
Abstract

“Although myriad fixation options exist for arthrodesis of the first metatarsal–phalangeal joint, the literature is not clear regarding the ability to permit early weight bearing.”
Although myriad fixation options exist for arthrodesis of the first metatarsal–phalangeal joint, the literature is not clear regarding the ability to permit early weight bearing. I have recently begun using a novel technique that allows for immediate protective weight bearing employing elastic memory implants developed and used extensively in Lyon, France. The implant, termed Ti-Fuse (Memometal, Inc., Memphis, TN) is a ridged elastic nail of lengths of 35, 40, 45, and 50 mm and a “T” peg at the distal end constructed of pure titanium (Figure 1). The implant is exceedingly easy to place (Figure 2) and when performed properly will function like an elastic nail employed in pediatric diaphyseal fractures of the axial limbs. Following preparation of the joint surfaces using the surgeon’s technique of choice such as hand instrumentation contouring, crescentic saw resection of the articular surface, or power reamers, the first metatarsal–phalangeal joint is aligned according to the patient’s particular anatomy with slight extension and valgus of the hallux and no frontal plane rotation. With the first metatarsal–phalangeal joint maintained in the desired position, the plantar–medial aspect of the base of the proximal phalanx is penetrated with a 1.8-mm drill and the appropriate length Ti-Fuse is loaded onto the specially designed implant driver pliers and tamped into place until the “T” portion of the implant contacts the phalangeal cortex. The proper alignment is such that the implant will enter the phalanx in similar fashion as one would do for crossed compression screw fixation but instead of penetrating the lateral cortex of the first metatarsal, the implant will deflect off of the lateral cortical wall and into the medullary canal of the first metatarsal with the “T” portion of the device seated firmly against the cortex. The same process is then performed starting at the dorsal–medial aspect of the first metatarsal head angling distally into the base of the proximal phalanx. A static metallic staple is then added dorsally across the first metatarsal–phalangeal joint to limit potential for rotation during the consolidation process (Figure 3).
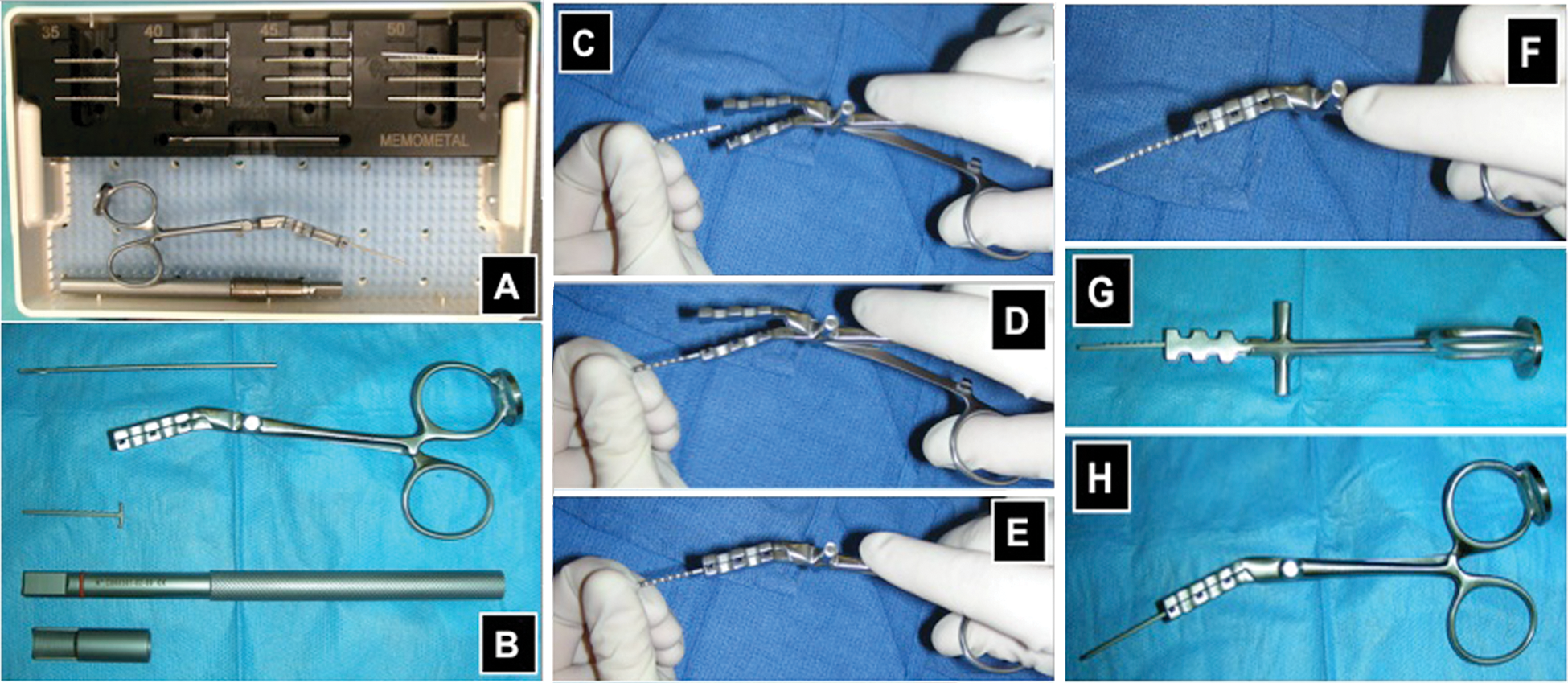
(A) Ti-Fuse instrument tray and implant set. (B) Close-up view, from top to bottom, of the 1.8-mm drill bit; implant driver pliers; 40-mm Ti-Fuse implant; impactor; impactor sleeve. The first step is to obtain the properly sized Ti-Fuse implant and to insert it into the implant driver pliers (C-F). Photograph of the Ti-Fuse implant secured within the implant driver pliers when viewed from the top (G) and side (H). Note the metallic expansion on the ring corresponding to the ring finger, which can accept contact from a mallet to begin to seat the implant; however, the pliers are usually simply manually inserted.
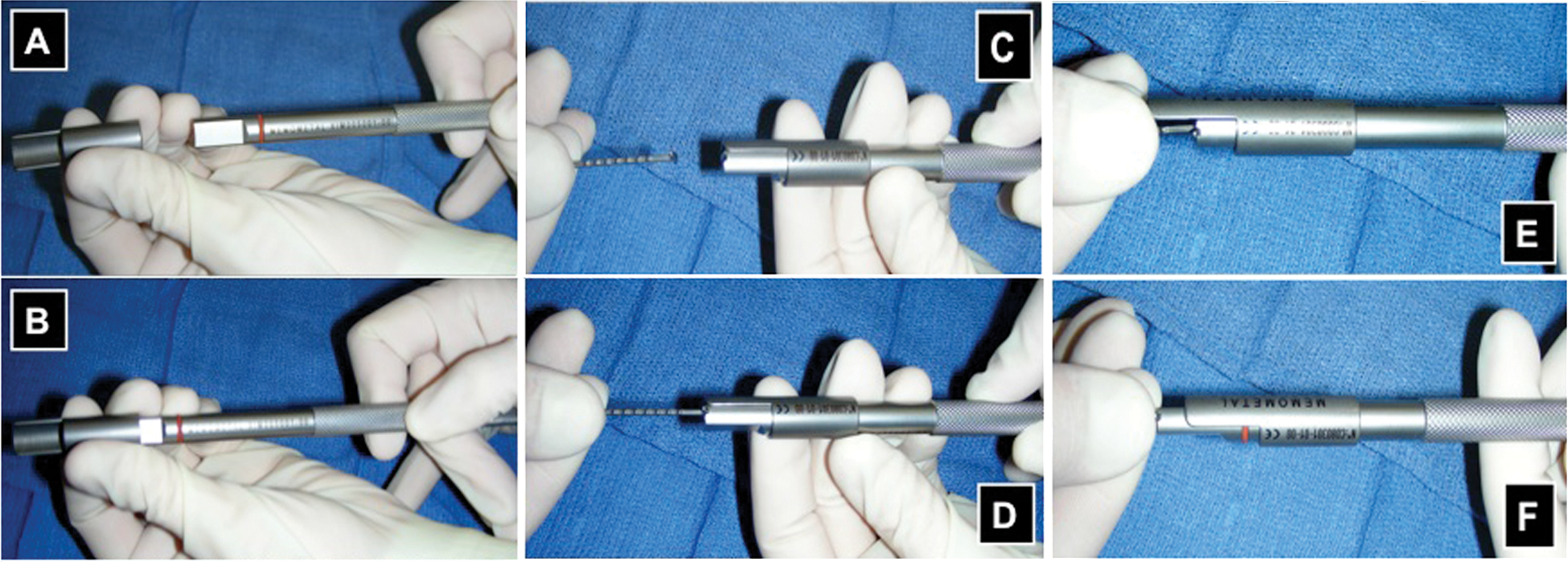
Once the Ti-Fuse implant is inserted into the bone it requires being impacted to generate compression. The impactor set-up consists of articulating two components together, the impactor itself (right side) and the impactor sleeve (left side) (A) by sliding the sleeve over the impactor itself (B). The Ti-Fuse is then placed within the groove at the end of the impactor (C and D) and the impactor sleeve is advanced distally until it contacts the bone surface (E). The impactor is then struck in controlled fashion with a mallet until the Ti-Fuse implant is fully seated (F).
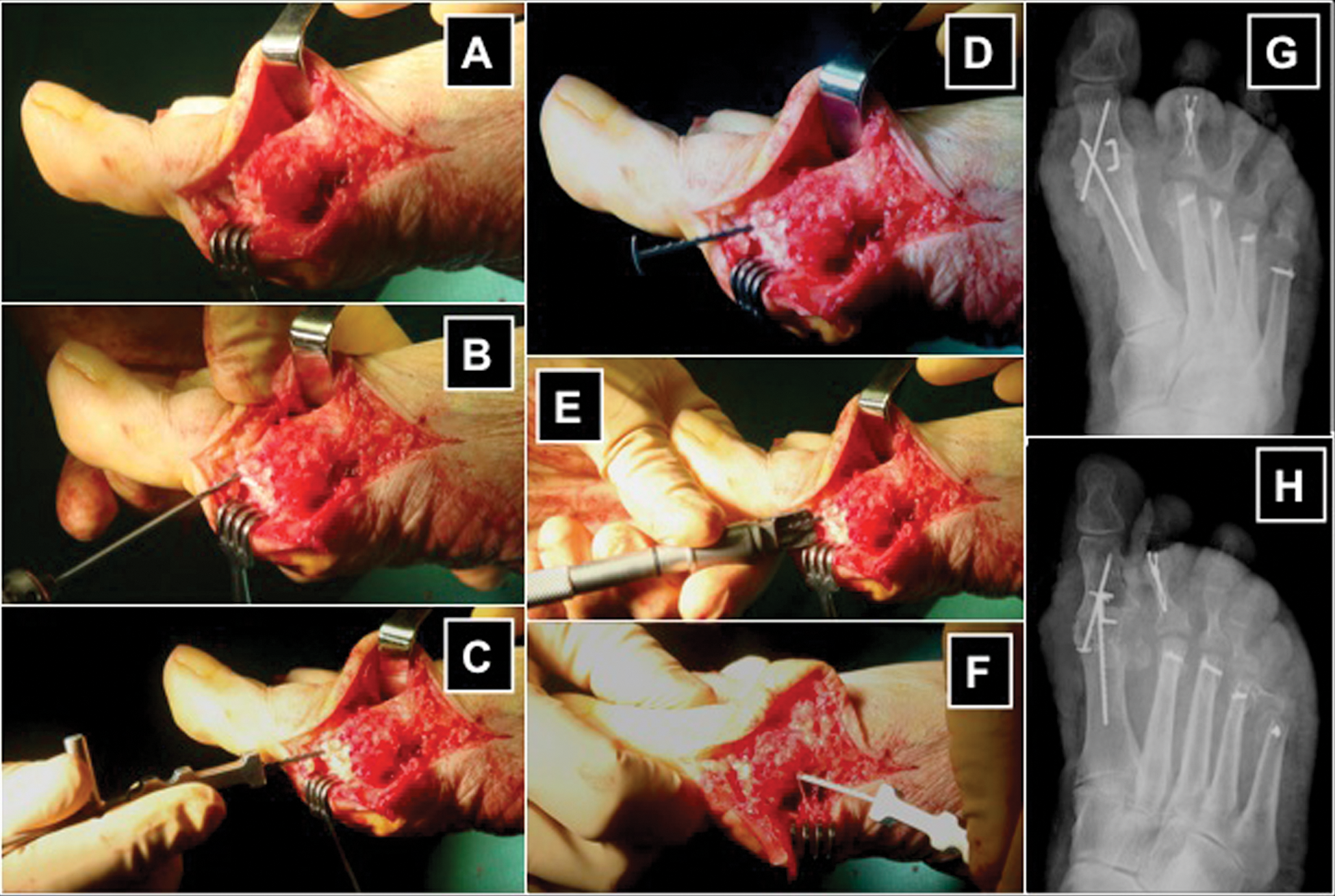
(A) Intraoperative photograph demonstrating medial approach to arthrodesis of the first metatarsal–phalangeal joint. (B) A 1.8-mm drill is employed to perforate the cortex about the base of the proximal phalanx and extends into the medullary bone of the first metatarsal head. The Ti-Fuse implant is then advanced into the predrilled hole until resistance if felt (C), at which time the implant driver pliers are removed (D). Note that the orientation of the “T” portion of the implant should be aligned at this point such that when it contacts the cortex of bone it will lay flush and allow for compression. The impactor and impactor sleeve is placed on the Ti-Fuse implant (E) and advanced with repeated controlled blows with a mallet until it sits flush against the cortex of bone. The same process is then repeated for the second Ti-Fuse implant from proximal to distal (F). The final step is to insert a static dorsal staple accross the midline of the first metatarsal–phalangeal joint. Postoperative anterior–posterior (G) and oblique (H) radiographs following first metatarsal–phalangeal joint arthrodesis with crossed Ti-Fuse implants and dorsal static staple, as well as, additional central metatarsal and toe procedures.
A recent unpublished study of 95 feet (83 patients) undergoing arthrodesis of the first metatarsal–phalangeal joint employing the technique described above and immediate weight bearing in a postoperative shoe revealed a nonunion rate of only 3.2% (3/95). In osteopenic bone, the presence of neuropathy, or excessive body weight, one or two supplemental Ti-Fuse implants and/or static dorsal staples are encouraged. Although additional scientific work needs to be conducted to determine the limitations of this internal fixation construct, I have been impressed with the ease of inserting the implants, removing them if needed, and reinserting them to a more appropriate configuration in a very timely manner and without the disruption to the osseous components that would occur if this was attempted with traditional forms of internal fixation. Finally,I have been equally impressed with the immediate stability afforded to the first metatarsal–phalangeal joint and the rapid nature in which solid clinical and radiographic arthrodesis has occurred.