions of Patient/Person-Centered Care.
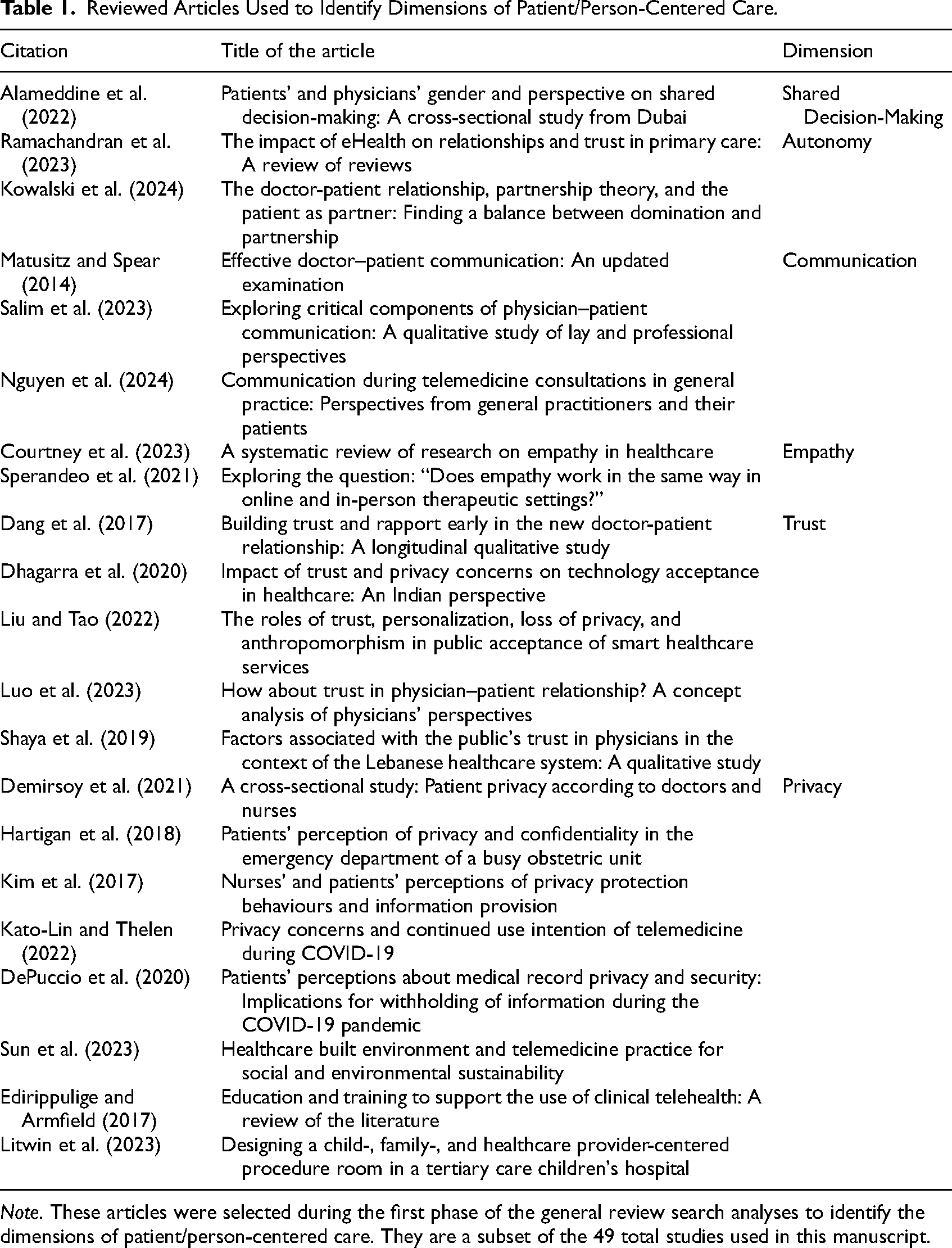
Note. These articles were selected during the first phase of the general review search analyses to identify the dimensions of patient/person-centered care. They are a subset of the 49 total studies used in this manuscript.
Subsequently, the research team convened for a series of structured meetings to engage in a collaborative and iterative process. During these sessions, individual themes were compared, discussed, and systematically organized into potential broader dimensions that captured the essence of the literature (Torraco, 2016). This phase resulted in the identification of six broad dimensions arguably important to patient-provider interactions in patient/person-centered care: Shared Decision-Making, Autonomy, Communication, Empathy, Trust, and Privacy. These dimensions reflect a synthesis of the most prominent and recurrent scholarly work and theoretical arguments present across the reviewed articles as they relate to patient-centered care within the context of face-to-face and telehealth modalities of treatment. It should be noted that this determination was made by the authors of this manuscript as an initial response to the first question and is subject to peer criticism and future modifications.
The second phase involved a Rapid Scoping Review within each of the six dimensions identified in the first phase. After each team member independently searched and identified available scholarly literature published during 2014–2024 aligned with the aforementioned dimensions, they conducted a thorough review of the articles to become familiar with the content and to identify salient concepts and theoretical propositions, in the contexts of traditional face-to-face interactions and telehealth modalities. Subsequently, theories and frameworks relevant to each of the six dimensions were searched and extracted using Google Scholar. The theories and frameworks were selected based on the number of citations and their relevance in their respective domains. These frameworks helped identify specific factors critical to optimizing patient–provider interactions. Published information on potential factors in the physical environment of care delivery that may influence the six identified dimensions was identified and extracted in this phase.
Figure 1 illustrates the key steps in the inquiry in a PRISMA-like diagram for better clarity. It should be noted that this study did not involve a systematic literature review, and hence, Figure 1 should not be read as a PRISMA diagram. It visualizes the selection of 21 frequently cited articles reviewed to identify dimensions of patient/person-centered care.
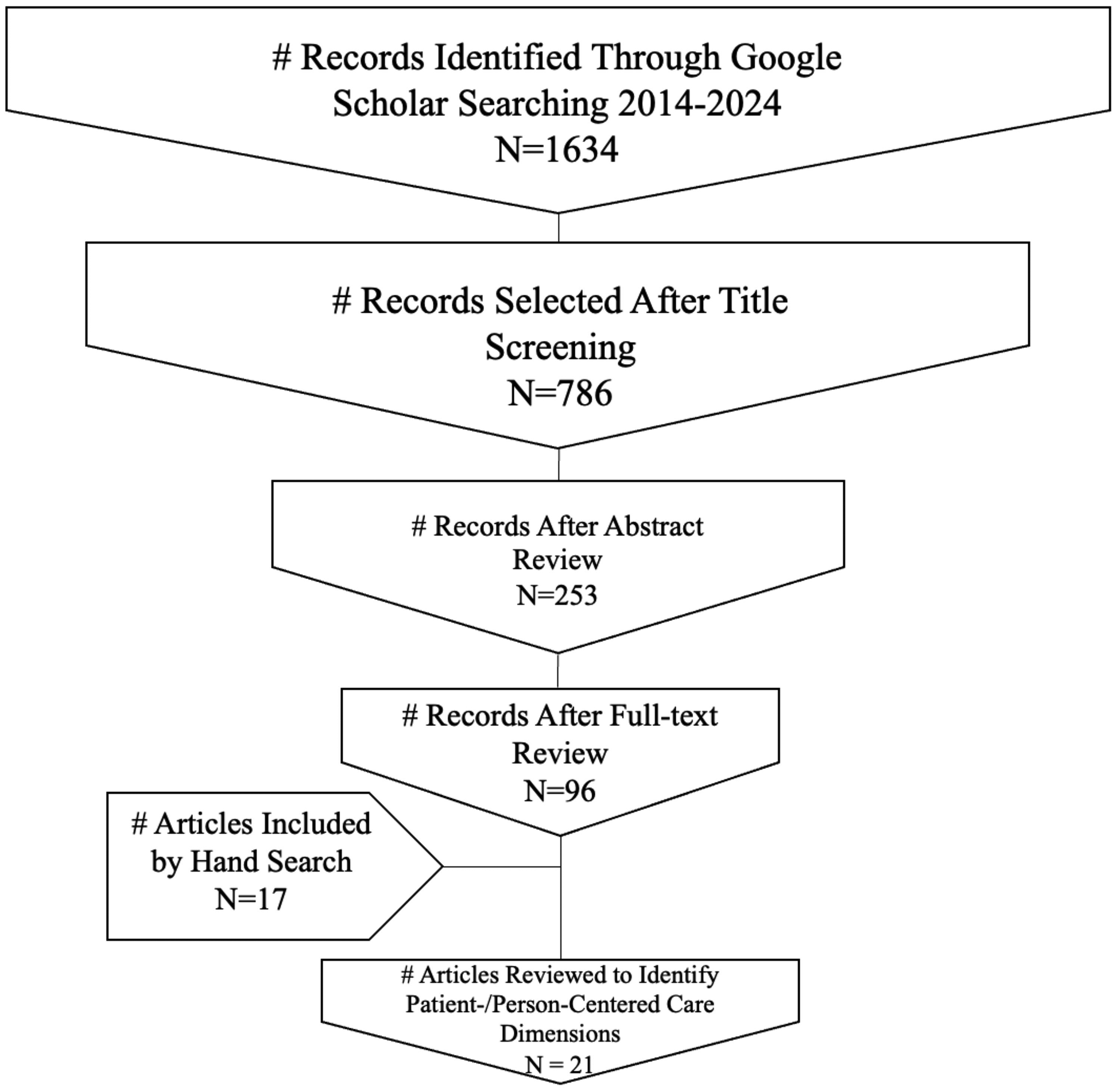
Flow chart illustrating key steps in the general review and analysis of articles used to identify patient/person-centered care dimensions.
Underlying Dimensions
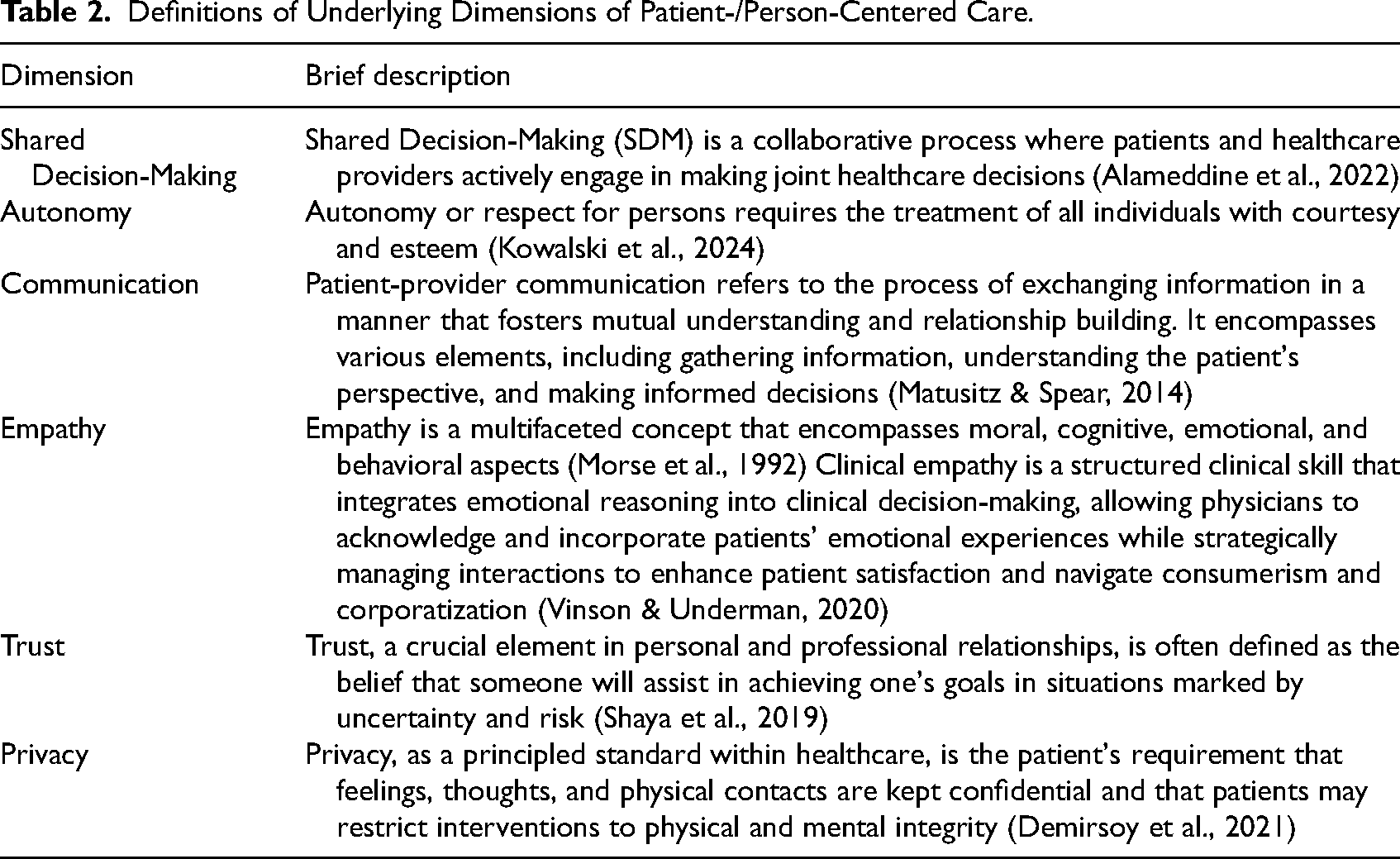
Table 2 provides brief descriptions of the dimensions based on established literature. Where multiple definitions exist, those closest to the operational definition of patient-centered care were adopted. Detailed discussions on these dimensions will be presented in a separate literature review publication by the authors. The present arguments focus mainly on examining the potential role of the physical environment in patient/person-centered telehealth care.
Definitions of Underlying Dimensions of Patient-/Person-Centered Care.
Interrelationships
A critical examination of the dimensions related to the built environment suggests that the dimensions of communication overlap with interaction, trust, perceived privacy, empathy, autonomy, and shared decision-making, and are not mutually exclusive, and that there are potential meaningful interrelationships and dependencies among them. Figure 2 provides a conceptual argument regarding interrelationships and dependencies. These arguments are based on critical thinking and brainstorming by the authors and are open to peer criticism.
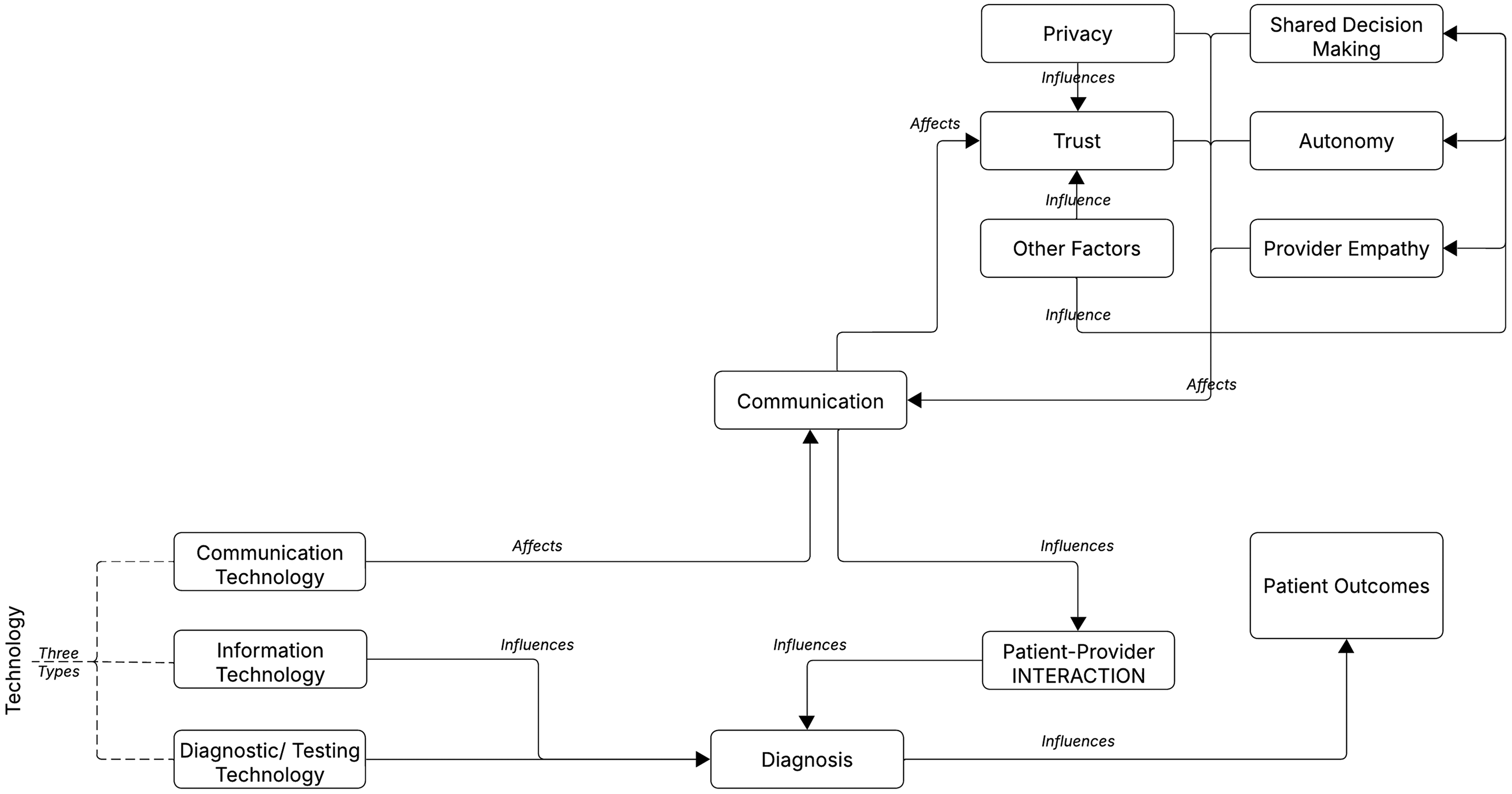
Suggested relationships between the dimensions of patient-/person-centered care.
As posited in Figure 2, the quality of patient–provider interaction is fundamental to optimal diagnosis and, consequently, patient outcomes, thereby contributing to the overall success and efficacy of care delivery. In healthcare communication, the distinction between interaction and communication is often unclear, with the two terms frequently used interchangeably. However, some studies have highlighted differences, suggesting that interaction is a broader concept that encompasses communication. Communication refers to the process by which individuals create and interpret meaning through the exchange of messages (Liu et al., 2023). This process does not necessarily require a response, meaning it can occur even when only one person is involved in sending or interpreting a message. In contrast, when the exchange of information results in reciprocal influence, where both the sender and receiver continuously affect each other, it is described as an interaction (Dar & Bernardet, 2020).
Interaction is characterized by the following: (1) reciprocity and mutual influence: interactions take place in the moment and involve mutual exchange, where all individuals actively engage and respond to one another, leading to a sense of psychological connection and shared involvement between the participants (Pan & Cheng, 2020) and (2) multimodal communication: interactions depend on both verbal and nonverbal signals. Successful communication requires aligning spoken messages with their delivery. Elements such as tone of voice, eye contact, facial expressions, gestures, and body posture should be consistent with verbal content to ensure clarity and effectiveness (Salim et al., 2023).
Multiple factors affect communication: the level of trust earned by the provider could determine the level of openness a patient is willing to adopt—the higher the trust, the greater the openness (Luo et al., 2023). Similarly, higher perceived privacy in the communication environment could result in greater openness in communication. It should be noted that actual privacy is not the same as perceived privacy, although both are important, and that both real and perceived privacy relate to four domains—visual, auditory, physical, and informational (Dhagarra et al., 2020; Litwin et al., 2023). Higher perceived privacy for the patient enables a greater sense of control for the patient, which may foster a greater level of participation and openness to communicate sensitive/personal information. Providing greater perceived privacy to a patient could, by itself, contribute to trust building (Kim et al., 2017). It may suggest empathy and care on the part of the provider. Similarly, higher quality communication resulting from higher perceived privacy could also contribute to the process of trust building (Dang et al., 2017).
Three other dimensions may also affect communication quality: provider empathy (Courtney et al., 2023), patient autonomy (Kowalski et al., 2024), and shared decision-making (Alameddine et al., 2022). Numerous operational, social, cultural, and other variables may influence the dimensions presented, as identified in the literature review. Discussions on those are outside the scope of the current article and are presented elsewhere.
Role of the Physical Environment
Could the physical environment play a role in the conceptual relationships articulated in Figure 2? The following arguments are also based on critical thinking and brainstorming by the authors and are open to peer criticism. The propositions here are intended as a starting point for engagement and further examination by the healthcare and healthcare design community. Figure 3 posits the potential role the physical environment of primary/preventive care may play in achieving patient/person-centered care objectives. Specific physical environment factors considered important are overlaid in Figure 3, positing possible relationships between attributes of the physical environment and dimensions of patient/person-centered care.
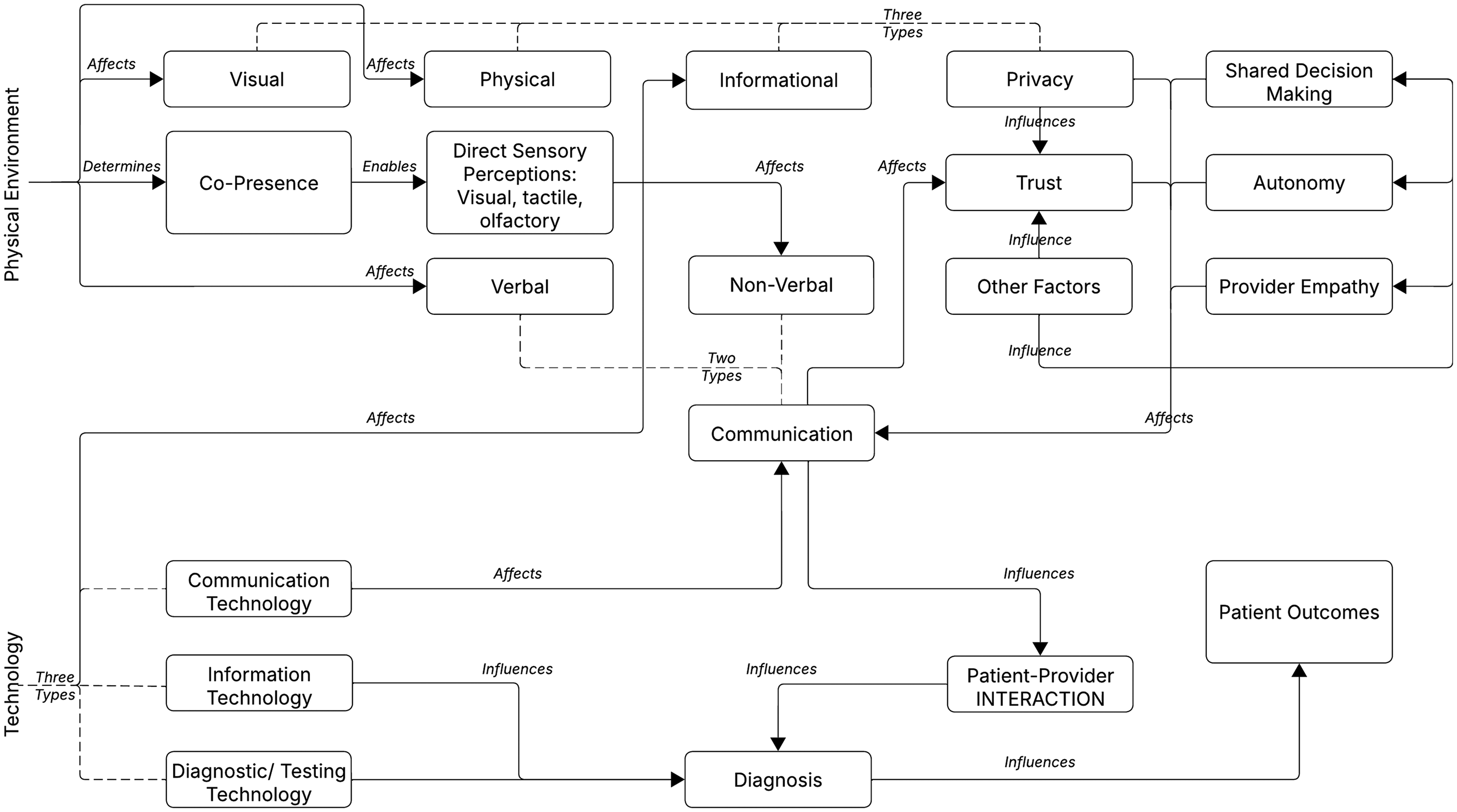
Physical environment factors potentially affecting dimensions of patient-/person-centered care.
As posited in the conceptual diagram, the design of the physical environment determines whether co-presence of the provider and patient is possible, as in a doctor's office. Co-presence, or the lack thereof, possibly affects the quality and efficacy of direct sensory perceptions. Direct sensory perceptions include the ability to see clearly (visual; visual examinations, eye contact, etc.), speak/hear clearly (auditory; speech clarity, intelligibility, speech privacy, etc.), touch (tactile; physical touch during examination, etc.), and smell (olfactory; ability to smell to detect olfactory indicators of illness, etc.). As previously discussed, patient–provider communication includes both verbal and nonverbal modalities. The physical environment directly affects the quality of verbal communication, including speech clarity, intelligibility, and speech privacy, through such physical properties as background noise, reverberation time, and sound isolation (Lo Castro et al., 2022; Puglisi et al., 2021).
Furthermore, physical design, by enabling co-presence, influences all types of nonverbal communication in the visual, tactile, and olfactory domains. Privacy is affected by both the physical environment and technology. The former directly affects visual, auditory, and physical privacy (Demirsoy et al., 2021; Hartigan et al., 2018). The fourth type of privacy is informational privacy, which is affected by both the type of technology adopted as well as the human–machine interface situated in the physical environment of care (DePuccio et al., 2020). For instance, the location and directionality of a monitor showing protected patient information may affect whether such information is visible to others, thereby affecting HIPAA (Health Insurance Portability and Accountability Act, 1996) regulations.
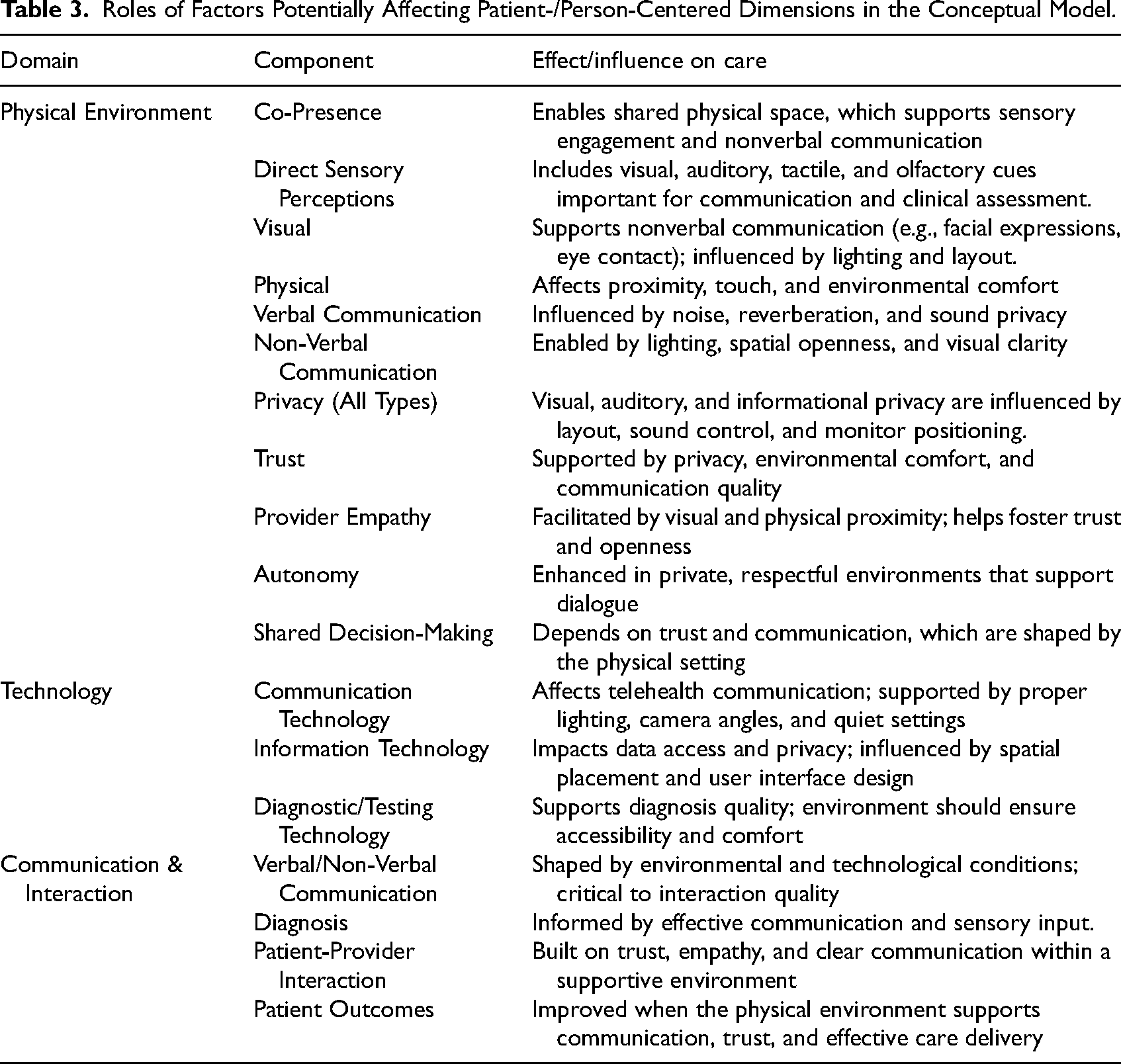
Finally, three types of technology could be argued to play important roles in the care process. Communication technology, in the context of telehealth, can affect patient–provider communication quality. Information technology and diagnostic/testing technology can affect the quality of diagnostic outcomes from the patient–provider interactions, consequently influencing patient outcomes. Table 3 summarizes the roles of factors within patient–provider interactions.
Roles of Factors Potentially Affecting Patient-/Person-Centered Dimensions in the Conceptual Model.
Although telehealth removes the shared physical space between patient and provider, the surrounding environment remains vital. Each setting, whether clinical, residential, or another location, provides a context that influences communication, clinical decision-making, and the therapeutic alliance (Duane et al., 2022; Sun et al., 2023). Environmental factors play a direct role in communication quality. Proper lighting enhances facial visibility and nonverbal cue interpretation (Taylor, 2024), while good camera positioning supports eye contact, which fosters trust and attentiveness (Henry et al., 2017). Cluttered backgrounds and visual distractions can reduce message clarity and credibility, making it harder for patients to stay engaged (Duane et al., 2022). Likewise, background noise and poor soundproofing disrupt verbal exchange, increasing the risk of miscommunication and dissatisfaction (Duane et al., 2022; Sun et al., 2023). Clinical guidelines emphasize the importance of quiet, private, well-lit, and organized spaces to minimize distractions and support nonverbal cue recognition like facial expressions and gaze, which are essential for engagement and trust (Meuter et al., 2021). A calm, comfortable setting also helps patients stay focused, lowers stress, and promotes more open participation (Sun et al., 2023).
Environmental issues like camera misalignment, screen glare, and household distractions can hinder dialogue and reduce consultation quality (Henry et al., 2017). In contrast, ergonomic setups with calming features, high-resolution video, and proper camera angles support natural conversation, eye contact, and patient comfort (Henry et al., 2017; Sun et al., 2023). A quiet, professional setting enhances credibility (Duane et al., 2022) and minimizes barriers to shared understanding (Henry et al., 2017). Thus, the telehealth environment actively shapes communication and patient outcomes (Duane et al., 2022; Sun et al., 2023).
Discussion
In light of the aforementioned findings and arguments, which dimensions of patient/person-centered care in telehealth could possibly be witnessing challenges? Considering the three environmental contexts of primary/preventive care delivery—homes during physician house calls, hospitals and doctors’ offices, and telehealth—one may argue that although the philosophy of patient/person-centered care originated in the twenty-first century, many of its desired dimensions of performance were already present in the house call model of care delivery in the twentieth century. Inside one's home, visual, auditory, and physical privacy was possibly guaranteed in most situations. Informational privacy was probably not an issue in that period. Both verbal and nonverbal modes of communication were enabled, owing to the co-presence of provider and patient. Optimal privacy possibly enhanced trust, and hence openness of communication as well as patient–provider interaction.
While novel strategies and ideas emerged during the past decades for implementing patient/person-centered care in hospital and doctor's office settings (Fix et al., 2018), the centralized model of care delivery has been plagued with challenges for several segments of the US population—those in remote locations, the infirm and elderly, and the financially challenged, among others (Andrilla et al., 2018). Telehealth is offering a model that parallels doctors’ house calls of previous centuries, which may overcome these challenges. The difference being that the physical presence of the provider (physicians, mental health providers, etc.) is substituted by virtual presence. While there is an undercurrent of understandable optimism and expectations regarding telehealth, one may ponder whether and how its performance on the six underlying dimensions of patient/person-centered care has possibly altered, when a physical separation is introduced between providers and patients.
It may be logically argued that provider–patient physical separation could affect all forms of nonverbal communication. For instance, the ability for visual inspection, ability to touch, ability to smell, ability to develop rapport through eye contact, monitor body language and gestures, examine facial expressions, skin color, and other forms of examinations available in traditional interaction modalities may be affected. Developing trust may pose a challenge, especially if such communications are affected. From the patient's perspective, the level of informational privacy as well as visual privacy may be unclear—such as a lack of control over (if) other people are in the physical space along with the provider. The range of diagnostic/testing technology available may be limited. On the positive side, the quality of verbal communication depends on the type of technology, which in some studies has been shown to improve telehealth (Kruse et al., 2017). Physical privacy possibly remains unchanged.
More consequently, the aforementioned possibilities beg the question as to whether telehealth interactions could be designed to be as similar as possible to in-person interactions on the six performance dimensions of patient/person-centered care. The ideal direction seems to be in approaching technology and the physical design of the care environment at both ends as a conceptual whole, rather than unrelated facets of a care delivery system.
Conclusion
Can the physical environment play a role in optimizing patient/person-centered care in telehealth? Published studies suggest that telehealth offers numerous benefits, especially in the context of care delivery to those in remote locations, the infirm, the elderly, the financially challenged, and other underserved communities. However, telehealth emerged as a modality of care delivery during a prevailing umbrella philosophy of patient/person-centered care. A review of the literature suggests six underlying dimensions of this philosophy: Shared Decision-Making, Autonomy, Communication, Empathy, Trust, and Privacy. With the physical separation of providers and patients, can it be argued that achieving optimal performance on one or more of these may require support from the physical environment? The authors posit that the ideal solution is in approaching technology and the physical design of the care environment at both ends as a conceptual whole, rather than unrelated facets of a care delivery system.
Implications for Practice
Conceptual examination suggests that the physical environment has a potential role to play in optimizing patient/person-centered care in telehealth. Consequently, consider the physical environment on both the provider and patient sides in addition to the communication media, in design.
Patient–provider interaction is more than patient–provider communication. Until further empirical evidence is made available through research studies, use the best judgment to optimize interaction through the design of both the technology and physical environment.
Supplemental Material
sj-pdf-1-her-10.1177_19375867251374670 - Supplemental material for The Potential Role of the Physical Environment in Telehealth: A Patient-Centered Care Perspective
Supplemental material, sj-pdf-1-her-10.1177_19375867251374670 for The Potential Role of the Physical Environment in Telehealth: A Patient-Centered Care Perspective by Debajyoti Pati, PhD, FIIA, IDEC, LEED®AP, Cameron C. Brown, PhD, LMFT-S (TX), AAMFT, Farzane Omidi, PhD, EDAC, LEED, Fatemeh Dianat, MArch, MS, LEED, and Daphne A. U. Chilaka, MSc,MS, WELL AP, LEED in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statement
Due to the conceptual nature of this manuscript, no data were collected. As there were no participants, no institutional approval was needed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.