
Abstract
Purpose
This study examines how operating room (OR) staff in Australia are engaged in OR design planning and how their professional experience shapes participation, safety considerations, and design priorities.
Background
The design of OR environments influences safety, efficiency, and workflow. Yet design processes are complex, requiring regulatory compliance, technical expertise, and integration of end-user perspectives.
Methods
A sequential exploratory mixed methods design was used. Phase one involved qualitative interviews with OR staff and design professionals (n = 16) to explore experiences of design processes and perceptions of safety. Phase two involved a national cross-sectional survey (n = 418) to assess broader patterns of engagement and role-based differences in safety and design priorities.
Results
Mixed methods integration showed that OR design in Australia is shaped by systemic and professional barriers, including fragmented communication, limited interdisciplinary engagement, and hierarchical decision-making. OR staff reported inconsistent or minimal involvement, while designers reported challenges embedding participatory approaches within project constraints. OR staff prioritized safety, ergonomics, and workflow efficiency, while designers focused more on regulatory and technical elements. Access to support, spatial layout, and ergonomic considerations emerged as top safety-related design features.
Conclusions
OR environments are shaped by the interaction of clinical, architectural, and institutional priorities, yet design processes often lack inclusive, safety-focused collaboration. Strengthening participatory mechanisms that integrate clinical expertise with technical and regulatory demands may improve the relevance and safety of surgical built environments. These findings can inform future policy, standards, and design frameworks to support more collaborative OR planning.
Well-designed operating rooms (ORs) are essential for patient safety, surgical precision, and staff efficiency, with layout and spatial organization shaping clinical workflows and outcomes (Allison et al., 2021; Bayramzadeh et al., 2018b; Joseph et al., 2018, 2021; Koch et al., 2020; MohammadiGorji et al., 2024; Oh et al., 2024). OR environments are inherently complex spaces, requiring seamless integration of advanced technologies, infection control measures, and multidisciplinary workflows. Within these spaces, surgical teams collaborate using their specialized expertise to address challenges with patient care (Sutherland-Fraser et al., 2022), while managing complex surgical procedures requiring teamwork, concentration and focus, highlighting the importance of involving OR staff in design decisions to ensure safety, functionality, and efficiency. Literature has emphasized the value of evidence-based design approaches that incorporate the insights of end users (Bayramzadeh et al., 2018a; Carthey, 2020; Elf et al., 2020; Kim et al., 2024; Ulrich et al., 2008). Participatory methodologies have been proposed as strategies to incorporate end-user insights and experiences within built environment design, ensuring that those who use the space contribute meaningfully to its planning and development (Carthey, 2021; Vargas et al., 2022).
Within healthcare infrastructure projects, participatory design typically involves structured consultation processes, workshops, mock-ups, simulation exercises, and user group meetings, where clinical staff contribute experiential knowledge regarding workflow, equipment use, patient safety, and operational requirements. The Australasian Health Facility Guidelines (AusHFG) (Australasian Health Infrastructure Alliance, 2025), alongside various local and national standards, guide healthcare built environment design within Australia. The AusHFG provides guidance for health facility planning and design, including functional content, spatial requirements, and performance expectations for clinical areas such as ORs. While not legislation, the guidelines are widely adopted by state health departments and are referenced within healthcare capital works projects to support consistent design standards and align with international healthcare design guidelines. Planning processes typically involve health department representatives and a lead design team including architects, engineers, and health planners (New South Wales Government, 2024). Local clinical and operational teams are engaged by design teams to represent service needs (Bernhardt et al., 2022; Blanch & Frazer, 2023), although the extent of their involvement may vary (Carthey, 2021; Pomare et al., 2021). Despite substantial investment in healthcare infrastructure globally, limited research has examined how OR staff contribute to built environment planning and the optimization of OR design. Understanding OR staff participation in design processes and identifying the factors that enable or hinder engagement is essential for improving healthcare facility planning. For the purposes of this article, the interdisciplinary OR team, including nurses, surgeons, anesthetists, and technicians/orderlies, is collectively referred to as “OR staff.”
The aims of this study were to examine how OR staff in Australia are engaged in OR design planning processes and how professional experience shapes participation, perceived influence, and design priorities within these processes. Specifically, the study sought to address the research questions: how do OR staff experience and engage in OR design and planning processes; what factors do they perceive as influencing safety and functional performance within the OR environment; and how do perspectives on safety, workflow, and design priorities differ across professional roles? Safety was an inherent consideration within the study, initially informed by the researcher's clinical background as an OR nurse, where maintaining a safe environment is a central professional priority within perioperative care. On analysis of the data, the priority of safety was a significant concern of all participants and a necessary consideration in design planning. By identifying and analyzing the challenges and enablers of OR staff engagement, this study deepens understanding of how OR staff perspectives influence the design of OR environments. The findings highlight the importance of participatory design in healthcare and reveal key factors that shape meaningful involvement in built environment planning. These insights contribute to a broader discourse on collaborative design and have important implications for healthcare architects, policymakers, and hospital administrators aiming to align infrastructure development with clinical needs and patient care priorities.
Literature
A focused review of literature on OR design and staff engagement was undertaken using major health and design databases (Ovid, MEDLINE, PubMed, ProQuest, and CINAHL). Research on healthcare environments identifies Evidence-Based Design (EBD) as a framework linking physical settings with patient and staff outcomes (Brambilla & Capolongo, 2019; Brambilla et al., 2019; Elf et al., 2024; Ulrich et al., 2010; Zamani et al., 2023). EBD aligns environments with practices known to improve safety, performance, and well-being. While this study is situated within the Australian healthcare context, the review incorporated international literature to support broader transferability of findings across healthcare systems. Ulrich's Theory of Supportive Design (1991) highlighted the need for flexible, evidence-informed environments and the lack of reliable research to guide healthcare decision-makers.
Evidence-Based Design and the OR Environment
Recent developments in healthcare design have integrated EBD, human factors, and interdisciplinary collaboration to improve OR functionality (Battisto et al., 2023; Brambilla & Capolongo, 2019; Shultz et al., 2020). Simulation, human factors principles, and post-occupancy evaluations (POEs) improve workflow, patient safety, and staff performance (Allison et al., 2021; Bayramzadeh et al., 2018a, 2018b; Brambilla & Capolongo, 2019; MohammadiGorji et al., 2024; Wingler et al., 2018). However, OR built environment design research remains limited, focusing mainly on spatial layout, ergonomics, infection control, and technology (Allison et al., 2021; Joseph et al., 2019; Machry et al., 2020). In a review of safety, performance, and satisfaction outcomes, Joseph et al. (2018) found limited evidence to guide OR design, with few clear recommendations on how design decisions influence safety and performance. The US-led Realizing Improved Patient Care Through Human-Centered Design in the Operating Room (RIPCHD.OR) collaborative has advanced this field internationally through empirical analysis of staff movement, workflow, and spatial barriers (Allison et al., 2021).
Frameworks, Guidance, and Standards
POE frameworks and checklists exist, but few address the complexity of OR environments (Benitez et al., 2019; Brambilla & Capolongo, 2019; Elf et al., 2017). Blanch and Frazer (2023) identified the absence of a uniform framework guiding healthcare built environment POE processes across Australia and New Zealand, leading to inconsistencies in evaluation methods and outcomes. In Australia, the AusHFG provides high-level guidance for OR design, along with supplementary direction from the National Safety and Quality Health Service Standards (ACSQHC, 2021), Australian College of Operating Room Nurses Standards (ACORN, 2024), and the Australian Guidelines for the Prevention and Control of Infection in Healthcare (NHMRC, 2019). While these resources offer broad direction for OR Design in Australia and acknowledge the value of clinical expertise, they lack guidance to support structured OR staff participation. The absence of standardized tools for evaluating OR-specific design quality and stakeholder involvement highlights a persistent research–practice gap. Furthermore, frameworks, guidelines, and standards inform the technical and regulatory dimensions of OR design, but limited attention has been given to how OR staff are engaged in interpreting, applying, or influencing these requirements during planning processes. Understanding how staff navigate and contribute within these structured design environments is central to examining participatory practice.
Stakeholder Engagement in Healthcare Infrastructure Planning
Stakeholder engagement is widely recognized as critical to healthcare design, improving workflow, safety, and usability (Bayramzadeh et al., 2018a; Carthey, 2021; Joseph et al., 2018; Palmer et al., 2019; Shultz et al., 2020; Torres-Landa et al., 2019). Participatory and co-design methods encourage shared decision-making and interdisciplinary dialogue (Vargas et al., 2022), yet their use remains inconsistent. Despite recognized benefits, participatory design processes often lack clear frameworks and measurable outcomes (Carthey, 2020, 2021). Carthey (2021) identified the need for best practice guidelines to improve decision-making and participatory design outcomes in Australia, noting that health service planners and designers advocate for broader recognition and consistent application of the AusHFG as a design reference. Challenges associated with participatory design in healthcare include the complexity of healthcare systems, difficulty in translating stakeholder insights into actionable design requirements, and the time-intensive nature of facilitating perspective and consensus among diverse stakeholders with varying expectations (Lame et al., 2023; Palmer et al., 2019). In Australia, studies reveal uncertainty and limited consultation during hospital redevelopment projects (Pomare et al., 2021) and highlight trade-offs between patient privacy and staff visibility in new space configurations (Cusack et al., 2019). Collectively, the literature highlights the need for context-specific, interdisciplinary research that explores how OR staff experience, contribute to, and influence the design of safe, functional, and adaptive surgical environments. Despite recognition of participatory design principles within healthcare planning literature, empirical research examining how OR staff experience and perceive their involvement in OR-specific design processes remains limited, particularly within the Australian context. Further investigation is required to understand how professional experience shapes engagement and how participatory practices function in complex surgical environments.
Methods
Study Design
This study employed an exploratory sequential mixed methods design, underpinned by Constructivist Grounded Theory (CGT) as the qualitative framework (Charmaz, 2014; Creswell, 2021). A sequential approach was selected due to the limited evidence base surrounding OR staff engagement in design planning. The qualitative phase, grounded in participants' lived experiences, identified core concerns and concepts that informed the development of a quantitative questionnaire. The integration of qualitative and quantitative methods enabled the generation and subsequent examination of theoretical insights across a broader participant group, offering a comprehensive understanding of OR staff engagement in healthcare design, within the Australian context. The qualitative phase was designed to explore how OR staff experience and interpret their involvement in design planning processes. The subsequent quantitative phase extended these findings by examining patterns of engagement, perceived influence, and design priorities across a broader national sample. Figure 1 presents the visual model of the study design and outputs.
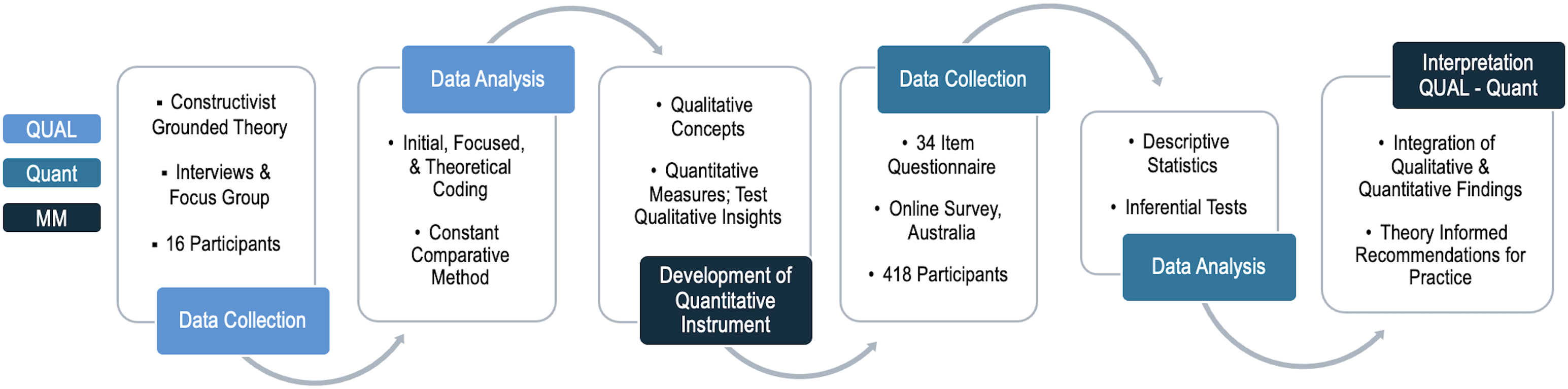
Exploratory Sequential Study Design.
Consistent with the CGT approach, existing healthcare design theories were not used to inform the design of this study, as the outcome of CGT is the identification of a new theoretical position. However, existing theoretical constructs emphasizing the role of environments in supporting task performance and reducing stress, critical considerations in the high-pressure, complex nature of ORs, informed the development of interview questions and a questionnaire (Brambilla & Capolongo, 2019; Shannon et al., 2020). These concepts shaped preliminary lines of inquiry, without imposing a predefined theoretical framework onto data coding or category development. Theoretical concepts drawn from healthcare design literature functioned as sensitizing concepts to guide early questioning, while analysis remained inductive and grounded in participant accounts. This study prioritized an emergent, participant-driven approach to understanding the factors shaping OR staff engagement.
Participants
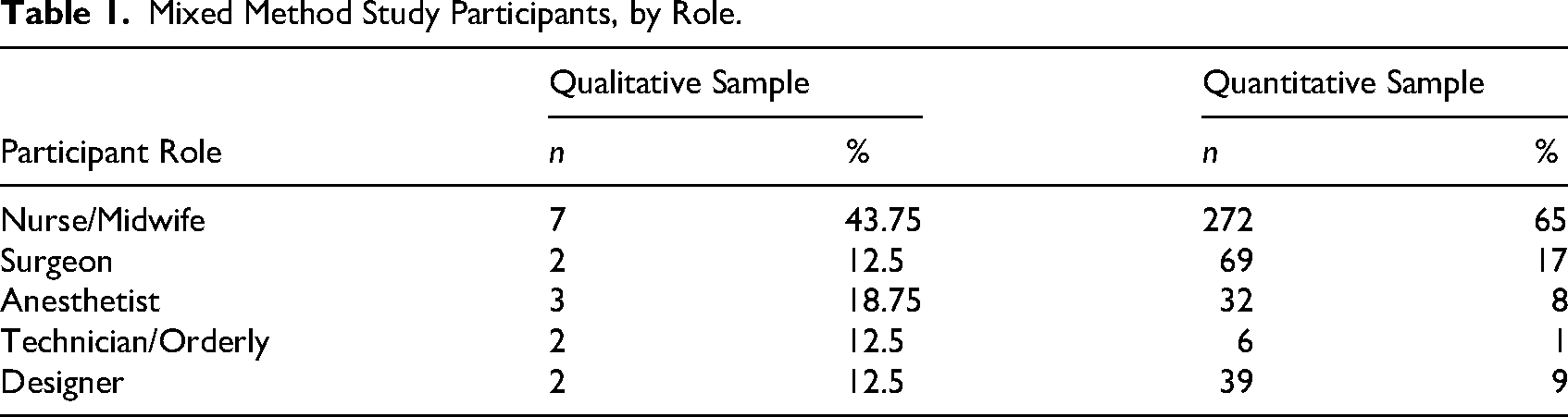
The study population comprised OR staff and individuals involved in healthcare design and planning within Australian healthcare settings. Eligibility criteria included current or recent experience working in OR environments or contributing to OR design or redevelopment processes. Individuals without OR-specific clinical or design experience were excluded from participation. Participants included both OR staff and design stakeholders as shown in Table 1. In Australian public hospitals, the OR team typically includes surgical and anesthetic consultants supported by registrars and resident/registered medical officers. Registered or licensed nurses undertake instrument, circulating, and anesthetic roles. Anesthetic nursing roles provide care to the patient and procedural support to the anesthetist. Theatre technicians/orderlies are ancillary staff who assist with OR setup, equipment positioning, and patient handling under clinical supervision (Sutherland-Fraser et al., 2022). In private hospitals, consultants often work with limited junior medical officer support, and technicians/orderlies may not be part of the OR team. For the purposes of this study, OR staff were defined as clinicians and support personnel working primarily within the OR environment. Staff exclusively working in pre-operative or post-anesthesia care areas were not included unless they had direct involvement in OR design planning processes. These role distinctions are relevant, as professional responsibilities and proximity to surgical workflows may influence how staff engage with, interpret, and prioritize design decisions. Although hospital design projects involve a wider interdisciplinary team, this study concentrated on OR staff and design professionals directly engaged in OR planning.
Mixed Method Study Participants, by Role.
Phase 1: Qualitative Methods and Findings
Details of qualitative methods, findings, and the development of the substantive theory are reported elsewhere (Irwin et al., 2024, 2025). In this article, Phase 1 findings are summarized to contextualize the development and examination of Phase 2 survey measures. A CGT approach enabled active researcher participation in theory development (Charmaz, 2014; Irwin et al., 2024, 2025). Qualitative enquiry explored how the built environment influenced the ability of OR staff to provide patient care, navigate the perioperative environment safely and efficiently, and contribute to OR design planning. Data were collected through fourteen individual semi-structured interviews and one focus group interview, with two participants, comprising a total of sixteen participants (N = 16). Additional focus groups were initially planned to facilitate role-specific group discussion; however, high clinical workloads and service pressures during the COVID-19 pandemic limited availability for group participation. As a result, individual interviews were prioritized to ensure participation from a diverse range of OR staff while accommodating scheduling constraints. Initially focusing on OR staff due to their direct experience within the surgical environment, through the constant comparative analysis method, it became evident that additional perspectives were needed to fully define and develop the emerging theory (Irwin et al., 2024). Designers involved in OR planning were subsequently included to provide insights into design processes, decision-making constraints, and the translation of clinical needs into spatial solutions. Interviews with designers were guided by the same overarching topic areas, with additional probing questions focused on design governance and decision-making. This iterative sampling approach is consistent with CGT principles, allowing emerging concepts to be further refined and elaborated. The input of designers enriched the analysis by revealing gaps between OR staff expectations and the practical challenges of implementing design changes, contextualizing clinical concerns within broader architectural, regulatory, and logistical frameworks, allowing for a more comprehensive understanding of how design decisions are made. Interview questions included prompts related to staff perceptions of safety for themselves and patients within the OR. Through constant comparison, it became evident that the consideration of safety was the framework by which participants described and interpreted workflow, environmental constraints, and design challenges. OR staff consistently described environmental and design-related issues that they felt impacted safe practice. Highlighting the advantage of using CGT to uncover new insights, safety became an analytic lens through which engagement in design planning was interpreted. Constant comparative analysis, including initial, focused, and theoretical coding, identified four interrelated concepts shaping OR design planning: (1) Engagement, Respect and Collaboration; (2) Foreseeing and Responding to Safety Concerns; (3) Enhancing Design Planning to Minimize Internal and External Consequences; and (4) Ambiguous Application of Standards in OR Design Planning (Irwin et al., 2024, 2025). Both OR staff and Design participants described engagement as relational and often hierarchical, where inclusion was influenced by power dynamics, professional identity, and communication processes. Safety concerns were grounded in the lived experience of workflow, hazards, and spatial constraints and the coordination of care within the built environment, with OR staff frequently anticipating and voicing additional risks not always visible within formal planning structures. OR design was conceptualized as a negotiated social process influenced by competing priorities, professional identity, and structural limitations. Standards and guidelines were viewed as influential but inconsistently translated into practice. Analysis of data was conducted inductively, with codes and categories developed from the data. Memo writing and iterative comparison supported refinement of emerging theoretical relationships. Sample adequacy was determined through constant comparison and iterative analysis, with theoretical sampling used to refine emerging categories. Analysis and recruitment continued until categories were well developed in terms of their properties and relationships, and no new conceptual insights were generated. This point of theoretical sufficiency informed the decision to conclude data collection (Charmaz, 2014). Consistent with CGT, this interpretation was co-constructed through interaction between participant accounts and the researcher's clinical background in perioperative practice. Reflexive memoing was undertaken throughout the analysis to critically examine how the researcher's perspective informed, rather than predetermined, the development of categories. Findings revealed the need for greater engagement, respect, and collaboration in OR design processes and highlighted the importance of incorporating OR staff lived experiences to address safety concerns effectively.
Phase 2: Quantitative Methods
Phase 2 involved creating a cross-sectional questionnaire to examine and extend concepts generated in Phase 1. These concepts were operationalized into measurable variables to assess the role of OR staff in shaping OR environments. Existing tools lacked specificity for OR design outcomes or staff engagement (Brambilla & Capolongo, 2019). To address this, the questionnaire drew on health design taxonomies (Anåker et al., 2017), foundational theory (Shannon et al., 2020), and empirical evidence (Allison et al., 2021; Joseph et al., 2018). In the absence of existing validated instruments specific to OR design engagement, these sources were used to inform construct clarity and terminology rather than to impose predefined theoretical domains for analysis. The work by Anåker et al. (2017) helped categorize environmental aspects, such as social, functional, and structural qualities, while Shannon et al.'s (2020) review informed how emerging concepts could be described in relation to broader healthcare design theory constructs. Items tested the emerging theory and included demographics, professional roles, and design involvement. Survey items were derived directly from Phase 1 categories. Draft items were reviewed for clarity and relevance by experienced OR staff and healthcare design professionals. Questions examined experience across specialties, agreement with design statements, and frequency of design-related issues. Ranking tasks and Likert scales prioritized design elements and assessed alignment with qualitative findings, with distinct question sets reflecting unique disciplinary perspectives. OR staff with prior design involvement completed four additional questions on engagement. OR staff completed 11 items based on direct experience within the OR, while designers answered nine modified items reflecting their indirect exposure.
Data Collection
Data were collected via a 34-item online questionnaire using REDCap, hosted by the University of Adelaide, between July 2023 and March 2024. The questionnaire was piloted with expert perioperative staff and design team members to ensure logical flow, clarity, and data capture effectiveness (Polit & Beck, 2020). Pilot responses were excluded from analysis. Pilot testing focused on face validity, item comprehension, completion time, and functionality of ranking tasks rather than psychometric validation. Minor revisions were made to wording and response options before wider distribution. Participants from the qualitative phase contributed to piloting, providing feedback that informed revisions to language and instruction, particularly for ranking questions. Ethical approval was granted by the university ethics committee (H-2023-095) in May 2023. Convenience sampling was used, with recruitment conducted through professional membership organizations and specialist networks, as no comprehensive national sampling framework exists for OR staff or healthcare designers involved in OR projects in Australia. Participation was based on voluntary self-selection among eligible individuals who received the survey invitation through these networks. Findings are therefore indicative rather than representative of all OR staff and designers in Australia. Approval was obtained from these organizations to distribute the online survey via email, social media, and newsletters across Australia. Initial plans to recruit through large membership bodies were revised due to changes in organizational processes. Alternative strategies targeting individual membership groups for surgeon and anesthetist recruitment were adopted.
Analysis
Despite initial recruitment challenges, 478 responses were received. Of these, 418 responses met the inclusion criteria and were retained for analysis; the remaining responses were excluded due to incompleteness or ineligibility. Ineligible responses included individuals who did not meet the defined inclusion criteria of current or prior OR experience or direct involvement in healthcare design planning. Incomplete responses were defined as surveys missing substantial sections of core engagement or design-related items, preventing meaningful analysis. A priori sample size calculation indicated that a minimum of 385 participants was required to achieve a 95% confidence level with a ± 5% margin of error. With the survey link distributed via professional membership organizations' newsletters and social media posts, the total number of individuals who received the survey invitation was unknown. Descriptive statistics, including frequencies, means, and standard deviations, were used to summarize demographic characteristics and overall response patterns. Analyses were conducted using IBM SPSS Statistics (for Mac, version 20, IBM). Likert scale items, treated as ordinal data, were summarized using medians and interquartile (IQR) ranges to reflect central tendency and variability (Dancey & Reidy, 2024). To support meaningful interpretation, several continuous response variables were stratified into categorical groupings, including years of experience, number of design projects participated in, and hours worked per week. Similarly, responses to items exploring observed or experienced issues within the OR were categorized to reflect frequency of occurrence (0 = never, rare 1–10, often 11–50, frequent >50). This grouping enabled comparative analysis across distinct participant subgroups and facilitated identification of patterns within and between categories. For ranked items, higher median scores indicated greater perceived importance (1 = less important to 5 = most important). Inferential analyses were conducted using nonparametric tests for ranked data and non-normally distributed observational data. Mann–Whitney U tests were applied for binary group comparisons, while Kruskal–Wallis tests were applied for comparisons across multiple groups. Where significant differences were identified by Kruskal–Wallis tests, Mann–Whitney U tests were applied for pairwise comparisons. This was an exploratory analysis; therefore, p-values are reported without correction for multiple testing and should be interpreted as indicative rather than conclusive (Dancey & Reidy, 2024). All statistical procedures were developed in consultation with a statistician, and the analyses were reviewed prior to final reporting. Integration occurred through comparison of quantitative patterns with qualitatively derived categories to assess consistency, divergence, and variation across professional groups. The quantitative phase was not designed to confirm the qualitative findings, but to explore their distribution and relative emphasis across a broader national sample.
Results: Quantitative Findings
The quantitative findings are presented in relation to the study research questions, focusing on patterns of engagement in OR design planning, perceived barriers and enablers, and the prioritization of safety and functional considerations across professional groups.
Participant Characteristics
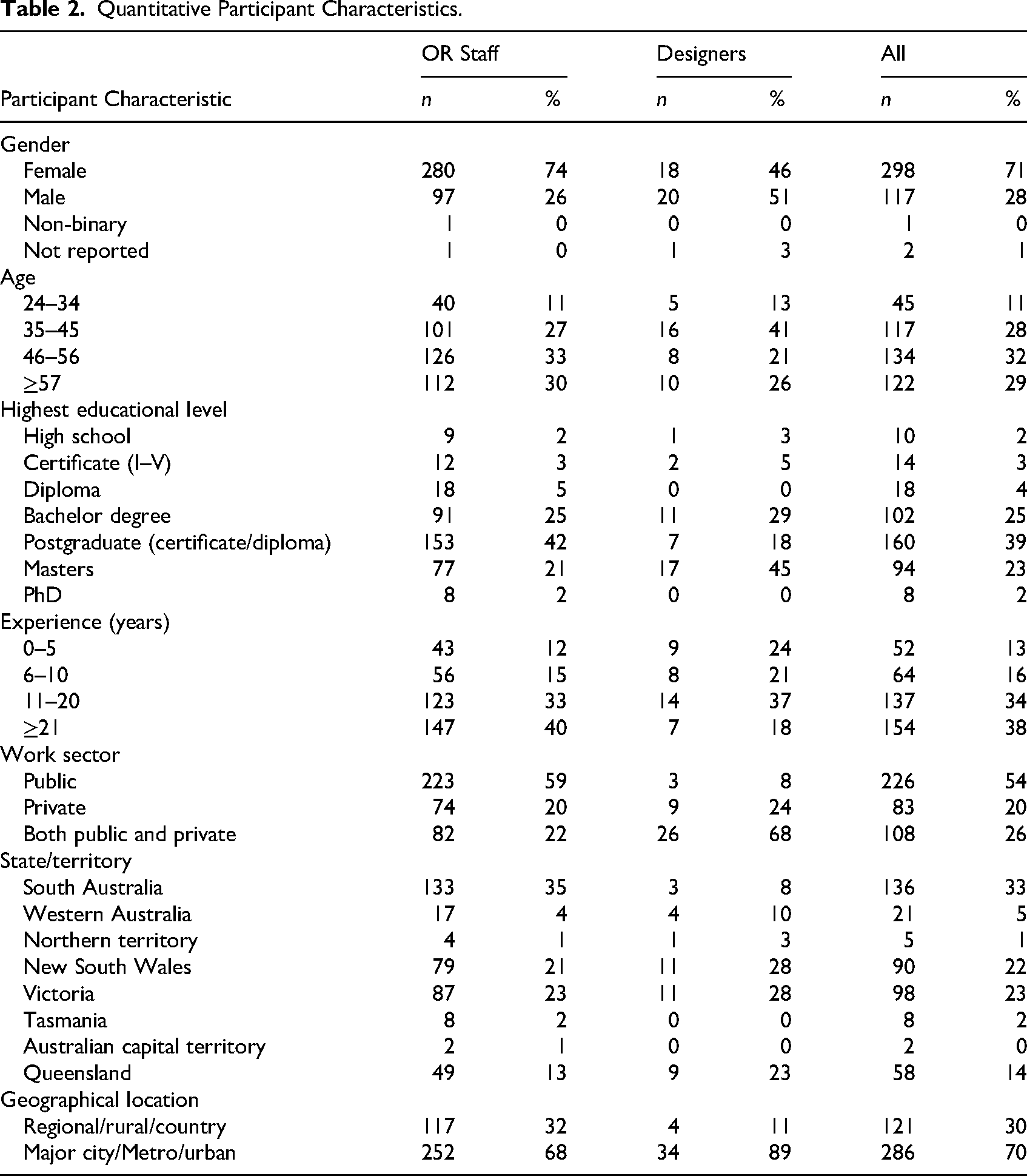
A total of 418 participants completed the questionnaire, representing all Australian states and territories. Most were nurses (65%), followed by surgeons (17%), anesthetists (8%), designers (9%), and technicians/orderlies (1%) (Table 1). Over half worked in the public sector, and most were based in major cities. Participants ranged from 24 to 78 years (M = 49.6) and were predominantly female. Demographics are summarized in Table 2.
Quantitative Participant Characteristics.
OR Staff Roles, Experience, and Expertise
OR staff demographics are summarized in Table 3. Most OR staff were aged 46–56 years (M = 49.7) OR staff were mainly metropolitan-based, with some regional/rural representation among nurses and surgeons. Anesthetists were less represented in rural settings, aligning with Australian models of care where general practitioners often deliver anesthetic care (Gilchrist et al., 2023). Nurses were mainly employed in the public sector, while surgeons and anesthetists reported a more even public and private distribution. Educational attainment was high, with many holding postgraduate qualifications. Clinical experience was extensive, averaging over 20 years. Most surgeons and anesthetists were senior consultants. Weekly OR hours averaged 30.8, with nurses and anesthetists often exceeding 39 hrs. Participants represented diverse surgical specialties. Nearly all worked in integrated surgical units, with fewer in gastroenterology/procedure rooms, single specialty, or co-located interventional suites.
Quantitative OR Staff Participant Characteristics.
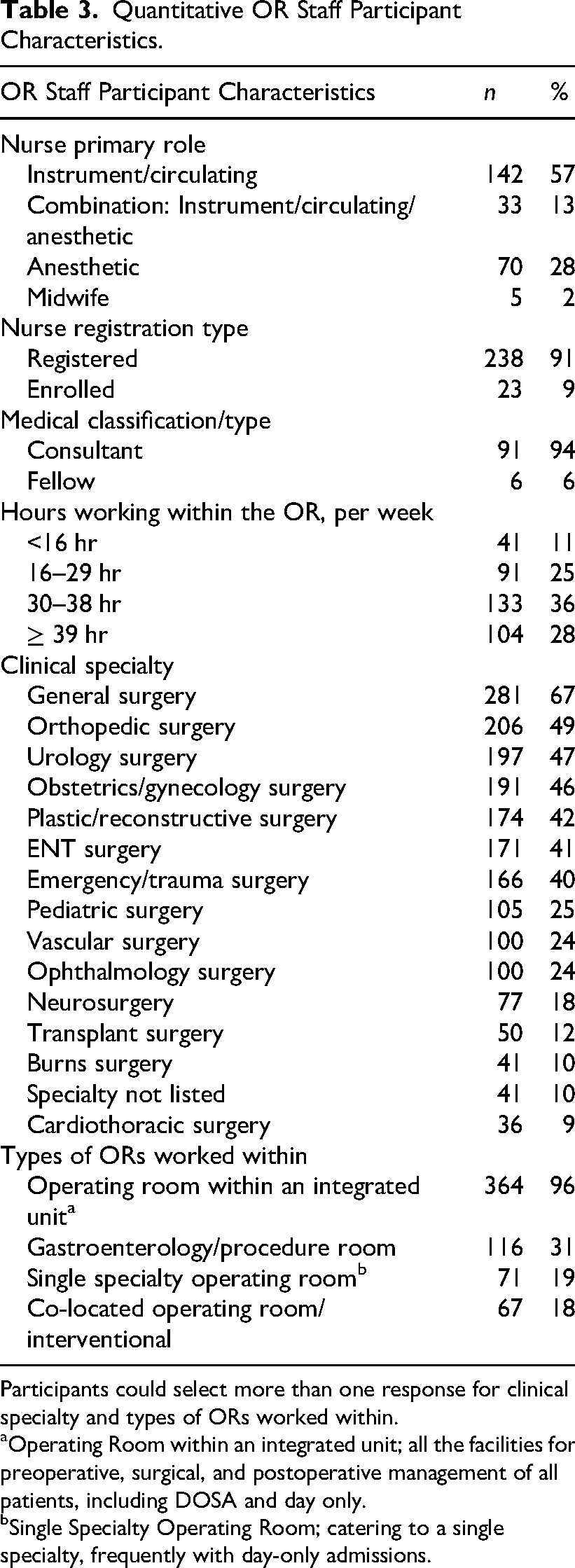
Participants could select more than one response for clinical specialty and types of ORs worked within.
Operating Room within an integrated unit; all the facilities for preoperative, surgical, and postoperative management of all patients, including DOSA and day only.
Single Specialty Operating Room; catering to a single specialty, frequently with day-only admissions.
Designer Roles, Experience, and Exposure
Designer demographics are summarized in Table 4. Most were aged 35–45 years (M = 47.9) and based in eastern Australian states where hospital redevelopment and health infrastructure investment are most concentrated. Architects comprised the largest professional group and held advanced qualifications, reflecting the complexity of healthcare projects. Designers averaged 13.9 years of experience. Designers were asked to report the number of hours of OR work they had observed to understand their exposure to clinical practice. While the mean number of observed patient care hours was 361.92 (SD = 1117.72), the median was substantially lower at 10 hr, indicating a small number of participants reported extensive clinical observation. Similarly, the mean number of OR projects involved was 69.82 (SD = 202.48), with a median of 10, again reflecting a highly skewed distribution (Online Supplementary Figure 1). This variability may influence how design decisions reflect clinical workflow and safety needs.
Quantitative Designer Participant Characteristics.
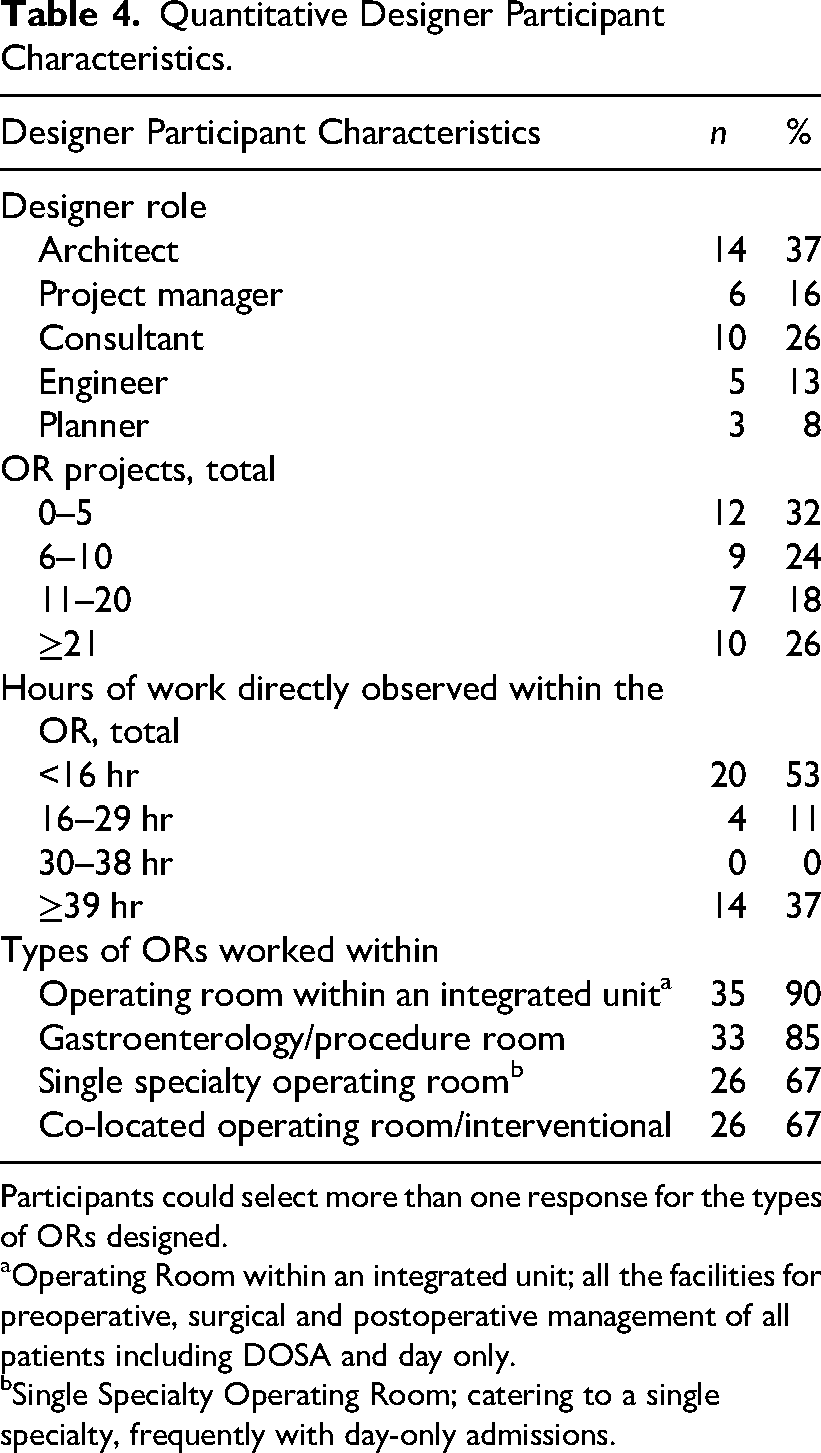
Participants could select more than one response for the types of ORs designed.
Operating Room within an integrated unit; all the facilities for preoperative, surgical and postoperative management of all patients including DOSA and day only.
Single Specialty Operating Room; catering to a single specialty, frequently with day-only admissions.
Shaping the OR: Engagement and Experiences
Engagement of OR staff in design planning was generally limited, with two-thirds reporting no prior involvement (N=166, 66%). Engagement included attending staff meetings, reviewing plans, providing feedback, or contributing to user groups. Among those who participated (N = 126), nurses and anesthetists were most engaged, while surgeons and technicians/orderlies were least involved (Figure 2). A summary of engagement is presented in Table 5. Participation most often took the form of providing feedback on floor plans or simulations, with fewer involved in sustained or embedded roles such as user group membership or developing functional briefs. These findings align with qualitative insights indicating that staff engagement was largely consultative rather than collaborative.
Engagement of OR staff in design planning was generally limited, with two-thirds reporting no prior involvement.
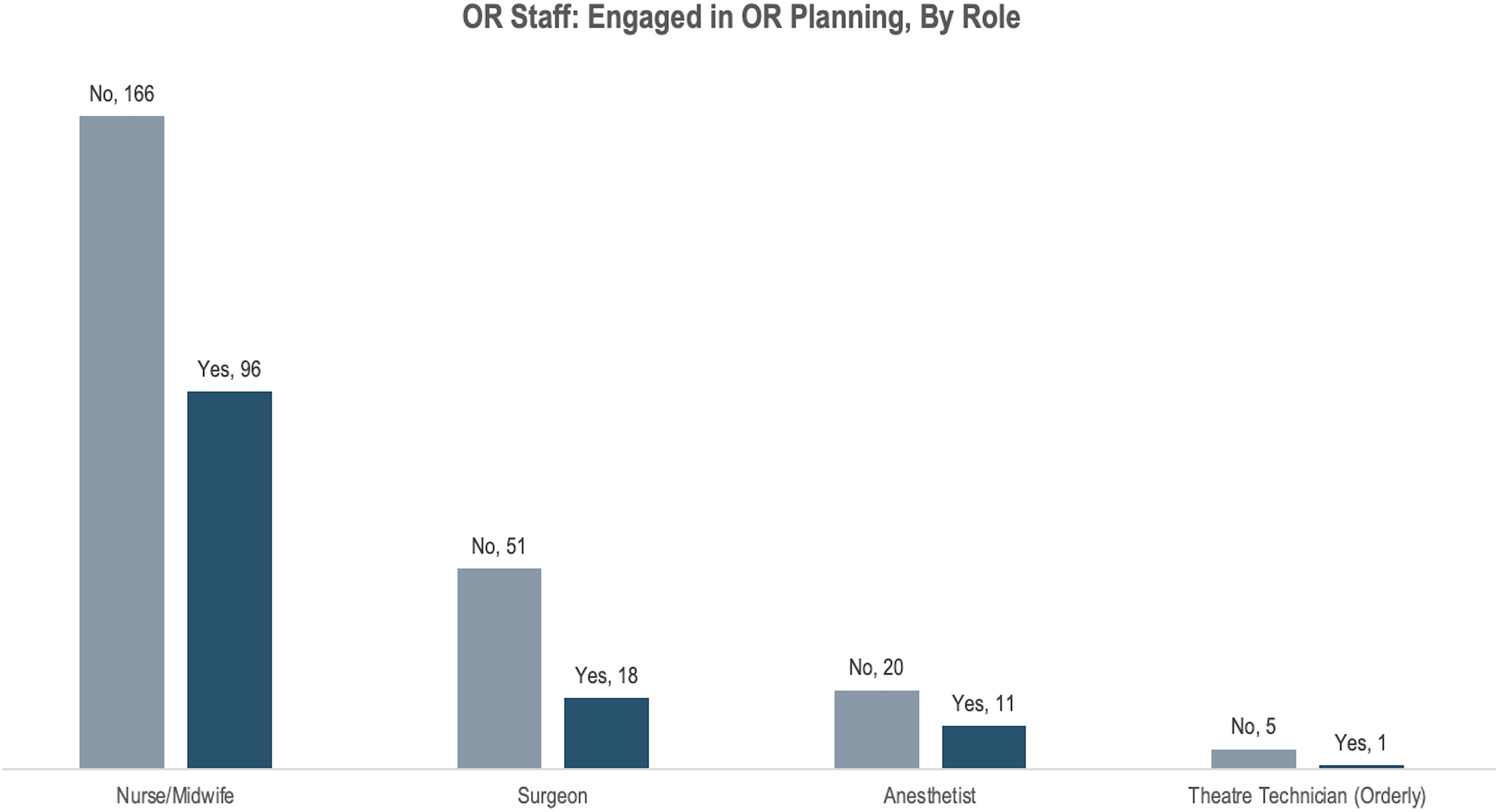
Or Staff Engagement in Design Planning, by Role.
Summary of Engagement in Design Planning.
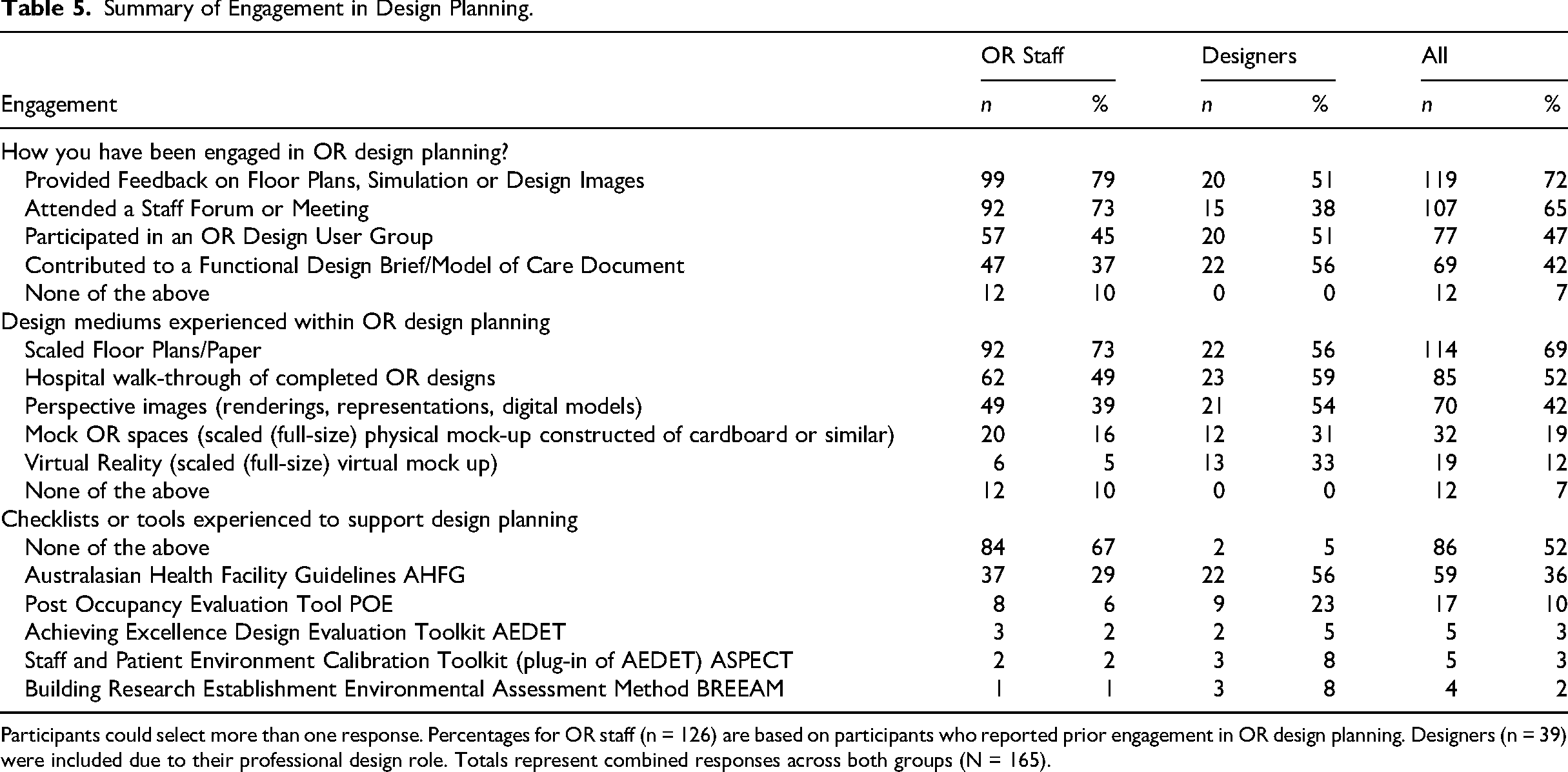
Participants could select more than one response. Percentages for OR staff (n = 126) are based on participants who reported prior engagement in OR design planning. Designers (n = 39) were included due to their professional design role. Totals represent combined responses across both groups (N = 165).
Exposure to design tools varied, with floor plans, walkthroughs, and images most common, while advanced methods like VR were rare, particularly among OR staff (Figure 3). The AusHFG was most frequently identified resource used to support planning, while other resources were rarely referenced, indicating variable integration of formal evaluation methods. When raising safety concerns, most OR staff did so during floor plan or simulation reviews, with others engaging through discussions with managers, colleagues, or designers directly (Figure 4). Nurses were more likely to raise concerns through managerial or peer channels, while anesthetists and surgeons often engaged through formal user groups or direct communication with designers. Very few OR staff participants (2%) reported not raising safety concerns during design planning. Participants consistently rated nurses as the most critical contributors to OR design, with each professional group rating their own role as most critical to the design process, reflecting patterns of self-prioritization (Supplementary Table 1). Collectively, these findings indicate the inconsistent inclusion of clinical voices in OR design and demonstrate gaps in interdisciplinary collaboration during the planning process.
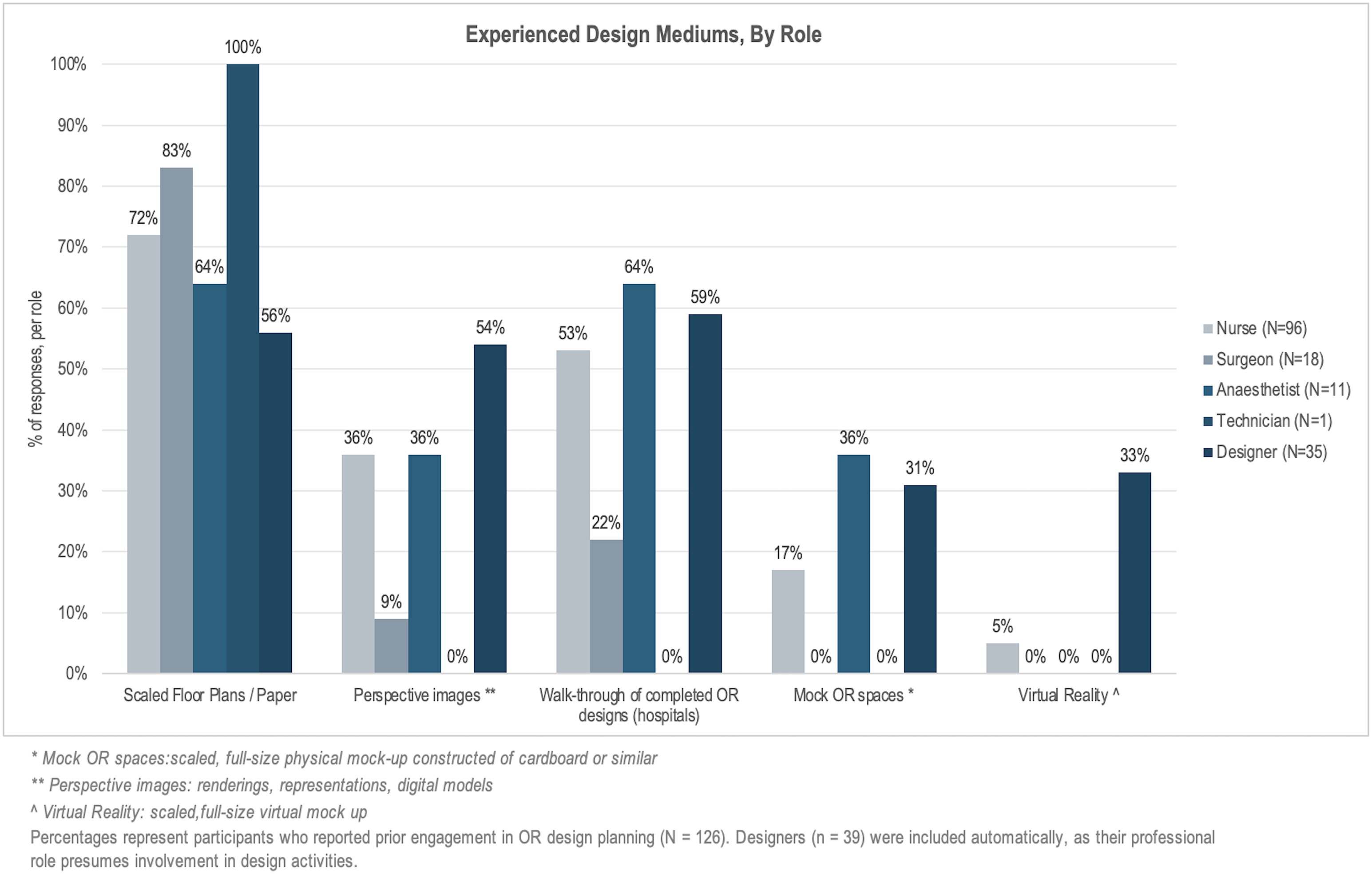
Experienced Design Mediums, by Role.
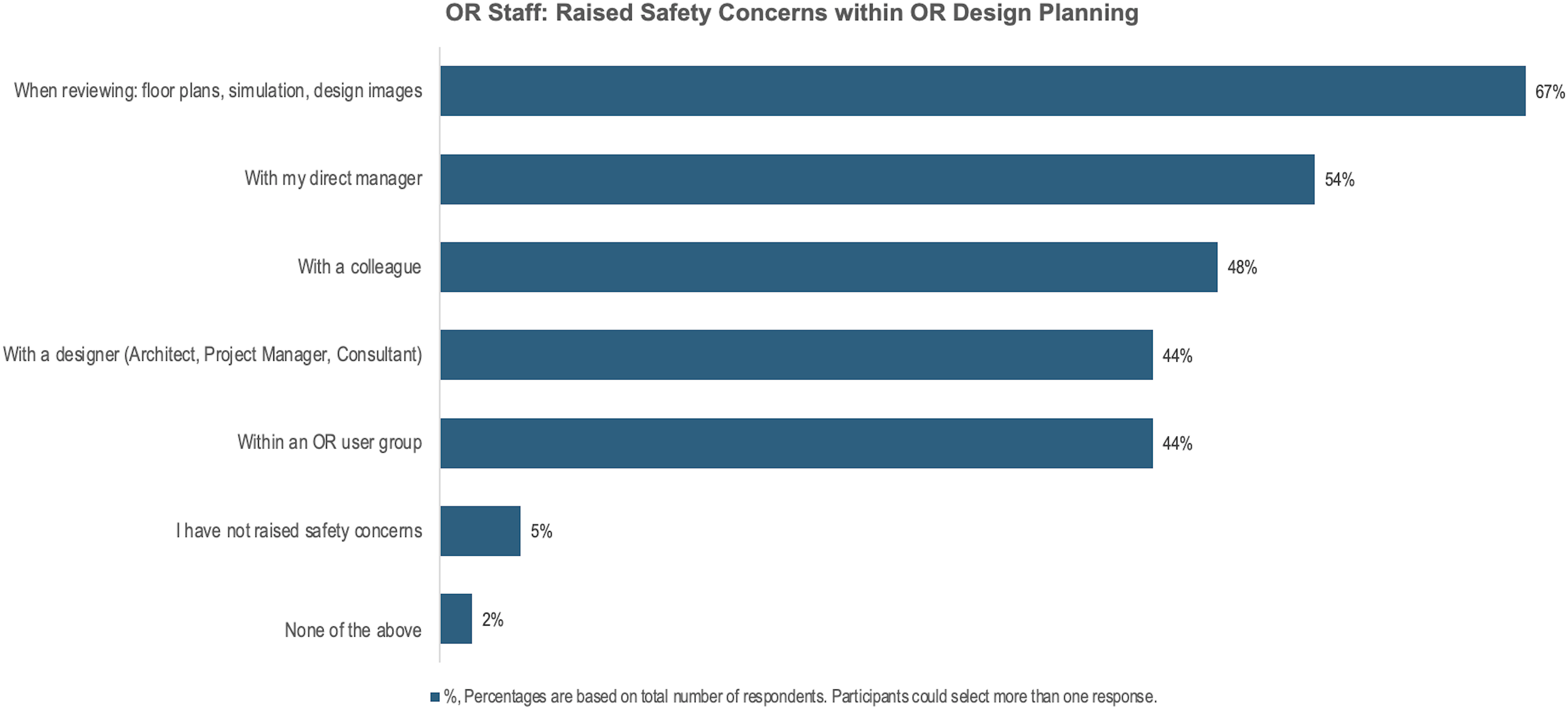
Safety Concerns Raised by OR Staff, Within Design Planning.
Design Challenges Experienced and Observed by Designers
Among designer respondents (n = 39), survey items exploring observed challenges during OR planning processes indicated hierarchy-driven decision-making, dominance by certain roles, and blind spots from poorly timed contributions. Common concerns raised by staff included space and equipment storage, equipment positioning to reduce strain/injury, alarms, travel distances, and cleanliness. Issues such as OR doors, acoustics, and trip hazards were also noted. Designers with greater OR project experience were more likely to encounter discussions on cleanliness, equipment positioning, overlooked workflow considerations, and nursing representation in user groups (Table 6).
Designers Observed/Experienced Within OR Design Planning.
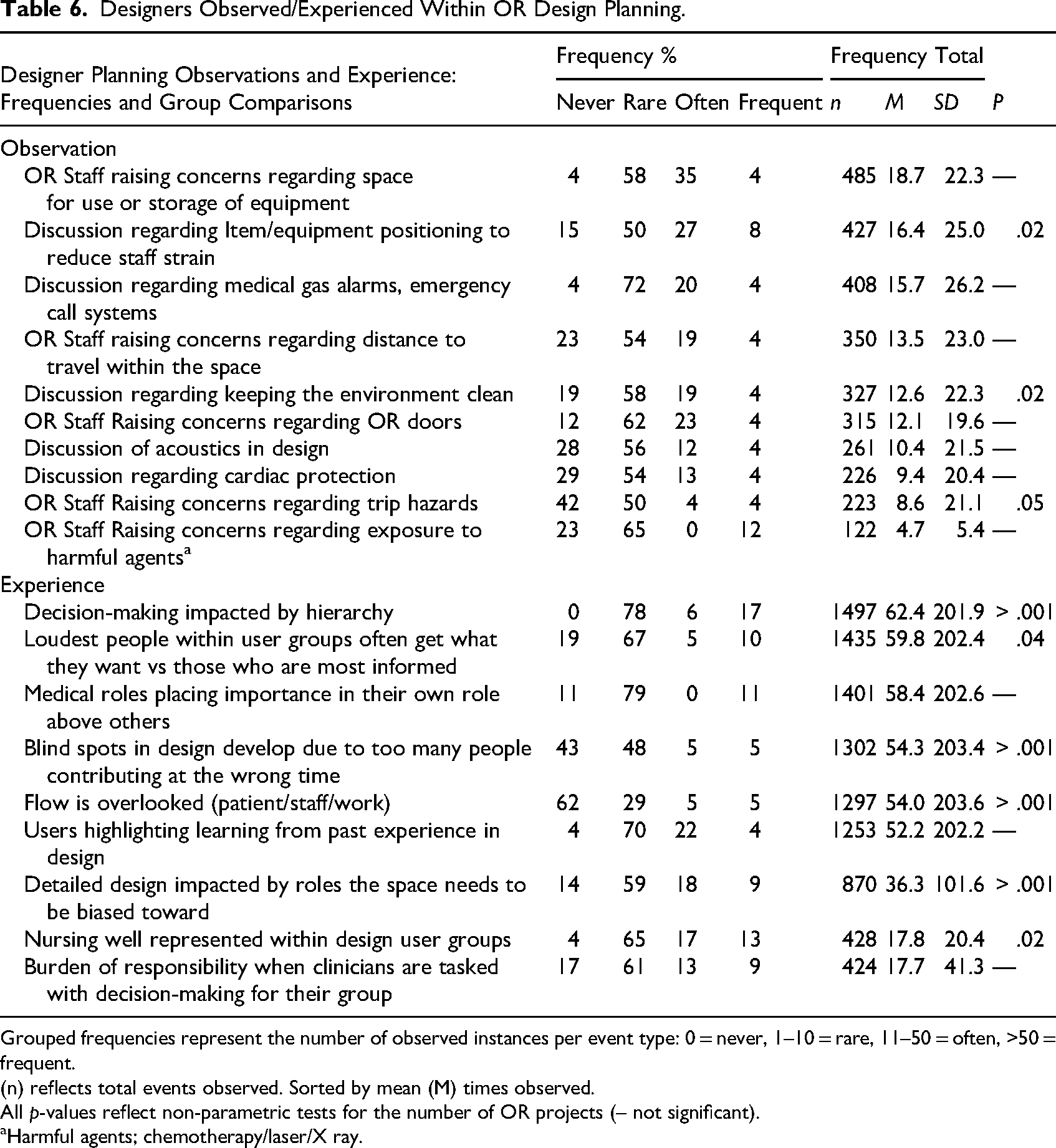
Grouped frequencies represent the number of observed instances per event type: 0 = never, 1–10 = rare, 11–50 = often, >50 = frequent.
(n) reflects total events observed. Sorted by mean (M) times observed.
All p-values reflect non-parametric tests for the number of OR projects (– not significant).
Harmful agents; chemotherapy/laser/X ray.
Awareness and Use of Standards/Guidelines
Among participants with prior OR design experience, more than half reported not using any listed checklists or tools during planning (Table 5). Awareness of standards was generally high, but application was inconsistent (Online Supplementary Table 2). OR staff most often referenced standards informally in discussions or independent review, while designers applied them formally in team decisions or integrated planning. These findings suggest a gap between awareness and the systematic application of standards/guidelines.
Perceived Capabilities, Barriers, and Enablers to Design Participation
Responses are presented separately for OR staff and designers to reflect differences in professional positioning within design processes. Participants rated barriers, enablers, and their own capabilities related to engaging in OR design planning (Table 7). There was strong agreement regarding the importance of clinical knowledge and experience. Items related to current practice, familiarity with standards, and OR-specific requirements, such as airflow, storage, and workflow, were ranked highly. Despite valuing standards, findings have demonstrated that knowledge and application of standards were inconsistent, highlighting a disconnect between perceived importance and practice. OR staff emphasized operational knowledge, while designers valued environmental and design expertise, reflecting how professional background and experience shape perceptions of relevant capabilities. The most reported barrier was not being invited to participate, followed by concerns about whether contributions were heard or respected. Other barriers include interpersonal conflict and planning complexity. Designers more commonly reported concerns about conflict, while OR staff more strongly agreed that their perspectives were overlooked. Key enablers included clear communication, managers facilitating active end-user involvement, relevant experience, and protected time to contribute. VR and simulation were also viewed as helpful. Self-rated capability was moderate to high overall, reflecting differences in exposure and role relevance. Designers reported the greatest confidence in their own knowledge/skill. These findings suggest that both access and professional identity shape readiness to engage meaningfully in OR design processes.
Key enablers included clear communication, managers facilitating active end-user involvement, relevant experience, and protected time to contribute.
Capabilities, Barriers, and Enablers to Design Participation.
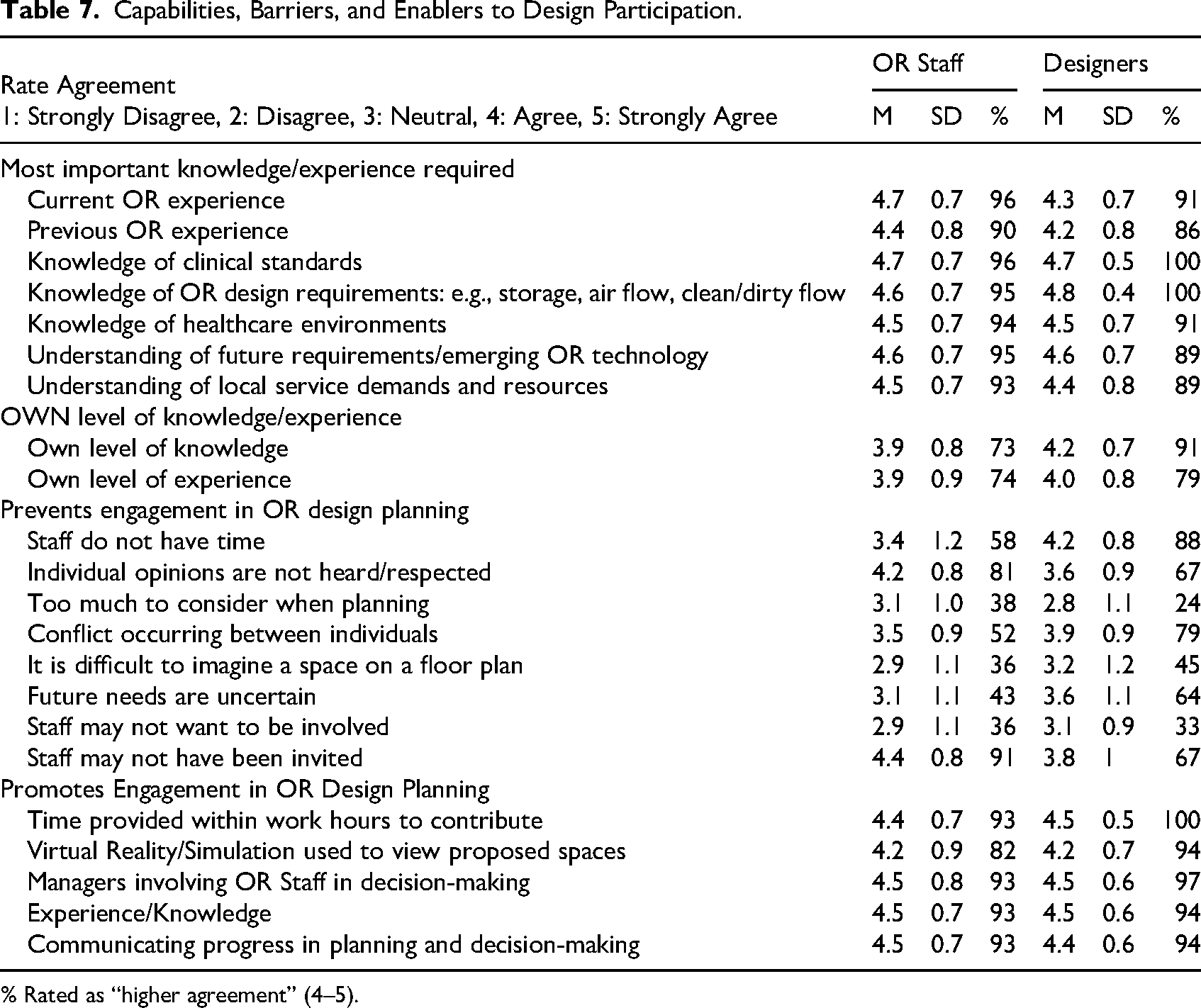
% Rated as “higher agreement” (4–5).
Prioritization of Safety in the OR Built Environment
Safety prioritization is presented here as an expression of how professional experience shapes design perspectives within planning processes. Participants ranked predefined OR design considerations across patient safety, staff safety, physical environment, and building structure, summarized in Table 8. Access and proximity to support were the top-ranked patient safety priority, while ergonomics emerged as the top priority for staff safety. Fixed structures and room layout were most important within the physical space domain, and storage, including stock, equipment, and waste, ranked highest for building structure. While there was general agreement on the importance of these elements, the professional role influenced how specific aspects were valued. Designers focused on infrastructure-level concerns such as air quality and structural placement, while OR staff prioritized practical elements like equipment access and safe movement. Anesthetists placed greater weight on ergonomics and ease of movement than surgeons; nurses rated storage higher, while surgeons emphasized communication/information technology and proximity to adjacent clinical areas higher. Prior design experience and demographic factors also shaped priorities, with less experienced participants focusing more on physical elements and younger participants valuing access to support. Despite these differences, there was strong consensus around key safety issues, especially those affecting patients among both OR staff and designers. This shared prioritization reflects a broad alignment and patient safety focus within OR Design.
Access and proximity to support were the top-ranked patient safety priority, while ergonomics emerged as the top priority for staff safety.
Ranked Safety Importance Across Four Domains: Patient Safety, Staff Safety, Physical Space, Building Structure.
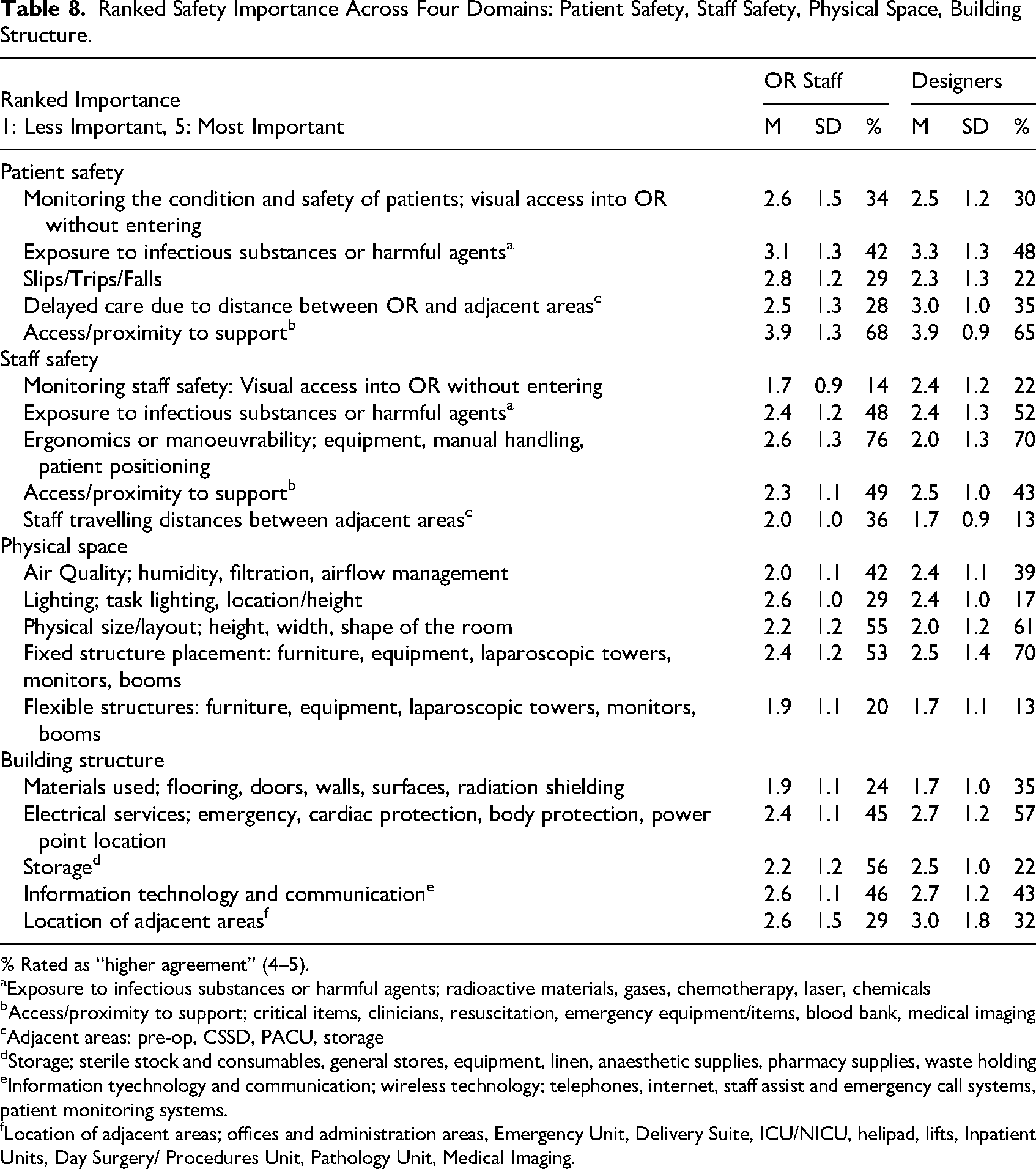
% Rated as “higher agreement” (4–5).
Exposure to infectious substances or harmful agents; radioactive materials, gases, chemotherapy, laser, chemicals
Access/proximity to support; critical items, clinicians, resuscitation, emergency equipment/items, blood bank, medical imaging
Adjacent areas: pre-op, CSSD, PACU, storage
Storage; sterile stock and consumables, general stores, equipment, linen, anaesthetic supplies, pharmacy supplies, waste holding
Information tyechnology and communication; wireless technology; telephones, internet, staff assist and emergency call systems, patient monitoring systems.
Location of adjacent areas; offices and administration areas, Emergency Unit, Delivery Suite, ICU/NICU, helipad, lifts, Inpatient Units, Day Surgery/ Procedures Unit, Pathology Unit, Medical Imaging.
Safety and Workflow Challenges Encountered by OR Staff
This section reports OR staff self-reported observations and experiences within existing OR environments, rather than direct observation conducted as part of this study. These findings draw on OR staff observations and experiences within the OR, highlighting the safety and workflow challenges they encounter in practice and how these may inform design priorities. Observations and experiences across OR settings revealed frequent and varied safety and workflow issues, with notable differences by staff role and characteristics (Table 9). Median and IQR values indicate the typical number of observations per month, while frequency groupings reflect the proportion of responses across categories. Tripping over cables or equipment, injuries caused by trip hazards, door malfunctions, exposure to harmful agents, and cluttered environments were most frequently observed. Delays in patient care due to walking distances or communication barriers caused by noise occurred less often. Experiential data highlighted OR staff frequently adjusted movement to avoid hazards and reported long walking distances to collect items for patient care and transport patients. While a high burden of trip-related risks was evident, fewer participants reported personally sustaining an injury from such hazards. Differences emerged by gender, years of experience, and role. Gender influenced reports of trip hazards and walking distances, while years’ of experience affected perceptions of trip hazards and travel related delays. Nursing role differences, such as circulating vs anesthetic roles, were evident for both trip related incidents and walking distances. Most hazards varied across roles, reflecting differences in responsibilities and role based workflow. These findings indicate the persistence of design related hazards and the uneven impact across staff groups. Trip hazards, clutter, and spatial inefficiencies were consistently reported, while noise and physical workload introduced additional barriers. The variability across roles demonstrates the need for inclusive, interdisciplinary design processes and role specific strategies to improve OR safety and workflow.
OR Staff Observed/Experienced Within the OR.
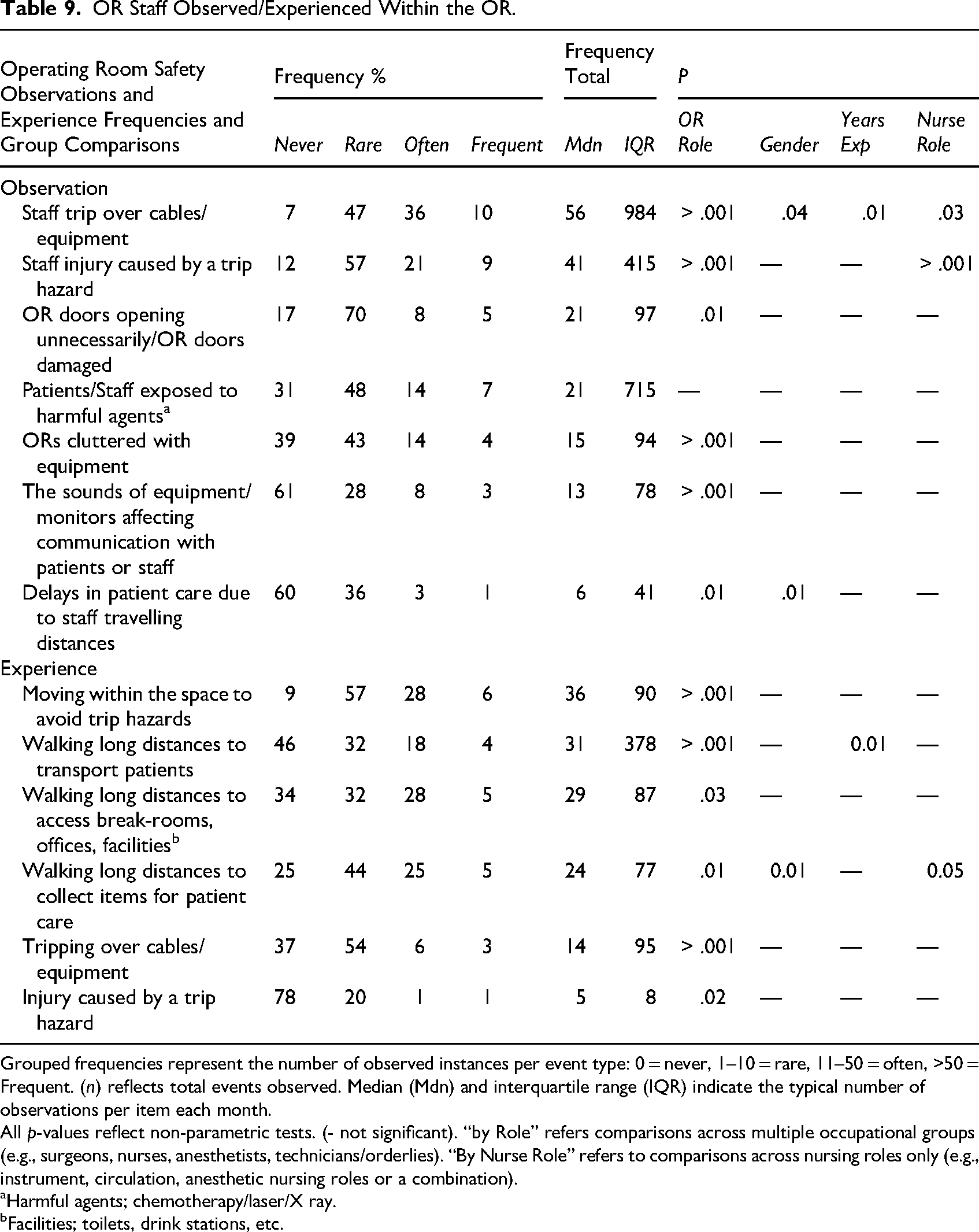
Grouped frequencies represent the number of observed instances per event type: 0 = never, 1–10 = rare, 11–50 = often, >50 = Frequent. (n) reflects total events observed. Median (Mdn) and interquartile range (IQR) indicate the typical number of observations per item each month.
All p-values reflect non-parametric tests. (- not significant). “by Role” refers comparisons across multiple occupational groups (e.g., surgeons, nurses, anesthetists, technicians/orderlies). “By Nurse Role” refers to comparisons across nursing roles only (e.g., instrument, circulation, anesthetic nursing roles or a combination).
Harmful agents; chemotherapy/laser/X ray.
Facilities; toilets, drink stations, etc.
OR Staff and Designer Perspectives on Safety Focused Design
To explore participants’ understanding of how built environment features influence safety and the value of clinical involvement in design, Likert scale statements were developed based on Phase 1 findings. Responses showed strong agreement, reinforcing key concepts from the broader mixed methods analysis (Table 10). There was widespread consensus that OR staff bring valuable perspectives, and strong endorsement of the importance of flexible OR spaces to accommodate emergencies and surgical specialty variation, timely access to essential items, and support for safe care. Many acknowledged that ineffective workflow, often shaped by the built environment, creates challenges, and agreed that design teams are not always reflective of end users, reinforcing a perceived disconnect. Moderate agreement was observed for technical concepts, such as the influence of spatial layout on staff and patient flow, and that design flaws often only emerge post-occupancy. Lowest agreement related to balancing stakeholder input, reflecting differing views on inclusive engagement. Comparing OR staff and designers revealed distinct perspectives. OR staff expressed concern that functional elements may be overlooked and that design problems often emerge post-occupancy. They emphasized that OR layout is shaped by fixed infrastructure, such as power access and booms. Designers, in contrast, focused on flexibility to accommodate varied surgical procedures and the challenge of balancing OR staff input during design planning. These differences highlight distinct priorities: OR staff focus on operational and functional needs, while designers emphasize spatial adaptability and structural considerations. Collectively, these findings demonstrate patterns consistent with earlier qualitative insights while also revealing variation across professional groups, illustrating the complexity of safety centered OR design where technical expertise and experiential knowledge jointly shape how design is understood, implemented, and evaluated.
Agreement With Qualitative Concepts.
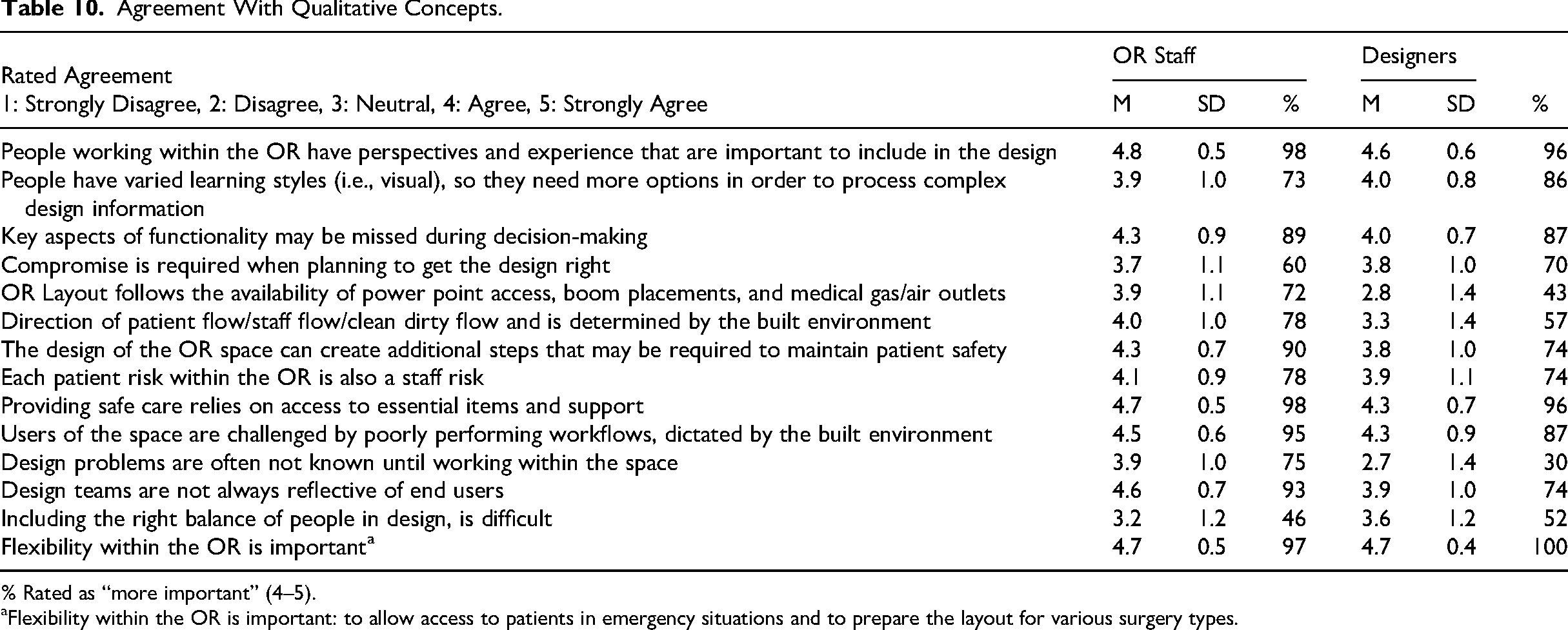
% Rated as “more important” (4–5).
Flexibility within the OR is important: to allow access to patients in emergency situations and to prepare the layout for various surgery types.
Discussion
This study reveals that staff involvement in OR design planning is limited due to entrenched hierarchies, fragmented communication, and a lack of structured participatory frameworks and institutional support. OR staff consistently prioritize safety concerns grounded in daily work, including ergonomics, hazards, clutter, and workflow efficiency, shaped by direct interaction with spatial layouts, equipment, and clinical processes. When engaged, staff identify safety issues, demonstrating a clear understanding of the impact of design on workflow and care delivery. Despite experience and willingness, OR staff reported limited involvement, with perceptions of exclusion and communication breakdowns presenting greater barriers than lack of interest or capability. This demonstrates a disconnect between staff readiness and systems enabling meaningful involvement. Environmental challenges are unevenly experienced across roles, yet staff insights provide operationally specific strategies to mitigate safety risks. Hierarchical dynamics were recognized as influencing OR design planning, limiting participation of diverse roles, aligning with Etherington et al. (2021), who found that gender composition shapes who is heard and respected in OR teams. Deliberate strategies to address power imbalances through equitable engagement and inclusive leadership may support improvements in both design outcomes and OR staff involvement. These findings position safety not as an isolated design outcome, but as a central lens through which OR staff interpret and engage with design planning processes.
Designers value clinical input but face challenges in achieving balanced stakeholder representation, timely engagement, and translating clinical perspectives into actionable decisions. OR staff engagement in design planning provides designers with insights into clinical realities. Designers rely on select staff input to identify workflow inefficiencies and safety risks due to limited direct observation and inconsistent use of design tools such as checklists or simulations. Both OR staff and designers identified space, ergonomics, and storage as central to safe OR environments. OR staff prioritized ergonomics, access to support and essential items, and storage, while designers confirmed these concerns were raised in planning discussions, including equipment positioning and storage. Recurring issues included door functionality, acoustics, and trip hazards. OR staff strongly agreed that poor design can cause inefficient workflows and that design teams often lack adequate OR end-user representation. Differences in how the built environment is experienced reflect variations in responsibilities, risk exposure, and spatial interaction, yet consensus on key safety concerns provides a foundation for collaboration. OR staff indicated design problems, such as poor layout or workflow inefficiencies, were often identified post-occupancy, outside formal evaluation processes, suggesting missed opportunities for feedback and iterative improvement. Poorly considered layouts may introduce safety hazards, increase staff workload, and, in some cases, compromise patient care, placing additional pressure on staff to work around environmental limitations. Inefficient workflows caused by design flaws, such as congested spaces or limited access to essential equipment, can heighten staff stress and workload. Oh et al. (2024) highlighted stressors within the OR include noise, disorganized flow, poor lighting, clutter, and insufficient facilities. Improved design may reduce staff stress and enhance patient safety.
Professional background and experience shape how safety is understood and addressed. When understanding is not co-constructed through collaboration, design outcomes may fail to meet diverse needs. Differences between staff and designers reflect competing priorities consistent with realistic conflict theory (Sherif, 1958). OR staff viewed participation as critical for safeguarding safety and workflow, whereas designers frequently worked within constraints of budget, space, and regulation. These competing priorities position engagement as a form of scarce resource negotiation. Moving from consultation to collaboration, by embedding staff voices throughout planning, may strengthen alignment between critical operational needs and design decisions. Gaps remain between awareness of standards and consistent application, highlighting the need for structured collaboration and embedded feedback loops. Persistent differences between design intent and operational reality reveal limitations in current participatory practices. Without structured, iterative processes, participatory design can inadvertently create barriers rather than solutions (Lame et al., 2023; Palmer et al., 2019). Addressing these challenges requires integrating end-user insights and design expertise to create safe, adaptable environments aligned with practice realities. This study extends existing participatory design literature by empirically demonstrating how professional role, experience, and hierarchical positioning shape engagement patterns within OR-specific planning contexts. By integrating national survey data with grounded qualitative insights, the findings move beyond general calls for participation to identify concrete relational, structural, and perceptual factors that influence whether engagement is experienced as meaningful.
Moving from consultation to collaboration, by embedding staff voices throughout planning, may strengthen alignment between critical operational needs and design decisions.
Mixed Method Integration
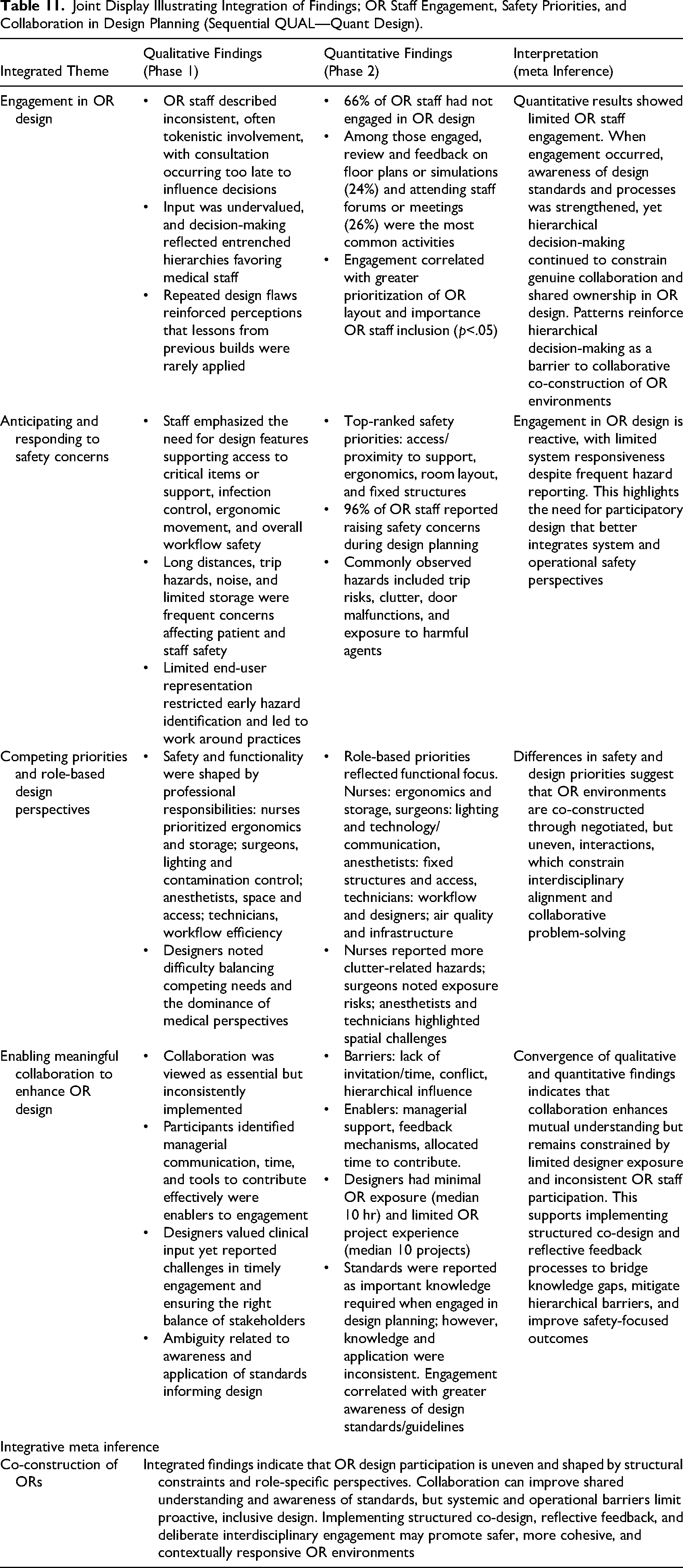
Mixed methods integration combined qualitative and quantitative data to assess coherence (Guetterman et al., 2015). In this study, integration highlighted patterns in safety priorities and interdisciplinary engagement in OR design. Qualitative findings informed the quantitative phase and interpretation. Staff experiences and motivations were captured qualitatively, while quantitative data showed patterns in safety observations and engagement. Designers’ challenges emerged qualitatively; quantitative data highlighted their limited observation of clinical work. Integration clarified role based differences, why they persist, and how they manifest. A key insight is the relational nature of staff engagement, which is both a technical and affective process shaped by perceptions of respect, inclusion, and shared purpose. This approach illustrates how staff identified and responded to safety concerns and highlighted barriers and enablers to participation to meaningful participation. Conflicting design priorities stem from negotiations among roles, influenced by power dynamics, role expectations, and experiences. These negotiated outcomes determine the balance, or imbalance, of priorities reflected in the final design. This interdisciplinary lens reconciled user and designer perspectives, contributing to a mid range explanatory theory framing OR design as a social process shaped by negotiation, collaboration, and shared purpose. Rather than functioning as confirmatory validation, the quantitative phase enabled examination of the distribution, variation, and relative emphasis of qualitatively derived concepts across a broader professional group. Table 11 illustrates how qualitative insights informed quantitative measures and subsequent meta inferences.
Joint Display Illustrating Integration of Findings; OR Staff Engagement, Safety Priorities, and Collaboration in Design Planning (Sequential QUAL—Quant Design).
Conclusion
This study highlights the significant role OR staff expertise can play in shaping safe and functional surgical environments and reinforces the need to embed their voices throughout planning, moving beyond consultation to genuine collaboration. Differences between OR staff and design perspectives reflect the complexity of OR planning, where technical and experiential knowledge must converge. Strengthening engagement through orientation to design processes, access to immersive technologies, and leadership approaches that promote equity and interprofessional dialogue may strengthen the integration of clinical expertise, inform spatial decisions, and bridge gaps between design intent and operational needs. Enhancing feedback loops and identifying latent issues early can further support the translation of clinical insights into effective design configurations. Transparent reporting of project outcomes and lessons learned would also contribute to sector-wide learning. Future efforts should focus on integrating clinical insights into standardized frameworks, fostering interdisciplinary collaboration, and evaluating the impact of inclusive design strategies on safety and performance. By adopting iterative, evidence-informed approaches, healthcare organizations are better positioned to create OR environments that better reflect real-world needs and support high-quality care.
Limitations
Inclusion criteria allowed for participants with relevant experience within the past 5 years, potentially affecting recall for questions related to observation or experience. Participation was voluntary and recruitment occurred through professional networks and membership organizations, which may have attracted individuals with particular interest in OR design engagement. Recruitment presented challenges due to distribution via professional membership organizations and time constrained professionals, though 434 participants across both phases reflects the relevance of the topic. Although multiple focus groups were initially planned to enable role-specific discussion, high clinical workloads and service pressures during the COVID-19 pandemic limited availability for group participation, resulting in greater reliance on individual interviews. Forced ranking items helped surface design and safety priorities but may have been time consuming to complete, contributing to partial responses. These patterns likely reflect both survey design and participant workload. The study was conducted in Australia, therefore professional roles and models of design planning may differ internationally, which may limit transferability. The questionnaire used in this study was newly developed to capture OR staff and designer perspectives on OR design engagement and safety. While informed by prior research and empirical findings, it has not undergone formal psychometric validation beyond pilot testing for clarity and feasibility. The inclusion of designers strengthened the interdisciplinary perspective of the study; however, designer participation was smaller than OR staff groups across both phases. In addition, the study examined perceived and experienced impacts of the built environment rather than objectively measured environmental or clinical outcomes. While participant accounts provide valuable insight into how design is understood and navigated in practice, the study design does not permit attribution of specific safety or workflow outcomes to particular built environment features. Future research integrating environmental measurement or clinical outcome data with staff perspectives would support examination of causal relationships.
Implications for Practice
Embedding structured stakeholder engagement throughout design planning may strengthen the integration of clinical perspectives to inform decisions affecting workflow, safety, and care delivery.
There is a need to strengthen post-occupancy evaluation and feedback loops to support the identification and resolution of safety and workflow issues not evident during planning.
Expanding access to participatory design tools such as virtual reality, simulation, and mock-ups may enhance interdisciplinary collaboration and design literacy.
Developing shared design toolkits and resources can guide participatory processes, integrate evidence-based principles, and facilitate knowledge exchange across projects.
Supplemental Material
sj-docx-1-her-10.1177_19375867261454387 - Supplemental material for Operating Room Staff Engagement in Design Planning: A Mixed Methods Study of Professional Perspectives in Australia
Supplemental material, sj-docx-1-her-10.1177_19375867261454387 for Operating Room Staff Engagement in Design Planning: A Mixed Methods Study of Professional Perspectives in Australia by Kasey Irwin, Janet Kelly and Frank Donnelly in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-doc-2-her-10.1177_19375867261454387 - Supplemental material for Operating Room Staff Engagement in Design Planning: A Mixed Methods Study of Professional Perspectives in Australia
Supplemental material, sj-doc-2-her-10.1177_19375867261454387 for Operating Room Staff Engagement in Design Planning: A Mixed Methods Study of Professional Perspectives in Australia by Kasey Irwin, Janet Kelly and Frank Donnelly in HERD: Health Environments Research & Design Journal
Footnotes
Author Note
Frank Donnelly is now at the School of Nursing, Murdoch University, Western Australia. This study was approved by both the University of Adelaide Human Resource Ethics Committee (H-2020-34823/ H-2023-095) and Central Adelaide Local Health Network Human Resource Ethics Committee (CALHN 1374). The authors have no conflicts of interest to report. The authors received no financial support for the research, authorship, or publication of this article. GPT-5 mini (OpenAI, 2023) was used to assist with language refinement and article structure; all content, interpretation, and decisions remained solely the author's responsibility.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.