
Abstract
Objectives
This study was conducted to investigate the effect of light brightness on stress, anxiety, and psychological well-being during non-stress test (NST) measurements.
Background
Emotional and environmental factors that may cause stress and anxiety in pregnant women should be carefully evaluated and the necessary measures should be taken before and during the applications to pregnant women.
Methods
This research was conducted with 100 pregnant women as a randomized controlled experimental study. Data were collected using a personal information form, the psychological well-being questionnaire (PWQ), the perceived stress scale (PSS), and the state-trait anxiety inventory (STAI), which were administered before and after the NST measurement.
Results
There were significant intra-group differences between the mean pre-test (before NST) and post-test (after NST) scores of the pregnant women in the intervention group on the scales used in the study [PWQ pre-test (33.90 ± 9.18) and post-test (36.24 ± 7.83); PSS pre-test (32.26 ± 6.74) and post-test (27.0 ± 4.13); STAI pre-test (48.88 ± 4.04) and post-test (46.26 ± 3.97)] (p < 0.05). The difference between the mean pre-test (33.98 ± 9.11) and post-test (33.86 ± 9.04) PWQ scores of the pregnant women in the control group was insignificant. But there was a significant difference between the mean pre-test (32.08 ± 6.64) and post-test (33.0 ± 6.77) PSS scores of this group (p < 0.05).
Conclusions
The results of the study indicated that reducing ambient light brightness levels during NST measurements increased pregnant women's psychological well-being and reduced their stress and anxiety.
Introduction
Women experience numerous physiological and psychological changes throughout their lives (Shagana et al., 2018). Having a positive and healthy pregnancy, one of these processes, plays a vital role (Jha et al., 2021). Various methods are used to evaluate maternal and fetal health during pregnancy. The uncertainty about fetal health assessment methods and the results of these applications can lead to stress and anxiety in expectant mothers. Pregnancy itself is associated with heightened stress and anxiety responses, and these psychological changes may increase sensitivity to environmental stimuli (Pascal et al., 2023). The non-stress test (NST) is the most common method employed to assess fetal health in the prenatal period as it is easy to administer, non-invasive, and quickly interpretable (Hernandez Engelhart et al., 2023). A non-stress test is given to every pregnant woman who presents to the hospital for check-ups and who is at the ≥28th week of gestation. During NST, all pregnant women are exposed to disturbing levels of artificial light that produce excessive brightness and environmental pollution (Falchi et al., 2016; Leccese et al., 2016). Although NST is not an invasive and painful procedure, it may increase the level of anxiety as it lasts at least 20 min and the pregnant woman is exposed to light, sound, and strangers in the environment during the procedure (Dolker & Başar, 2019). These environmental and emotional stressors can elevate stress and anxiety, potentially influencing test outcomes and leading to inaccurate results (Vo et al., 2020). Therefore, emotional and environmental factors that may contribute to stress and anxiety in pregnant women should be carefully evaluated, and appropriate measures should be implemented before and during the procedure (Leccese et al., 2016; Güney et al., 2022).
Studies have shown that reduced light levels may have positive effects on physiological and emotional outcomes. For example, dim lighting has been reported to improve sleep quality (Wams et al., 2017), reduce negative emotional responses during labor (Silva & Shimo, 2017), and shorten the duration of labor (Maria et al., 2022). These findings suggest that light intensity may be associated with stress-related processes and may influence hormonal responses. However, studies directly examining the effects of light brightness on stress, anxiety, and psychological well-being in pregnant women during the non-stress test (NST) are limited. Given that NST is a commonly used assessment method that may cause stress and anxiety in pregnant women (Dolker & Başar, 2019), investigating the effects of environmental modifications such as light intensity during this procedure is of particular importance. Therefore, this study aimed to evaluate the effect of light brightness during NST on stress, anxiety, and psychological well-being in pregnant women.
Methods
Study Design
The research was conducted as a randomized controlled experimental trial and conducted in accordance with the CONSORT-SPI 2018 guidelines (Figure 1). The trial protocol was registered (NCT06504810).
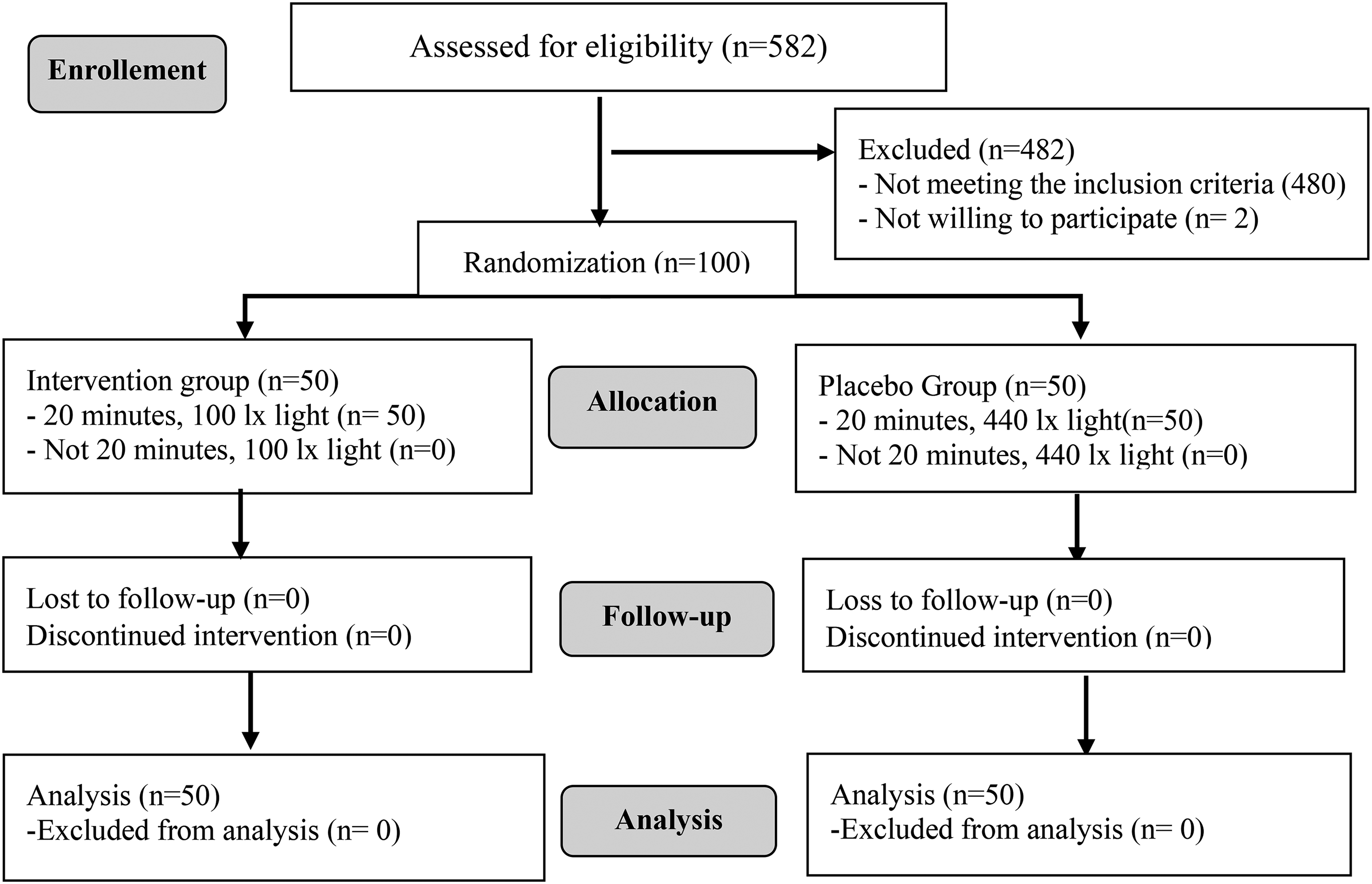
Figure showing the CONSORT flowchart.
Randomization
To avoid bias when assigning participants to the intervention and control groups, they were randomly assigned and concealed. An independent statistician followed the block randomization method to assign the pregnant women to the groups. For randomization of 100 mothers, ten combinations of the letters “A” and “B” (two blocks of equal size) were created. The intervention and control groups were determined by drawing lots for the letters A and B. For selection into groups or the random permuted block technique, random numbers generated on a computer were used. The randomization process was achieved by randomly assigning 10 combinations 10 times. Socio-demographic and descriptive characteristics of the mothers in the intervention and control groups were similar, and statistical analyses showed no significant difference between the groups (p > 0.05) (Table 1).
Comparison of Participants’ Control Variables Between Intervention and Control Groups.
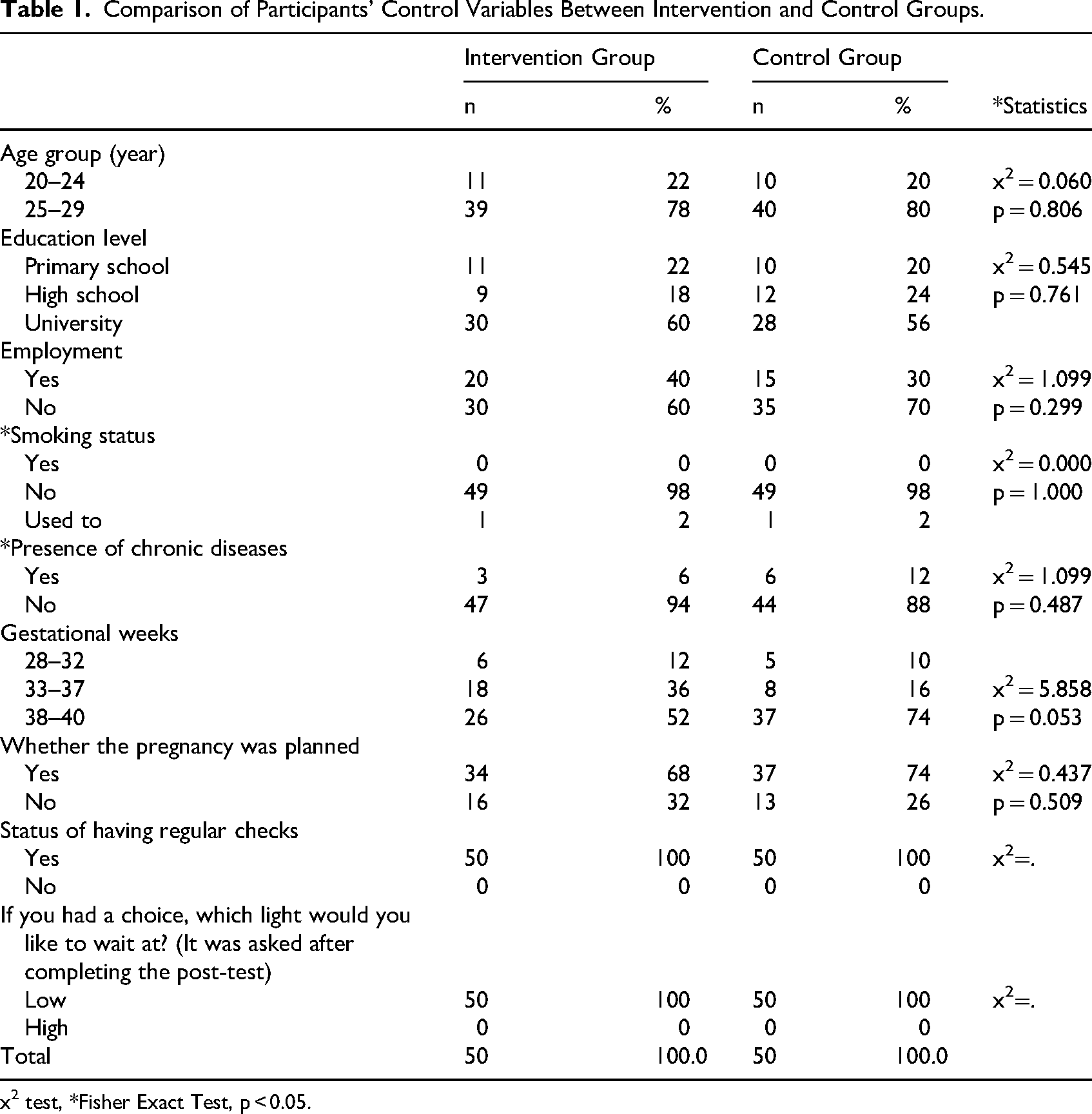
x2 test, *Fisher Exact Test, p < 0.05.
Blinding and Bias
In this study, blinded design was used for the assignment of participants to groups, analysis of data, and reporting of results. Since the participants were not informed about the group to which they were assigned, the study was conducted as a single-blind design. Participants were unaware of the room's brightness while performing the NST procedure. The pretest and posttest data were transferred to the computer by an independent person who knew nothing about the intervention and control groups. When the data were transferred to the computer, the intervention or control groups were not named, but codes “A” and “B” were used. The statistician who carried out randomization analyzed the data and prepared the report. To avoid statistical bias, the codes indicating the intervention and control groups were disclosed after the statistical analysis was done and the study report was prepared.
Population-Sample
Participants were pregnant women who presented to a state hospital in a province in Turkey for examination. The study was conducted in the NST room of this hospital between August 16, 2024 and October 20, 2024. The sample of the study was calculated as 94 participants (47 in the intervention and 47 in the control group) on the G*Power 3.1 software, based on a power value of 1-β=0.95, an error level of α=0.05, and an assumed effect size of f = 0.67 (Yağmur & Türkmen, 2017). However, considering possible dropouts during the study, the sample size was determined to be 50 participants for the experimental group and 50 for the control group. This was done to ensure that the analyses could be performed with sufficient power and to maintain the balance of randomization. The study was completed with 100 pregnant women, including 50 in the intervention and 50 in the control group (Figure 1).
Participants, Location, and Features of the Study
Participants were consisted of pregnant women who underwent NST in a state hospital in a province in Turkey. A midwife worked routinely in the NST room. There were no windows in the room. The room received no light from outside and was therefore illuminated only with dome lights. No directed or other types of lighting were used. The NST room was quiet and adequately heated.
Data Collection Tools
Personal Information Form: This form was prepared by the researchers in line with the literature. It has nine questions about pregnant women's sociodemographic (age, education status, employment status) and obstetric characteristics (gestational week, the pregnancy being planned) (Hernandez Engelhart et al., 2023; Dolker & Başar, 2019).
The Psychological Well-Being Questionnaire (PWQ): The PWQ was developed by Diener et al. (Diener et al., 2009) and its Turkish validity study was conducted by Telef (Telef, 2013). It has a total of eight items, which are scored between 1 and 7. High scores on the scale indicate psychological resilience. The internal consistency coefficient of the scale had been determined as 0.87 in the Turkish adaptation study. In this study, Cronbach's alpha value of the scale was found to be 0.846.
The Perceived Stress Scale (PSS/PSS-14): The PSS scale was developed by Cohen et al. (Cohen et al., 1983) and was adapted to Turkish by Eskin et al. (Cronbach's alpha: 0.84). It is used to evaluate the stress perceptions of individuals. High scores show high levels of perceived stress. The PSS has two sub-dimensions called “stress/discomfort perception” and “inadequate self-efficacy perception” (Eskin et al., 2013). The alpha value was found to be 0.833 in the current study.
The State-Trait Anxiety Inventory (STAI): This inventory was developed by Spielberger et al. Spielberger et al., 1971), and its Turkish validity and reliability study was conducted by Öner and Le Compte (Cronbach's alpha: between 0.83 and 0.92) (Öner & Le Compte, 1983; Öner, 1997). It has 20 items, which are scored on a four-point Likert-type scale. There are two types of statements on the scale: direct and reversed (Öner & Le Compte, 1983). The alpha value of the scale was found to be 0.848 in the current study.
Data Collection and Implementation of the Intervention
The researcher provided all participants with detailed information about the purpose of the study, the intervention process, and the participation requirements. Informed consent was obtained prior to the intervention from all pregnant women in the intervention and control groups who voluntarily agreed to participate in the study.
In the study, pretest data were collected after the pregnant women in the intervention group were informed about the research prior to the intervention. Following the pretest, participants were allowed to rest for 30 min under lighting conditions adjusted according to their respective groups. After the total 30-min period (comprising 20 min for NST measurement and 10 min for preparing the pregnant women before and after the procedure) the questionnaire was administered again and posttest data were collected.
Intervention Group
The same color temperature, bluish-cold white, was used in the intervention and control groups. Before the NST measurements were initiated, the pregnant women in the intervention group were informed about the procedure, and the necessary preparations were carried out by the researchers. A light brightness of 100lx was used in the intervention group. In the current study, the luminance of the lactation room was reduced to 100 lux based on previous studies (Canazei et al., 2022; Chen et al., 2021). The NST room was illuminated by a lampshade. After the pretest, the participants were first allowed to rest for 30 min under lighting adjusted to 100 lx. Subsequently, an NST was performed on the participant under the same light intensity. The intervention, the preliminary preparation of the pregnant woman, the briefing, and the NST measurement took an average of 30 min. After the NST procedure was completed, the posttest was administered to the participants. After the intervention was completed and the posttest was run, two light brightness, 100 lx and 440 lx, were shown to the mothers, and they were asked which light they would prefer for room lighting if they had a choice. Before and during the study, an experienced electrical engineer in the field of electrical systems for the hospital was consulted to adjust the light color temperature and brightness. The room's light brightness was monitored by measuring it every 10 min with a light meter.
Control Group
Before the NST measurements were initiated, the pregnant women in the control group were informed about the procedure, and the necessary preparations were carried out by the researchers. A light brightness of 440 lx was used in the control group. In the current study, the luminance of the lactation room was 440 lux based on previous studies (Canazei et al., 2022; Chen et al., 2021). The NST room was illuminated by a lampshade. After the pretest, the participants were first allowed to rest for 30 min under lighting adjusted to 440 lx. Subsequently, an NST was performed on the participant under the same light intensity. The intervention, the preliminary preparation of the pregnant woman, the briefing, and the NST measurement took an average of 30 min. After the NST procedure was completed, the posttest was administered to the participants. After the intervention was completed and the posttest was run, two light brightness, 100 lx and 440 lx, were shown to the mothers, and they were asked which light they would prefer for room lighting if they had a choice. Before and during the study, an experienced electrical engineer in the field of electrical systems for the hospital was consulted to adjust the light color temperature and brightness. The room's light brightness was monitored by measuring it every 10 min with a light meter.
Data Analysis
The data were analyzed on SPSS 24.0 software. The chi-square test was employed to compare the control variables of the intervention and control groups. The normality of the data was evaluated with the Kolmogorov-Smirnov test, and it was determined that the data showed a normal distribution (Tabachnick & Fidell, 2013). A dependent groups t-test was performed to compare mean pre-test and post-test scale scores, and an independent groups t-test was done to compare the mean scale scores of the participants in the intervention and control groups. Cronbach's alpha value was calculated to evaluate the internal consistency of the scales. The significance level was determined as p < 0.05.
Ethical Considerations
The approval of the Osmaniye Korkut Ata University Health Sciences Research Ethics Committee was obtained to conduct the research (Ethics Committee Date: 10.07.2024, No: E.185316). Institutional permission was obtained from the Provincial Health Directorate of the province where the study would be conducted. The questionnaire did not include any items about participants’ identity, and participation in the study was voluntary. After the pregnant women who agreed to participate in the study were informed about the purpose and content of the research, their verbal and written consent was obtained.
Results
It was determined that 78% of the pregnant women in the intervention group were aged between 25 and 29, 60% were university graduates, 60% were unemployed, 98% were non-smokers, and 94% did not have a chronic disease. In addition, 52% were in their 38th to 40th weeks of gestation, 68% had a planned pregnancy, 100% had regular pregnancy check-ups, and 100% preferred a low light brightness during the NST measurement.
Eighty percent of the pregnant women in the control group were between the ages of 25 and 29, 56% were university graduates, 70% were unemployed, 98% were non-smokers, and 88% did not have a chronic disease. Additionally, 74% were in their 38th to 40th weeks of gestation, 74% had a planned pregnancy, 100% had regular pregnancy check-ups, and 100% preferred a low light brightness during the NST measurement.
No statistically significant difference was found between the intervention and control groups in terms of education level, age, employment status, smoking, presence of chronic diseases, gestational week, having a planned pregnancy, and having regular check-ups during pregnancy (p˃0.05) (Table 1).
The intra-group comparison of the mean pre-test and post-test scores of the women in the intervention group on the scales indicated that there was a decrease in post-test scores [PWQ pre-test (33.90 ± 9.18) and post-test (36.24 ± 7.83); PSS pre-test (32.26 ± 6.74) and post-test (27.0 ± 4.13); and STAI pre-test (48.88 ± 4.04) and post-test (46.26 ± 3.97)], with the difference between the two means being statistically significant (p < 0.05) (Table 2).
Within-Group Comparison of the Intervention and Control Groups from the Mean Scores of Pre-Test and Post-Test Applications of PWQ, PSS, and STAI (n = 100).
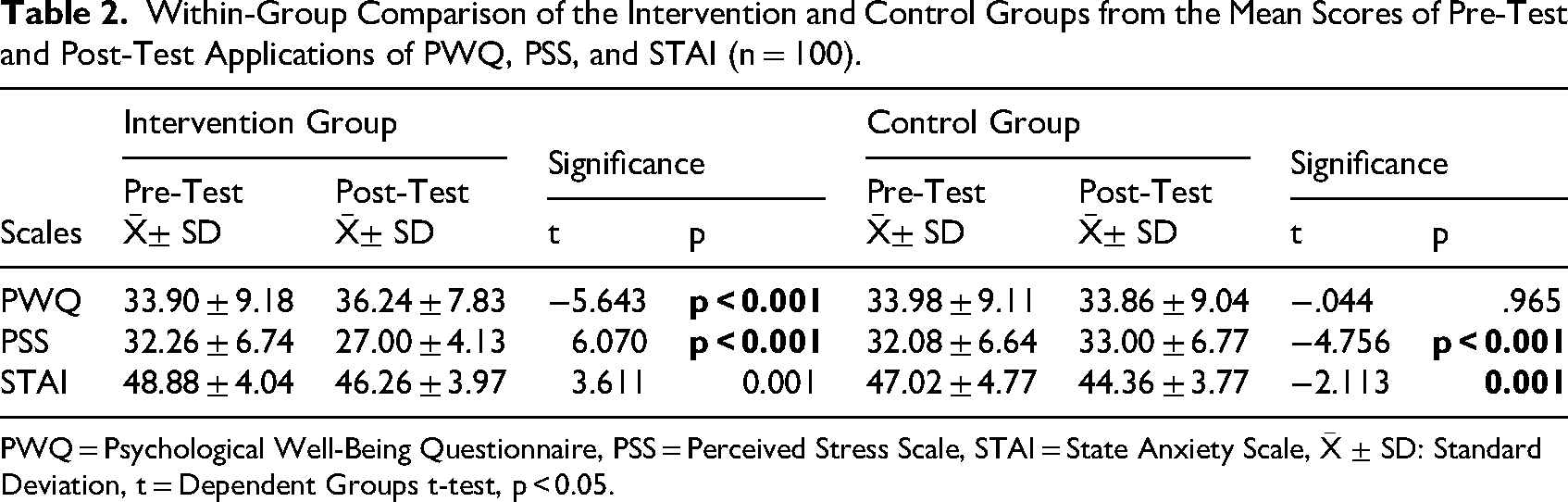
PWQ = Psychological Well-Being Questionnaire, PSS = Perceived Stress Scale, STAI = State Anxiety Scale,
According to the control group comparison of the mean pre-test (33.98 ± 9.11) and post-test (33.86 ± 9.04) PWQ scores of the women in the control group, the difference between the scores was not statistically significant (p > 0.05). The comparison of the mean pre-test (32.08 ± 6.64) and post-test (33.0 ± 6.77) PSS scores of the women in the control group indicated an increase in the post-test score, and the difference between the two scores was statistically significant (p < 0.05). Also, the mean scores of the pregnant women in the control group on the STAI pre-test (47.02 ± 4.77) and post-test (44.36 ± 3.77) were compared, and it was determined that the mean post-test scores decreased and that the difference between the two means was statistically significant (p < 0.05) (Table 2).
The difference between the mean pre-test PWQ scores of the pregnant women in the intervention and control groups was not statistically significant (p˃0.05). The comparison of the mean post-test scores on the same scale showed that the score of the intervention group increased, but that the difference between them was not statistically significant (p > 0.05). The difference between the mean pre-test PSS scores of the pregnant women in the intervention and control groups was not statistically significant (p˃0.05). When the mean post-test scores were compared, it was found that the score of the intervention group decreased and that the difference between them was statistically significant (p < 0.05). The difference between the mean pre-test STAI scores of the pregnant women in the intervention and control groups was not statistically significant (p˃0.05). The comparison of the mean post-test scores showed a decrease in the mean post-test score of the intervention group, with the difference between the two means being statistically significant (p < 0.05) (Table 3).
Comparison of the Mean Pre-Test and Post-Test Scores of the Women in the Intervention and Control Groups on the PWQ, PSS, and STAI Scales Between (Between Group Comparison) (n = 100).
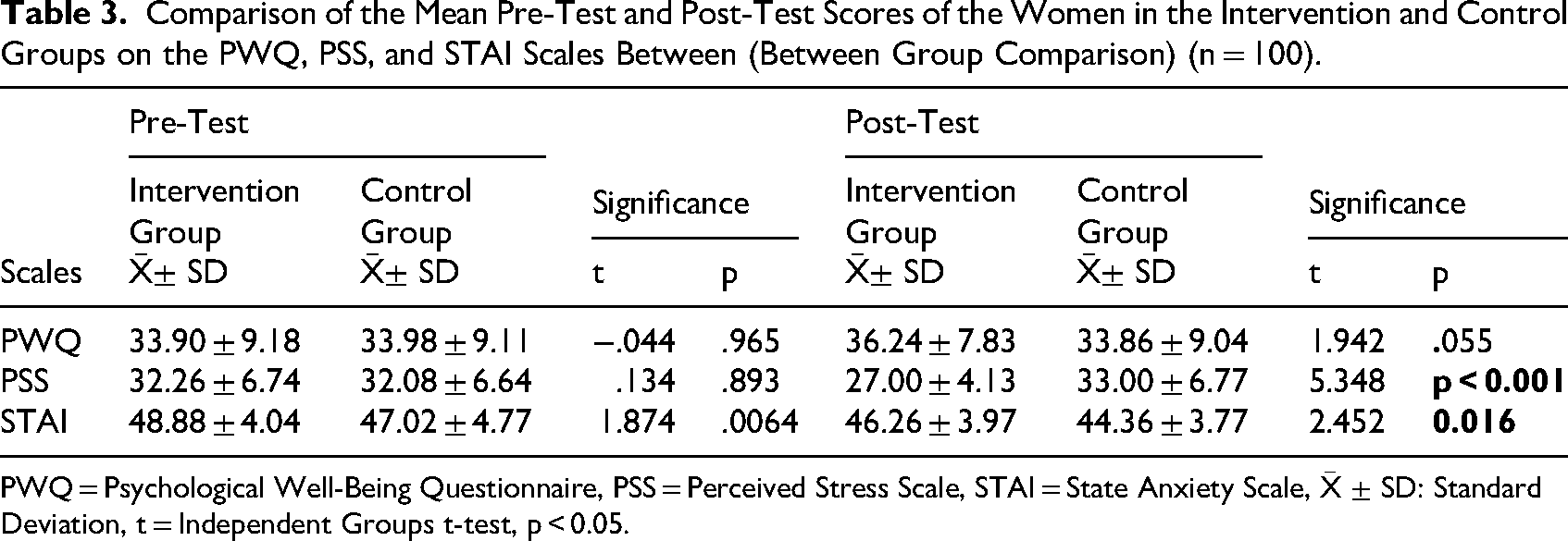
PWQ = Psychological Well-Being Questionnaire, PSS = Perceived Stress Scale, STAI = State Anxiety Scale,
It was determined that the difference between the mean pre- and post-intervention systolic blood pressure, pulse, respiration, and fetal heart movement scores of the pregnant women in the intervention and control groups was not statistically significant (p > 0.005). The mean diastolic blood pressure score of the pregnant women in the control group increased following NST and the difference between this score and the mean post-NST diastolic blood pressure score of the pregnant women in the intervention group was significant (p < 0.005) (Table 4).
Evaluation of Pre- and Post-NST Vital Signs.
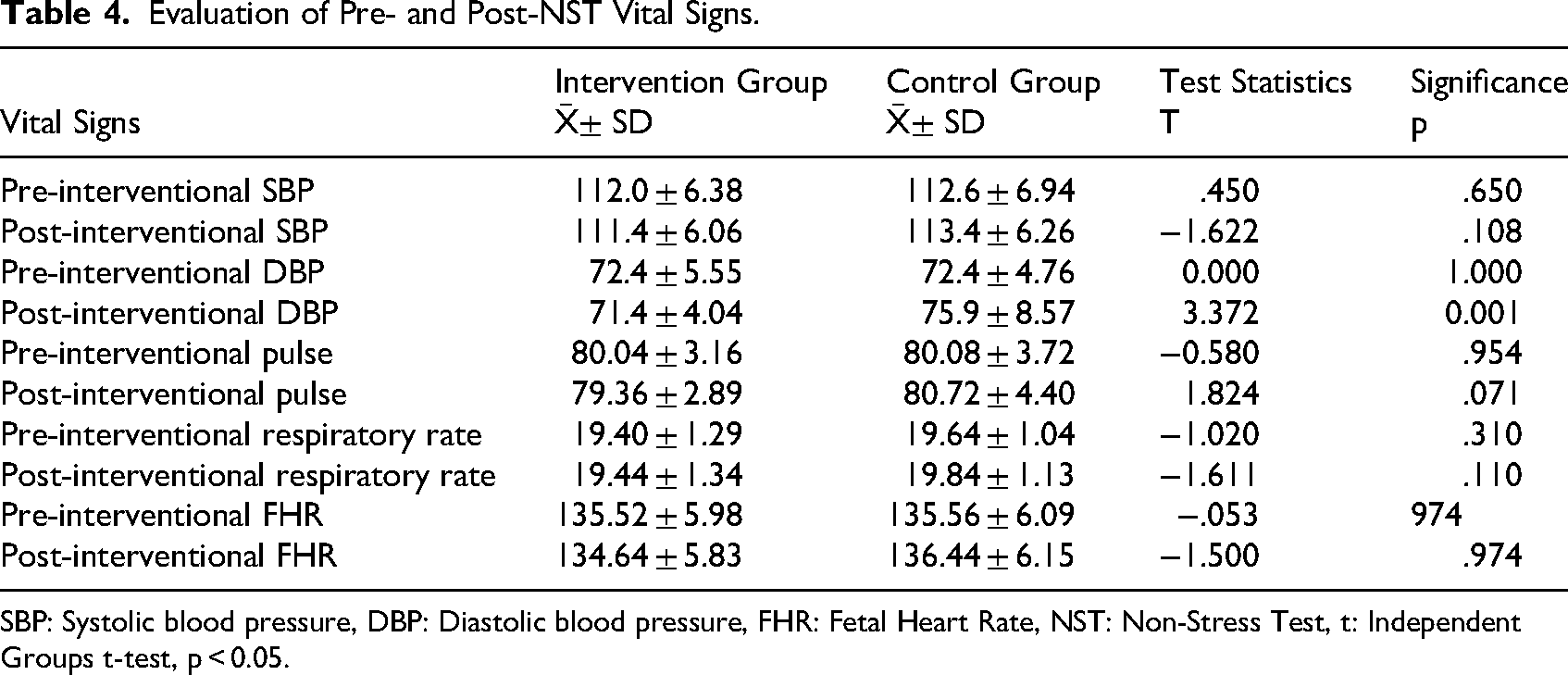
SBP: Systolic blood pressure, DBP: Diastolic blood pressure, FHR: Fetal Heart Rate, NST: Non-Stress Test, t: Independent Groups t-test, p < 0.05.
Discussion
This study examined the effect of light intensity during the non-stress test (NST) on stress, anxiety, and psychological well-being in pregnant women. Given the limited number of studies directly addressing the impact of environmental lighting during NST, the findings were interpreted within the context of related clinical and experimental literature.
In the present study, pregnant women in the intervention group who were exposed to dim lighting during NST demonstrated a significant reduction in stress and anxiety levels and a significant increase in psychological well-being following the procedure. These findings are consistent with previous studies suggesting that reduced light intensity may have beneficial effects on emotional and physiological responses. Silva and Shimo (2017) reported that women exposed to dim lighting during labor experienced fewer negative emotional responses, such as fear and discomfort. Similarly, Maria et al. (2022) showed that the application of dim lighting during the first stage of labor shortened the duration of labor. Considering that a shorter labor duration may contribute to reduced stress and improved hormonal regulation, these findings support the results of the present study. Research in the fields of sleep and neurophysiology also aligns with these findings. Wams et al. (2017) found that individuals exposed to lower light levels before sleep experienced fewer nocturnal awakenings and improved REM sleep, while Canazei et al. (2022) demonstrated that lower illuminance levels facilitated sleep onset and promoted more restful sleep. Although these studies were not conducted in pregnant populations, they support the notion that light intensity can influence neuroendocrine processes associated with stress and emotional regulation.
The physiological mechanisms underlying these effects are thought to be related to the stimulation of the neocortex and the activation of stress-related hormonal pathways by bright light exposure. Bright light has been shown to stimulate the sympathetic nervous system, increasing the secretion of stress hormones such as adrenaline, whereas dim lighting may promote parasympathetic activity and contribute to a calmer emotional state (Nakada et al., 2023). This mechanism may explain the reductions in stress and anxiety and the improvement in psychological well-being observed among pregnant women exposed to dim lighting in the present study. Furthermore, pregnancy itself is associated with heightened stress and anxiety responses, which may enhance sensitivity to environmental stimuli such as light, noise, and procedural factors (Pascal et al., 2023; Öztaş & Taş, 2025).
In contrast, an increase in stress and anxiety levels was observed in the control group during the NST procedure. Although NST is not an invasive or painful intervention, its duration and pregnant women's exposure to environmental stimuli such as bright light, sound, and unfamiliar individuals may contribute to increased anxiety (Dolker & Başar, 2019). Moreover, excessive artificial light exposure has been reported to intensify stress responses (Falchi et al., 2016; Leccese et al., 2016). Therefore, the increase in stress and anxiety observed in the control group is consistent with existing literature.
When physiological parameters were evaluated, no significant differences were observed between the intervention and control groups in maternal vital signs or fetal heart rate, with the exception of diastolic blood pressure. The post-NST increase in diastolic blood pressure observed in the control group may be attributed to enhanced sympathetic activation and stress responses induced by bright light exposure. Similar associations between light exposure, stress, and cardiovascular responses have been reported in previous studies (Nakada et al., 2023; Sunwoo et al., 2017). The absence of adverse effects on fetal heart rate suggests that dim lighting during NST represents a safe environmental modification. Although fetal outcomes were not the focus of this study, it is possible that maternal responses to light may indirectly influence fetal health, which could be explored in future research.
In conclusion, the findings of this study are consistent with existing literature indicating that light intensity influences emotional and physiological responses. Reducing light brightness during NST was associated with decreased stress and anxiety and improved psychological well-being in pregnant women, highlighting the importance of creating more mother-friendly NST environments.
The strength of the current study was that it was a randomized, placebo-controlled intervention study, the sample size was calculated using a power analysis, and valid and standard measurement tools were employed to collect data. The effect of different levels of light brightness on pregnant women's stress and anxiety was determined in the present study; therefore, the light brightness of the NST room can be adjusted to reduce their stress and anxiety levels. In addition, reducing the light brightness will both relieve the pregnant woman in terms of stress and anxiety and make a positive contribution to hospitals in terms of cost and energy savings.
The Limitations of the Study
The study has several limitations. The study results were limited to pregnant women. The data were based on pregnant women's self-reports, which constituted another limitation of the study. In addition, the short-term effect of light brightness was evaluated, but long-term effects were not examined in this study. Another limitation of the study is that individual differences in stress reactivity and psychological vulnerability were not assessed, so some women's responses during the NST may have differed, representing a potential source of bias.
Conclusion
In the present study, it was found that reducing the light intensity during the non-stress test enhanced pregnant women's psychological well-being while decreasing their stress and anxiety levels. Understanding how varying light brightness levels influence stress and anxiety in pregnant women can facilitate the adjustment of room lighting during the NST to alleviate these negative effects. Moreover, lowering light intensity may offer hospitals additional benefits by reducing costs and energy consumption. This approach could contribute to the identification and standardization of cost-effective lighting strategies aimed at supporting the mental health of pregnant women.
Understanding how varying light brightness levels influence stress and anxiety in pregnant women can facilitate the adjustment of room lighting during the NST to alleviate these negative effects.
Implications for Practice
Reducing light brightness during non-stress testing may be a simple, non-invasive strategy for improving the psychological well-being of pregnant women.
Healthcare professionals may consider adjusting ambient lighting in NST rooms to create a calmer environment.
Lower-brightness lighting can also help healthcare facilities minimize energy consumption and costs.
Standardizing lighting conditions during prenatal procedures may positively support maternal health.
Footnotes
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Osmaniye Korkut AtaUniversity (Ethics Committee Date: 10.07.2024, Number: E.185316).
Consent to Participate
People who accepted to participate in the study were informed about the study, and their written consent was obtained prior to the study
Consent for Publication
The researchers gave permission for the study to be published.
Author Contributions
E.Y. and F.P. conceptualized the study and supervised. E.Y. collected the data. E.Y. and F.P. analyzed the data. All authors prepared the manuscript and reviewed and provided approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing and Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.