
Abstract
The authors present a case of a 62-year-old male with a symptomatic isolated midfoot metastasis as the first clinical presentation of a primary pulmonary tumor. In this case of a metastatic adenocarcinoma, the lesion leading to diagnosis was located in the foot. The poor outcome and the sparse relevant literature are presented in brief.
“In our case of a metastatic adenocarcinoma, the lesion leading to diagnosis was located in the foot.”
Although the axial skeleton is a common site of metastases, the tarsal bones are rarely affected, especially by isolated metastases. A symptomatic isolated midfoot metastasis as the first clinical presentation of a primary pulmonary tumor is even less common.
Such a presentation can mislead the physician and considerably delay the diagnosis.
In our case of a metastatic adenocarcinoma, the lesion leading to diagnosis was located in the foot. The poor outcome and the sparse relevant literature are presented in brief.
Case Report
A 62-year-old previously healthy male was referred to our clinic with a 4-month history of midfoot pain after an ankle sprain. Plain anteroposterior and lateral foot radiographs showed advanced lytic changes occupying the lateral half of the navicular (Figure 1). The lesion lacked a sharp margin and was causing thinning of the cortical bone. Although it appeared expansile, the gross shape of the navicular was not altered. The adjacent bones were unremarkable.

Anteroposterior and lateral radiographs of the foot 10 weeks after trauma showing a lytic lesion involving the navicular and the talar neck.
The patient was initially treated with an injection of cortisone into the talonavicular joint. His symptoms did not improve, and further imaging showed progression of lysis in the navicular, thought to be due to infection.
The differential diagnosis included a primary bone tumor, an atypical infection, gout, and Weiss-Muller syndrome.1-3 Further investigation by computed tomography scan, magnetic resonance imaging, and 3-phase technetium bone scan confirmed the presence of an osteolytic solitary lesion in the navicular (Figure 2A and B). The patient was then referred to the senior author.
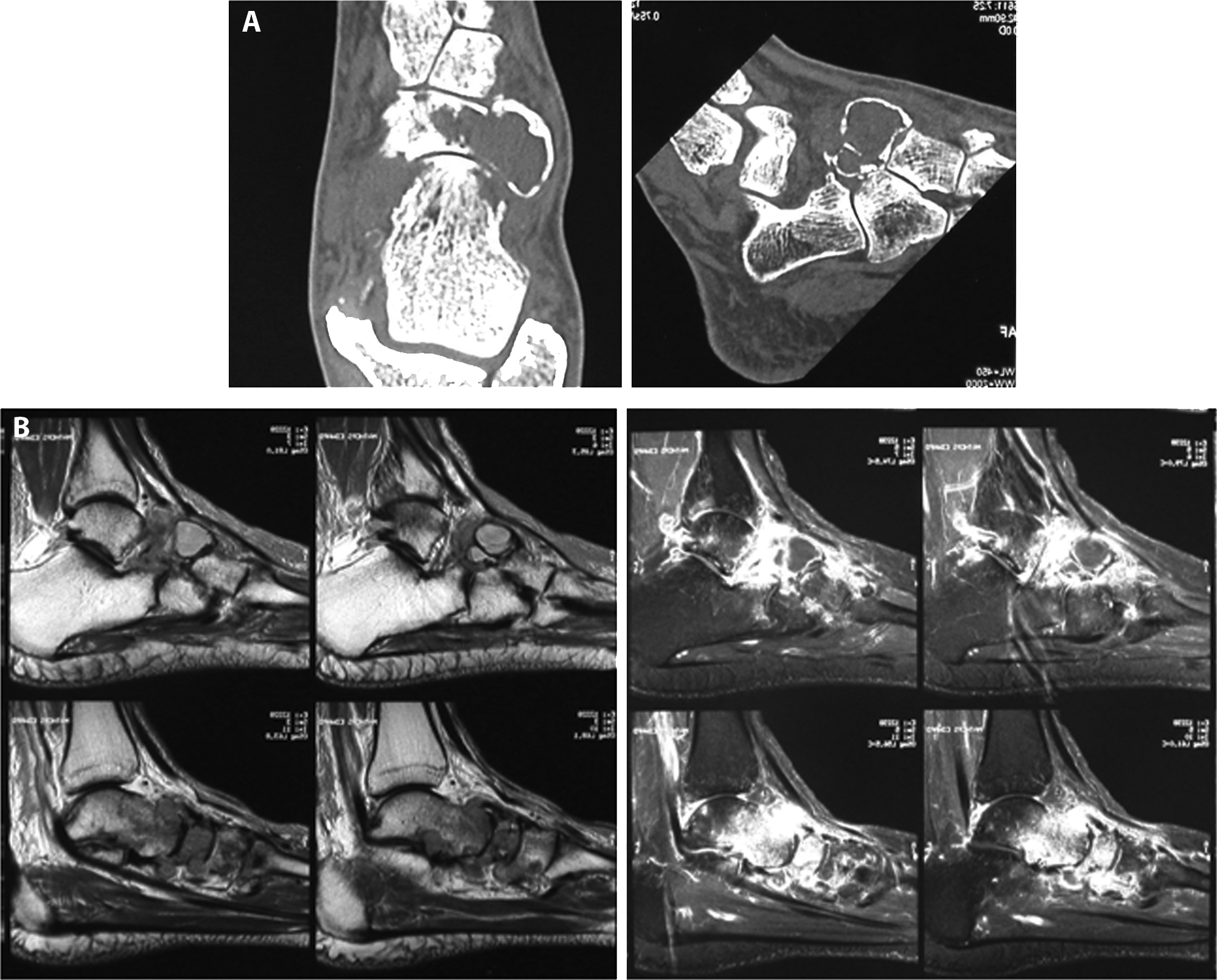
(A) Sagittal and lateral computed tomography scan of the foot at 3 months after first complaint showing a gross destruction of the navicular with interruption of the cortices and involvement of the adjacent bones. (B) Lateral magnetic resonance imaging scan T1-weighted and T2-weighted at 3 months after first complaints showing an important perinavicular soft tissue reaction.
An open bone biopsy confirmed the diagnosis of a metastatic lesion of a not yet known primary tumor. This primary adenocarcinoma in the lower left lobe of the lung was confirmed by staging; additionally, malignant retroperitoneal lymphadenopathy was diagnosed.
A musculoskeletal oncologist was then consulted. Due to the poor prognosis, the gross bony destruction, and the questionable healing potential of the region, no aggressive local treatment such as radical excision was implemented. The primary tumor was treated with a course of chemotherapy (carboplatin and gemcitabine). The patient died within 1 year after the initial diagnosis.
Discussion
This incidental finding of a rare destructive lesion of the tarsus brought us to review the current literature about the incidence, diagnostic tools, and treatment options in primary bone manifestations of malignant tumors.
Solitary bony metastases as the first presentation of a malignant tumor are very rare.4-6 This can lead to delayed presentation and diagnosis, especially with lack of symptoms of the primary tumor. 7 Similar pitfalls have been reported in the rare appearance of tuberculosis in the foot. 8 Only 8% of all primary metastatic tumors originate from the lung.9,10 In the foot, metastases are extremely rare (0.007% to 0.3%).11-14 Casadei et al have observed 11 cases of acro-metastases out of more than 13 000 musculoskeletal tumors treated between 1904 and 1988.15-17 The reasons for such a low incidence are not completely clear. Metastases to bone follow 2 different pathways: local spread or blood flow dissemination. The latter is responsible for the distal localization to hands and feet. Differential diagnoses have to been made carefully. 18
In 1997, Ozdemir et al 19 performed a retrospective assessment on 196 tumors of the foot and ankle out of 1786 bone and soft tissue tumors. Of the 196, 87.2% were benign and 12.8% malignant; 98.9% were primary and only 2 (1.1%) were metastatic tumors. One hundred forty (71.4%) of the patients underwent surgery, whereas the remaining 56 (28.6%) were treated nonoperatively. Of the 140 surgical cases, 13 (9.3%) had a recurrence, 3 (2.1%) died, and 124 (88.6%) had a clinical cure. For most of the patients who required surgery, limb preserving procedures were sufficient, whereas amputations were required for 14 patients. 19
The most recent literature review by Maheshwari et al in 2008 shows an incidence of bone involvement in foot metastases of 6.2% in 241 cases in the English literature since 1920. 5
Conclusion
In this case of an isolated adenocarcinoma metastasis in the navicular, the foot lesion eventually led to the diagnosis. Unfortunately, as in this case, the rarity of the metastatic lesions may lead the treating physician to initially consider more common diagnoses such as trauma, infection, or avascular necrosis. This often leads to delayed diagnosis, which potentially compromises patient outcome. Following tumor staging, the prognosis is often poor and the treatment is usually palliative and needs to be adapted to each patient’s individual situation.