
Abstract
Aim
To compare the perspectives of two stakeholder groups, adult day care center (ADCC) managers and family members of older adults with disabilities or dementia, regarding ADCC site and building design features.
Background
The ADCCs provide community-based services for older adults with disabilities or dementia and support family caregivers. Different stakeholder groups, including managers and family caregivers, may have varying views on the planning and design of health facilities. However, little is known about how managers and family members differ in their views on ADCC planning and design.
Methods
We adopted a cross-sectional exploratory design across Taiwan. Ten site selection factors and eight building design factors were used to construct an analytic hierarchy process questionnaire. A total of 81 managers and 59 family members were included, and the data were collected using one-on-one interviews. Pairwise comparisons between factors were conducted to obtain the eigenvectors (priority weights), and weight differences between the managers and family members were calculated using t-tests.
Results
Managers placed higher importance on community attitudes and governmental support, while family members emphasized access to health services, transportation, and public safety. In building design, family members valued clearer spatial visibility, whereas managers placed relatively greater emphasis on temperature control.
Conclusions
Managers and family members of service users weighed site and building design factors differently, especially in the domains related to “support and attitudes” and “services, systems, and policies.” These findings highlight important differences between these two stakeholder groups and provide critical insights for the planning and design of ADCCs.
Keywords
Population aging and advancements in medical technology have increased the number of older adults living with chronic disabilities or dementia and intensified the demand for community-based long-term care and supportive built environments (Kumar et al., 2023). Adult day care centers (ADCCs) are a key service model in emerging community care networks. They provide daytime supervision, health and activity programs, and social participation opportunities for community-dwelling older adults with disabilities or dementia while also alleviating feelings of loneliness and reducing the burden of caregiving for families (Ellen et al., 2017; Sadarangani et al., 2021, 2024). Because many users tend to visit ADCCs for several days per week over prolonged periods, decisions regarding where these centers are located and how they are designed have major implications for their safety, engagement, and well-being.
Over the past decade, the Taiwanese government has actively promoted the establishment of ADCCs through various subsidy schemes in collaboration with private social welfare organizations. These initiatives have led to a rapid increase in both the demand for and the number of ADCCs (Department of Long-Term Care, Ministry of Health and Welfare, Taiwan, 2024). However, because of the limited funding and resources available for facility renovation, making appropriate decisions regarding the location and building design of ADCCs is crucial. Consequently, careful planning and design are essential to ensure that ADCCs meet the diverse needs of service users and their families.
The initial stage of planning and designing new health-promoting facilities is particularly essential because decisions made at this stage can shape workflows and user satisfaction for many years to come (Elf et al., 2015). Previous research into ADCCs and other similar settings has typically focused on either users or professionals in isolation, most often utilizing qualitative methods to explore their experiences and needs, highlighting that individuals in different roles and contexts may hold distinct views on how such facilities should be planned and designed (Miedema et al., 2018). However, quantitative evidence directly comparing how managers and family members of service users prioritize specific site-specific and building-specific design features remains scarce. This knowledge gap runs deep because managers are primarily responsible for operational feasibility and regulatory compliance, whereas family members are more directly concerned with everyday usability, accessibility, and perceived safety.
The analytic hierarchy process (AHP), developed by Saaty (2012), is a decision-making method that integrates qualitative judgments and quantitative weighting within a hierarchical structure. It enables multiple stakeholders’ opinions to be captured by structuring selection factors into levels and using pairwise comparisons to derive priority weights for each factor. According to the literature, the AHP can provide robust support for medical and health-care decision-making and mitigate the risk of problematic choices (Khan & Ali, 2020). In addition, it can be applied in health-care facility site planning (Şahin et al., 2019).
In this study, we used the AHP to examine how managers and family members of service users prioritize specific site and building design features for ADCCs. Our goal was to identify the respective prioritization patterns of these two groups of individuals and determine the differences between them on the basis of their AHP-derived weights.
Methods
Study Design
This cross-sectional exploratory study was conducted in several ADCCs across Taiwan. Figure 1 illustrates a typical range of exterior and interior environments in the participating centers, including multipurpose activity spaces, rural outdoor settings, and semi-outdoor transitional areas. This study was divided into three stages in accordance with the standard AHP procedure (Saaty, 2012).

Environmental settings in participating adult day care centers (ADCCs): (A) multipurpose activity room with homelike furnishings and nostalgic decorations to create a familiar atmosphere; (B) rural ADCC with a garden and outdoor sitting area that allows older adults to enjoy daylight; and (C) urban ADCC where an existing balcony has been modified into a semi-outdoor space to provide a place for sitting in the sun.
In Stage 1, the hierarchical structure of the selection factors was established. First, an internal scoping literature review and a previous empirical study on ADCC managers’ views (Su et al., 2020) were used to identify potential environmental factors relevant to ADCC site selection and building design. Second, these factors were mapped onto the “Environmental Factors” component of the International Classification of Functioning, Disability, and Health (World Health Organization, 2001) to group them into broader dimensions and more specific subdimensions. Third, an expert panel reviewed the operational definitions and suitability of each factor and refined the final list used in the questionnaire.
In Stage 2, on-site visits were made to the participating ADCCs for questionnaire administration. During each visit, a trained researcher individually met with the center manager and, when applicable, one family member to provide study information, obtain written informed consent, and administer the AHP questionnaire in a face-to-face session. As part of a parallel study, some managers also participated in brief qualitative interviews and environmental walkthroughs; the methods and findings pertaining to this qualitative component have been reported elsewhere (Su et al., 2020), and this article reports only the questionnaire data.
In Stage 3, the data collected were analyzed. This analytical procedure included establishing pairwise comparison matrices, conducting consistency tests, analyzing the overall weights of the selection factors (e.g., ADCC site and building design features), examining the weights at each hierarchical level, and comparing the results of the managers and family members.
Ethical Considerations
This study was conducted in accordance with institutional and national ethics guidelines and the Declaration of Helsinki. The protocol was approved by the Institutional Review Board of National Yang-Ming University (now National Yang Ming Chiao Tung University) (approval no. YM104067E). Before data collection, center managers and family members received written information about the study and provided written informed consent. Participation was voluntary, and participants could decline or withdraw at any time without consequences for employment or services. Questionnaire data were coded, stored securely, and analyzed in aggregate to protect privacy and confidentiality.
Participants
The first-stage expert panel comprised two architects and three long-term care professionals purposively selected in accordance with the following criteria: (1) holding a professional license in architecture or rehabilitation (e.g., physical therapy); (2) currently working in the planning, design, management, or evaluation of long-term care or community-based services for older adults, with at least 5 years of experience; and (3) having a history of engaging in projects related to the built environment of health-care or long-term care facilities, including ADCCs. All experts were practicing in Taiwan and were familiar with the local policies, regulations, and service models for ADCCs. They reviewed the operational definition and suitability of each selection factor, discussed discrepancies, and reached a consensus on the final set of factors and their hierarchical structure before the questionnaire survey was administered.
The second-stage participants comprised 83 ADCC managers and 64 service users’ family members. Managers were eligible if they had held a management-level position in a registered ADCC for at least 3 months. Managers working in centers that had been in operation for less than 6 months were excluded. Family members were eligible if they (1) were aged ≥20 years, (2) were within the third degree of kinship to the service user, (3) had a relative who attended an ADCC for at least 4 h per day on at least 2 days per week, and (4) lived in the same household and were familiar with the service user's daily living situation. Family members whose relatives had used ADCC services for less than 3 months were excluded.
Analytic Hierarchy Process Hierarchical Structure Questionnaire Design
We selected 10 site-related and 8 building-design-related factors from the internal scoping review and organized them into a hierarchical structure for the AHP questionnaire. We then grouped these factors into three site-related and two building-design-related dimensions and formulated operational definitions accordingly (Supplemental Material 1). To maintain the hierarchy within the respondents’ information-processing capacity, we followed Miller's (1956) seven-plus-or-minus-two rule and Saaty's (2012) recommendation that no more than seven factors should be compared within a single AHP level (i.e., each level containing at most seven factors). An expert panel reviewed the operational definition and suitability of each factor and reached a consensus on the final hierarchical structure for site and building design features. The AHP questionnaire utilized Saaty's (2012), p. 9-point rating scale and pairwise comparisons. Specifically, factors at each level were compared with respect to the factor immediately above. For a level with n factors, n (n − 1)/2 pairwise comparisons were required to simplify the task and help the respondents focus on the relative importance of two factors. The AHP questionnaire is detailed in Supplemental Material 2.
Analytic Hierarchy Process Questionnaire Data Collection Process
Managers were recruited from ADCCs across Taiwan through a stratified sampling technique (Portney & Watkins, 2009). After these managers were contacted by email or phone and informed of the study, appointments were made for on-site visits. During these visits, we provided detailed verbal and written information, explained the AHP and the operational definition of each selection factor, and obtained written informed consent before administering the AHP questionnaire in a one-on-one session. We also asked the managers to help identify family members of service users who met the inclusion criteria. We invited interested family members to the ADCC at a scheduled appointment, where we again explained the study, obtained written informed consent, and individually administered the questionnaire.
During on-site visits, both managers and family members completed the questionnaire face-to-face with a researcher at the ADCC. Participants could choose a comfortable location within the center; whenever possible, a quiet room or corner was used. At the start of each session, the researcher emphasized that responses would be anonymous, used only for research, and that participants could skip any item they did not wish to answer. There was no time limit, and participants completed the questionnaire at their own pace; on average, completion took about 45 min and did not exceed 60 min.
Data Analysis
We used SPSS version 18.0 (SPSS, Chicago, IL, USA) for data entry and descriptive statistics and Expert Choice version 11.5 for the construction of AHP pairwise comparison matrices for site- and building-design-related selection factors. For each matrix, we calculated the principal eigenvalue and its associated eigenvector. In the AHP framework, the eigenvector represents the set of relative weights that best fits the pattern of pairwise comparison judgments across all factors in the matrix, and the corresponding eigenvalue indicates how consistent these judgments are. In the present study, the normalized elements of the principal eigenvector were treated as the local priority weights of the selection factors within each matrix. Global weights for the lowest-level factors were obtained by multiplying their local weights by the weights of the higher-level criteria along each branch of the hierarchy. Matrix consistency was evaluated using a consistency ratio (CR) of ≤0.10, as outlined by Saaty (2012). Responses with inconsistent matrices (CR > 0.10) were excluded, resulting in 140 valid cases (81 managers and 59 family members). Independent-samples t-tests (α = 0.05) were used to determine the differences between managers and family members in terms of the weights assigned to site and building design factors for ADCC planning and design.
Results
Participant Characteristics
A total of 147 questionnaires (83 by managers and 64 by family members of service users) were returned by 83 ADCCs (Table 1). After seven inconsistent AHP responses were excluded, 140 valid questionnaires remained for analysis (81 by managers and 59 by family members). Although the two groups were broadly comparable in terms of gender (78.3% vs. 71.9% women), proportion of community-based ADCCs (92.8% vs. 93.8%), and urban versus rural ADCCs, some contextual differences were observed. For example, managers were more likely to work in publicly funded centers (public management of public organizations or private management of public organizations, 28.9% in total), whereas family members were almost exclusively affiliated with privately operated centers (92.2%). In addition, managers were more concentrated in the central region (37.3%), whereas family members were more concentrated in the eastern region (18.8% vs. 8.4% among managers). On average, managers had approximately 8 years of experience working in long-term care.
Basic Information and Characteristics of the Participants.
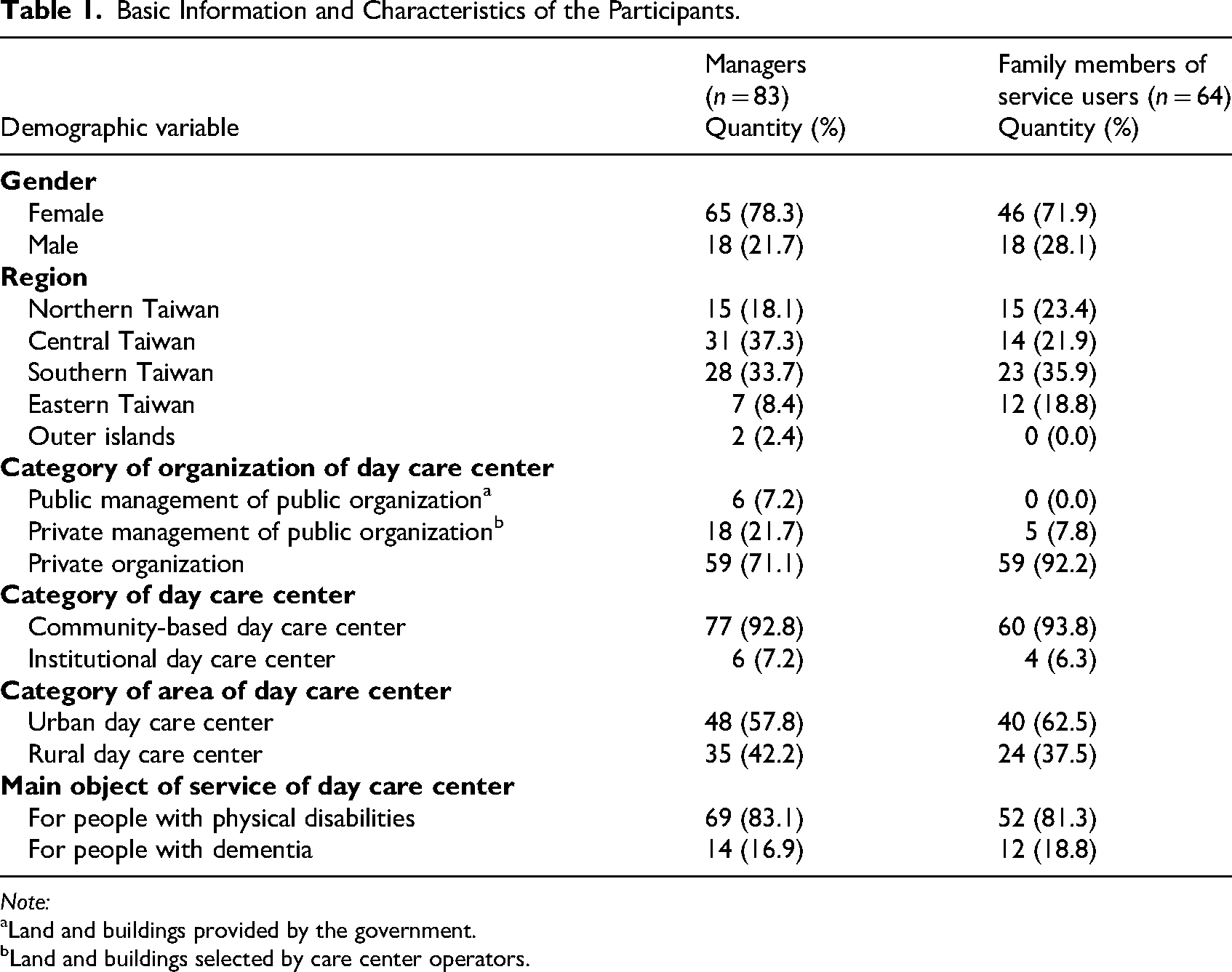
Note:
Land and buildings provided by the government.
Land and buildings selected by care center operators.
Of the 64 family members who initially responded to the questionnaire (before the AHP consistency examination), 36 (56.3%) were sons or daughters of service users, 21 (32.8%) were daughters-in-law of service users, 3 (4.7%) were spouses or common-law partners of service users, and 4 (6.3%) were related to service users in other manners. On average, service users visited ADCCs for 4.41 days per week and used their services for 32.59 h per week, with median service use duration of 11 months. These discrepancies in organizational type, regional distribution, and caregiving roles may partly shape the perspectives of managers and family members and should be considered when interpreting group differences in their AHP-derived preferences for ADCC site and building design features.
Site Selection
Table 2 summarizes the AHP weights, ranks, and between-group differences for ADCC site selection factors. Supplemental Material 3 provides detailed Levels 1 and 2 weights and CRs, and Supplemental Material 4 provides full statistics from independent-samples t-tests. At the dimensional level, both managers and family members prioritized health services, health systems, and health policies, followed by support and attitudes, the natural environment, and human-made changes to the environment. At the factor level, managers prioritized community support, particularly the attitudes of local residents and authorities. They also prioritized health services and policies and transportation services. By contrast, family members prioritized health services, health systems, health policies, and transportation services, followed by the attitudes of authorities, the attitudes of local residents, and public safety. Independent-samples t-tests revealed significant between-group differences in terms of population, health, attitudes of local residents, attitudes of authorities, transportation services, and public safety. Managers prioritized community attitudes and population, whereas family members prioritized health, transportation, and safety-related factors.
Managers prioritized community attitudes and population, whereas family members prioritized health, transportation, and safety-related factors.
Global AHP Weights, Ranks, and Between-Group Differences for ADCC Site Selection Factors by Stakeholder Group.
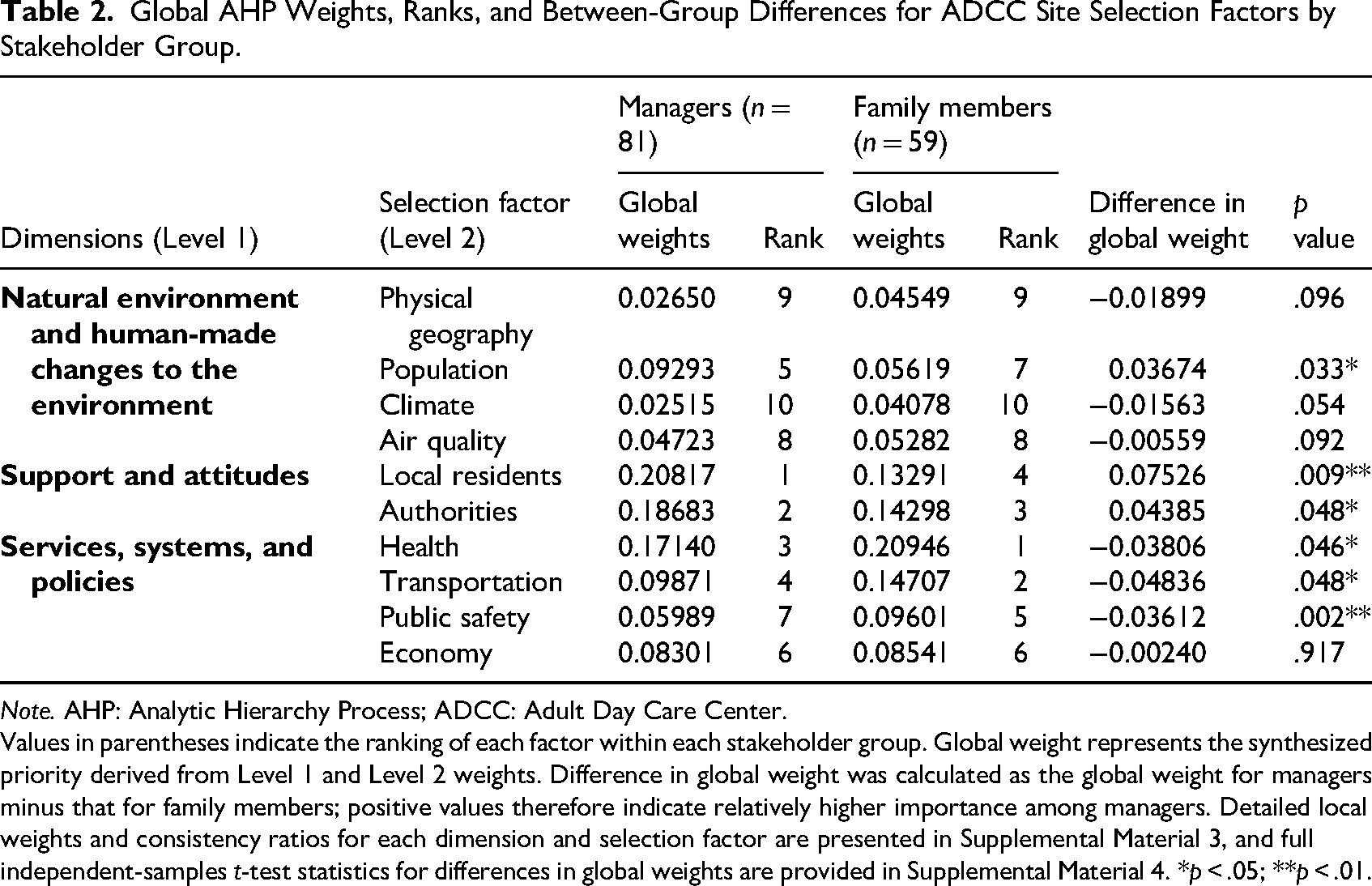
Note. AHP: Analytic Hierarchy Process; ADCC: Adult Day Care Center.
Values in parentheses indicate the ranking of each factor within each stakeholder group. Global weight represents the synthesized priority derived from Level 1 and Level 2 weights. Difference in global weight was calculated as the global weight for managers minus that for family members; positive values therefore indicate relatively higher importance among managers. Detailed local weights and consistency ratios for each dimension and selection factor are presented in Supplemental Material 3, and full independent-samples t-test statistics for differences in global weights are provided in Supplemental Material 4. *p < .05; **p < .01.
Selection of Building Design Features
Table 3 summarizes the AHP weights, ranks, and between-group differences for ADCC building design features. Supplemental Material 5 provides detailed Levels 1 and 2 weights and CRs, and Supplemental Material 6 provides full statistics from independent-samples t-tests. At the dimensional level, both managers and family members prioritized the basic requirements of buildings instead of the dimensions of design, construction, and building products and technology. In terms of individual features, managers prioritized facility design, followed by daylight and ventilation quality, while also prioritizing entrance and exit design. Family members demonstrated a slightly different pattern. They prioritized daylight quality, facility design, and exterior and interior spatial vision, followed by entrance and exit design. Between-group comparisons revealed significant differences in exterior and interior spatial vision and in the quality of temperature adjustment. Family members prioritized clearer spatial visibility, whereas managers prioritized effective temperature control.
Family members prioritized clearer spatial visibility, whereas managers prioritized effective temperature control.
Global AHP Weights, Ranks, and Between-Group Differences for ADCC Building Design Feature Selection Factors by Stakeholder Group.
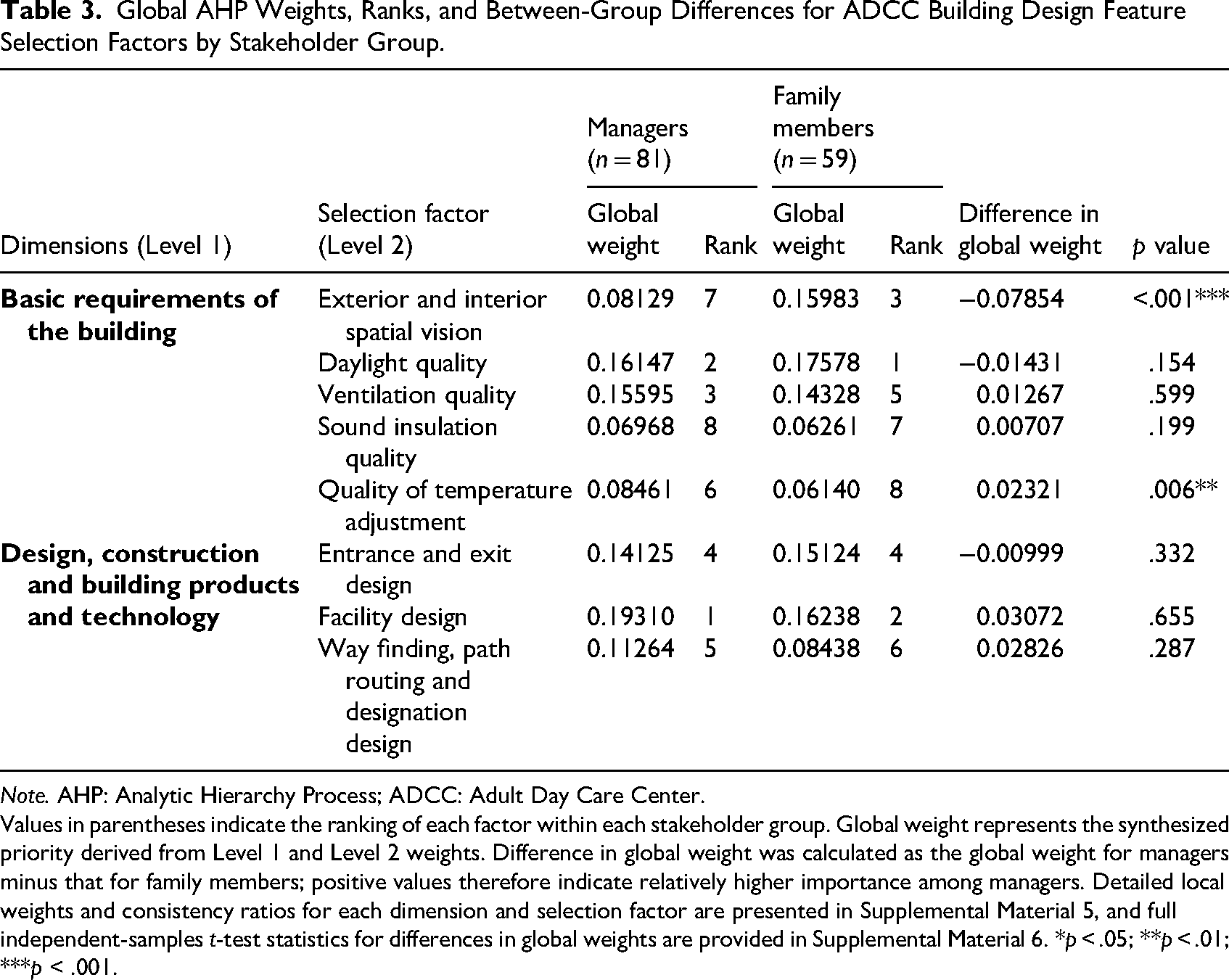
Note. AHP: Analytic Hierarchy Process; ADCC: Adult Day Care Center.
Values in parentheses indicate the ranking of each factor within each stakeholder group. Global weight represents the synthesized priority derived from Level 1 and Level 2 weights. Difference in global weight was calculated as the global weight for managers minus that for family members; positive values therefore indicate relatively higher importance among managers. Detailed local weights and consistency ratios for each dimension and selection factor are presented in Supplemental Material 5, and full independent-samples t-test statistics for differences in global weights are provided in Supplemental Material 6. *p < .05; **p < .01; ***p < .001.
Discussion
One major challenge in planning and designing ADCCs is that decisions are often driven by regulatory and financial considerations rather than by the priorities of those who use and operate these centers. Managers must balance limited resources and policy requirements, whereas family members focus more on safety, accessibility, and meaningful engagement for older adults with disabilities or dementia. In this study, approximately one-third of managers worked in publicly operated or publicly commissioned centers, whereas almost all family members used privately operated centers. These contextual differences may shape their experiences of resource constraints and service accessibility and, in turn, influence their priorities for site selection and building design. By explicitly comparing the priorities of these two stakeholder groups, our study provides empirical evidence to inform decisions about ADCC site selection and physical environment design so that they better reflect the needs of actual users.
By explicitly comparing the priorities of these two stakeholder groups, our study provides empirical evidence to inform decisions about ADCC site selection and physical environment design so that they better reflect the needs of actual users.
For site selection, both groups regarded health services, health systems, and health policies as a high-priority factor, but family members ranked it first whereas managers ranked it third. Managers tended to adopt a professional and policy-oriented perspective, emphasizing alignment with health and regulatory frameworks, whereas family members often expected additional user-oriented services such as rehabilitation and therefore placed stronger emphasis on this factor. The two groups also differed significantly in how they weighted transportation-related services, systems, and policies. Family members appeared to be more concerned with parking convenience and travel arrangements than with shuttle services, which service users seldom use. These findings align with Kurowski-Burt and Haddox (2017), who found that weak transportation networks limit access to health-promoting facilities for people with disabilities.
For building design features, managers and family members showed significant differences in importance assigned to exterior and interior spatial vision. Chaudhury and Xu (2022) reported that environmental familiarity, a homelike atmosphere, and the absence of oppressive spatial qualities are important for quality of life among residents in long-term care facilities. Our findings suggest that family members, in particular, are sensitive to these aspects when evaluating ADCC design features. Many participating ADCCs attempted to foster familiarity by incorporating homelike furnishings and nostalgic decorative elements into multipurpose spaces to support social participation and reminiscence among older adults (Figure 1A).
Participants in our study also considered the support and attitudes of local residents to be relatively important for site selection (ranked first by managers and fourth by family members), which likely reflects the frequent opposition to welfare facilities in Taiwanese communities. Local residents may petition against new ADCCs because of concerns about noise, environmental quality, or property values, thereby impeding efforts to integrate institutions into the neighborhood and limiting older adults’ access to services near their homes. Proactive communication strategies, such as informational meetings before service initiation, can help clarify the aims and functions of ADCCs and address misconceptions about potential negative impacts. In addition, some ADCCs have begun to adopt integrated service models and to increase interaction with community-dwelling older adults by collaborating with community health centers, senior clubs, and senior learning centers, thereby embedding health promotion and lifelong learning within the ADCC. Planning such integrated service roles at an early stage may, in turn, influence subsequent site and building design choices.
The attitudes of authorities were also viewed as important in site selection (ranked second by managers and third by family members). This reflects the influence of local government land-use planning, including designation of sites for elderly welfare institutions and policy support. For building design, facility design was rated highly (ranked first by managers and second by family members), probably because most Taiwanese ADCCs are retrofitted from other building types. When existing buildings already include accessible facilities and fire protection equipment, construction costs can be reduced. Because government agencies maintain safety inspection records, they are positioned to assist nongovernmental organizations in identifying suitable private sites or negotiating the use of public buildings for ADCC operations.
Daylight quality was another key building feature (ranked second by managers and first by family members). Prior research indicates that lighting and daylight can enhance mood and activity engagement among older adults in long-term care (Chaudhury & Xu, 2022), consistent with practical experience. However, in hot and humid climates such as Taiwan, solar exposure, especially between May and September, can cause overheating and glare, reducing thermal comfort and limiting the use of common spaces. Thus, building orientation, position relative to neighbors, and facade and shading design must be considered together to provide controllable daylight while protecting users from solar gain. Semi-outdoor transitional spaces, such as covered verandas or balconies, allow older adults to enjoy daylight and outdoor views without direct exposure to sunlight (Figure 1C). In contrast, participants rated temperature adjustment and sound insulation as less important, likely because air conditioning, shading, and acoustic treatments can be upgraded later, whereas decisions about window size, orientation, and external shading must be made earlier. Nonetheless, the potential for overheating underscores that thermal comfort and acoustic quality should be treated as integral components of the building envelope and facade design, especially when window areas are prioritized to maximize daylight.
Divergent views between health service providers and users are common, and shared decision-making (SDM) has been widely adopted to balance clinical evidence with patients’ needs and values. Elf et al. (2015) proposed applying a similar SDM process between professionals and users when planning and designing health-promoting facilities, in addition to providing evidence on architecture and medical treatment. Surveys of stakeholder views, such as those used in this study, can provide an overview of managers’ and family members’ priorities. Hence, SDM can help ensure that ADCCs are planned and designed in a manner that closely matches the expectations of managers, family members, and local residents who are likely to use or be affected by these facilities.
Strengths, Limitations, and Directions for Future Research
This study has several strengths. First, we captured the perspectives of two stakeholder groups, ADCC managers and service users’ family members, rather than focusing on either group alone. Second, we used the AHP to translate their qualitative preferences into quantitative weights, enabling comparisons of priorities for site selection and building design features. Third, by organizing the selection factors within an ICF-based framework (World Health Organization, 2001) and providing clear rankings, our findings can inform evidence-informed decisions by planners, architects, and policymakers regarding new or renovated ADCCs.
However, this study also has some limitations. First, it had a cross-sectional design. Although we identified the order and relative weights of the captured selection factors, we could not verify their effects on user satisfaction or health outcomes. Second, most of the questionnaires were administered in semiopen areas within ADCCs because private rooms were limited. Consequently, the possibility of being overheard may have discouraged some participants from providing critical responses and may have introduced social desirability bias. Third, because of the unmeasured differences in cultural background, organizational type, and regional context and because all participating ADCCs were located in Taiwan within a specific long-term care policy framework, our findings may not be generalizable to other settings. Fourth, all selection factors were predefined, and other relevant factors may have been overlooked. Finally, the two stakeholder groups were unequal in size, and the family member group was heterogeneous despite coresidency criteria. Because we did not stratify priorities by caregiver relationship, some within-group variation may not have been captured.
Future studies should examine whether ADCCs with strong political support, alignment with local community attitudes, and stakeholder-informed site and design decisions can achieve more favorable outcomes and higher satisfaction for service users, family caregivers, and staff. Mixed-methods and codesign studies involving managers, family members, frontline staff, service users, and local residents should further examine how SDM regarding the environments of ADCCs is implemented in practice and how such participatory processes influence acceptance, perceived fairness, and long-term use.
Conclusion
Managers of ADCCs and family members of service users tend to weight selection factors differently, particularly in domains related to support and attitudes and to health services, systems, and policies. By foregrounding the perspectives of stakeholder groups whose voices are rarely incorporated when health-promoting facilities are planned, this study offers guidance for selecting ADCC sites and building design features, especially in countries with social and policy contexts similar to those of Taiwan. Addressing these opinion gaps in planning and policy processes may facilitate the establishment and use of ADCCs and may help ensure that their physical environments better reflect the needs of those who use and operate them.
Implications for Practice
When selecting ADCC sites, planners and architects should prioritize access to nearby health services, reliable public or shuttle transportation, and neighborhood safety, as both managers and family members rated these as high-priority services–systems–policy factors.
In building design, architects and interior designers should ensure barrier-free circulation (e.g., level entrances, elevators, accessible toilets, and bathrooms), clear interior visibility, and simple, legible layouts so that staff can supervise users effectively and older adults with disabilities or dementia can navigate more safely and independently.
ADCC managers and health-care professionals can use these findings to advocate for sites and building features that directly support safety, accessibility, and meaningful social participation for older adults with disabilities or dementia.
When planning new centers or renovating existing ones, managers can involve family members and frontline staff in structured discussions (e.g., using simplified AHP-based ranking exercises) to make trade-offs explicit and cocreate a prioritized list of site and design requirements.
Clinicians and care teams can incorporate knowledge of local residents’ attitudes and community support into care planning and outreach strategies, helping to reduce stigma, improve acceptance of ADCCs, and encourage families to use these services earlier and more consistently.
Supplemental Material
sj-docx-1-her-10.1177_19375867261433021 - Supplemental material for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features
Supplemental material, sj-docx-1-her-10.1177_19375867261433021 for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features by Shwn-Jen Lee, Sheng-Wen Su and Hong-Ji Luo in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-2-her-10.1177_19375867261433021 - Supplemental material for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features
Supplemental material, sj-docx-2-her-10.1177_19375867261433021 for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features by Shwn-Jen Lee, Sheng-Wen Su and Hong-Ji Luo in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-3-her-10.1177_19375867261433021 - Supplemental material for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features
Supplemental material, sj-docx-3-her-10.1177_19375867261433021 for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features by Shwn-Jen Lee, Sheng-Wen Su and Hong-Ji Luo in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-4-her-10.1177_19375867261433021 - Supplemental material for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features
Supplemental material, sj-docx-4-her-10.1177_19375867261433021 for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features by Shwn-Jen Lee, Sheng-Wen Su and Hong-Ji Luo in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-5-her-10.1177_19375867261433021 - Supplemental material for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features
Supplemental material, sj-docx-5-her-10.1177_19375867261433021 for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features by Shwn-Jen Lee, Sheng-Wen Su and Hong-Ji Luo in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-docx-6-her-10.1177_19375867261433021 - Supplemental material for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features
Supplemental material, sj-docx-6-her-10.1177_19375867261433021 for Stakeholder Differences in Preferences for Adult Day Care Center Site and Building Design Features by Shwn-Jen Lee, Sheng-Wen Su and Hong-Ji Luo in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors are grateful to Mr. Shun-Chih Wang, Section Chief, General Planning Division, Architecture and Building Research Institute, Ministry of the Interior, Taiwan, for his support for the study. The authors would like to thank Wallace academic editing (![]() ) for their expertise in English language editing.
) for their expertise in English language editing.
Ethical Approval and Informed Consent Statements
The study protocol was reviewed and approved by the Institutional Review Board of National Yang-Ming University (now National Yang Ming Chiao Tung University) (IRB No. YM104067E). Written informed consent was obtained from all participants prior to study initiation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Architecture and Building Research Center, Ministry of the Interior, Taiwan funded a part of this study (grant number PG10202–0039). The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.