
Abstract
Objective
The study aimed to examine empirical studies published between 2003 and 2025 to identify elements of physical environments influencing health outcomes and experiences of children and families.
Background
In the past 40 years, research has shown that the physical environment influences the health and well-being of patients in the healthcare environment. However, similar research in the context of “pediatric inpatient wards” remains underexplored.
Methods
PubMed, Embase, Scopus, and Web of Science were used to identify relevant articles. All extracted articles underwent a three-step screening process using PRISMA. A total of 30 eligible articles were used for the analysis. The protocol is registered at PROSPERO (CRD42023408997).
Results
Key findings reveal positive and negative impacts of identified elements. Positive-effect elements include play spaces, space for parents, natural light, connections with nature, and so on, which promote comfort, healing, and emotional resilience. Conversely, negative-effect elements, such as noise, artificial lighting, uncomfortable temperature, and so on, contribute to stress and disrupted sleep. Mixed effects were observed for elements like art and television, which underscore the complexity of designing environments that address the diverse needs of different age groups and genders.
Conclusions
The review findings highlight significant knowledge gaps. The study also tries to bridge existing gaps between research and practice by systematically identifying environmental elements, offering actionable insights to architects, designers, healthcare providers, and policymakers. Future research must adopt rigorous, culturally inclusive approaches to advance the field of pediatric healthcare design and ensure equitable care across diverse sociocultural contexts.
Keywords
Introduction
The role of physical environment in the healing and restorative effects on patients within healthcare settings has emerged as an important factor among healthcare providers, architects, and environmental psychologists (Devlin & Arneill, 2003; Gao & Zhang, 2020; Ulrich, 2001; Ulrich et al., 2008; Verderber et al., 2021). The concept of “evidence-based design,” introduced by Roger Ulrich in 1984, marked a transformative moment in healthcare architecture (Sal Moslehian et al., 2020). Ulrich's experiment demonstrated that the view of nature through windows significantly improved patients’ recovery from surgery (cholecystectomy)—sparking interest in how the physical environment affects patients’ well-being (Ulrich, 1984). Renewed interest in the “evidence-based healthcare design” has resulted in a significant body of research documenting the physical environment and its impact on the patient's health and well-being (Halawa et al., 2020; Phiri, 2014; Rashid, 2013; Ulrich et al., 2008; Van Hoof et al., 2015). While empirical studies have explored the role of physical environments in general healthcare settings, the unique needs of pediatric patients and their families have only gathered attention in recent years (Pasha & Shepley, 2013; Peditto et al., 2020).
Empirical studies have explored the role of physical environments in general healthcare settings, the unique needs of pediatric patients and their families have only gathered attention in recent years.
In 1987, the first book on the design of healthcare facilities, especially for children, was published by Olds and Daniel (1987) named “Child health care facilities: Design guidelines—Literature outline.” Before that, very little information was available on healthcare design for children—architects and designers were dependent on journal photo essays for reference (Shepley, 2001). In 1998, Shepley and colleagues conducted a literature review, from mid-1987 to mid-1997, to identify publications that could support the development of design guidelines on healthcare environments for children and their families, and also to uncover the relationship between healthcare environment and children (Shepley et al., 1998). A total of 59 articles were identified for the review, in which most were contextualized in “neonatal intensive-care units” and very few on “pediatric inpatient wards” (Shepley, 2001; Shepley et al., 1998).
Every year, millions of children visit inpatient wards in hospitals to receive care (Campbell et al., 2008; Nayak et al., 2026; Reid & Fang, 2022). Inpatient wards are designated areas within hospitals where patients remain for at least one night to receive medical care, which includes intensive monitoring, evaluation, and various diagnostic tests and procedures (Gao & Zhang, 2020). Admissions to these wards typically occur through the emergency or outpatient department (Newnham et al., 2012; Zhang et al., 2014). One of the common challenges faced by hospitals in many countries is “prolonged hospital length of stays in inpatient wards,” which not only increases the healthcare cost for patients but also decreases patient satisfaction levels (Gao & Zhang, 2020; Sahiledengle et al., 2020). Especially in the case of the pediatric population (children), prolonged hospitalization significantly increases stress and elevates anxiety levels (Mîndru et al., 2016). Therefore, this study aims to systematically review and analyze existing research on the impact of the physical environment of pediatric inpatient wards on children and their families, by addressing the research question—how does the physical environment of pediatric inpatient wards affect children and their families?
Methods
In this review, a systematic literature search was carried out to investigate the empirical evidence on the effects of physical environment on children and their families in pediatric inpatient wards, using the PRISMA (Preferred Reporting Items for Systematic reviews and Meta Analyses) checklist (Page et al., 2021) and Cochrane Handbook for Systematic Reviews of Interventions (Chandler et al., 2019). Before starting the literature synthesis process, the research team registered the study protocol with the International Prospective Register of Systematic Reviews (PROSPERO) at crd.york.ac.uk/prospero on April 12, 2023, registration number CRD42023408997.
Search Strategy
Following the PRISMA checklist, the review team developed the strategy to identify articles with the defined eligibility criteria. Articles reporting on original works published in the English language since 2003 were eligible for the review. An initial search was performed on June 19, 2023, with a revised search on December 10, 2025. As the review focused on determining the relationship between physical environment and health outcomes, the PEO (Population/Patient, Exposure/Environment, Outcome) framework was used to define inclusive and exclusive criteria (Hosseini et al., 2024), as shown in Supplemental Appendix 1. The eligibility criteria were set by all authors.
Using the four selected databases (PubMed, Embase, Scopus, and Web of Science), the team ran several iterations of “search terms” to attune the search strategy for each database according to its interface, aiming to identify relevant articles as per the set eligibility criteria. The search was performed in PubMed using “Title/Abstract”; Embase—“Title + Abstract”; Web of Science—“Topic”; and in Scopus—“Article title + Abstract + Keywords.” The final “search terms” were specified in Supplemental Appendix 2. The team had used the Population–Exposure (P–E) model of the PEO framework to define the search terms. The rationale was that some or all outcome measures might not be mentioned in titles and abstracts, which would reduce the identification of key articles (Eriksen & Frandsen, 2018; Tsafnat et al., 2018).
Population of interest was defined by using terms related to children and adolescents—as well as—their parents, families, and caregivers. The inpatient wards, physical environment, and terms associated with them served as the exposure (see Supplemental Appendix 2).
Study Selection
Studies were selected in two phases. In the first phase, an initial search was conducted on June 19, 2023. Using the mentioned search strategy, the initial search resulted in the collection of a total of 3,483 articles (603 in PubMed, 983 in Embase, 462 in Web of Science, and 1,435 in Scopus). All extracted articles were then stored in EndNote 20.6 software (Gotschall, 2021) by one reviewer, and then duplicates were removed, resulting in 2,001 unique articles. After that, study selection went through a three-step screening process.
The first screening process was the retrieval of articles. If the articles were published before 2003 (year), not in English, not in full text, and not peer-reviewed/original research—then they were excluded (n = 709), and the remaining articles (n = 1,292) were proceeded to the second screening process.
The second screening process was based on titles and abstracts. Using the mentioned exclusion criteria, the set of remaining unique articles were divided into six categories based on consensus between two individual reviewers—applicable for full-text review (n = 25), study does not address Population/Patient (n = 41), study does not address Exposure/Environment (E1) (n = 44), study does not address Exposure/Environment (E2) (n = 107), literature review (n = 27), and other off subjects’ research/not related to topic (n = 1,048). If the inclusion of the article was not clear through its “title” and “abstract,” then the study was moved to the next screening step. Disagreements were resolved by a third reviewer/methodologist (an expert in the systematic literature reviews).
The third screening process was on full texts. At this stage, full texts of 25 articles were independently assessed by two individual reviewers. After a thorough assessment, 13 articles were excluded (see Figure 1 for detailed exclusion reasons). Simultaneously, reference-snowballing/citation searching had been performed for all 25 articles (applicable for the full-text review) by two individual reviewers—initially using the title and abstract of each reference; if not clear with the title/abstract, full texts of the remaining were screened to check their eligibility. As a result, 16 articles were added to the eligible articles’ list with consensus of all the reviewers (see Figure 1).
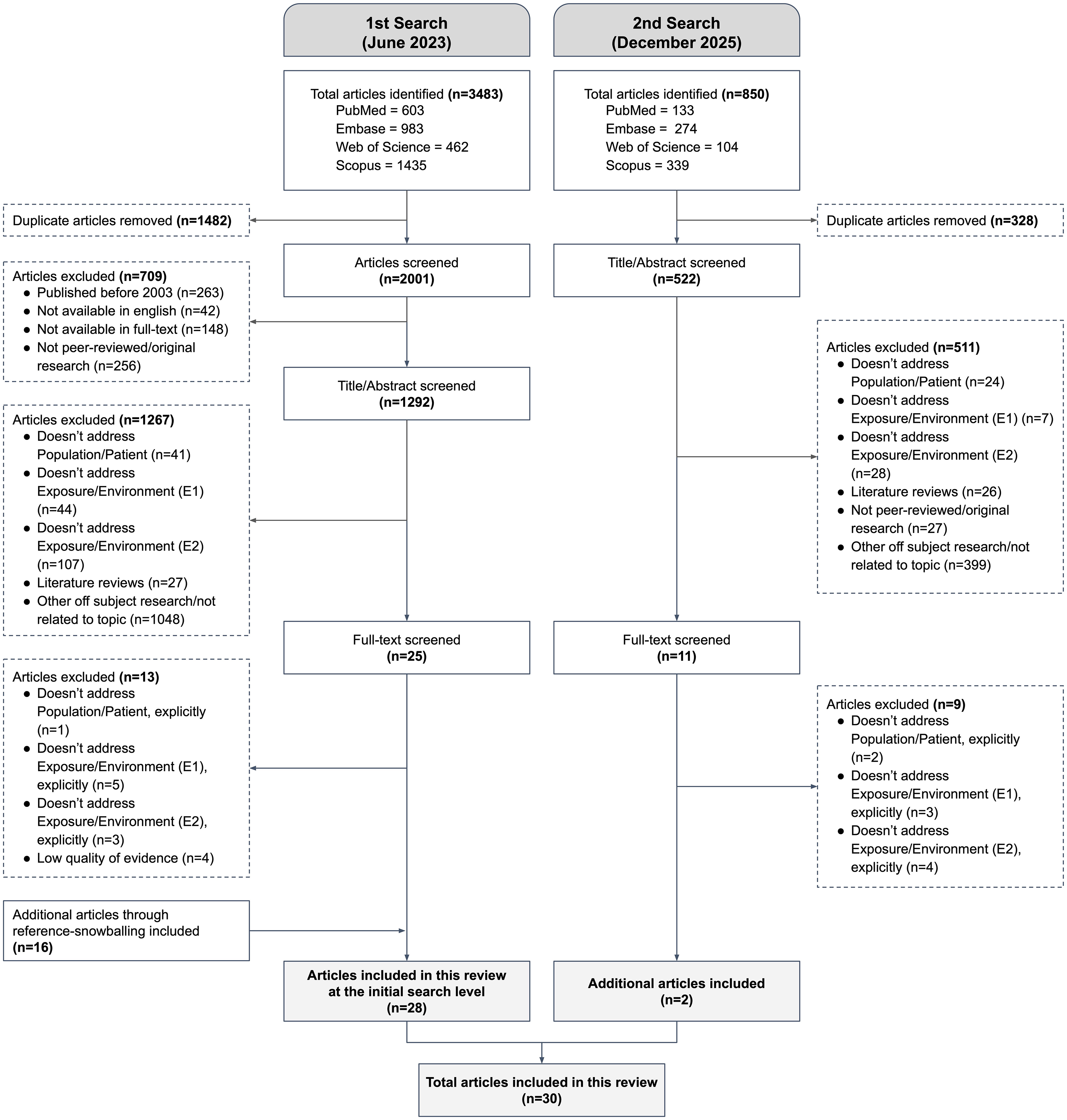
PRISMA Flow Diagram used in this Systematic Review. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta Analyses.
In the second phase, searches were revised on December 10, 2025 using the same databases and screening processes. Additionally, two articles were included at this stage with the consensus of all the reviewers (see Figure 1 for the detailed synthesis process). Finally, a total of 30 articles were eligible for analysis.
Data Extraction
Total eligible articles (n = 30) were used for analysis. A spreadsheet was created by one reviewer to extract data from each included study, later reviewed and cross-checked by other reviewers. Information related to—article information (title, year of publication, name of journal, first author), study context (country of first author, setting), participants (sample type, sample size, sample age), research details (research design, primary methods used, aim/research questions), and outcomes were extracted (see Supplemental Appendix 4). Simultaneously, two independent reviewers evaluated each article's methodological quality and risk of bias. Each study was assigned to a level of evidence (1 to 6) using the Levels of Evidence for Healthcare Design model (Stichler, 2010; see also Gripko et al., 2023; Marquardt et al., 2014), and quality was assessed using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). The team discussed any discrepancies in assessment until reaching a consensus; a third and/or fourth reviewer acted as a tie-breaker when needed.
Data Synthesis
The review team created a data synthesis spreadsheet to analyze content-based relationships between the physical environment of inpatient wards and the experiences of children and their parents. To address the primary research question, the eligible articles were analyzed by categorical variables (age group and medical condition of patients) and contextual variables (environmental elements/space and its impact). Later, the coding strategy (Gibbs, 2018) was used to find outcomes, as shown in Supplemental Appendix 3. In particular, the reported impacts were classified as either positive, negative, mixed, or no effect. The analysis aimed to provide preliminary insights into the findings rather than establishing a definitive conclusion.
Results
In total, 30 articles were included in the analysis. Across all selected studies, 29 (96.7%) were focused inside the inpatient wards, while 1 (3.3%) was focused on patients’ passive garden use through windows of the inpatient ward. User samples in all studies were mostly children aged 3–18 years—in some cases adolescents until 21 years (Meltzer et al., 2012)—with varying medical conditions. All the selected articles were organized as per their study type and relative quality using the MMAT and Levels of Evidence for Healthcare Design in Figure 2.
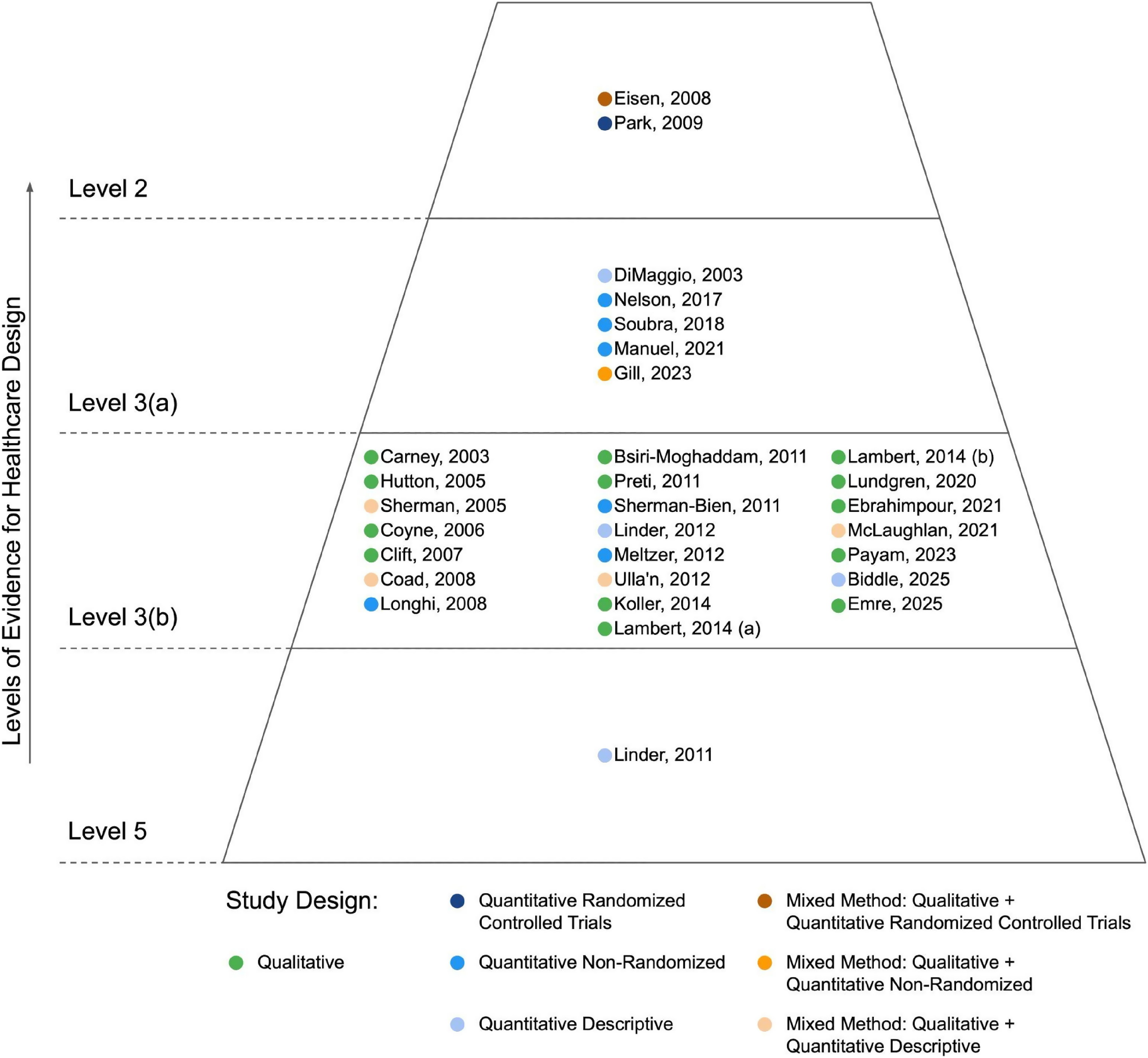
Study Types and their Relative Quality Using MMAT and Levels of Evidence for Healthcare Design. MMAT = Mixed Methods Appraisal Tool.
According to the Levels of Evidence for Healthcare Design model (Stichler, 2010; see also Gripko et al., 2023; Marquardt et al., 2014), the majority of the selected articles were classified as Level-3(b) (73.333%), then as Level-3(a) (16.667%), a minority were under Level-2 (6.667%) and Level-5 (3.333%). Since literature reviews and professional standards/guidelines were excluded from the eligibility criteria of this review, therefore no study was classified as Level-1 and Level-4. As per the MMAT (Hong et al., 2018), a large number of the articles used qualitative methods (43.3%, n = 13), followed by quantitative methods (n = 11) and mixed methods (n = 6). Figure 3 shows the assessment of methodological quality of the articles included in this review.
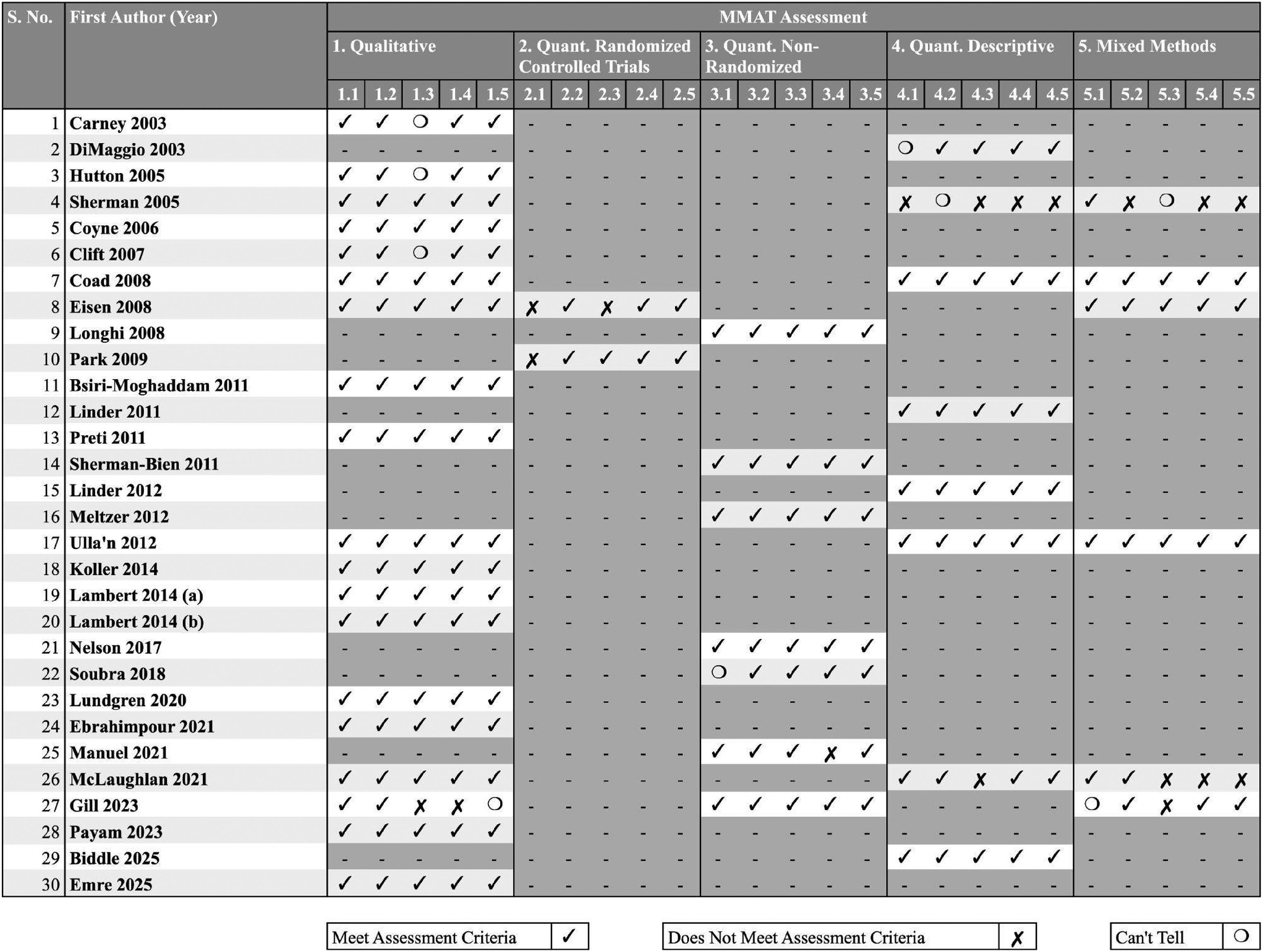
MMAT Assessment of all the Selected Articles. MMAT = Mixed Methods Appraisal Tool.
Three studies (Gill et al., 2023; McLaughlan & Willis, 2021; Sherman et al., 2005) rated low in the MMAT assessment, but they were not excluded due to recommendations outlined in the MMAT user guide (Hong et al., 2018). Although MMAT discourages converting rating into an overall score, multiple categories marked as “can't tell” or “does not meet assessment criteria” suggest poor methodological quality. Despite the lack of explicit responses to the screening questions, the content of these articles suggested that these studies were empirical and thus eligible for data synthesis.
Thematic analysis of all the selected articles identifies 23 categories which closely align with the “built environment design variable” defined by Ulrich et al. (2010). All contextual variables (environmental element/space and its impact) can be seen in Figure 4, which summarizes the data extraction findings and explains the effect of these elements on children, as per the defined codes.
Thematic analysis of all the selected articles identifies twenty-three categories which closely align with the ‘built environment design variable’ defined by Ulrich.
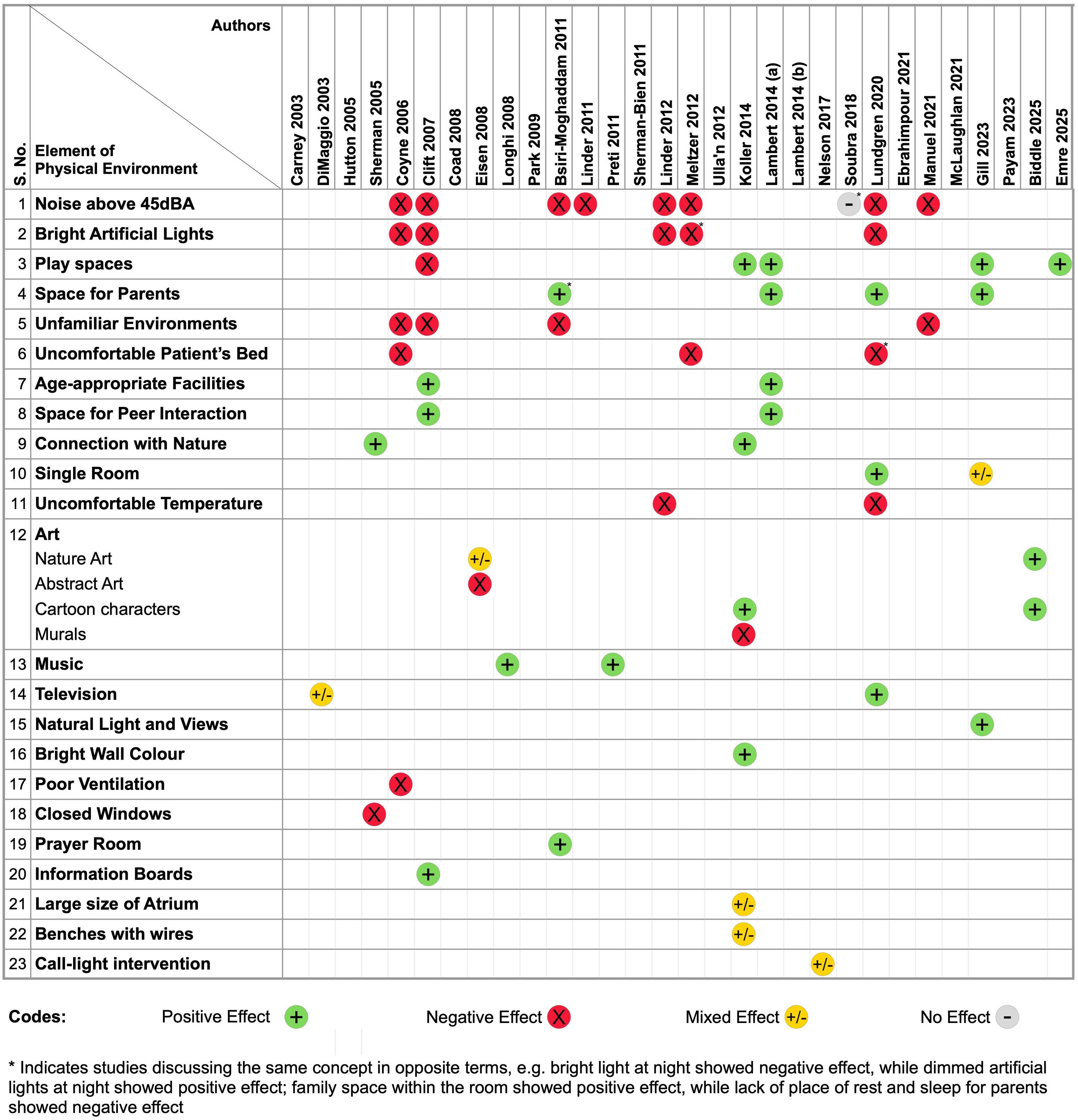
Impact of the Physical Environment of Pediatric Inpatient Wards on Children.
Findings from the Literature Synthesis
Inpatient wards are often stressful environments and may induce fear among children. However, the current literature shows several evidence-based approaches to improve these environments for children and opens a wide range of avenues for future research. Figure 4 displays the list of “elements of physical environments” that have been discussed in the selected 30 articles. “Noise level in the healthcare environment” had been a hot topic in 30% of articles. Other than that, “artificial light” (16.67%), “play spaces” (16.67%), “spaces for parents” (13.33%), “unfamiliar environment” (13.33%), “art” (10%), and “patient's bed” (10%) were discussed in three or more studies. Each element was coded as either “positive effect,” “negative effect,” “mixed effect,” or “no effect,” as shown in Figure 4. Patient/family outcomes for each element can be seen in Figure 5, based on findings.
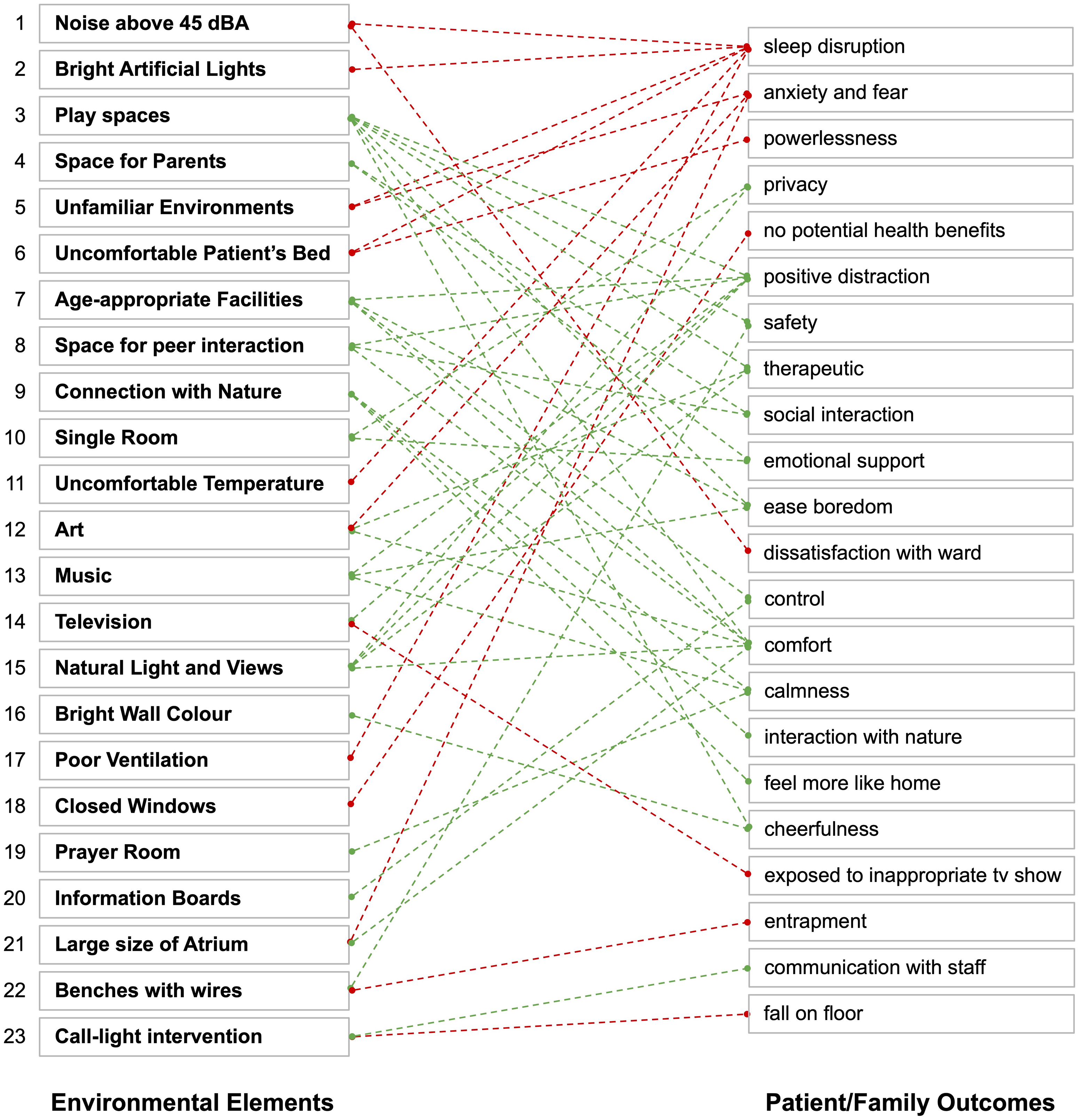
Patient/Family Outcomes of the Physical Environment (Pediatric Inpatient Wards).
Positive Effect
In 11 studies (Biddle et al., 2025; Bsiri-Moghaddam et al., 2011; Clift et al., 2007; Emre et al., 2025; Gill et al., 2023; Koller & McLaren, 2014; Lambert et al., 2014a; Longhi & Pickett, 2008; Lundgren et al., 2020; Preti & Welch, 2011; Sherman et al., 2005), 11 elements of the physical environment were identified to be explicitly associated with positive effects.
Play Spaces
Spaces dedicated to play provided a crucial role in creating positive distraction for children in pediatric inpatient wards. According to Koller and McLaren (2014), spaces that provided opportunities to play were more than just a distraction, as they provided a safe and therapeutic environment to cope with stress and anxiety. In an interview, a child appreciated play space as one of the interesting things in the hospital (Gill et al., 2023). Ward-based play areas were favorable in the inpatient ward due to their proximity and ease of accessibility (Lambert et al., 2014a). However, Clift et al. (2007) reported that adolescents often found playrooms designed for younger children unappealing, underscoring the need for age-appropriate recreational facilities. A recent study by Emre et al. (2025) found that providing board games as part of “bedside support practice” helped children psychologically—making them feel good and happy as well as reducing pain and anxiety. Children described these bedside play activities as educational and entertaining in terms of enjoyment and spending quality time.
Space for Parents
Dedicated spaces for parents were recognized as an essential part of the physical environment of pediatric inpatient wards, as they promoted social interaction within the ward (Lambert et al., 2014a). These spaces are perceived to have a positive effect both during the day and night times, as they provide practical and emotional support to children (Lundgren et al., 2020). Gill et al. (2023) reported findings from a study in which families and children appreciated the privacy provided by single rooms that enabled families to be together. Conversely, the absence of a dedicated space for parents could be a cause of concern for the children. Bsiri-Moghaddam et al. (2011) reported that children were concerned or worried about the discomfort and troubles of their parents due to the absence of a dedicated space for parents/caregivers.
Age-Appropriate Leisure and Recreational Facilities
They were reported to provide positive distraction to different age groups of children, especially within the ward (Clift et al., 2007; Lambert et al., 2014a). Facilities with gaming devices such as—PlayStations, Xbox, Nintendo DS, iPods, and computers/laptops to play games; televisions to watch films, view photos, and listen to music; internet-enabled devices with cameras to connect with friends through social media—enabled children to combat/alleviate boredom, enriched a sense of control and reduced a sense of isolation, especially for those who required extended hospital stay (Lambert et al., 2014a). Lambert et al. (2014a) emphasized that these facilities had to be both age-appropriate and gender-inclusive to meet the diverse needs of children across age groups and genders. Additionally, Clift et al. (2007) highlighted that these facilities not only created a positive hospital experience for children but also helped parents and healthcare professionals in assessing the patient's health improvement.
Space for Peer Interaction
Spaces for peer interaction reduced the feelings of anxiety and isolation by providing multiple distractions and opportunities for social engagement (Clift et al., 2007). Spaces like gardens, playgrounds, common seating areas, and so on, fostered peer interaction, enabling children to build and maintain relationships with fellow patients and family members (Lambert et al., 2014a). Integration of these spaces within inpatient wards could ensure accessibility for all children—including those with restricted movement, confined to bed, or in isolation—allowing them to independently engage in activities without leaving their immediate surroundings (Lambert et al., 2014a).
Connection with Nature
Connection with nature fostered a sense of relaxation for children (Koller & McLaren, 2014). A study on healing gardens revealed that being surrounded by plants and trees allowed children to interact with both natural and structural elements, enhancing their connection with nature (Sherman et al., 2005). Koller and McLaren (2014) further highlighted the calming effect of plants and trees, with some participants expressing that it made them feel calmer and more pleasant when they saw plants/trees, while others believed that plants were important as they “made the space feel more like home,” especially when they could not go outside.
Single Rooms
They offered privacy and personal space that pediatric patients and their families appreciated (Gill et al., 2023; Lundgren et al., 2020). According to Gill et al. (2023), these rooms were especially important in the pediatric context—comprising the patient, parents, and siblings—to stay together as a family and provide emotional support to each other. However, while families preferred the intimacy and comfort of single rooms, they often felt a sense of disconnect from healthcare professionals due to the reduced visibility and accessibility of nursing staff (Gill et al., 2023).
Music
Particularly, live music was shown to provide numerous benefits to children in inpatient wards. It could significantly increase oxygen saturation levels, thus improving the physiological and psychological states of pediatric patients (Longhi & Pickett, 2008). Music also served as an important positive distraction, helping children and their parents/caregivers alleviate the stress and anxiety of hospitalization, as well as the distress associated with physical conditions (Preti & Welch, 2011).
Others
“Natural light and views” received positive feedback from children, families, and nurses for creating brighter surroundings by allowing sunlight to fill the inpatient rooms and providing windows with views of the outdoors, which enhanced their comfort and sense of privacy (Gill et al., 2023). “Bright wall color” could create a cheerful environment for children, countering the sadness often associated with hospital visits (Koller & McLaren, 2014). “Prayer room” provided a calming space where individuals, especially parents during their child's surgery, turned to God in times of distress (Bsiri-Moghaddam et al., 2011). “Information boards” alleviated adolescents’ fears and fostered a more positive hospitalization experience by providing essential information to them (Clift et al., 2007).
Negative Effect
In 9 studies (Bsiri-Moghaddam et al., 2011; Clift et al., 2007; Coyne, 2006; Linder & Christian, 2011, 2012; Lundgren et al., 2020; Manuel et al., 2021; Meltzer et al., 2012; Sherman et al., 2005), 7 elements of the physical environment were identified to be explicitly associated with negative effects.
Noise Above 45 dBA
Studies had identified a noisy environment as a primary cause of nighttime awakenings in pediatric inpatient wards, which directly influenced the health and recovery of children (Coyne, 2006; Linder & Christian, 2011, 2012; Manuel et al., 2021; Meltzer et al., 2012; Soubra et al., 2018). Factors like telephones ringing, nurses talking, younger children crying, and so on, added to the noise level of the wards, which had been reported by some children as the cause of their sleep disruption (Coyne, 2006). Elevated noise levels negatively affected the physical and psychological health of children (Clift et al., 2007), leading to dissatisfaction with the ward environment among children (Bsiri-Moghaddam et al., 2011). Noise also served as an additional physiological and psychological stressor, particularly for children undergoing chemotherapy, where it could adversely affect their health and recovery (Linder & Christian, 2011). A quantitative study showed that nighttime sleep was strongly influenced by elevated sound levels at the child's bedside (r = −0.72, p < 0.01), compared to bright artificial light and uncomfortable temperature (Linder & Christian, 2012). Unfamiliar noise in or near patient rooms also hindered adolescents’ ability to fall asleep (Lundgren et al., 2020).
Bright Artificial Lights
Bright lights at night in the inpatient wards had been recognized as a cause of sleep disruption among children, affecting their physical and psychological health (Clift et al., 2007; Coyne, 2006; Linder & Christian, 2012). A qualitative interview study reported that adolescents preferred dark rooms to sleep and wished for the provision of blinds (Lundgren et al., 2020). Likewise, an exploratory study suggested that dimming artificial lights at night might have had a synergistic effect in creating a calm and restful environment (Meltzer et al., 2012). These findings supported Ulrich's theory of supportive design for healthcare (Ulrich, 2000).
Unfamiliar Environments
The unfamiliarity of inpatient healthcare environments had been reported to create feelings of anxiety and fear among children and adolescents (Bsiri-Moghaddam et al., 2011; Clift et al., 2007; Coyne, 2006). Previous hospitalizations did not necessarily mitigate this stress, as the presence of unfamiliar medical equipment and the need to adapt to separation from parents and familiar caregivers remained daunting (Bsiri-Moghaddam et al., 2011; Coyne, 2006). In some cases, unfamiliarity was also the reason for nighttime awakenings in children (Manuel et al., 2021).
Uncomfortable Patient's Bed
An uncomfortable bed had been reported as one of the reasons for children's sleep disruption (Meltzer et al., 2012). A lack of choice or control over the bed space may have conveyed a sense of powerlessness to children (Coyne, 2006). According to Lundgren et al. (2020), incorporating height-adjustable beds could have alleviated some of these issues by allowing children to adjust the bed to their comfort, enhancing usability and overall satisfaction.
Uncomfortable Temperature
Temperature, whether it was too cold or slightly elevated in the inpatient ward, could significantly affect the comfort and well-being of children (Linder & Christian, 2012; Lundgren et al., 2020). Although the impact of ambient temperature on sleep quantity might have been less pronounced compared to factors like sound and light, findings suggested that slight thermal discomfort influenced the nighttime sleep of children (Linder & Christian, 2012).
Others
“Poor ventilation”: low and improper ventilation in the inpatient wards was reported to contribute to an environment that made it difficult for children to fall asleep (Coyne, 2006). “Closed windows”: the absence of open windows in the inpatient wards limited children from experiencing maximal potential health benefits from their views of nature (Sherman et al., 2005).
Mixed Effect
In 5 studies (Biddle et al., 2025; DiMaggio et al., 2003; Eisen et al., 2008; Koller & McLaren, 2014; Nelson & Staffileno, 2017), 5 elements of the physical environment were identified to be associated with mixed effects.
Art
“Artworks” in hospitals, particularly drawings and cartoon characters, were appreciated by many children due to their comforting effect (Koller & McLaren, 2014). However, the impact of “artwork on walls” was found to be mixed, with responses varying by age, gender, context, and type. In a comparative study, “representational nature art” was highly preferred art image for most of the age groups and genders—the preference remained consistent in favor of nature irrespective of their cognitive developmental stages (Eisen et al., 2008). Notably, adolescents aged 14–17 showed significant differences in diastolic blood pressure ratings, with the nature art group (N = 6, M = 125.17, SD = 6.21) performing worse than the no-art group in phase-1 studies (Eisen et al., 2008). Psychophysiological measures (Varni PedsQL™ Present Functioning Module, blood pressure, and respiratory rates) did not support the hypothesis that “nature art would have therapeutic benefit of stress reduction,” but same measures suggested that nature art positively influenced more males than females (Eisen et al., 2008). On the other hand, “abstract art” had been marked higher for worry ratings among children compared to nature art, with a significant focus on concerns like “worry what would happen to me” (Eisen et al., 2008). Similarly, a study on healing ceilings reported that children preferred more realistic-style artwork—such as animals, nature, and cartoons painted in a bright color palette—over representational content (Biddle et al., 2025). Furthermore, “murals” depicting specific scenes sometimes triggered negative emotions in some children, as in the case of an 11-year-old boy who felt anger at a mural depicting people sitting by the ocean, which reminded him of what he was missing (Koller & McLaren, 2014).
Television
They provided a medium for children to entertain themselves during the daytime, helping them cope with long and often monotonous days (Lundgren et al., 2020). But, it also posed a challenge, as children were significantly more likely to be exposed to inappropriate programming when it was controlled by an adult (DiMaggio et al., 2003). However, this could have been converted into an opportunity to educate parents in hospitals on “appropriate television viewing habits” for children at home (DiMaggio et al., 2003).
Call-Light Intervention
These had improved patient satisfaction by automating communication between patients and the nursing team, ensuring prompt responses to call lights (Nelson & Staffileno, 2017). However, a post-intervention analysis had shown an increase in patient fall rates, though event review of each fall did not indicate call light response as a factor in the fall (Nelson & Staffileno, 2017).
Others
“Large size of atrium” had been found to evoke mixed feelings in children, making some feel comfortable, safe, and relaxed, while others found the large size of the atrium to be scary and intimidating (Koller & McLaren, 2014). “Overhanging benches with protective cages and wires” had mixed effects—the overhanging benches symbolized protection for some while evoked a sense of entrapment for others (Koller & McLaren, 2014).
No Effect
In a single study, noise was found to have no effect. As a significant ambient stressor, noise had detrimental effects, especially on vulnerable children (Soubra et al., 2018). Although measures to reduce ambient noise levels—such as the use of an oiled door knob, resetting the time of the floor cleaning machine, adjustment of telephone sound level to below 45 dBA, allocation of special rooms for nurses and physicians to discuss patient-related issues, adjusting the intercom sound level to below 45 dBA, establishing a second nursing station to relieve the congested primary nursing station, distribution of noise reduction stickers at the main entrance of the unit to reinforce the noise reduction campaign, and so on—had shown some effectiveness in reducing ambient noise levels, but they had not significantly improved the patient satisfaction level (Soubra et al., 2018). Soubra et al. indicated that “small patient sample size” could be the reason for this discrepancy.
Discussion
The findings from this systematic review offer significant implications for future research and the design of healthcare environments tailored specifically for children and families. By systematically identifying environmental elements that impact the well-being of children and families in pediatric inpatient wards, the review tries to bridge existing gaps between research and practice, offering actionable insights to architects, designers, healthcare providers, and policymakers.
Implications for Research
The review findings highlight significant knowledge gaps and identify potential avenues for future research. In total, 60% of studies did not explicitly aim to investigate human–environment relationships in the inpatient wards—they were either focused on finding children's preferences or other unrelated aspects (such as analyzing policy recommendations, day and nighttime sleep patterns, etc.). More research was from the children's perspective (Biddle et al., 2025; Carney et al., 2003; Clift et al., 2007; Coad & Coad, 2008; Coyne, 2006; Ebrahimpour et al., 2021; Eisen et al., 2008; Hutton, 2005; Koller & McLaren, 2014; Lambert et al., 2014a, 2014b; Lundgren et al., 2020; McLaughlan & Willis, 2021; Park, 2009; Payam et al., 2023; Ullán et al., 2012), which provided valuable insights but could not elaborate on the direct impact of the physical environment on children. This underscores the need for more targeted studies that systematically examine the impact of the physical environment on the experiences, health outcomes, and overall well-being of children in inpatient wards.
This review identified only two studies (Eisen et al., 2008; Park, 2009) that met Level-2 criteria of “level of evidence for healthcare design.” Level-2 evidence typically includes studies with strong methodologies, such as well-designed experimental or quasi-experimental approaches (Gripko et al., 2023; Marquardt et al., 2014; Stichler, 2010). Expanding the number of such studies would significantly enhance the rigor of the evidence base in this field (Stichler, 2010). Such studies would not only enhance the credibility and reliability of the evidence but also help uncover novel elements and their potential impacts. Additionally, they could also help to validate or challenge existing findings, thereby contributing to a deeper and more comprehensive understanding of effective healthcare design interventions or strategies.
This review also highlights a significant gap in the empirical research on the physical environment of pediatric inpatient wards in the Global South, where children aged 0–15 years constitute approximately 40% of the total population, compared to less than 20% in the Global North (Odeh, 2010). This lack of empirical data on pediatric healthcare environments from the Global South indicates a paucity of research about the cultural and contextual nuances that influence children's experiences of the healthcare environments. Future research can provide valuable insights into the varying needs of children in various socio-cultural settings, contributing to a more inclusive and contextually relevant evidence base for the design of responsive and supportive healthcare environments.
This review explicitly elaborates on the elements of the physical environment that affect children and their families in inpatient wards. Eleven elements of the physical environment—play spaces, space for parents, age-appropriate leisure and recreational facilities, space for peer interaction, connection with nature, single rooms, music, natural light and views, bright wall color, prayer room, and information boards—contribute to creating a supportive and healing environment for children in inpatient wards (Biddle et al., 2025; Bsiri-Moghaddam et al., 2011; Clift et al., 2007; Emre et al., 2025; Gill et al., 2023; Koller & McLaren, 2014; Lambert et al., 2014a; Longhi & Pickett, 2008; Lundgren et al., 2020; Preti & Welch, 2011; Sherman et al., 2005). Integrating these physical elements in the healthcare environment may create a positive and comforting atmosphere for children. Conducting experimental research on these environmental elements may provide clearer insights into their impact on children.
Other seven elements—noise, bright artificial lights, unfamiliar environments, uncomfortable patient's bed, uncomfortable temperature, poor ventilation, and closed windows—negatively affect the children's well-being in the inpatient wards (Bsiri-Moghaddam et al., 2011; Clift et al., 2007; Coyne, 2006; Linder & Christian, 2011, 2012; Lundgren et al., 2020; Manuel et al., 2021; Meltzer et al., 2012; Sherman et al., 2005). These seven elements of the physical environment highlight the importance of attenuating these environmental variables to reduce stress in children through design and quality improvement interventions, ensuring that children experience a more supportive and healing environment in the inpatient wards. Another five elements of the physical environment—art, television, large size of atrium, overhanging benches with protective cages and wires, and call-light intervention—offer mixed results (Biddle et al., 2025; DiMaggio et al., 2003; Eisen et al., 2008; Koller & McLaren, 2014; Nelson & Staffileno, 2017). While some provide comfort, entertainment, or improve communication, others can trigger negative emotions. Understanding the underlying causes behind the positive and negative effects relationship is essential for developing a nuanced understanding of these elements, aiding in the future designs of healthcare environments that better support children's physical and psychological well-being.
There is a pressing need to understand the impact of the physical environment on children across all age groups. Several studies have highlighted that adolescents need physical environments which are different from those designed for younger children (Battle et al., 1989; Blumberg & Devlin, 2006; Clift et al., 2007; Fisher & Kaufman, 1996; Gillies, 1992; Hutton, 2005; Miller, 1996). However, there is limited evidence on the specific needs of other age groups—infants, toddlers, preschool, and school-going children. Therefore, there is a need to uncover the nuances of human–environment interactions and identify perceived needs of children across all age groups in healthcare settings.
Future research can also investigate the use of interactive displays for positive distraction, as these displays provide an engaging experience for children without the need to touch or be in contact with any surface, especially in healthcare settings where the spread of infection is a major concern (Babbu & Haque, 2021; Biddiss et al., 2013). In addition, emerging therapeutic digital technologies such as virtual reality for pain management, telepresence systems for family connection, and personalized smart environmental controls can also be considered for further research in pediatric inpatient wards (Storey et al., 2025; Su et al., 2025; Weibel et al., 2023). There is also a pressing need to explore the design for special neurological conditions, which can integrate sensory-responsive environmental elements aimed at improving the comfort and well-being of children with sensory processing differences like autism, attention-deficit/hyperactivity disorder, and so on (Abdallah, 2025; Williams et al., 2023). Furthermore, research should also consider the expectations and interactions of digitally native children, assessing how this may shape their healthcare experiences in the future.
Implications for Design
Findings from the review offer directions for designers to create supportive environments for children in inpatient wards—by creatively integrating elements of physical environments that are associated with positive effects (see Figure 6). For example, play spaces inside the ward not only act as a positive distraction but also provide a therapeutic environment which eventually helps to reduce stress and anxiety in children as well as in their families (Koller & McLaren, 2014; Lambert et al., 2014a). Creating space for parents near the patient beds can help to promote social interaction among parents and also provide emotional support to children throughout their hospital stay (Bsiri-Moghaddam et al., 2011; Gill et al., 2023; Lambert et al., 2014a; Lundgren et al., 2020).
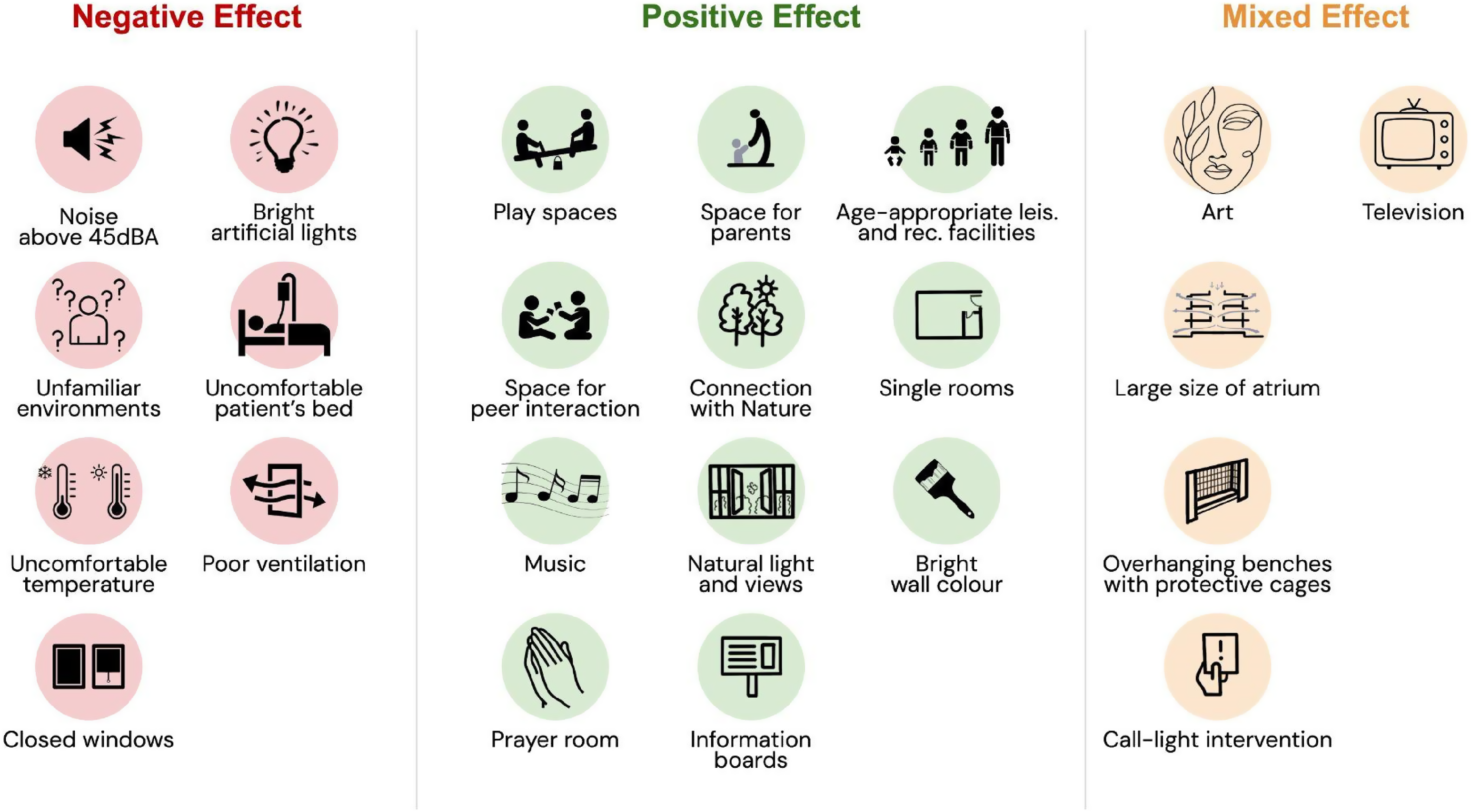
List of Elements of Physical Environment with their respective Effects on Children in Pediatric Inpatient Wards, based on Literature Evidence.
A crucial challenge in the design of pediatric environments is to cater to the children's developmental and psychological needs. For this, design strategies should prioritize the provision of age-appropriate design considerations which can be extended to all facilities, instead of being limited to leisure and recreational facilities. These spaces inside inpatient environments will not only help in creating social connections, but also reduce the feeling of isolation and boredom among children (Clift et al., 2007; Lambert et al., 2014a).
Access to natural light, views of nature through windows, music, and a medium to connect with nature could be prioritized in designs to leverage the therapeutic effects of these environmental elements (Gill et al., 2023; Koller & McLaren, 2014; Longhi & Pickett, 2008; Preti & Welch, 2011; Sherman et al., 2005). Noise levels and artificial lighting were among the most reported environmental elements with negative effects (Bsiri-Moghaddam et al., 2011; Clift et al., 2007; Coyne, 2006; Linder & Christian, 2011, 2012; Lundgren et al., 2020; Manuel et al., 2021; Meltzer et al., 2012; Soubra et al., 2018). Architects and environmental designers can develop innovative environmental interventions to reduce ambient noise levels as per the recommended guidelines and optimize artificial lights to mimic circadian light cycles with “acoustic and lighting design.” Single rooms, although they offer privacy and family support, pose challenges such as reduced healthcare staff visibility and accessibility (Gill et al., 2023; Lundgren et al., 2020). Future designs of inpatient rooms must strike a fine balance between the need for privacy and family support for children and families, with visibility and accessibility for healthcare staff. Mixed effects of elements like art and television underscore the importance of curating appropriate content and offering parental control, which is in sync with the children's emotional states and relevant to their age group. Designers could collaborate with child psychologists and healthcare staff to integrate interactive art, safe entertainment options, and informative visual communication to create restorative healthcare environments that support the well-being of pediatric patients in positive ways.
Bridging Research and Practice
By synthesizing the available empirical evidence on pediatric inpatient ward environments, this review highlights critical design and research considerations that can inform the design of restorative and supportive healthcare environments for children. Integrating child-centered, age-sensitive, family supportive, and positive-distraction elements into healthcare settings can create environments that not only support recovery but also promote the holistic well-being of pediatric patients (Alhsainat & Günçe, 2024; Committee on Hospital Care and Institute for Patient-and Family-Centered Care, 2012; Jiang, 2020). Simultaneously, fostering a culture of evidence-based design that prioritizes participatory, multidisciplinary, and culturally inclusive approaches will ensure continuous improvements in the design of pediatric healthcare environments (Jaušovec & Gabrovec, 2023; Taylor, 2016).
If evidence from literature reviews on the topic beyond the scope of the current study are collated, a comprehensive list of environmental elements with respect to their effects on children can help researchers, designers, and practitioners to develop a set of evidence-based guidelines for the design of restorative and supportive pediatric healthcare environments. Therefore, more rigorous research is needed across geographies and cultures to directly examine human–environment interactions in pediatric inpatient wards as well as other pediatric healthcare environments to advance evidence-based design practices in the domain of “children healthcare design and planning.”
More rigorous research is needed across geographies and cultures to directly examine human–environment interactions in pediatric inpatient wards as well as other pediatric healthcare environments to advance evidence-based design practices in the domain of ‘children healthcare design and planning.’
Limitation
Like other systematic literature reviews, this study also has some limitations. It is possible that the removal of non-English articles may have resulted in the omission of relevant research articles, particularly those from non-English-speaking countries. This limitation may have disproportionately affected the representation of evidence from the Global South, where research is more likely to be published in local languages, potentially contributing to an underrepresentation of cultural and contextual findings. The reliance on four databases—PubMed, Embase, Scopus, and Web of Science Core Collection—may have led to an incomplete capture of all relevant articles, although the authors attempted to mitigate this through a comprehensive search strategy and reference snowballing process. In line with the Cochrane Handbook (Chandler et al., 2019), a quantitative estimate of inter-rater agreement was not calculated as study selection relied on independent screening and consensus discussion among all the reviewers. Finally, scientometric studies always reflect the current state of the literature at the time of analysis and cannot rule out the research impact of newer publications and citations.
Conclusion
Following a systematic database search and rigorous assessment of relevant literature, this review emphasizes the impact of the physical environment of pediatric inpatient wards on children and their families. Findings from 30 empirical studies coded in four categories—positive, negative, mixed, and no effect—highlight the important elements of the physical environment that can reduce stress, promote healing, and foster a sense of comfort and safety for children and their families. The review also tries to bridge the gap between research and practice, offering actionable recommendations for creating evidence-based, age-sensitive, and child-centric designs of inpatient wards that cater to children's developmental, emotional, and psychological needs. However, the scarcity of high-quality studies and underrepresentation of diverse geographical and cultural contexts, particularly from the Global South, calls for more rigorous and inclusive global research-informed-design efforts. Such studies are essential for advancing the field of pediatric healthcare design and ensuring that healthcare environments support holistic well-being across all sociocultural settings.
Implications for Practice
Findings from the review offer directions for designers to create supportive environments for children in inpatient wards—by creatively integrating elements of physical environments that are associated with positive effects.
A crucial challenge in the design of pediatric environments is to cater to the children's developmental and psychological needs. For this, design strategies should prioritize the provision of age-appropriate design considerations which can be extended to all facilities, instead of being limited to leisure and recreational facilities.
Access to natural light, views of nature through windows, music, and a medium to connect with nature could be prioritized in designs to leverage the therapeutic effects of these environmental elements.
Noise levels and artificial lighting were among the most reported environmental elements with negative effects. Architects and environmental designers can develop innovative environmental interventions to reduce ambient noise levels as per the recommended guidelines and optimize artificial lights to mimic circadian light cycles with “acoustic and lighting design.”
Designers should collaborate with child psychologists and healthcare staff to integrate interactive art, safe entertainment options, and informative visual communication to create restorative healthcare environments that support the well-being of pediatric patients in positive ways.
Supplemental Material
sj-docx-1-her-10.1177_19375867261451751 - Supplemental material for Impact of Physical Environment of Pediatric Inpatient Wards on Children: A Systematic Literature Review
Supplemental material, sj-docx-1-her-10.1177_19375867261451751 for Impact of Physical Environment of Pediatric Inpatient Wards on Children: A Systematic Literature Review by Renuka Singh, Sachit Anand, Aakash Johry and Gourab Kar in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Vijay Kumar Verma from Indian Institute of Technology Delhi, for his valuable assistance in facilitating library access and supporting the collection of relevant articles.
Ethical Approval and Informed Consent Statements
This article does not contain any studies with human or animal participants.
Author Contributions
Conceptualization: RS, SA, AJ, and GK; data curation: RS; formal analysis: RS, SA, AJ, and GK; funding acquisition: N/A; investigation: RS, SA, AJ, and GK; methodology: RS, SA, AJ, and GK; project administration: RS, SA, AJ, and GK; resources: RS, SA, AJ, and GK; software: RS; supervision: SA, AJ, and GK; validation: SA, AJ, and GK; visualization: RS; writing—original draft: RS; writing—review and editing: RS, SA, AJ, and GK. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that supports this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.